Embed Size (px)
Citation preview

Flying Blind Without Instruments
Treating Hypertension in the Elderly
Will Bynum, MDAttending Faculty, NCC Family Medicine Residency
Fort Belvoir, VA

Outline
• Limitations of JNC-8 guidelines
• Practical approach to avoiding adverse events
• Brief overview of recommended medications
Overall Goal: to increase awareness of the complexities of treating hypertension in the highly heterogenous elderly population

CaseMrs. S is a 92 year old who you are seeing in the nursing home. No complaints today.
PMHx: HTN, HLP, CAD s/p stent in 1997, severe OA
Meds: ASA 81 mg, lipitor 20 mg, Vit D 1000 IU
Recent Vital Signs
P 75 BP 164/72P 68 BP 162/71P 80 BP 157/68
Today’s Vital Signs
P 73 RR 18 BP 166/70T 98.4
*Remainder of physical exam unremarkable*Recent labs normal

In addition to advising lifestyle change, would you
start a medication?

Treating Blood Pressure in Elderly Patients
Part I: The (mis)guidelines

What does JNC-8 say?
• In adults > 60 yo, initiate pharmacologic therapy for BP >150/90
• Treat to a goal of <150/90
• If patient is already on anti-hypertensive and SBP is less than 140, no need to stop medication if the patient is tolerating it well
JAMA. Feb 5 2014;311(5):507-520

What does “general population” mean?
What about the diastolic blood pressure?
What do these studies show and in whom?

Study Age of Participants
Mean BP of Participants
Study Population Characteristics
SHEP > 60
Mean: 71 (SD 6.7)
14% were >80 yo
170/76 Community Dwelling
94% had no impairment in ADLs
0.4% had e/o cog. impairment
Syst-Eur > 60
Mean: 73 yo (SD 6.7)
174/85 Community dwelling
MRC > 60
Mean: 70.4
180s/90s Community dwelling
Meta-Analysis
(8 studies)
> 60 174/83 Community dwelling
The DataRandomized Controlled Trials
Primary Finding
36% reduction in stroke
13% reduction in all-cause mortality
42% reduction in stroke
31% reduction in non-fatal CV events
25% reduction in stroke
17% reduction in all CV events
Active treatment…13% reduction all-cause18% reduction CV deaths30% reduction stroke23% reduction coronary

What about patients >80 years old?
HYVET Trial

HYVET Trial

The HYVET Trial – Results
• 30% reduction in non-fatal stroke• 39% reduction in stroke-related mortality• 21% reduction in all-cause mortality• 29% reduction in CV-related mortality• 64% reduction in CHF incidence
• Fewer adverse effects in the treatment group (358) than the placebo group (448)
NEJM 2008;358(18)1887-98

Inclusion Criteria - AGE Age >80
Inclusion Criteria - BP SBP > 160, DBP < 110
Exclusion Criteria Secondary HTN, hemorrhagic stroke in last 6 months, heart failure requiring an anti-HTN med, Cr >1.7, diagnosis of clinical dementia, and a requirement of nursing care
Who was actually enrolled?
80 – 84 yo: 74%
>90 yo: 4.6%
85 – 89 yo: 22.4%
Who was actually enrolled? Mean BP: 173/90
This study best applies to a patient… • who does not have dementia
• who does not have a borderline DBP
• in his/her early 80’s • who is functional
HYVET – a deeper look

The (mis)guidelinesRe-cap
• HTN studies in the elderly only represent a healthy subset of the population
• Guidelines do not take heterogeneity into account
• Thus, the guidelines may not apply to the patient in front of you

Treating Blood Pressure in Elderly Patients
Part II: First do no harm?

First Do No Harm
The Mortality Curve J

The Lancet. 1987;329(8533):581-584
Mortality & MI

Annals of Internal Medicine. 2006;144(12):884-893
Data from the INVEST trial
Mortality & MI

Low diastolic blood pressure is associated with increased risk of mortality and MI
There is no evidence that sets a safe minimum DBP
Expert Opinion: In the elderly treat to a minimum DBP of…• 60 in patients without CAD• 65 in patients with CAD
Mortality & MI

Gait Speed & Mortality
Gait speed is a “strong and consistent predictor of adverse outcomes” in community-dwelling older people”
Slowed gait speed is a predictor of functional disability
Also a marker for falls and increased mortality
The Journal of Nutrition, Health & Aging. Dec 2009;13(10):881-

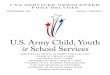
Fast Walkers
Slow Walkers
No Walkers Archives Intern Med. 2012;172(15):1162-1168
<4 seconds to walk 10 feet
>4 seconds to walk 10 feet
Unable to participate in test
2,340 patients >65 years old

Fast Walkers: Elevated SBP (>140) associated with increased mortality risk (OR 1.35)Slow Walkers: no association between elevated BP and mortality
No Walkers: Elevated SBP (>140) and DBP (>90) associated with decreased mortality risk (HR 0.38 and 0.10)
Gait Speed & Mortality
Archives Intern Med. 2012;172(15):1162-1168

Gait Speed & Mortality
Use gait speed to help determine if your patient is a good candidate for anti-hypertensive therapy
• Consider therapy in fast walkers• Use extreme caution in non-walkers
BP >140/90 appears to be most protective in patients with significantly lower functional ability

Incidence of orthostasis in 21% (Syst-Eur) and 17% (SHEP) of patients after starting treatment
The Lancet. 1997;350(9080):757-764JAMA. 1991;265(24):3255-3264
Orthostasis is associated with increased risk of…• Falls• Future CV events• Congestive heart failure• Incidental atrial fibrillation
Hypertension. 2010;56(1):56Hypertension. 2012;59(5):913-8J Intern Med. 2010;268(4):383-9
J Am Geriatr Soc. 2011;59(3):383-9 Am J Med. 2000;108(2):106-
111
Orthostasis

Screen for orthostatic hypotension…
• BEFORE starting anti-hypertensives in the elderly
• In patients already on anti-hypertensives who have borderline blood pressure
Orthostasis

Being on an anti-hypertensive is a known risk factor for falls (OR 1.2 – 1.4 if no prior fall, 2.1 – 2.3 if prior fall)
Arch Intern Med. 2009;169(21):1952
JAMA Int Med 2014;174(4):588-95
Falls are strongly associated with hip fractures• 90% of hip fractures in the elderly occur
following a simple fallBaumgaertner MR, Higgins TF. Femoral neck fractures.
Falls & Hip Fractures

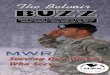
Arch Intern Med. 2012;172(22):1739-1744
• Case series that evaluated association between initiation of an anti-hypertensive in the elderly and risk of immediate hip fracture after initiation
• Average age of patients = 81 yo. All were community dwelling
Falls & Hip Fractures

Falls & Hip Fractures

Falls & Hip Fractures
Increased risk of hip fracture in the 45 days following initiation of therapy (OR 1.45 for all classes)
Beta blockers (OR 1.58) ACEI/ARBs (OR 1.53)
Thiazides (OR 1.33) CCB’s (OR 1.30)
Consider the patient’s fall risk when makingthe decision to start an anti-hypertensive
Mitigate other falls risk factors, especially in the first 45 days after initiation of therapy

Re-CapUse caution in starting/continuing anti-hypertensive therapy in the following:
• Borderline diastolic BP (60-65)• Low functional status• Increased falls risk • Underlying orthostatic hypotension• Non-community dwelling • Old old (>85 yo)
Permissive systolic hypertension appears to be protective

Treating Blood Pressure in Elderly Patients
Part III: The meds

MedicationsInitial Monotherapy
• Thiazides: appear to be the best overall 1st line choice
• CCB’s: 1st line but may have increased risk of heart failure
• ACEI/ARBs: acceptable but best used as 2nd/3rd line
• Avoid Beta Blockers & Vasodilators as 1st line treatment
JAMA 2002;288(23):2981-2997

MedicationsCombination Therapy
• ACCOMPLISH trial (mean age 68, mean BP 145/80) showed…ACEI + CCB >> ACEI + Thiazide
NEJM. 2008;359(23):2417
• ESH/ESC & JNC-8 recommend any combination of ACEI, CCB, and thiazide

Putting it All Together
• The decision to treat, not treat, or continue treatment in elderly patients is very complex
• The guidelines are based on studies of community-dwellers who were more or less healthy, young-old, and with mean SBP 170-180
• The benefits of treating SBP >160 are tremendous in relatively healthy, community-dwelling, young-old patients
• However, hypertension may be protective, especially in patients with lower functional ability

• The data shows a consistent association between low DBP and mortality. Remember 65 & 60
• Other risks include MI, falls (especially 1st 45 days), and orthostasis
• Start treatment with a thiazide in most patients. Calcium channel blockers are also first line option
• Any combination of thiazides, CCBs, and ACE/ARB is acceptable
Putting it All Together

Questions?