Embed Size (px)
Citation preview

Dr Alison
KnowlesCertifying Consultant and
Abortion Provider
16:30 - 17:25 WS #83: Abortion - Where We Are Now
17:35 - 18:30 WS #95: Abortion - Where We Are Now (Repeated)
Ms Kathy
Le Haavre

FIRST TRIMESTER ABORTION
Dr Alison Knowles
Kathy Le Haavre

ABORTION
WORKSHOP 1. PERSPECTIVES FROM THE PAST , FOUNDATIONS FOR THE FUTURE.
2. FIRST TRIMESTER MEDICAL ABORTION.
3. WHAT WE WANT FROM YOU.
4. WHAT DO YOU WANT FROM US ?

Perspectives from the Past
Foundations for the Future


PRE 1978
Abortion was illegal
Abortionists were fined and went to prison
Women had backstreet abortions
Women died from abortion
Women became infertile because of unsafe abortion
Women had forced adoption
Newborns were taken off their mothers and sent to orphanages
Women flew to Australia to get abortions
1977-1978
Royal Commission on Contraception, Sterilisation and Abortion
Contraception, Sterilisation and Abortion Act 1977
Crimes Act 1961

1978 -
CURRENT
Abortion is ‘sort of’ legal
Abortion is safe
Services have developed ad-hoc
Huge variation in service delivery between DHBs
DHBs have dropped the ball and outsourced the work
Abortion rates have increased and decreased
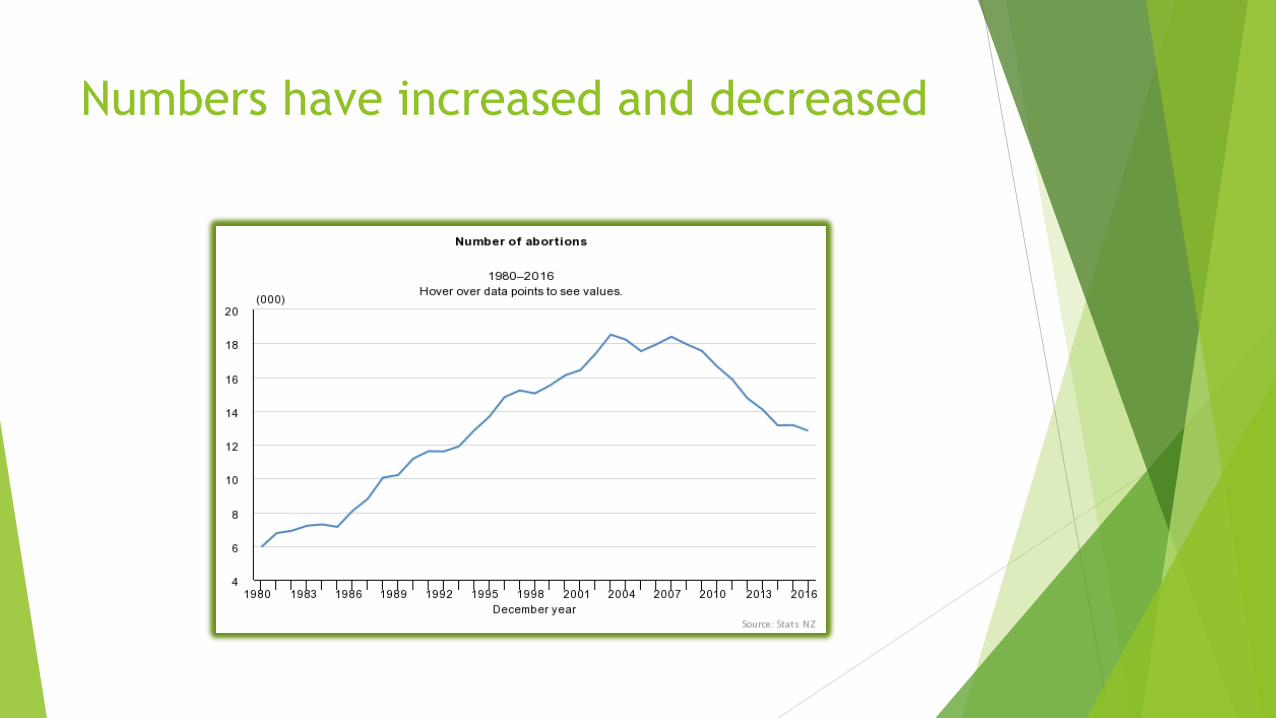
Numbers have increased and decreased



1979
2019

PERSPECTIVES FROM THE PAST
1940 1980 2017
Aotearoa NZ
population
1,700,000 3,100,000 4,800,000
Abortions 4,000 5,945 13,285
Abortions per
100,000
235 191 276
Deaths from
abortion
22 0 0
Head of State King George VI Queen Elizabeth II Queen Elizabeth II
Governor
General
Sir Cyril Newall Sir David Beattie Dame Patsy Reddy
Prime Minister Peter Fraser Robert Muldoon Jacinda Ardern
Chief Justice Sir Michael Myers Sir Ronald Davison Dame Sian Elias
O&G trainees NZ RCOG Mainly men RNZCOG Mainly men RANZCOG 90%
women
GP trainees NZ RNZCGP 63% women

AD HOC DEVELOPMENT OF SERVICES Pre 2000 - patients from Midcentral, Bay of Plenty, Hawkes Bay,
Lakes, Tairawhiti, Taranaki, Waikato, flew or drove to AMAC in Auckland.
2000 - WDHB started a service which served Waikato, Lakes, and Bay of Plenty. AMAC workload almost halved overnight.
2000 – current - Waikato DHB outsourced the doctoring part of abortion care to a private contractor. Abortions provided in Hamilton, Tokoroa, Thames
2013 – Tauranga FP started EMA. Waikato workload reduced significantly. Thames lists alternate weeks.
2018 – Waikato DHB closed Tokoroa abortion service, Lakes DHB opened a service. Waikato workload reduced again.

BUILD IT AND THEY WILL
COME
TAURANGA FAMILY PLANNING – ABOUT 250 PER YEAR since
2013
ROTORUA WOMEN’S HEALTH CLINIC Te Aka Tauawhi Tangata
600 IN FIRST YEAR 2018

BUILD IT AND THEY WILL COMELakes DHB First Trimester Service : OUTCOMES First 52 weeks
MTOPS 151
STOPS 443
TOTAL 594
Minimum gestation 4w5d
Maximum gestation 13w6d
Mean gestation 9w0d
Mean STOP gestation 9w4d
Mean MTOP gestation 7w1d
Mean wait from referral to TOP 9.2d
Clients discharged with LARC 60%
Women under 9w who chose MTOP 58%

PERSPECTIVES FROM THE PAST tick
FOUNDATIONS FOR THE FUTURE tick
WHERE WE ARE NOW
Minister of Justice to Law Commission :
Please review:
1. Criminal aspects of abortion law
2. Statutory grounds for abortion
3. Process for receiving services

ALTERNATIVE APPROACHES TO ABORTION LAW. Ministerial Briefing paper.
MODEL A No statutory test must be
satisfied before an abortion
could be performed.
The decision to have an
abortion made by woman in
consultation with her health
practitioner
MODEL B A statutory test would need to
be satisfied but the test would
be in health legislation rather
than Crimes Act.
The test : the health
practitioner who performs
abortion would need to believe
the abortion is appropriate in
the circumstances, having
regard to the woman’s physical
and mental health and
wellbeing
MODEL C For pregnancies of not more
than 22 weeks gestation – same
as MODEL A
For pregnancies of more than
22 weeks – same as MODEL B

NOW IT’S UP TO
PARLIAMENT
CONSCIENCE VOTE

IF WE DID GET DECRIMINALISATION……..
PERFECT ABORTION CARE IN AN IMPERFECT WORLD
1. AVAILABLE tick
2. SAFE tick
3. LEGAL tick
4. FREE tick
5. WOMEN CENTRED – CHOICE – ACCESS – QUALITY work in progress

Why you should consider providing
abortion care ?
CHALLENGING WORK
REWARDING WORK / GRATEFUL PATIENTS
GREAT WORK STORIES
SESSIONAL WORK / PART TIME WORK
LIMITED OR NO ON CALL / AFTER HOURS WORK
TEAM WORK – counsellors, social work, nursing, medical

CHALLENGING WORK
Doing an ERPOC awake on every women you meet
No anaesthetist – the buck stops with you – resuscitation (over sedation, anaphylaxis, haemorrhage) , difficult IV access
Past year : * phaeochromocytoma
* tubal ectopics
* scar ectopic
* methamphetamine (fidgety, talkative, aggressive, irrational)
* heterotopic pregnancy
* STOP down to under 5 weeks and up to 14.0 weeks
* post STOP/MTOP haemorrhage
* quadruplets at over 12 weeks
* fetal abnormality
* morbid obesity
* multiple LSCS / LLETZ scarring

A DAY IN THE LIFE OF…
WEDNESDAY 1. 26Y Maori 7w1d G5P3M1 (2NVD 1LSCS- whangai) PPHX1 2U transfusion.
Working part time. Partner student, completed family. Rental with 2 kids and partner. STOP + MIRENA
2. 19Y NZE/Maori 12w0d G1P0 Unemployed, applying for a course. Pregnant to BF. STOP + JADELLE
3. 27Y NZE 13w6d G3P1T1 (1NVD not in her custody 1 MTOP) High on methamphetamine, agitated, fidgety, poor concentration. Went AWOL 1 hour after miso. Didn’t reply to calls or texts. Referrer notified, SW notified.
4. 24Y Canadian. 10w5d G1P0 Working holiday, BF in Australia. STOP + No contraception
5. 39Y NZE 10w3d G2P0M1 Never wanted children. STOP + NFP
6. 31Y CookIsMaori 14w0d G8P4T1M2 4NVD(1 stillborn 27w, 1STOP, 2 miscarriages (one at 19weeks). Use oven to heat house. STOP + MIRENA
7. 25Y NZE 5w3d G1P0 Lives with partner who has 2 kids and shared custody, works fulltime in café. MTOP + COC
8. 16Y NZE 6w0d G1P0 High School. STOP + COC
9. 26Y NZE 8w1d G4P2M1 Left abusive relationship with father of children in February. Has split with FOP. MTOP + DP
After work checked MTOP HCG results from last week – one MTOP failure. Same day mife/miso @ 5w6d. HCG#1 32,000 (16May) HCG#2 60,000 (22May)
REWARDING WORK
Grateful patients – these are the very same women you care for at every
other stage of their lives.
During a day at work you hear up to 12 stories of 12 decisions, some agonising
and some straightforward, but none of them taken lightly.
You are helping patients at a very difficult time. There is nothing more
personal and private for a woman than deciding whether to continue a
pregnancy and have a baby or end a pregnancy by having an abortion.

GREAT WORK STORIES
Drugs
Abuse (physical/sexual/emotional)
Poverty
Tragedy
Crime
Migration / dislocation
Alcohol
Rape / Incest
Poor physical health
Fetal abnormality
Ambition
Depression / anxiety
Bad luck
Grief

TEAM WORK

WOMENS HEALTH CARE
INCLUDES ABORTION CARE
GPs PROVIDE MOST OF THE
WOMENS HEALTH CARE IN NZ
ABORTION CARE IS WOMENS
HEALTH CARE





























