Embed Size (px)
Citation preview
Fieldwork Site Profile (FS-PRO): Learning Opportunities and Resources
I Please fill in and return to your affiliated university occupational therapy program.
I Site and Contact Information
Name of site: MUHC (McGill Universitv Health Centre) 1 Name of programlsector: MNH (Montreal Neurological Hospital) and RVH (Royal Victoria Hospital)
Name of contact person: Priscilla Lam Wai Shun
Title of contact person: Occupational Therapist, student coordinator MNH and RVH
Address: Royal Victoria Hospital, O.T. Department local A3.20 I 687 PINE AVE WEST, H3A 1Al
Phone*: (514) 843-1 573 Fax': (514) 843-2881
E-mail address': [email protected]
Web site: nla I Supporting material about the site and occupational therapy services attached
(e.g. pamphlet, brochure, fact sheet) *of contact person
If you have any questions or comments, please contact your university representative:
The MUHC is a fusion of 5 hospitals. The Montreal Children Hospital is a stand-alone; all adult
services are integrated under one director. For the purposes of clinical supervision, adult services are organised in 4 sections. Each section has its own
FS-PRO, namely: , - Physical Medicine MGH: Francine Desrosiers
(Responsible) -Physical Medicine RVH*: Priscilla Lam
(Responsible) -Psychiatry MGH: Hiba Zafran
A member of the , -Psychiatry RVH-AMI: Hiba Zafran Coordinators *includes MNH and MCI . . .. . - -. . . - .. . . . . .- . - .- .. . . . . . . . . -. . . .. . ... . ... .. . .. .. -. .. . , . . - .. . .. . . . . .. .. . . ., , . .- . , . ,... . , , - . , . . , . . .. . ,. , , , . . , . . .. . , . , , , ... ,
a sub-committee of
University Fieldwork Committee (UFCC) ,
the Association of (2005 revised edition)
Fieldwork Site Profile (FS-PRO): Learning Opportunities and Resources
Copy and complete for individual location or program as appropriate.
Name of program 1 site: (if different from page I ) :
Characteristics of Occupational Therapy Services:
Contact information if different from page one:
1. Occupational therapy services are organized on: (XI an O.T. department basis a program basis
Location of occupational therapy services in the building:
No O.T. on site other:
Description (e.g. the mission and vision of your organization, occupational therapy philosophy and role of occupational therapy within your organization): The MUHC represents the first and largest voluntary merger of university teaching hospitals in
Canada. The partners include the McGill University Faculty of medicine, four institutions serving adult patients (Montreal General Hospital, Royal Victoria Hospital, Montreal Chest Institute and the Montreal Neurological Hospital) and the Montreal Children's Hospital. The vision of the MUHC consists of a facility offering care of the highest quality to patients of all ages and offering continuity of care across settings in the health network. The patient and family are central to the way care is organized. They are encouraged to participate actively in the healing process. Patient care is coordinated by multidisciplinary teams working to treat patients with increasingly complex problems.
I Occupational Therapy Philosophy OT services are offered in a client centred model where the client is encouraged to be an active
participant in his therapy. We believe that a balanced integration of physical, cognitive, social, cultural and spiritual elements is essential for restoration of health. We promote collaborative decision-making within interdisciplinary teams because we believe that this is essential for effective care. Occupational therapists are encouraged to participate in ongoing education and professional development as well as in research activities because we believe that evidence- based practice will lead to improved delivery of services to clients.
Role of OT within the MUHC The McGill University Health Centre is a tertiary, acute facility, which employs over 40
Occupational Therapists in the adult sites. OTs are members of a variety of multidisciplinary teams and they work closely with other health care professionals to facilitate prompt and appropriate discharge of inpatients, back to their homes andlor to other health care institutions in the community, depending on their needsllevel of independence. In outpatient clinics, OTs assist patients in resuming or maintaining occupational performance.
2. System(s) / services in which you practice: Public sector Private practice
UFCC- ACOTUP Fieldwork Site Profile: Learning Opportunities and Resources - E-version - 2005 Revised Edition
Rehabilitation centre [XI Outpatient clinic [XI Hospital Long term care centre IXJ Home care IXI Day hospital Insurance industry IXI Community setting School
Other:
3. Occupational therapy roles: IXI Direct care IXI Indirect care Consultation [XI Research
[XI Administration IXI Other: Teaching
4. Client life span: Children Adolescents IXI Adults Older adults
Fieldwork Site Profile: Learning Opportunities and Resources - E-version - 2005 Revised Edition 3
Characteristics of Occupational Therapy Services (continued):
5. Client conditions: Mental health Physical health Combined Other
Please list common client issues :
1 . Physical andlor cognitive impairments
2. Ability to manage basic ADLs
3. Ability to perform IADLs
4. Safety for DIC home and or need for outpatient Flu andlor need for inpatient rehabilitation
Most frequently seen diagnostic categories:
-Surgery
-plastic surgery
-0rthopaedic surgery (hip replacement, etc.) (MGH only)
-vascular surgery
-transplant
-ear, nose and throat specialities
-Medicine
-general medicine (de-conditioning, pneumonia, etc.)
-rheumatology
-cardiology (chronic heart failure, etc.)
-active geriatrics
-palliative care (MGH only)
-hematology I oncology
-Respiratory
-Acute and chronic pulmonary conditions (COPD, etc.)
-Neuroscience
-Neurology (multiple sclerosis, stroke, etc.)
-Neurosurgery (brain tumors, spinal stenosis, etc.)
-Traumatic Brain Injury (MGH only)
-Epilepsy
6. Occupational therapy focus:
UKC- ACOTUP Fieldwork Site Profile: Learning Opportunities and Resources - E-version - 2005 Revised Edition 3
I Site:
Please describe common areas of practice, interventions and programs :
Occupational therapy is a practice that utilizes the analysis and application of functional activities in order to promote andlor maintain independence in the areas of self-care, productivity and leisure. Occupational therapy components (physical andlor cognitive status mainly) as well as the patients' environment and their impact on occupational performance are assessed. Through the interpretation of evaluations, a plan of intervention is developed in collaboration with the patient, family and other members of the interdisciplinary team. For the inpatient population, the goal of the intervention is to promote functional independence and facilitate a prompt and safe discharge. For the outpatient population, the goal of the intervention is to facilitate participation in occupational performance. The Canadian Model of Occupational Performance is used as our frame of reference. Different models of practice (biomechanical, rehabilitation, motor control, neurobehavioral, etc.) are used to guide our interventions. The choice of the model depends on the patient's diagnosis.[:
Program Description
MEDICINE
There are 5 therapists to cover all medical referrals (RVH and MGH). Typical client groups include respiratory (COPD) pneumonia, CHF, general de-conditioning and oncology. Clients are primarily referred for functional assessments to evaluate safety and ability to return home. The functional assessment includes evaluations of eating and feeding. When patients are experiencing swallowing problems (dysphagia) the OT performs a bedside assessment and occasionally Modified Barium Swallows are used. ADL evaluations, IADL screening (Barthel index), Driving Screening (Trail making A and B, Bell, MVPT, etc.) and recommendations for improving function are provided. Periodic re-evaluation is done as time permits. The average L.O.S. is 11 days and about 3 weeks for complex clients.
SURGERYIORTHOPAEDIC
Types of patients include cardiac, transplant, polytrauma, multiple #'s, amputees, and spinal cord injury. Four staff are allocated to the in-patient surgical population (Note: orthopaedic is exclusive to the MGH). The OT's role is to assist in determining functional capacities, provision of aids, positioning splints (e.g. footdrop) and facilitating discharge from hospital to home, rehab centre, or LTC residence.
ACUTE GERIATRICS
Services are provided by one full time OT in both the MGH and RVH, where a strong interdisciplinary approach is used. Family meetings and education to caregivers is an important part of the service. The overall goals are to increase functional autonomy and to co-ordinate discharge planning. Referrals are from the Emergency room and in-hospital transfers from other wards. Clients are generally 75 and over, frail, with general deterioration of function. Typical admissions are for falls, acute confusional states, dementia work-up, pneumonia and de- conditioning. Transfers from other floors include post MI and post fracture clients. Typical evaluations used include Barthel, OARS, cognitivelperceptual screening and dysphagia evaluation. Average L.O.S. is 40 days.
I GERIATRIC DAY HOSPITAL
The OT at the RVH is a member of an interdisciplinary team, and is responsible for the assessment, planning and implementation of specific treatment for a geriatric out patient population. This includes preventing disability, and assisting clients to achieve optimum function and independence in ADL, IADL and mobility, in a clientele with physical and mild cognitive impairments. The OT completes an evaluation with recommendations, provides rehabilitation and re-assessment when indicated, and undertakes home visits to assess safety and function when necessary. The OT at the GDH also participates in team meetings, and participates in decision-
UKC- ACONP Fieldwork Site Profile: Learning Opportunities and Resources - E-version - 2005 Revised Edition
making and problem solving with other team members. Assessment reports include functional and measurable goals, and outcome measures are regularly used in assessment and in clinical decision making. The average length of stay can vary from 2-4 weeks for an evaluation to 3-4 months for rehabilitation.
1 TRANSITIONAL CARE UNIT
A part-time OT offers services to long term care patients (0.5 F.T.E on the S7W unit of the RVH) and by consultation (geriatric OT) at the MGH. Patients are awaiting placement in a long-term care facility outside of the acute care hospital. The OT is an active member of the multidisciplinary team. Interventions undertaken by OT include dysphagia assessmentlrecommendations, positioning and wheelchair clinics, functional re-assessment and recommendations to improvelmaintain autonomy and quality of life on the unit. The average length of stay of patients is 2-4 months.
I NEUROSURGERY
Occupational Therapists provide services to the neurosurgery in and out patient population of the MNH. The vast majority of patients are seen on an in-patient basis and suffer from a wide variety of conditions such as cerebral haemorrhage, aneurysm, brain tumour, spinal stenosis andlor compression, etc ... The main goal of OT is to monitor patients' functional status pre and post- operatively and asses ADL in order to assist with decision making pertaining to discharge planning. The OT acts as a consultant on the pre-admission and peri-operative unit and is an active member of the brain tumour multidisciplinary team.
I NEUROLOGY
Neurological clients are located on the 14th floor of the MGH as well as at the Montreal Neurological Hospital. Typical clients suffer from CVA, MS, ALS, Guillain Barre Syndrome, myasthtenia gravis, neuropathy and spinal cord injuries. Evaluations include eating, feeding and dysphagia (bedside exam and occasionally MBS), general motor assessment (ROM, balance, strength, co-ordination), ADL function (Barthel, in-house evaluation), cognitivelperceptual function (OSOT, PECPA, MOCA, MMSE, CCT). Most patients are seen on an in-patient basis and the overall goals of OT are to improve ADL independence and to assist with appropriate discharge planning. The length of stay varies with condition, but the average for the Neurosciences is 12 days. Strong multidisciplinary approach is used.
I OUT-PATIENTS
Five occupational therapists (MGH and RVH) offer services to the hand injured out patient population. The majority of the caseload is referred by plastic surgery, but referrals are also received from rheumatology, orthopaedics and out patient clinics. The OT assists the client in the evaluation and treatment of oedema, scar adherence and hypertrophy, decreased range of motion and strength, impaired sensation, etc ... The focus is to return the client to this former level of functioning in selfcare, work and leisure activities. The OT's are an integral part of the plastic surgery team and cover the plastic surgery clinics.
INPATIENT-PLASTICSThe inpatient plastic referrals are seen by the hand specialists at the RVH and MGH. Referrals include individuals with trauma of the hand (e.g. burns, replantation and severe fractures). The average length of stay for these clients is 3-5 days, with out patient follow- up afterwards. OT interventions consist primarily of splinting to immobilize and protect healing structures and early range of motion if applicable to prevent stiffness and deformities. A multidisciplinary approach is used.
Hours of operations: Normally 8:00 AM to 4:00 PM ; Monday to Friday
1- ACOTUP Fieldwork Site Profile: Learning Opportunities and Resources - E-version - 2005 Revised Edition
Site. -
Learning Opportunities and Resources for Students:
1. Access to a library (either on or off-site) : yes no
2. Internet access: yes no
3. Other learning opportunities and resources for students (please list):
(e.g. interprofessional contacts, field trips, resource binders): Listed below are a variety of opportunities and activities in which students may become involved during their stage at the RVH or MNH. Not all these opportunities or experiences may be relevant depending on the learning objectives. Equally they may not be possible given time constraints. It is suggested students review and discuss these opportunities with their supervisor. - RVH library : 4'h floor, Hershey Pavillion - MNH library :2nd floor - Textbooks are available in the department for reference -Ward Rounds - In-service Education (in OT dept. or within programs) - Grand Rounds - Presentations (from suppliers of medical equipment) - Meetings with other health care professionals - Utilization of standardized evaluations (e.g. Jamar dynamometer, MMSE, Bells test, PECPA, etc.) - Fabrication of splints (mainly in outpatient hand therapy) -Wheelchair and positioning clinics - Utilization of patient education tools (e.g. energy conservation pamphlet, etc.) - Observation of surgery
4. Please state your general learning and performance expectations of students (other then the ones from the University) to assist them in preparing for fieldwork education at your site.
UFCC- ACOTI.JP Fieldwork Site Profile: Learning Opportunities and Resources - E-version - 2005 Revised Edition 7
8 uo!a!p3 pas!~atl sooz - uo!sla~-3 - sa3~nosay pue e!l!unvoddo Bu!u~ea~ :alyo~d a~!s yo~pla!j dM03V -333ll
-
spe~y.~o~ luapnls JOJ wnpuappe aaS
1. Orientation session offered upon students arrival:
yes no, it will be available on (specijl date):
2. Space and resources available to students (phone, desk, computer, work station, etc.):
Desk, chair, locker, computer, phone
3. Policies and procedures information available:
IXj yes, location: O.T. Department A3.20
no, it will be available on (specijl date):
4. Health and safety policy in place:
IXl yes no, it will be available on (specijl date): O.T. Department A3.20
5. Emergency procedures information available:
IXj yes, location: O.T. Department A3.20
no, it will be available on (specijl date):
6. Contingency plan available (for absent fieldwork educator during placement):
no, it will be available on (specijl date):
yes. Please outline its major characteristics:
Supervisory Contingency Plan
Whenever the supervising occupational therapist is absent, arrangements will be made for the student to be supervised by one of the other occupational therapists. In the event of long term absence from the supervising therapist (longer than 5 days) the student's supervision and evaluation will be reassigned to one of the other occupational therapists.
I Site
I
I
I
I
I
Administrative Resources:
UKC- ACOTUP Fieldwork Site Profile: Learning Opportunities and Resources - E-version - 2005 Revised Edition 9
Administrative Resources (continued):
7. Continuing education plan in place for occupational therapists on site:
no, it will be available on (specify date):
yes. Please outline its major characteristics:
Please outline your site's continuing education policy or describe how occupational therapists remain current in issues that impact their professional practice. Also, describe use of evidence based practice:
1. See attached copy of Department Policy and Procedure on Professional Development.
1 2. List of courses attended by staff in the previous fiscal year which supports the above policy.
3. In addition to the above, on a personal basis one staff is presently pursuing post-graduate studies for a Masters degree in bioethics.
1 4. In-service in OT dept. and journal clubs within programs
5. Financial support is also available though bursaries awarded by MUHC
OT interventions at the RVHIMNH change with each new evidence brought forth by OT staff (information obtained at conferences or in literature for example). Review of literature combined with clinical expertise are key factors in the discussions regarding new suggested intervention approaches.
Amenities Available to Students:
1. Cafeteria: yes no
2. Kitchen facilities: IXl microwave oven IXI refrigerator other: stove
3. Locker: yes no
4. Bicycle rack: IXl yes no
5. Parking: IXl yes, cost: 15$ per day no
6. Public transportation available: yes no
7. Other (please list):
UFCC- ACOTUP Fieldwork Site Profile: Learning Opportunities and Resources - E-version - 2005 Revised Edition 6
Site Requirements for Students:
1. Immunization: (XI yes no If yes, specify in box below.
2. Criminal 1 police record check: yes IXJ no If yes, specify in box below.
3. Dress code: (XI yes no If yes, specify in box below.
4. A car is required during placement hours: yes no
If yes, describe the site "gas reimbursement" policy for OT students, in the box below.
Please specify additional information andlor requirements (e.g. mask fit testing):
Immunization as per University policy
Students are expected to dress in a professional manner (No jeans, no bellies!,no cleavage, no see
throughs, no flipflops, no shorts, no halter tanks, minimal jewellery, closed shoes to protect from
injury)
1. Please call, write or email clinical coordinator AT LEAST one week prior to start of stage
2. Reports: At mid term you will be expected to give verbal feedback to your supervisor. For the final report you will EXCHANGE reports, with your supervisor. You will PRIOR TO THIS MEETING have completed and printed a copy of the McGill evaluation, as well as the department evaluation. The department appreciates receiving honest feedback so we can improve the learning opportunity and your honesty cannot influence your report, as it has already been written.
3. Review notes from courses such as "Assessment of performance" and "Functional anatomy" (please discuss with student coordinator if needed)
I . Pre-placement information package sent to student (e.g. reading list or material, schedule): yes no
Sisnatures:
Profile completed by: Priscilla Lam Wai Shun, Clinical coordinator RVHIMNHIMCI date: 2006102109
(Name and title)
UFCC- ACOTUP Fieldwork Site Profile: Learning Opportunities and Resources - E-version - ZOOS Revised Edition 8
S~te
My organization wishes to offer placements to occupational therapy students from:
(XI my affiliated University [XI Canadian universities (X1 International O.T. programs
For fieldwork education purposes, I hereby authorize my affiliated university occupational therapy program to forward the information included in the FS-PRO to students and fieldwork coordinators from other occupational therapy programs.
I shall ensure that students will be supervised by qualified occupational therapists who have a minimum of one year of professional experience, and hold credentials with their provincial regulatory body.
Signature: date:
UFCC- ACOTUP Fieldwork Site Profile: Learning Opportunities and Resources - E-venton - ZOOS Revised Edition 9
Addendum:
Please note the following requirement for all MUHC (network) placements
MANDATORY pre-requisite
All students must complete the OASIS training module in advance of beginning their assigned clinical course at an adult MUHC site. All supervisors expect students to be familiar with the MUHC electronic charting system.
Please refer to this link:
http://formationoacis.com/muhc/
Student must advise the AACCE once they have completed these mandatory on-line modules.
r . - -
Centre universitaire de santt McGill McGill University Health Centre
.c-
POLICY AND PROCEDURE OCCUPATIONAL THERAPY SERVICES - MUHC
PAGE: 1 OF: 2
1 TITLE: PROFESSIONAL DEVELOPMENT
EFFECTIVE DATE REVISION # REVISED DATE SECTION: 8 TEACHING EDUC. & PROFESSIONAL DEVELOPMENT
POLICY1 PRcXEDURE #: 8.3
POLICY: The MUHC is committed to improving the skills and knowledge of employees, to enhance their contribution to patient care, as well as to increase employee job satisfaction and development. The employee is equally responsible (see code of ethics and job description) for self-continuing education to ensure competence and develop proficiency in the therapeutic areas of their profession. It is therefore, expected that all staff will attend and participate in the educational inservice program within the department as well as attend continuing education programmes offered to professional groups internal and external to the institution.
When possible (financial restraints as well as coverage issues) each employee is accorded study leave comparable with the number of hoursldays worked per week. This is not in the collective agreement and may be recinded. If the course occurs on a day when a part-timer is not scheduled to work, then they can a) take the course on their own time or b) take a scheduled work day off in lieu of or c) request to be paid an
, additional day.
If a course is held on the weekend (either one or both days) time off in lieu from the therapist's professional development bank can be taken. But it MUST be taken immediately before or after (i.e. not a week later).
Every staff member has a schedule (days and hours of work). Unless there is a stat holiday, approved vacation or leave of absence all staff are thus expected to be "at work".
Time reported on the Non Patient Care Activities (NPCA) sheet for professional development, education etc. are activities LESS THAN 2 HOURS e.g. participation in Grand Rounds, department in-services etc. Regardless of location (internal or external to the MUHC) if more than two hours will be spent on NPCA activities a request for time off must be submitted and approved PRIOR to the event. Failure to do so may result in non-payment of the time spent away from the job.
Staff MUST get approval for TIME OFF and before proceeding to requestlsubmit for funding. Focus for staff development and allocation of resources (pending availability) is dependent or identified through QA activities, performance appraisals and hospital and department needs.
Staff are encouraged to apply for Grants and Bursaries. 7) Gustav Levinschi Foundation Award: Aim - to provide funds for staffing, equipment or other materials
for projects which cannot be established due to lack of funding. It is anticipated that the project will be funded in the future through other means. Applications to request funding will be sent to departments beginning of October to be submitted mid November (RVH ONLY).
2) Aitken or *Laidley Fellowship Awards (members des ordres only): Aim - help professionals in their training and increase expertise. Candidate expected to contribute a new skill or body of knowledge. Applications to request funding will be sent to departments beginning of April to be submitted mid May (RVH ONLY).
3) Muldisciplinary Council: Aim -these bursaries are to be used by ALL members of the MDC within the MUHC to attend a conference, workshop, course or to being in a speaker on a particular topic. Applications to request funding will be sent two timelyear 1 - August due mid September 2 -January due mid February
When possible department resources will be made available to support staff in addition to the paid time off.
PROCEDURE: 1. Each section of the department will maintain a list of ward rounds and meetings. Participation is
encouraged when time away from patient treatment permits. Time spent attending ward rounds will be documented daily according to the stats policy of the department.
2. All staff attending staff in-service training, seminars, lectures (informal internal to the institution) will record time in stats NPCA , if it is less than two hours. All requests for activities of more than two hours must be submitted on a time off request sheet.
3. All staff wishing to attend formal courses (usually with cost and time implication) should be prepared to present the material at an in-service education session to arrange a series of lectures. Time off to attend a course must be submitted in writing and approved BEFORE applying for funding.
4. The department Head is responsible for the compilation and reporting of educational activities.
Please note that staff can request (from the union) access to the unused funds set aside for union liberation to pay their salary for the day at the MGH.
*Laidley - if requesting geriatric or ophthalmology
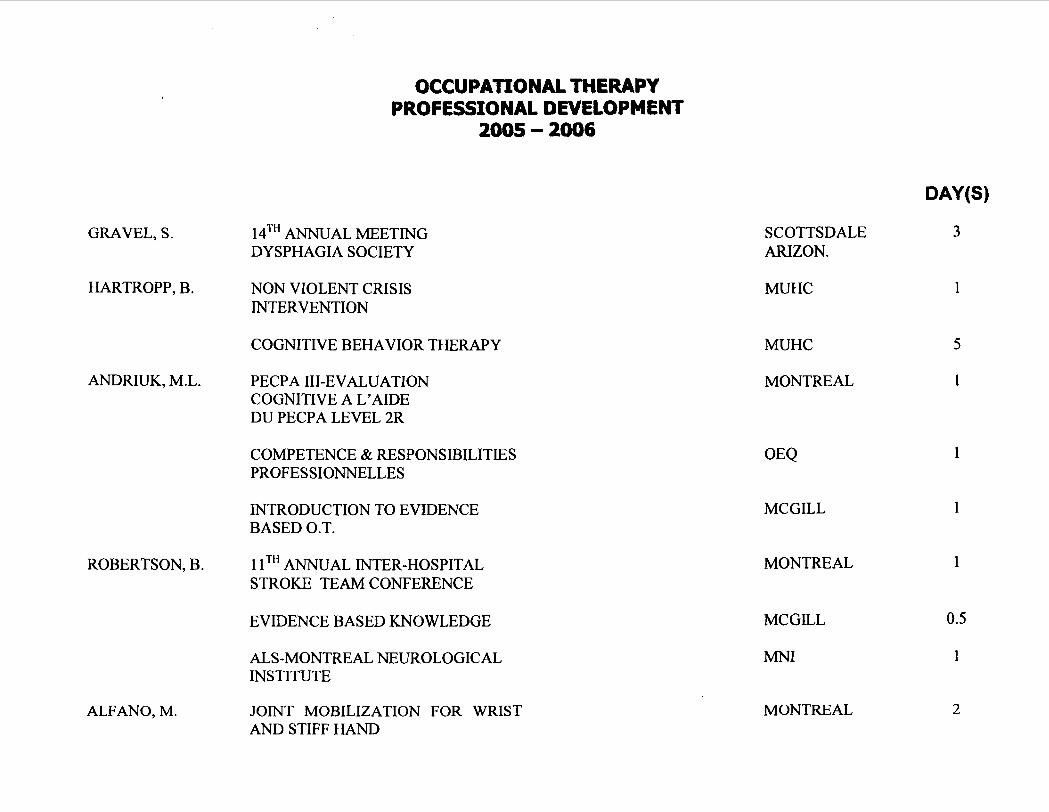
OCCUPATIONAL THERAPY PROFESSIONAL DEVELOPMENT
2005 - 2006
GRAVEL, S. 14TH ANNUAL MEETING DY SPHAGIA SOCIETY
HARTROPP, B. NON VIOLENT CRISIS INTERVENTION
COGNITIVE BEHAVIOR THERAPY
ANDRIUK, M.L. PECPA 111-EVALUATION COGNITIVE A L'AIDE DU PECPA LEVEL 2R
COMPETENCE & RESPONSIBILITIES PROFESSIONNELLES
INTRODUCTION TO EVIDENCE BASED O.T.
ROBERTSON, B. 1 lTH ANNUAL INTER-HOSPITAL STROKE TEAM CONFERENCE
EVIDENCE BASED KNOWLEDGE
ALS-MONTREAL NEUROLOGICAL INSTITUTE
ALFANO, M. JOJNT MOBILIZATION FOR WRIST AND STIFF HAND
SCOTTSDALE ARIZON.
MUHC
MUHC
MONTREAL
MCGILL
MONTREAL
MCGILL
MNI
MONTREAL
DAY (S)
3
OCCUPATIONAL THERAPY
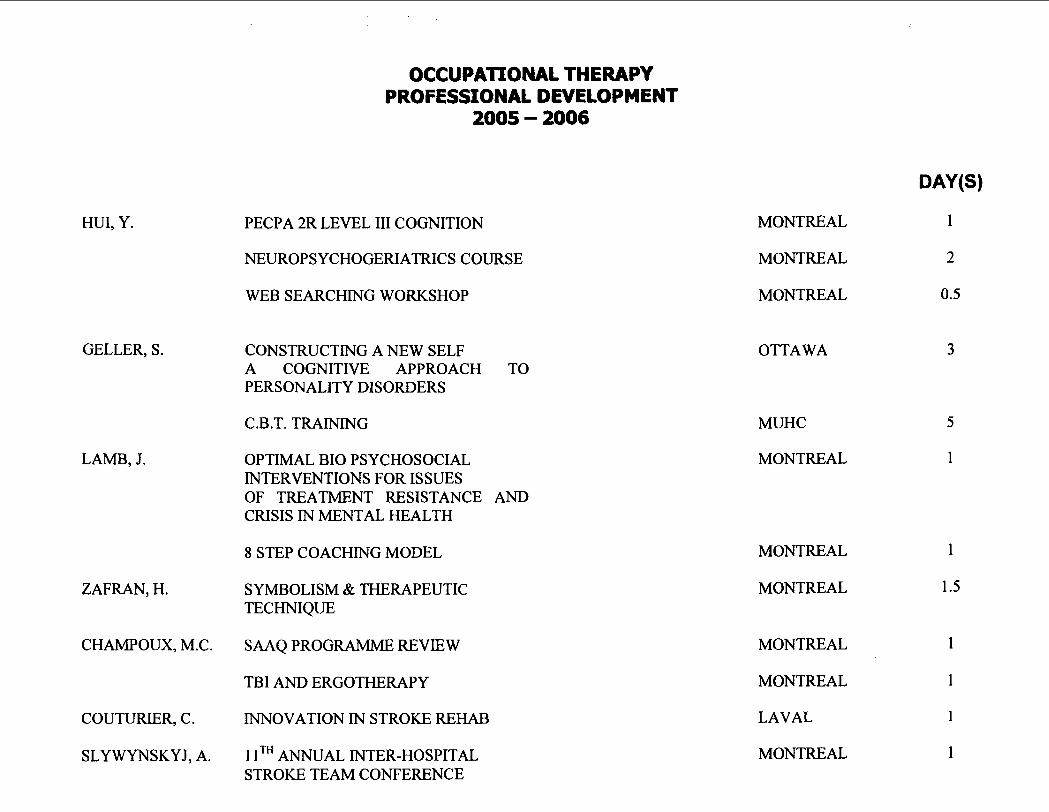
HUI, Y.
PROFESSIONAL DEVELOPMENT
PECPA 2R LEVEL I11 COGNITION
NEUROPSYCHOGERIATRICS COURSE
WEB SEARCHING WORKSHOP
GELLER, S. CONSTRUCTING A NEW SELF A COGNITIVE APPROACH TO PERSONALITY DISORDERS
C.B.T. TRAINING
LAMB, J. OPTIMAL BIO PSYCHOSOCIAL INTERVENTIONS FOR ISSUES OF TREATMENT RESISTANCE AND CRISIS IN MENTAL HEALTH
8 STEP COACHING MODEL
ZAFRAN, H. SYMBOLISM & THERAPEUTIC TECHNIQUE
CHAMPOUX, M.C. SAAQ PROGRAMME REVIEW
TBI AND ERGOTHERAPY
COUTURIER, C. INNOVATION IN STROKE REHAB
SLY WYNSKYJ, A. 1 lTH ANNUAL INTER-HOSPITAL STROKE TEAM CONFERENCE
MONTREAL
MONTREAL
MONTREAL
OTTAWA
MUHC
MONTREAL
MONTREAL
MONTREAL
MONTREAL
MONTREAL
LAVAL
MONTREAL
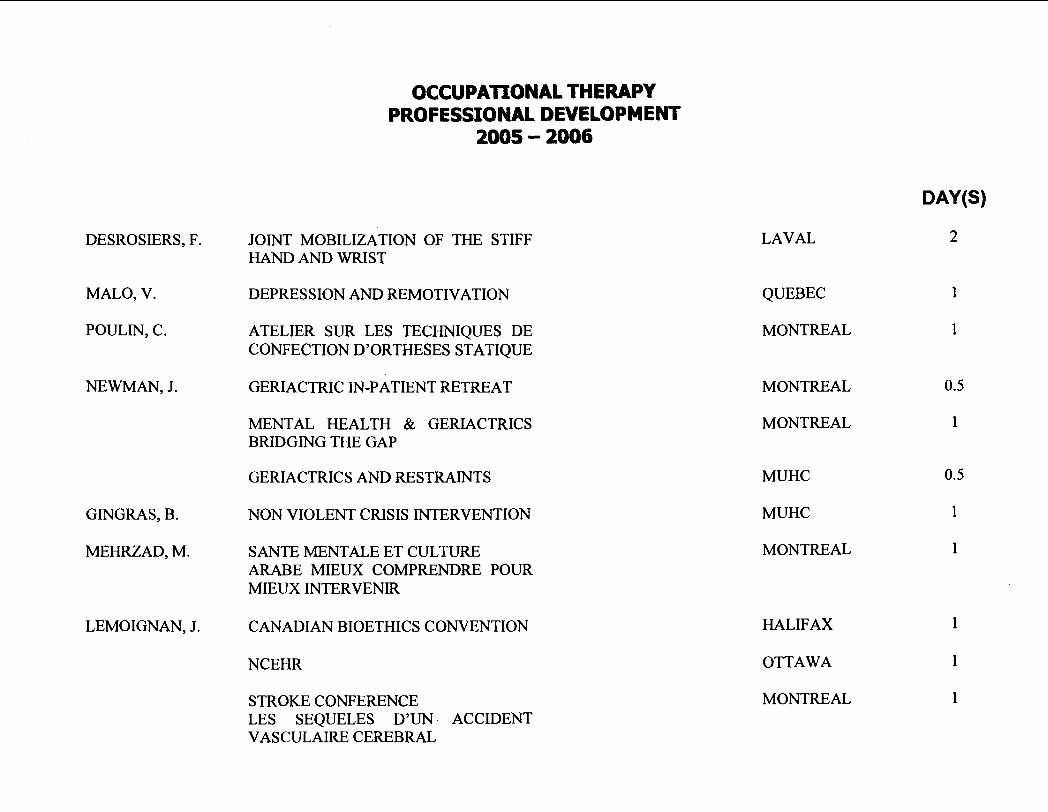
OCCUPAlIONAL THERAPY PROFESSIONAL DEVELOPMENT
DESKOSIERS, F. JOINT MOBILIZATION OF THE STIFF HAND AND WRIST
MALO, V. DEPRESSION AND REMOTIVATION
POULIN, C. ATELIER SUR LES TECHNIQUES DE CONFECTION D'ORTHESES STATIQUE
NEWMAN, J. GERIACTRIC IN-PATIENT RETREAT
MENTAL HEALTH & GERIACTRICS BRIDGING THE GAP
GERIACTRICS AND RESTRAINTS
GINGRAS, B. NON VIOLENT CRISIS INTERVENTION
MEHRZAD, M. SANTE MENTALE ET CULTURE ARABE MIEUX COMPRENDRE POUR MIEUX INTERVENIR
LEMOIGNAN, J. CANADIAN BIOETHICS CONVENTION
NCEHR
STROKE CONFERENCE LES SEQUELES D'UN ACCIDENT VASCULAIRE CEREBRAL
LAVAL
QUEBEC
MONTREAL
MONTREAL
MONTREAL
MUHC
MUHC
MONTREAL
HALIFAX
OTTAWA
MONTREAL
DAY (S)
2
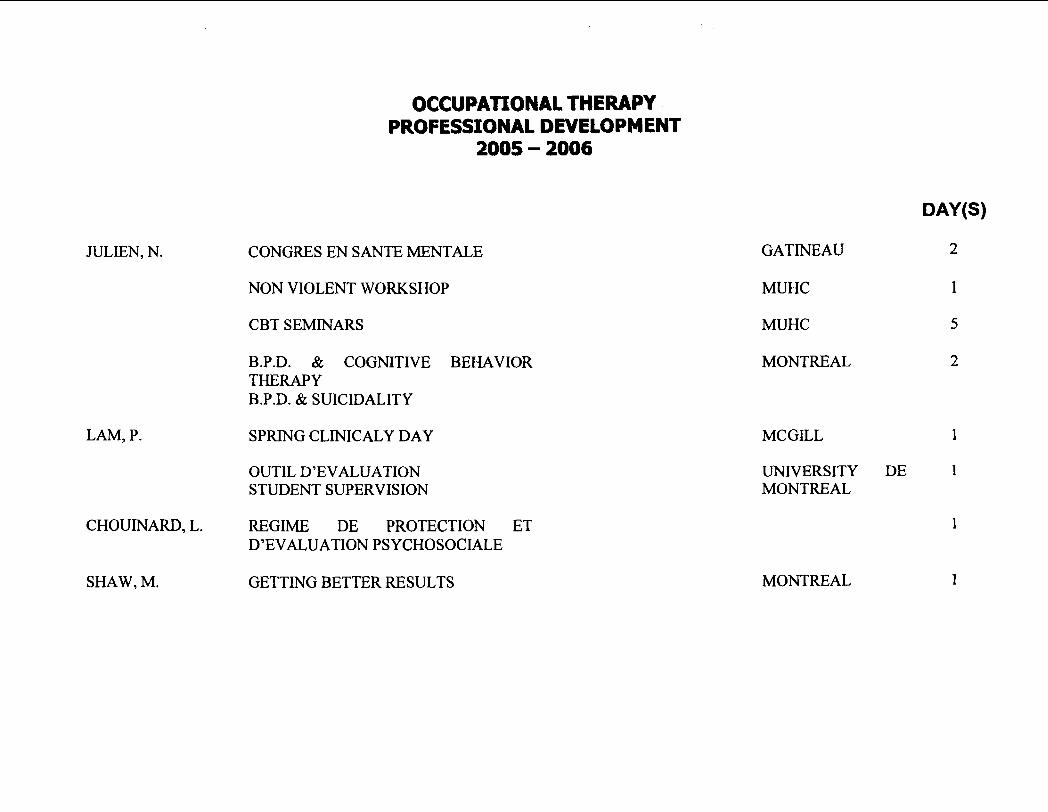
OCCUPATIONAL THERAPY PROFESSIONAL DEVELOPMENT
2005 - 2006
JULIEN, N. CONGRES EN SANTE MENTALE
NON VIOLENT WORKSHOP
CBT SEMINARS
B.P.D. & COGNITIVE BEHAVIOR THERAPY B.P.D. & SUICIDALITY
LAM, P. SPRING CLINICALY DAY
OUTIL D'EVALUATION STUDENT SUPERVISION
CHOUINARD, L. REGIME DE PROTECTION ET D'EVALUATION PSYCHOSOCIALE
SHAW, M. GETTINGBETTERRESULTS
DAY(S)
GATINEAU 2
MUHC 1
MUHC 5
MONTREAL 2
MCGILL 1
UNIVERSITY DE 1 MONTREAL
MONTREAL
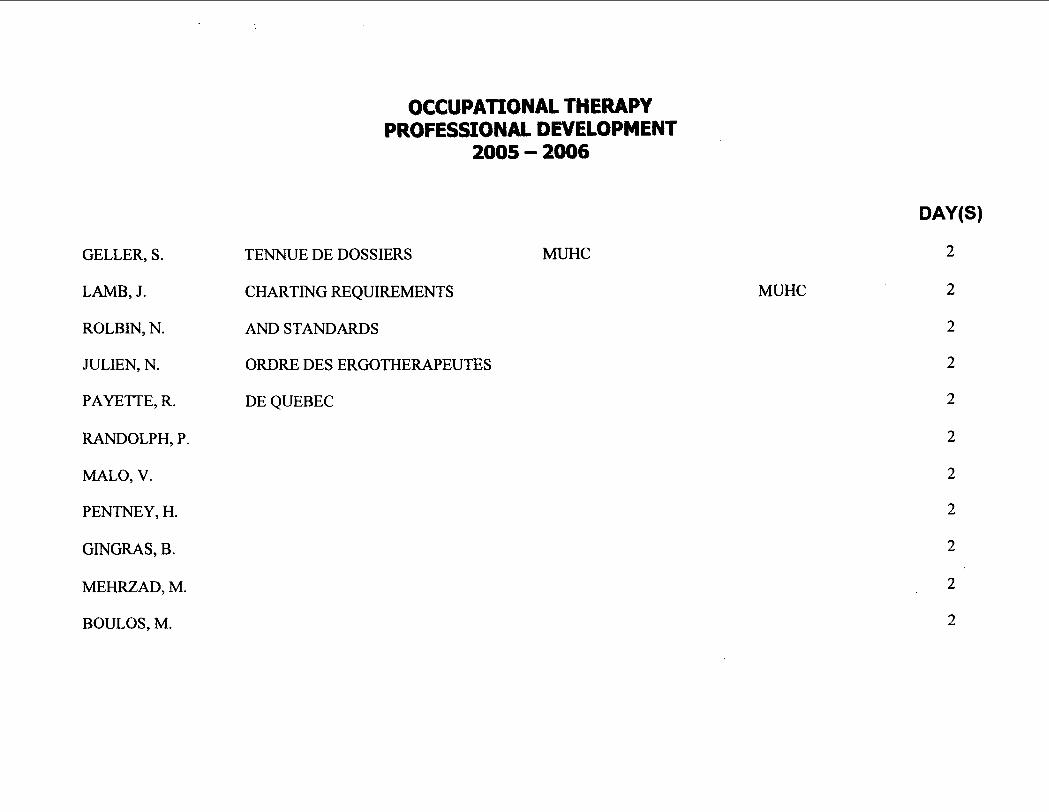
OCCUPATIONAL THERAPY PROFESSIONAL DEVELOPMENT
2005 - 2006
MUHC GELLER, S. TENNUE DE DOSSIERS
LAMB, J. CHARTING REQUIREMENTS
ROLBIN, N. AND STANDARDS
JULIEN, N. ORDRE DES ERGOTHERAPEUTES
PAYETTE, R. DE QUEBEC
RANDOLPH, P.
MALO, V.
PENTNEY, H.
GINGRAS, B.
MEHRZAD, M.
BOULOS, M.
MUHC
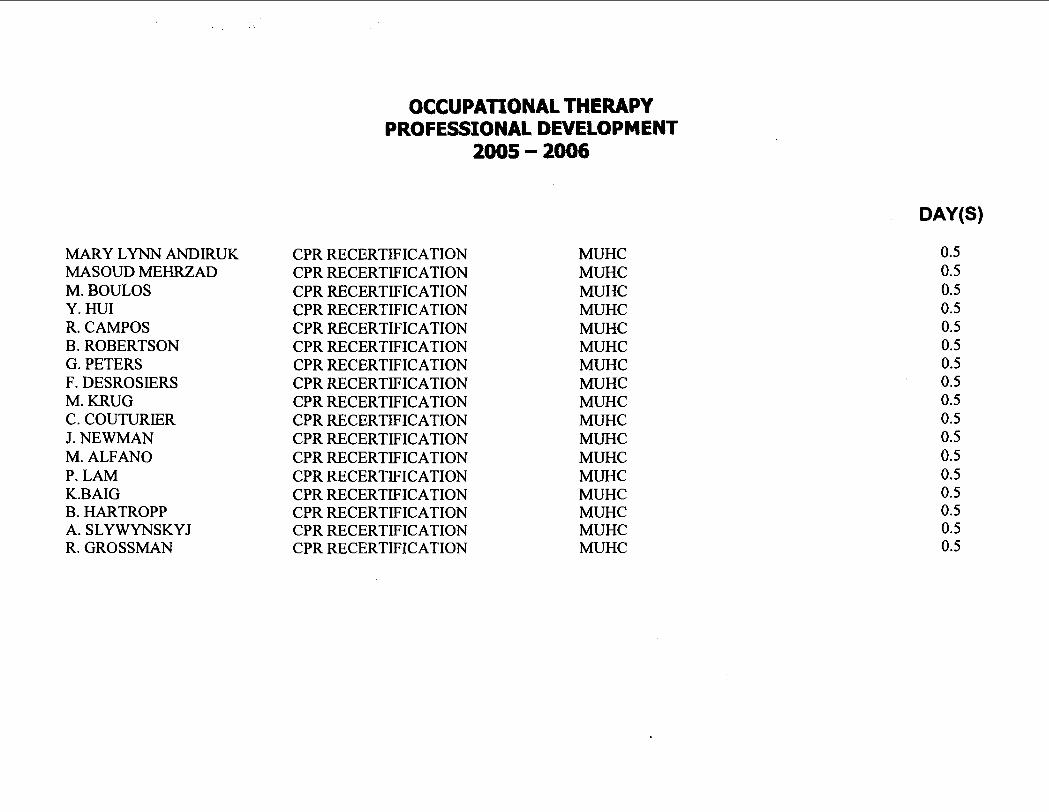
MARY LYNN ANDIRUK MASOUD MEHRZAD M. BOULOS Y. HUI R. CAMPOS B. ROBERTSON G. PETERS F. DESKOSIERS M. KRUG C. COUTURIER J. NEWMAN M. ALFANO P. LAM K.BAIG B. HARTROPP A. SLYWYNSKYJ R. GROSSMAN
OCCUPATIONAL THERAPY PROFESSIONAL DEVELOPMENT
2005 - 2006
CPR RECERTIFICATION CPR RECERTIFICATION CPR RECERTIFICATION CPR RECERTIFICATION CPR RECERTIFICATION CPR RECERTIFICATION CPR RECERTIFICATION CPR RECERTIFICATION CPR RECERTIFICATION CPR RECERTIFICATION CPR RECERTIFICATION CPR RECERTIFICATION CPR RECERTIFICATION CPR RECERTIFICATION CPR RECERTIFICATION CPR RECERTIFICATION CPR RECERTIFICATION
MUHC MUHC MUHC MUHC MUHC MUHC MUHC MUHC MUHC MUHC MUHC MUHC MUHC MUHC MUHC MUHC MUHC
!!I!!! OCCUPATIONAL THERAPY v U-I CONTRACT - HAND THERAPY
STUDENT: SUPERVISOR: SECTION: DATE:
ROLE OF THE COORDINATOR
1. Orientation to safety procedure 2. Orientation to the OT department, the OT staff and the hospital 3. Orientation to the student manual 4. Acts as a third party between student and supervisor in case of difficulty 5 . Responsible to forward all the evaluation forms to the university upon completion of the
placement.
ROLE OF THE SUPERVISOR
1. Will orient the student to the specific clinical program with emphasis on: - Tour of the physical environment of department - Orientation to the evaluation forms - Orientation to the treatment modalities and patient education materials - Orientation to the team members - Demonstrate the education materials (library, books, journals, etc) - Orientation to the medical chart
2. On the first day, will clarify with the student: - Student learning techniques i.e. visual observations vs. reading vs. demonstration - Objectives and expectations - Contracts - Competency based fieldwork evaluation
3. Will schedule a minimum of one weekly formal supervision session.
4. Whenever possible, will demonstrate, explain and provide rationalization to the intervention prior to expecting the student to perform the same task.
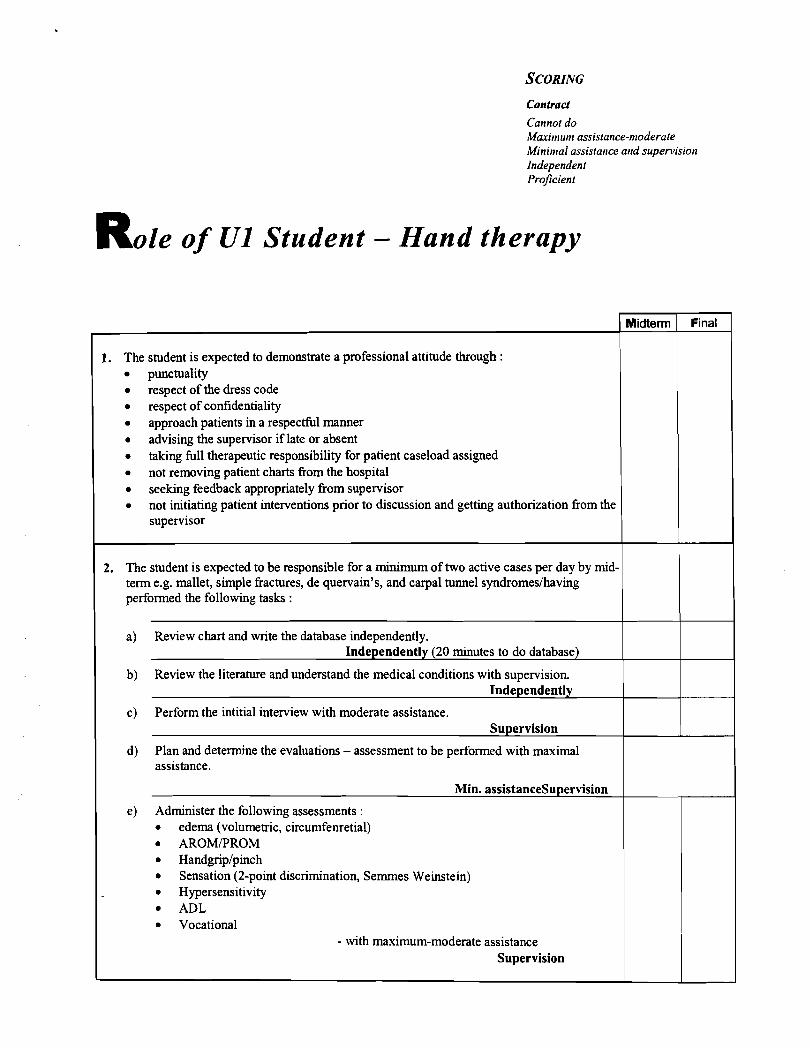
Contract
Cannot do Maxitntct~~ assistance-t~loderate Mininlal assistarlce ar~d supen~isiot~ Independent Proficient
R o l e of UI Student - Hand therapy
1. The student is expected to demonstrate a professional attitude through : punctuality respect of the dress code respect of confidentiality approach patients in a respectful manner advising the supervisor if late or absent taking full therapeutic responsibility for patient caseload assigned not removing patient charts from the hospital seeking feedback appropriately from supervisor not initiating patient interventions prior to discussion and getting authorization from the supervisor
2. The student is expected to be responsible for a minimum of two active cases per day by mid- term e.g. mallet, simple fractures, de quervain's, and carpal tunnel syndromeslhaving performed the following tasks :
a) Review chart and write the database independently. Independently (20 minutes to do database)
b) Review the literature and understand the medical conditions with supervision. Independently
c) Perform the intitial interview with moderate assistance. Supervision
d) Plan and determine the evaluations - assessment to be performed with maximal assistance.
&fin. assistancesupervision
e) Administer the following assessments : edema (volumetric, circumfenretial) AROWPROM Handgriplpinch Sensation (2-point discrimination, Sernrnes Weinstein) Hypersensitivity ADL Vocational
- with maximum-moderate assistance Supervision
Midterm Final
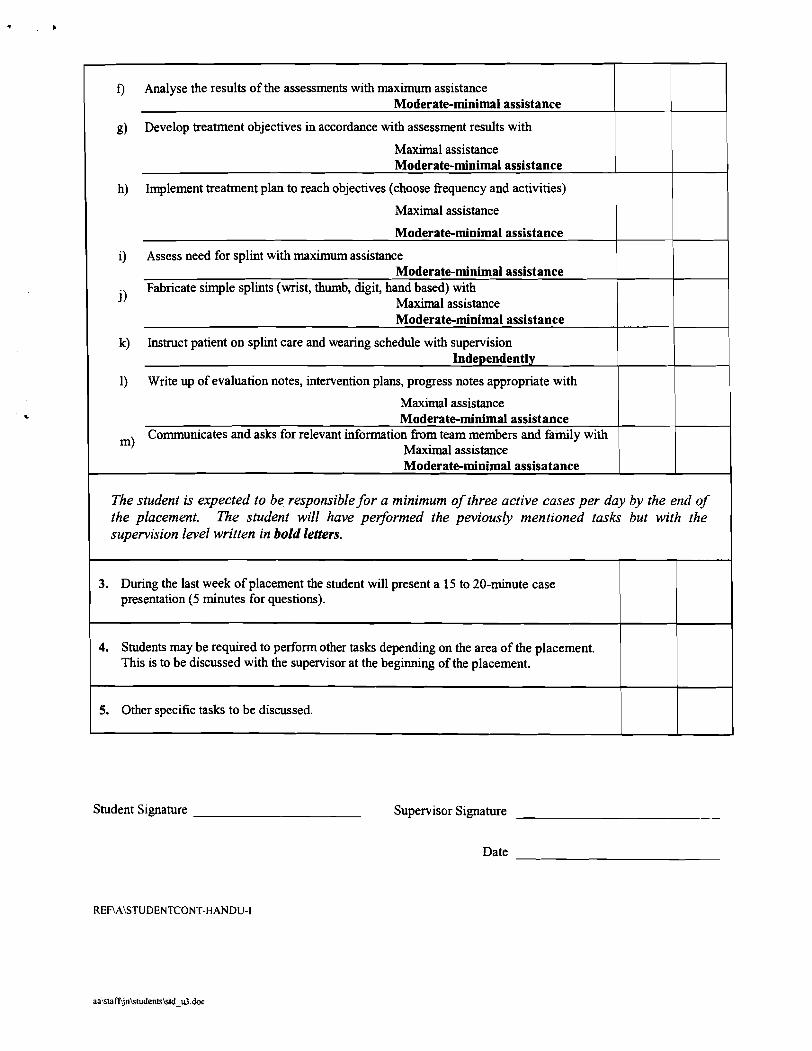
I 0 Analyse the results of the assessments with maximum assistance 1 1 Moderate-minimal assistance
I I
I g) Develop treatment objectives in accordance with assessment results with
Maximal assistance Moderate-minimal assistance
h) Implement treatment plan to reach objectives (choose frequency and activities)
Maximal assistance
Moderate-minimal assistance
i) Assess need for splint with maximum assistance Moderate-minimal assistance
j) Fabricate simple splints (wrist, thumb, digit, hand based) with
Maximal assistance Moderate-minimal assistance
k) Instruct patient on splint care and wearing schedule with supervision
1) Write up of evaluation notes, intervention plans, progress notes appropriate with
I Maximal assistance Moderate-minimal assistance
m) Communicates and asks for relevant information from team members and family with
Maximal assistance Moderate-minimal assisatance
The student is expected to be responsible for a minimum of three active cases per day by the end of the placement. The student will have peijiormed the peviously mentioned tasks but with the supervision level written in bold letters.
3. During the last week of placement the student will present a 15 to 20-minute case presentation (5 minutes for questions).
4. Students may be required to perform other tasks depending on the area of the placement. This is to be discussed with the supervisor at the beginning of the placement.
1 5. Other specifle tasks to be discussed.
Student Signature Supervisor Signature
Date
OCCUPATIONAL THERAPY U-I1 CONTRACT - HAND THERAPY
STUDENT: SUPERVISOR: SECTION: DATE:
ROLE OF THE COORDINATOR
I. Orientation to safety procedure 2. Orientation to the OT department, the OT staff and the hospital 3. Orientation to the student manual 4. Acts as a third party between student and supervisor in case of difficulty 5 . Responsible to forward all the evaluation forms to the university upon completion of the
.
placement.
ROLE OF THE SUPERVISOR
1. Will orient the student to the specific clinical program with emphasis on: - Tour of the physical environment of department - Orientation to the evaluation forms - Orientation to the treatment modalities and patient education materials - Orientation to the team members - Demonstrate the education materials (library, books, journals, etc) - Orientation to the medical chart
2. On the first day, will clarify with the student: - Student learning techniques i.e. visual observations vs. reading vs. demonstration - Objectives and expectations - Contracts
- Competency based fieldwork evaluation
3. Will schedule a minimum of one weekly formal supervision session.
4. Whenever possible, will demonstrate, explain and provide rationalization to the intervention prior to expecting the student to perfom the same task.
Contract Cannot do Maximum assistance-nroderate Minimal assistance and slrpervision Independent Proficient
R o l e of U-11 Student - Hand therapy
1. The student is expected to demonstrate a professional attitude through : punctuality respect of the dress code respect of confidentiality approach patients in a respectful manner advising the supervisor if late or absent taking full therapeutic responsibility for patient caseload assigned not removing patient charts fiom the hospital seeking feedback appropriately fiom supervisor not initiating patient interventions prior to discussion and getting authorization fiom the supervisor
Midterm
2. The student is expected to be responsible for following 3 patients per day by mid-term (e.g. mallet, simple fractures, de quervain's, and carpal tunnel syndrome) having performed the following tasks :
Final
a) Review chart and write the database independently. Independently
b) Review the literature and understand the medical conditions independently. Independently
c) Perform the initial interview independently. Independently
d) Plan and determine the evaluations - assessments to be performed with minimal assistance and supervision.
I Independently e) Administer the following assessments :
edema (volumetric, circumferential) AROM/PROM Handgriplpinch Sensation (2-point discrimination, Semmes Weinstein) Hypersensitivity ADL, functional hand evaluation such as Jebsen Vocational
- with moderate assistance - supervision Independently
I f) Analyse the results of the assessments with moderate-minimal assistance 1 I Supervision
I I
I g) Develop treatment objectives in accordance with assessment results with I I I Moderate-minimal assistance Supervision
h) Implement treatment plan to reach objectives (choose frequency and activities)
I Moderate-minimal assistance
Supervision
i) Assess need for splint with moderate-minimal assistance Supervision
j) Fabricate simple splints (e.g. wrist, thumb, digit, hand based) with
Moderate-minimal assistance Supervision
k) Instruct patient on splint care and wearing schedule independently Independently
1) Write up of evaluation notes, intervention plans, progress notes as appropriate with
I Moderate-minimal assistance 1 1 I Supervision
m) Communicates and asks for relevant information from team members and family with
Moderate-minimal assistance Supervision
The student is expected to be responsible for a minimum of 5 cases per day by the end of the placement. The student will have peflormed the peviously mentioned tasks but with the supervision level written in bold letters.
3. During the last week of placement the student will make a 15 minute presentation of a project (5 minutes for questions).
4. Students may be required to perform other tasks. This is to be discussed with the supervisor at the beginning of the placement.
5. Other specific tasks to be discussed.
Student Signature Supervisor Signature
Date
OCCUPATIONAL THERAPY U-I11 CONTRACT - HAND THERAPY
STUDENT: SUPERVISOR: SECTION: DATE:
ROLE OF THE COORDINATOR
1. Orientation to safety procedure 2. Orientation to the OT department, the OT staff and the hospital 3. Orientation to the student manual 4. Acts as a third party between student and supervisor in case of difficulty 5 . Responsible to forward all the evaluation forms to the university upon completion of the
placement.
ROLE OF THE SUPERVISOR
1. Will orient the student to the specific clinical program with emphasis on: - Tour of the physical environment of department - Orientation to the evaluation forms - Orientation to the treatment modalities and patient education materials - Orientation to the team members - Demonstrate the education materials (library, books, journals, etc) - Orientation to the medical chart
2. On the first day, will clarify with the student: - Student learning techniques i.e. visual observations vs. reading vs. demonstration - Objectives and expectations - Contracts
- Competency based fieldwork evaluation
3. Will schedule a minimum of one weekly formal supervision session.
4. Whenever possible, will demonstrate, explain and provide rationalization to the intervention prior to expecting the student to perform the same task.
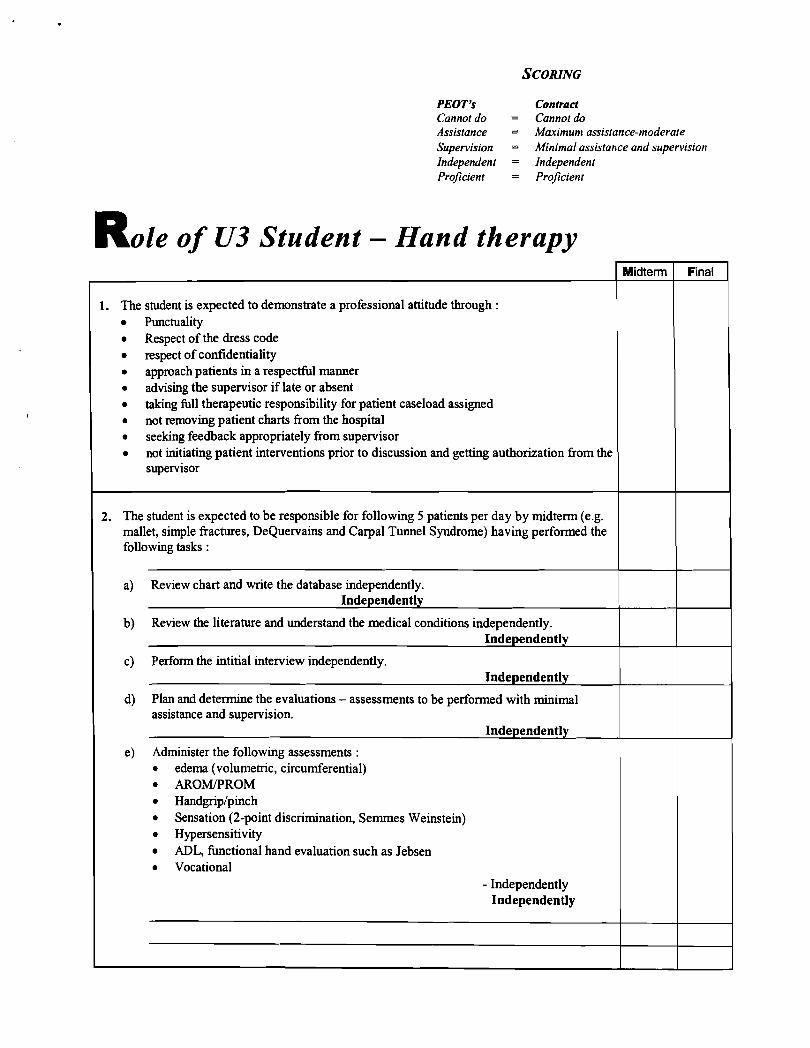
PEOT's Contract Cannot do = Cannot do Assistance = Maximunt assistance-moderate Supervision = Minimal assistar~ce and supervisior~ Independent = Independent Proficient = Proficient
R o l e of U3 Student - Hand therapy Midterm 1 Final
1. The student is expected to demonstrate a professional attitude through : Punctuality Respect of the dress code respect of confidentiality approach patients in a respecthl manner advising the supervisor if late or absent taking full therapeutic responsibility for patient caseload assigned not removing patient charts from the hospital seeking feedback appropriately from supervisor not initiating patient interventions prior to discussion and getting authorization from the supervisor
2. The student is expected to be responsible for following 5 patients per day by midterm (e.g. mallet, simple fractures, DeQuervains and Carpal Tunnel Syndrome) having performed the following tasks :
a) Review chart and write the database independently. Independently
b) Review the literature and understand the medical conditions independently. Independently
c) Perform the intitial interview independently. Independently
d) Plan and determine the evaluations - assessments to be performed with minimal assistance and supervision.
Independently
e) Administer the following assessments : edema (volumetric, circumferential) AROMPROM Handgrip/pinch Sensation (2-point discrimination, Semrnes Weinstein) Hypersensitivity ADL, hctional hand evaluation such as Jebsen Vocational
- Independently Independently
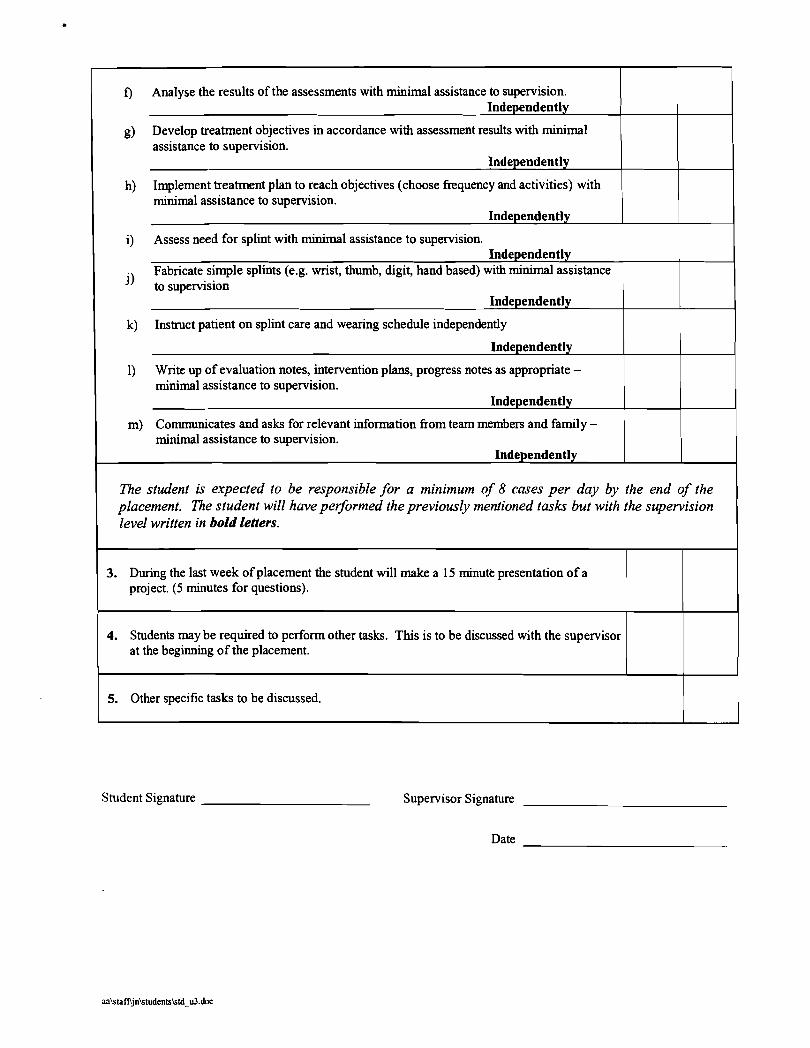
f) Analyse the results of the assessments with minimal assistance to supervision. Indeoendentlv
g) Develop treatment objectives in accordance with assessment results with minimal assistance to supervision.
Independently
h) Implement treatment plan to reach objectives (choose frequency and activities) with minimal assistance to supervision.
Independently
i) Assess need for splint with minimal assistance to supervision. 1 1 Independently
I , Fabricate simple splints (e.g. wrist, thumb, digit, hand based) with minimal assistance 1 1 " to supervision I I I Independently
I I
1 k) Instruct patient on splint care and wearing schedule independently
Independently
1) Write up of evaluation notes, intervention plans, progress notes as appropriate - minimal assistance to supervision.
Independently
m) Communicates and asks for relevant information from team members and family - minimal assistance to supervision.
Independently
The student is expected to be responsible for a minimum of 8 cases per day by the end of the placement. The student will have performed the previously mentioned tasks but with the supervision level written in bold letters.
3. During the last week of placement the student will make a 15 minutk presentation of a project. (5 minutes for questions).
4. Students may be required to perform other tasks. This is to be discussed with the supervisor at the beginning of the placement.
5. Other specific tasks to be discussed.
Student Signature Supervisor Signature
Date
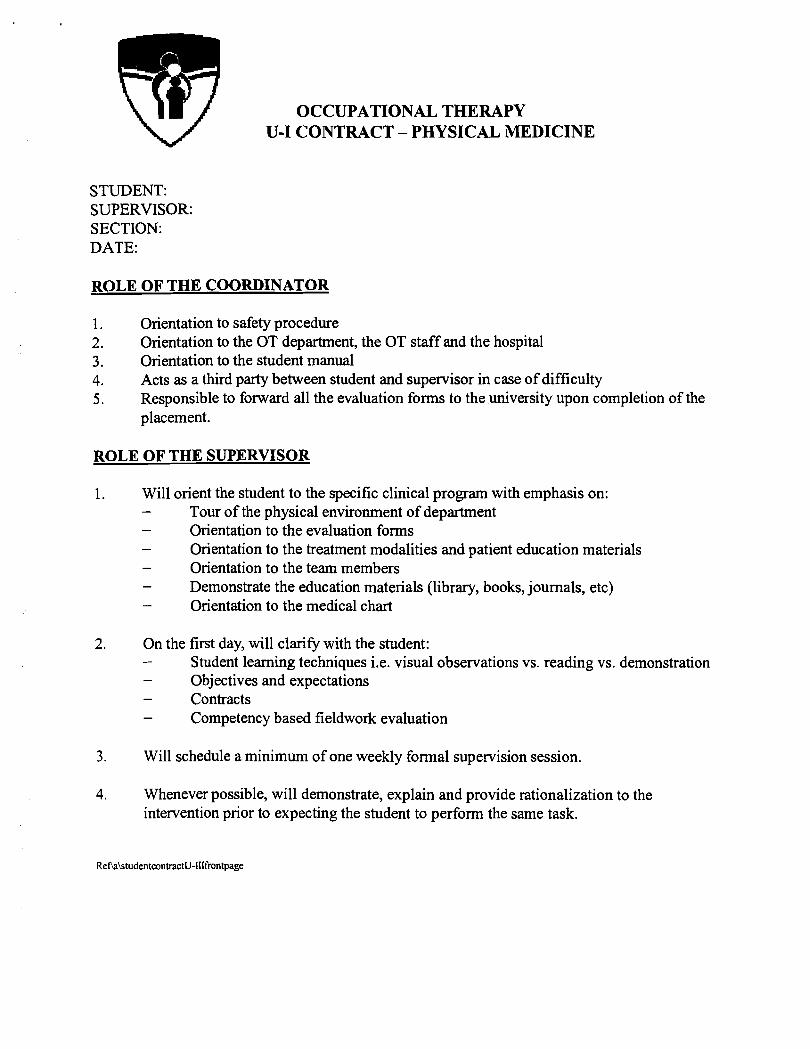
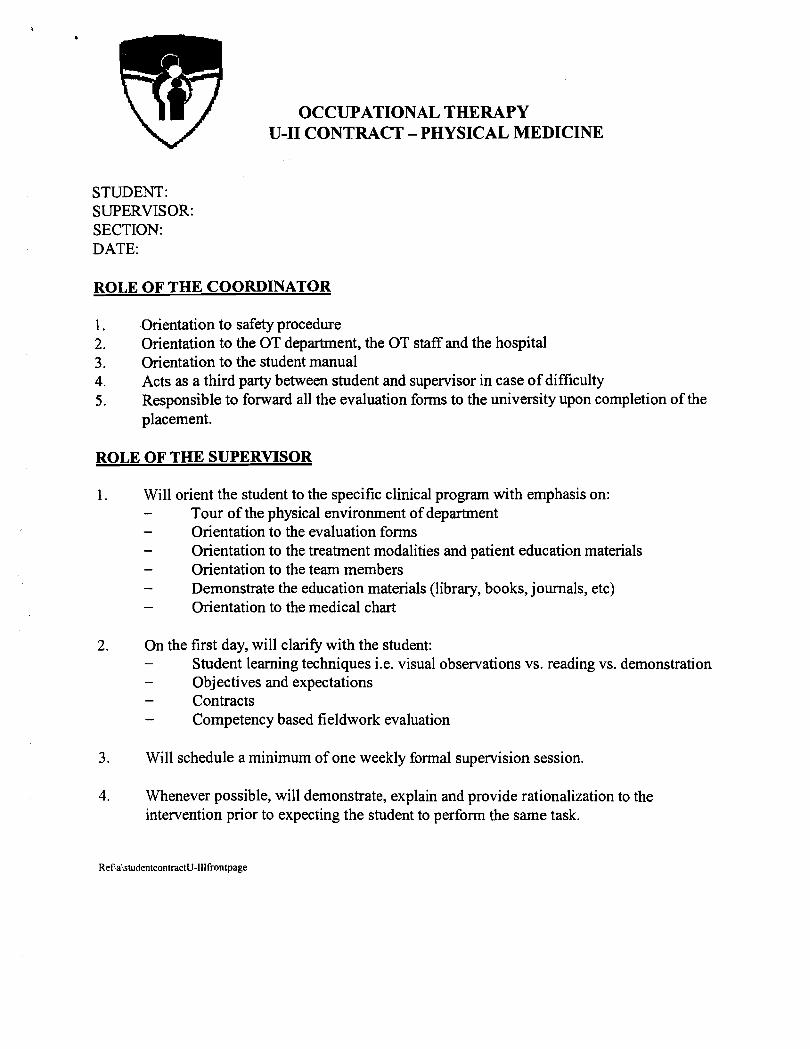
OCCUPATIONAL THERAPY U-I CONTRACT - PHYSICAL MEDICINE
STUDENT: SUPERVISOR: SECTION: DATE:
ROLE OF THE COORDINATOR
1. Orientation to safety procedure 2. Orientation to the OT department, the OT staff and the hospital 3. Orientation to the student manual 4. Acts as a third party between student and supervisor in case of difficulty 5 . Responsible to forward all the evaluation forms to the university upon completion of the
placement.
ROLE OF THE SUPERVISOR
1. Will orient the student to the specific clinical program with emphasis on: - Tour of the physical environment of department - Orientation to the evaluation forms - Orientation to the treatment modalities and patient education materials - Orientation to the team members - Demonstrate the education materials (library, books, journals, etc) - Orientation to the medical chart
2. On the first day, will clariQ with the student: - Student learning techniques i.e. visual observations vs. reading vs. demonstration - Objectives and expectations - Contracts - Competency based fieldwork evaluation
3. Will schedule a minimum of one weekly formal supervision session.
4. Whenever possible, will demonstrate, explain and provide rationalization to the intervention prior to expecting the student to perform the same task.
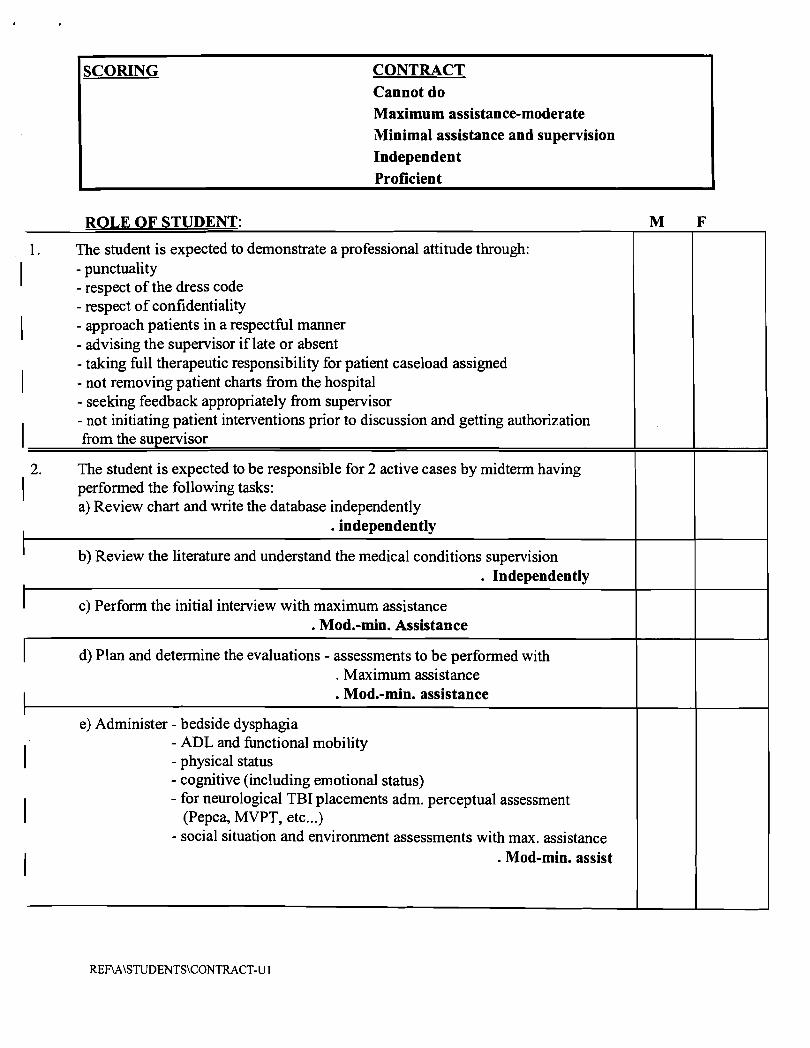
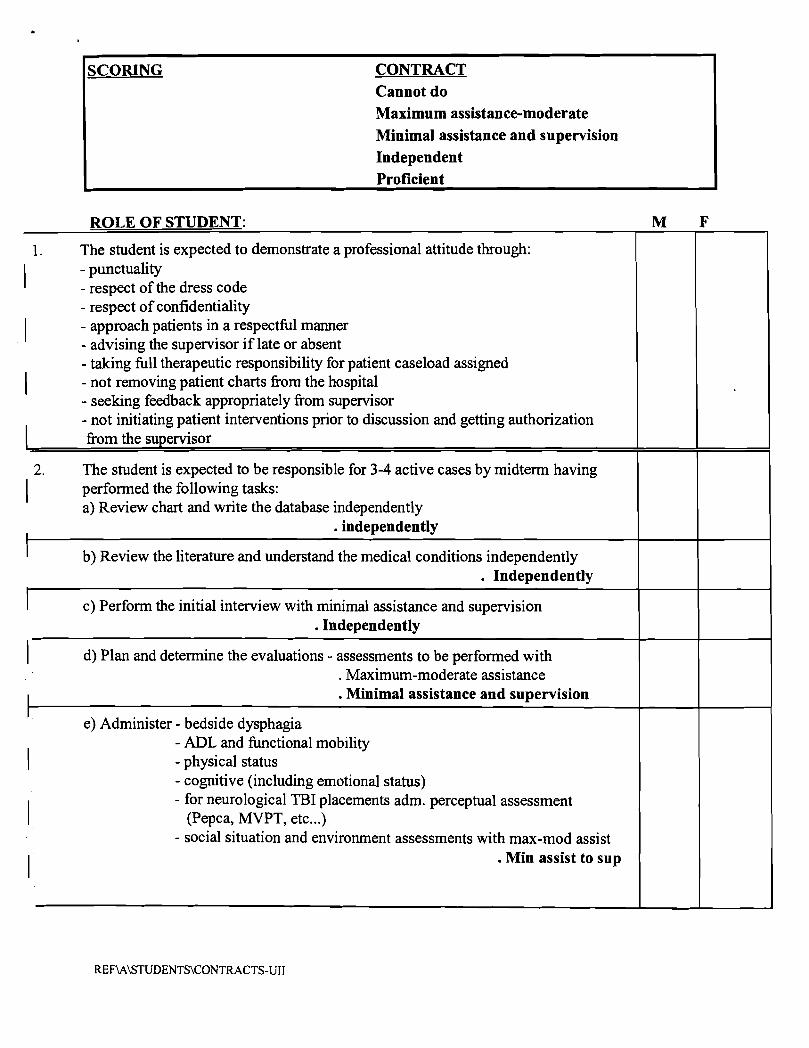
SCORING CONTRACT Cannot do Maximum assistance-moderate Minimal assistance and supervision Independent Proficient
ROLE OF STUDENT:
1. The student is expected to demonstrate a professional attitude through:
I - punctuality - respect of the dress code - respect of confidentiality
I - approach patients in a respectful manner - advising the supervisor if late or absent - taking full therapeutic responsibility for patient caseload assigned
I - not removing patient charts from the hospital - seeking feedback appropriately from supervisor
I - not initiating patient interventions prior to discussion and getting authorization from the supervisor
2. The student is expected to be responsible for 2 active cases by midterm having
I performed the following tasks: a) Review chart and write the database independently
. independently I
I b) Review the literature and understand the medical conditions supervision . Independently
I I c) Perform the initial interview with maximum assistance
. Mod.-min. Assistance r I d) Plan and determine the evaluations - assessments to be performed with
. Maximum assistance
. Mod.-min. assistance
e) Administer - bedside dysphagia
I - ADL and finctional mobility - physical status - cognitive (including emotional status) - for neurological TBI placements adm-. perceptual assessment
(Pepca, MVPT, etc ...) - social situation and environment assessments with max. assistance
. Mod-min. assist
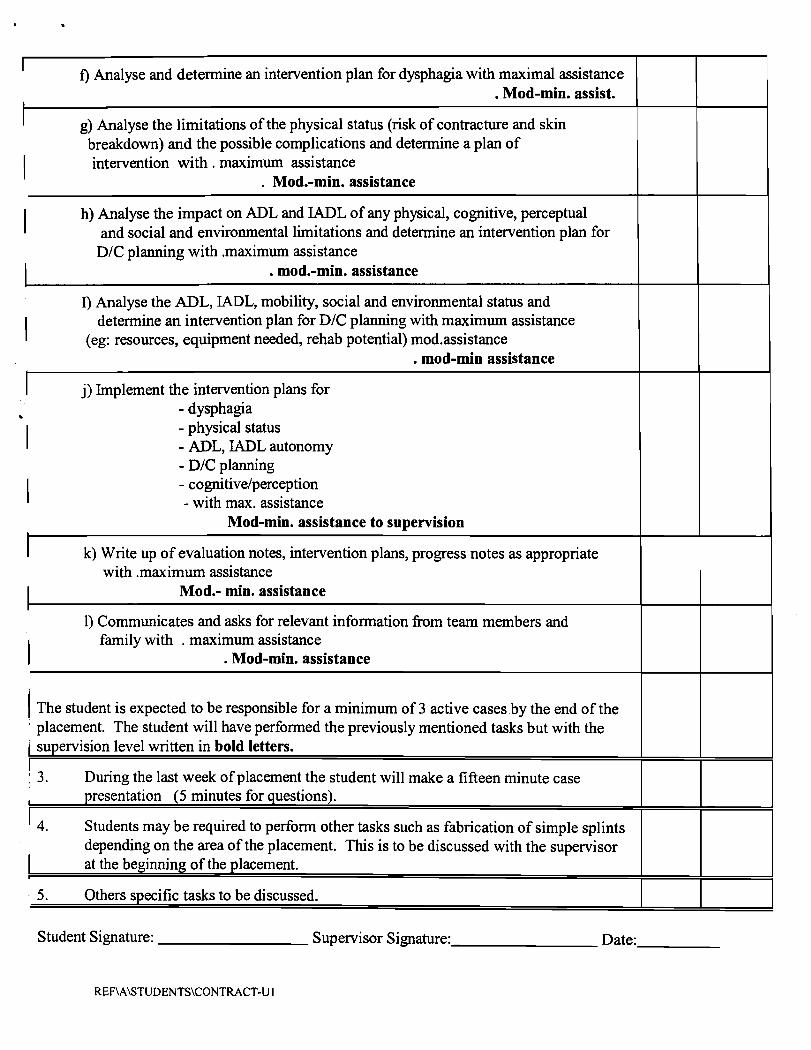
I f) Analyse and determine an intervention plan for dysphagia with maximal assistance
. Mod-min. assist.
g) Analyse the limitations of the physical status (risk of contracture and skin breakdown) and the possible complications and determine a plan of
I intervention with . maximum assistance . Mod.-min. assistance
I h) Analyse the impact on ADL and IADL of any physical, cognitive, perceptual and social and environmental limitations and determine an intervention plan for
D/C planning with .maximum assistance . mod.-min. assistance
I) Analyse the ADL, IADL, mobility, social and environmental status and
I determine an intervention plan for D/C planning with maximum assistance (eg: resources, equipment needed, rehab potential) mod.assistance
. mod-min assistance
j) Implement the intervention plans for - dysphagia .
I - physical status - ADL, WDL autonomy - D/C planning
I - cognitive/perception - with max. assistance
Mod-min. assistance to supervision
k) Write up of evaluation notes, intervention plans, progress notes as appropriate with .maximum assistance
Mod.- min. assistance
1) Communicates and asks for relevant information from team members and
I family with . maximum assistance . Mod-min. assistance
( The student is expected to be responsible for a minimum of 3 active cases by the end of the ' placement. The student will have performed the previously mentioned tasks but with the / supervision level written in bold letters.
1 3. During the last week of placement the student will make a fifteen minute case I presentation (5 minutes for questions).
I 4. Students may be required to perform other tasks such as fabrication of simple splints depending on the area of the placement. This is to be discussed with the supervisor at the beginning of the placement.
I
5. Others specific tasks to be discussed.
Student Signature: Supervisor Signature: Date:
REF\A\STUDENTS\CONTRACT-U 1
OCCUPATIONAL THERAPY U-I1 CONTRACT - PHYSICAL MEDICINE
STUDENT: SUPERVISOR: SECTION: DATE:
ROLE OF THE COORDINATOR
1. Orientation to safety procedure 2. Orientation to the OT department, the OT staff and the hospital 3. Orientation to the student manual 4. Acts as a third party between student and supervisor in case of difficulty 5 . Responsible to forward all the evaluation forms to the university upon completion of the
placement.
ROLE OF THE SUPERVISOR
1. Will orient the student to the specific clinical program with emphasis on: - Tour of the physical environment of department - Orientation to the evaluation forms - Orientation to the treatment modalities and patient education materials - Orientation to the team members - Demonstrate the education materials (library, books, journals, etc) - Orientation to the medical chart
2. On the first day, will clarify with the student: - Student learning techniques i.e. visual observations vs. reading vs. demonstration - Objectives and expectations - Contracts - Competency based fieldwork evaluation
3. Will schedule a minimum of one weekly formal supervision session.
4. Whenever possible, will demonstrate, explain and provide rationalization to the intervention prior to expecting the student to perform the same task.
SCORING CONTRACT Cannot do Maximum assistance-moderate Minimal assistance and supervision Independent Proficient
ROLE OF STUDENT:
1. The student is expected to demonstrate a professional attitude through:
I - punctuality - respect of the dress code - respect of confidentiality
I - approach patients in a respectful manner - advising the supervisor if late or absent - taking full therapeutic responsibility for patient caseload assigned
I - not removing patient charts from the hospital - seeking feedback appropriately from supervisor - not initiating patient interventions prior to discussion and getting authorization
I from the supervisor
2. The student is expected to be responsible for 3-4 active cases by midterm having
I performed the following tasks: a) Review chart and write the database independently
. independently
b) Review the literature and understand the medical conditions independently . Independently
c) Perform the initial interview with minimal assistance and supervision . Independently
1 d) Plan and determine the evaluations - assessments to be performed with . Maximum-moderate assistance . Minimal assistance and supervision
e) Administer - bedside dysphagia - ADL and functional mobility
I - physical status - cognitive (including emotional status) - for neurological TBI placements adm. perceptual assessment
(Pepca, MVPT, etc ...) - social situation and environment assessments with max-mod assist
. Min assist to sup
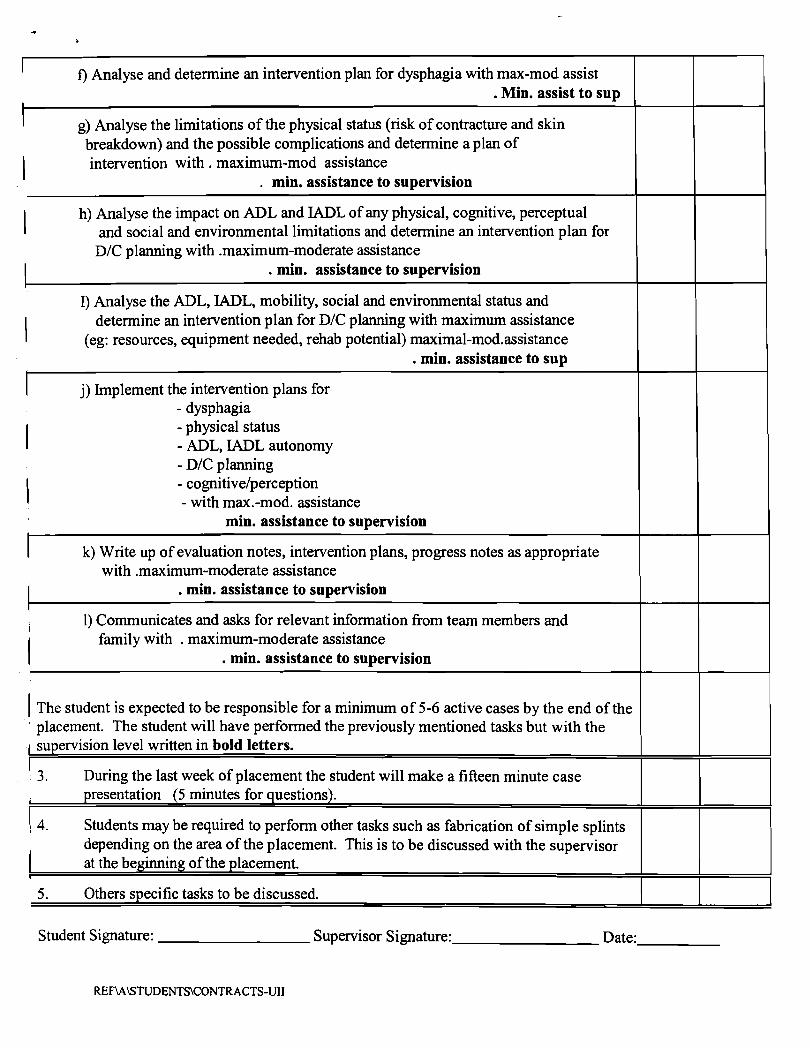
I f ) Analyse and determine an intervention plan for dysphagia with max-mod assist . Min. assist to sup
g) Analyse the limitations of the physical status (risk of contracture and skin breakdown) and the possible complications and determine a plan of
I intervention with . maximum-mod assistance . min. assistance to supervision
I h) Analyse the impact on ADL and IADL of any physical, cognitive, perceptual and social and environmental limitations and determine an intervention plan for
D/C planning with .maximum-moderate assistance . min. assistance to supervision
I) Analyse the ADL, IADL, mobility, social and environmental status and
I determine an intervention plan for D/C planning with maximum assistance (eg: resources, equipment needed, rehab potential) maximal-mod.assistance
. min. assistance to sup
j) Implement the intervention plans for - dysphagia
I - physical status - ADL, IADL autonomy - D/C planning
I - cognitivelperception - with max.-mod. assistance
min. assistance to supervision
k) Write up of evaluation notes, intervention plans, progress notes as appropriate with .maximum-moderate assistance
. min. assistance to supervision
1) Communicates and asks for relevant information fiom team members and
i family with . maximum-moderate assistance . min. assistance to supervision
1 The student is expected to be responsible for a minimum of 5-6 active cases by the end of the ' placement. The student will have performed the previously mentioned tasks but with the 1 supervision level written in bold letters.
I 3. During the last week of placement the student will make a fifteen minute case i presentation (5 minutes for questions).
4. Students may be required to perform other tasks such as fabrication of simple splints depending on the area of the placement. This is to be discussed with the supervisor at the beginning of the placement.
I
5. Others specific tasks to be discussed.
Student Signature: Supervisor Signature: Date:
REF\A\STUDENTS\CONTRACTS-UII
OCCUPATIONAL THERAPY U-I11 CONTRACT - PHYSICAL MEDICINE
STUDENT: SUPERVISOR: SECTION: DATE:
ROLE OF THE COORDINATOR
1. Orientation to safety procedure 2. Orientation to the OT department, the OT staff and the hospital 3. Orientation to the student manual 4. Acts as a third party between student and supervisor in case of difficulty 5 . Responsible to forward all the evaluation forms to the university upon completion of the
placement.
ROLE OF THE SUPERVISOR
1. Will orient the student to the specific clinical program with emphasis on: - Tour of the physical environment of department - Orientation to the evaluation forms - Orientation to the treatment modalities and patient education materials - Orientation to the team members - Demonstrate the education materials (library, books, journals, etc) - Orientation to the medical chart
2. On the first day, will clarify with the student: - Student learning techniques i.e. visual observations vs. reading vs. demonstration - Objectives and expectations - Contracts - Competency based fieldwork evaluation
3. Will schedule a minimum of one weekly formal supervision session.
4. Whenever possible, will demonstrate, explain and provide rationalization to the intervention prior to expecting the student to perform the same task.
PEOT's Contract Cannot do = Cannot do Assistance = Maximum assistance-moderate Supervision = Minimal assistance and s~cpervision Independent = Independent Proficient = Proficient
R o l e of ~3 Student
1. The student is expected to demonstrate a professional attitude through : Punctuality Respect of the dress code respect of confidentiality approach patients in a respectful manner advising the supervisor if late or absent taking full therapeutic responsibility for patient caseload assigned not removing patient charts from the hospital seeking feedback appropriately from supervisor not initiating patient interventions prior to discussion and getting authorization from the supervisor
2. The student is expected to be responsible for 4-6 active cases by midterm having performed the following tasks :
a) Review chart and write the database independently. Independently (20 minutes to do database)
b) Review the literature and understand the medical conditions independently. Independently
c) Perform the intitial interview independently. Independently
d) Plan and determine the evaluations - assessment to be performed with mininum assistance and supervision.
Independently
e) Administer : ADL and functional mobility physical status cognitive for neurological TBI placements administer perceptual assessment (Pepca, MVPT, etc.) social situation and environment assessments with (minimum assistance and supervision applies to all of above for midterm) bedside dysphagia
Independently (applies to all except dysphagia)
Midterm Final
f) Analyse and determine an intervention plan for dysphagia with minimal assistance to ' supervision.
Independently
g) Analyse the limitations of the physical status (risk of contracture and skin breakdown) and the possible complications and determine a plan of intervention with minimal assistance and supervision.
Independently
h) Analyse the impact of ADL and IADL of any physical, cognitive, perceptual and social and environmental limitations and determine an intervention plan - minimal assistance.
Independently
i) Analyse the ADL, IADL, mobility, social and environmental status and determine an intervention plan for DIC planning with maximum assistance.
Independently
j) Implement the intervention plans for dysphagia physical status ADL, IADL autonomy DIC planning cognitivelperception (minimum assistance and supervision applies to all for midterm)
Independently
k) Write up of evaluation notes, intervention plans, progress notes as appropriate - minimal assistance.
Independently
1) Communicates and asks for relevant information from team members and family - independently.
Independently
The student is expected to be responsible for a minimum of 6-8 active cases by the end of [he placement. The student will have peformed the previously mentioned tasks but with the supervision level written in bold letters.
3. During the last week of placement the student will present a 15 to 20-minute project (5 minutes for questions).
4. Students may be required to perform other tasks such as fabrication of simple splints depending on the area of the placement. This is to be discussed with the supervisor at the beginning of the placement.
1 5. Other specific tasks to be discussed. 1 I I
Student Signature Supervisor Signature
Date