Embed Size (px)
Citation preview


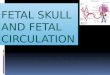
Fetal Skull Development
Develops from the mesoderm and the neural crest.
By end of the 4th week loosely woven tissue – embryonic connective tissue
Differentiation of cells within the skull is different. The flat bones ossifies from the membrane. Whist other bones form cartilage after which ossification takes place

Fetal Skull Development
Skull is divided into 2 parts: Neurocranium –protecting the
brain which is known as the vault. This is subdivided into:
1. Dermatocranium – parietal & frontal2. Chondrocranium –occipital,
temporal, sphenoid – base of the skull. Fusion of cartilage
Viscerocranium – forms the face – starts with the mandible at 6 weeks gestation

Fetal Skull
29 bones 8 form the cranium 14 form the face 7 form the base

The vault of the skull comprises Two frontal bones Two parietal bones One occipital bone Two temporal bones.


Sutures Lambdoidal suture: separates the
occipital bone from the parietal bones
Sagital suture: lies between 2 parietal bones
Coronal suture: separates frontal bones from parietal bones
Frontal suture:runs between two halves of frontal bones

Anterior fontanelle /bregma: Found at junction of sagital coronal and frontal suture.
Broad, diamond shaped.
3-4 cm long and 1.5 – 2cm wide.
Closes at 18 months

Fontanelles. Posterior fontanelle or lambda:
located at junction of lambdoid and sagital sutures.
Triangular
Closes by 6 weeks of age


Diameters of fetal skull:
Biparietal diameter : this is 9.5 cm . this is the diameter between two parietal eminences.
Bitemporal diameter: this is 8.2 cm- diameter between the furthest points of the coronal suture at the temples.

Super sub parietal -8.5 cm. – it extends from a point placed below one parietal eminence to a point placed above the other parietal eminence. Of the opposite side.
Bi-mastoid diameter-7.5cm- it is the distance between the tips of the mastoid processes. The diameter is incompressible and it is impossible to reduce the length of the bimastoid diameter by obstetrical operation.

Suboccipitobregmatic: This is 9.5 cm, the diameter from below the occipital protuberance to the centre of the anterior fontanelle or bregma.
Suboccipitofrontal: This is 10 cm- the diameter from below the occipital protuberance to the center of the frontal suture
Occipitofrontal: This is 11.5 cm- the diameter from the occipito protuberance to the glabella.

Mentovertical: This is 13.5 cm- the diameter from the point of the chin to the highest point on the vertex
Submentovertical: This is 11.5 cm- the diameter from the point where the chin joins the neck to the highest point on the vertex.
Submentobregmatic: This is 9.5 cm-the diameter from the point where the chin joins the neck to the centre of the bregma.



MOULDING OF THE HEAD
Occurs with descent of the fetal head into the pelvis to reduce the head circumference
Frontal bones slip under parietal bones
Parietal bones override each other
Parietal bones slip under the occipital bone

MOULDING OF THE HEAD
DEGREE OF MOULDINGAssessed vaginally 0 suture lines are separate +1 suture lines meet +2 suture lines overlap but can be reduced by
gentle digital pressure +3 overlap irreducible

Caput succedaneum

Cephal hematoma

False cerebri and tentorium cerebelli

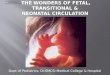
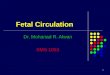
Fetal circulation


The fetal circulation differs mainly from the adult ones by the presence of 3 major vascular shunts. Ductus venosus: between umbilical vein and inferior venacava
Foramen ovale: Between the right and left atrium
Ductus arteriosus: Between the pulmonary artery and descending aorta.


1. The umbilical vein transports blood rich in oxygen and nutrients from the placenta to the fetal body. This vein travels along the anterior abdominal wall of the fetus to the liver, and then the umbilical vein divides into branches.
2. About half of the blood passes into the liver and the rest enters a shunting vessel called ductus venosus that bypasses the liver. The ductus venosus travels a short distance and joins the inferior venacava.


3. There the oxygenated blood from the placenta is mixed with deoxygenated blood from the lower parts of the fetal body. This blood continues through the venacava to the right atrium.
4. As the blood relatively high in oxygen enters the right atrium of the fetal heart, a large proportion of it is shunted directly into the left atrium through an opening in the atrial septum called the foramen ovale.

5. The more highly oxygenated blood that enters the left atrium through the foramen ovale is mixed with a small amount of deoxygenated blood returning from the pulmonary veins. This mixture moves into the left ventricle and is pumped into the aorta.
6. Some of this blood reaches the myocardium by means of coronary arteries. And some reaches the tissues of the brain through the carotid arteries.


7. The rest of the blood entering the right atrium, as well as the large proportion of the deoxygenated blood entering from the superior venacava, passes into the right ventricle and out through the pulmonary artery
8. Enough blood reaches the lung tissue to sustain them. Most of the blood in the pulmonary artery bypasses the lungs by entering the ductus arteriosus, which connects the pulmonary artery to the descending portion of the aorta arch

9. Some of the blood carried by the descending aorta leads to various parts in the lower regions of the body.
10.The rest of the blood passes into the umbilical arteries which branch from internal iliac arteries and lead to the placenta.


REVIEW OF LITERATURE
Noninvasive Assessment of the Early Transitional Circulation in Healthy Term Infants.
Author: Popat H, Kluckow M.
Source Department of Neonatology, Royal
North Shore Hospital and University of Sydney, Sydney, N.S.W., Australia.

Abstract Background: The early neonatal
circulatory transition usually occurs smoothly but occasionally it is incomplete or reverts to the fetal state of high pulmonary vascular resistance, resulting in significant neonatal morbidity.
Objective: To define the normal values for echocardiographic parameters during the early transitional circulation in term infants.

Methods: Two-dimensional, M-mode, pulsed
and color flow Doppler echocardiography
was used to assess healthy term infants in
the first 4 h of life. Left and right ventricular
outputs (LVO and RVO) and myocardial
performance indices (MPI), left ventricular
fractional shortening, end-systolic diameter
and end-diastolic diameter, ductal size,
shunt and peak velocities, tricuspid
regurgitation and left pulmonary artery
diastolic velocities were documented.

Results: A total of 21 normal term infants were
assessed with median gestation of 39 weeks, birth
weight of 3,470 g and postnatal age of 3 h and 22
min. The median echocardiographic values were
LVO 193 ml/kg/min, RVO 216 ml/kg/min, left MPI
0.41, right MPI 0.63, and fractional shortening 29%.
The ductus was patent in all 21 infants with a
median size of 2.3 mm; ductal flow was bidirectional
in 86% with median peak left-to-right velocity of
1.07 m/s. The median left pulmonary artery diastolic
velocity was 0.31 m/s and physiological tricuspid
regurgitation was present in all infants.

Conclusion: This study defines normal
values for echocardiographic
measurements in healthy term infants
during the first 4 h after birth. These
normative data may be useful in early
identification of infants with abnormal
circulatory transition, allowing more
rapid determination of cardiovascular
dysfunction.

2. journal of reproductive medicine. 1976 Jun;16(6):321-4.
Intrauterine spontaneous depression of fetal skull: a case report and review of literature.
Author: Guha-Ray DK.

Abstract
Intrauterine depression of fetal skull,
with or without fracture, unassociated
with any known trauma during
pregnancy or delivery, is extremely
rare in Western countries though not
so rare in Africa among African women.
Usually fetal skull depression is caused
by forceps or digital pressure of the
obstetrician during manual rotation.

Forty such cases are reported in the
literature-nine in Western countries and
the remaining 31 over a period of three
years at Harare Hospital Maternity
Centre, Salisbury, Rhodesia, Africa.
There, an incidence of one in 4,000
deliveries was observed among the
African women but none in 6,000
deliveries of European women during the
same period at a nearby hospital.

The presentation of this paper is made
in view of the rarity of intrauterine
spontaneous fetal skull depression in
Western countries and the not so
infrequent occurrence in African and
possibly other developing countries
and because of the persistent
controversy about the treatment of
this condition.

3.child’s nervous system:ChNS: Official journal of the international society for pediatric neuro surgery . 1996 Feb;12(2):117-20.
Craniocerebral birth trauma caused by vacuum extraction: a case of growing skull fracture as a perinatal complication.
AUTHOR: Papaefthymiou G, Oberbauer R, Pendl G.
Source Universitäts-Klinik für Neurochirurgie,
Karl-Franzens-Universität Graz, Austria.

Abstract
A case of growing skull fracture
following birth trauma and caused by
vacuum extraction is reported in order
to emphasize the incidence of this
peculiar head injury at the beginning
of extrauterine life and to point out its
relation to possible neuropsychological
disturbances that may appear later in
childhood.

Delivery by vacuum extraction increases the
incidence of perinatal injuries and
consequently the incidence of neurological
deficits in children. Neurosurgical repair is
advocated as the appropriate treatment, with
the aim not only of cosmetically correcting
the lesion's typical subgaleal protuberance
with cranioplasty, but also of performing a
water-tight closure of the dura, enabling the
cerebral cortex to "fill in" the intracerebral
lesion

The surgical technique and gross pathology of
the lesion are described together with
radiological findings before and after surgery.
Reports by other authors are reviewed in an
attempt to identify the conditioning factors and
pathological features of this traumatic injury to
skull and brain in neonates and infants. The
literature on cranial fractures associated with
intracerebral lesions at this age shows a
significant difference in recovery and outcome
from that after similar lesions in older children.

Bibliography
Brian Magowan, Philip Owen, James Drife, Clinical obstetrics and gynecology, second edition, Edinburgh. Elseviers Ltd. 2009
D. C Dutta Textbook of obstetrics including
perinatology and contraception, 6th edition. Culcutta. Published by new central book agency private Ltd.
Diane M Fraser, Margerett A Cooper. Myles
textbook of midwives. 15th edition. London. Elsevier publication 2009

Holland and Brews. Manual of obstetrics , updated by Shirish N Daftary, Sudip Chakravarthy 3rd edition . Chennai. Elsevier India pvt ltd 2011.
Kamini Rao. Textbook of midwifery and obstetrics
for nursing . Newdelhi. Elseviers publication 2011 Oa Ojo Enang Bassery Briggs . A textbook for
midwives in the tropics. 2nd edition. Newdelhi Jaypee brothers pvt ltd.
Lowdermilk , Perry. Matternity Nursing 7th edition .
Missouri; Elseviers Pvt Ltd 1983.