Embed Size (px)
DESCRIPTION
Presentation on Fetal Circulation
Citation preview

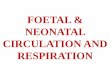
THE WONDERS OF FETAL, TRANSITIONAL &
NEONATAL CIRCULATION
Dept of Pediatrics, Dr.SMCSI Medical College & Hospital

The Fetal Circulation

Introduction:
"Nature is neither lazy nor devoid of foresight. Having given the matter thought, she knows in advance that the lung of the fetus does not require the same arrangements of a perfected lung. She has therefore anastomosed the pulmonary artery with the aorta, and the left and right atria. . . .“
-Galen, 2nd
Century

FETAL NEWBORN
Gas exchange Placenta Lungs
RV,LV circuit Parallel Series
Pulmonary circulation Vasoconstricted Dilated
Fetal myocardiumContractility,Compliance Less Good
Dominant ventricle Right Left
Change in Structure Umbilical vein Ligamentum teres Umbilical artery Medial umb ligament Ductus venosus Ligamentum venosum Ductus arteriosus Ligamentum
arteriosum Foramen ovale Fossa ovalis

4 unique FETAL CVS structures : FOUR SHUNTS

COURSE OF FETAL CIRCULATION: 1.Placenta: Has the lowest vascular resistance in the fetus. Receives the largest amount of combined (Rt + Lt) Ventricular Output (55%)
Placenta

2. Superior Vena Cava: Drains the upper part of the body,including the brain
(15% of combined ventricular output). Most of SVC blood goes to the Right Ventricle.

3. Inferior Vena Cava: Drains lower part of body and placenta (70% of combined ventricular output)
Part of IVC blood with high O2 goes into LA via Foramen Ovale.
Remaining IVC blood enter RV and Pulmonary artery.
Since blood is oxygenated in the placenta, Oxygen saturation in IVC (PO2 = 26-28%) is higher than that in SVC (12-14%).

COURSE OF FETAL CIRCULATION: Most of SVC blood (less oxygenated blood) goes into RV. Most of IVC blood (high O2 concentration) is directed by the
Crista Dividens to the LA through Foramen ovale. Rest of IVC blood enters RV & pulmonary artery. Less oxygenated blood in Pulmonary artery flows through
Ductus Arteriosus to descending aorta and then to placenta for oxygenation.

COURSE OF FETAL CIRCULATION: The Result is: Brain and coronary circulation receive blood with
higher concentration (PO2 = 28 mm Hg) than the lower part of the body (PO2 = 24 mm Hg)

FETAL CIRCULATION: The pathway: Placenta Oxygenated blood Umbilical vein Hepatic circulation Bypasses liver &
joins IVC via ductus
venosus
Partially mixes with poorly oxygenated IVC
blood derived from lower part of fetal body
Umbilical vein
Hepatic portal vein
Ductus venosus

FETAL CIRCULATION:
Combined lower body blood plus umbilical venous blood flow (PO2 of ≈26–28 mm Hg) passes through IVC to the Right atrium and is preferentially directed across the foramen ovale to the left atrium.
The blood then flows into the left ventricle and is ejected into the ascending aorta.
Fetal SVC blood, which is considerably less oxygenated (PO2 of 12–14 mm Hg), enters the Right atrium and preferentially traverses the tricuspid valve, rather than the foramen ovale, and flows primarily to the right ventricle.

FETAL CIRCULATION:
From the right ventricle Pulmonary artery.
Because the pulmonary arterial circulation is vasoconstricted, only about 10% of right ventricular outflow enters the lungs.
The rest 90% blood (which has a PO2 of ≈18–22 mm Hg) bypasses the lungs and flows through the ductus arteriosus into the descending aorta to perfuse the lower part of the fetal body.
It the returns to the placenta via the two umbilical arteries.

Thus, upper part of fetal body (including coronary & cerebral arteries and those to upper extremities) is perfused exclusively from the Left ventricle with blood that has a slightly higher PO2 , than the blood perfusing the lower part of the fetal body, which is derived mostly from the Right ventricle.
Only a small volume of blood from the ascending aorta
(10% of fetal cardiac output) flows across the aortic isthmus to the descending aorta.

Thus, upper part of fetal body (including coronary & cerebral arteries and those to upper extremities) is perfused exclusively from the Left ventricle with blood that has a slightly higher PO2 , than the blood perfusing the lower part of the fetal body, which is derived mostly from the Right ventricle.
Only a small volume of blood from the ascending aorta
(10% of fetal cardiac output) flows across the aortic isthmus to the descending aorta.

LA LV Aorta Ductus arteriosus Foramen ovale RV SVC
upper body IVC
50% through 50% to ductus venosus Portal
circulation
Umbilical Vein
Oxy.blood PLACENTA
Pulm artery Lungs

Aorta Deoxygenated blood
Descending aorta
Abdominal aorta
Common iliac artery
Umbilical arteries
PLACENTA Oxygenation
Umbilical Vein

FETAL CIRCULATION: The total fetal cardiac output—the combined
output of both the left and right ventricles—is ≈ 450 mL/kg/min.
Descending aortic blood flow : -65% returns to placenta; -Remaining 35% perfuses the fetal organs
& tissues.
Right ventricular output is about 1.3 times the left ventricular flow.
Thus, during fetal life the right ventricle -is pumping against systemic blood
pressure -is performing greater volume of work
than LV.

The Transitional Circulation

TRANSITIONAL CIRCULATION:
At birth
Mechanical expansion of lungs Increase in arterial PO2
Rapid DECREASE in pulmonary vascular resistance
Removal of the low-resistance placental
circulation
INCREASE in systemic vascular resistance.

TRANSITIONAL CIRCULATION:
Right ventricle output now flows entirely into the pulmonary circulation.
Pulmonary vascular resistance becomes lower than systemic vascular resistance,
Shunt through ductus arteriosus
reverses & becomes left to right.

TRANSITIONAL CIRCULATION:
High arterial PO2 (In several days)
Constriction of ductus arteriosus
It closes, becoming the ligamentum arteriosum.

TRANSITIONAL CIRCULATION: Increased volume of pulmonary blood
flow returning to left atrium
Increases left atrial volume and pressure
Closure of foramen ovale (functionally) (Although the foramen may remain probe
patent)
Becomes Fossa Ovalis

Removal of the placenta from the
circulation
Also results in closure of the ductus venosus.
The left ventricle is now coupled to the high-resistance systemic circulation its wall thickness and mass begin to increase.
In contrast, the right ventricle is now coupled to the low-resistance pulmonary circulation its wall thickness and mass decrease slightly.

The left ventricle in the fetus pumped blood only to the upper part of the body and brain
After birth, LV must deliver the entire systemic cardiac output (≈350 mL/kg/min). (almost 200% increase in output)
This marked increase in left ventricular performance is achieved through a combination of hormonal and metabolic signals, including an INCREASE IN :
-The level of circulating catecholamines and
-The myocardial receptors (β-adrenergic)
(through which catecholamines have their effect)

When congenital structural cardiac defects are superimposed on these dramatic physiologic changes, they often impede this smooth transition and markedly increase the burden on the newborn myocardium.
In addition, because the ductus arteriosus and foramen ovale do not close completely at birth, they may remain patent in certain congenital cardiac lesions.

Patency of these fetal pathways may either : Provide a lifesaving pathway for blood to bypass a
congenital defect (eg: -Patent ductus in Pulmonary atresia or COA. -Foramen ovale in Transposition of the great
vessels) or Present an additional stress to the circulation (eg: -Patent ductus arteriosus in a premature
infant, -RtLt shunt in infants with pulmonary
hypertension)
Therapeutic agents may either : Maintain fetal pathways open - PGE1
Promote their closure - Indomethacin
POLICE – PGE1 Opens,
Indomethacin Closes

The Neonatal Circulation

Neonatal Circulation: Adaptation to extrauterine life: Some of these
changes are instantaneous with the 1st breath, whereas others develop over a period of hours or days.
Gas exchange: Transferred from the placenta to the lungs.
Systemic blood pressure: After an initial slight fall in systemic BP, progressive rise occurs with increasing age.
Heart rate: Elimination of Placental circulation
Increase in systemic vascular resistance
Baroreceptor response Slowing of HR

Neonatal Circulation: Decrease in PVR:
With the onset of ventilation, pulmonary vascular resistance is markedly decreased, as a consequence of both
active (PO2 related) and passive (mechanical related) pulmonary vasodilation.
In a normal neonate, closure of the ductus arteriosus and the fall in pulmonary vascular resistance result in a decrease in pulmonary arterial and right ventricular pressures.

Neonatal Circulation: Decrease in PVR:
The major decline in pulmonary resistance from the high fetal levels to the low “adult” levels in the human infant at sea level usually occurs within the 1st 2–3 days but may be prolonged for 7 days or more.
Over the 1st several weeks of life, pulmonary vascular resistance decreases even further, secondary to remodeling of the pulmonary vasculature, including thinning of the vascular smooth muscle and recruitment of new vessels.

Neonatal Circulation:
Decrease in pulmonary vascular resistance influences the timing of clinical appearance of many congenital heart lesions that are dependent on the relative systemic and pulmonary vascular resistance.
Eg: Left-to-right shunt through VSD may be minimal in 1st wk after birth when pulmonary vascular resistance is still high.
As pulmonary resistance decreases in the next
1-2 weeks, the volume of the left-to-right shunt through an unrestrictive ventricular septal defect increases and eventually leads to symptoms of heart failure.

Differences between neonatal circulation and that of older infants:
(1) Right-to-left or left-to-right shunting may persist across patent foramen ovale;
(2) In the presence of cardiopulmonary disease,
continued patency of ductus arteriosus may allow left-to-right, right-to-left, or bidirectional shunting;
(3) The neonatal pulmonary vasculature constricts more vigorously in response to hypoxemia, hypercapnia, and acidosis;
(4) The wall thickness and muscle mass of the neonatal left and right ventricles are almost equal;

Differences between neonatal circulation and that of older infants: contd…
(5) Newborn infants at rest have relatively high oxygen consumption, which is associated with relatively high cardiac output.
(6) Newborn cardiac output (about 350 mL/kg/min) falls in the 1st 2 mo of life to about 150 mL/kg/min and then more gradually to normal adult C.O of about 75 mL/kg/min.
(7) High percentage of fetal hemoglobin present in the newborn may interfere with delivery of oxygen to tissues in neonate, so increased cardiac output is needed for adequate delivery of oxygen

CLOSURE of:
Foramen ovale : Functional Closure: 3rd month of life. Anatomical closure of septum primum & septum
secundum by 1 year of age.
Ductus arteriosus : Functional Closure: By 10–15 hr in a normal
neonate. Anatomic closure: May take several weeks.

CLOSURE OF DUCTUS ARTERIOSUS:
In a full-term neonate, oxygen is the most important factor controlling ductal closure.
When the PO2 of the blood passing through the ductus reaches about 50 mm Hg, the ductal wall constricts.
The effects of oxygen on ductal smooth muscle may be direct or mediated by its effects on prostaglandin synthesis.
Gestational age also appears to play an important role;
The ductus of a premature infant is less responsive to oxygen, even though its musculature is developed.

SUMMARY

Reference: Nelson Textbook of Pediatrics Park – Pediatric Cardiology for Practitioners Kulkarni – Pediatric Cardiology IB Singh – Embryology O.P Ghai – Essential Pediatrics

Thank you!