Slide 1
Fetal circulationDr Shreetal Rajan Nair Fetal circulationFetal
circulation : Physiological and morphological aspectsPost natal and
transitional circulation: Changes at birth and
thereafterPathophysiological considerations in CHDsAll our present
day knowledge about fetal circulation is based on continuing
research of more than 40 years.
Most of the work has been done in fetal lambs whose circulation
closely resembles to that of human fetal circulation.Fetal
circulation Fetal circulationCentral circulation Arteries Veins
Shunts Peripheral components Various regional vascular beds
Salient featuresPresence of shuntsParallel arrangement of two
main arterial systems and their respective ventricles.Preferential
streaming of blood High impedance and low flow of pulmonary
circulation.Low impedance and high flow of placental
circulation.Placenta is the site of gas exchange
Shunts in the fetal circulation The fetal circulation is
characterised by four shunts.
first, within the placentasecond, across the ductus
venosusthird, through the foramen ovalefourth, across the ductus
arteriosus The PlacentaFacilitates gas and nutrient exchange
between maternal and fetal blood.The blood itself does not mix.
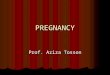
Umbilical CirculationPair of umbilical arteries carry
deoxygenated blood & wastes to placenta.
Umbilical vein carries oxygenated blood and nutrients from the
placenta.
Arrangement of blood vessels in placenta
Oxygen exchange functionHigher hemoglobin level in fetus as
compared to mother facilitates oxygen uptake by the fetus in the
placenta.Oxygen dissociation curve of fetal red cells is shifted to
left as compared to adult red cells.HbF has less affinity towards
organic phosphates like 2,3 DPG and ATP.
Oxygen exchange functionThese phosphates that are present in red
cells compete with oxygen for binding to hemoglobin.Affinity of
reduced hemoglobin to 2,3 DPG is higher than that of oxyhemoglobin
and this facilitates oxygen delivery at tissue site.
Oxygen exchange functionAs CO2 crosses placenta from fetus to
mother, it creates a local acidosis.In the face of decreasing pH,
mothers hemoglobin shows less affinity towards Hb and oxygen
release is enhanced[Bohr effect]This supports diffusion of more
oxygen across the diffusion membrane to fetus. Umbilical vein to
portal circulationSome blood from the umbilical vein enters the
portal circulation allowing the liver to process nutrients.The
majority of the blood enters the ductus venosus, a shunt which
bypasses the liver and puts blood into the hepatic veins.
Foramen ovaleBlood is shunted from right atrium to left atrium,
skipping the lungs.
Is a valve with two flaps that prevent back-flow.
Foramen ovale
Ductus arteriosusThe blood pumped from the right ventricle
enters the pulmonary trunk. Most of this blood is shunted into the
aortic arch through the ductus arteriosus.
Fetal circulation physiologyMost of the unsaturated blood
reaches the right ventricle and this blood is channelled via the
ductus arteriosus and descending aorta to the placenta for
oxygenation
Most of the saturated blood reaches the left ventricle which is
driven into the ascending aorta to the heart and brain
Ref : Moss and Adams textbook of congenital heart diseasesRef :
Moss and Adams textbook of congenital heart diseases21How this is
achieved? By the appropriate mixing of the venous blood returning
to the heart
And its preferential streaming Central venous circulation5
sources: upper body - SVC myocardium coronary sinus the lungs
pulmonary veins the lower body - IVC placenta umbilical vein ductus
venosus IVC
Least saturated blood
From upper body via SVC
From myocardium via coronary sinus
This blood is directed to the RV via the tricuspid valveVenous
return from lungsNot well saturated Preferential flow to RV is not
possible because of the normal drainage of pulmonary veins to LABut
pulmonary blood flow only 8% of combined ventricular outputSo no
appreciable effect on oxygen delivery
Inferior venacaval returnLower body
Placenta
How this blood is preferentially directed to the RVSVC blood is
directed away from the foramen ovale and through the tricuspid
valve due to the leftward and superior course of the eustachian
valve The location of the coronary sinus caudad to the foramen
causes venous blood from the myocardium to flow through the
tricuspid valve to the RV How preferential flow occursLower body
flow except that from the liver ascends the distal IVC and this
stream of relatively desaturated blood enters the lateral margin of
the right atrium and directed to the RV via TVUmbilical venous
return to the LVVenous flow from the liver from right lobe to the
RV and the left lobe to the LV via foramen ovale
Venous return to heartUmbilical vein gives branches to left lobe
of liver and then divides into DV and arcuate vein.Arcuate vein
joins the portal vein and then gives of branches to right lobe of
liver.Left hepatic vein joins the DV at its entry to IVC and Right
hepatic vein joins the IVC directly.
Venous return to heartRight lobe of liver receives poorly
oxygenated portal venous blood and left lobe receives well
oxygenated umbilical venous blood.Both lobes receive small
contribution of blood from hepatic artery.Saturation of RHV is
lower than that of LHV.Venous return to heartPosterior and left
stream of IVC blood carries oxygenated blood while anterior and
right stream carries poorly oxygenated blood.Preferential streaming
of DV and LHV blood across the foramen ovale and abdominal IVC and
RHV blood across the TV.
Venous return to heartEustachian valve helps to direct the IVC
blood to cross the foramen ovale.The lower margin of septum
secundum [crista dividens] helps to direct the left posterior
stream to preferentially across the foramen ovale.SVC blood is
directed aross the TV.
THE PRENATAL PULMONARY CIRCULATIONPhysiologic regulation of
pulmonary vascular resistance Pulmonary vascular resistance in the
fetal lung is initially highThe most prominent factor associated
with high fetal pulmonary vascular resistance is the normally low
blood O2 tension (pulmonary arterial blood pO2 = 17 to 20 torr).PVR
in FETUS is highIn the fetus and newborn, all small pulmonary
arteries have a thicker medial smooth muscle layer in relation to
diameter than similar arteries in adults.This increased muscularity
is partly responsible for the increased vasoreactivity and
pulmonary vascular resistance in the fetus, particularly near
term.PULMONARY CIRCULATIONExperiments show fetal PBF increases
dramatically in response to increase in maternal PO2.This response
is evident only in latter part of gestation.Doppler studies
indicate similar changes in humans as well.Modulation of pulmonary
vascular toneOxygen modulates the production of both prostacyclin
and endothelium-derived nitric oxide (EDNO); two potent vasoactive
substances that may in part underlie the responses of the
developing pulmonary circulation to changes in
oxygenationVasoconstrictors in the pulmonary circulation of the
fetus, such as alpha agonists, thromboxane, and the leukotrienes
are other mediators of increased pulmonary vascular toneCombined
ventricular outputThe combined ventricular outputThe term 'combined
ventricular output(CVO)' has been applied to the output of the two
ventricles, and it also represents total venous return to the fetal
heart.
The right ventricle ejects about 55-65%, and the left only
35-45% of CVO.
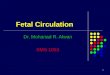
Adapted from Hursts THE HEARTHursts THE HEART43Cardiac output
and its distribution
CVO is 450 ml/kg/wt
UV flow is 200 ml/mt/kg [45% of CVO]
Of this,110 ml/mt [24%] passes through DV and 90 ml/mt[21%]
passes through hepatic circulationCardiac output and its
distribution
Portal venous flow forms 7% and of CVO and abdominal IVC blood
forms 30% of CVO.
Total venous return to heart from IVC is 315 ml/mt and
represents 70% of CVO.
Of this 115 ml/mt [25% of CVO] passes through FO and and 200
ml/mt [44%] passes through TV.Cardiac output and its
distribution
Venous return to heart from SVC is 90 ml/mt/ and represents 21%
of CVO most of this passes through tricuspid valve.
RV ejects about 300 ml/mt or about 55% of CVO.
About 35 ml/mt [8% of CVO] enters the pulmonary circulation
Cardiac output and its distribution
About 265 ml/mt [60%]passes through ductus arteriosus.
LV ejects 150 ml/kg [ 45% ].
Of this,90 ml/mt [20%] distributed to head and upper half and 45
ml/mt [10%]passes through isthmus.
3% of CVO enters coronary circulation.
Cardiac output in human fetus Fetus increases the cardiac output
by increasing the heart rate as it is incapable of increasing the
stroke volume Myocardium is underdeveloped Fluid content is more
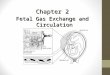
Myocardium surrounded by fluid filled lungBLOOD OXYGEN
SATURATIONS
Adapted from Hursts THE HEART
Blood oxygen saturationsThe highest partial pressure of oxygen
(Po2) is found in the umbilical vein (32 mm Hg) The brain and
coronary circulation receive blood with higher oxygen saturation
(Po2 of 28 mm Hg) when compared to the saturation in the blood
supply to the lower body (Po2 of 24%)The atrial and ventricular
pressures The wide communication at the atrial level (foramen
ovale) allows for near equalization of atrial and ventricular
end-diastolic pressures. Similarly, at the great vessel level, the
nonrestrictive ductus arteriosus allows equalization of systolic
pressures in the aorta and the pulmonary artery and, in the absence
of aortic or pulmonic stenosis, at the ventricular level
Adapted from Hursts THE HEART
Rudolph congenital heart diseases55 What happens at birth?The
change from fetal to postnatal circulation happens very
quickly.Changes are initiated by babys first breath.
Post natal circulationThe changes in the central circulation at
birth are primarily caused by external events rather than by
primary changes in the circulation itself
What are the changes?rapid and large decrease in pulmonary
vascular resistancedisruption of the umbilical-placental
circulationAbruptly at birth, the ductus arteriosus changes from a
right-to-left conduit of blood to the descending aorta, to a
left-to-right conduit of blood to the lungsPOST NATAL PULMONARY
CIRCULATION PULMONARY CIRCULATIONBreathing at birth is associated
with a marked fall in PVR and rise in PBF.PA pressure does not fall
as rapidly and remain elevated till the ductus is widely
patent.Once the ductus is closed, PA pressure can vary independent
of systemic pressure. The transitional circulationIn humans by 24
hours of age, mean pulmonary arterial blood pressure may be only
half systemic. After the initial rapid decrease in pulmonary
vascular resistance and pulmonary arterial blood pressure, there is
a slow, progressive decrease, with adult levels reached after 2 to
6 weeks. This is due to vascular remodeling, muscular involution,
and rheologic changes.
In the first 4 to 6 weeks after birth, there is progressive
involution of the circumferential medial smooth muscle with overall
reduction in medial muscular thickness of the walls of the small
pulmonary arteries
CLOSURE OF THE SHUNTSDuctus arteriosus closurePostnatal closure
of the ductus arteriosus is effected in two phases. Immediately
after birth, contraction and cellular migration of the medial
smooth muscle in the wall of the ductus arteriosus produce
shortening, increased wall thickness, and protrusion into the lumen
of the thickened intima (intimal cushions or mounds), resulting in
functional closure . This commonly occurs within 12 hours after
birth in full-term human infants The second stage usually is
completed by 2 to 3 weeks in human infants, produced by infolding
of the endothelium, disruption and fragmentation of the internal
elastic lamina, proliferation of the subintimal layers, and
hemorrhage and necrosis in the subintimal region. The mounds
enlarge progressively, and there is connective tissue formation and
replacement of muscle fibers with fibrosis and permanent sealing of
the lumen to produce the ligamentum arteriosumClosure of the ductus
arteriosusThe increased level of oxygen probably causes
vasoconstriction of the ductal musculature, but there are strong
suggestions that a reduction in circulating prostaglandins of the E
series plays a roleOxygen, prostaglandin E2 (PGE2) levels, and
maturity of the newborn are important factors in closure of the
ductus. Acetylcholine and bradykinin also constrict the ductus.
Closure of the umbilical vein and ductus venosusAs the placental
circulation stops at birth the flow to the umbilical vein and hence
the ductus venosus stopsIt closes by a process of fibrous
obliteration of the lumen almost similar to the process involved in
the closure of the ductus arteriosusIt completely obliterates by
the seventh postnatal dayClosure of the foramen ovaleClosure of the
foramen ovale at birth is entirely passive, secondary to
alterations in the relative return of blood to the right and left
atriaAt birth combined ventricular output returning from the lung
changes from 8% prenatally to >50% Left atrial pressure thus
exceeds right, and the redundant flap of tissue of the foramen
ovale that previously bowed into the left atrium is now pressed
against the septumFate of the shuntsForamen ovaleCloses shortly
after birth, fuses completely in first year.Ductus arteriosusCloses
soon after birth, becomes ligamentum arteriosum in about 3
months.Ductus venosusLigamentum venosumUmbilical arteriesMedial
umbilical ligamentsUmbilical vein Ligamentum teresBlood circulation
in various regional vascular bedsPost natal changes in various
circulatory bedsSkin blood flow is high in utero as the vessels are
dilated because the skin is exposed to warm amniotic
fluid.Cutaneous vasoconstriction occurs post natally as evaporation
from skin starts.Cutaneous flow falls and the vascular resistance
increases. Post natal changes in various circulatory bedsCoronary
Blood flow decreases dramatically as the oxygen content
increases.
Cerebral circulation also behaves in the same fashion as
coronary circulation. Post natal changes in various circulatory
bedsHepatic blood flow falls rapidly post natally with reduction in
umbilical venous return and then increases as the GI flow is re
established.Hepatic blood flow progressively increases after birth
and by 7 days after birth reaches a level of 250 ml/minute /100 g
by which time there is no flow through ductus venosus.Changes in
Cardiac outputOxygen consumption increases from 6-8 ml/mt/kg body
weight pre natally to 15 20 ml/mt/kg post natallyChanges in Cardiac
outputMechanismsNeonate has to increase the metabolism to increase
the body temperature as it is exposed to external
temperature.Improved diastolic function due to removal of
compression by maternal organs and uterus causes increased cardiac
filling and hence the cardiac output.Changes in Cardiac
outputMechanismsPerinatal increase in thyroid hormones is the
principal mechanism for increase in cardiac output.
Improvement in myocardial growth and maturation brought about by
cortisol may also play important role.Changes in hemoglobin and
tissue oxygen deliveryHuman new born has a high hemoglobin level
(about 16g/dl) so that the oxygen carrying capacity is quiet high
and the total amount of oxygen transported to tissues is quiet
high.Since the Hb F levels are still high facilitation at tissue
site is not as great as in adults.Over the first 8-10 weeks after
the birth,Hb concentration falls to 10-11 g/dl. This is accompanied
by loss of Hb F and almost 100% is adult type. Fetal circulation in
pathological conditionsFetal circulation in pathological
conditionsDevelopment of a structural abnormality will modify the
fetal circulation.This will affect the development of other
components and can lead to other defects.The impact of a defect
will depend on its severity and time of gestation at which it
occurs. Fetal circulation in pathological conditionsCardiovascular
malformations may: cause hydrops fetalis by increasing venous
pressure change the volume or direction of blood flow cause
obstruction to blood flow alter the oxygen saturation of blood
delivered to various organs.Fetal circulation in pathological
conditionsMany of the defects, though it modifies the circulation,
will not significantly affect fetal perfusion and hence the growth
and development.This is because of the presence of shunts and
mixing of blood.Fetus tolerates the obstructive lesions very
much.Fetal circulation is jeopardized by regurgitant lesions and
myocardial disease.
Pulmonary edema in a fetusIncreased fluid accumulation in the
lung of the fetus is manifested as pulmonary lymphangiectasia.This
occurs only in those conditions in which pulmonary venous pressure
can be raised to high levels, such as total pulmonary venous
drainage with obstruction and aortic or mitral atresia with a small
or closed foramen ovale.
PDA O2PGE2,PGE1 and PGI2 concentrationPulmonary vascular
resistance Surfactant replacement therapyAbility of fetal
myocardium to handle cardiac outputSeptal defectsThey in general do
not modify the fetal circulation significantly.VSD may have a
transient left to right shunt in systole.In OP ASD, due to close
proximity of defect with TV, more than normal amount of SVC blood
may enter the LA. Septal defectsIn atrioventricular septal defects,
the obligatory flow from LV to RA will result in decrease in LV
output and an increase in RV output.This will reduce the flow
across the isthmus and can predispose to coarctation.It is the
degree of severity of AV valve lesion and regurgitation which will
determine the outcome.PATENT FORAMEN OVALEASSOCIATIONSCryptogenic
strokedecompression sickness (arterial gas embolism from the venous
side) migraine headaches.Platypnea-orthodeoxia syndrome (dyspnea
and arterial desaturation in the upright position, which improves
on lying down)LVOT ObstructionSevere obstruction developing early
result in a small LV with an increased mass.
RV is able to compensate fully if LVOTO develops slowly.
LVOT ObstructionSVC flow courses normally.
Majority of IVC blood flow crosses TV to RV.
Flow across the ductus increases.
PBF has higher than normal saturation.
A retrograde flow in arch and ascending aorta indicates severe
obstruction
706065626075/490/575/5070/45Aortic arch abnormalitiesMost of the
alteration in the circulation are due to co existing intra cardiac
defects.Common features are, reduced flow in to ascending aorta,
increased flow in to the pulmonary trunk and greater proportion of
CVO carried across ductus to descending aorta.The decreased volume
loading of LV may possibly interfere with its development. Mitral
and aortic atresiaAll blood must pass through RV and ductus has to
provide for both AA and DA blood flow.Complete mixing of blood
occurs in RA and saturation in PA,AA and DA are all same.If the
foramen ovale is sufficiently large and ductus accomodates whole of
systemic blood flow, there will be no significant interference with
intrauterine development and survival. Left to right flow through
foramen ovale seen.
704060606070/270/40Mitral and aortic atresiaIf the foramen ovale
is restrictive, severe pulmonary venous hypertension develops.If
the ductus does not enlarge to accommodate the whole of systemic
blood flow increased blood flow to lungs and pulmonary hypertension
develops.Both these can lead to increased development of smooth
muscle in the pulmonary vasculature.
70406363 6363100/470/3RVOTO with intact IVSIn pulmonary atresia,
all systemic venous blood is carried to left side through foramen
ovale and all blood supply to DA is provided through isthmus.Larger
than normal foramen ovale, left sided chambers,AA and aortic
isthmus.RVOTO with intact IVSIf severe RVOTO develops early in
gestation,the flow through the ductus is reversed and carries only
8 to 10 % of cardiac output.The ductus will be narrower and will
make an acute inferior angle with aorta.The ductus will remain
patent for longer than normal durationRVOTO with intact IVSIf the
fetus develops significant TR,RV pressure remains low and
myocardial sinusoids and coronary fistulae do not develop.If TR
does not develop,significant RV systolic pressure develops and if
occurs early in gestation, intramyocardial sinusoids and coronary
fistulae develop.TAPVCUsually does not affect the development of
fetus.If whole of PV return drains to RA,LV will be totally free of
PV blood and hence will be of higher saturation.Left atrium and
left ventricle will be relatively small in TAPVC.TOF and related
disordersDoes not appear to affect fetal circulation adversely.The
volume and direction of flow across the PA and ductus are dependent
on the severity of obstruction.Total flow through the ductus will
be reduced considerably if there is severe RVOTOTOF and related
disordersThis can markedly reduce the diameter of fetal ductus and
also reduce the development of smooth muscle in its wall.If blood
flows from aorta to PA in fetal life,the orientation of ductus
changes and it forms an acute inferior angle with aorta.AA and the
isthmus carries large than normal amount of blood and they tend to
be larger.
705565636070/470/470/45TOF with absent PVDuctus is frequently
either atretic or not developed.RV would be subjected to both
volume and pressure overload and this can develop in
utero.Significant pulmonary regurgitation can seriously affect
perfusion of pulmonary vessels and cause abnormal development of
intrapulmonary vessels.
TGACompatible with fetal survival and normal intrauterine
development.Does not affect the pattern of venous return.Blood with
higher oxygen saturation will go to lungs. This will reduce the PVR
and hence increase in PBF. TGAThis will reduce the blood flow
across the ductus and increases the flow across the isthmus.Blood
with lower oxygen saturation perfuses coronary and cerebral
circulation.Hence cerebral and coronary blood flow are increased
considerably.
70405570556570/470/370/4570/45TGA with VSDBidirectional shunting
occur depending on after load of each ventricle.
The difference in saturation between AA and DA will be
lesser.TGA with VSD and PSAlmost complete admixture of SVC and IVC
streams in RV.AA and DA will have similar oxygen saturations.Blood
flow in the ductus will be from aorta to PA.
70405565 656570/470/470/45Truncus arteriosusVarious degree of
mixing occurs just above the semilunar valve.Degree of mixing
depends on morphology.In type 1,there is differential streaming of
blood and in others there will be complete mixing. Ductus is
usually small or absent and increased flow traverses through
isthmus and it is large.Ebsteins anomalySevere TR can manifest as
in utero cardiac failure especially if foramen ovale is
restrictive.Marked enlargement of RA and atrialised RV can cause
septal displacement and compromise LV output.Functional pulmonary
atresia can result and ductal flow may be reversed.
Ebsteins anomalyMarked enlargement of right atrium can cause
pulmonary hypoplasia Severe TR alters the preferential drainage of
venacaval blood and causes complete mixing of blood in right
atrium. Tricuspid atresiaAll of the venous return traverses foramen
ovale and it is considerably larger than normal .Complete admixture
of blood in the left atriumIt is compatible with normal
intrauterine development and survival. Tricuspid atresiaIf IVS is
intact, whole PBF is from aorta through ductus and ductal flow is
lesser than normal.75% of combined VO traverses the isthmus and it
tends to be larger.In the presence of VSD, the flow pattern is
decided by the size of the defect and presence of pulmonary
stenosis.
Some clinical pearlsUmbilical vein catherisation Umbilical vein
catheterization may be a life-saving procedure in neonates who
require vascular access and resuscitation. Indications To gain
vascular access during emergency resuscitation,central venous
access in neonate,exchange transfusionsContraindications
Omphalitis,peritonitis,NECSome clinical pearlsThe fact that the
right lobe of the liver receives blood of considerably lower oxygen
saturation probably explains the frequent presence of a larger
number of hemopoietic cells in the right as compared with the left
lobe of the liverREFERENCES1.BRAUNWALDS HEART DISEASES2.HURSTS THE
HEART3.RUDOLPHS CHD4.MYUNG PARKS PEDIATRIC CARDIOLOGY5.
Distribution and regulation of blood flow in the fetal and neonatal
lamb;A M RUDOLPH; Circ Res. 1985;57:811-8216.Preferential streaming
of ductus venosus blood to the brain and heart in fetal
lambs;Edelstone DI, Rudolph AM; 1979 Dec;237(6):H724-9; Am J
Physiol.7. The ductus venosus;Kiserud T; Semin Perinatol. 2001
Feb;25(1):11-20.8. Assessment of Flow Events at the Ductus
VenosusInferior Vena Cava Junction and at the Foramen Ovale in
Fetal Sheep by Use of Multimodal Ultrasound Klaus G. Schmidt,MD;
Norman H. Silverman,MD; Abraham M. Rudolph,MD; Circulation. 1996;
93: 826-833
Thank you
Flow Chart of Fetal Circulation