Embed Size (px)
Citation preview

Breast Cancer Research and Treatment 83: 149–159, 2004.© 2004 Kluwer Academic Publishers. Printed in the Netherlands.
Report
Fatigue, weight gain, lethargy and amenorrhea in breast cancer patientson chemotherapy: is subclinical hypothyroidism the culprit?
Nagi Kumar2, Kathryn A. Allen1, Diane Riccardi1, Barry B. Bercu5, Alan Cantor2,Sue Minton4, Lodovico Balducci3, and Paul B. Jacobsen3
1Department of Nutrition, 2Department of Cancer Control, 3Department of Psychosocial & Palliative Care,4Department of Medical Oncology and 5Department of Pediatrics & Pharmacology & Therapeutics, H. LeeMoffitt Cancer Center & Research Institute, University of South Florida, University of South Florida Collegeof Medicine, Tampa, FL, USA
Key words: breast cancer, cytotoxic therapies, fatigue, thyroid function, weight gain
Precis: Breast cancer patients on cytotoxic agents experience progressive weight gain, amenorrhea, fatigueand lowered physical activity, loss of ovarian function, which are also symptoms of hypothyroidism, indicating thevalue of screening breast cancer patients for thyroid function, including subclinical hypothyroidism at diagnosisor pre-treatment, which may improve quality of life and mortality.
Summary
Background. The purpose of this study was to prospectively observe the relative contribution of each viable mech-anism such as hyperphagia, physical activity, body composition, steroid hormonal and thyroid function, fatiguescores on changes in body weight in breast cancer patients, receiving adjuvant chemotherapy.
Methods. This was a prospective observational research design where 198 consecutive breast cancer patientsreceiving adjuvant chemotherapy were monitored from start to end and 6 months post-therapy on changes inanthropometics, fatigue, nutritional intake, physical activity, thyroid and steroid hormones.
Results. We observed a weight gain over >5 lb in 22.2% of this patient population with a significant andprogressive gain of 6.7 lb (P < 0.0001) at 6 months. Ninety four percent of all patients reported fatigue and 56% ofpatients reported lowered physical activity. A significant reduction in serum free and total estradiol (P < 0.0001)was observed indicative of reduction in ovarian function with 86% amenorrehic at the end of treatment. A signifi-cant reduction in mean serum triiodothyronine uptake levels (P < 0.05), in addition to a significant increase in TBG(P < 0.0001) from baseline to end of chemotherapy, was observed. In addition 20–25% of this patient group wasalready diagnosed with clinical hypothyroidism at diagnosis and treated. Changes in fatigue frequency and serumsex-hormone-binding globulin (SHBG) were variables significantly predictive of weight gain (P < 0.0001).
Conclusions. Cytotoxic agents may influence thyroid function in breast cancer patients contributing to andprogressively worsening symptoms such as weight gain, amenorrhea, fatigue and lowered physical activity inthis population. The present study indicates the value of screening breast cancer patients for thyroid function atdiagnosis or pre-treatment.
Introduction
The American Cancer Society estimates that in 2002about 203,500 new cases of invasive breast cancer(stages I–IV) will be diagnosed among women in theUnited States. Carcinoma in situ (CIS) accounts forabout 54,300 new cases each year. Ranking second
among cancer deaths in women, breast cancer is ex-pected to claim the lives of 39,600 women this year[1]. Most of these patients will be diagnosed with stageI or II disease, and a significant proportion of thesewomen will be treated with chemotherapy in additionto surgery and/or radiation therapy. Although the ben-efits of adjuvant chemotherapy and radiation therapy

150 N Kumar et al.
are well-established, and although several side effectssuch as cancer cachexia challenge the health profes-sionals in other cancers, one of the most distressingside effects as reported by breast cancer patients isweight gain [2–8, 32]. Weight gain, anywhere from5 to 50 lb in breast cancer patients receiving adjuvanttherapy, has now been documented consistently forthe past two decades [9–11, 39, 40] in 50–96% of allbreast cancer patients receiving adjuvant chemother-apy [3] irrespective of stage of disease, more so amongpre-menopausal women compared to post-menopausalwomen [9]. In addition, significant gain in weighthas been observed in patients receiving prednisone asa chemotherapeutic regimen or when multiple agentsare used [10, 39] compared to single agent therapies.Bonadonna et al. found that longer duration of chemo-therapy increased the total amount of weight gained[41] and oral agents produce greater weight gains thaninfusion-based therapies [42]. Weight gain in this pop-ulation may prove to be a more serious side effectthan others, since it cannot only decrease quality oflife but may potentially increase rate of recurrenceand threaten long-term survival [1–3, 8]. The impactof weight gain may be even more profound, becauseit may predispose women to heart disease, diabetes,gall bladder disease, endometrial cancer and ortho-pedic disturbances. These chronic illnesses may posea greater concern, since women with early stage breastcancer will be cured of the disease but may suffer long-term negative consequences as a result of treatment. Inaddition to weight gain, data have consistently demon-strated that cancer-related fatigue is an immense prob-lem associated with pervasive disturbances in qualityof life in addition to functional limitations, negativemood, or sleep disturbances and virtually every aspectof life being affected [43, 44], including both their ownand their caregiver’s careers and economic status [45].Chemotherapeutic agents have been shown to causefibrotic changes and follicular destruction in the ova-ries and pre- and peri-menopausal women have beenobserved to have reduced serum estradiol levels duringchemotherapy [27–29]. Although there have been nosystematic studies, it has also been suggested that hor-monal agents, cytotoxic drugs and radiation therapymay influence thyroid function in breast cancer pa-tients [48]. Although the incidence of these symptomsis widely reported, the etiology of these symptoms stillcontinues to be unclear. It is thus important to sys-tematically examine the etiology of these symptomsand critical to then develop interventions targeted tothis population to enhance functional health status, im-
prove effects of cancer and its treatment and promotehealth behaviors that may reduce the risk of secondmalignancies and thus the threat to long-term sur-vival. The purpose of this study was to prospectivelyand systematically observe the relative contribution ofeach viable mechanism such as nutritional intake (hy-perphagia), physical activity levels, body composition,steroid hormonal function, thyroid function, fatiguescores to changes in body weight in a group of pre-menopausal and post-menopausal stages I–III breastcancer patients, receiving adjuvant chemotherapy.
Subjects and methods
A total of 198 consecutive pre-menopausal and post-menopausal patients recruited over a 36-month period,with primary, operable, stages I–IIIB, auxiliary lymphnode positive and negative breast cancer patients whohad consented to be treated using one of three adju-vant or systemic chemotherapy protocols at theH. Lee Moffitt Cancer Center & Research Insti-tute during the study period were consecutivelyrecruited to the study. Women, of all races andethnicity, between ages 25 and 75, and breast can-cer patients who will receive Cytoxan/ Methotex-trate/5FU (CMF), Cytoxan/Adriamycin/5FU(CAF) orCytoxan/Adriamycin (CA) chemotherapy regimenswith or without radiation therapy at first screeningcontact were admitted to the study.
Upon recruitment, and upon receiving consentfrom subjects, information regarding personal andmedical history, hormonal and reproductive history,exercise, smoking and alcohol use, history and an-thropometric measurements such as subject’s height,weight, skinfolds and circumference measurementswere obtained. Blood was drawn the same time of day,between 7:00 AM and 12:00 noon, for each individualfor analysis of total and free estradiol, sex-hormone-binding globulin and thyroid-binding globulin as-sessment for T3 uptake. Based on our preliminaryobservations of the first 176 subjects recruited, in thelast subset of 22 subjects recruited, the protocol wasamended to include additional thyroid marker assayssuch as serum free and total T4 and TSH levels atbaseline and post-chemotherapy. Subjects completeda self-administered version of the Stanford-five cityProject Questionnaire to monitor Activity Levels, astandard 4-day diet record (FDFR), menstrual histo-ries. The Fatigue Symptom Inventory (FSI) was usedto quantify fatigue in these subjects [1] and this was
Is subclinical hypothyroidism the culprit? 151
obtained from subjects at each visit for chemotherapy.The FSI, is a 14-item self-report measure designedto assess the severity, frequency, and daily patternof fatigue as well as its perceived interference withquality of life. Severity is measured on separate 11-point scales (0 = not at all fatigued; 10 = as fatiguedas I could be) that assess most, least, and averagefatigue in the past week as well as current fatigue.Frequency is measured as the number of days in thepast week (0–7) that respondents felt fatigued as wellas the extent of each day on average they felt fatigued(0 = none of the day; 10 = the entire day). Perceivedinterference is measured on separate 11-point scales(0 = no interference; 10 = extreme interference) thatassess the degree to which fatigue in the past weekwas judged to interfere with general level of activity,ability to bathe and dress, normal work activity, abilityto concentrate, relations with others, enjoyment of life,and mood. These interference ratings can be summedto obtain a total perceived interference score. The finalitem provides qualitative information about possiblediurnal variation in the daily experience of fatigue.Additional information about the FSI can be found inHann et al. (Quality of Life Research, 7, 301–310,1998) [12]. Two-day food records (TDFR) were sub-sequently analyzed by Nutrition IVo software to yieldmacro and micronutrient intake. Upon completion ofthe study, data regarding patients’ disease relatedprognostic indicators were extracted from their med-ical chart. Patients who completed the study were con-tacted by telephone at six (6) months post-completionof chemotherapy to obtain weight at that time.
Statistical analysis
The statistical analyses focused on both the changein weight from baseline to completion of therapyand the change in weight over 6 months post-therapyfrom baseline. The statistical analysis, in additionused paired t-tests to observe changes in mean ste-roid hormones, nutritional intake, thyroid hormones,activity levels and fatigue scores from baseline to endof therapy, using only those patients who completetheir chemotherapy regimen receiving at least 75%of each prescribed drug. This statistical analysis con-sisted of two stages – initial variable screening andmodel building. In the initial screening stage, we con-sidered, in a univariate fashion, the association ofeach variable collected that might be associated withweight gain. For continuous variables, this was done
by calculating the Pearson correlation coefficient ofthat variable with weight gain and its p-value. For dis-crete variables we compared the mean weight gain forthose women with each value of the variable by pooledt-tests (two values) and one-way ANOVAs (more thantwo values). Those variables with at least ‘suggestive’univariate p-values (p < 0.10) were used in a stepwisemultiple regression to determine a set of variables in-dependently predictive of weight gain. This was doneby performing a series of regressions. Each startedwith all of the variables passing this initial screen. Thevariable yielding the smallest p-value was then chosenfirst. In the next step the variable with the smallest p-value in the model based on the variable previouslychosen was added. The process was continued until noadditional variables were significant (p < 0.05) in themodel including the previously chosen variables. Inthis way we were able produce a formula for predict-ing weight gain based on a set of ‘predictor’ variables
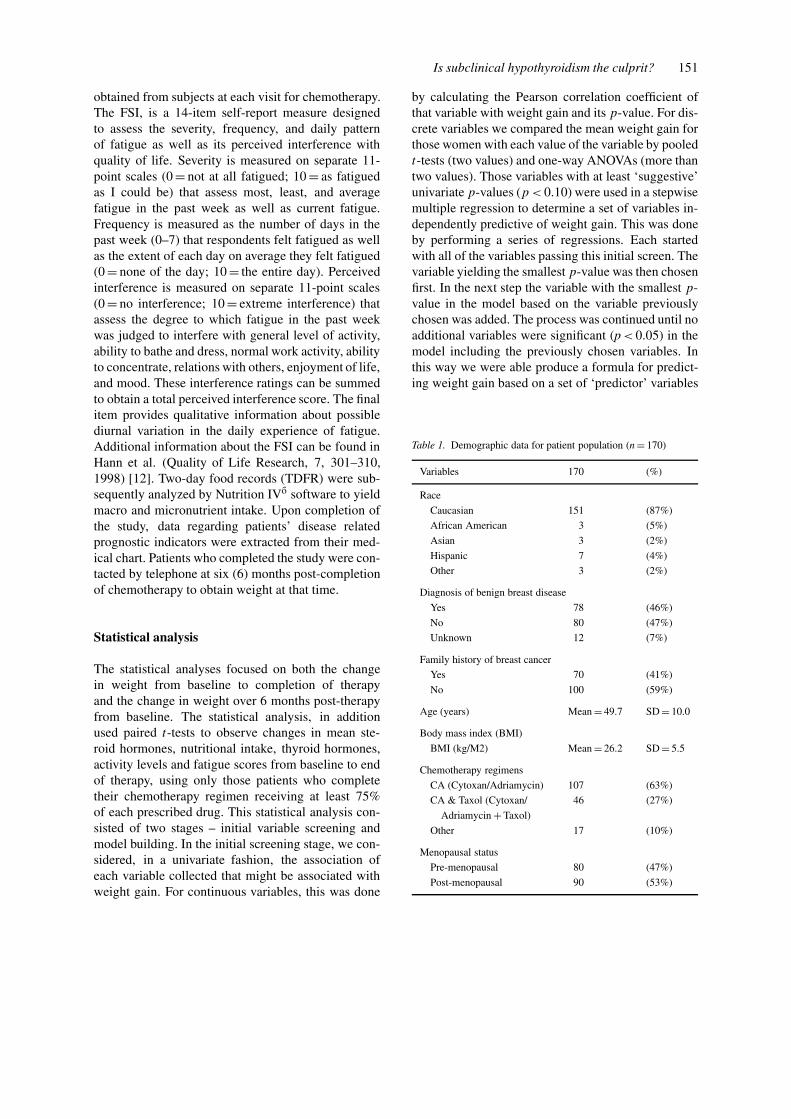
Table 1. Demographic data for patient population (n = 170)
Variables 170 (%)
Race
Caucasian 151 (87%)
African American 3 (5%)
Asian 3 (2%)
Hispanic 7 (4%)
Other 3 (2%)
Diagnosis of benign breast disease
Yes 78 (46%)
No 80 (47%)
Unknown 12 (7%)
Family history of breast cancer
Yes 70 (41%)
No 100 (59%)
Age (years) Mean = 49.7 SD = 10.0
Body mass index (BMI)
BMI (kg/M2) Mean = 26.2 SD = 5.5
Chemotherapy regimens
CA (Cytoxan/Adriamycin) 107 (63%)
CA & Taxol (Cytoxan/ 46 (27%)
Adriamycin + Taxol)
Other 17 (10%)
Menopausal status
Pre-menopausal 80 (47%)
Post-menopausal 90 (53%)

152 N Kumar et al.
Table 2. Weight from baseline to end of chemotherapy and 6 months post-treatment
Variable Baseline End of treatment (n = 170) P 6 months (n = 151) Pa
Mean ± SD Mean ± SD Mean ± SD
Weight (kg) 70.6 ± 14.1 71.0 ± 15.3 0.2 73.7 ± 15.7 <0.0001
a Comparison to baseline, paired t-test.
as well as an estimate for the standard error of each ofits regression coefficient.
Results
One hundred ninety eight (198) subjects were re-cruited, of whom 170 subjects were retained in thestudy until the end of chemotherapy and 151 sub-jects were able to provide weight change data at 6months post-chemotherapy. Twenty eight (28) of the198 subjects who met eligibility criteria and were re-cruited, dropped out of the study during the course ofthe study period. Reason for discontinuing the studywere inability to complete their activity records (14subjects), did not wish to participate anymore (6 sub-jects), or too ill to complete study instruments or thestudy (8 subjects). We have thus successfully recruitedand retained 86% of the sample planned for the study,in a period of 36 months. The demographic data forthe patient population in this study are described inTable 1. A predominant 87% of the women in ourstudy were Caucasian with 13% from minority groups.Forty six percent of the women had a history of fibro-cystic breast disease. Forty one percent (41%) had afamily history (first degree) of breast cancer. The aver-age age of these subjects was 49.7 years and 47% werepre-menopausal prior to start of treatment.
The data on change in weight from baseline topost-treatment are displayed in Table 2. Although thisweight gain at end of treatment was not statisticallysignificant, 22.2% of these patients gained 5 lb or moreduring treatment. We attribute the control of weightgain to close monitoring by dietitians during treat-ment (every 3 weeks) and the self-monitoring tools(2-day diet record) used in the study to document in-take. However, these patients gained an average of6.7 lb at post 6 months from baseline, post-treatment,which was statistically significant (P < 0.0001). Ashypothesized, we observed a significant gain in weightin breast cancer patients undergoing chemotherapy.Although this weight gain was not statistically signifi-cantly immediately at end of treatment, it occurred in
the 6 months from baseline, post-treatment, indicat-ive of progressive weight gain, even after treatment.In addition, there were no significant differences inweight changes in women who were pre-menopausalor post-menopausal at baseline.
Ninety four percent (94%) of all patients report-ed increased frequency of fatigue at end of treatment,compared to 42% at start of treatment as measured bythe Fatigue Symptom Scale. In assessing the severity,frequency, and daily pattern of fatigue as well as itsperceived interference with quality of life scores asmeasured by the Fatigue Symptom Scale (FSI), fa-tigue frequency, which is measured as the number ofdays in the past week (0–7) that respondents felt fa-tigued as well as the extent of each day on averagethey felt fatigued (0 = none of the day; 10 = the entireday) was one of the variables most predictive of weightgain in this patient population (p < 0.05). In addition,56% of patients reported lowered physical activityat the end of treatment compared to baseline activ-ity levels, based on hours of work outside the home.Subjects who gained more than 5 lb during treatmentlowered hours of work by a mean of 6.5 h per weekand subjects who gained less than 5 lb during treat-ment lowered their work hours by a mean of 4.27 hper week, both of which were clinically significant,although not statistically significant.
Two-day food records (TDFR) provided informa-tion on dietary intake, reporting types and amounts offoods consumed, and methods of preparation. Eachpatient completed the TDFR on a weekly basis, at
Table 3. Nutritional intake of major nutrients from baseline to endof chemotherapy (n = 170)
Variable Baseline End of treatment Change Pa
Mean ± SD Mean ± SD
Calories 1460 ± 407 1457 ± 462 −1.17 0.20
(kcal)
Fats (g) 48.9 ± 20.9 50.3 ± 20.1 −1.44 0.15
Fiber (g) 13.9 ± 12.1 12.2 ± 7.8 −2.4 0.1
a Comparison of baseline to end of treatment, paired t-test.

Is subclinical hypothyroidism the culprit? 153
Table 4. Steroid hormone levels from baseline to end of chemotherapy (n = 170)
Variable Baseline End of treatment Change Pa
Mean ± SD Mean ± SD
Free estradiol (pg/Ml) 0.9 ± 1.1 0.4 ± 1.0 −0.6 <0.0001
Total estradiol (pg/ml) 55.8 ± 65.7 23.2 ± 69.0 −33.7 <0.0001
SHBG (nmol/l) 46.8 ± 25.3 59.4 ± 29.0 +12.4 <0.0001
a Comparison of baseline to end of treatment, paired t-test.
Table 5. Thyroid hormone levels from baseline to end of chemotherapy
Variable Baseline End of treatment Change Pa
Mean ± SD Mean ± SD
Free T4 (ng/Dl) (n = 22) 1.54 ± 0.39 1.44 ± 0.40 −0.04 0.70
Total T4 (ug/dl) (n = 22) 7.40 ± 1.94 7.60 ± 1.34 +0.19 <0.0001
T3 uptake (%) (n = 159) 1.04 ± 0.24 0.99 ± 0.14 −0.05 <0.05
TBG (mg/dl) (n = 151) 2.00 ± 0.39 2.19 ± 0.37 +0.19 <0.0001
TSH (mU/l) (n = 22) 1.60 ± 1.17 1.56 ± 1.13 −0.01 0.97
a Comparison of baseline to end of treatment, paired t-test.
baseline through the first 12 weeks of chemother-apy and at post-treatment. Data collected were sub-sequently analyzed by Nutrition IV® software to yield13 dietary analyses, which included total caloriesconsumed (kcal), as well as protein, carbohydrate,and lipid composition (g) and percentages of calo-ries. Changes in nutritional intake of major nutrientsfrom baseline to end of chemotherapy is displayedin Table 3. There were no significant changes innutritional intake of major nutrients contributing to in-creased caloric intake, although we observed changesin eating behaviors during treatment in this patientpopulation. Food aversions were specific and short-lived, and occurred in 83% of the sample, with amean of 2.4 aversions per afflicted patient. Frequencycounts revealed food groups most prone to aversion.Sweet foods represented 12% of total aversions, ac-quired by 28% of the subjects. Other food groupsthat had a higher prevalence of aversion included veg-etables, concentrated largely on strong tasting foodslike tomatoes, onions, coffee, carbonated drinks, spicyfoods, red meats, and fruits, especially citrus. Afrequency count revealed that patients generally ex-perienced short-lived aversions, most of which lastedonly for one cycle of chemotherapy (72.7%) or inthe second cycle of chemotherapy (23.6%). Patientsconsumed newer foods over the course of treatmenteither in response to finding replacements for foodaversions or as a conscious decision to incorporate
healthier food choices into their diet. Patients mostcommonly increased intake of fruits (43.4% patients),vegetables (42.7% of patients), and dairy products(41.3% of patients). Most frequently indicated ‘com-fort’ foods, or those that the patient claimed had a pos-itive physical effect, included dairy products (45.8%of patients), sweet foods (38.2% of patients), and saltyfoods (36.8%patients), such as potato chips and saltinecrackers.
Mean changes in steroid hormone levels frombaseline to end of therapy are displayed in Table 4.There was a significant reduction in mean serum freeestradiol (P < 0.0001) and total estradiol (P < 0.0001)indicative of reduction in ovarian function. Although47% of the subjects in this study were pre-menopausalat baseline, 86% were amenorrehic at the end of treat-ment. In addition, there was a significant increase inmean serum sex-hormone-binding globulin (SHBG)from baseline to end of therapy (P < 0.0001).
Mean changes in thyroid hormones from baselineto end of chemotherapy are displayed in Table 5. Weobserved a significant reduction in mean serum triio-dothyronine (T3) uptake levels (P ≤ 0.05), in additionto a significant increase in TBG (P ≤ 0.0001) frombaseline to end of chemotherapy, possibly indicativeof lowered thyroid function. The baseline mean T3resin uptake levels in the breast cancer patient pop-ulation in this study was 1.04 nmol/l, which is lowerthan the ranges reported in normal adults as well as

154 N Kumar et al.
Table 6. Final model of the stepwise regression procedure with dependent variable: changein weight
Variable Parameter estimate Standard error P
Intercept 1.67640 0.73254 0.0237
Change in SHBG −0.07070 0.02843 0.0142
Change in fatigue frequency −0.47928 0.22161 0.0324
breast cancer patients by Hansen et al. (1999) [16],decreasing further to 0.99 nmol/l after chemotherapy.In a subset of 22 subjects, we examined changesin additional thyroid function parameters. Althoughchanges in serum TSH and total T4 were observed inthis small sample from baseline to post-chemotherapy,these values were still within the normal range andthus unlikely to be clinically significant.
In addition, the subjects who had a previous diag-nosis of hypothyroidism and those who were alreadytaking a thyroid hormone supplement were not includ-ed in our study, and were eliminated during the screen-ing process, as they met the criteria for exclusion,which included those subjects who were clinicallyhypothyroid and were on thyroid hormone supple-mentation. However, we kept a record of all subjectsscreened for this study and the criteria that was used toinclude or not include them from this study. From thisdata, we observed, that one out of every 4–5 patientsscreened to be recruited in this clinical trial, based onthe criteria of exclusion, was eliminated because theyalready had a diagnosis of clinical hypothyroidism atdiagnosis and were on thyroid hormone therapy. Thus20–25% of the breast cancer population was hypo-thyroid and on treatment at diagnosis, even prior tochemotherapy compared to 4–10% who may be sub-clinically hypothyroid [17] in the general population.
Those variables with at least ‘suggestive’ uni-variate p-values (p < 0.10) were used in a stepwisemultiple regression to determine a set of variablesindependently predictive of weight gain. Table 6 dis-plays the final model using the stepwise regression.Based on this model, increase fatigue frequency andserum sex-hormone binding globulin were the vari-ables that significantly predictive of weight gain in thispatient population (p < 0.05).
Discussion
We have thus systematically and prospectively ex-amined the prevalence and the relative contribution
of eating behavior, physical activity, steroid hor-monal changes, thyroid function and fatigue in agroup of breast cancer patients on chemotherapy onweight gain. We observed significant and progressivefatigue, lowered physical activity, amenorrhea andlowered thyroid function, with changes in fatigue fre-quency and serum sex-hormone-binding globulin mostpredictive of weight gain in this patient populationduring chemotherapy. These changes in symptomsoccurred irrespective of menopausal status. Thesechanges in symptoms of fatigue, weight gain, amen-orrhea, lowered physical activity or lethargy, whichwe observed, are also clinical symptoms observedin hypothyroidism. The symptoms were observed tobe progressive from baseline to end of chemotherapyand at 6 months post-chemotherapy from baseline.Although our study had a limited sample with validthyroid markers and thus not conclusive, it is biologi-cally plausible that breast cancer patients may sufferfrom hypothyroidism or be subclinically hypothyroid,even at diagnosis and prior to start of chemotherapy.We thus propose that cytotoxic agents may influencethyroid function in breast cancer patients contribut-ing to and progressively worsening symptoms such asweight gain, amenorrhea, fatigue and lowered physicalactivity in this population.
The association between thyroid disorders and riskof breast cancer has long been a subject of debate.Although several studies have shown the associationbetween thyroid disease and predisposition to breastcancer [52–54], others have not shown this association[49–51], although most of these studies identifiedthyroid disease from clinical histories and medical re-cords and therefore did not consider specific, reliableindices of thyroid function. Epidemiological studieshave shown geographical variations in the prevalenceof breast cancer and attribute this variation at least inpart to thyroid function [14]. Japanese women suf-fering from Hashimoto’s thyroiditis (chronic lympho-cytic thyroiditis) have reportedly a 5-fold increasein breast cancer risk compared to those without evi-dence of autoimmune thyroid disease [15]. However,

Is subclinical hypothyroidism the culprit? 155
when the association of Hashimoto’s thyroiditis andbreast cancer was studied in the US [16], this risk wasnot evident. Recent studies have reported an increasedprevalence of antithyroid antibodies in patients withbreast cancer [52]. Research has, in addition, demon-strated that clinically evident non-toxic goiter is signif-icantly more common in breast cancer patients thanin age-matched controls [54]. Thyroid dysfunction isalso an important problem in patients receiving highdose chemotherapy and bone marrow transplantation(BMT) [48]. Hypothyroidism is one of the most com-mon forms of thyroid disorders after BMT, which isconsidered immune-mediated thyroid injury contribut-ing to the development of post-transplant hypothyroid-ism. These thyroid hormone changes may be mediatedin part by cytokines and inflammatory mediators, in-terfering with the peripheral conversion of T4 to T3,the active and potent thyroid hormone.
Although the classic clinical spectrum of hypo-thyroidism with symptoms of lethargy and myxedemais well known to the practitioner, it is rarely seenin today’s clinical practice [17]. In contrast, practi-tioners frequently see patients with very mild thyroiddysfunction. Unlike patients with overt hypothyroid-ism, these patients have normal levels of thyroxineand triiodothyronine and only mild elevation in thyro-tropin levels. This condition is commonly termed‘subclinical hypothyroidism’ or ‘mild hypothyroid-ism’ [17, 55].
Several pathogenic factors may be attributed to thisassociation. Firstly, since both breast cancer and hy-pothyroidism may have a genetic pre-disposition, thegenetic association cannot be discounted. The pres-ence of an iodine pump in both the thyroid and thebreast [56] makes the association of the effect ofthyroid on breast, biologically plausible [57]. Clin-ical trials have shown a resolution of fibrocystic breastdisease and breast pain in women treated with ele-mental iodine [58]. In a retrospective follow up studyof cancer mortality of 7338 women with thyroid dis-ease, Goldman et al. (1990) [22] observed an excessnumber of deaths in breast cancer survivors withthyroid disease [SMR = 1.6 (95% CI 1.0–2.6)], indi-cating increased cancer mortality in this subgroup ofbreast cancer patients with thyroid disease. The de-gree of thyroid function disturbance correlates withlow levels of thyroid hormones and poor prognosisin severe illnesses. Thus the potential for the exis-tence of mild or subclinical hypothyroidism in breastcancer patients, and the progression of this mild hypo-thyroidism to potentially overt hypothyroidism during
chemotherapy is biologically plausible and cannot bediscounted.
While the cause of weight gain in breast cancerpatients remains unknown, some proposed expla-nations for weight gain in breast cancer patients onchemotherapy include psychological factors such aschange in coping mechanisms leading to a change ineating behavior. However, we failed to observe hy-perphagia in our study and only observed transientchanges in eating behavior that did not have a statis-tical nor clinically significant impact on weight gain.Patients made alternative choices of foods over thecourse of treatment either as a reaction to chemother-apy and to replace foods they displayed aversions to oras a conscious decision to incorporate healthier foodchoices into their diet. While aversions to these foodgroups may reduce intake, increased intake in these‘alternates’ or ‘comfort foods’ may be, conversely, apotential explanation for compensating for this deficit.Weight gain during chemotherapy could thus not beexplained by food choices and changes in eating pat-terns, as these changes were only transient and of shortduration.
Although fatigue is reported widely in breast can-cer patients on treatment and post-treatment [59–65],the physiological basis of fatigue has never been ex-amined and to our knowledge this has never beencorrelated to clinically overt or subclinical hypo-thyroidism in this patient population. A review ofthe literature suggests that breast cancer patients whoundergo adjuvant chemotherapy or autologous bonemarrow transplantation experience clinically signifi-cant levels of fatigue for months or even years fol-lowing the completion of active treatment. In contrast,there is little evidence that patients who receive onlyregional therapy (i.e., surgery plus adjuvant radiother-apy) experience clinically significant fatigue as a long-term treatment side effect [65]. Fatigue is also widelyreported in the literature in patients diagnosed withhypothyroidism. In a recent letter to Lancet, Lindstedtet al. [24] reported relief of symptoms when patientswith chronic fatigue and chronic lymphocytic thyroid-itis were treated with thyroxine. In this large sampleof over 2000, 50% of the patients with 3.0–4.0 mU/lserum concentrations of thyrotropin, had autoimmunethyroid disease. Most patients had normal serum TSH.These findings, in addition to raising questions regard-ing normal reference limits for TSH in the diagnosis ofthyroid dysfunction, raises the question about whetherthe beneficial effects of thyroxine therapy in thesepatients is restricted to thyroid dysfunction or if there

156 N Kumar et al.
is also an effect on autoimmune manifestations ofautoimmune thyroid disease. It may be important torecognize that severe illness of any type predictablyleads to abnormal thyroid function tests with the firstapparent changes occurring in total T3, indicative ofsick euthyroidism. It may be critical to differentiatebetween the overlap of symptoms between patientswith hypothyroidism and sick euthyroidism, as thismay be an important factor that predicts treatment re-sponse. As we did not measure concentrations of totalT3 in this study, which is essential for the diagnosisof sick euthyroid syndrome, we are unable to makethis distinction at this time in this patient population.In addition, as this study was exploratory in nature,to examine the various factors that may contribute toweight gain, we failed to examine thyroid functionmore thoroughly, including subclinical abnormalities.
As reported previously by Huntington and oth-ers [18–20], we observed a significant decrease inphysical activity as indicated in reduction in hoursof employment and purposeful physical activity perweek. The decrease in activity level from fatiguemay contribute to the weight gain patients experi-ence during treatment. Patients who demonstrated ageneral decrease in activity level since beginning treat-ment gained significantly more weight than those whoreported no change or an increase in activity level[18, 19]. Huntington also attributes weight gain ofover 10 lb seen in 50% of patients treated with CMF(cyclophosphamide, methotrexate, and fluorouracil) orCMFVP (CMF plus vincristine and prednisone) to adecrease in activity level during chemotherapy [11,36]. This reduction in physical activity may in fact berelated to fatigue attributed to lowered thyroid func-tion, as thyroid hormones play a critical role in theregulation of resting metabolic rate. If chemotherapycauses a decrease in the production or function ofthyroid hormones, this may further lower metabolicrate. This effect may be even more exaggerated inwomen with pre-existing subclinical hypothyroidism.The decrease in resting metabolic rate may contrib-ute to lowered activity level from fatigue leading toweight gain that patients experience during treatment.Obesity, progressive weight gain, low resting energyexpenditure (REE) and increase body fat percent-age has been reported in hypothyroidism, includingsubclinical hypothyroidism [66]. Similarly, in ourstudy, we observed a progressive significant increasein weight of 6.7 lb, even 6 months post-chemotherapy.Treatment for hyperthyroidism with development ofhypothyroidism, even transiently, was associated with
weight gain [25, 26]. Thus progressive weight gain is acommon phenomena observed both in hypothyroidismand during chemotherapy, specifically in the breastcancer patient population.
Chemotherapeutic agents have been shown tocause fibrotic changes and follicular destruction in theovaries and pre- and peri-menopausal women havebeen observed to have reduced serum estradiol levelsduring chemotherapy [27, 28, 33]. Even though notclearly established, it is questionable if the abruptmenopause induced by chemotherapy can aggravate alatent predisposition towards developing thyroid dys-function. Especially with increasing doses in adjuvantand neo-adjuvant chemotherapy and combination ther-apies including radiation therapy, induction of subclin-ical hypothyroidism is a possibility. Thyroid hormonesproducing an alteration in estrogen metabolism havebeen postulated as a plausible mechanism in breastcancer. It is well known that hypothyroidism impairsreproductive function both in human and experimentalanimals [10, 31]. Experimental and clinical studiessuggest that subclinical hypothyroidism is associatedwith ovulatory dysfunction and infertility [32, 33, 41,42]. Irregular estrous cycle was observed in several an-imal species. In women, hypothyroidism is associatedwith delayed onset of puberty, anovulation, ammen-orrhea or hyperrmenorrhea, menstrual irregularity,infertility and increased frequency of spontaneousabortions, all of which may be attributed to decreasedLH secretion [10]. Severe hypothyroidism is com-monly associated with failure to ovulate. In addition,in animal models, hypothyroidism produced a dys-function in the pituitary–ovarian axis that impairedfollicular maturation and development of corpora lutea[10, 37, 46]. In women with subclinical hypothyroid-ism and ovulatory dysfunction, thyroxine therapy mayrestore fertility. Hypothyroidism and low iodine intakemay be important etiological factors of estrogen de-pendent tumors of the breast, endometrium and ovary.In addition, an increased incidence of galactorheacaused by hyperprolactinemia has been observed inwomen with hypothyroidism. It is proposed [13, 35]that estrogen receptor density may be increased in hy-pothyroidism as is certain monoamine receptor densit-ies, which would amplify the effect of high circulatingestrogen levels in hypothyroidism. A recent reporthas shown that in women with hypothyroidism treatedwith thyroxine, estrogen therapy may increase theneed for thyroxine as adequate concentrations of T4must be present for estrogenization to occur [11, 36,37, 66]. On the other hand, in women receiving andro-

Is subclinical hypothyroidism the culprit? 157
gen therapy for breast cancer, a requirement to reducethe dose of levothyroxine has been reported [25, 36].In addition to increase in body fat, menopause is alsoknown to trigger a change in body fat distributionwith a shift from gluteal/femoral fat to the abdominalarea which is associated with lowered metabolic activ-ity [27–30], which can be demonstrably preventedwith estrogen replacement therapy. Variations in basalmetabolic rate (BMR) of up to 6–10% have also beenreported to occur during the course of the menstrualcycle [47, 67] possibly secondary to changes in theendocrine state [27, 28]. This effect may be even moreexaggerated in women with pre-existing subclinicalhypothyroidism.
In addition, we observed a significant increase inmean serum sex-hormone-binding globulin (SHBG)from baseline to end of therapy (P < 0.0001). Thischange in steroid hormones may in addition, be a re-sult of treatment for breast cancer, which is targetingsteroid hormone function. We and others have showna decreased serum SHBG in breast cancer patientsand inversely higher levels of serum free estradiolcompared to controls subject, free of breast cancer[1]. In addition, liver sex-hormone-binding globulinbiosynthesis is regulated by triiodothyronine (T3). Hy-pothyroid patients have a higher proportion of moreacidic SHBG isoforms [14, 15]. Body mass index,body composition and thyroid function, have all beenassociated with changes in SHBG, as observed in thisstudy.
Future directions
Although it is well established that patients withtreated hyperthyroidism, neck irradiation, post-partumthyroiditis and certain autoimmune disorders, are atincreased risk of hypothyroidism [17], to date, thepotential for the existence of mild or subclinical hy-pothyroidism in breast cancer patients, and the pro-gression of this mild hypothyroidism to potentiallyovert hypothyroidism during chemotherapy has neverbeen studied. To our knowledge, our study is thefirst to identify the potential for this to exist in thispatient population and an explanation for the pos-sible physiological basis of fatigue and weight gainin breast cancer patients on chemotherapy. Mostimportantly, the present study indicates the value ofscreening breast cancer patients for thyroid functionat diagnosis or pre-treatment. In addition, the efficacyof treating breast cancer patients with hypothyroid-
ism (subclinical to overt), if present at diagnosis, withthyroid hormone therapy to prevent progression toovert hypothyroidism, and the extent to which symp-toms of weight gain, depression, amenorrhea andfatigue can be reversed, remains unanswered.
It is critical to first characterize variances in thyroidfunction in breast cancer patients compared to age andmenopausal stage-matched controls using sensitivemarkers of thyroid function in evaluating potential ab-normalities, including subclinical abnormalities. Thisrelationship may also be an important factor in theindividual’s susceptibility to breast cancer. If thereis an association between thyroid function and breastcancer risk, this is a subgroup of patients who mustbe screened/assessed and treated to prevent furtherprogress of thyroid dysfunction during treatments forcancer, such as chemotherapy and radiation therapy, toovert hypothyroidism. A therapeutic trial of efficacyof treating hypothyroidism is warranted in this groupof patients. If effective, this may prevent the resultingsymptoms such as fatigue, weight gain, depression,amenorrhea and poor quality of life, which may posea threat to long-term survival.
Acknowledgements
We thank Margaret Huffman DTR and Jayne Wellnerfor their assistance with data analysis and manage-ment. This study was supported by The U.S. ArmyMedical Research and Material Command DAMD-17-98-8240.
References
1. Cancer Facts & Figures. American Cancer Society, Atlanta2003
2. Knobf MK, Mullen JC, Xistris D, Mortiz PA: Weight gain inwomen with breast cancer receiving adjuvant chemotherapy.Oncol Nurs Forum 10: 28–34, 1983
3. Huntington MO: Weight gain in patients receiving ad-juvant chemotherapy for carcinoma of the breast. Cancer 56:472–474, 1985
4. Boyd NF: Nutrition and breast cancer. J Natl Cancer Inst 85:6–7, 1993
5. Prozato P et al.: Megasterol acetate: phase II study of a singledaily administration in advanced breast cancer. Breast CancerRes Treat 17: 51–54, 1990
6. Dixon J, Moritz D, Baker F: Breast cancer and weight gain; anunexpected finding. Oncol Nurs Forum 5: 5–7, 1978
7. Demark-Wahnefried W, Winer EP, Rimer BK: Why womengain weight with adjuvant chemotherapy for breast cancer. JClin Oncol 11: 1418–1429, 1993
158 N Kumar et al.
8. Levine EG, Racqynski JM, Carpenter JT: Weight gain withbreast cancer adjuvant treatment. Cancer 67: 1954–1959, 1991
9. Camoriano JK, Loprinzi CL, Ingle JN, Therneau TM, KrookJE, Veeder MH: Weight change in women treated with ad-juvant therapy or observed following mastectomy for node-positive breast cancer. J Clin Oncol 8: 1327–1334, 1990
10. Chlebowski RT, Weiner JM, Reynolds R et al.: Long-termsurvival following relapse after 5-FU but not CMF adjuvantbreast cancer therapy. Breast Cancer Res Treat 7: 23–30, 1986
11. Cruz JM, Muss HB, Brockschidt JK, Evans G: Weight changesin women with metastatic breast cancer treated with mega-sterol acetate: a comparison of standard versus high-dosetherapy. Semin Oncol 17: 63–67, 1990
12. Hann et al.: Qual Life Res 7: 301–310, 199813. Schapira DV, Kumar NB, Lyman GH: Obesity, body fat distri-
bution and sex hormones in breast cancer patients. Cancer 67:2215–2218, 1991
14. Brenta G, Schnitman M, Gurfinkiel M, Damilano S, PieriniA, Sinay I, Pisarev MA: Variations of sex hormone-bindingglobulin in thyroid dysfunction. Thyroid 9: 273–277, 1999
15. Brenta G, Bedecarras P, Schnitman M, Gurfinkiel M,Damilano S, Campo S, Pisarev MA: Characterization of sexhormone-binding globulin isoforms in hypothyroid women.Thyroid 12: 101–105, 2002
16. Hansen D, Bennendbaek FN, Hansen LK et al.: Thyroid func-tion, morphology and autoimmunity in young patients withinsulin-dependent diabetes mellitus. Eur J Endocrinol 140:512–518, 1999
17. Cooper DS: Subclinical hypothyroidism. N Engl J Med 345:260–265, 2001
18. Huntington MO: Weight gain in patients receiving ad-juvant chemotherapy for carcinoma of the breast. Cancer 56:472–474, 1985
19. Demark-Wahnefried W et al.: Reduced rates of metabo-lism and decreased physical activity in breast cancer pa-tients receiving adjuvant chemotherapy. Am J Clin Nutr 65:1495–1501, 1997
20. DeGeorge D, Gray JJ, Fetting JH, Rolls BJ: Weight gain inpatients with breast cancer receiving adjuvant treatment as afunction of restraint, disinhibition, and hunger. Oncol NursForum 17(Suppl): 23–30, 1990
21. Kumar NB, Cantor A, Allen K, Cox CE: Android obesityat diagnosis and breast carcinoma survival. Cancer 88:2751–2757, 2000
22. Goldman MB, Monson RR, Maloof F: Cancer mortality inwomen with thyroid disease. Cancer Res 50: 2283–2289, 1990
23. Stein KD, Jacobsen PB, Hann DM, Greenberg H, Lyman G:Impact of hot flashes on quality of life among postmeno-pausal women being treated for breast cancer. J Pain SymptomManage 19: 436–445, 2000
24. Lindstedt G, Eggertsen R, Sundbeck G, Eden S, Nystrom E:Thyroid dysfunction and chronic fatigue. Lancet 358(9276):151, 2001
25. Dale J, Daykin J, Holder R et al.: Weight gain followingtreatment for hyperthyroidism. Clin Endocrinol 55: 233–239,2001
26. Tigas S, Idiculla J, Beckett G, Toft A: Is excessive weightgain after ablative treatment of hyperthyroid due to inadequatethyroid hormone therapy? Thyroid 10: 1107–1111, 2000
27. Lincoln SR, Ke RW, Kutteh WH: Screening for hypothyroid-ism in infertile women. J Reprod Med 44(5): 455–457,1999
28. Krassas GE: Thyroid disease and female reproduction. FertilSteril 74: 1063–1070, 2000
29. Doufas AG, Mastorakos G: The hypothalamic–pituitary–thyroid axis and the female reproductive system. Ann NYAcad Sci 900: 65–76, 2000
30. Clur A: Di-iodothyronine as part of the oestradiol and cat-echol estrogen receptor – the role of iodine: resting metabolicrate and diet induced thermogenesis in abdominal and gluteal-femoral obese women before and after weight reduction. AmJ Clin Nutr 47: 840–847, 1988
31. Pringle T: The relationship between thyroxine, oestradiol,and postnatal alopecia, with relevance to women’s health ingeneral. Med Hypotheses 55: 445–449, 2000
32. Foltz AT: Weight gain among stage II breast cancer patients: astudy of five factors. Oncol Nurs Forum 12: 21–26, 1985
33. Rose D, Davies T: Ovarian function in patients receiving ad-juvant chemotherapy for breast cancer. Lancet 1: 1174–1176,1977
34. Wade GN, Gray JM, Blaustein JD: Effects of estrogens andantiestrogens on eating behavior, metabolism, and energybalance 7(Suppl): 61–68, 1993
35. denBesten C, Vansant G, Westrate JA, et Poirier MF, LooH, Galinowski A et al.: Sensitive assay of thyroid stimulat-ing hormone in depressed patients. Psychiatry Res 57: 41–48,1995
36. Sher L, Rosenthal NE, Wehr TA: Free thyroxine and thyroid-stimulating hormone levels in patients with seasonal affectivedisorder and matched controls. J Affect Disord 56: 195–199,1999
37. Armada-Dias L, Carvalho JJ, Breitenbach MMD et al.: Is theinfertility in hypothyroidism mainly due to ovarian or pituitaryfunctional changes? Br J Med Biol Res 34: 1209–1215, 2001
38. Arafah BM: Increased need for thyroxine in women with hy-pothyroidism during estrogen therapy. N Engl J Med 344:1743–1749, 2001
39. Heasmand KZ, Sutherland HJ, Campbell JA: Weight gain dur-ing adjuvant Chemotherapy for breast cancer. Breast CancerRes Treat 5: 195–200, 1985
40. Huntington MO: Weight gain in patients receiving adjuvantchemotherapy for carcinoma of the breast. Cancer 56: 472–474, 1985
41. Bonadonna G, Valagussa P, Rossi A: Ten-year experiencewith CMF based adjuvant chemotherapy in resectable breastcancer. Breast Cancer Res Treat 5: 95–115, 1985
42. Knobf M: Physical and psychological distress associated withadjuvant chemotherapy in women with breast cancer. J ClinOncol 4: 678–684, 1986
43. Portenoy RK, Miaskowski C: Assessment and management ofcancer-related fatigue. In: Berger A, Weissman D, PortenoyRK (eds) Principles and Practice of Supportive Oncology. JBLippincott, Philadelphia, 1998, pp 109–118
44. Portenoy RK, Itri LM: Cancer-related fatigue: guidelines forevaluation and management. The Oncologist 4: 1–10, 1999
45. Curt GA: Impact of fatigue on quality of life in oncologypatients. Semin Hematol 37: 14–17, 2000
46. Bastracchea J, Hortobagyi GN, Smith TL, Kau SC: Obesityas an adverse prognostic factor for patients receiving adjuvantchemotherapy for breast cancer. Ann Intl Med 119: 18–25,1993
47. Bisdee JT, James WPT, Shaw MA: Changes in energy ex-penditure during the menstrual cycle. Brit J Nutr 61: 187,1989
48. Kami M, Tanaka Y, Chiba S et al.: Thyroid function after bonemarrow transplant: possible association between immune-mediated thyrotoxicosis and hypothyroidism. Transplantation15: 71, 2001

Is subclinical hypothyroidism the culprit? 159
49. Smyth PP: The thyroid and breast cancer: a significant associ-ation? Ann Med 29: 189–191, 1997
50. Shering SG, Zbar AP, Moriarty M, McDermott EW,O’Higgins NJ, Smyth PP: Thyroid disorders and breast cancer.Eur J Cancer Prev 5: 504–506, 1996
51. Cutuli B, Quentin P, Rodier JF, Barakat P, Grob JC: Severe hy-pothyroidism after chemotherapy and locoregional irradiationfor breast cancer. Radiother Oncol 57: 103–105, 2000
52. Giani G, Flerbracci P, Bonacci R et al.: Relationship betweenbreast cancer and thyroid disease: relevance of autoimmunethyroid disorders in breast malignancy. J Clin EndocrinolMetab 81: 990–994, 1996
53. Rasmussen B, Feldt Rasmussen U, Hegadus L et al.: Thyroidfunction in patients with breast cancer. Eur J Cancer ClinOncol 23: 553–556, 1987
54. Adampoulus DA, Vassilarus D, Kapolla N et al.: Thyroid dis-ease in patients with benign and malignant mastopathy. Cancer57: 125–128, 1987
55. Fatourechi V: Subclinical thyroid disease. Mayo Clin Proc76(4): 413–416, 2001
56. Brown Grant K: The iodine concentrating mechanism of themammary gland. J Physiol 135: 644–654, 1957
57. Eskin BA: Iodine metabolism and breast cancer. Trans NYAcad Sci 11: 911–941, 1970
58. Ghent WR, Eskin BA et al.: Iodine replacement in fibrocysticbreast disease. Can J Surg 36: 459, 1993
59. Jacobsen PB, Azzarello L, Hann DM: Relation of catastroph-izing to fatigue severity in women with breast cancer. CancerRes Therapy Contr 8: 55–164, 1999
60. Jacobsen PB, Hann DM, Azzarello LM, Horton J, Balducci L,Lyman GH: Fatigue in women receiving adjuvant chemother-
apy for breast cancer: characteristics, course, and correlates.J Pain Symp Manage 18: 233–242, 1999
61. Jacobsen PB, Stein K: Is fatigue a long-term side effect ofbreast cancer treatment? Cancer Contr 6: 256–263, 1999
62. Kirsh K, Passik S, Holtsclaw E, Donaghy K, Theobald, D: Iget tired for no reason: a single item screening for fatigue.J Pain Sympt Manage 22: 931–937, 2001
63. Sadler IJ, Jacobsen PB: Progress in understanding fatigueassociated with breast cancer treatment. Cancer Invest 19:723–731, 2001
64. Sadler IJ, Jacobsen PB, Booth-Jones M, Belanger H, WeitznerMA, Fields KK: Preliminary evaluation of a clinical syndromeapproach to assessing cancer-related fatigue. J Pain SymptManage 23: 406–413, 2002
65. Stein KD, Jacobsen PB, Hann DM, Greenberg H, Lyman G:Impact of hot flashes on quality of life among postmenopausalwomen being treated for breast cancer. J Pain Sympt Manage19: 436–445, 2000
66. Tagliaferri M, Berselli ME, Calo G, et al.: Subclinical hypo-thyroidism in obese patients: relation to resisting metabolicexpenditure, serum leptin, body composition and lipid profile.Obes Res 9: 196–201, 2001
67. Solomon SJ, Kurzer MS, Calloway DH: Menstrual cycle andbasal metabolic rate in women. Am J Clin Nutr 36: 611, 1982
Address for offprints and correspondence: Nagi Kumar, Ph.D.,R.D., Department of Interdisciplinary Onc., H. Lee Moffett CancerCenter, University of South Florida, 12901 Magnolia Drive, Tampa,FL 33612-9497, USA; Tel.: +1-813-903-6885; Fax: +1-813-632-1334; E-mail: [email protected]
















![The Culprit [2]](https://img.pdfslide.us/doc/110x75/56816247550346895dd28534/the-culprit-2.jpg)