Embed Size (px)
Citation preview

Amenorrhea Amenorrhea and Hirsutismand Hirsutism
05.04.200905.04.2009
Dr. Pradeep GargDr. Pradeep GargAssistant ProfessorAssistant Professor
Department of Obstetrics and GynaecologyDepartment of Obstetrics and Gynaecology
AIIMS, New DelhiAIIMS, New Delhi

Amenorrhea: DefinitionAmenorrhea: Definition
PrimaryPrimary
No menses by 16 years with normal secondary sexual No menses by 16 years with normal secondary sexual characteristics, or.characteristics, or.
No menses by 14 years with absent secondary sexual No menses by 14 years with absent secondary sexual characteristicscharacteristics
SecondarySecondary
Cessation of menses for 3 cycles / 6 months in absence of Cessation of menses for 3 cycles / 6 months in absence of pregnancy/lactation.pregnancy/lactation.

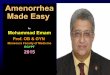
Amenorrhea: EtiologyAmenorrhea: Etiology
IVIV
IIIIII
IIII
II
MenstruationMenstruation
Hypothalamus
Pituitary
Ovaries
Outflow tract
FSH LH
E P

Amenorrhea : EtiologyAmenorrhea : EtiologyCompartment I (Uterine/Outflow tract)Compartment I (Uterine/Outflow tract) Mullerian abnormalities :Mullerian abnormalities :
-- Utero-vaginal agenesis (MRKH Syndrome)Utero-vaginal agenesis (MRKH Syndrome)
-- Imperforated hymenImperforated hymen
-- Transverse vaginal septumTransverse vaginal septum
Testicular feminization (AIS)Testicular feminization (AIS)
Asherman’s syndrome:Asherman’s syndrome:
-- Secondary to uterine/cervical surgerySecondary to uterine/cervical surgery
-- Secondary to infections (TB, PID)Secondary to infections (TB, PID)

Mayer-Rokitansky-Kuster-Hauser Syndrome Mayer-Rokitansky-Kuster-Hauser Syndrome (utero-vaginal agenesis)(utero-vaginal agenesis)
15% of primary amenorrhea 15% of primary amenorrhea Normal secondary development Normal secondary development
& external female genitalia& external female genitalia Normal female range Normal female range
testosterone leveltestosterone level Absent uterus and upper vagina Absent uterus and upper vagina
& normal ovaries& normal ovaries Karyotype 46-XXKaryotype 46-XX 15-30% renal, skeletal and 15-30% renal, skeletal and
middle ear anomaliesmiddle ear anomalies

Imperforate HymenImperforate Hymen

Androgen InsensitivityAndrogen Insensitivity Normal breasts but no sexual Normal breasts but no sexual
hairhair Normal looking female external Normal looking female external
genitaliagenitalia Absent uterus and upper Absent uterus and upper
vaginavagina Karyotype 46, XYKaryotype 46, XY Male range testosterone levelMale range testosterone level Treatment : gonadectomy after Treatment : gonadectomy after
puberty + HRTpuberty + HRT

Amenorrhea : EtiologyAmenorrhea : Etiology
Compartment II (Gonadal failure)Compartment II (Gonadal failure)
Turner syndrome 45xO/mosaic/partial deletions Turner syndrome 45xO/mosaic/partial deletions
Pure gonadal dysgenesis.Pure gonadal dysgenesis.
Mixed gonadal dysgenesisMixed gonadal dysgenesis
Premature ovarian failurePremature ovarian failure
Autoimmune/RT/CT/ galactosemia Autoimmune/RT/CT/ galactosemia
Resistant ovary syndromeResistant ovary syndrome

Turner syndromeTurner syndrome
Karyotype 45 XKaryotype 45 X Generally grow slowly so shorter Generally grow slowly so shorter Associated stigmata Associated stigmata
Lymphadema at birthLymphadema at birth Webbed neckWebbed neck Disorder of heart and kidney (most commonly horse shoe) and great vessels (most Disorder of heart and kidney (most commonly horse shoe) and great vessels (most
commonly coaraction of aorta)commonly coaraction of aorta) Diabetes mellitesDiabetes mellites Thyroid disorderThyroid disorder HypertensionHypertension Do not develop breast at pubertyDo not develop breast at puberty


Premature ovarian failurePremature ovarian failure
Ovarian failure is normal occurrence during menopauseOvarian failure is normal occurrence during menopause EtiologyEtiology
1.Genetic disorder – Mosaicism or XO or XY or deletion of portion of 1.Genetic disorder – Mosaicism or XO or XY or deletion of portion of chromosomechromosome
2.Iatrogenic causes2.Iatrogenic causes RadiationRadiation ChemotherapyChemotherapy Surgical interference with blood supplySurgical interference with blood supply InfectionInfection
3.Autoimmune disorder – as a part of polyglandular syndrome3.Autoimmune disorder – as a part of polyglandular syndrome

Amenorrhea:EtiologyAmenorrhea:Etiology
Compartment III (Pituitary)Compartment III (Pituitary)
Hormone secreting. Adenomas Hormone secreting. Adenomas
Non functional adenoms.Non functional adenoms.
TB/ sarcoid granulomas. Dermoid cystTB/ sarcoid granulomas. Dermoid cyst
Necrosis (Sheehan’s syndrome) Necrosis (Sheehan’s syndrome)

Amenorrhea:EtiologyAmenorrhea:EtiologyCompartment IV (Hypothalamic)Compartment IV (Hypothalamic) Constitutional delay (Physiological)Constitutional delay (Physiological) Malnutrition, anorexia nervosa, vigorous exercise, Malnutrition, anorexia nervosa, vigorous exercise,
stress, anxiety. stress, anxiety. Drugs: Phenothiazines, antihypertensive,Drugs: Phenothiazines, antihypertensive,
antidepressants, hormonal contraception. antidepressants, hormonal contraception. Genetic (Kallman’s)- Triad of anosmia, hypogonadism Genetic (Kallman’s)- Triad of anosmia, hypogonadism
and color blindnessand color blindness Organic disease/ Injury to mid/brain Organic disease/ Injury to mid/brain
Tumors (craniopharyngiomas, gliomas)Tumors (craniopharyngiomas, gliomas)
Infitrative lesions, trauma, irradiation. Infitrative lesions, trauma, irradiation.

Amenorrhea: EtiologyAmenorrhea: Etiology Other Endocrine dysfunctionOther Endocrine dysfunction - - --
Hyper/hypothyroidismHyper/hypothyroidism
-- CAH/Cushing’s syndromeCAH/Cushing’s syndrome
-- Virilising adrenal/ ovarian tumors.Virilising adrenal/ ovarian tumors.
-- Granulosa-theca tumor ovary, C L cystGranulosa-theca tumor ovary, C L cyst
-- Obesity, Polycystic ovarian diseaseObesity, Polycystic ovarian disease
General General --
-- Chronic renal, liver, lung diseaseChronic renal, liver, lung disease
-- Chronic infections , diabetes mellitus.Chronic infections , diabetes mellitus.

Amenorrhea: ClassificationAmenorrhea: ClassificationPhysiologicalPhysiological PathologicalPathological
- PrepubertyPrepuberty Primary Primary SecondarySecondary- PregnancyPregnancy- Lactation Lactation With (n) secWith (n) sec Without (n)Without (n)- Menopause Menopause sexual charac.sexual charac. sexual charac.sexual charac.
- Think ?- Think ? HypogonadismHypogonadismPregnancyPregnancy (gonadal failure)(gonadal failure)Mullerian anomalyMullerian anomaly - Gonadal dysgen- Gonadal dysgenAISAIS - Irradiation- Irradiation- Chemotherapy- Chemotherapy- Galectosemia- GalectosemiaOtherOther- Anorexia nervosa- Anorexia nervosa- Kallman syndrome- Kallman syndrome- Pituitary damage- Pituitary damage - Surgery, irradiation- Surgery, irradiation- Constitutional delay- Constitutional delay

Secondary AmenorrheaSecondary Amenorrhea
Pregnancy!Pregnancy! CNS disordersCNS disorders Pituitary glandPituitary gland ThyroidThyroid OvaryOvary UterusUterus Systemic disordersSystemic disorders
Renal failure, liver disorders, DMRenal failure, liver disorders, DM Medications: anti-psychotics, reserpineMedications: anti-psychotics, reserpine

Secondary AmenorrheaSecondary Amenorrhea
CNS disordersCNS disordersChronic hypothalamic anovulationChronic hypothalamic anovulation
StressStressIncreased exercise levelsIncreased exercise levelsAnorexia nervosaAnorexia nervosa
Head traumaHead traumaSpace-occupying lesionsSpace-occupying lesions

Secondary AmenorrheaSecondary Amenorrhea
Pituitary disordersPituitary disorders HyperprolactinemiaHyperprolactinemia
ProlactinomaProlactinoma MedicationsMedications PCOSPCOS Renal failureRenal failure
HypoprolactinemiaHypoprolactinemia Pituitary resectionPituitary resection Sheehan’s syndromeSheehan’s syndrome
Thyroid disordersThyroid disorders Hyper- or hypothyroidismHyper- or hypothyroidism

Secondary AmenorrheaSecondary Amenorrhea
Ovulation disordersOvulation disorders Polycystic ovarian syndromePolycystic ovarian syndrome Premature ovarian failurePremature ovarian failure
Uterine abnormalitiesUterine abnormalities Asherman’s syndromeAsherman’s syndrome Cervical stenosisCervical stenosis
Drug-induced amenorrheaDrug-induced amenorrhea Hormonal contraceptivesHormonal contraceptives GnRH analoguesGnRH analogues

Amenorrhea: Diagnostic Amenorrhea: Diagnostic Evaluation Evaluation
Rule out pregnancy Rule out pregnancy Pelvic USG: uterus, ovariesPelvic USG: uterus, ovaries KaryotypeKaryotype Screening urinary/skeletal abnScreening urinary/skeletal abnss
MRI/Laparoscopic visualization MRI/Laparoscopic visualization Stepwise evaluation & hormonal assessment Stepwise evaluation & hormonal assessment
TSH, Prolactin, FSH, LH, Estradiol, TSH, Prolactin, FSH, LH, Estradiol, TestosteroneTestosterone
If indicated

Amenorrhea : Diagnostic Amenorrhea : Diagnostic Evaluation Evaluation
Step 1Step 1
--TSH, Prolactin TSH, Prolactin
-- Progesterone Challenge testProgesterone Challenge test
Positive withdrawal bleed:Positive withdrawal bleed:
uterus: endogenous estrogen primed, reactive uterus: endogenous estrogen primed, reactive vaginal outflow vaginal outflow tract patenttract patent
minimal ovarian, pituatary, CNS Function present.minimal ovarian, pituatary, CNS Function present.
No further diagnostic evaluation neededNo further diagnostic evaluation needed
Negative: withdrawal: Go to Step2Negative: withdrawal: Go to Step2

Amenorrhea : Diagnostic Amenorrhea : Diagnostic Evaluation Evaluation
Step 2Step 2
Estrogen + Progesterone Challenge : if negative Estrogen + Progesterone Challenge : if negative withdrawalwithdrawal
Mullerian agensis/ defects Mullerian agensis/ defects
Asherman’s syndrome/TB endometritis, Asherman’s syndrome/TB endometritis, hypoestrogenism- if positive withdrawal then hypoestrogenism- if positive withdrawal then hypoestrogenismhypoestrogenism

Amenorrhea: Diagnostic Amenorrhea: Diagnostic EvaluationEvaluation
Step 3Step 3
Determination of FSH and LH levelsDetermination of FSH and LH levels
Normal 5-20 Normal 5-20 5-40 IU/ml5-40 IU/ml
Ovarian failure Ovarian failure Pituitary/CNS failurePituitary/CNS failure
FSH > 20FSH > 20 < 5 or N< 5 or N
LH >40LH >40 < 5 or N< 5 or N
(Hyper-gonadotropic) (Hypo-gonadotropic)(Hyper-gonadotropic) (Hypo-gonadotropic)

Amenorrhea: Diagnostic Amenorrhea: Diagnostic EvaluationEvaluation
Step 4Step 4
High FSHHigh FSH
-- Karytype if age< 30 yearsKarytype if age< 30 years
-- Work up for autoimmune diseaseWork up for autoimmune disease
-- CBC, ESR, free TCBC, ESR, free T44, TSH, antibodies, Ca, P, TSH, antibodies, Ca, P
-- Total protein, A:G, ANA, glucose,Total protein, A:G, ANA, glucose,
Serum progestrone, 17 OHPSerum progestrone, 17 OHP
(to rule out 17 (to rule out 17 hydroxylase deficiency) hydroxylase deficiency)

Amenorrhea: Treatment PrinciplesAmenorrhea: Treatment Principles Objectives of Treatment Objectives of Treatment
-- Initiate menstruation & reproductive Initiate menstruation & reproductive potential, potential, in whom it is possible in whom it is possible
-- Appropriate medical & surgical management Appropriate medical & surgical management for for adequate physical development and coital adequate physical development and coital relationsrelations
-- Detection and management of any of the Detection and management of any of the threatening condition.threatening condition.
-- Prevention of osteoporosisPrevention of osteoporosis

Thorough physical exam and r/o any systemic ds Thorough physical exam and r/o any systemic ds e.g. hypo or hyperthyroidism.e.g. hypo or hyperthyroidism.
Absence of sec sex character + failure of Absence of sec sex character + failure of development of pubic / axillary hair s/o turner’s development of pubic / axillary hair s/o turner’s syndrome or pituitary infantilismsyndrome or pituitary infantilism
Hirsutism + amenorrhoea --> viritizing tumour of Hirsutism + amenorrhoea --> viritizing tumour of ovary, PCODovary, PCOD
Adiposity and striae on body may suggest cushing’s Adiposity and striae on body may suggest cushing’s syndromesyndrome
Amenorrhea: Treatment Amenorrhea: Treatment PrinciplesPrinciples

Primary AmenorrheaPrimary Amenorrhea
TreatmentTreatmentCyclic estrogen/progestinCyclic estrogen/progestin
Remove gonadal streaks if XY or mosaicRemove gonadal streaks if XY or mosaicIncreased (52%) risk of gonadoblastomas, Increased (52%) risk of gonadoblastomas,
dysgerminomas, and yolk sac tumorsdysgerminomas, and yolk sac tumors
Pulsatile GnRH for ovulation induction in select Pulsatile GnRH for ovulation induction in select patientspatients
Surgical resection of intrauterine, cervical, and Surgical resection of intrauterine, cervical, and vaginal adhesions/septavaginal adhesions/septa

Amenorrhea: Treatment Amenorrhea: Treatment PrinciplesPrinciples
Treatment of underlying causeTreatment of underlying cause General General : : diet, exercisediet, exerciseHypothyroidismHypothyroidism : : ThyroxineThyroxineTB endometritisTB endometritis : : ATTATTHyperprolactemiaHyperprolactemia : : BromocryptineBromocryptinePCO with hirsutismPCO with hirsutism :: Cyclic progestins, Cyclic progestins,CAHCAH :: Corticosteroids Corticosteroids

Amenorrehea: Treatment Amenorrehea: Treatment PrinciplesPrinciples
Surgical managementSurgical management-- Correction of Obstruction collectionCorrection of Obstruction collection
-- Vaginoplasty in vaginal atresia, 5 Vaginoplasty in vaginal atresia, 5 reductase reductase deficiency & androgen end organ defectsdeficiency & androgen end organ defects
-- Removal of testicular tissue if Y cell line + Removal of testicular tissue if Y cell line + -- Neurosurgery for craniopharyngioma,Neurosurgery for craniopharyngioma,
pituitary tumor causing cushing’s disease;pituitary tumor causing cushing’s disease;prolactinomas,prolactinomas,

Amenorrhea:Treatment Amenorrhea:Treatment PrinciplesPrinciples
Asherman’s syndromeAsherman’s syndrome HSG/Hysteroscopy to confirm diagnosisHSG/Hysteroscopy to confirm diagnosisHysteroscopic lysis of adhesionsHysteroscopic lysis of adhesions
-- Foley’s 3 ml Foley’s 3 ml 3 months 3 months
-- Broad spectrum antibiotics Broad spectrum antibiotics 10 d10 d
-- High dose estrogens High dose estrogens 2 months 2 months
add MPA add MPA 3-months 3-months

HIRSUTISMHIRSUTISM
HIRSUTISMHIRSUTISM : APPEARANCE OF EXCESSIVE : APPEARANCE OF EXCESSIVE COARSE (TERMINAL)HAIR IN A PATTERN COARSE (TERMINAL)HAIR IN A PATTERN NOT NORMAL IN THE FEMALENOT NORMAL IN THE FEMALE
Definition highlights the abnormal distribution of Definition highlights the abnormal distribution of excess hair growth ,such as facial ,chest,or excess hair growth ,such as facial ,chest,or upper abdominal hairupper abdominal hair

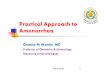
BASIC FACTS ABOUT HAIRBASIC FACTS ABOUT HAIR
PITUITARY
ADRENAL OVARY
PITUITARY
ADRENALOVARY
DHEAS
DHEA
AND,STEN,ONE
PERIPHERALCONVERSION
TESTOSTERONE
HAIR FOLLICLE
DIHYDROTESTERONE
DHEAS
ACTH

DEFINITIONDEFINITION
HYPERTRICHOSISHYPERTRICHOSIS : GROWTH OF HAIR IN : GROWTH OF HAIR IN EXCESS OF THE NORMAL WHILE LIMITED EXCESS OF THE NORMAL WHILE LIMITED TO A NORMAL PATTERN OF DISTRIBUTIONTO A NORMAL PATTERN OF DISTRIBUTION
It is frequently associated with the use of It is frequently associated with the use of medication such as antiepileptics medication such as antiepileptics

DEFINITIONDEFINITION
VIRILIZATIONVIRILIZATION : REFERS TO CONCURRENT : REFERS TO CONCURRENT PRESENTATION OF PRESENTATION OF HIRSUTISMHIRSUTISM WITH A WITH A BROAD RANGE OF SIGNS SUGGESTIVE OF BROAD RANGE OF SIGNS SUGGESTIVE OF ANDROGEN EXCESSANDROGEN EXCESS,SUCH AS ,SUCH AS
ACNE,ACNE,DEPPENING OF THE VOICE ,DEPPENING OF THE VOICE ,A DECREASE IN BREAT SIZEA DECREASE IN BREAT SIZECLITORAL HYPERTROPHYCLITORAL HYPERTROPHY

DEFINITIONDEFINITION
INCREASED MUSCLE MASS INCREASED MUSCLE MASS
AMENORREA / OLIGOMENORRHEAAMENORREA / OLIGOMENORRHEA
Virilization is seen less frequently than hirsutism Virilization is seen less frequently than hirsutism and may reflect a severe underlying pathologic and may reflect a severe underlying pathologic condition ,such as malignancycondition ,such as malignancy
Hirsutism and virilization are closely linked and Hirsutism and virilization are closely linked and hirsutism may actually be the first manifestation of a hirsutism may actually be the first manifestation of a condition that ultimately will lead to virilization if left condition that ultimately will lead to virilization if left untreateduntreated

Etiology Etiology
Sensitivity of androgens Sensitivity of androgens Circulating androgensCirculating androgens
Total circulating testosterone Total circulating testosterone
SHBGSHBG AlbuminAlbumin FreeFree
Men Men 78%78% 19%19% 3%3%
Normal womenNormal women 80%80% 19%19% 1%1%
Hirsute womenHirsute women 79%79% 19%19% 2%2%

CAUSES OF HIRSUTISMCAUSES OF HIRSUTISM
Excess androgen production Excess androgen production Relative circulating androgen excess and low Relative circulating androgen excess and low
binding globulinsbinding globulinsExcess end organ responseExcess end organ responsePatient perceptionPatient perception

Causes Causes Idiopathic Idiopathic Drug inducedDrug induced Ovarian:Ovarian:
-- PCOS PCOS
-- HyperthecosisHyperthecosis
-- Vinilizing tumourVinilizing tumour Adrenal:Adrenal:
-- CAHCAH
-- Adrenal tumours Adrenal tumours
-- Cushing’s syndromeCushing’s syndrome Virilisation in pregnancy: LuteomaVirilisation in pregnancy: Luteoma OthersOthers:: hypothyroidism, hyperprolactinemia, anorexia nervosa, Insulin resistance hypothyroidism, hyperprolactinemia, anorexia nervosa, Insulin resistance
sydrome.sydrome.

PRESENTATION OF HIRSUTISMPRESENTATION OF HIRSUTISM
Hirsutism alone is the greatest Hirsutism alone is the greatest challenge,patients usually go to dermatologistchallenge,patients usually go to dermatologist
Hirsutism wIth acne is frequently in teenage girlsHirsutism wIth acne is frequently in teenage girlsHirsutism with ovulatory disorders comes mostly Hirsutism with ovulatory disorders comes mostly
to gynecologistto gynecologistHirsutism with virilization requires immediate Hirsutism with virilization requires immediate
work-upwork-up

Evaluation of a patientEvaluation of a patient HistoryHistory
Time of onsetTime of onset :: Puberty, PregnancyPuberty, Pregnancy
DurationDuration :: Rapid/slow growthRapid/slow growth
SymptomsSymptoms :: Headache, Visual Headache, Visual disturbances, pain abdomen, lump disturbances, pain abdomen, lump abdomen, galactorrhoea.abdomen, galactorrhoea.
Other endocrinopatiesOther endocrinopaties :: Hypothyroidism, HyperprolactinemiaHypothyroidism, Hyperprolactinemia
Family historyFamily history :: CAH, IdiopathicCAH, Idiopathic
DrugsDrugs :: Androgens, danazol, 19-nor progesterone, Androgens, danazol, 19-nor progesterone, Minoxidil.Minoxidil.

ExaminationExamination
Thyroid, galactorrhoeaThyroid, galactorrhoea
Acne/seborrhaea/alopecia, Hirsutism scoring Acne/seborrhaea/alopecia, Hirsutism scoring (FG Score)(FG Score)
Abdomen/ pelvic examAbdomen/ pelvic exam
Other signs of virilization- clitoromegalyOther signs of virilization- clitoromegaly

Hirsutism scoringHirsutism scoring ((Ferriman Gallwey Ferriman Gallwey score)score)
Body area Body area ScoreScore Upper lipUpper lip All graded from 0-4All graded from 0-4 ChinChin 0=no hisutism0=no hisutism ChestChest 4= severe4= severe Upper abdomenUpper abdomen Score>8= hirsutismScore>8= hirsutism Lower abdomenLower abdomen Upper armUpper arm ThighsThighs Upper backUpper back Lower backLower back

Lab evaluation Lab evaluation
Normal valuesNormal values HirsutismHirsutism
TestosteroneTestosterone 20-80 mg/dl20-80 mg/dl (N) to (N) to > 200-tumor> 200-tumor
Free testosteroneFree testosterone 0.6-6.8 pg/ml0.6-6.8 pg/ml SHBGSHBG 18-114 n mol/L18-114 n mol/L
DHEASDHEAS 100-350µg/dl100-350µg/dl (N) to (N) to > 700-Adrenal> 700-Adrenal
170HP170HP 30-200mg/dl30-200mg/dl -CAH-CAH

Work- upWork- upS-Testosterone S-Testosterone
<2000ng/dL<2000ng/dL >2000ng/dL>2000ng/dL
TumourTumour LH/FSHLH/FSH TSH TSH DHEASDHEAS ProlactinProlactin USG USG
OvaryOvary AdrenalAdrenal
-- Imaging / USG / CT / MRIImaging / USG / CT / MRI-- Selective venous angiographySelective venous angiography-- Laparoscopy / laparotomyLaparoscopy / laparotomy

Work- upWork- up17- OHP17- OHP
<200ng/dl<200ng/dl >200ng/dl>200ng/dl
CAH excludedCAH excluded
ACTH stimulation testACTH stimulation test
NormalNormal AbnormalAbnormal
21-hydroxylase21-hydroxylase CAH CAHdef.excludeddef.excluded

Work- upWork- up
Idiopathic hirsutismIdiopathic hirsutism
– (N) menstrual cycles(N) menstrual cycles
– (N) lab evaluation(N) lab evaluation
Etiology ? Etiology ? Sensitivity to androgensSensitivity to androgens

Management of hirsutismManagement of hirsutism Treatment of etiological causeTreatment of etiological cause -- AnovulationAnovulation
-- CAHCAH-- Adrenal tumorAdrenal tumor-- Ovarian tumorOvarian tumor
Idiopathic hirsutismIdiopathic hirsutism Pharmacologic therapyPharmacologic therapy Non- pharmacologic adjunctsNon- pharmacologic adjuncts
-- Weight reduction ( in obese women)Weight reduction ( in obese women)-- Cosmetic therapyCosmetic therapy-- Depilatory creamDepilatory cream- - BleachBleach- - Electrolysis/laserElectrolysis/laser- - ShavingShaving

Management of hirsutismManagement of hirsutism Ovarian causeOvarian cause -- OCPOCP
-- Progesterone therapyProgesterone therapy -- Insulin sensitisers (Metformin)Insulin sensitisers (Metformin)
-- GnRH a with add back therapyGnRH a with add back therapy Adrenal cause- steroids to suppress adrenalAdrenal cause- steroids to suppress adrenal
Anovulation with desire of conception-Anovulation with desire of conception- Induction of ovulationInduction of ovulation
-- Pharmacologic (clomiphene, letrrozole, gonadotrophins)Pharmacologic (clomiphene, letrrozole, gonadotrophins)-- Surgical- ovarian drillingSurgical- ovarian drilling

OCPsOCPs E2 component - E2 component - SHBGSHBG free T free T
LHLH P Component- Cycle controlP Component- Cycle control
Prevents endometrial hyperplasiaPrevents endometrial hyperplasia E2+P- contraceptionE2+P- contraception Advantage Advantage
-- ContraceptionContraception
-- Cycle regulationCycle regulation
-- Reduce menstrual blood lossReduce menstrual blood loss

Anti-androgensAnti-androgens SpironolactoneSpironolactone Cyproterone acetate (CPA)Cyproterone acetate (CPA) FinasterideFinasteride FlutamideFlutamide Other drugs with antiandrogenic actionOther drugs with antiandrogenic action
-- Cimetidine- weak antiandrogen Cimetidine- weak antiandrogen
-- KetoconazoleKetoconazole
Contraindicated in women desirous of conceptionContraindicated in women desirous of conception

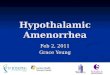
Peripheral action of Peripheral action of antiandrogensantiandrogens
55 reductase reductase
Testosterone Testosterone DHT DHT Androgen receptor Androgen receptor
Finasteride Finasteride SironolactoneSironolactone
Ketoconozol Ketoconozol CPACPA
FlutamideFlutamide

Surgical managementSurgical management In PCOSIn PCOS
-- Wedge resection?Wedge resection?-- Ovarian drillingOvarian drilling
In tumour In tumour -- Adrenal tumour excisionAdrenal tumour excision-- Ovarian tumour excisionOvarian tumour excision
Androgen secreting ovarian tumorsAndrogen secreting ovarian tumors ThecomasThecomas Sertoli-leydig cell tumors (Androblastoma)Sertoli-leydig cell tumors (Androblastoma) Sclerosing stromal tumorSclerosing stromal tumor LuteomaLuteoma GynandroblastomasGynandroblastomas Stromal hyperplasia/hyperthecosisStromal hyperplasia/hyperthecosis Management - Surgical (conservative) Management - Surgical (conservative)