Embed Size (px)
Citation preview

Clinical Endocrinology (1995) 43, 225-229
Familial hyperparathyroidism associated with jaw fibroma: case report and literature review
Hlroyukl lnoue', Hltoshl Mlkl', Kazushl Oshlmo', Katuhlro Tanaka', Yasumasa Monden', Aklhlro Yamamotot, Susumu Kagawat, Nobuya Sanot, ElJl Hayash&, Masaru Nagayamas and Yoshlo Hayashll *Second Department of Surgery, Urology and SSecond Department of Pathology, School of Medicine, University of Tokushirna; §First Department of Oral and Maxillofacial Surgery and l O r a l Pathology, School of Dentistry, University of Tokushima
(Received 7 July 1994; returned for revision 14 September 1994; finally revised 18 October 1994; accepted 12 December 1994)
Summary
A 53-year-old female sulierlng from renal stones and hypercalcaemla was diagnosed as having prlmary hyper- parathyroldlsm caused by hyperplasia of the Parathyroid glands. She underwent total parathyroldectomy and Implantation of Parathyroid tissue. Alter one year, she underwent surgery for a jaw tumour. The pathological findings Indicated It to be a cementlfylng fibroma. Jackson et a/. (1990) reported the familial assoclatlon of hyper- parathyroldlsm with jaw tumours, and they suggested that this condition represents a new cllnlcal syndrome. We believe that our case belongs to this syndrome.
Jackson (1958) published the first report of a family with familial hyperparathyroidism associated with jaw tumours. Since then, several similar families have been reported. Jackson et al. (1990) have suggested that this condition represents a new syndrome. We have treated a patient with the characteristics of this syndrome. We describe our case and review the literature.
Case report
In August 1987, a 53-year-old female presented with right lower abdominal pain. Bilateral renal stones and hyper- calcaemia were detected. She was referred to our hospital for further examination and treatment in November 1987. At
Correspondence: Hiroyuki Inoue, Second Department of Surgery, School of Medicine, University of Tokushima, Kuramoto-cho, Tokushima 770, Japan. Fax: 0886 33 7144.
0 1995 Blackwell Science Ltd
that time, she was asymptomatic. She had been operated for cholelithiasis, uterine myoma and endometriosis in 1984.
Physical examination revealed a 2-cm tumour in the lower portion of the right lobe of the thyroid gland, but no other abnormalities were detected.
Laboratory findings on admission are shown in Table 1. Serum calcium was 3.33 mmol/l (normal 2.13-2.63), C-terminal portion of parathyroid hormone (C-PTH) 2.4 pg/l (normal 0.1 -0-5), mid-portion of parathyroid hormone (MID-F'TH) 3100ng/l (normal 130-490), and
Table 1 Laboratory data on initial assessment
Indicator Value
WBC RBC Hb Haematocrit Platelets Total protein Albumin Urea Creatinine GOT GPT Alkaline phosphatase Calcium
Phosphate
C-PTH
MID-PTH
intact-PTH
Thyroid hormones Calcitonin Gastrin VIP ACTH PRL GH Urinary adrenahe Urinary noradrenaline TRP
6 x 109/1
I32 g/1 0.37
3.9 x 10'2/1
265 x 109/1 66 g/l 42 g/l S-Ommol/l 71 pmol/l 11 IU/l 12 IU/l 117IU/I 3.33 mmol/l (2.13-2.63) 0%7mmol/l (0.65- 1.30) 2.4 (0.1-0.5) 3 I00 ng/l
95 ng/l
normal 30 ng/l 72.7 ng/l c 25 ng/l < 1 ng/l 200 mU/1 6.2 mU/1 57 nmol/d 250 nmol/d
(1 30-490)
(10-50)
66% (85-98)
~~
TRP, tubular reabsorption of phosphate.
225

226 H. lnoue eta/ .
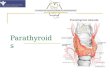
tumours. A 201T1-99mT~ subtraction scintigram disclosed four areas of uptake (Fig. 1). Other hormonal and radiographic investigations of the pituitary gland, pancreas and adrenal glands revealed no abnormalities. A diagnosis of primary hyperparathyroidism resulting from hyperplasia was made.
In December 1987, our patient underwent total para- thyroidectomy and implantation of a small portion of parathyroid tissue in the forearm. All four parathyroid glands were hyperplastic (Fig. 2). During the operation, a 0.5-cm papillary thyroid carcinoma was detected in the left lobe of the thyroid gland, and thyroidal lobectomy and lymph node dissection of the central cervical compartment were performed (Fig. 3). Histological examination showed several lymph node metastases. Since this operation, the patient has been hypocalcaemic and has required vitamin D3.
In December 1988, she sought medical advice about a hard, painless swelling, measuring 4cm, in the body of the left mandible. However, she had first noticed the swelling several years previously. It showed abnormal uptake of isotope in a bone scintigram (Fig. 4). Radiographic examination revealed radioopaque areas surrounded by a radiolucent lesion in the left mandible. In March 1989, the
intact parathyroid hormone (i-PTH) 95 ng/l (normal 10- exostotic mass was excised. Histological examination 50). A11 of these values were considerably elevated. showed numerous islands of cementum in cellular
Ultrasonography of the neck revealed two hypoechoic fibrous tissue (Fig. 5) . It was diagnosed as a cementifying tumours, and an enhanced CT scan of the neck showed three fibroma.
Fig. 1 201TI-wmT~ subtraction scintigram showing four areas of isotope uptake. This suggests the presence of hyperplastic parathyroid glands.
Fig. 2 Histological appearance of the parathyroid glands revealing proliferation of chief cells and eosinophilic cells. H & E staining, x 200.
0 1995 Blackwell Science Ltd, Clinical Endocrinology, 43,225-229

Hyperparathyroidism and jaw tumours 227
Flg. 3 Operation findings: Q, four hyperplastic parathyroid glands; a, a papillary thyroid carcinoma and m, several metastatic lymph nodes, were detected.
we measured Serum levels in other family members (Fig. 6) . The patient’s 19-year-old nephew had a
Fig. 4 Bone scintigram showing an area of abnormal uptake in the left mandible.
serum calcium level of 2.95mmol/l and i-PTH level of 79 ng/l. In August 1994, neck exploration was carried out. A Dlscusslon
parathyroid adenoma, measuring 13 mm, was removed Jackson (1958) reported four cases from a single family from the right inferior gland. No other family member has who had hyperparathyroidism associated with jaw yet shown evidence of endocrine or jaw tumours. tumours. Subsequently, several reports of familial
Flg. 5 Histological features of the jaw tumour showing islands of cementum-substance in cellular fibrous tissue. H & E staining, x 200.
0 1995 Blackwell Science Ltd, Clinical Endocrinology, 43,225-229

228 H. lnoue et a / .
56 yrs, CVD
55 yrs. DM 57 yrs, b P HT 59 yrs Ca : 2.53 Ca : 2.33 Ca : 3.33
24 yrs 35 yrs Ca : 2.15
19yrs 22yrs 26yrs Ca : 2.95 Ca : 2.3 Ca : 2.63 Ca : 2.25
FIg. 6 Family pedigree showing serum calcuim levels. CVD, Cerebrovascular disease; DM, diabetes mellitus; HT, hypertension; Ca, serum calcium level (normal 2.1 3-2.63 mmol/l). The proband is indicated with an arrow.
hyperparathyroidism with jaw lesions have been reported (Firat & Stutzman, 1968; Kennett & Pollick, 1971; Dinnen et a[., 1977; Rosen & Palmer, 1981; Warnakulasuriya et al., 1985; Mallette et al., 1987) (Table 2). Jackson et al. (1990)
Table 2 Reports of familial hyperparathyroidism associated with jaw tumours
suggested that the association of familial hyperparathyroid- ism and ossifying fibroma of the jaw was a new clinical syndrome. We call this condition ‘Jackson’s syndrome’ in this paper. Jackson’s syndrome is characterized by the following: (1) the hyperparathyroidism in Jackson’s syn- drome is primary. This hyperparathyroidism is often caused by a disorder of several parathyroid glands. Jackson et al. (1990) distinguished the hyperparathyroidism in Jackson’s syndrome from that found in multiple endocrine neoplasia (MEN) on the basis of DNA linkage analysis. Thus, Jackson’s syndrome is not associated with pituitary tumours, pancreatic islet cell tumours or phaeochromocy- toma; (2) the jaw tumours in Jackson’s syndrome are cementifying and ossifying fibromas. These jaw tumours do not include bone lesions resulting from hyperparathyroid- ism, e.g. the so-called brown tumour of bone. In an analysis by Hamner et al. (1968), cementifying and ossifying fibromas of the jaw were classified as fibro-osseous tumours of periodontal membrane origin.
Odontogenic tumours are uncommon in the mandible and maxilla. Regezi et al. (1978) reviewed 706 odontogenic tumours, which represented 1.3% of 54534 biopsy specimens submitted to their department of oral pathology. The incidence of cementifying fibroma was 2% of these odontogenic tumours. Therefore, it is
Affected family members Reported Age and sex Parathyroids Jaw tumours
Reference year of proband of proband of proband Hyperpara. +jaw. t. Hyperpara. only Jaw t. only
Jackson Jackson et al.
Firat and Stutzman
Kennett and Pollick
Dinnen et a f .
Rosen and Palmer
Warnakulasuriya et a[.
Mallette et al.
Inoue et al.
1958 1990
1968
1971
1977
1981
1985
1987
1995
29 M
60 F
14 F
33 F
18 M
25 F
31 M
36 M
53 F
1 adenoma
2 hyperplasia Fibrous and 1 adenoma dysplasia
1 adenoma Osteitis fibrosa
1 carcinoma and 1 hyperplasia
1 carcinoma Ossifying fibroma
Carcinoma Non-ossi fying fibroma
4 adenomas Cementifying fibroma
2 adenomas Ossifying fibroma
4 hyperplasia Cementifying fibroma
cystica
1 daughter, 3 uncles 1 aunt and 1 niece
1 daughter
1 brother
1 uncle
Mother
I brother
1 brother
2 sons
1 brother, 1 aunt, 2 cousins and
1 nephew 2 brothers
Father
1 brother 1 uncle
1 nephew
1 son
1 nephew
Hyperpara, hyperparathyroidism. Jaw t.; Jaw tumours.
0 1995 Blackwell Science Ltd, Clinical Endocrinology, 43,225-229

Hyperparathyroidism and jaw tumours 229
unlikely that hyperparathyroidism and cementifying fibroma of the jaw would occur together by chance. Primary hyperparathyroidism is usually caused by a single adenoma, but in our case, all four parathyroid glands showed hyperplasia. The parathyroid glands of the reported cases of Jackson’s syndrome often showed multiple adenomas or hyperplasia. Our patient’s 19-year-old nephew was recently diagnosed as having primary hyper- parathyroidism resulting from a parathyroid adenoma. The serum calcium level in our patient’s 26-year-old niece was at the upper limit of normal. Our case is an example of Jackson’s syndrome, and further examinations of the family are now being performed.
Eight families with familial hyperparathyroidism asso- ciated with jaw tumours have been reported in the English literature (Table 2). Dinnen et al. (1977) described two families with familial hyperparathyroidism associated with jaw tumours. In one of these two families, the pathological findings of jaw tumours were not reported; they might, therefore, have been merely brown tumours resulting from hyperparathyroidism. In the eight families, 20 individuals manifested hyperparathyroidism and jaw tumours, 10 showed only hyperparathyroidism, and four had only jaw tumours. The association of hyperparathyroidism with jaw tumours is not necessarily contemporaneous. In four of the 20 patients the jaw tumours were preceded by the hyperparathyroidism and in nine jaw tumours manifested before the hyper- parathyroidism. We therefore suggest that the course of familial hyperparathyroidism be observed over a long time.
References
Dinnen, J.S., Greenwood, R.H., Jones, J.H., Walker, D.A. & Williams, E.D. (1977) Parathyroid carcinoma in familial hyperparathyroidism. Journal of Clinical Pathology, 30,966-975.
Firat, D. & Stutzman, L. (1968) Fibrous Dysplasia of the Bone: Review of twenty-four cases. American Journal of Medicine, 44,
Hamner, J.E., Scofieid, H.H. & Cornyn, J. (1968) Benign fibroosseous jaw lesions of periodontal membrane origin: an analysis of 249 cases. Cancer, 22,861-878.
Jackson, C.E. (1958) Hereditary Hyperparathyroidism associated with recurrent pancreatitis. Annals of Internal Medicine, 49,829- 836.
Jackson, C.E., Norum, R.A., Boyd, S.B., Talpos, G.B., Wilson, S.D., Taggart, R.T. & Mallette, L.E. (1990) Hereditary hyperparathyroidism and multiple ossifying jaw fibromas: A clinically and genetically distinct syndrome. Surgery, 108,
Kennett, S. & Pollick, H. (1971) Jaw lesions in familial hyperparathyroidism. Oral Surgery, 31,502-510.
Mallette, L.E., Malini, S., Rappaport, M.P. &Kirkland, J.L. (1987) Familial cystic parathyroid adenomatosis. Annals of Internal Medicine, 107, 54-60.
Regezi, J.A., Kerr, D.A. & Courtney, R.M. (1978) Odontogenic tumors: analysis of 706 cases. Journal of Oral Surgery, 36,
Rosen, I.B. &Palmer, J.A. (1981) Fibroosseous tumors of the facial skeleton in association with primary hyperparathyroidism: An endocrine syndrome or coincidence? American Journal of Surgery, 142,494-498.
Warnakulasuriya, S. , Markwell, B.D. & Williams, D.M. (1985) Familial hyperparathyroidism associated with cementifying fibromas of the jaws in two siblings. Oral Surgery, 59,269-274.
421-429.
1006- 10 13.
771-778.
0 1995 Blackwell Science Ltd, Clinical Endocrinology, 43, 225-229