Embed Size (px)
Citation preview

CONCISE COMMUNICATIONS 1907
10.
11.
12.
13.
human cytokine and cytokine rerponse pathway genes by KSHV. Science 274:1739-1744, 1996 Simpson GR, Schulz TF, Whitby D, Cook PM, Boshoff C, Rainbow I,, Howard MR, Gao SJ, Bohenzky KA, Simmonds P, Lee C, de-Ruiter A, Hatzakis A, Teder RS, Weller IV, Weiss RA, Moore PS: Prevalence of Kaposi's sarcoma-associated herpesvirus infection measured by antibodies to recombinant capsid protein and latent immunofluorescence antigen. Lancet 348:1133-1138, 1996 Gao SJ, Kingsley L, Li M, Zheng W, Parravicini C, Ziegler J, Newton R, Rinaldo CR, Saah A, Phair J, Detels R, Chang Y, Moore PS: Seroprevalence of KSHV antibodies among North Americans, Italians, and Ugandans with and without Kaposi's sarcoma. Nat Med 2:925-928, 1996 Kedes DH; Operskalski E; Busch M; Kohn R, Flood J , Ganem D: The seroprevalence of human herpes virus 8 (HHV 8): distribution of infection in Kaposi's sarcoma risk groups and evidence for sexual transmission. Nat Med 2:918-924, 1906 Lennette ET, Blackbourn DJ, Levy JA: Antibodies to human herpesvirus type 8 in the general population and in Kaposi's sarcoma patients. Lancet 348:858-861, 1996
Familial antiphospholipid syndrome and HLA-DRB gene associations
Patients with antiphospholipid syndrome (AE'S), either primary APS or in the setting of systemic lupus erythematosus (SLE), may have a genetic predisposition for developing these diseases. Several facts support this genetic role: 1) concor- dance of disease in twins; 2) presence of immunologic labora- tory abnormalities in relatives of patients; 3) increased fre- quency in certain ethnic groups; and 4) increased frequency of certain HLA molecules in these patients (1-10). The most convincing evidence for a genetic predisposition is the cluster- ing of disease in families. This report describes a family with antiphospholipid antibodies (aPL), in whom HLA-DRB gene associations are observed.
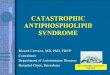
The family pedigree i s shown in Figure 1. The proband (I11 d), a 40-year-old man of mixed Native American-white origin, was referred for evaluation of an elevated activated partial thromboplastin time. He was well and denied having symptoms of connective tissue disease or coagulation prob- lems. The proband's father (I1 b) died at age 49 after a long history of polyarticular arthritis, photosensitivity, and multiple cerebrovascular accidents, consistent with SLE and the pres- ence of aPL. One of the proband's brothers (111 b) developed sagittal vein thrombosis in his forties. His younger brother (I11 c) died at age 33 after a 10-year history of manifestations related to lupus. Review of his medical records showed that he had arthritis, Raynaud's phenomenon, glomerulonephritis (World Health Organization class IV), interstitial pneumoni- tis, and congestive heart failure. The proband's mother (11 a), as well as 1 brother (111 a) and 2 nieces (IV a and b), are alive and well. The proband's grandfather (I b) died at age 85 with probable Alzheimer's disease, and the grandmother (I a) is still alive at age 94. Her past history is negative for signs or symptoms of a connective tissue disease or coagulation disorder.
Coagulation tests and anticardiolipin assays were done using commercially available kits. HLA molecular typing was performed using the Amplicor HLA-DRB test, graciously provided by Roche Diagnostic Systems.
I
I I
I l l
B1'1102,03 B1'14,07 B1'14,07
Lupus enficoagulent positive : Illb, llld Anticardiolipin entibodypositive : la, Illb,
Thmrnboticevents : Ilb. Illb. Ilk b Illc, l l ld 8
IV 0 0 Bl'l107,03 B1'1107.03
Figure 1. Family pedigree showing distribution of the HLA-DRB alleles. Open circles indicate female family members. Open boxes indicate male family members. Marked boxes indicate members who have died.
Anticardiolipin antibodies andlor lupus anticoagulant were present in 4 of 8 family members: I a, 111 b, IT1 c, and 111 d (Figure 1). Of these 4, I11 c is deceased and could not be typed for HLA-DRB1 alleles. The 3 others were positive for HLA-DRB1*14. No serologic data were available for TI b, although his haplotype, deduced through pedigree analysis, revealed that he too carried the DRBl"14 allele. Three members of the family (I1 b, 111 b, and 111 c) had thromboem- bolic manifestations consistent with the presence of aPL. None of the family members who were aPL negative showed any evidence of thrombosis or had the HLA-DRB1*14 allele. Three members of this family also carried the HLA-DR"07 allele (I1 a, not affected; 111 b and 111 d, both affected).
This is the first report of an association of aPL with the HLA-DRB1*14 allele. Two family members with aPL were also HLA-DR*07 positive, consistent with previously pub- lished data. In fact, several studies have examined the genetic
ociations of aPL (1-4,lO). However, given the paucity of the occurrence of familial APS, few studies have analyzed HLA haplotypes in this setting. One study by Dagenais et a1 (4), examining 14 members of a family with autoimmune diseases and aPL, found an increased incidence of HLA-DR4. Most other published reports that have documented the association of HLA genes with aPL expression involved unrelated patients. These studies suggest an increased association of aPL with HLA-DR4 (4,5,7-9), HLA-DR7 (6,8), DRw53 (7-9), and C4A or C4B null alleles (11). The ethnic background of the population being studied appears to be important. For exam- ple, Savi et a1 (6) found that HLA-DR7 was increased in a group of Italian patients, while HLA-DR4 was predominant in a group of English patients (3, and C4 null alleles were more commonly encountered in a group of black patients (11).
These findings raise several hypotheses regarding the possible association of HLA genes and immunologic disorders. HLA genes may be closely linked to genes involved in auto- immune diseases, and thus could be passed on, through linkage disequilibrium, with these disease genes. Alternatively, be- cause of their different abilities to present peptides, particular HLA molecules may have a direct role in the development of

1908 CONCISE COMMUNICATIONS
abnormal immune responses, as has been demonstrated in rheumatoid arthritis (12).
In summary, this is the first report of a possible linkage between the presence of the HLA-DRBI *14 allele and aPL. Further studies are warranted to evaluate the role of HLA molecules in the development of A P S .
Nancy Hudson, MD, FRCPC Lambert Busque, MD, FRCPC Joyce Rauch, PhD Jeannine Kassis, MD, FRCPC Paul R. Fortin, MD, FRCPC, MPH The Montreal General Hospital Montreal, Quebec, Canada
1.
2.
3.
4.
5.
Reveille JD, Anderson KL, Schrohenloher RE, Acton RT, Barger BO: Restriction fragment length polymorphism analysis of HLA- DR, DQ, DP and C4 alleles in Caucasians with systemic lupus erythematosus. J Rheumatol 18:14-18, 1991 Exner T, Barber S, Kronenberg H, Rickard KA: Familial associ- ation of the lupus anticoagulant. Br J Haematol 4.5:89-96, 1980 Matthey F, Walshe K, Mackie IJ, Machin SJ: Familial occurrence of the antiphospholipid syndrome. J Clin Pathol42:495-497, 1989 Dagenais P, Urowitz MB, Gladman DD, Norman CS: A family study of the antiphospholipid syndrome associated with other autoimmune diseases. J Rheumatol 19:1393-1396, 1992 McHugh NJ, Maddison PJ: HLA-DR antigens and anticardiolipin
antibodies in patients with systemic lupus erythematosus (letter). Arthritis Rheum 32:1623-1624, 1989
6. Savi M, Ferraccioli GF, Neri TM, Zanelli P, Dall’Aglio PP, Tincani A, Balestrieri G, Carella G, Cattaneo R: HLA-DR antigens and anticardiolipin antibodies in northern Italian sys- temic lupus erythematosus patients. Arthritis Rheum 31:1568- 1.570, 1988
7. May KP, West SG, Moulds J, Kotzin B L Different manifestations of the antiphospholipid antibody syndrome in a family with systemic lupus erythematosus. Arthritis Rhcum 36528-533, 1993
8. Goldstein R, Moulds JM, Smith CD, Sengar DPS: MHC studies of the primary antiphospholipid antibody syndrome and antiphos- pholipid antibodies in systemic lupus erythematosus. J Rheumatol
9. Asherson RA, Doherty DG, Vcrgani D, Khamashta MA, Hughes GRV: Major histocompatibility complex associations with primary antiphospholipid syndrome. Arthritis Rheum 35:124-125, 1992
10. Sebastiani G, Galeazzi M, Morozzi G, Marcolongo R: The immu- nogenetics of the antiphospholipid syndrome, anticardiolipin antibodies and lupus anticoagulant. Semin Arthritis Rhcum 25:
11. Wilson WA, Scopelitis E, Michalski JP, Pierangeli SS, Silveira LH, Elston RC, Harris EN: Familial anticardiolipin antibodies and C4 deficiency genotypes that coexist with MHC DQBl risk factors. J Rheumatol 22:227-235, 1995
12. Auger I, Escola J, Gorvel J, Roudier J : HLA-DR4 and HLA- DRlO motifs that carry susceptibility to rheumatoid arthritis bind 70-kD hcat shock proteins. Nal Mcd 2:306-310, 1996
23:1173-1179, 1996
414-420, 1996