Embed Size (px)
Citation preview

Arterial Thrombosis in Patients with AntiphospholipidSyndrome: A Review and Meta-AnalysisJesus Aibar Q1Q1
Q1, MD, PhD1,2 Sam Schulman, MD, PhD2,3
1Department of Internal Medicine, Hospital Clínic, IDIBAPS,University of Barcelona, Barcelona, Spain
2Department of Medicine, Thrombosis and Atherosclerosis ResearchInstitute, McMaster University, Hamilton, Ontario, Canada
3Department of Obstetrics and Gynecology, I.M. Sechenov FirstMoscow State Medical University, Moscow, Russia
Semin Thromb Hemost 2021;00:1–15.
Address for correspondence Sam Schulman, MD, PhD, ThrombosisService, HHS-General Hospital, 237 Barton Street East, Hamilton ON,L8L 2� 2, Canada (e-mail: [email protected]).
Antiphospholipid syndrome (APS) is an acquired autoimmunedisease that is characterized by the presence of recurrentthrombotic events (venous, arterial, and/or microvascular)and/or pregnancy morbidity. The classification criteria forresearch studies also require at least one laboratory criterion—lupus anticoagulant (LA; also called nonspecific inhibitor),cardiolipin (aCL) antibodies immunoglobulin G (IgG) and/or
IgM isotype, and/or β2-glycoprotein I antibodies (aβ2GPI) IgGand/or IgM isotype, with confirmation 12 weeks after theinitial sample.1 APS is classified according to the 2006 Sydneyinternational consensus criteria,1 which were a revision of theSapporo criteria.2 APS occurs as a primary condition or can beassociatedwithsystemic lupus erythematosus (SLE)oranotherautoimmune disease.
Keywords
► antiphospholipidsyndrome
► arterial thrombosis► stroke► recurrence► bleeding
Abstract There is a scarcity of high-quality randomized controlled trials (RCTs) comparingantithrombotic regimens for secondary prevention of arterial thrombosis (AT) inantiphospholipid syndrome (APS). We reviewed different antithrombotic regimensused for this purpose.We searched for studies onmanagement of AT in APS on PubMedand Web of Science. Eleven studies (5 RCTs, 3 prospective, and 3 retrospective cohortstudies) comparing different regimens and reporting outcomes specifically for patientswith index AT events were identified. Treatments were vitamin K antagonists (VKA; 9studies), non-VKA oral anticoagulant (NOAC; 3 studies), single antiplatelet therapy(SAPT; 7 studies), dual antiplatelet therapy (DAPT; 2 studies), and VKA combined withSAPT (4 studies). We performed a meta-analysis for the outcomes: recurrent AT, any(arterial or venous) recurrent thromboembolism, and major bleeding. Recurrent ATwas reduced with VKA plus SAPT versus VKA (risk ratio [RR]: 0.43; 95% confidenceinterval [CI]: 0.22–0.85) and with DAPT versus SAPT (RR: 0.29; 95% CI: 0.09–0.99). Anyrecurrent thromboembolism was reduced with VKA plus SAPT versus VKA alone (RR:0.41; 95% CI: 0.24–0.69) and versus SAPT alone (RR: 0.36; 95% CI: 0.13–0.96). Therewere no significant differences between other treatments for thromboembolism andfor none of the comparisons regarding major bleeding. In a sensitivity analysis,excluding low-quality studies, VKA was more effective than NOAC to prevent recurrentAT (RR: 0.25; 95% CI: 0.07–0.93). Combined antithrombotic therapy might be moreeffective than single agents as secondary prophylaxis in APSwith AT, and does not seemto compromise with safety, but the quality of evidence is generally low. NOACs shouldbe avoided for patients with APS and AT.
Issue Theme Recent Advances inThrombosis and Hemostasis—Part VII;Guest Editor: Sam Schulman, MD, PhD.
© 2021. Thieme. All rights reserved.Thieme Medical Publishers, Inc.,333 Seventh Avenue, 18th Floor,New York, NY 10001, USA
DOI https://doi.org/10.1055/s-0041-1725057.ISSN 0094-6176.
1

In a recent population-based study of patients with APS inthe United States, the overall annual incidence of APS was 2.1per 100,000 population (age- and sex-adjusted), and the prev-alence was 50 per 100,000 population.3 The incidence wasthe same amongmales and females. However, in a nationwidepopulation-based study performed inKorea, the incidence ratewas 0.75 per 100,000 person-years (95% confidence interval[CI]: 0.73–0.78); incidence in males: 0.59 (95% CI: 0.56–0.62)and females: 0.91 (95% CI: 0.87–0.96). Moreover, the incidencerates between males and females exhibited different patterns.Males had a peak incidence rate at 70 to 79 years of age, andfemalespresented incidencepeaksat 30 to39years andat70to79 years of age.4 Venous thromboembolism was the mostcommon clinical manifestation in the above-mentioned epi-demiological study,3,4 but serious arterial events were notuncommon, including stroke (35%) and peripheral arterialthrombosis (8%).
Several studies have evaluated the incidence of recurrentarterial and venous thrombosis after a first event in patientswith APS. There is evidence that after a first arterial or venousthrombosis, patients with APS have a higher risk of a newthrombosis than patients without APS.5 Moreover, patientswith APS and a first arterial thrombosis have a higher risk ofrecurrence than those with a first venous thrombosis.6–8
Furthermore, the risk of venous or arterial thrombosis isincreased in patients with positive LA, with medium or highlevels of aCL of the IgG or IgM type, and with double or triplepositivity of antiphospholipid antibodies (aPLs).9–14
Treatment of the first venous thrombosis in patients withdefinite APS should, according to different guidelines, bewith avitamin K antagonist (VKA) with a therapeutic range of inter-national normalized ratio (INR) of 2.0 to 3.0.15,16 The treatmentof choice for afirst arterial thrombosis is still amatter ofdebate.According to the European League Against Rheumatism(EULAR) recommendations for themanagementofAPSinadultspublished in 20196 and 2012 Guidelines on the Investigationand Management of APS,16 in patients with APS and a firstarterial thrombosis (excluding ischemic stroke) thetreatment iswith VKAwith a therapeutic range of INR 2 to 3. Unfortunately,randomized controlled trials (RCTs) of high quality in APSwitharterial thrombosis, comparing high- or moderate-intensityanticoagulation with VKA versus antiplatelet agents or acombination of both are lacking.15,17,18 In patients with strokeor transient ischemic attack (TIA), there is no evidence support-ingone treatment (VKAvs. antiplatelet agents vs. a combinationof both) over the other.17 Experts recommend therapy witheither antiplatelet agents or VKA (INR range: 2–3).17 The aimofthis review is to specifically analyze studies including patientswith definite APSwith recurrent arterial thrombosis to try andidentify the best treatment options for secondary prevention ofarterial thrombosis.We therefore performeda literature searchand a meta-analysis of the study-level data.
Methods
Search StrategyWe searched PubMed, the Cochrane database, and the Web ofScience, including all records from 1965 through January 31,
2020.MeSHand keyword termsusedwere APS, arterial throm-bosis, stroke, and recurrent thrombosis. Only articles publishedin English were considered for the review. We reviewed thetitles and abstracts of all the articles obtained and includedstudies thatdescribed the incidenceof recurrentarterial throm-bosis in patients with APS, who were over 18 years of age. Wealso reviewed the bibliographic references of all systematicreviews obtained to identify additional studies related toour search.
Inclusion and Exclusion CriteriaWe included full papers as well as abstracts, as long as therequired data were available. RCTs and prospective or retro-spective cohort studies comparing different oral antithrom-botic treatment regimens were eligible. The study populationhad to include patientswith arterial thrombosis but could alsoconsist of patients with other clinical manifestations providedthat the outcomes were reported separately for those witharterial thrombosis. Studies comparing a single treatmentregimen with historical data from other publications onanother regimen were excluded.
Treatment RegimensThe antiplatelet agents were aspirin (most of the cases),ticlopidine, clopidogrel, cilostazol, dipyridamole, beraprostsodium, sarpogrelate hydrochloride, and dilazep dihydrochlor-ide. Dual antiplatelet therapy (DAPT) was any combination ofthose. In the studies comparing VKAwith other regimens, thetherapeutic rangewas INR 2.0 to 3.0 with the exception for theAntiphospholipid Antibodies and Stroke Study (APASS), whichused INR1.4 to 2.8, and the studybyYamazaki et al,whichusedINR 2.0 to 2.5.19,20 Non-VKA oral anticoagulant (NOAC) wasmainly rivaroxaban, with the exception of one study, in whichalso apixaban and dabigatran were used.21
Outcome MeasuresThe outcomes were recurrent arterial thrombosis, anythromboembolism (arterial or venous thromboembolism),as well as major bleeding as defined by the original authors.Arterial events included stroke, TIA, myocardial infarction,peripheral arterial thromboembolism, systemic visceralarterial embolism, and central retinal artery occlusion.
Quality Assessment of StudiesFor the assessment of the quality of studies, we used theJadad score for RCTs,22 and the Newcastle–Ottawa Scale forcohort studies.23
Statistical AnalysisWe performed the analysis based on intention-to-treat andcalculated risk ratio (RR) and 95% CI. Meta-analysis wasperformed, using the random-effects model, when therewere at least two eligible studies comparing the same pairof treatment regimens and reporting the same type ofoutcome. The reason for this model was that we expected ahigh degree of heterogeneity. We quantified heterogeneityusing I2, where I2>50% corresponds to high and I2¼25 to 50%corresponds to moderate heterogeneity. Due to the small
Seminars in Thrombosis & Hemostasis Vol. 00 No. 0/2021 © 2021. Thieme. All rights reserved.
Arterial Thrombosis in Antiphospholipid Syndrome Aibar, Schulman2
number of studies for each comparison, it was not meaningfulto test for publication bias, using funnel plots. All tests weretwo-sided and we considered a p-value of <0.05 statisticallysignificant. For the meta-analysis, we used Review Manager(RevMan), version 5.3 (Copenhagen; The Nordic CochraneCentre, The Cochrane Collaboration, 2014).
Results
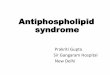
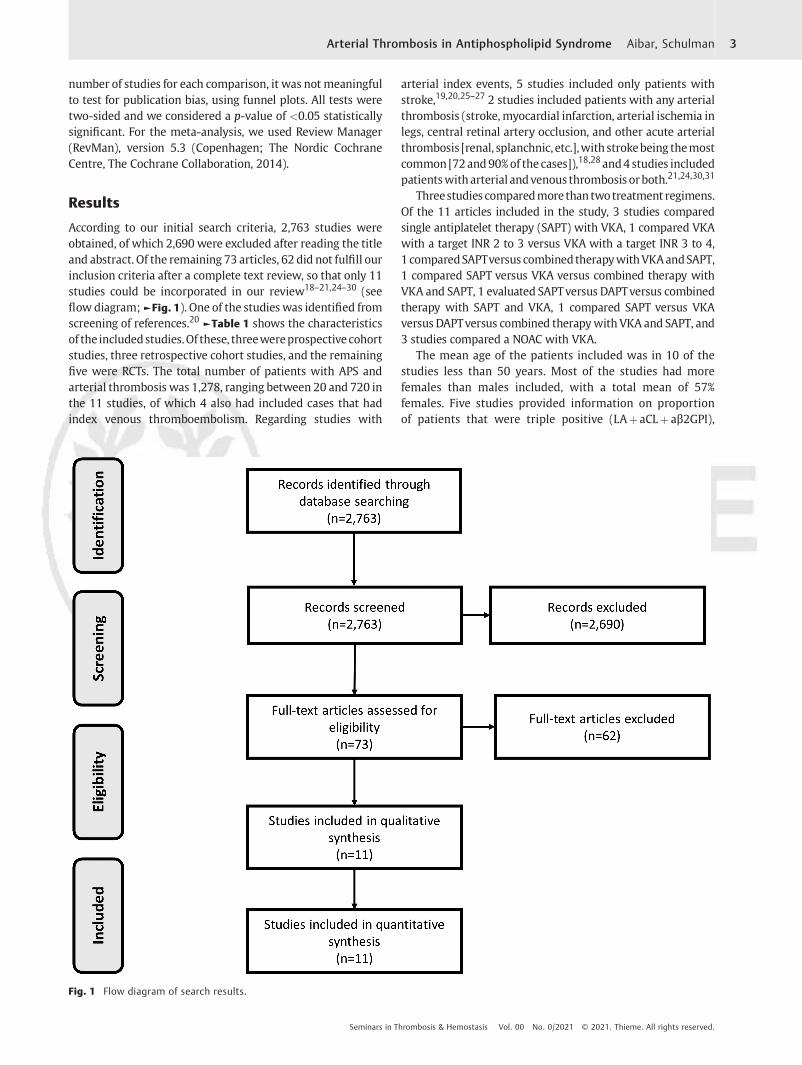
According to our initial search criteria, 2,763 studies wereobtained, of which 2,690 were excluded after reading the titleand abstract. Of the remaining 73 articles, 62 did not fulfill ourinclusion criteria after a complete text review, so that only 11studies could be incorporated in our review18–21,24–30 (seeflow diagram;►Fig. 1). One of the studies was identified fromscreening of references.20 ►Table 1 shows the characteristicsof the includedstudies.Of these, threewereprospectivecohortstudies, three retrospective cohort studies, and the remainingfive were RCTs. The total number of patients with APS andarterial thrombosis was 1,278, ranging between 20 and 720 inthe 11 studies, of which 4 also had included cases that hadindex venous thromboembolism. Regarding studies with
arterial index events, 5 studies included only patients withstroke,19,20,25–27 2 studies included patients with any arterialthrombosis (stroke,myocardial infarction, arterial ischemia inlegs, central retinal artery occlusion, and other acute arterialthrombosis [renal, splanchnic, etc.],with strokebeing themostcommon[72and90%of the cases]),18,28and4 studies includedpatientswith arterial andvenous thrombosis orboth.21,24,30,31
Threestudies comparedmore than twotreatment regimens.Of the 11 articles included in the study, 3 studies comparedsingle antiplatelet therapy (SAPT) with VKA, 1 compared VKAwith a target INR 2 to 3 versus VKA with a target INR 3 to 4,1 comparedSAPTversus combined therapywithVKAandSAPT,1 compared SAPT versus VKA versus combined therapy withVKA and SAPT, 1 evaluated SAPTversus DAPTversus combinedtherapy with SAPT and VKA, 1 compared SAPT versus VKAversus DAPTversus combined therapywithVKA and SAPT, and3 studies compared a NOAC with VKA.
The mean age of the patients included was in 10 of thestudies less than 50 years. Most of the studies had morefemales than males included, with a total mean of 57%females. Five studies provided information on proportionof patients that were triple positive (LAþ aCLþ aβ2GPI),
Fig. 1 Flow diagram of search results.
Seminars in Thrombosis & Hemostasis Vol. 00 No. 0/2021 © 2021. Thieme. All rights reserved.
Arterial Thrombosis in Antiphospholipid Syndrome Aibar, Schulman 3
Table
1Cha
racteristics
oftheinclud
edstud
ies
Stud
y(first
author,ye
ar)
APS
definition
N (num
ber
ofce
nters)
Design
Indicationfor
trea
tmen
tAge,
yFe
males,
%Triple
pos
itive,
%Prim
aryAPS
/seco
ndary
toSL
E,%/%
Trea
tmen
tsFo
llow-up
years
Crowther,20
0324
Sydn
eycriteria
114(13)
RCT
Arterialo
rve
nous
thrombo
sis
4260
Unk
nown
86/14
VKAINR2–
3vs.
VKAINR3–
42.7
Levine
,20
0419
Stroke
þaP
Lpo
sitive
720(44)
Prospe
ctive
withinRC
TStroke
6242
Unk
nown
Noda
taVKAvs.S
APT
2
Yamazak
i,20
0920
Noda
ta60
(Noda
ta)
RCT
Stroke
Noda
taNoda
taNoda
taNoda
taSA
PTvs.D
APT
vs.
VKAplus
SAPT
3
Oku
ma,
2009
25Sydn
eycriteria
20(1)
RCT
Stroke
4850
Noda
ta65
/35
SAPT
vs.V
KA
plus
SAPT
3.9(2)
Arauz
,201
126
Sapp
oro
criteria
92(1)
Prospe
ctive
coho
rtstud
yStroke
3471
Noda
ta10
0/0
SAPT
vs.V
KA
4.5
Jack
son,
2017
18Sydn
eycriteria
139(26)
Retrospec
tive
coho
rtstud
yAny
arterial
thrombo
sis
4366
3666
/34(any
autoim
mun
e)SA
PTvs.V
KAvs.
VKAplus
SAPT
4.24
Pyo,
2017
27Sydn
eycriteria
46(1)
Retrospec
tive
coho
rtstud
yStroke
4461
3758
/20(2%Be
hcet)
SAPT
vs.V
KA
4.3
Ohn
ishi,2
0192
8Sydn
eycriteria
90(1)
Retrospec
tive
coho
rtstud
yAny
arterial
thrombo
sis
4573
Noda
ta41
/59
SAPT
vs.V
KAvs.
VKAplus
SAPT
vs.D
APT
8
Peng
o,20
1829
Sydn
eycriteria
120(14)
RCT
Arterialo
rve
nous
thrombo
sis
ormicrothrombo
sis
4664
100
59/21(20%
othe
rau
toim
mun
e)Rivarox
aban
vs.V
KA
1.5
Ordi-R
os,20
1930
Sydn
eycriteria
190(6)
RCT
Arterialo
rve
nous
thrombo
sis
4964
6169
/31
Rivarox
aban
vs.V
KA
3
Malec
,20
2021
Sydn
eycriteria
176(1)
Prospe
ctive
coho
rtstud
yArterialo
rve
nous
thrombo
sis
4483
26Noda
taNOACvs.VKA
4.3
Abbrev
iation
s:APS
,antipho
spho
lipid
synd
rome;
DAPT
,dua
lantiplateletthe
rapy
;INR,
internationa
lnormalized
ratio;N
OAC,n
on-VKAoralan
tico
agulan
t;RC
T,rand
omized
controlle
dtrial;SA
PT,singlean
tiplatelet
therap
y;SLE,
system
iclupu
serythe
matos
us;VKA,vitamin
Kan
tago
nist.
Seminars in Thrombosis & Hemostasis Vol. 00 No. 0/2021 © 2021. Thieme. All rights reserved.
Arterial Thrombosis in Antiphospholipid Syndrome Aibar, Schulman4
ranging from 26 to 100%. The proportion of patients withprimary APS ranged from 41 to 84% in the seven studies thatcontained this information.
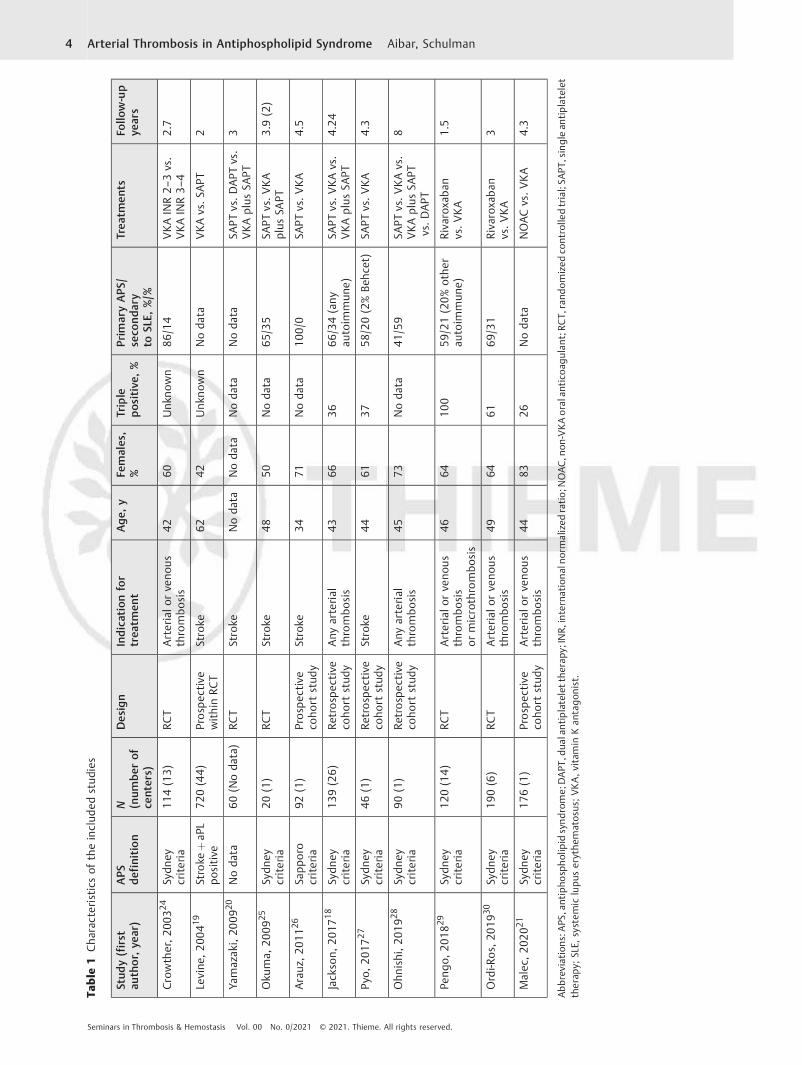
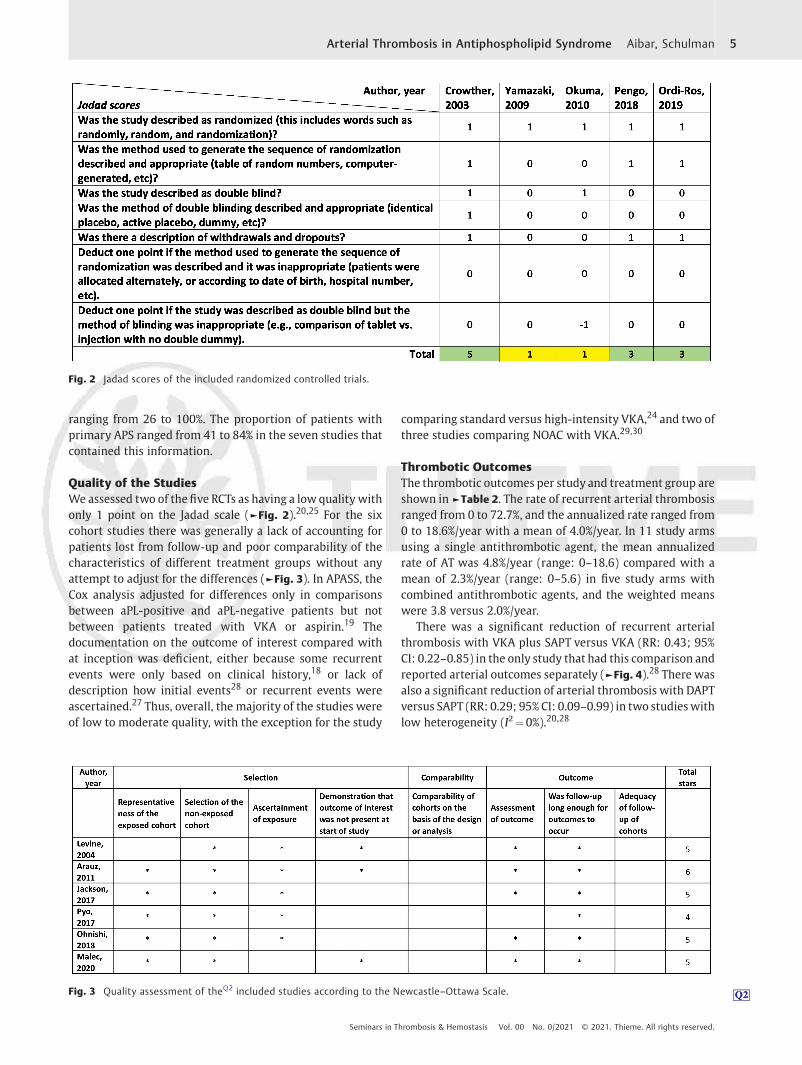
Quality of the StudiesWe assessed two of thefive RCTs as having a low quality withonly 1 point on the Jadad scale (►Fig. 2).20,25 For the sixcohort studies there was generally a lack of accounting forpatients lost from follow-up and poor comparability of thecharacteristics of different treatment groups without anyattempt to adjust for the differences (►Fig. 3). In APASS, theCox analysis adjusted for differences only in comparisonsbetween aPL-positive and aPL-negative patients but notbetween patients treated with VKA or aspirin.19 Thedocumentation on the outcome of interest compared withat inception was deficient, either because some recurrentevents were only based on clinical history,18 or lack ofdescription how initial events28 or recurrent events wereascertained.27 Thus, overall, the majority of the studies wereof low to moderate quality, with the exception for the study
comparing standard versus high-intensity VKA,24 and two ofthree studies comparing NOAC with VKA.29,30
Thrombotic OutcomesThe thrombotic outcomes per study and treatment group areshown in ►Table 2. The rate of recurrent arterial thrombosisranged from 0 to 72.7%, and the annualized rate ranged from0 to 18.6%/year with a mean of 4.0%/year. In 11 study armsusing a single antithrombotic agent, the mean annualizedrate of AT was 4.8%/year (range: 0–18.6) compared with amean of 2.3%/year (range: 0–5.6) in five study arms withcombined antithrombotic agents, and the weighted meanswere 3.8 versus 2.0%/year.
There was a significant reduction of recurrent arterialthrombosis with VKA plus SAPT versus VKA (RR: 0.43; 95%CI: 0.22–0.85) in the only study that had this comparison andreported arterial outcomes separately (►Fig. 4).28 There wasalso a significant reduction of arterial thrombosis with DAPTversus SAPT (RR: 0.29; 95% CI: 0.09–0.99) in two studieswithlow heterogeneity (I2¼0%).20,28
Fig. 3 Quality assessment of the Q2Q2Q2 included studies according to the Newcastle–Ottawa Scale.
Fig. 2 Jadad scores of the included randomized controlled trials.
Seminars in Thrombosis & Hemostasis Vol. 00 No. 0/2021 © 2021. Thieme. All rights reserved.
Arterial Thrombosis in Antiphospholipid Syndrome Aibar, Schulman 5

Table
2Initialthrom
boticev
ents
andthrombo
ticev
ents
during
follo
w-up,acco
rdingto
trea
tmen
tregimen
Stud
y(first
author,ye
ar)
NTo
talnum
ber
pertrea
tmen
tarm
(N)an
dnum
ber(%
)with
initialarterial
even
tPa
tien
tswitharterial
index
even
t(N
)an
dthrombo
ticev
ents,n(%
),during
follo
w-up
Crowther,20
0324
114
VKAINR3–
4(N
¼56
)14
(25%
)VKAINR2–
3(N
¼58
)13
(22.4%
)VKAINR3–
4(N
¼14
)1(7.1%)arterialþ2(14.3%
)ve
nous
VKAINR2–
3(N
¼13
)1(7.7%)arterialþ0ve
nous
Levine
,20
0419
720
SAPT
(N¼35
9)35
9(100
%)
VKA(N
¼36
1)36
1(100
%)
SAPT
(N¼35
9)80
(22.3%
)arterial
orve
nous
VKA(N
¼36
1)94
(26%
)arterial
orve
nous
Yamazak
i,20
0920
60SA
PT(N
¼20
)20
(100
%)
DAPT
(N¼20
)20
(100
%)
VKAþSA
PT(N
¼20
)20
(100
%)
SAPT
(N¼20
)3(15%
)arterial
DAPT
(N¼20
)0(0%)
VKAþSA
PT(N
¼20
)0(0%)
Oku
ma,
2009
2520
SAPT
(N¼11
)11
(100
%)
VKAþSA
PT(N
¼9)
9(100
%)
SAPT
(N¼11
)8(72.7%
)arterialþ0ve
nous
VKAþSA
PT(N
¼9)
2(22.2%
)arterialþ0ve
nous
Arauz
,201
126
92SA
PT(N
¼38
)38
(100
%)
VKA(N
¼54
)54
(100
%)
SAPT
(N¼38
)0
VKA(N
¼54
)8(14.8%
)arterialþ0ve
nous
Jack
son,
2017
1813
9SA
PT(N
¼43
)43
(100
%)
VKA(N
¼38
)38
(100
%)
VKAþSA
PT(N
¼58
)58
(100
%)
SAPT
(N¼43
)16
(37.2%
)arterial
orve
nous
VKA(N
¼38
)9(23.7%
)arterial
orve
nous
VKAþSA
PT(N
¼58
)4(6.9%)arterial
orve
nous
Pyo,
2017
2746
SAPT
(N¼22
)22
(100
%)
VKA(N
¼24
)24
(100
%)
SAPT
(N¼22
)6(27.3%
)arterial
orve
nous
VKA(N
¼24
)8(33.3%
)arterial
orve
nous
Ohn
ishi,2
0192
890
SAPT
(N¼41
)41
(100
%)
VKA
(N¼13
)13
(100
%)
VKAþSA
PT(N
¼21
)21
(100
%)
DAPT
(N¼15
)15
(100
%)
SAPT
(N¼41
)16
(39%
)arterialþ
2(4.9%)ve
nous
VKA(N
¼13
)10
(77%
)arterialþ
1(7.7%)ve
nous
VKAþSA
PT(N
¼21
)7(33.3%
)arterialþ
1(4.8%)ve
nous
DAPT
(N¼15
)2(13.3%
)arterialþ
1(6.7%)ve
nous
Peng
o,20
1829
120
NOAC(N
¼59
)21
(35.6%
)VKA(N
¼61
)22
(36.2%
)NOAC(N
¼21
)4(19%
)arterialþ0ve
nous
VKA(N
¼22
)0arterialþ0ve
nous
Ordi-R
os,20
1930
190
NOAC(N
¼95
)37
(39%
)VKA(N
¼95
)34
(35.8%
)NOAC(N
¼37
)7(18.9%
)arterialþ1(2.7%)ve
nous
VKA(N
¼34
)2(5.9%)arterialþ1(2.9%)ve
nous
Malec
,20
2021
176
NOAC(N
¼82
)22
(26.8%
)VKA(N
¼94
)20
(21.27
%)
NOACs(N
¼22
)2(9%)arterialþ1(4.5%)ve
nous
VKA(N
¼20
)2(10%
)arterialþ2(10%
)ve
nous
Abbrev
iation
s:DAPT
,du
alan
tiplatelettherap
y;INR,internationa
lnormalized
ratio;NOAC,no
n-VKAoral
antico
agulan
t;SA
PT,sing
lean
tiplatelettherap
y;VKA,vitamin
Kan
tago
nist.
Seminars in Thrombosis & Hemostasis Vol. 00 No. 0/2021 © 2021. Thieme. All rights reserved.
Arterial Thrombosis in Antiphospholipid Syndrome Aibar, Schulman6
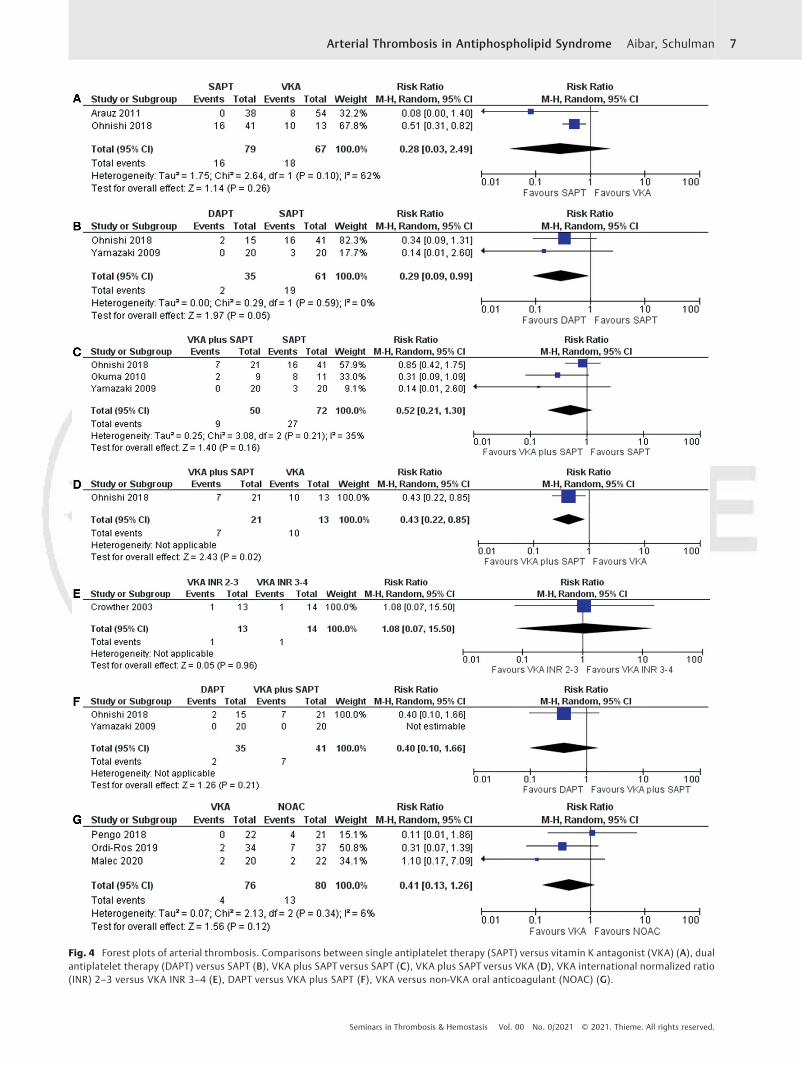
Fig. 4 Forest plots of arterial thrombosis. Comparisons between single antiplatelet therapy (SAPT) versus vitamin K antagonist (VKA) (A), dualantiplatelet therapy (DAPT) versus SAPT (B), VKA plus SAPT versus SAPT (C), VKA plus SAPT versus VKA (D), VKA international normalized ratio(INR) 2–3 versus VKA INR 3–4 (E), DAPT versus VKA plus SAPT (F), VKA versus non-VKA oral anticoagulant (NOAC) (G).
Seminars in Thrombosis & Hemostasis Vol. 00 No. 0/2021 © 2021. Thieme. All rights reserved.
Arterial Thrombosis in Antiphospholipid Syndrome Aibar, Schulman 7
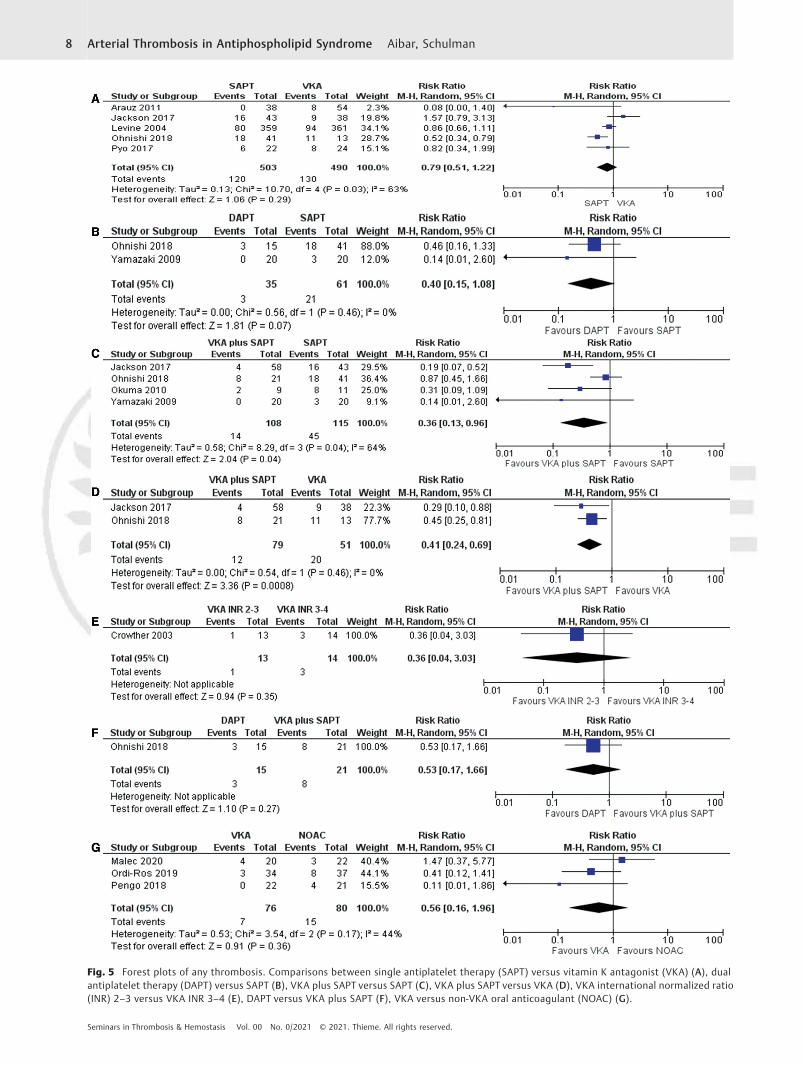
Fig. 5 Forest plots of any thrombosis. Comparisons between single antiplatelet therapy (SAPT) versus vitamin K antagonist (VKA) (A), dualantiplatelet therapy (DAPT) versus SAPT (B), VKA plus SAPT versus SAPT (C), VKA plus SAPT versus VKA (D), VKA international normalized ratio(INR) 2–3 versus VKA INR 3–4 (E), DAPT versus VKA plus SAPT (F), VKA versus non-VKA oral anticoagulant (NOAC) (G).
Seminars in Thrombosis & Hemostasis Vol. 00 No. 0/2021 © 2021. Thieme. All rights reserved.
Arterial Thrombosis in Antiphospholipid Syndrome Aibar, Schulman8

For the composite of arterial and venous thromboembo-lism, therewas a significant reduction of eventswith VKAplusSAPT versus VKA alone (RR: 0.41; 95% CI: 0.24–0.69) intwo studies with low heterogeneity (I2¼0%) (►Fig. 5).18,28
Likewise, there was a reduction with VKA plus SAPT versusSAPT alone (RR: 0.36; 95% CI: 0.13–0.96) in four studieswith high heterogeneity (I2¼64%).18,20,25,28 There was atrend to reduced events with DAPT versus SAPT (RR: 0.40;95% CI: 0.15–1.08) in two studies with low heterogeneity(I2¼0%).20,28
In seven studies, patients with arterial thrombosis asindex event had recurrence mostly as arterial thrombosisagain, in three studies therewere no data, and only one studyshowedmore recurrences as venous thrombosis than arteri-al thrombosis.
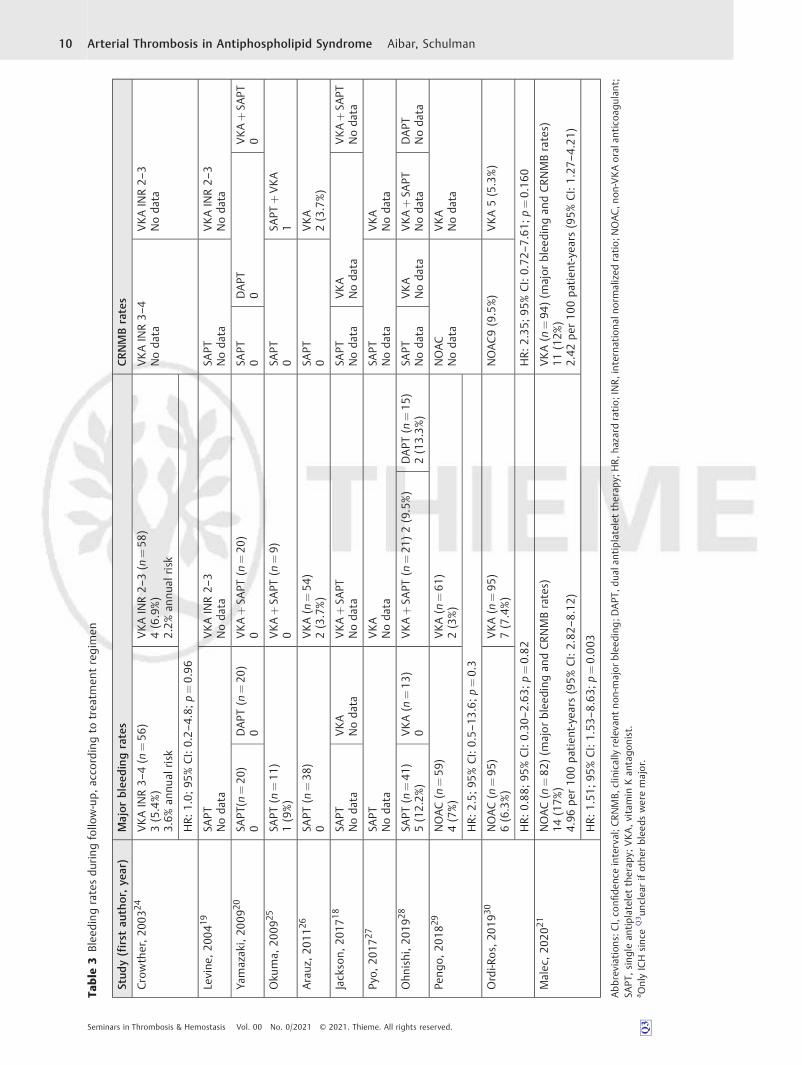
Bleeding OutcomeMajor bleeding events were reported and separated fromother bleeding in seven studies (►Table 3) and there was nosignificant difference in this outcome between any of thetreatment regimens compared (►Fig. 6).
HeterogeneityModerate to high heterogeneity was seen in some of thecomparisons and seemed to be due to very favorable resultsregarding any thrombotic recurrence and low risk of bleedingfor SAPT in the study byArauz et al,26possibly due to the lowermean age (34 years) versus the other studies. Furthermore, forthe outcome of recurrent arterial thrombosis, the heterogene-ity could have been due to the much higher proportionof secondary APS in the study by Ohnishi et al (55%)28 versusthe other studies.
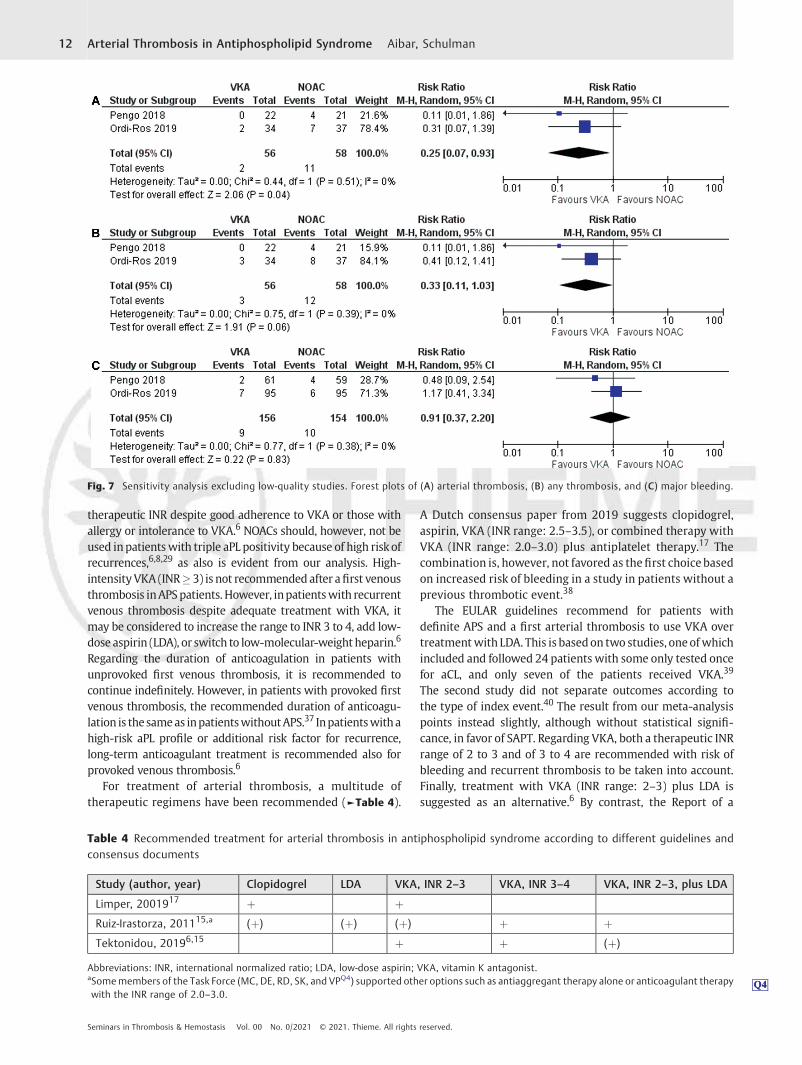
Sensitivity AnalysisA sensitivity analysis was performed for treatment regimenswith both high-quality RTCs and low-quality RCTs or low-quality cohort studies represented, excluding the low-qualitystudies. This situation only pertained to the comparison ofNOACs with VKA. After excluding the study by Malec et al,21
there was a significant reduction of arterial thrombosis withVKA versus NOAC (RR: 0.25; 95% CI: 0.07–0.93) and a trend toreductionof thecomposite thromboticoutcome(RR:0.33;95%CI: 0.11–1.03), without any difference in riskofmajor bleeding(2 studies, I2¼0%) (►Fig. 7).
Discussion
Arterial Thrombotic Manifestations of APSIn vascular APS, the most common presenting manifesta-tions, according to the Euro-Phospholipid Project,32,33 astudy performed in a cohort of 1,000 APS patients, weredeepvein thrombosis (DVT; 32%), pulmonary embolism (9%),and superficial thrombophlebitis in the legs (9%). Among thearterial thrombotic manifestations, stroke (13%), TIA (7%),and myocardial infarction (3%) were the most common.32 Ithas been suggested that more than 20% of strokes in patientunder 45 years are associated with APS.34,35 In a retrospec-tive study including 218 patients with primary APS and 288
with APS secondary to SLE, Soltész et al reported thatthrombotic manifestations were venous (DVT and pulmo-nary embolism) in 37%, coronary and carotid in 34%, andcerebrovascular in 40%.36 In a Japanese retrospective studywith 141 patients, arterial thrombosis was the presentingmanifestation in 66% (mainly as stroke) versus venousthrombosis in 33%.10 In a Korean nationwide population-based studywith 3,088 newly diagnosed APS patients, strokeor TIA was the most common manifestation (28%) followedby DVT (20%) and pulmonary embolism (17.5%).4
In the studies in our meta-analysis that recruited patientswith either arterial or venous thrombosis as indexevent, 64 to89%ofpatientspresentedwithvenous thrombosis.21,24,30,31 Inthe study by Pengo et al,31 stroke was the first APS manifesta-tion in 13% of the patients. Malec et al showed that 24% of thepatients had stroke (or TIA) as first APS manifestation.21 Thus,the proportionof APS patientswith arterial thrombosis asfirstevent varies from approximately 20% up to 74%, probablydepending on the type of patients referred, the profile of thecenter, and other selection bias.
Management of Arterial ThrombosisIn this meta-analysis of 11 studies, comparing seven differenttherapeutic constellations for the management of APS patientswith arterial thrombosis as first presenting manifestation, wemade some potentially interesting observations. For theprevention of recurrent arterial thrombosis, DAPT seemed tobe more effective than SAPT and similarly VKA plus SAPTappeared more effective than VKA alone (albeit based on onlyone small study). Recurrent arterial thrombosis or venousthromboembolism gave the impression of being reduced withVKA plus SAPT both when compared with VKA alone and toSAPT alone, and DAPT demonstrated a trend to better effectcomparedwith SAPT. Thus, it is possible that patients with APSand arterial thrombosis may benefit from a combination ofantithrombotic agents, with reservations for the low quality ofmost of the included studies and the small number of patientsand events. None of our comparisons of treatment regimensidentifieda significantdifference in the riskofmajor bleeding. Itis reasonable to assume that with the hypercoagulable stateassociated with APS, the risk of recurrent thrombotic eventsoutweighs the risk of bleeding complications even with themore aggressive treatment regimens. Furthermore, our sensi-tivityanalysiswithonlystudiesofhighquality showedthatVKAis superior to NOAC for reducing the risk of recurrent AT aswellas (borderline significance) for the composite of arterial andvenous thromboembolism.
The treatment of thrombosis in APS has been studiedduring the past three decades. Factors that can modify theresponse to the treatment include aPL profile (double, triplepositivity, LA), primary versus secondary APS, increasingnumber of criteria for definite APS, the site of thrombosis(arterial or small vessel), male sex, and the presence of othercardiovascular risk factors.8,35
Guideline RecommendationsAccording to the EULAR recommendations, a NOAC could beconsidered for patients who are not able to maintain a
Seminars in Thrombosis & Hemostasis Vol. 00 No. 0/2021 © 2021. Thieme. All rights reserved.
Arterial Thrombosis in Antiphospholipid Syndrome Aibar, Schulman 9
Table
3Blee
ding
ratesdu
ring
follo
w-up,
acco
rdingto
trea
tmen
tregim
en
Stud
y(first
author,ye
ar)
Major
blee
dingrates
CRNMBrates
Crowther,20
0324
VKAINR3–
4(n
¼56
)3(5.4%)
3.6%
annu
alrisk
VKAINR2–
3(n
¼58
)4(6.9%)
2.2%
annu
alrisk
VKAINR3–
4Noda
taVKAINR2–
3Noda
ta
HR:
1.0;
95%CI:0.2–
4.8;
p¼0.96
Levine
,20
0419
SAPT
Noda
taVKAINR2–
3Noda
taSA
PTNoda
taVKAINR2–
3Noda
ta
Yamazak
i,20
0920
SAPT
(n¼20
)0
DAPT
(n¼20
)0
VKAþSA
PT(n
¼20
)0
SAPT
0DAPT
0VKAþSA
PT0
Oku
ma,
2009
25SA
PT(n
¼11
)1(9%)
VKAþSA
PT(n
¼9)
0SA
PT0
SAPT
þVKA
1
Arauz
,201
126
SAPT
(n¼38
)0
VKA(n
¼54
)2(3.7%)
SAPT
0VKA
2(3.7%)
Jack
son,
2017
18SA
PTNoda
taVKA
Noda
taVKAþSA
PTNoda
taSA
PTNoda
taVKA
Noda
taVKAþSA
PTNoda
ta
Pyo,
2017
27SA
PTNoda
taVKA
Noda
taSA
PTNoda
taVKA
Noda
ta
Ohn
ishi,2
0192
8SA
PT(n
¼41
)5(12.2%
)VKA(n
¼13
)0
VKAþSA
PT(n
¼21
)2(9.5%)
DAPT
(n¼15
)2(13.3%
)SA
PTNoda
taVKA
Noda
taVKAþSA
PTNoda
taDAPT
Noda
ta
Peng
o,20
1829
NOAC(n
¼59
)4(7%)
VKA(n
¼61
)2(3%)
NOAC
Noda
taVKA
Noda
ta
HR:
2.5;
95%CI:0.5–
13.6;p¼0.3
Ordi-R
os,20
1930
NOAC(n
¼95
)6(6.3%)
VKA(n
¼95
)7(7.4%)
NOAC9(9.5%)
VKA5(5.3%)
HR:0
.88;
95%CI:0.30
–2.63;
p¼0.82
HR:2
.35;
95%CI:0.72
–7.61;
p¼0.16
0
Malec
,20
2021
NOAC(n
¼82
)(m
ajorblee
ding
andCRNMBrates)
14(17%
)4.96
per10
0pa
tien
t-years(95%
CI:2.82
–8.12)
VKA(n
¼94
)(m
ajor
blee
ding
andCRNMBrates)
11(12%
)2.42
per10
0pa
tien
t-years(95%
CI:1.27
–4.21)
HR:1
.51;
95%CI:1.53
–8.63;
p¼0.00
3
Abbrev
iation
s:CI,co
nfide
nceinterval;C
RNMB,
clinicallyreleva
ntno
n-majorblee
ding
;DAPT
,dua
lantiplatelettherap
y;HR,h
azardratio;INR,interna
tion
alno
rmalized
ratio;N
OAC,n
on-VKAoral
antico
agulan
t;SA
PT,sing
lean
tiplatelettherap
y;VKA,vitamin
Kan
tago
nist.
a OnlyICH
sinc
eQ3
Q3un
clea
rifothe
rblee
dsweremajor.
Seminars in Thrombosis & Hemostasis Vol. 00 No. 0/2021 © 2021. Thieme. All rights reserved.
Arterial Thrombosis in Antiphospholipid Syndrome Aibar, Schulman10
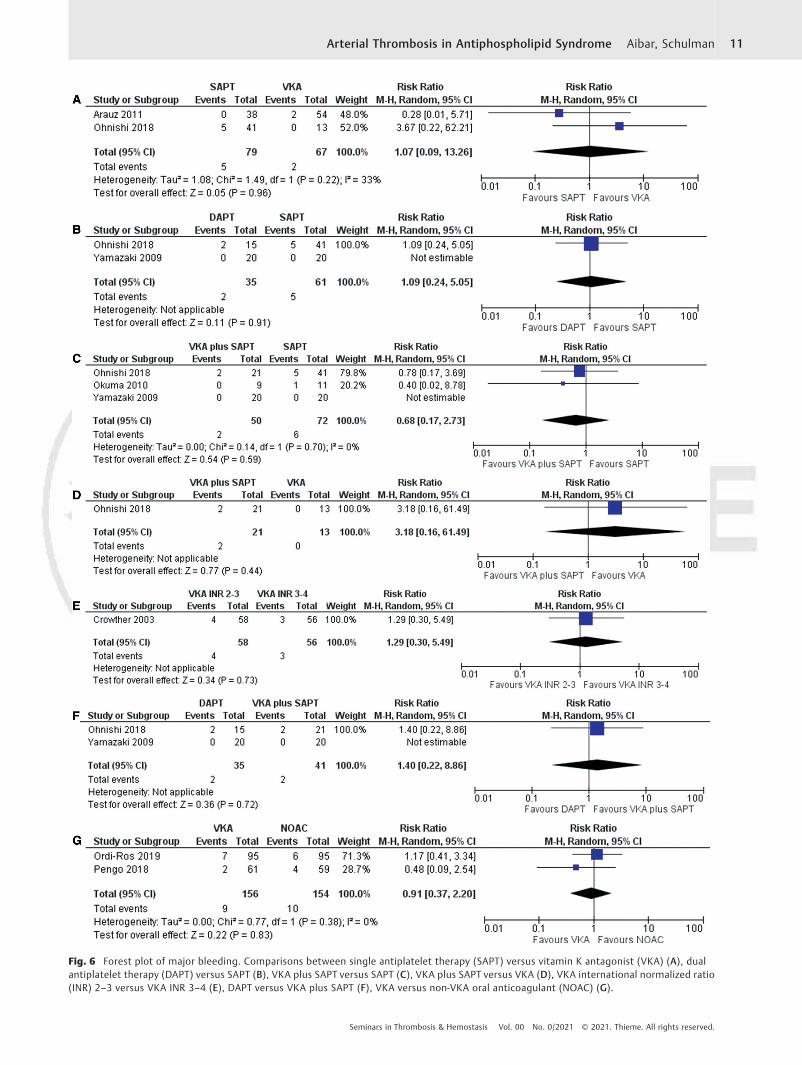
Fig. 6 Forest plot of major bleeding. Comparisons between single antiplatelet therapy (SAPT) versus vitamin K antagonist (VKA) (A), dualantiplatelet therapy (DAPT) versus SAPT (B), VKA plus SAPT versus SAPT (C), VKA plus SAPT versus VKA (D), VKA international normalized ratio(INR) 2–3 versus VKA INR 3–4 (E), DAPT versus VKA plus SAPT (F), VKA versus non-VKA oral anticoagulant (NOAC) (G).
Seminars in Thrombosis & Hemostasis Vol. 00 No. 0/2021 © 2021. Thieme. All rights reserved.
Arterial Thrombosis in Antiphospholipid Syndrome Aibar, Schulman 11
therapeutic INR despite good adherence to VKA or those withallergy or intolerance to VKA.6 NOACs should, however, not beused inpatientswith triple aPL positivity because of high riskofrecurrences,6,8,29 as also is evident from our analysis. High-intensityVKA (INR� 3) is not recommended after afirst venousthrombosis inAPSpatients. However, inpatientswith recurrentvenous thrombosis despite adequate treatment with VKA, itmay be considered to increase the range to INR 3 to 4, add low-dose aspirin (LDA), or switch to low-molecular-weight heparin.6
Regarding the duration of anticoagulation in patients withunprovoked first venous thrombosis, it is recommended tocontinue indefinitely. However, in patients with provoked firstvenous thrombosis, the recommended duration of anticoagu-lation is thesameas inpatientswithoutAPS.37 Inpatientswithahigh-risk aPL profile or additional risk factor for recurrence,long-term anticoagulant treatment is recommended also forprovoked venous thrombosis.6
For treatment of arterial thrombosis, a multitude oftherapeutic regimens have been recommended (►Table 4).
A Dutch consensus paper from 2019 suggests clopidogrel,aspirin, VKA (INR range: 2.5–3.5), or combined therapy withVKA (INR range: 2.0–3.0) plus antiplatelet therapy.17 Thecombination is, however, not favored as thefirst choicebasedon increased risk of bleeding in a study in patients without aprevious thrombotic event.38
The EULAR guidelines recommend for patients withdefinite APS and a first arterial thrombosis to use VKA overtreatmentwith LDA. This is basedon two studies, oneofwhichincluded and followed 24 patients with some only tested oncefor aCL, and only seven of the patients received VKA.39
The second study did not separate outcomes according tothe type of index event.40 The result from our meta-analysispoints instead slightly, although without statistical signifi-cance, in favor of SAPT. Regarding VKA, both a therapeutic INRrange of 2 to 3 and of 3 to 4 are recommended with risk ofbleeding and recurrent thrombosis to be taken into account.Finally, treatment with VKA (INR range: 2–3) plus LDA issuggested as an alternative.6 By contrast, the Report of a
Fig. 7 Sensitivity analysis excluding low-quality studies. Forest plots of (A) arterial thrombosis, (B) any thrombosis, and (C) major bleeding.
Table 4 Recommended treatment for arterial thrombosis in antiphospholipid syndrome according to different guidelines andconsensus documents
Study (author, year) Clopidogrel LDA VKA, INR 2–3 VKA, INR 3–4 VKA, INR 2–3, plus LDA
Limper, 2001917 þ þRuiz-Irastorza, 201115,a (þ) (þ) (þ) þ þTektonidou, 20196,15 þ þ (þ)
Abbreviations: INR, international normalized ratio; LDA, low-dose aspirin; VKA, vitamin K antagonist.aSomemembers of the Task Force (MC, DE, RD, SK, and VP Q4Q4
Q4) supported other options such as antiaggregant therapy alone or anticoagulant therapywith the INR range of 2.0–3.0.
Seminars in Thrombosis & Hemostasis Vol. 00 No. 0/2021 © 2021. Thieme. All rights reserved.
Arterial Thrombosis in Antiphospholipid Syndrome Aibar, Schulman12

Task Force at the 13th International Congress on Antiphos-pholipid Antibodies in 2011 recommended for patients withdefinite APS and arterial thrombosis either VKA (INR>3.0) orLDA plus VKA (INR range: 2–3).15 Some members of the TaskForce were of the opinion that LDA alone or VKA (INR range:2–3) would also be acceptable.
We have here analyzed 11 studies that recruited patientswith APS and arterial thrombosis and with separate outcomereporting for patients with index arterial thrombosis, withsome of the studies also including patients with venousthrombosis. In slight contrast tomost of the above-mentionedrecommendations, we found that combination therapy (VKAplus SAPT or DAPT) seems to provide better secondaryprophylactic effect than any single agent. Some interestingstudies were not included in this meta-analysis because theylacked a control group or used historical cohorts as a controlgroup such as the studies byRuiz-Irastorza et al41 andDerksenet al42 or because they did not specify thrombotic recurrencesaccording to the thrombotic index event (arterial or venousthrombosis) such as the WAPS study43 or the studies byTaraborelli et al,11 Khamashta et al,44 and Rosove et al.45
None of the guidelines or consensus statements providesuggestions or recommendations on duration of antithrom-botic therapy specifically for arterial thrombosis. There are,however, general recommendations to continue indefinitelyfor patients with definite APS and thrombosis (grade 1C),15
and that a decision to discontinue anticoagulation in patientswith APS should be taken at an expert center.17 We did notattempt to explore this question in our analysis.
Bleeding on Management of Arterial Thrombosis inAPS PatientsBleeding still remains a major concern of treatment with anyanticoagulant and obviously raises concerns when combinedantithrombotic therapy issuggested. TreatmentwithVKAhasahigh bleeding risk because of narrow therapeutic range, and alarge number of food and drug interactions. Several studieshave assessed the risk of bleeding in patients receiving VKA.46
Chai-Adisaksopha et al evaluated the risk of bleeding inpatients on NOACs, concluding that these were associatedwith less major bleeding, intracranial bleeding, clinicallyrelevant nonmajor bleeding (CRNMB), fatal bleeding, and totalbleeding than VKA (RR: 0.76, p<0.01) without an increase inthe riskofgastrointestinalbleeding.47►Table 4 shows the ratesof bleeding in the studies included in our review according tothedifferent regimensof treatment.Of the11studies analyzed,only eight studies evaluated bleeding episodes. Of these, sevenstudies reported major bleeding and one of them jointlyreported major bleeding and CRNMB.21 ►Fig. 6 shows theRRs for major bleeding according to the different treatmentscompared. As can be observed, there were no statisticallysignificant differences between the any of the treatmentsanalyzed.
Limitations
There are several limitations to our meta-analysis. First, thecriteria used for the diagnosis of APS varied with one study
using the Sapporo criteria, others the Sydney criteria, and thelargest study recruiting patients with only a single test foraPL.19 Second, several of the studies hadvery small numbers ofpatients in the different treatment groups resulting in highimprecision in the risk estimates. Third, we combined studieswith different designs and there was also heterogeneityregarding proportions of caseswith indexeventbeing a stroke,of triple positive cases, and of primary versus secondary APS.Fourth, for some pairs of treatment regimens there was onlyone study with estimable results and ideally a meta-analysisshould include results from at least four studies.
Conclusions
Arterial thrombosis is a common manifestation in patientswithAPSwith the incidence ranging from23 to 74%. Ischemicstroke is the most frequently studied arterial event. Inpatients with arterial thrombosis as first manifestation ofAPS, the recurrence is usually another arterial thrombosis.
Most studies report lower bleeding rates than recurrentthrombotic rates, probably because the included patientswith thrombotic events and APS are young with few comor-bidities and because of their hypercoagulable state.
It is difficult to give a strong recommendation regardingbest anticoagulant treatment in patients with arterialthrombosis as first manifestation of APS, due to the lowquality in several of the studies and the imprecision in therisk estimates. However, among all therapeutic regimensevaluated, it seems that the combined treatments with SAPTand VKA or with two antiplatelet agents might have betterefficacy and possibly without a reduction in safety. It wouldbe very interesting to see these two alternatives compared inawell-designed RCT. Such a RCT should test noninferiority ofDAPTversus VKA plus SAPT, since DAPT has the advantage ofeasier management.
FundingThis work was supported by a grant from Hospital Clinic,IDIBAPS and University of Barcelona (Estada Retribuïdaper ampliació d’estudis).
Conflict of InterestDr. Schulman reports research grants from Octapharmaand Boehringer-Ingelheim and honoraria from Alnylam,Bayer, Boehringer-Ingelheim, Bristol-Myers Squibb, Daii-chi-Sankyo, and Sanofi.
References1 Miyakis S, Lockshin MD, Atsumi T, et al. International consensus
statement on an update of the classification criteria for definiteantiphospholipid syndrome (APS). J Thromb Haemost 2006;4(02):295–306
2 Wilson WA, Gharavi AE, Koike T, et al. International consensusstatement on preliminary classification criteria for definite anti-phospholipid syndrome: report of an international workshop.Arthritis Rheum 1999;42(07):1309–1311
3 Duarte-García A, Pham MM, Crowson CS, et al. The epidemiologyof antiphospholipid syndrome: a population-based study. Arthri-tis Rheumatol 2019;71(09):1545–1552
Seminars in Thrombosis & Hemostasis Vol. 00 No. 0/2021 © 2021. Thieme. All rights reserved.
Arterial Thrombosis in Antiphospholipid Syndrome Aibar, Schulman 13

4 Hwang JJ, Shin SH, Kim YJ, et al. Epidemiology of antiphospholipidsyndrome in Korea: a nationwide population-based study. JKorean Med Sci 2020;35(05):e35
5 Kearon C, Parpia S, Spencer FA, et al. Antiphospholipid antibodiesand recurrent thrombosis after a first unprovoked venous throm-boembolism. Blood 2018;131(19):2151–2160
6 Tektonidou MG, Andreoli L, Limper M, et al. EULAR recommen-dations for the management of antiphospholipid syndrome inadults. Ann Rheum Dis 2019;78(10):1296–1304
7 Tektonidou MG, Ioannidis JPA, Boki KA, Vlachoyiannopoulos PG,Moutsopoulos HM. Prognostic factors and clustering of seriousclinical outcomes in antiphospholipid syndrome. QJM 2000;93(08):523–530
8 Dufrost V, Risse J, Reshetnyak T, et al. Increased riskof thrombosisin antiphospholipid syndrome patients treated with direct oralanticoagulants. Results from an international patient-level datameta-analysis. Autoimmun Rev 2018;17(10):1011–1021
9 Oku K, Amengual O, Yasuda S, Atsumi T. How to identify high-riskAPS patients: clinical utility and predictive values of validatedscores. Curr Rheumatol Rep 2017;19(08):51
10 Fujieda Y, Atsumi T, Amengual O, et al. Predominant prevalence ofarterial thrombosis in Japanese patients with antiphospholipidsyndrome. Lupus 2012;21(14):1506–1514
11 Taraborelli M, Reggia R, Dall’Ara F, et al. Longterm outcome ofpatients with primary antiphospholipid syndrome: a retrospec-tive multicenter study. J Rheumatol 2017;44(08):1165–1172
12 Pengo V, Ruffatti A, Legnani C, et al. Clinical course of high-riskpatients diagnosed with antiphospholipid syndrome. J ThrombHaemost 2010;8(02):237–242
13 Galli M, Luciani D, Bertolini G, Barbui T. Lupus anticoagulants arestronger risk factors for thrombosis than anticardiolipin anti-bodies in the antiphospholipid syndrome: a systematic review ofthe literature. Blood 2003;101(05):1827–1832
14 Schulman S, Svenungsson E, Granqvist SDuration of Anticoagu-lation Study Group. Anticardiolipin antibodies predict early re-currence of thromboembolism and death among patients withvenous thromboembolism following anticoagulant therapy. Am JMed 1998;104(04):332–338
15 Ruiz-Irastorza G, Cuadrado MJ, Ruiz-Arruza I, et al. Evidence-based recommendations for the prevention and long-term man-agement of thrombosis in antiphospholipid antibody-positivepatients: report of a task force at the 13th International Congresson antiphospholipid antibodies. Lupus 2011;20(02):206–218
16 Keeling D, Mackie I, Moore GW, Greer IA, Greaves MBritishCommittee for Standards in Haematology. Guidelines on theinvestigation and management of antiphospholipid syndrome.Br J Haematol 2012;157(01):47–58
17 Limper M, de Leeuw K, Lely AT, et al. Diagnosing and treatingantiphospholipid syndrome: a consensus paper. Neth JMed 2019;77(03):98–108
18 Jackson WG, Oromendia C, Unlu O, Erkan D, DeSancho MTAnti-phospholipid Syndrome Alliance for Clinical Trials and Interna-tional Networking. Recurrent thrombosis in patients withantiphospholipid antibodies and arterial thrombosis on antith-rombotic therapy. Blood Adv 2017;1(25):2320–2324
19 Levine SR, Brey RL, Tilley BC, et al; APASS Investigators. Anti-phospholipid antibodies and subsequent thrombo-occlusiveevents in patients with ischemic stroke. JAMA 2004;291(05):576–584
20 YamazakiM, Kadohira Y,MaekawaM, et al. Combined antiplateletagents might help prevent arterial thrombosis in antiphospholi-pid syndrome. J Thromb Haemost 2009;7(Suppl 2):720–721
21 Malec K, Broniatowska E, Undas A. Direct oral anticoagulants inpatients with antiphospholipid syndrome: a cohort study. Lupus2020;29(01):37–44
22 Jadad AR, Moore RA, Carroll D, et al. Assessing the quality ofreports of randomized clinical trials: is blinding necessary?Control Clin Trials 1996;17(01):1–12
23 Wells G, Shea B, O’Connell D, et al. The Newcastle-Ottawa Scale(NOS) for assessing the quality of nonrandomised studies inmeta-analyses. 2013. Accessed October 9, 2020 at: http://wwwohri-ca/programs/clinical_epidemiology/oxfordasp Q5Q5
Q5
24 Crowther Q6Q6Q6 MA, Ginsberg JS, Julian J, et al. A comparison of two
intensities of warfarin for the prevention of recurrent thrombosisin patients with the antiphospholipid antibody syndrome. N EnglJ Med 2003;349(12):1133–1138
25 Okuma H, Kitagawa Y, Yasuda T, Tokuoka K, Takagi S. Comparisonbetween single antiplatelet therapy and combination of anti-platelet and anticoagulation therapy for secondary prevention inischemic stroke patients with antiphospholipid syndrome. Int JMed Sci 2009;7(01):15–18
26 Arauz A, Roa LF, Hernandez B, et al. Aspirin versus anticoagulationin young patients with cerebral infarction secondary to primaryantiphospholipid syndrome [in Spanish]. Rev Neurol 2011;53(10):584–590
27 Pyo JY, Jung SM, Lee SW, Song JJ, Lee SK, Park YB. Subsequentthrombotic outcomes in patients with ischemic stroke withantiphospholipid antibody positivity. Yonsei Med J 2017;58(06):1128–1134
28 Ohnishi N, Fujieda Y, Hisada R, et al. Efficacy of dual antiplatelettherapy for preventing recurrence of arterial thrombosis inpatients with antiphospholipid syndrome. Rheumatology (Ox-ford) 2019;58(06):969–974
29 Pengo V, Denas G, Zoppellaro G, et al. Rivaroxaban vs warfarin inhigh-risk patients with antiphospholipid syndrome. Blood 2018;132(13):1365–1371
30 Ordi-Ros J, Sáez-Comet L, Pérez-Conesa M, et al. Rivaroxabanversus vitamin K antagonist in antiphospholipid syndrome: arandomized noninferiority trial. Ann Intern Med 2019;171(10):685–694
31 Pengo V, Banzato A, Bison E, Zoppellaro G, Padayattil Jose S, DenasG. Efficacy and safety of rivaroxaban vs warfarin in high-riskpatients with antiphospholipid syndrome: rationale and designof the Trial on Rivaroxaban in AntiPhospholipid Syndrome(TRAPS) trial. Lupus 2016;25(03):301–306
32 Cervera R, Piette JC, Font J, et al; Euro-Phospholipid Project Group.Antiphospholipid syndrome: clinical and immunologic manifes-tations and patterns of disease expression in a cohort of 1,000patients. Arthritis Rheum 2002;46(04):1019–1027
33 Cervera R, Boffa MC, Khamashta MA, Hughes GRV. The Euro-Phospholipid project: epidemiology of the antiphospholipid syn-drome in Europe. Lupus 2009;18(10):889–893
34 Ricarte IF, Dutra LA, Abrantes FF, et al. Neurologic manifestationsof antiphospholipid syndrome. Lupus 2018;27(09):1404–1414
35 Uthman I, Noureldine MHA, Ruiz-Irastorza G, Khamashta M.Management of antiphospholipid syndrome. Ann Rheum Dis2019;78(02):155–161
36 Soltész P, Veres K, Lakos G, Kiss E, Muszbek L, Szegedi G. Evaluationof clinical and laboratory features of antiphospholipid syndrome: aretrospective study of 637 patients. Lupus 2003;12(04):302–307
37 Kearon C, Akl EA, Ornelas J, et al. Antithrombotic therapy for VTEdisease: CHEST guideline and expert panel report. Chest 2016;149(02):315–352
38 Cuadrado MJ, Bertolaccini ML, Seed PT, et al. Low-dose aspirin vslow-dose aspirin plus low-intensity warfarin in thromboprophy-laxis: a prospective, multicentre, randomized, open, controlledtrial in patients positive for antiphospholipid antibodies (ALIWA-PAS). Rheumatology (Oxford) 2014;53(02):275–284
39 Verro P, Levine SR, Tietjen GE. Cerebrovascular ischemic eventswith high positive anticardiolipin antibodies. Stroke 1998;29(11):2245–2253
40 Wang CR, Liu MF. Rituximab usage in systemic lupus erythema-tosus-associated antiphospholipid syndrome: a single-centerexperience. Semin Arthritis Rheum 2016;46(01):102–108
41 Ruiz-Irastorza G, Khamashta MA, Hunt BJ, Escudero A, CuadradoMJ, Hughes GRV. Bleeding and recurrent thrombosis in definite
Seminars in Thrombosis & Hemostasis Vol. 00 No. 0/2021 © 2021. Thieme. All rights reserved.
Arterial Thrombosis in Antiphospholipid Syndrome Aibar, Schulman14

antiphospholipid syndrome: analysis of a series of 66 patientstreated with oral anticoagulation to a target international nor-malized ratio of 3.5. Arch Intern Med 2002;162(10):1164–1169
42 Derksen RH, de Groot PG, Kappelle LJ. Low dose aspirin afterischemic stroke associated with antiphospholipid syndrome.Neurology 2003;61(01):111–114
43 FinazziG,Marchioli R, BrancaccioV, et al. A randomized clinical trial ofhigh-intensity warfarin vs. conventional antithrombotic therapy forthe prevention of recurrent thrombosis in patientswith the antiphos-pholipid syndrome (WAPS). J Thromb Haemost 2005;3(05):848–853
44 Khamashta MA, Cuadrado MJ, Mujic F, Taub NA, Hunt BJ, HughesGR. The management of thrombosis in the antiphospholipid-antibody syndrome. N Engl J Med 1995;332(15):993–997
45 Rosove MH, Brewer PMC. Antiphospholipid thrombosis: clinicalcourse after the first thrombotic event in 70 patients. Ann InternMed 1992;117(04):303–308
46 Lopes LC, Spencer FA, Neumann I, et al. Bleeding risk in atrialfibrillation patients taking vitamin K antagonists: systematicreview and meta-analysis. Clin Pharmacol Ther 2013;94(03):367–375
47 Chai-Adisaksopha C, CrowtherM, IsayamaT, LimW. The impact ofbleeding complications in patients receiving target-specific oralanticoagulants: a systematic review and meta-analysis. Blood2014;124(15):2450–2458
Seminars in Thrombosis & Hemostasis Vol. 00 No. 0/2021 © 2021. Thieme. All rights reserved.
Arterial Thrombosis in Antiphospholipid Syndrome Aibar, Schulman 15


![Case Report Lower Limb Ischemia: Aortoiliac Thrombosis Related to Antiphospholipid ... · 2019. 7. 31. · CaseReportsinSurgery ndings in patients, Radiology ,vol. ,no., pp. ,. []A.Ru](https://img.pdfslide.us/doc/110x75/60b93438547c9430b3265add/case-report-lower-limb-ischemia-aortoiliac-thrombosis-related-to-antiphospholipid.jpg)










![Hematological Malignancies and Arterial Thromboembolism · thrombosis in ET has been predicted by thrombosis history, older age, cardiovascular risk factors and JAK2V617F [37]. Extreme](https://img.pdfslide.us/doc/110x75/5e8e8e6f639a7b2284701bf6/hematological-malignancies-and-arterial-thromboembolism-thrombosis-in-et-has-been.jpg)