Embed Size (px)
Citation preview
Extern conference
A 1-year-3-month-old boy
presented with generalized edema
for 1 month
20 December 2007
History A 1-year-3month-old boyChief complaint :
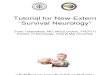
Generalized edema for 1 month
Present history: He was no underlying disease.1 month PTA, his mother noticed that her
child had enlarged abdomen and edema of both feet and ankles. The patient’s body weight increased 4 kg in 2mo.
History- Normal urination and defecation, no gross
hematuria- No previous history of fever, cough, sore
throat and skin infection- No rash, no arthralgia - No dyspnea, no orthopnea- No chronic diarrhea
History Past history
Caesarean section due to previous C/Sbirth weight 2616 gm, Apgar score 9,10
Family historyNo history of kidney disease in family
Nutritional statusSolid food 3 feedsPowdered milk 8 oz 3 feeds per day
Drugs and immunizationNo history of drug allergyNo routine drug use
ImmunizationUp to date
Developmental historySay some words and walk
History
Physical Examination Vital signs : T 36.9 C, PR140/min,
BP 99/72 mmHg, RR 32/min GA : 1 3/12-year-Thai boy, uncooperative, not
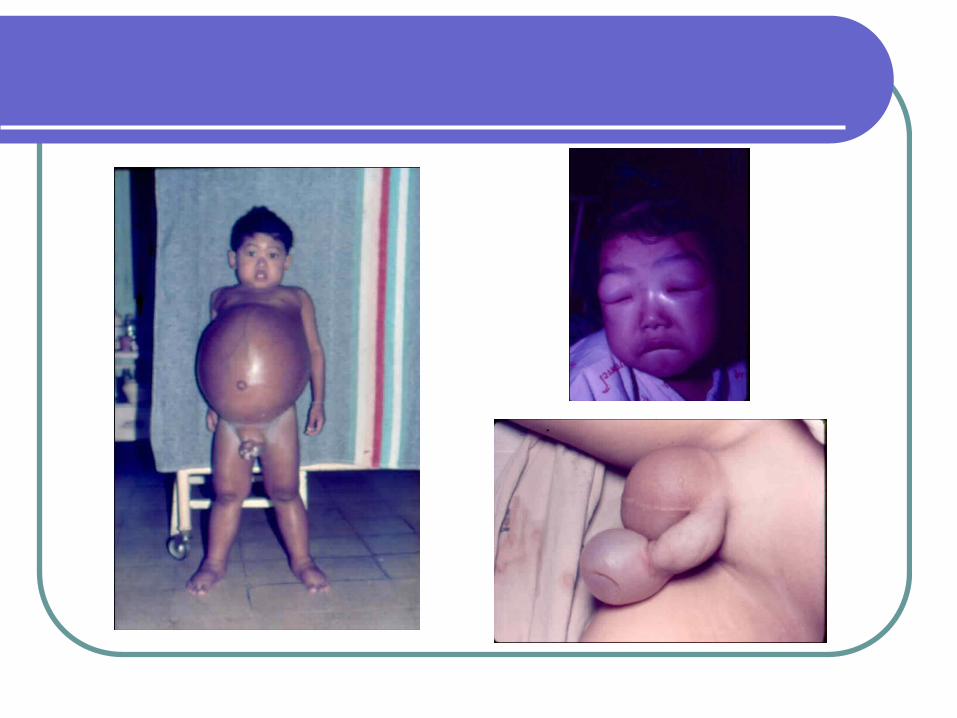
pale, no jaundice, no dyspnea, no cyanosis, puffy eye lids, generalized pitting edema 1+
Ht 80 cm (P50-75), BW 11 kg (P50-75), HC 46 cm (P25-50), Abdominal circumference 49 cm
HEENT : no dental caries
no injected pharynx and tonsils Lungs : clear CVS : normal S1 and S2, no murmur Abdomen : soft, not tender, liver and spleen not
palpable, no palpable mass, mild ascites, bowel sound active
KUB: CVA-not tender, bimanual palpation-negative Genitalia: scrotal edema Others: unremarkable
Physical Examination
PROBLEM LIST
Generalized pitting edema for 1 month
Weight gain 4 kg in 2 months
Generalized edema Nephrotic syndromeAcute or chronic glomerulonephritisCongestive heart failureProtein losing enteropathyProtein malnutrition
DIFFERENTIAL DIAGNOSIS
Nephrotic syndrome
PROVISIONAL DIAGNOSIS
Characteristic features of nephrotic syndrome
1.Generalized pitting edema 2.Hypoalbuminemia (≤2.5g/dl)3.Hypercholesterolemia (≥250g/dl)4.Heavy proteinuria (≥40 mg/m²/hr)
Question 1
“What is the initial investigation
in this patient?”
INVESTIGATIONS AT INITIAL PRESENTATION
Complete blood countRenal profiles, urinalysis and quantification
for urinary protein excretionSerum albuminLipid profiles
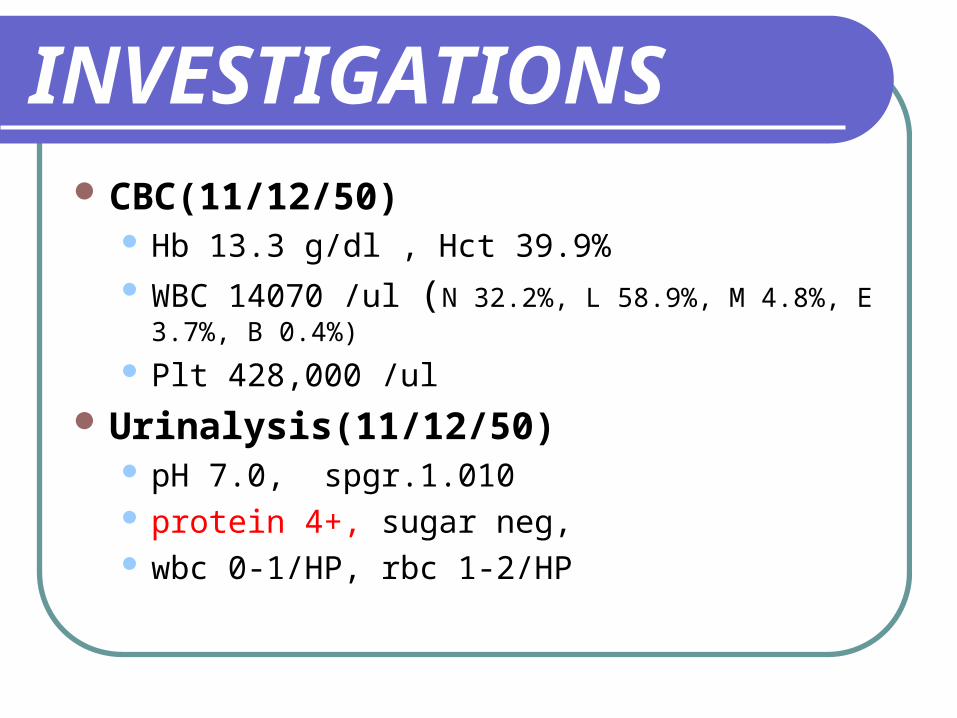
INVESTIGATIONS CBC(11/12/50)
Hb 13.3 g/dl , Hct 39.9% WBC 14070 /ul (N 32.2%, L 58.9%, M 4.8%, E 3.7%, B
0.4%)
Plt 428,000 /ul
Urinalysis(11/12/50) pH 7.0, spgr.1.010 protein 4+, sugar neg, wbc 0-1/HP, rbc 1-2/HP
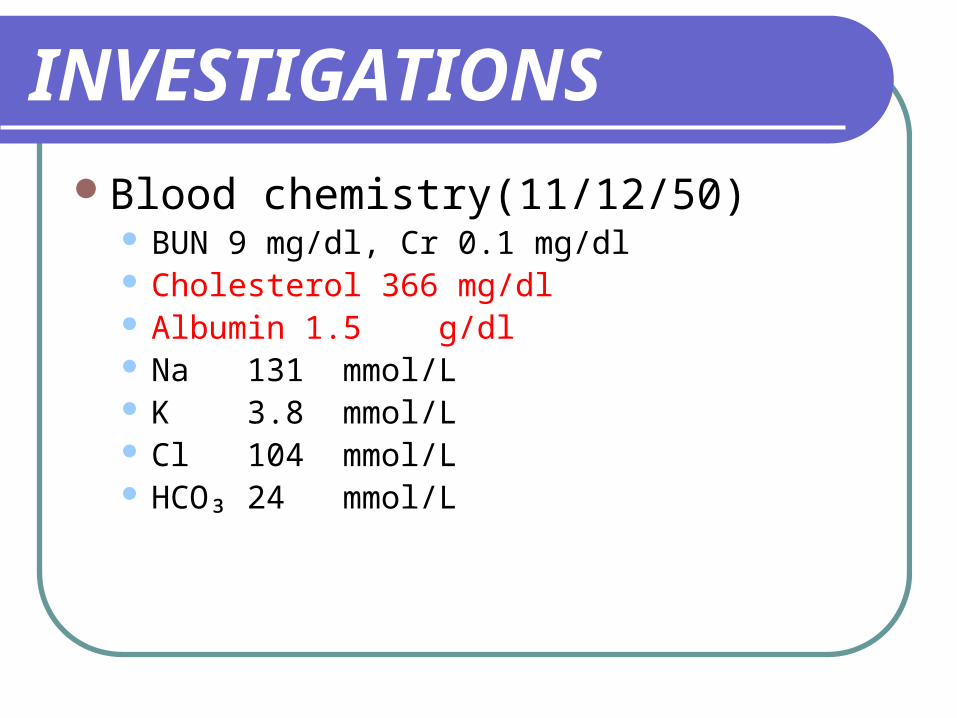
Blood chemistry(11/12/50) BUN 9 mg/dl, Cr 0.1 mg/dl Cholesterol 366 mg/dl Albumin 1.5 g/dl Na 131 mmol/L K 3.8 mmol/L Cl 104 mmol/L HCO₃ 24 mmol/L
INVESTIGATIONS
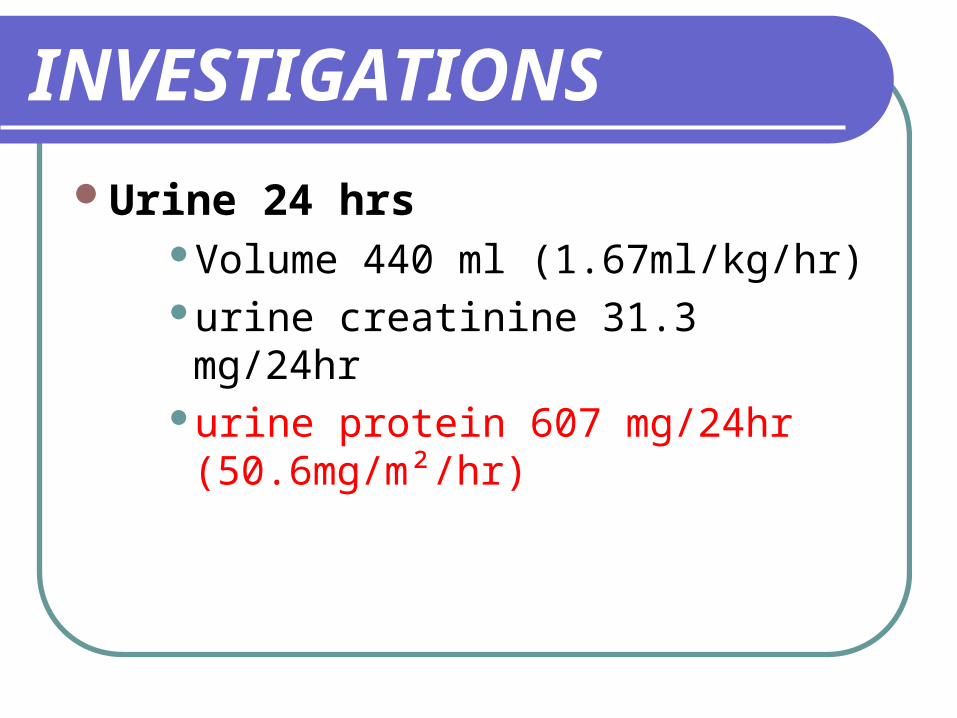
Urine 24 hrsVolume 440 ml (1.67ml/kg/hr)urine creatinine 31.3 mg/24hrurine protein 607 mg/24hr
(50.6mg/m²/hr)
INVESTIGATIONS
Diagnosis
Nephrotic syndrome
Types of nephrotic syndrome
Primary nephrotic syndrome(90%)
Secondary nephrotic syndrome(10%)
Nephrotic syndrome
Primary nephrotic syndrome(90%)Most common at age 2-6 yr
(6 mo. patient has been reported)Male : female = 2 : 1
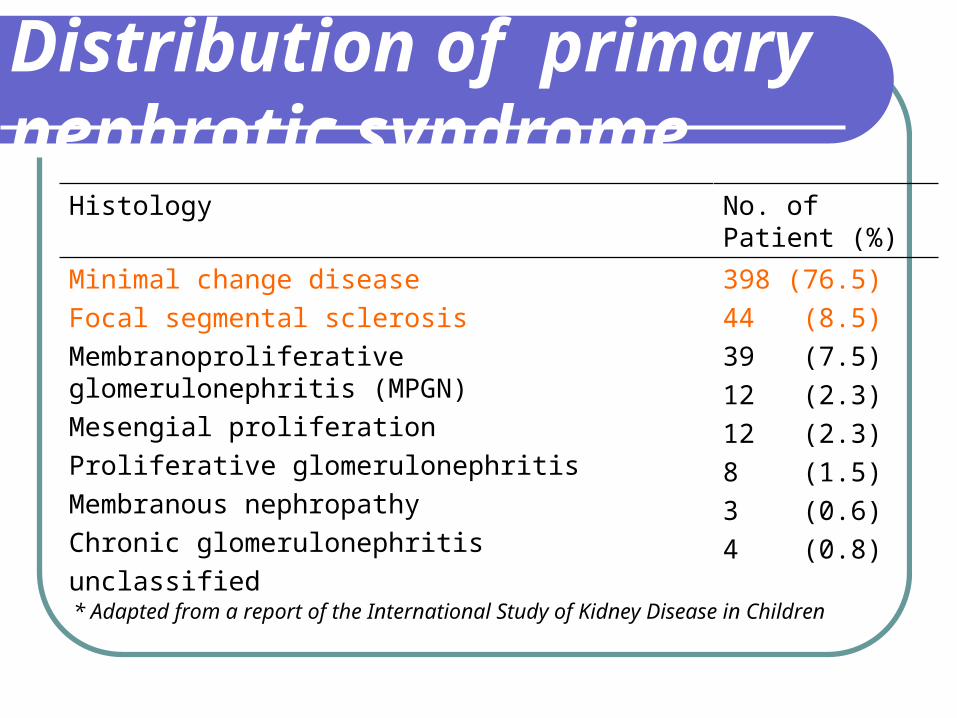
Distribution of primary nephrotic syndrome
Histology No. of Patient (%)
Minimal change disease
Focal segmental sclerosis
Membranoproliferative glomerulonephritis (MPGN)
Mesengial proliferation
Proliferative glomerulonephritis
Membranous nephropathy
Chronic glomerulonephritis
unclassified
398 (76.5)
44 (8.5)
39 (7.5)
12 (2.3)
12 (2.3)
8 (1.5)
3 (0.6)
4 (0.8)
* Adapted from a report of the International Study of Kidney Disease in Children
Nephrotic syndrome
Secondary nephrotic syndrome(10%) Suspected in
Age>8 yrsHypertension HematuriaRenal dysfunctionExtrarenal symptoms (rash, arthralgia, fever)
Secondary nephrotic syndromeCauses
InfectionsDrugs Immunologic or allergic disordersMalignant diseaseGlomerular hyperfiltration
In this patientPrimary nephrotic syndrome
More common (90%)Lower age groupMaleNo clinical suspection of secondary
nephrotic syndrome
ManagementGeneral
Low salt, normal protein for age dietSalt poor albumin/diuretic if indicatedClear infectionEducation Immunization
ManagementSpecific
PrednisoloneCyclophosphamide Cyclosporin Levamisole
Indications for renal biopsy
Pretreatment Macroscopic hematuria Persistent hypertension and microscopic
hematuriaRenal failure not attributable to hypovolemiaLow plasma C3Onset age < 6 months
Before start steroid therapy
Complete physical examinationCXR, PPD skin testStool conc. for parasiteDental exam
In this patientComplete physical examinationCXR: no infiltrationPPD skin test: negativeStool conc. for parasite: not found 3 daysDental exam: no dental caries
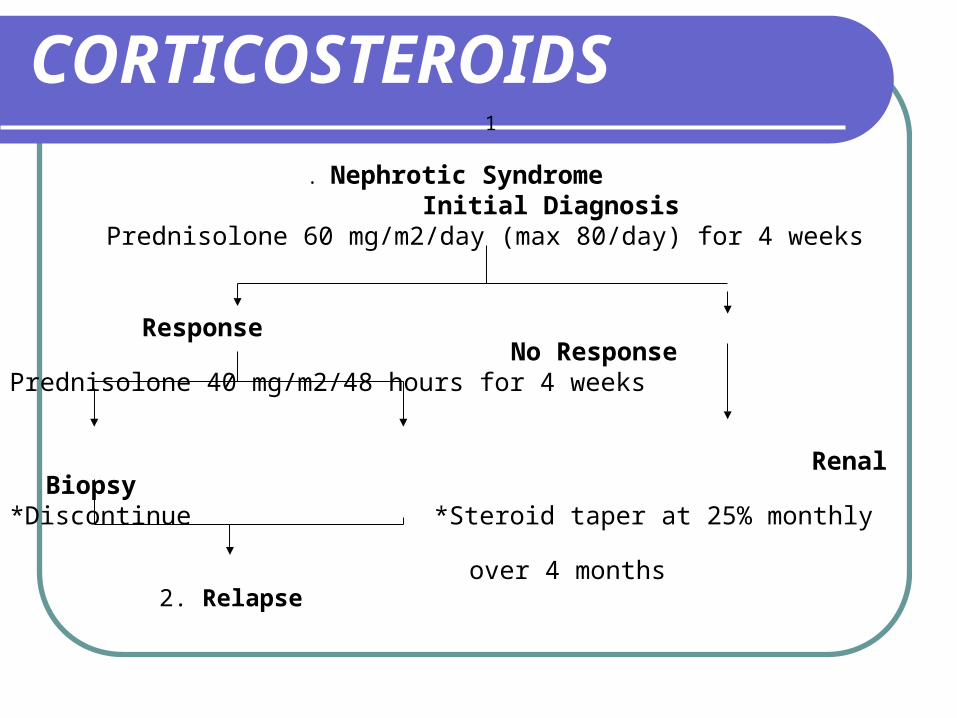
CORTICOSTEROIDS 1
. Nephrotic Syndrome Initial Diagnosis
Prednisolone 60 mg/m2/day (max 80/day) for 4 weeks
Response No ResponsePrednisolone 40 mg/m2/48 hours for 4 weeks
Renal
Biopsy*Discontinue *Steroid taper at 25% monthly
over 4 months
2. Relapse
Progression
Admit 11-14/12/50V/S stableBW 11 – 11.1 kgBalanced I/O
Discharge14/12/50Home med
Prednisolone[5] 4 tab oral OD pcFollow up
OPD 2 weeks with urinalysis
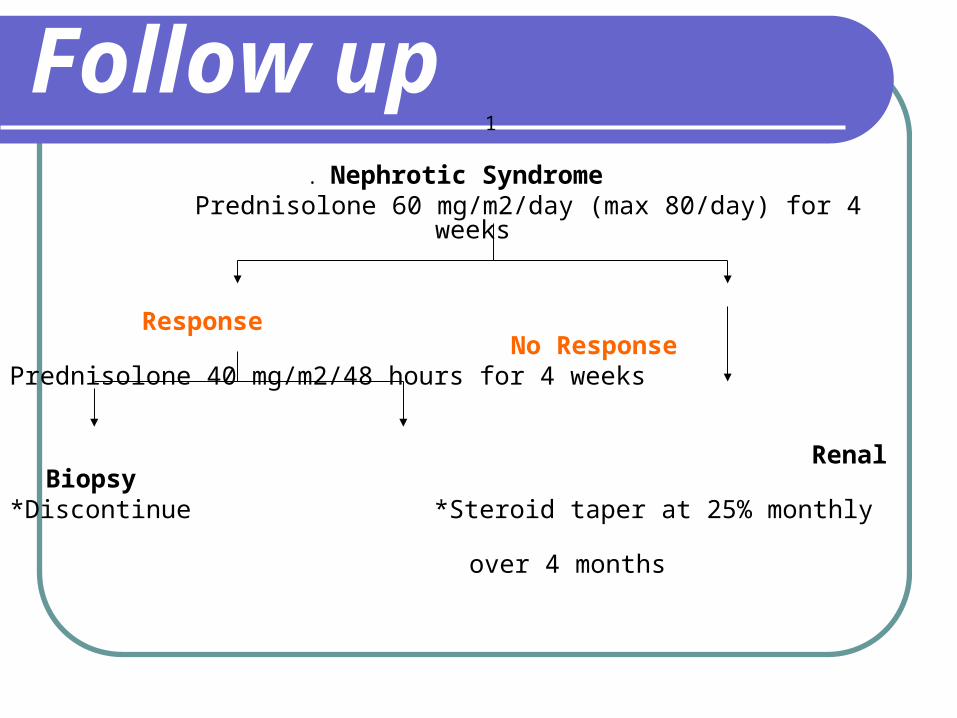
Follow up 1
. Nephrotic Syndrome Prednisolone 60 mg/m2/day (max 80/day) for 4 weeks
Response No ResponsePrednisolone 40 mg/m2/48 hours for 4 weeks
Renal
Biopsy*Discontinue *Steroid taper at 25% monthly
over 4 months
INDICATIONS FOR RENAL BIOPSY
Steroid resistantSteroid dependenceFrequent relapse
Definitions REMISSION:
Urinary protein excretion < 4 mg/m2/hour or urine dipstix nil/trace for 3 consecutive days.
RELAPSE: Urinary protein excretion > 40 mg/m2/hour or urine dipstix ++ or more for 3 consecutive days.
FREQUENT RELAPSES: Two or more relapses within 6 months of initial response or four or more relapses within any 12 month period.
Definitions STEROID DEPENDENCE:
Two consecutive relapses occurring during the period of steroid taper or within 14 days of its cessation.
STEROID RESISTANCE: Failure to achieve remission in spite of 4 weeks of
standard prednisolone therapy
Question 2
‘What will you advice the
patient’s caregiver ?”
PrognosisThe prognosis depends on the cause of
nephrotic syndrome. It is usually good in children.Minimal change disease responds very well
to steroids and does not cause chronic renal failure.
Focal segmental glomerulosclerosis frequently lead to end stage renal disease.
Prognosis Children who present with hematuria and
hypertension are more likely to be steroid resistant
Poor patient response to steroid therapy seems to be the finding most predictive of a poor outcome
Frequent relapses are more common with
young age of onset and in boys.
Patient Education
Nephrotic syndrome is a chronic illness characterized by relapses and remissions
Ensure normal activity and school attendance.
Infections are an important cause of morbidity and mortality
Patient Education
Live vaccines can be administered 6 weeks after cessation of corticosteroid therapy.
Peer support and psychological counseling are important.






![Uveitic macular edema: a stepladder treatment paradigm€¦ · of macular edema [1,3–4], this review will focus on uveitic macular edema specifically. Uveitic macular edema Macular](https://img.pdfslide.us/doc/110x75/5ed770e44d676a3f4a7efe51/uveitic-macular-edema-a-stepladder-treatment-paradigm-of-macular-edema-13a4.jpg)