Embed Size (px)
Citation preview

Poster Design & Printing by Genigraphics® - 800.790.4001
Evaluation of Keros Score in Patients with Congenital AnosmiaEvaluation of Keros Score in Patients with Congenital Anosmia
Katherine Johnson, MD1; Derick Leight, MD2; Josh Wood1; Fang Qiu1; Donald Leopold, MD1
1University of Nebraska Medical Center, Omaha, NE 2Boystown National Research Hospital, Omaha, NE
INTRODUCTION DISCUSSIONRESULTS
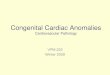
Figure 1. Olfactory Fossa Height MeasurementA-B= Olfactory Fossa Height
ABSTRACT
Objectives:1.Identify features of Kallman’s
syndrome2. Describe olfactory embryologic development3. Describe the Keros classification4. Recognize significance of olfactory fossa height and congenital anosmia
Study Design:Retrospective chart review
Methods:Review of CT or MRI with
measurement of olfactory cleft height
Results:Patients with congenital
anosmia had a flat olfactory cleft (low Keros score) when compared to normal controls
Conclusions:Patients with flat olfactory clefts noted on imaging may also suffer from olfactory dysfunction
• Total number of participants: 104•Control: 57: Smell Disturbances: 47 subjects
• Smell disturbance etiologies:Post Head Trauma (13%)Congenital (10%)
• 2 patients with Kallmann’s SyndromePost Upper Respiratory Infection (URI) (23%)Rhinosinusitis (13%)Other/Unknown (40%)
• No differences between men and women• Congenital had a statistically significant younger
age group• Comparisons were made separately for right and
left nasal passageways• Lower olfactory fossa height in congenital anosmia
vs. controls• Left side: 2.24mm less in congenital vs. control
(p<0.0001) (see figure 2)• Right side: 0.95mm less in congenital vs. control
(p<0.004) (see figure 3)
Study Design• Retrospective chart review• Study participants: rhinology patients with
diagnosis of taste and smell disturbances (ICD-9 781.1), CT or MRI scan on file
• Etiology of smell disturbance recorded• Control patients: CT or MRI on file without
opacity on scan• CT/MRI reviewed and olfactory fossa height recorded to nearest 100th of an inch
• See Figure I (A-B = Fossa Height)• Aquarius NetViewer Software package used
Study Aims• Compare olfactory fossa heights in participants with smell disturbance to control participants
Statistical Analysis• Kruskal Wallis test was used to determine difference in cleft heights between etiology groups
A flat olfactory cleft on imaging should raise suspicion for congenital anosmia.
Permanent sense of smell loss is an uncommon complaint for Americans. Approximately 2 million people estimated to suffer from permanent disturbances. Olfactory ability is also known to diminish with age.
Etiology of Olfactory Loss• Transport: Physical barriers to transmission
• Nasal polyposis• Neural: Damaged or absent olfactory neurons
• Kallmann’s Syndrome, head trauma• Sensory: Damage to the olfactory
neuroepithelium.•Post-URI, post radiation therapy
Embryology of the Olfactory System• Development begins at 24 days’ gestation• Olfactory epithelium visible at 28 days
• Cell axons grow into telencephalon• Ethmoid bone ossifies around axons,
forming cribriform plate• Axonal growth relies on GnRH
GnRH and Olfactory Development• Travel from nasal epithelium into anterior pituitary• Cytokines (FBGF) direct GnRH migration• Kallmann Syndrome: absence of GnRH
• Hypogonadism, congenital anosmia, and lack of olfactory bulbs• Olfactory neuroepithelium is rudimentary vs. normal controls
Keros Classification• Olfactory cleft defined by roof of ethmoid and lateral lamella of cribriform plate (see figure 1)• Depth of fossa described by Keros in 1964
• Type I: <3mm; Type II: 4-7mm; Type III: >8mm
• Keros score not previously correlated with smell disturbances
METHODS
1 Ciofalo, A., Filiaci, F., Romeo, R., & Zambetti, G. (2006). Epidemiological aspects of olfactory dysfunction. Rhinology, 44(1), 78-82.
2 Boyce, J., & Shone, G. (2006). Effects of ageing on smell and taste. British Medical Journal, 82, 239-241.
3 Galle, S., Gouweloos, J., & de Haan, A. (2009). Sense of smell disorder and health-related quality of life. Rehabilitation Psychology, 54(4), 404-412.
4 Bhattacharyya S, B. M. (2008). Competence, specification and commitment to an olfactory placode fate. Development, 134(24), 4165-74.
5 Wray, S. (2010). From nose to brain: Development of gonadotrophin-releasing hormone-1 neurons. Journal of Neuroendocrinology, 22, 743-753.
6 Kanaho Y, Enomoto M, Endo D, Maehiro S, Park MK, Murakami S. (2009). Neurotrophic effect of gonadotropin-releasing hormone on neurite extension and neuronal migration of embryonic gonadotropin-releasing hormone neurons in chick olfactory nerve bundle culture. J Neurosci Res, 87(10), 2237-44.
7 Kim HG, Bhagavath B, Layman LC. Clinical manifestations of impaired GnRH neuron development and function. Neurosignals, 16(2), 165-82.
8 Schwob, J., Leopold, D., Mieleszko Szumowski, K., & Emko, P. (1993). Histopathology of olfactory mucosa in kallmann's syndrome. Annals of Otology, Rhinology, and Laryngology, 102(2), 117-122.
9 Keros P. On the practical value of differences in the level of the lamina cribrosa of the ethmoid. ZLaryngol Rhinol Otol. 1962;41:809–13. (German)
10Quinton R, Duke VM, de Zoysa PA, Platts AD, Valentine A, Kendall B, Pickman S, Kirk JM, Besser GM, Jacobs HS, Bouloux PM. (1996). The neuroradiology of kallmann's syndrome: A genotypic and phenotypic analysis. J Clin Endocrinol Metab., 81(8), 3010-3017.
11 Abolmaali, N., Hietschold, V., Vogl, T., Huttenbrink, K., & Hummel, T. (2002). MR evaluation in patients with isolated anosmia since birth or early childhood. American Journal of Neuroradiology, 157, 157-163.
12Qiuyi Qu, Jianfeng Liu, Daofeng Ni, Qiuhang Zhang, Dazhang Yang, Naya Wang, et al. (2010). Diagnosis and clinical characteristics of congenital anosmia: Case series report. Journal of Otolaryngology-Head & Neck Surgery, 39(6), 723-731.
13Assouline S, Shevell MI, Zatorre RJ, Jones-Gotman M, Schloss MD, Oudjhane K. (1998). Children who can't smell the coffee: Isolated congenital anosmia. J Child Neurol., 13(4), 168-72.
CONCLUSIONS
REFERENCES
Katherine Johnson, MDUniversity of Nebraska Medical CenterEmail: [email protected]: 402-559-7777Website: www.unmc.edu/ent
CONTACT
AB
• Goal of study: evaluate olfactory fossa height(Keros score) in patients with olfactory disturbances
• Unexpected finding: patients with congenital anosmia had lower olfactory cleft (Keros Type I) vs. normal controls
Embryology and Flat Olfactory Cleft • Embryologic etiology not fully understood• Olfactory epithelium, cribriform plate, and
olfactory bulb development rely on normal GnRH function
Congenital Anosmia (CI)•Defined as inability to detect odors from birth
•Diagnosis often unrecognized•Can occur isolated or with other syndromes
• Kallmann Syndrome most widely known• Diagnosis of CI
• History of life-long smell loss• Elimination of other causes• Evaluate for lack of puberty to consider
Kallmann diagnosis
Figure 2: Left Nostril Mean Olfactory Fossa Height
Figure 3: Right Nostril Mean Olfactory Fossa Height











![Anosmia and ageusia: common findings in COVID‐19 patients and ageusia... · Anosmia has already been reported in the course of severe acute respiratory syndrome (SARS) [2] and other](https://img.pdfslide.us/doc/110x75/5f5db0cfe6b3ba6b26757b86/anosmia-and-ageusia-common-findings-in-covida19-and-ageusia-anosmia-has.jpg)