Embed Size (px)
Citation preview
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
MIPS Molecular Imaging Program at Stanford
Stanford University School of Medicine
Department of Radiology
Andrei Iagaru, MD
Evaluation of Infection/Inflammation: What is the Role of PET/CT?
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
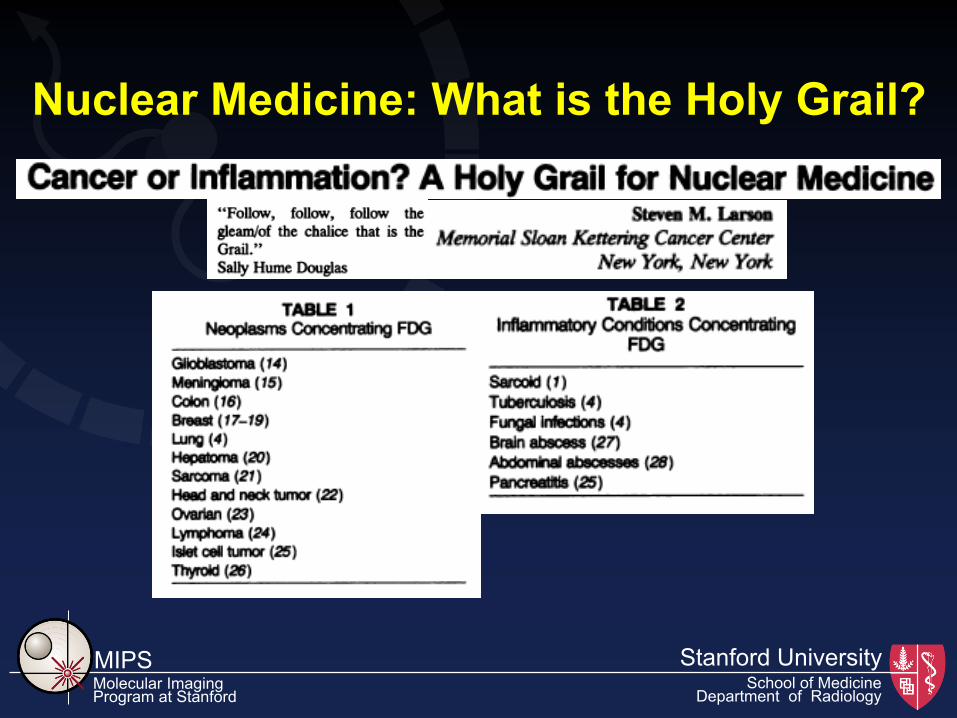
Holy Grail: Ø The dish, plate or cup used by Jesus Christ at the Last
Supper, said to possess miraculous powers Ø Later became the object of many chivalrous quests
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
Nuclear Medicine: What is the Holy Grail?
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
PET/CT in Infection/Inflammation
ü 18F FDG labeled WBC’s vs. 18F FDG
ü Applications of 18F FDG PET/CT in infection and/or inflammation: Ø Fever of unknown origin
Ø Prosthesis evaluation
Ø Chronic osteomyelitis
Ø Diabetic foot
Ø Vasculitidies
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
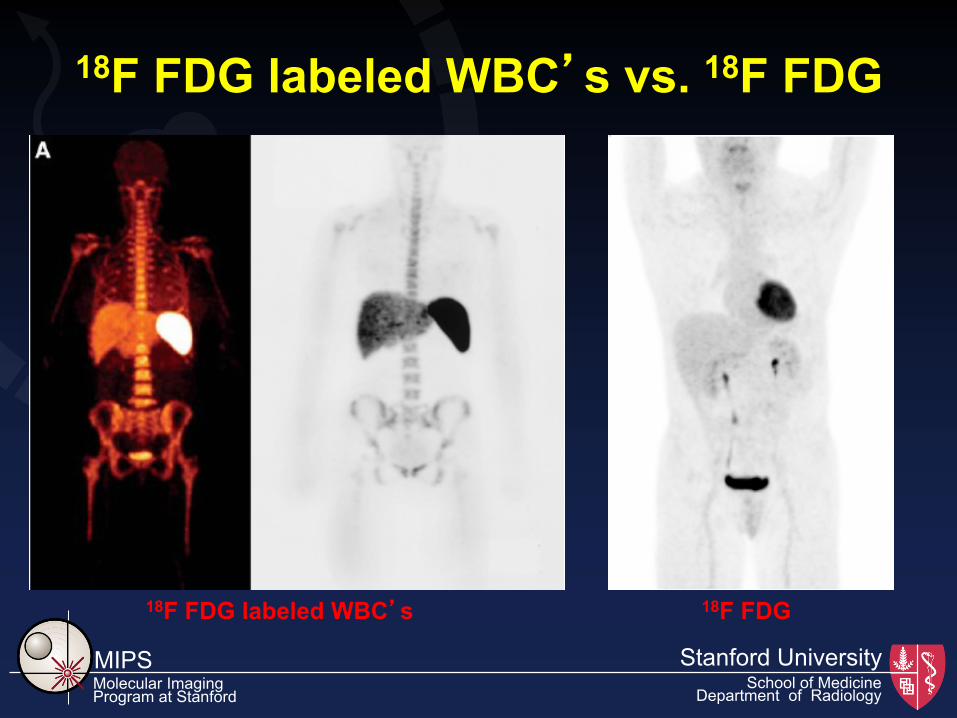
18F FDG labeled WBC’s vs. 18F FDG
18F FDG labeled WBC’s 18F FDG
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
18F FDG labeled WBC’s vs. 18F FDG
ü Specificity
ü Risks associated with labeling
ü Imaging at 3-5 hours…enough for WBC localization???
ü How stable is the labeling
ü Cost
ü Non-specificity
ü Can something (i.e., FDG) be good for everything???
ü Cost
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
ü 4 normal adult volunteers
ü WBC’s can be readily labeled with 18F FDG
ü Labeled WBC’s show reasonable stability in vivo for several hours after injection
ü Dosimetry data similar to 111In labeled WBC’s
ü Good quality PET images can be obtained up to 6 hours after injection
ü No GI uptake was appreciated on any of the scans
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
ü 21 patients (8 women, 13 men), 24-84 years-old (mean: 56)
ü Inclusion criteria: suspected infection and FUO
ü Exclusion criteria: WBC<2000, favorable response to antibiotics, preganancy, age<18 years
ü Results: median labeling efficiency 80% (24-96%; mean 75%) and mean labeling stability 90%
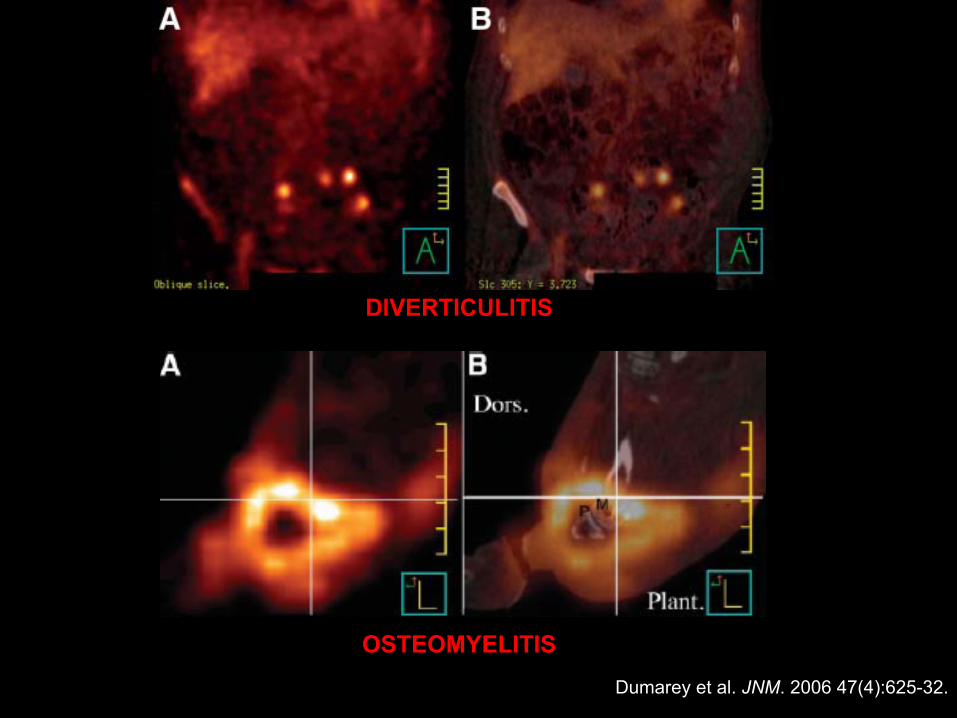
Dumarey et al. JNM. 2006 47(4):625-32.
DIVERTICULITIS
OSTEOMYELITIS
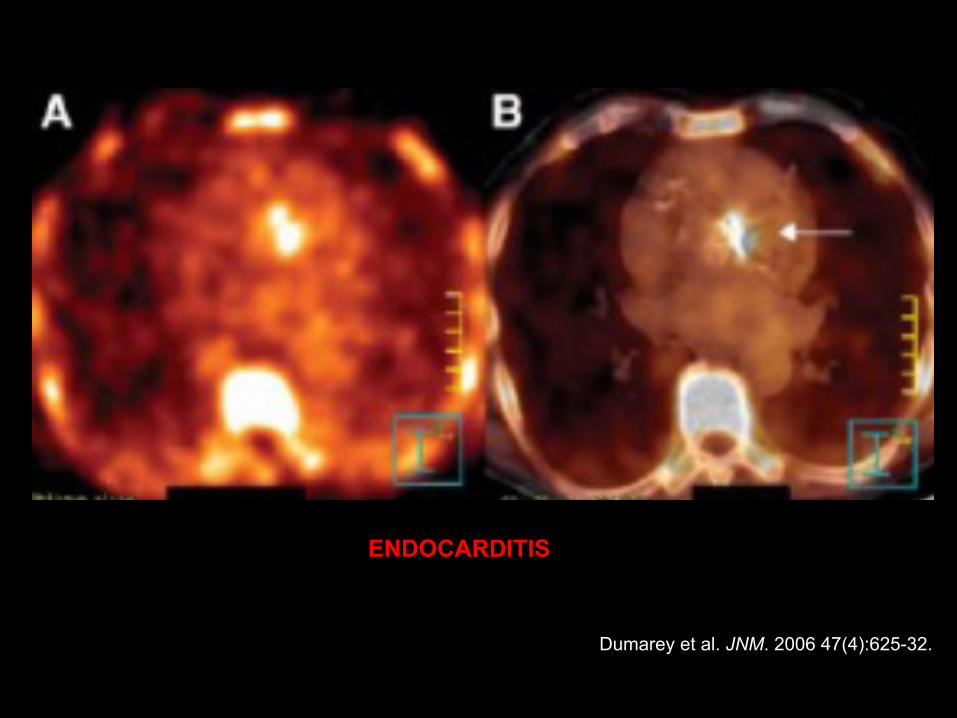
Dumarey et al. JNM. 2006 47(4):625-32.
ENDOCARDITIS
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
ü 51 patients (26 women, 25 men), 32-86 years-old (mean: 59)
ü 8 subjects excluded: inadequate 18F labeling (6), camera malfunction (1), non-cooperant (1)
ü Labeling efficiency 72% for 18F vs. 90% for 111In (P < 0.001)
ü WBC’s viability of 98% for 18F vs. 97% for 111In
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
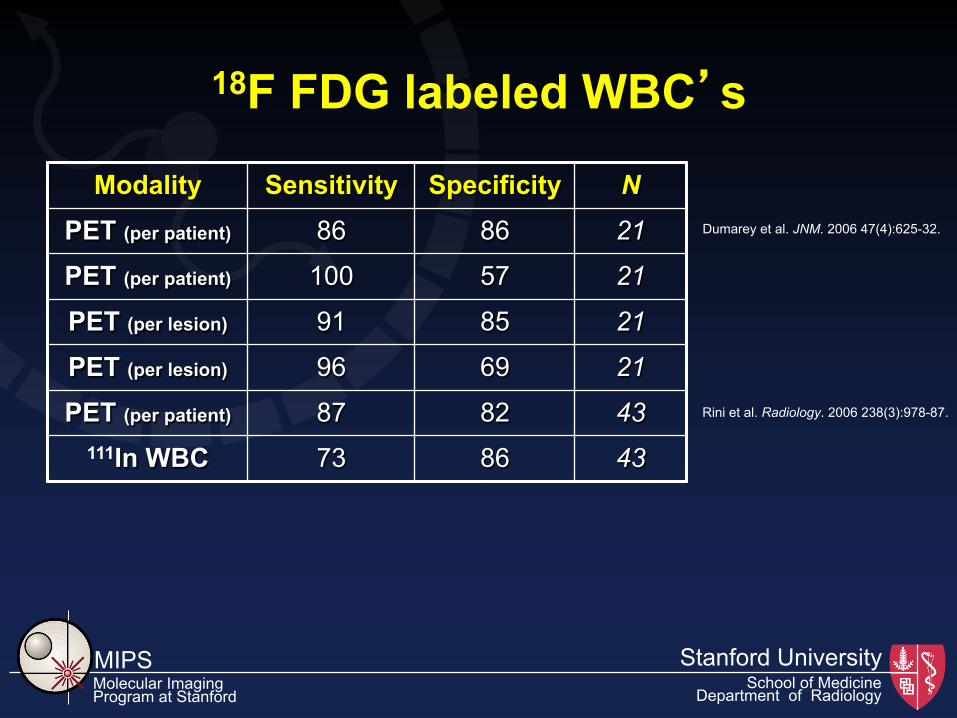
Modality Sensitivity Specificity N PET (per patient) 86 86 21
PET (per patient) 100 57 21
PET (per lesion) 91 85 21
PET (per lesion) 96 69 21
PET (per patient) 87 82 43 111In WBC 73 86 43
18F FDG labeled WBC’s
Dumarey et al. JNM. 2006 47(4):625-32.
Rini et al. Radiology. 2006 238(3):978-87.
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
18F FDG PET/CT in FUO Definition:
a) Petersdorf and Beeson (1961)
Ø recurrent fever of 38.3 or higher
Ø lasting 2-3 weeks or longer
Ø undiagnosed after 1 week of hospital evaluation (revised: after appropriate outpatient or inpatient evaluation)
b) Durack and Street (1991)
Ø classic FUO in non-immunocompromised patients
Ø nosocomial FUO
Ø neutropenic FUO
Ø FUO associated with HIV infection
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
Sources of FUO ü Infections: 13-43%
ü Autoimmune/colagen vascular disease/neoplasm: up to 54%
ü Unknown: 10-40%
67Ga citrate whole-body scan
18F FDG PET/CT
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
ü 19 patients underwent 111In WBC scan and 18F FDG PET within 1 week
ü Inclusion criteria: documented FUO
ü Exclusion criteria: preganancy, age<18 years
ü Results:
Ø final diagnosis in 12/19 cases
Ø 7 cases: infection/inflammation
Ø 1 case: neoplasm
Ø 4 cases: autoimmune disease
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
ü 35 patients underwent 18F FDG PET
ü Inclusion criteria: documented FUO
ü Exclusion criteria: preganancy, age<18 years
ü Results:
Ø final diagnosis in 19/35 cases
Ø 6 cases: infection
Ø 4 cases: neoplasm
Ø 6 cases: inflammation
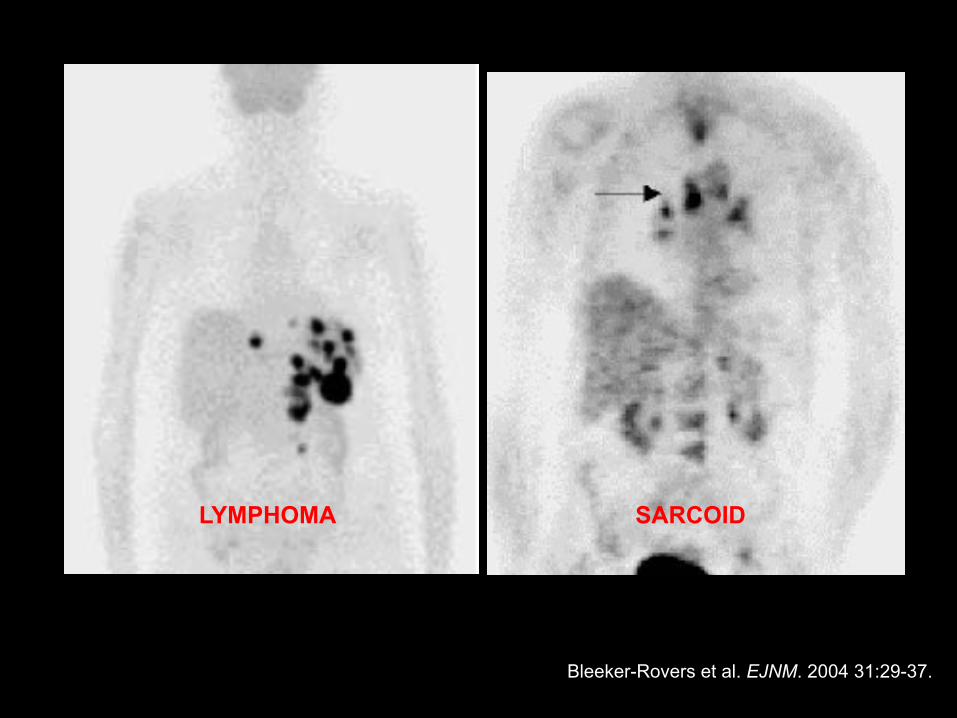
Bleeker-Rovers et al. EJNM. 2004 31:29-37.
LYMPHOMA SARCOID
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
ü 16 patients underwent 18F FDG PET
ü Inclusion criteria: documented FUO
ü Exclusion criteria: preganancy, age<18 years
ü Results:
Ø final diagnosis in 11/16 cases
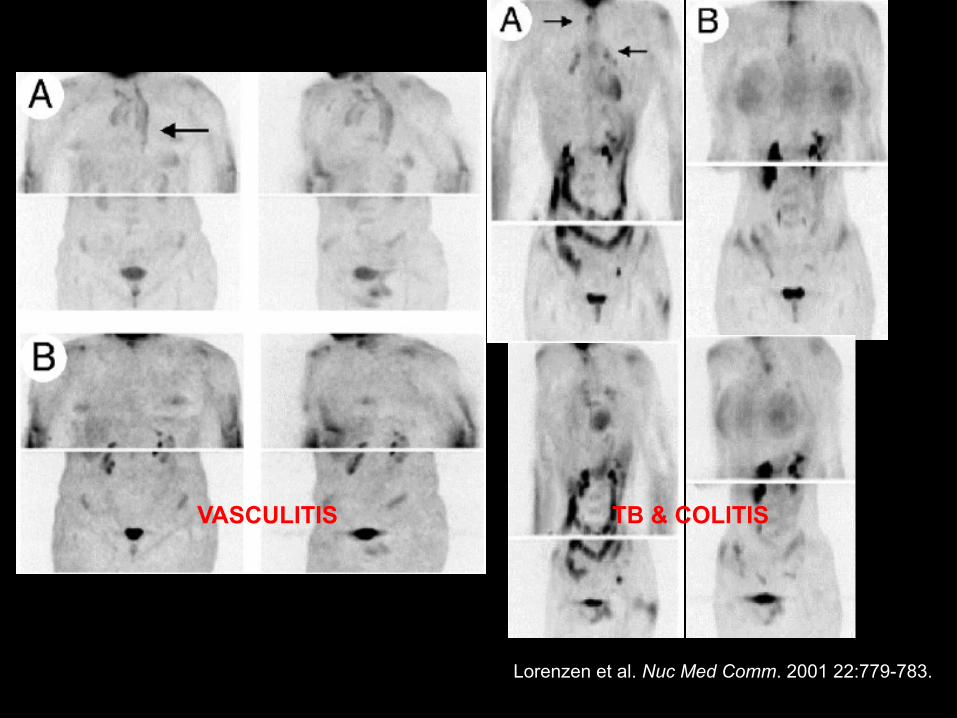
Lorenzen et al. Nuc Med Comm. 2001 22:779-783.
VASCULITIS TB & COLITIS
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
ü 18 patients underwent 18F FDG PET and 67Ga scintigraphy
ü Inclusion criteria: documented FUO
ü Exclusion criteria: pregnancy, age<18 years
ü Results:
Ø 8 cases: infection
Ø 2 cases: neoplasm
Ø 5 cases: auto-immune disorders
Ø 3 cases: unknown
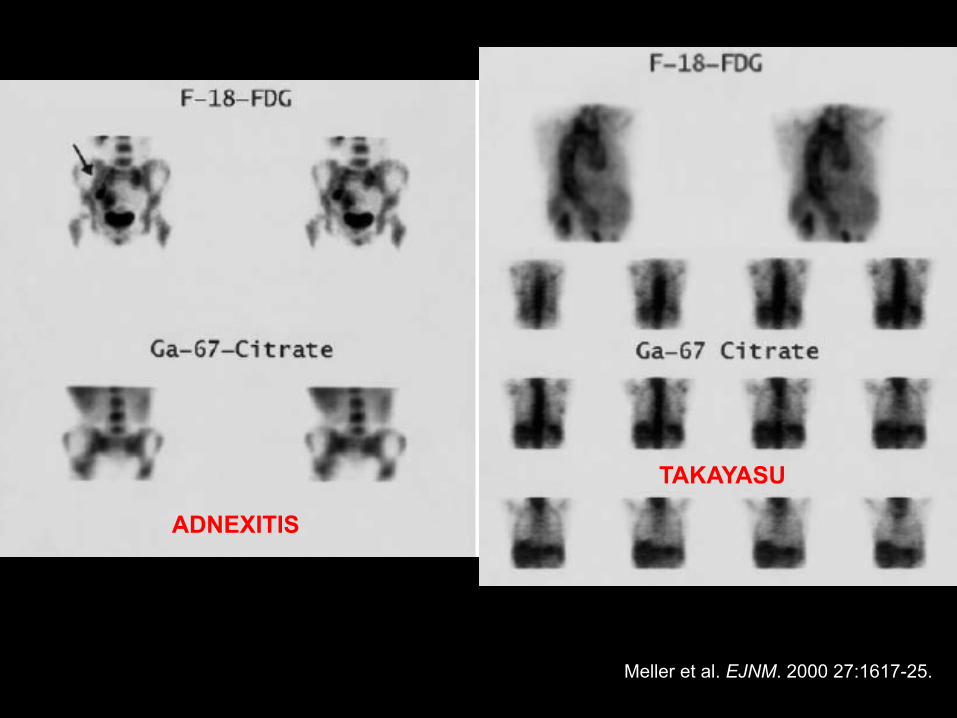
ADNEXITIS
TAKAYASU
Meller et al. EJNM. 2000 27:1617-25.
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
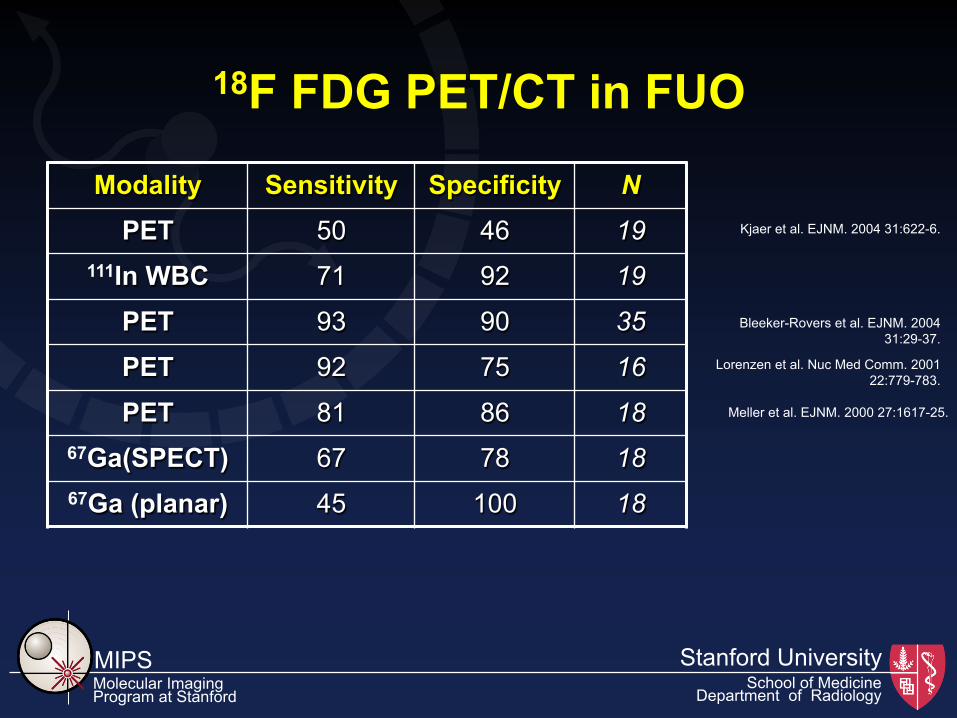
Modality Sensitivity Specificity N PET 50 46 19
111In WBC 71 92 19
PET 93 90 35
PET 92 75 16
PET 81 86 18 67Ga(SPECT) 67 78 18 67Ga (planar) 45 100 18
18F FDG PET/CT in FUO
Kjaer et al. EJNM. 2004 31:622-6.
Meller et al. EJNM. 2000 27:1617-25.
Bleeker-Rovers et al. EJNM. 2004 31:29-37.
Lorenzen et al. Nuc Med Comm. 2001 22:779-783.
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
18F FDG PET/CT for Evaluation of Joint Prostheses
Definitions: ü Total joint replacement is a surgical procedure in which a diseased or damaged joint, such as a hip or knee, is removed and replaced with artificial components ü Modern-day joint replacement surgery has been performed in the United States since the 1970s
ü More than 700,000 individuals had hip or knee replacement surgery in 2002
ü Infected prostheses have mostly an indolent course, with progressive joint pain; however, some present acutely, with high fever, joint pain, swelling, and erythema
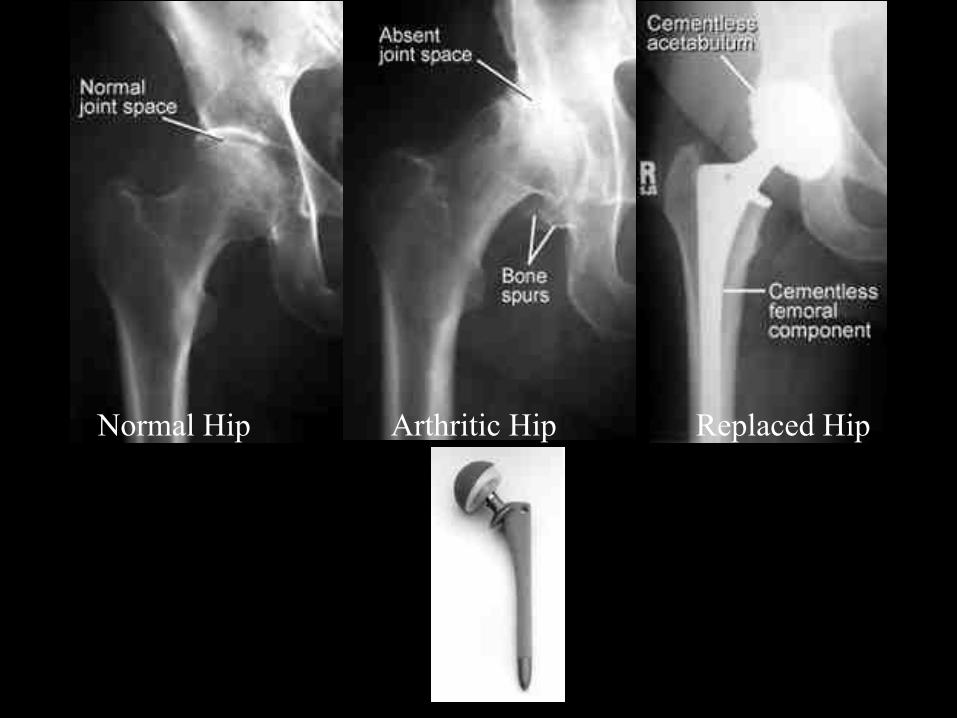
Normal Hip Arthritic Hip Replaced Hip

Normal Knee Arthritic Knee Replaced Knee
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
Infection in Joint Prostheses
Risk factors: ü prior surgery at site of
prosthesis ü rheumatoid arthritis ü corticosteroid therapy ü diabetes mellitus ü obesity ü malnutrition ü old age
Pathogenesis: ü Occurs in osseous tissue
adjacent to prosthesis: Ø bone cement interface Ø bone contiguous with
prosthesis (cement-less devices)
ü Results from: Ø local inoculation at surgery
or post-op spread from wound sepsis
Ø hematogenous spread
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
Infection in Joint Prostheses
Management: ü Retain / replace prosthesis
Ø simple debridement (retaining prosthesis) plus antibiotics - only successful in 20% of cases
Ø removal of prosthesis, antibiotics for 6wks, re-implantation of prosthesis - 90%+ success
Ø removal of prosthesis, immediate re-implantation, antibiotics - 70%+ success
ü Resection arthroplasty ü Suppressive long-term antibiotics
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
ü 23 patients (14 women, 9 men), 35-83 years-old
ü Inclusion criteria: painful hip or knee prosthesis
ü Results:
Ø PET was false negative for loosening in 1 case
ü Conclusion:
Ø PET can be useful in differentiating between loose and infected prosthesis
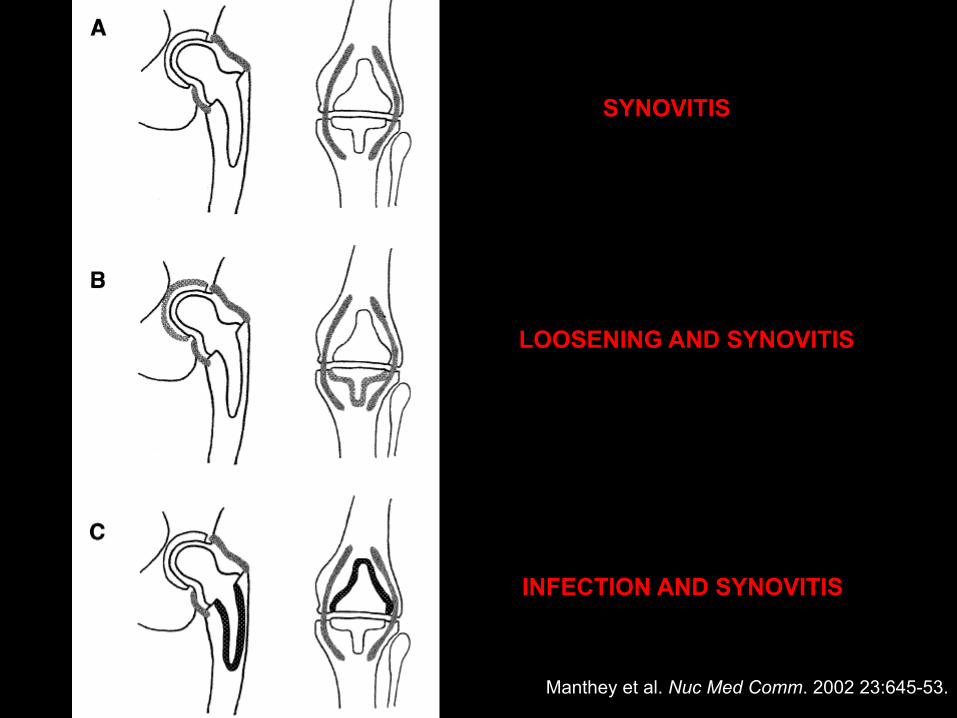
Manthey et al. Nuc Med Comm. 2002 23:645-53.
INFECTION AND SYNOVITIS
LOOSENING AND SYNOVITIS
SYNOVITIS
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
ü 50 patients (31 women, 19 men), 42-86 years-old
ü Inclusion criteria: painful hip prosthesis
ü Results:
Ø PET was 91% sensitive and 92% specific
Ø 3 phase bone scan was 78% sensitive and 70% specific
Ø no significant differences between cemented and uncemented
ü Conclusion:
Ø PET can better differentiate between aseptic loosening and infection
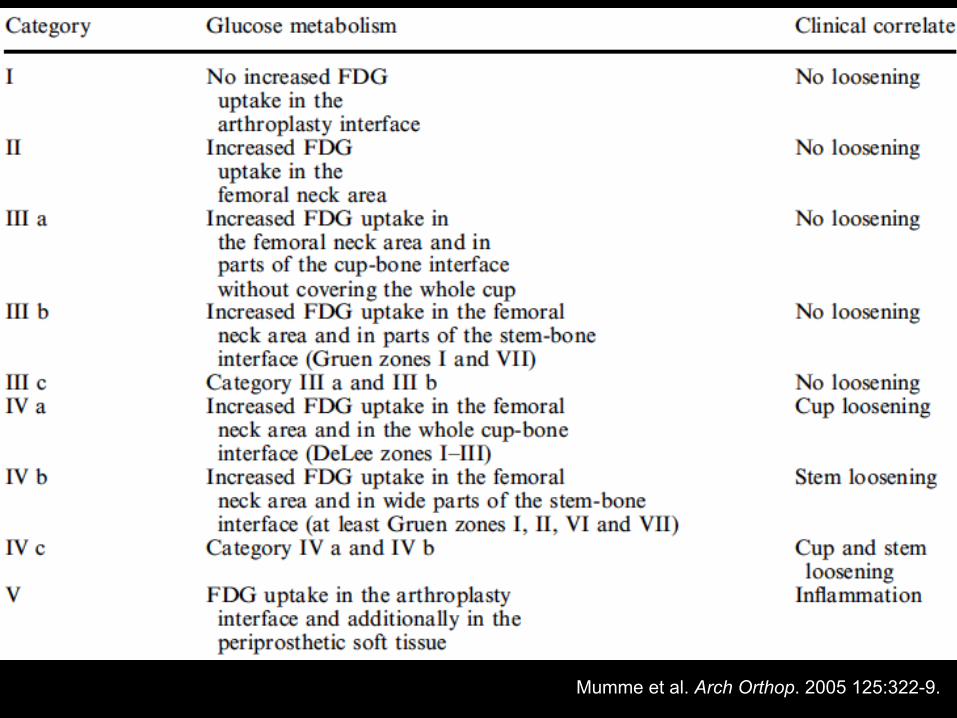
Mumme et al. Arch Orthop. 2005 125:322-9.
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
ü 21 patients (13 women, 8 men), 33-78 years-old
ü Inclusion criteria: suspicion for infected knee prosthesis
ü Results:
Ø WBC scan alone was 100% sensitive and 53% specific
Ø PET alone was 100% sensitive and 73% specific
Ø in combination with 3PBS, sensitivities increased to 93% for WBC scan and 80% for PET
ü Conclusion:
Ø PET seems to offer no additional benefit
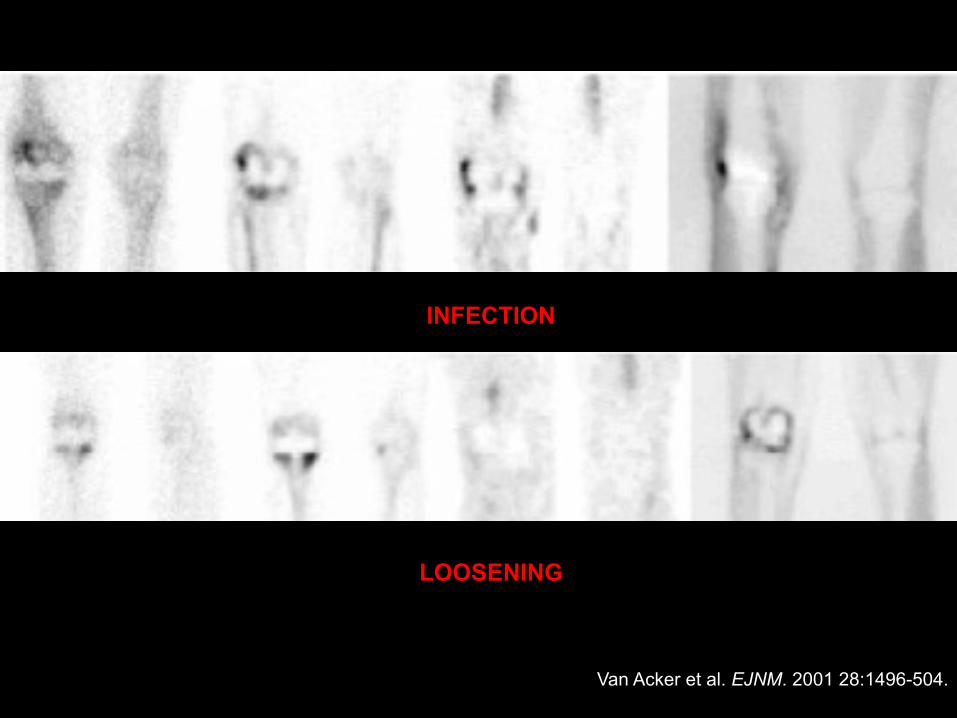
Van Acker et al. EJNM. 2001 28:1496-504.
INFECTION
LOOSENING
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
ü 59 patients (37 women, 22 men), 35-89 years-old
ü Inclusion criteria: painful prosthesis (40 hip, 19 knee)
ü Results:
Ø PET sensitivity was 100, 96, 52, 36% and specificity was 9, 35, 44, 97% based on different interpretation criteria
Ø WBC/sulphur colloid scan was 100% sensitive and 91% specific
ü Conclusion:
Ø PET is less accurate and can’t replace WBC/SC scanning
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
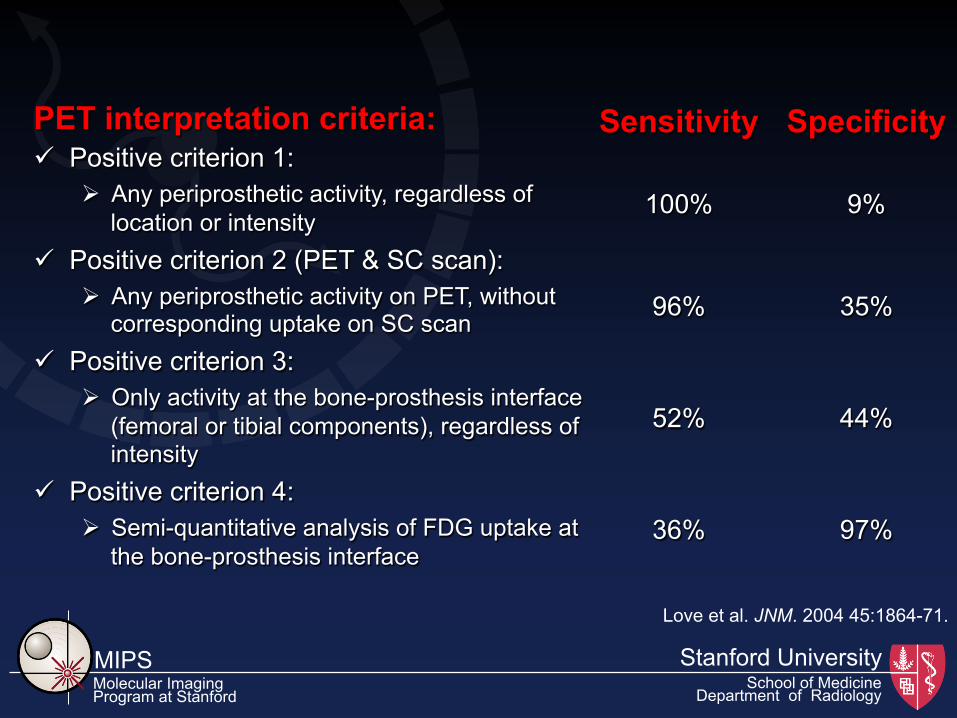
Sensitivity Specificity
100%
9%
96%
35%
52%
44%
36%
97%
PET interpretation criteria: ü Positive criterion 1:
Ø Any periprosthetic activity, regardless of location or intensity
ü Positive criterion 2 (PET & SC scan): Ø Any periprosthetic activity on PET, without
corresponding uptake on SC scan ü Positive criterion 3:
Ø Only activity at the bone-prosthesis interface (femoral or tibial components), regardless of intensity
ü Positive criterion 4: Ø Semi-quantitative analysis of FDG uptake at
the bone-prosthesis interface
Love et al. JNM. 2004 45:1864-71.
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
18F FDG PET/CT in Chronic Osteomyelitis ü Chronic osteomyelitis is a severe, persistent, and sometimes incapacitating
infection of bone and bone marrow that results when the inflammatory process continues over time, leading to bone sclerosis and deformity
ü It is often a recurring condition because it is difficult to treat definitively
ü It may result from: Ø inadequately treated acute osteomyelitis;
Ø hematogenous osteomyelitis;
Ø trauma;
Ø iatrogenic causes such as joint replacements and the internal fixation of fractures;
Ø compound fractures;
Ø infection with organisms, such as Mycobacterium tuberculosis and Treponema species (syphilis);
Ø contiguous spread from soft tissues, as in diabetic ulcers or ulcers in peripheral vascular disease.
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
ü 33 patients (7 women, 26 men), 17-80 years-old (mean: 50)
ü Inclusion criteria: suspected chronic osteomyelitis (>6 weeks)
ü Exclusion criteria: trauma/surgery within 6 months of PET, antibiotic therapy, preganancy, age<18 years
ü PET/CT had overall sensitivity of 94% and specificity of 87%
ü For lesions in the axial PET/CT was 88% sensitive and 100% specific, while for the appendicular skeleton it was 100% sensitive and 85% specific
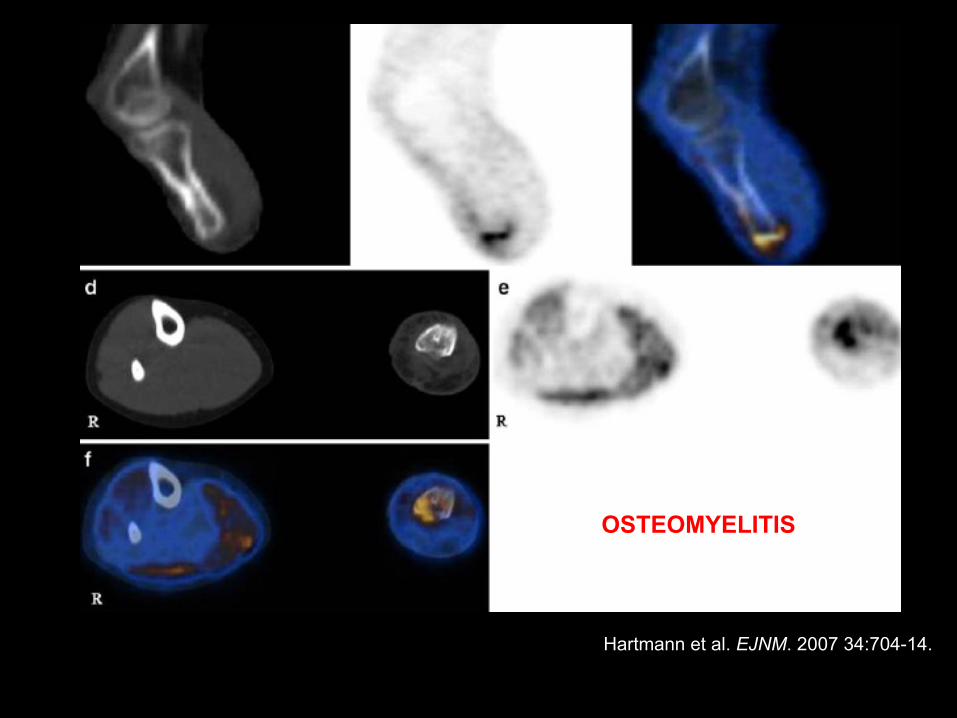
Hartmann et al. EJNM. 2007 34:704-14.
OSTEOMYELITIS
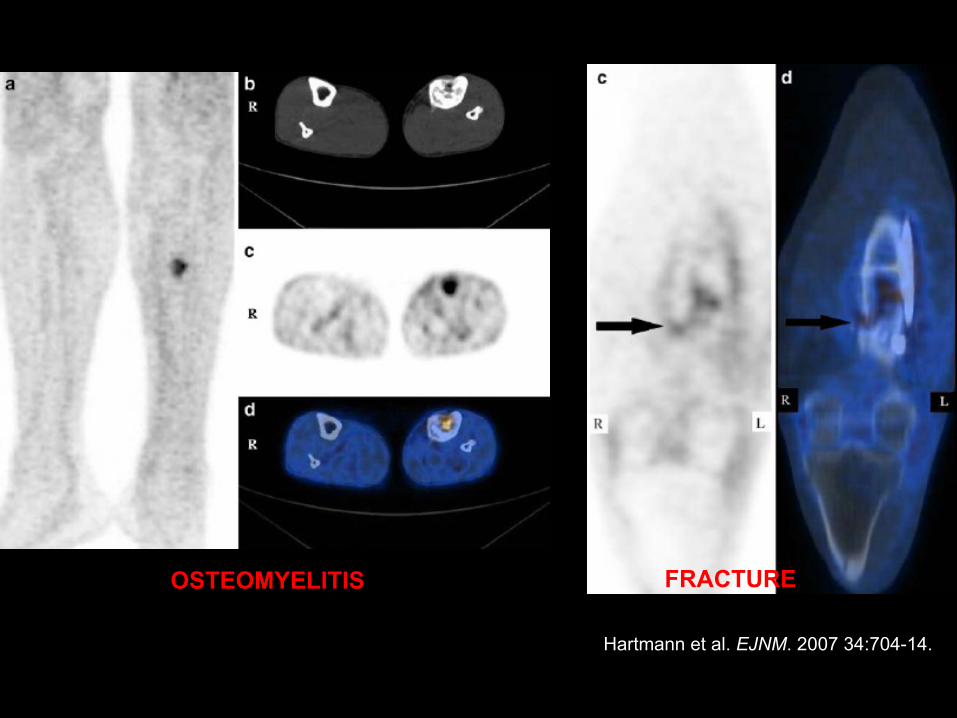
Hartmann et al. EJNM. 2007 34:704-14.
OSTEOMYELITIS FRACTURE
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
18F FDG PET/CT for Evaluation of the Diabetic Foot
ü Osteomyelitis of the foot is a challenging diagnosis and affects up to 15% of diabetic patients, often as a result of direct contamination from a soft tissue lesion
ü Early diagnosis of osteomyelitis in the diabetic foot is crucial because antibiotic therapy can be curative and prevent amputation
ü Plain radiograph is the first-line imaging modality to evaluate the foot, BUT…
ü MRI is considered the modality of choice to evaluate for diabetic foot osetomyelitis and associated soft-tissue abnormalities
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
ü 14 patients (4 women, 10 men), 29-70 years-old (mean: 54)
ü Inclusion criteria: suspected infected diabetic foot
ü Exclusion criteria: preganancy, age<18 years
ü PET/CT correctly localized 8 foci in 4 patients to bone, indicating osteomyelitis
ü PET/CT excluded osteomyelitis in 5 foci in 5 patients, indicating soft tissue uptake only
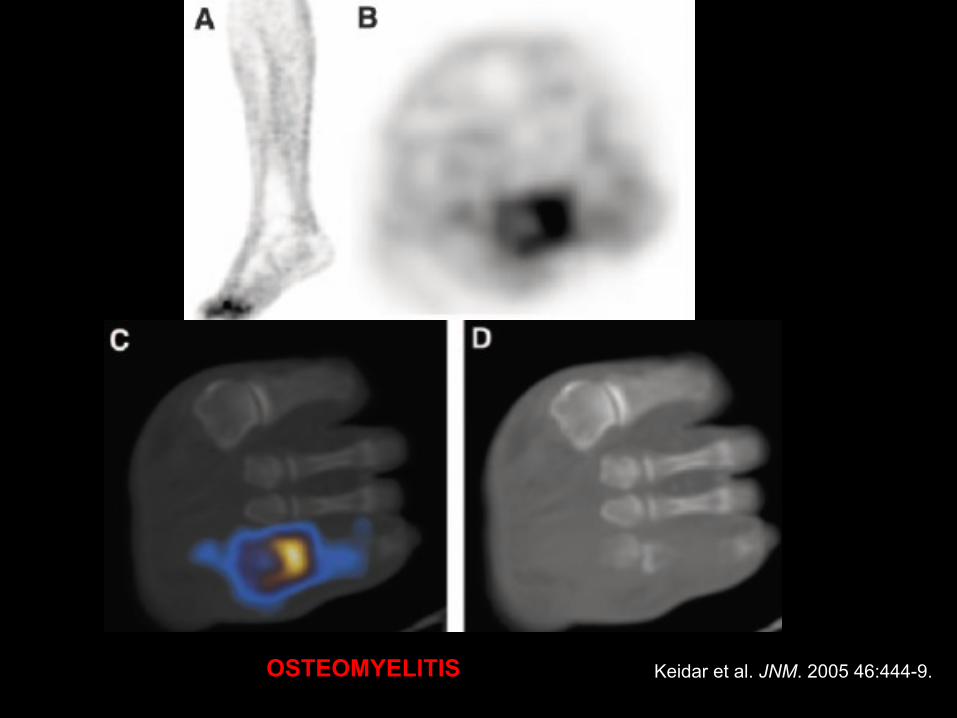
Keidar et al. JNM. 2005 46:444-9. OSTEOMYELITIS
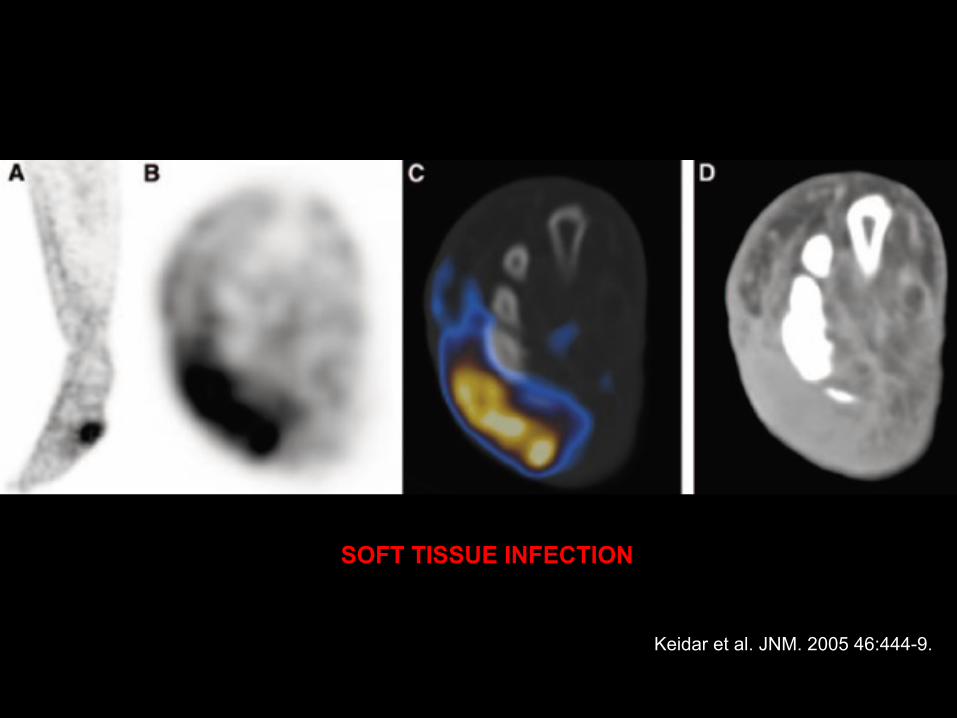
Keidar et al. JNM. 2005 46:444-9.
SOFT TISSUE INFECTION
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
ü 17 patients (6 women, 11 men) with Charcot’s neuro-arthropathy, 59.4 ± 8.6 year-old
ü Inclusion criteria: Charcot’s neuro-arthropathy
ü Exclusion criteria: preganancy, age<18 years
ü PET/CT had a sensitivity of 100% and specificity of 93.8%
ü MRI had a sensitivity of 76.9% and specificity of 75%
ü Soft tissue infection was diagnosed in 7/17 patients (43.7%)

Basu et al. Nuc Med Comm. 2007 28:465-72.
OSTEOMYELITIS
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
18F FDG PET/CT in Vasculitides Definition:
Presence of leukocytes in the vessel wall with reactive damage to mural structures
Loss of integrity g bleeding Compromise of lumen g ischemia
When to suspect?
Systemic symptoms + Single or multi-organ dysfunction Pathophysiology of vessel damage in vasculitic syndromes:
ü Pathogenic immune complex formation and/or deposition ü Production of antineutrophilic cytoplasmic antibodies ü Pathogenic T lymphocyte responses and granuloma formation
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
Small Vessel ü Churg-Strauss ü Wegener’s ü Microscopic Polyangiitis ü HSP ü Essential Cryoglobulinemia ü Hypersensitivity vasculitis ü Vasculitis 2nd to CTD ü Vasculitis 2nd to viral infection
Classification of Vasculitides
Large Vessel ü Takayasu arteritis ü Giant Cell Arteritis
Medium Vessel ü PAN ü Kawasaki’s ü Isolated CNS vasculitis
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
Secondary Vasculitis Syndromes ü Drug-induced vasculitis ü Serum sickness ü Vasculitis associated with other
primary diseases ü Infection ü Malignancy ü Rheumatic disease
Primary Vasculitis Syndromes ü Wegener's granulomatosis ü Churg-Strauss syndrome ü Polyarteritis nodosa ü Microscopic polyangiitis ü Giant cell arteritis ü Takayasu's arteritis ü Henoch-Schönlein purpura ü Idiopathic cutaneous vasculitis ü Essential mixed cryoglobulinemia ü Behçet's syndrome ü Isolated vasculitis of the central
nervous system ü Cogan's syndrome ü Kawasaki disease
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
Coagulopathies/thrombotic diseases ü Antiphospholipid antibody syndrome ü Thrombotic thrombocytopenic
purpura Neoplasms ü Atrial myxoma ü Lymphoma ü Carcinomatosis Sarcoidosis Atheroembolic disease Goodpasture's syndrome Amyloidosis Migraine Cryofibrinogenemia
Infectious Diseases ü Bacterial endocarditis ü Disseminated gonococcal infxn ü Pulmonary histoplasmosis ü Coccidioidomycosis ü Syphilis ü Lyme disease ü Rocky Mountain spotted fever ü Whipple's disease Drug toxicity ü Cocaine ü Amphetamines ü Ergot alkaloids ü Methysergide ü Arsenic
Other disorders mimicking vasculitis
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
ü 35 patients (25 women, 10 men), 72.7±6.7 years-old
ü Inclusion criteria: biopsy proven GCA
ü Results:
Ø vascular FDG uptake was noted in 29 patients (83%)
Ø the patients who relapsed had similar decrese in uptake after therapy as the ones who where in remission
ü Conclusion:
Ø GCA relapse can not be predicted by PET
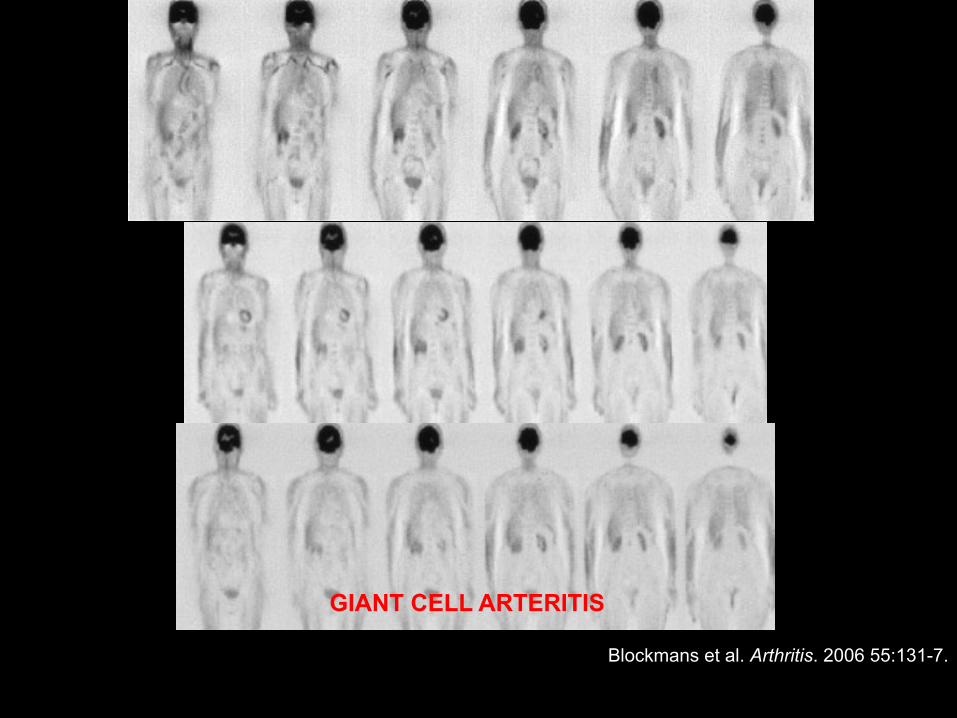
Blockmans et al. Arthritis. 2006 55:131-7.
GIANT CELL ARTERITIS
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
ü 22 patients (16 women, 6 men), 73.3±7.5 years-old
ü Inclusion criteria: clinical GCA; major vessel U/S examination
ü Results:
Ø all patients with signs of GCA on U/S had FDG uptake on PET
Ø when U/S was only positive in the temporal arteries, PET was completely negative
ü Conclusion:
Ø PET is not suitable for diagnosis of temporal arteritis
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
ü 30 patients with large vessel vasculitis and 31 controls
ü Results:
Ø Sensitivity of 73.3% (95% CI 54.1-87.7%), specificity of 83.9% (95% CI 66.3-94.5%), PPV of 81.5% (95% CI 61.9-93.7%) NPV of 76.5% (95% CI 58.8-89.3%)
Ø The diagnostic accuracy was higher in patients not receiving immunosuppressive drugs (93.3 vs 64.5%, p = 0.006)
Ø FDG PET increased the clinical diagnostic accuracy from 54.1 to 70.5% (p = 0.04)
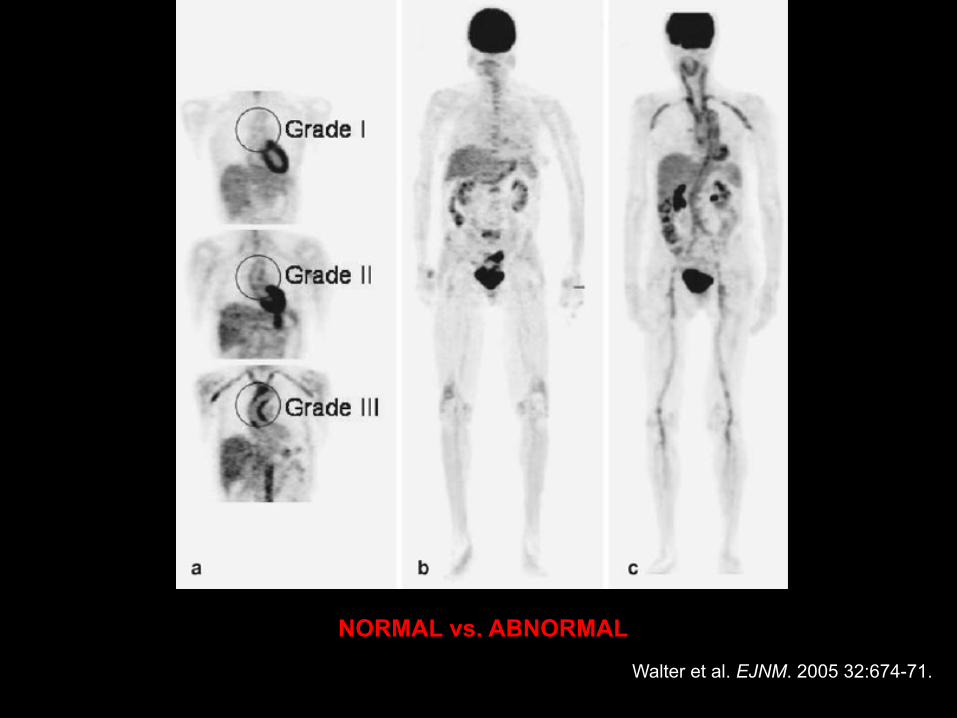
NORMAL vs. ABNORMAL Walter et al. EJNM. 2005 32:674-71.
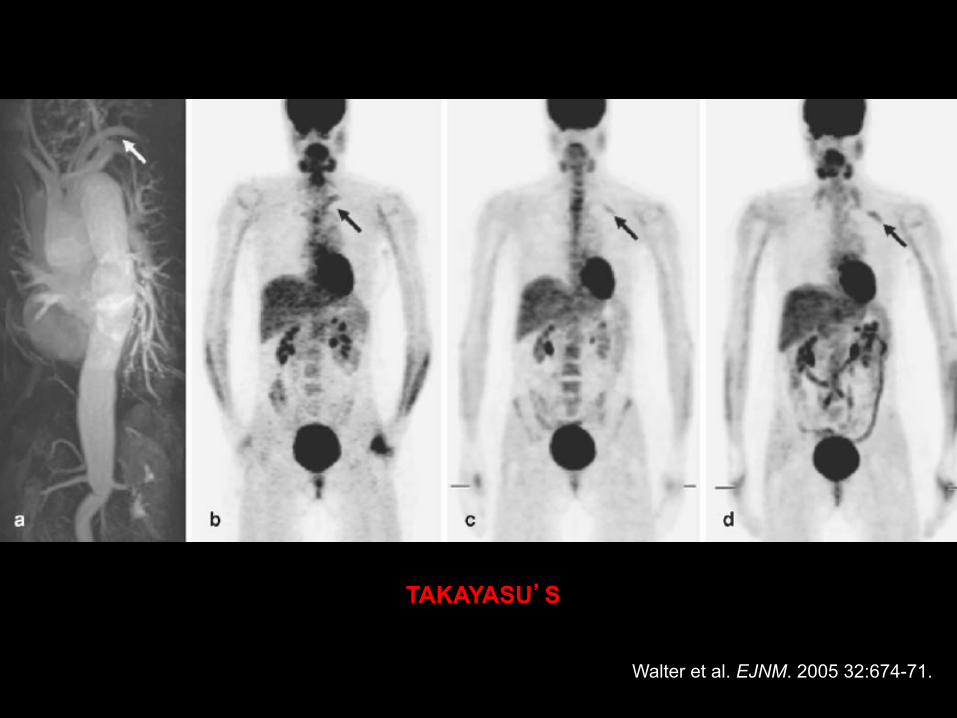
TAKAYASU’S
Walter et al. EJNM. 2005 32:674-71.
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
ü 18 patients (17 women, 1 man), 23-64 years-old
ü Inclusion criteria: Takayasu’s arteritis
ü Results:
Ø sensitivity was 92% and specificity was 100%
Ø NPV of 85% and PPV of 100% in initial evaluation of patients with suspected vasculitis
ü Conclusion:
Ø FDG PET can be used to diagnose early disease, to detect active disease and to monitor the effectiveness of therapy
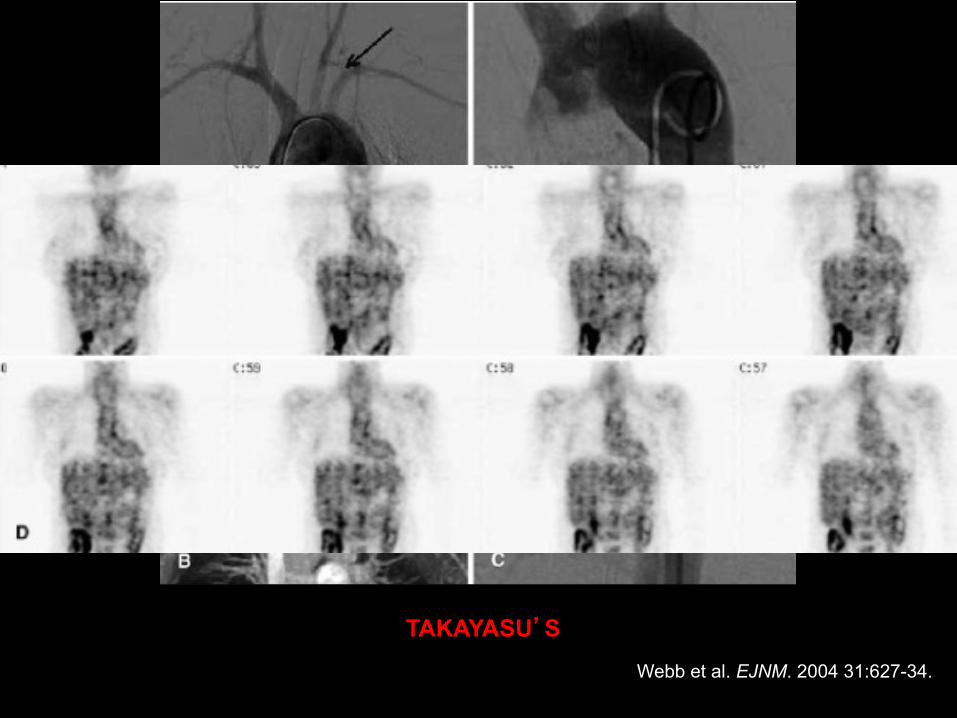
TAKAYASU’S Webb et al. EJNM. 2004 31:627-34.
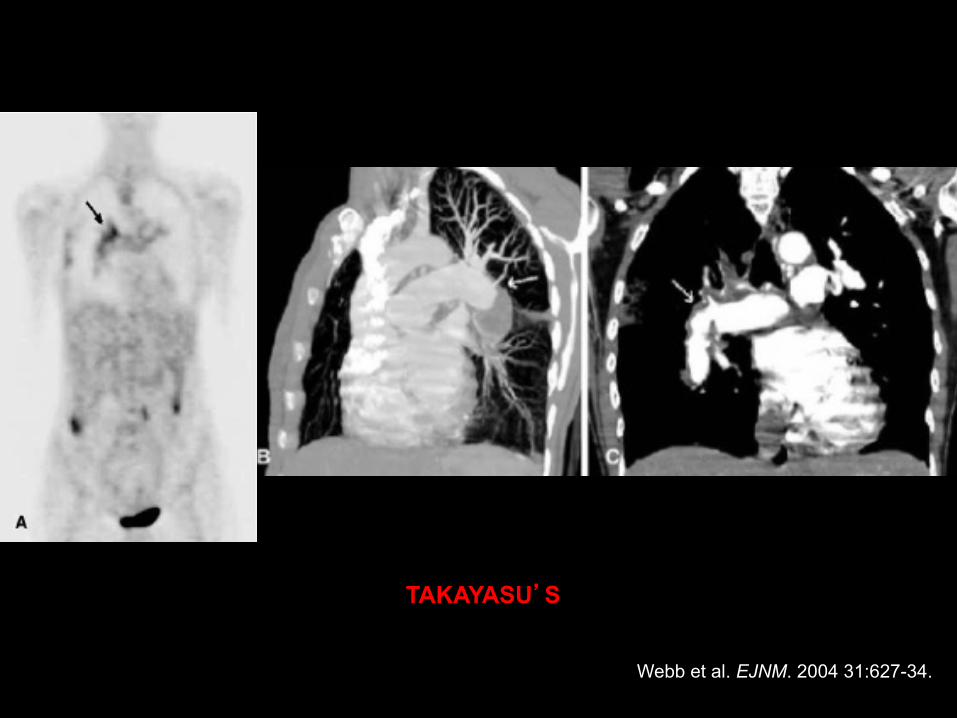
TAKAYASU’S
Webb et al. EJNM. 2004 31:627-34.
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
ü 15 patients (9 women, 6 men), 26-76 years-old
ü Inclusion criteria: early aortitis (FUO, elevated ESR/CRP, FDG uptake in the aorta); MRI available
ü Results:
Ø at baseline PET was abnormal in 56% of the cases, while MRI was abnormal in 53%
Ø 80% showed normalization on PET after therapy
ü Conclusion:
Ø PET and MRI have comparable results, but PET showed more areas of disease involvement, with better evaluation of response to therapy
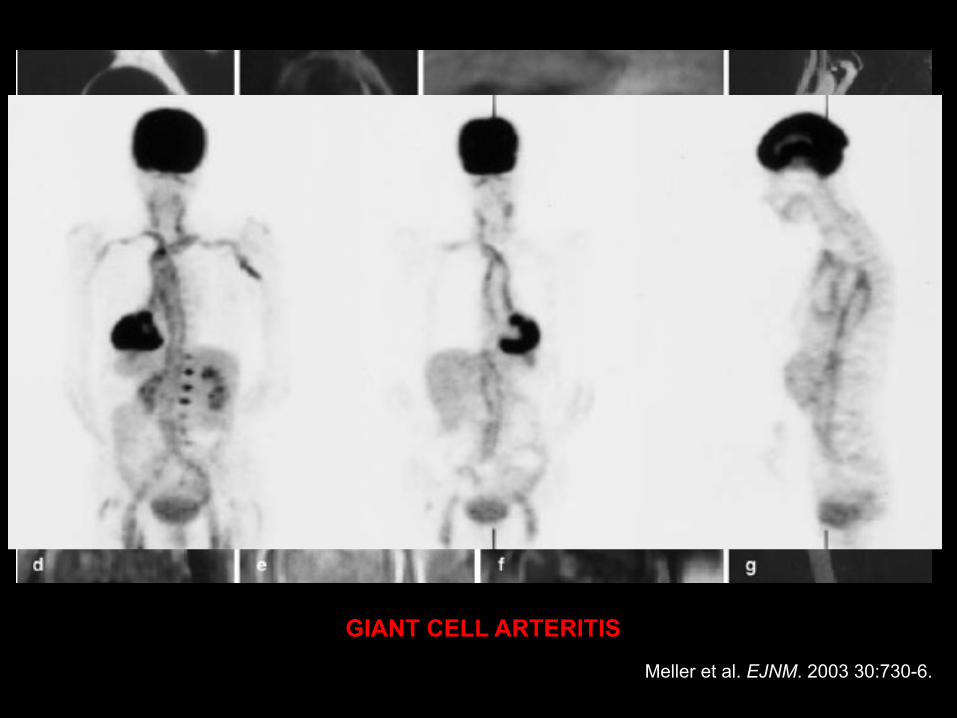
GIANT CELL ARTERITIS Meller et al. EJNM. 2003 30:730-6.
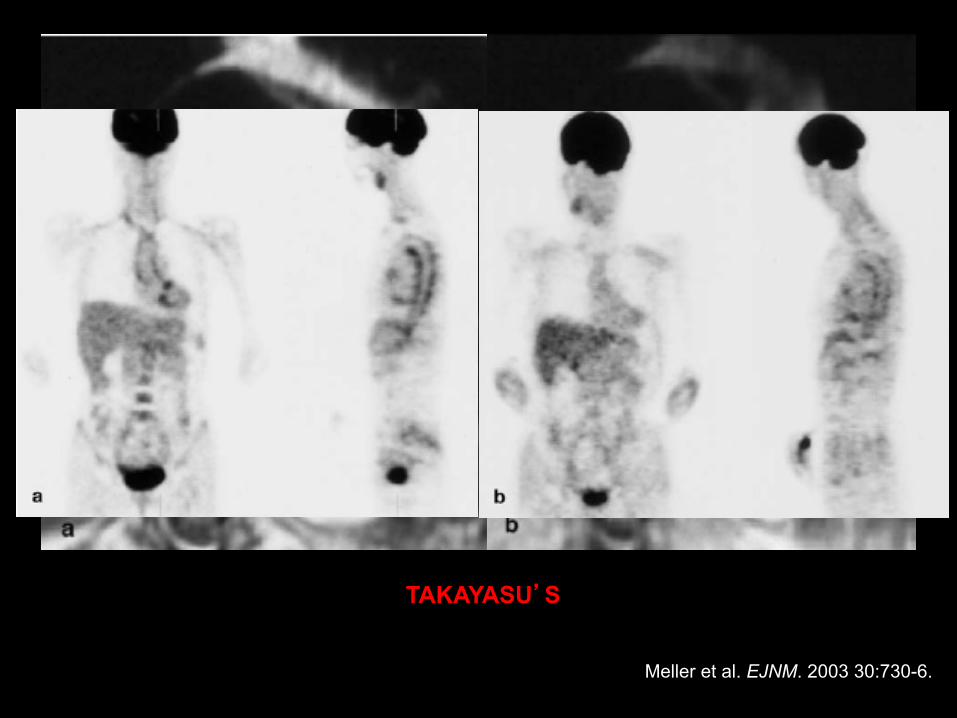
TAKAYASU’S
Meller et al. EJNM. 2003 30:730-6.
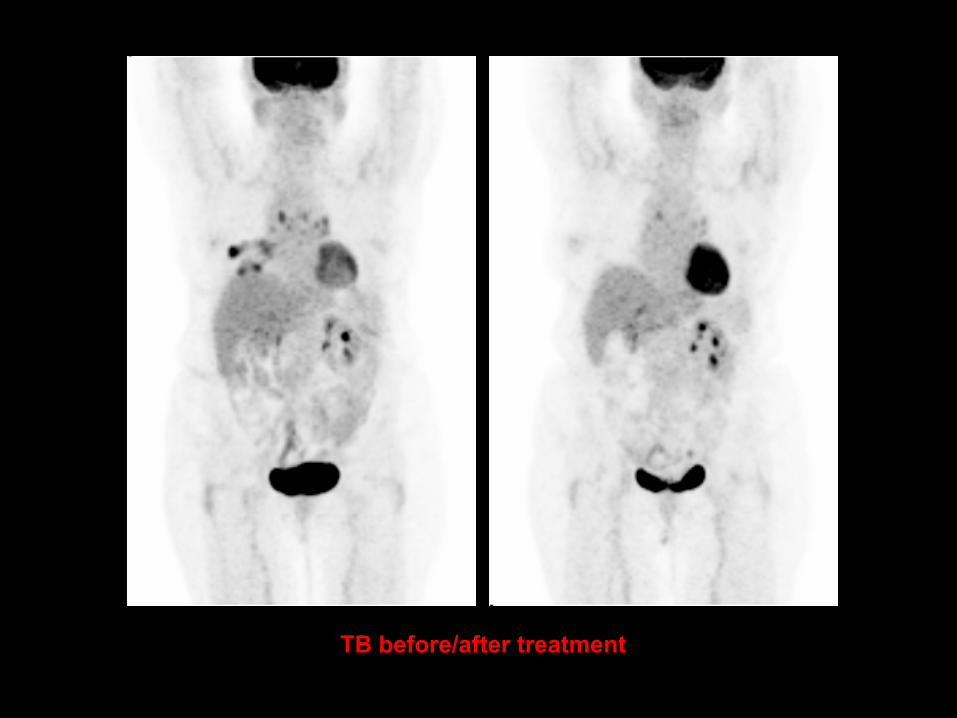
TB before/after treatment
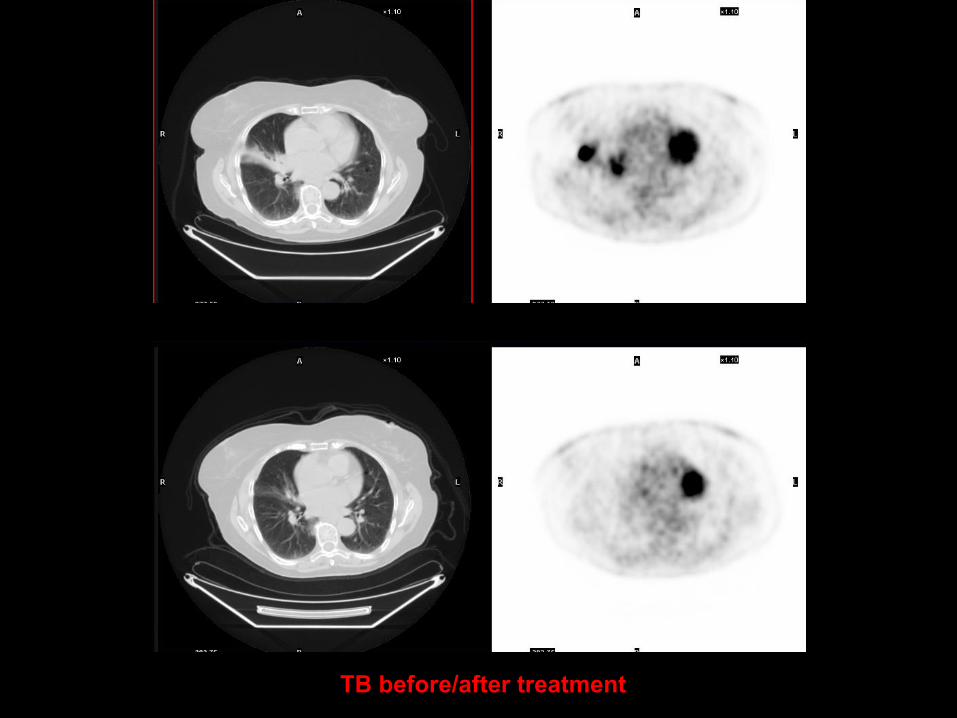
TB before/after treatment
a

TAKAYASU’S
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
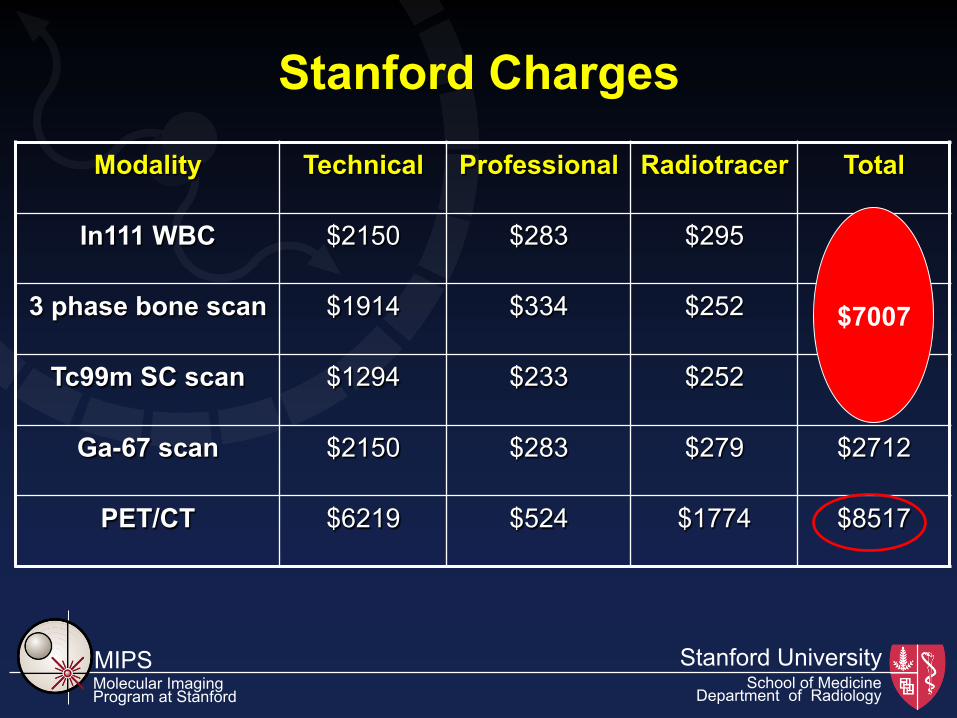
Modality Technical Professional Radiotracer Total
In111 WBC $2150 $283 $295 $2728
3 phase bone scan $1914 $334 $252 $2500
Tc99m SC scan $1294 $233 $252 $1779
Ga-67 scan $2150 $283 $279 $2712
PET/CT $6219 $524 $1774 $8517
Stanford Charges
$7007
MIPS Stanford University Molecular Imaging Program at Stanford
School of Medicine Department of Radiology
“FDG’s exquisite sensitivity suggests that it may be useful in a FUO, an entity with diverse etiologies. In addition to tumor and infection, other conditions that may present as a FUO, including vasculitis, thromboembolic disease, sarcoidosis and chronic granulomatous disease, are associated with increased FDG uptake. FDG PET appears to be sensitive for detecting focal infection and may be useful for detecting infected prosthetic vascular grafts, mycotic aneurisms, lung abscesses and intra-abdominal infections. FDG PET also may be useful for diagnosing musculoskeletal infection, especially in the setting of previous trauma and metallic implants. The fact that increased FDG uptake occurs in many neoplasms is both a relative advantage and a relative disadvantage.”

THANK YOU!
http://nuclearmedicine.stanford.edu