Embed Size (px)
Citation preview

Estimation of Intravascular Fluid Status
and Organ Perfusion Part II:Illustrative Cases
Mark Lepore, MD
November 17 &
December 3, 2008

Objectives
• Background: Fluid Distribution in the Body
• Relationship of Intravascular Volume (Preload) to Perfusion of Organs
• How to Estimate Intravascular Fluid Volume
• How to Measure Organ Perfusion
• Fluid Options
• Illustrative Cases

Objectives
• Physiology of Fluid Distribution in the BodyPhysiology of Fluid Distribution in the Body
• Relationship of Intravascular Volume Relationship of Intravascular Volume (Preload) to Perfusion of Organs(Preload) to Perfusion of Organs
• How to Estimate Intravascular Fluid How to Estimate Intravascular Fluid VolumeVolume
• How to Measure Organ PerfusionHow to Measure Organ Perfusion
• Fluid OptionsFluid Options
• Illustrative Cases

Case # 1
• G.M., 45 year old male admitted to SPH with altered mental status, anasarca, alcohol withdrawal
• Child’s C Cirrhosis due to alcoholism
• Intubated for pneumonia and respiratory failure, started on broad spectrum antibiotics

Case #1 (continued)
• On Hospital Day #5, the covering House Officer called for decreased Urine output down to 15-20ml hour

Case #2 Picture
More History
Labs
More Data?

Vital Signs
• Blood pressure 106-145/61-72, Pulse 69-95, Respirations 22 and riding the ventilator
• Afebrile
• O2 Sat decreasing to the low 90s despite 100% FiO2

Physical Exam
• Anasarca
• Riding the ventilator
• Breath sounds rhonchorus bilaterally
• Abdomen distended

Chest X-Ray

More History
• The patient had an episode of desaturation into the mid 60% range, necessitating bagging back to the 90% range.

Labs
• Na 140, K 4.4, Chloride 111, Bicarb 23, BUN 17, Creatinine 1, Calcium 7.8
• WBC 16.4 (stable for prior 3 days)

More Data?
• Fluid boluses were given x 3 with no change in urine output
• The patient was 9.5 Liters positive overall in his first 5 days of the hospital stay

Discussion
• Cirrhotics are at risk for third-spacing all of their fluid, including into their lungs
• In the face of adequate blood pressures, a trial of Lasix is indicated given the severe desaturations
• With Lasix administration (40mg IV with little response, followed by 80mg IV with better urine output), O2 Saturation improved, and FiO2 was able to be weaned to 80% by the following morning

Discussion (continued)
• Creatinine bumped to 1.8 the next morning, and albumin was initiated, along with cessation of the diuresis
• IV Fluids were minimized
• Urine output continued to and the patient’s renal function improved back to normal over the following 5 days

Case #2
• R.S., 45 year old male with ischemic cardiomyopathy, known EF 10% in 2006, presented short of breath, hypotensive, and dizzy.
• Rash on left lower extremity painful
• By history, had been without medications for 3 months, but had recently acquired them and was trying to overcompensate

Case #2 (continued)
• Admitted to the ICU with a blood pressure of 67/42

Case #5 Picture
More History
Labs
More Data?

Vital Signs
• 67/42 in ER, Pulse 102, RR 24, O2 Sat 100% on 3 Liters
• Afebrile

Physical Exam
• Tangential in thought, in No Acute Distress
• S1 S2 tachycardic
• Rales at bases, with some bilateral rhonchi
• 3+ pitting edema Left > Right with erythema, warmth, and weeping of left shin

Chest X-Ray

More History

Labs
• Sodium 131, Potassium 3.7, Chloride 94, Bicarb 30, BUN 30, Creatinine 1.4
• NT-pro-BNP 12,000
• INR 5.2, on Coumadin
• Troponin 0.05
• TSH 4.85
• Digoxin 0.5
• CRP 11.75
• WBC 11, 84% Neutrophils, 5% Bands

More Data?
• Echocardiogram (2 years prior to admission): Ejection Fraction 10% with some diastolic dysfunction and minor valvular insufficiency

Discussion
• The hypotension in the face of possible sepsis from cellulitis takes precedence, even with an ejection fraction of 10% with diastolic dysfunction
• The patient responded favorably to gentle (250ml at a time) boluses with improved blood pressures into the low 100s systolic, and was transferred to DOU the next day

Case #3
• 58 year old male with known Child’s C Cirrhosis
• Admitted for Upper GI Bleed for which he is transfused and receives an EGD with banding
• Goes into Florid Delirium tremens on Hospital Day #3
• Subsequently develops respiratory failure necessitating intubation

Case #3 (continued)
• Pressors and antibiotics were started for his pneumonia and he survives acutely to get off the pressors.
• Urine output, however, falls off severely, associated with a drastic increase in serum creatinine from 1 to 6.2

Case # 3 Picture
More History
Labs
More Data?

Vital Signs
• Exam: BP 102/60, P=104, R=20 (riding the ventilator)
• Ventilator settings: SIMV 420 x 20, FiO2 50%, PEEP 5
• O2 Sat 93-95%

Physical Exam
• No rales appreciated. No S3.
• Impressive ascites but not tense
• 2-3+ peripheral edema
• Chest X-ray shows bilateral infiltrates
• Unclear if he has JVD

Chest X-Ray

Labs
• Sodium 149, Potassium 4.4, Chloride 110, Bicarb 26, BUN 89, Creatinine 6.1
• WBC 11.1 (stable), Hb 10.1, Plt 65 (stable)

More Data?
• No more data needed

Discussion
• Fluid Status is unclear in this patient• What IS clear is that his poor renal
function is going to kill him• The goal is to push him to the point of
being absolutely sure that he is not volume depleted
• Despite aggressive hydration, even to the point of overload, his renal function did not improve, and he was placed on comfort measures and subsequently passed away

Case #4
• 40 year old female with 18 year history of diabetes, presented to the hospital in congestive heart failure, with nausea and vomiting and presumed uremia. Creatinine 7, BUN 83.
• On Hospital Day # 3, the house officer is called for the patient’s oxygen saturation dropping to the 70% range on Room Air

Case #7 Photo
More History
Labs
More Data?

Vital Signs
• Blood pressure 206/119
• Pulse 132
• Respirations 30
• Temperature 101.7
• O2 Sat 99% on Non-Rebreather

Physical Exam
• Tachypneic, mildly diaphoretic female
• S1 S2 tachycardic
• Small rales and “cardiac wheeze” present on the right lung field
• No significant peripheral edema
• No JVD

Labs
• NT-pro BNP = 30,000 (was 40,000)
• BUN/creatinine = 22/3.5 (both down)
• UA 26-50 WBC, small Leukocyte Esterase
• WBC 13.1 with 89 N, 2 Bands (up from 6.7 with normal diff in the morning)
• Blood glucose = 230
• Lactic Acid = 0.6

Chest X-Ray

More History
• 3.5 Liters removed with dialysis that same day
• Tunneled dialysis catheter placed 2 days prior at St. John’s

More Data?
• No more data needed
• The patient vomited twice during dialysis

Discussion
• The preponderance of evidence points to the patient being septic and either probably euvolemic or more likely hypovolemic (fever, 3.5 Liters removed, rising WBC count, diabetic on dialysis --setup for infection).
• The only data pointing to overload is the Chest X-ray and the BNP (both of which are not specific)

Discussion (continued)
• As she had been in the hospital for 72 hours, the patient was started on broad antibiotic coverage for Hospital Acquired Pneumonia (Vanco/Zosyn/Levo to cover MRSA and Pseudomonas)
• Blood cultures returned within 12 hours with S. aureus

Case # 5• 82 year old female with a significant
history of dementia, presented to the ER with a mechanical fall off of the toilet and a forehead laceration
• Head CT Negative• The patient was sitting in the ER all night
with an IV running, and was found the next morning to look “a little blue” and “a little short of breath”
• O2 Sat 80% on 5 Liters O2 by nasal cannula

Case # 5
• Vital signs in the ER revealed a blood pressure of 86/40 and pulse of 110.

Case # 5 (continued)
• The ER gave the patient a 500ml bolus of Normal Saline, with no improvement in her blood pressure or tachycardia; her O2 Sat was up to 92% but on 10 Liters facemask
• They then gave her Lasix 40mg IV along with 500ml more of Normal Saline, to the same (lack of) effect on blood pressure or pulse

Case # 9 Picture
More History
Labs
More Data?

Vital Signs
• Blood pressure persistently in the 80s systolic
• Poor urine output
• Pulse 102-110
• Respirations 25
• O2 Sat 92-94% on 10 Liters facemask

Physical Exam
• Mild respiratory distress
• Obese neck – unable to determine JVD
• S1 S2 very distant breath sounds
• Rales ¾ of the way up her lung fields
• Abdomen benign
• 3+ pitting edema peripherally

Chest X-Ray

More History
• By history, the patient claimed to have “Class 4 Heart Failure”

Labs
• Na 132, K 3.5, Cl 100, Bicarb 28, BUN 34, Creatinine 2.1, Glucose 180
• WBC 8.2, Hb 10.4, Plt 303

Discussion
• Massive fluid overload in the face of hypotension is CARDIOGENIC SHOCK
• Giving this patient who is clearly intravascularly overloaded is incorrect
• Giving fluids with Lasix is also incorrect• In the face of hypotension, PRESSORS would
be the first step (e.g. Dopamine) to increase contractility, heart rate, and maximize the Frank-Starling curve
• If she was not very hypotensive, PRELOAD REDUCTION (Lasix or Nitrates) would be your first step

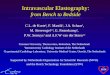
Frank-Starling Curve

Discussion
• In the face of massive overload and hypotension, pressors to maintain MAP + diuresis to optimize the Frank-Starling Curve is the proper treatment
• If it was not clear that she was overloaded (it was), getting more data (BNP, CVP) would be indicated
• Echocardiogram would be indicated acutely as well

Case #6
• S.G., 45 year old diabetic male admitted to the ICU on one of my ICU calls when I was a 2nd year resident
• 4 blue extremities, hypotensive, significant peripheral edema.

Case # 6 Picture
More History
Labs
More Data?

Vital Signs
• Blood pressure 80/40
• Pulse 120
• Respirations 35
• O2 Sat 84% on Room Air

Physical Exam
• 4 blue extremities, cool, to the knees/elbows
• S1 S2 tachycardic
• Rales halfway up the lung fields
• 2+ peripheral edema
• Equivocal JVD (large neck)

Chest X-Ray ??

More History
• Progressive weakness over prior days to weeks
• No history of fever, chills, cough, dysuria

Labs
• CK 1983, MB 64, Troponin 0.24
• Sodium 122, K 5.4, Chloride 85, Bicarb 16, Glucose 46, BUN 100, creatinine 1.8
• AST = 2502, ALT 4943, Alk Phos 283
• WBC 19.3, Hb 16.8, Platelets 94, N 91, Bands 4
• Fibrinogen 80, PTT>200

More Data?
• MUCH more data needed

Discussion
• In a diabetic, there should be large concern for sepsis in the face of hypotension (perhaps the patient isn’t mounting a WBC or fever response)
• Correct response should be a fluid bolus given the history and hypotension
• However, an astute clinician was very concerned about systolic heart failure given the severely cyanotic limbs and multi-organ failure

Discussion (continued)
• Swan Ganz catheter was inserted, finding a Cardiac Index of 1.5, SVRI of 3000, and wedge pressure of 23
• The patient had nitroprusside started, with improvement in renal function and blood pressure; Dobutamine would have been a reasonable alternative
• He was eventually converted to high-dose captopril
• Echocardiogram performed the next morning revealed 4 chamber hypokinesis and an ejection fraction of 10-15%

Case #7
• E.H., 52 year old female transferred to the DOU for increasing respiratory distress, abdominal pain
• Known pulmonary hypertension, severe, on three different therapies (2 oral, 1 subcutaneous pump), of unclear origin
• Desatting to 85% on high-flow oxygen

Case # 7 Picture
More History
Labs
More Data?

Vital Signs
• Pulse 120-130, BP 130/80, Respirations 25, Afebrile
• O2 Sat 90% on Non-Rebreather

Physical Exam
• Mildly tachypneic, complaining of severe abdominal pain, in moderate distress
• S1 S2 tachycardic
• Bilateral coarse rhonchi
• Abdomen mildly distended, tender in epigastrium
• 2-3+ pitting edema

Chest X-Ray

More History
• Long-standing Pulmonary Hypertension
• DNR/DNI

Labs
• Na 134, K 2.1, Chloride 98, Bicarb 24, BUN 39, Creatinine 1.8, Glucose 107 (BUN 52, Creatinine 2.8 on admission)
• WBC 7.4, Hb 10.5, Platelet 169,000, normal differential
• Pro-NT-BNP 16,307 3 days earlier
• Fluid balance NEGATIVE 5.8 Liters over prior 3 days

Discussion
• The worsening pulmonary function likely takes precedence over her renal insufficiency
• The renal function had actually IMPROVED since admission, with her fluid balance being 6 Liters negative over the prior 3 days
• The patient was further diuresed with some continued improvement in her BUN/creatinine

Discussion (continued)
• Other causes of worsening oxygenation were considered:– C Cardiac– D Drugs– S Secretions, Splinting– P Pneumothorax– I Infection– E Embolism– S Spasm (broncho)

Discussion (continued)
• She was given Morphine for her abdominal pain/splinting
• Full strength Lovenox was ordered for concern for PE
• CT Angiogram was considered but cancelled due to her renal function; Lower extremities Dopplers and Echocardiogram were normal

Case # 8
• 68 year old Pakistani man with a 4 month history of diarrhea, weight loss, failure to thrive; 3 month history of tremor, dysphagia with limited po intake and difficulty ambulating, and a 2 week history of being bed-bound, presented to the ER with a 3 day history of dry cough and shaking chills but no fever and a history of possible aspiration 3 days prior

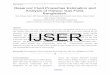
Chest X-Ray Admission

Case #8 (continued)
• Found to be bone-dry in the ER with a BUN of 111, creatinine of 6
• Resuscitated with 2 Liters Normal Saline, 2 Units Packed Red Blood Cells, and 200ml of 25% Albumin
• Found to be very hypoxic after resuscitation, necessitating intubation
• Initial A-a gradient of 21, A-a gradient 680 after resuscitation

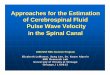
Chest X-Ray after Fluids

Case #8 (continued)
• For concern of hypoxia and acidemia, the patient was dialyzed after being intubated
• The patient became tachycardic to 150 from a baseline of 100
• Fluid challenge was initiated, with pulse coming down to 135 with 500ml of NS

Case # 8 Picture
More History
Labs
More Data?

Vital Signs
• Initially in ER: 99/63, T=97.6, Pulse 105, Respirations 30, 64kg
• In ICU: 111-128/59-66, Pulse = 130-135 prior to dialysis
• 100/55, Pulse = 146-148 after dialysis

Physical Exam
• Afebrile
• Extremely cachectic
• Mucus membranes very dry
• Equivocal JVD: elevated JVP with inspiration on the ventilator, would completely go away with expiration
• Tachycardia, distant heart sounds
• Bilateral rhonchi without focal findings
• No peripheral edema

More History
• Known diastolic dysfunction with EF 63% four months prior
• History of Blastocystis hominis in stool, s/p treatment x 2
• On very fixed po intake: “more than adequate” water consumption per family, but only tolerating 3-4 Boost Shakes per day
• +History of pneumonia recently

Labs
• WBC 8.1, Hb 7.1, Hct 21.3, Plt 194, Normal differential
• Na 134, K 6.2, Chloride 109, Bicarb 12, BUN 115, Creatinine 6.4
• NT-pro-BNP 2367

More Data?
• Cardiac Index Arterial Line started, with Cardiac Index ~2.9
• CVP 5-9
• SvO2 70-72

Discussion• Data suggesting overload:
– EXTREMELY hypoxic– Some fluctuating JVD– History of Diastolic Dysfunction– Poor lung exam with crackles
• Data suggesting dry– HISTORY– Probable pneumonia– Physical exam: Mucus membranes like the
Sahara desert– Response to fluid challenge – less tachycardia

Discussion (continued)
• Data negating overload– Got very tachycardic with removal of some
fluid with dialysis
• Data negating dry– Severely hypoxic

Discussion (continued)
• What takes precedence?– Tachycardia to 130?– Hypoxic with FiO2 100%?– ATN/Acute Renal Failure?

Discussion (continued)
• The preponderance of the data, including less tachycardia with fluid challenge, led to continued fluid hydration with improvement in tachycardia
• Oxygenation improved rather precipitously after the patient was moved for a CT Scan, suggesting mucus plug dislodging
• 3 days later, the patient finally mounted an elevated white blood cell count

Case # 9
• J.F., 45 year old female released from jail and immediately struck by a car, admitted as a Tier I Trauma
• Sustained multiple injuries: – Left severely comminuted and displaced mid-
shaft femur fracture– Left open tibia fracture– Splenic Laceration– C2 Fracture, stable

Case # 9
• Brought to the OR for Ex-lap and for washout and Ex-Fix of the left tibia
• Found to have hemoperitoneum and a splenic laceration necessitating splenectomy, washout, and the abdomen was left open with Ioban dressing over it
• Needed massive transfusion, including 20 Units of PRBCs, 12 Units of FFP, 2 Units of Platelets, and a large amount of crystalloid

Case # 9 (continued)
• The patient stabilized, with INR coming down to 1.2, blood pressure improving to low 100s, tachycardia persisting.
• At ~hour 19 of hospitalization, the patient developed progressive hypotension down to the 70s systolic, tachycardia with pulse up to 130.
• Crystalloid resuscitation was ordered, followed by blood and FFP with the thought that she was bleeding again

Case # 10 Picture
More History
Labs
More Data?

Vital Signs
• After 10 liters of NS + 2 Units PRBCs + 2 Units FFP in about 2 hours:
• 86/57, Pulse = 115 (down from 130), Respirations = 25, O2 Sat on FiO2 100%, PEEP 5 is 95%

Physical Exam
• Uncomfortable, bucking the ventilator• S1 S2 tachycardic, regular rhythm• Wheeze with prolonged expiratory phase• Abdomen with increasing distension, small
amount of serosanguinous fluid seen under the Ioban dressing
• Left thigh with posterior ecchymosis, not in traction, appearing significantly larger than the right thigh
• Total body (including facial) edema seen

Chest X-Ray

More History
• The patient also had blood coming from her Endotracheal tube suctioning
• Regarding patient-ventilator dyssynchrony, the Minute Ventilation had declined to between 3.5 to 4.5 Liters/minute
• The ventilator was pressure limited at Peak Pressures of 38, with tidal volumes as low as 160
• No change with Albuterol MDIs

More History (continued)
• Paralytics were attempted to make the patient stop bucking the ventilator
• Despite 70mg of Rocuronium, the patient continued to buck the ventilator
• After her Chest X-ray, the patient was noted to be no longer bucking the ventilator, with Vt of 270ml (set at 270ml) and peak pressures remaining 38
• Levophed was started for persistently low blood pressures

Labs
• Repeat ABG: 7.05/ 50 / 103 / 13 / -16 (90 minutes prior, ABG was
7.28 / 39 / 107 / 18 / -8)
• Hemoglobin on ABG 10.5
• Other labs pending

More Data?
• Bladder Pressure = 28

Discussion
• Abdominal Compartment Syndrome should be considered with hypotension, decreased urine output, and increased airway pressures in the face of massive IV hydration and fluid overload
• With taking up one side of the Ioban dressing to relieve pressure, the blood pressure increased to 90 and peak airway pressures improved to 29

Discussion (continued)
• The patient returned to the OR where a liver hematoma was found
• A retroperitoneal hematoma was seen on the left
• No significant active bleeding was seen• Bilateral Chest tubes were placed with
500ml removed from the right and 100ml from the left
• The abdomen was opened slightly further and left open, with better relief of pressure

Case # 10
• J.A., 47 year old Mexican male with a prolonged history of hypertension and diabetes
• Chief complaint of itching and nausea

Case # 10 Picture
Labs
Hospital Course

Vital Signs
• BP 165/90, Pulse 88, Respirations 18, Temperature 99, O2 Sat 99% on Room Air

Physical Exam
• Pleasant, in no distress, no respiratory distress
• No JVD
• S1 S2 RRR
• Lungs clear bilaterally
• Extensive excoriations on his back
• No peripheral edema

Chest X-Ray

Labs
• Sodium 137, K 4.8, Cl 102, Bicarb 19, BUN 150, Creatinine 16.7, Glucose 128, Corrected Calcium 6.6
• WBC 6.6, Hb 5.6, Platelet count 212

Hospital Course
• The patient was transfused 4 Units of PRBCs

Discussion
• The patient had normal vital signs and was not tachycardic despite his severe anemia
• It was probably reasonable to transfuse up to a hemoglobin of 7.0, though there is a significant risk of fluid overload with transfusion

Case # 11
• W.Y., 43 year old African American male with developmental delay, resident in a board and care
• Admitted through the ER with significant anxiety, shortness of breath, tachypnea, and fever, quickly intubated

Case # 10 Picture
More History
Labs
More Data?

Vital Signs
• BP 168/98, Pulse 118-125, Respirations in the 50s in the ER prior to intubation, now in the 20s, Temperature 102.2, O2 Sat 80% on Room Air

Physical Exam
• Moderate to severe respiratory distress prior to intubation
• No JVD appreciated
• S1 S2 tachycardic
• Lungs bibasilar crackles with diminished breath sounds at the right base
• No peripheral edema, very dry skin

Chest X-Ray

More History
• Treated with Amoxicillin for a Urinary Tract Infection 1 week prior to admission
• Developmentally delayed, with Tri-counties managing his care, but alert, interactive, and talking at baseline

Labs• Na 127, K 3.3, Chloride 100, Bicarb 15,
BUN 11, creatinine 2, Glucose 102• AST 17, ALT 27, Alk Phos 41• Total protein 17.7, Albumin 1.9• CRP 1.6, INR 1.5• WBC 7.8, Hb 4.9, Plt 229,000, 73% N,
10% Bands• Troponin 0.1, CK 256• NT-pro-BNP 124• UA 100 protein, Spec grav >1.030

More Info?
• CT Abdomen and Pelvis lytic lesions in the pelvis and an old T6 compression fracture

Discussion
• With his tachycardia, it would be reasonable to try to transfuse him to somewhere around a Hb=7.0
• However, with a total protein of 17.7, after 2 Units of PRBCs, his hemoglobin only went up to 5.6

Discussion (continued)
• Treatment of this patient to improve his anemia is actually to REMOVE PROTEIN through Plasmapheresis with saline repletion
• He received ~4 Units of PRBCs total, with Hb never getting above 5.8
• He became very intravascularly overloaded with the blood products, resolved with plasmapheresis
• Strep pneumonia grew out from blood cultures

Discussion (continued)
• He has undergone chemotherapy with Velcade, thalidomide, and Decadron, with improvement in his IgG down to 1350mg as of 11/3/08, and will undergo two more cycles followed by thalidomide as maintenance therapy for his Multiple Myeloma

Case #12
• R.W., 30 year old female with a significant psychiatric history, s/p multiple suicide attempts in the past, admitted after a polysubstance overdose with Wellbutrin, Lexapro, Lisinopril, Hydrochlorothiazide, and washed down with Isopropyl Alcohol
• Started bradying down in the ER, followed by PEA after intubation

Case #12 (continued)
• Initial ABG with pH < 6.76, PCO2 62, PO2 232 while being bagged during CPR
• With Epinephrine and Chest Compressions, the patient regained a pulse and was brought up to the ICU
• Central line was placed and large volume fluid resuscitation was initiated
• The patient received 6 amps of sodium bicarbonate and Levophed and Dopamine at maximum dose were quickly titrated to maximum dose of both

Case # 10 Picture
More History
Labs
More Data?

Vital Signs
• Blood pressure from the arterial line 72/50
• Pulse 115, Respirations 18 riding the ventilator
• O2 Sat unobtainable due to low blood pressure; PaO2 on 100% FiO2 = 91

Physical Exam
• Intubated, occasionally overbreathing the ventilator with increase in peak airway pressures to the high 30s
• S1 S2 tachycardic and distant• Lungs mostly clear• Abdomen distended, not soft• No peripheral edema• Warm• Intact femoral pulses even with BP in 60s
by the arterial line

Chest X-Ray

More History
• Bedside echocardiogram in the ED revealed relatively intact cardiac function
• Formal echocardiogram the following day revealed an EF of 71%, some mild LVH with diastolic dysfunction

Labs
• Initial ABG: pH<6.76/PCO2 62/ PO2 230/ Bicarb 7, Base Deficit -30
• Lactic Acid 26.4• Next ABG: 7.17/ 33/ 98/ 12/ -15• Next ABG: 7.46/ 25/ 50/ 17/ -5, Hb 10.5• WBC 12.4, Hb 16.5, Plt 419• Na 138, K 3.2, Chloride 97, Bicarb 14,
BUN 6, Creatinine 1.2, Calcium 10, LFTs nl, Salicylates 4.2, Acetaminophen <2, Serum Osm 305

More Info?
• CVP = 26
• SvO2 = 45
• Temperature Normal at 97.6

Discussion
• During refractory hypotension, it is VITAL to have a normal temperature and a normal pH in order for your pressors to work
• The CVP was very helpful in managing therapy
• Dobutamine was tried without benefit; pressors were overall lowered as IV Fluids were turned down, with decline in the CVP over the following 12 hours to single digits

Discussion (continued)
• The patient strangely responded to boluses of IV calcium (with an increase in SBP by 20 with each calcium bolus)
• Glucagon was ineffective
• Family members were unable to find any calcium channel blocker bottles at home or in the garbage
• Intra-lipid infusion was given to unbind the Wellbutrin from binding sites to then eliminate it

Discussion (continued)
• In all ingestions, checking an Osmolar Gap is very important (Calculated Osm = 2(Na) + BUN/2.8 + Glucose/18)
• Poison Control can be a great resource• Isopropyl alcohol in excess of an Osmolar
Gap of 100 can cause cardiovascular collapse, but lower doses generally don’t
• The patient was presented at Poison Control’s Grand Rounds yesterday.

References
• Tung R, et al. Utility of B-type Natriuretic Peptide for the Evaluation of Intensive Care Unit Shock. Crit Care Med 2004; 32: 1643-47.
• Resuscitation end points in severe sepsis: Central venous pressure, mean arterial pressure, mixed venous oxygen saturation, and … intra-abdominal pressure. Crit Care Med 2008; 36 (3): 1012-13.
• Vincent JL, et al. Fluid Challenge Revisited. Crit Care Med 2006; 34 (5): 1333-7.
• Michard F, et al. Predicting Fluid Responsiveness in ICU Patients. Chest 2002; 121: 2000-8.
• A Comparison of Albumin and Saline for Fluid Resuscitation in the Intensive Care Unit. New Engl J Med 2004; 350: 2247-56.
• Koustova E, et al. Effects of Lactated Ringers Solutions on Human Leukocytes. J Trauma. 2002; 52(5): 872-8. Phua J, et al. Lactate, Procalcitonin, and Amino-Terminal Pro-B-Type Natriuretic Peptide Verses Cytokine Measurements and Clinical Severity Scores for Prognostication in Septic Shock. Shock. 2008; 29 (3): 328-333.

References
• Murphy G, et al. Increased Mortality, Post-operative Morbidity, and Cost after Red Blood Cell Transfusion in Patients Having Cardiac Surgery. Circulation. 2007; 116: 2544-52.
• Janette O’Neal, VCMC Blood Bank Director, 2008.• DeLoughery T. Blood Component Therapy. SCCM 2007 Critical
Care Review Course.• Canadian Critical Care Trials Group. Transfusion Requirements in
Critical Care. New Engl J Med 1999; 340 (6): 409-17.• Hebert P, et al. Contraversies in RBC Transfusion in the Critically Ill.
Chest 2007; 131 (5): 1583-90.