Embed Size (px)
Citation preview
Diabetes und KHK
Carsten Tschöpe
ESC-update 2015
• TECOS -> Sitagliptin
• ELIXA -> Lixisenatide
• EMPARG -> Empagliflozin
• ALBATROSS -> Aldosteron Inhibition
• ARTS-HF -> Finerenone
• BACC -> Troponin bei ACS
Bellytina64
• TECOS -> Sitagliptin
• ELIXA -> Lixisenatide
• EMPARG -> Empagliflozin
• ALBATROS -> Aldosteron Inhibition
• ARTS-HF -> Finerenone
• BACC -> Troponin bei ACS
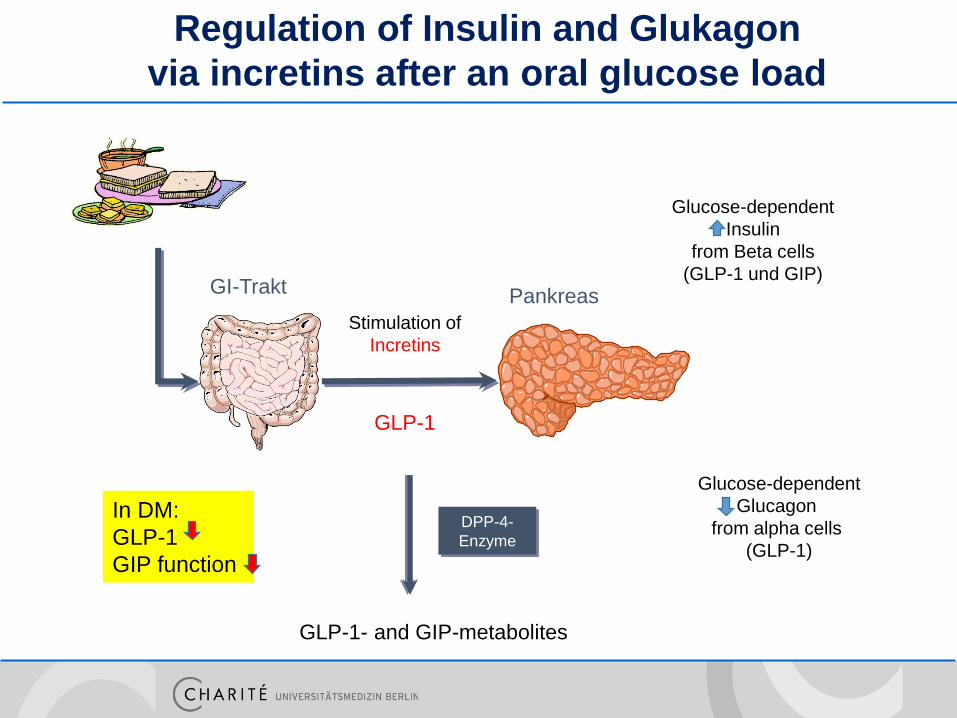
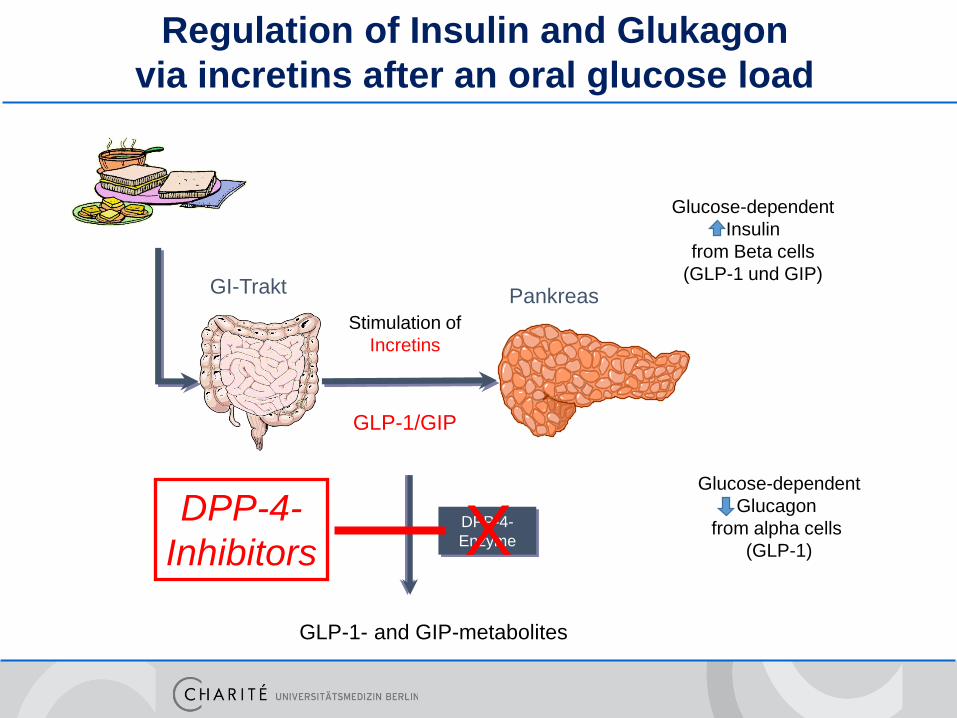
GLP-1- and GIP-metabolites
DPP-4-
Enzyme
GLP-1
Stimulation of
Incretins
PankreasGI-Trakt
Glucose-dependent
Glucagon
from alpha cells
(GLP-1)
Glucose-dependent
Insulin
from Beta cells
(GLP-1 und GIP)
Regulation of Insulin and Glukagon
via incretins after an oral glucose load
In DM:
GLP-1
GIP function
GLP-1- and GIP-metabolites
DPP-4-
Enzyme
GLP-1/GIP
Stimulation of
Incretins
PankreasGI-Trakt
Glucose-dependent
Glucagon
from alpha cells
(GLP-1)
Glucose-dependent
Insulin
from Beta cells
(GLP-1 und GIP)
Regulation of Insulin and Glukagon
via incretins after an oral glucose load
XDPP-4-
Inhibitors
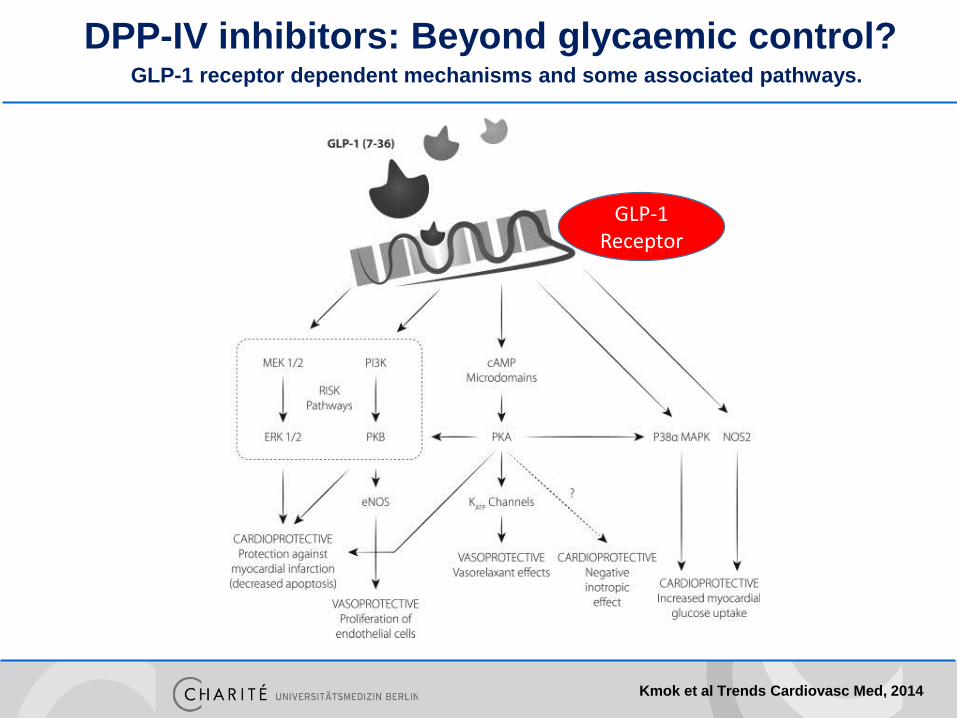
GLP-1 receptor dependent mechanisms and some associated pathways.
Kmok et al Trends Cardiovasc Med, 2014
DPP-IV inhibitors: Beyond glycaemic control?
GLP-1 Receptor
Saxagliptin and Cardiovascular Outcomes in Patients with Type 2 Diabetes Mellitus
Benjamin M. Scirica, M.D., M.P.H., Deepak L. Bhatt, M.D., M.P.H., Eugene Braunwald, M.D., P. Gabriel Steg, M.D., Jaime Davidson, M.D., Boaz Hirshberg,
M.D., Peter Ohman, M.D., Robert Frederich, M.D., Ph.D., Stephen D. Wiviott, M.D., Elaine B. Hoffman, Ph.D., Matthew A. Cavender, M.D., M.P.H., Jacob A. Udell, M.D.,
M.P.H., Nihar R. Desai, M.D., M.P.H., Ofri Mosenzon, M.D., Darren K. McGuire, M.D., Kausik K. Ray, M.D., Lawrence A. Leiter, M.D., Itamar Raz, M.D., for the
SAVOR-TIMI 53 Steering Committee and Investigators
N Engl J MedVolume 369(14):1317-1326
October 3, 2013
Scirica BM et al. N Engl J Med 2013
SAVOR-TIMI 53
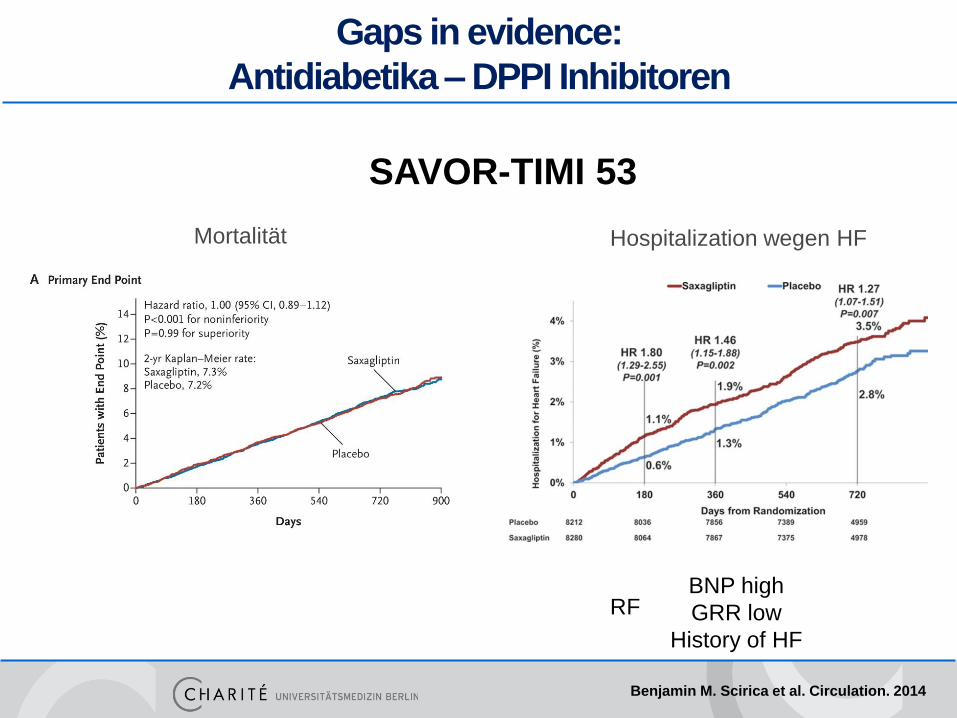
Gaps in evidence:
Antidiabetika – DPPI Inhibitoren
Benjamin M. Scirica et al. Circulation. 2014
SAVOR-TIMI 53
Mortalität Hospitalization wegen HF
BNP high
GRR low
History of HF
RF
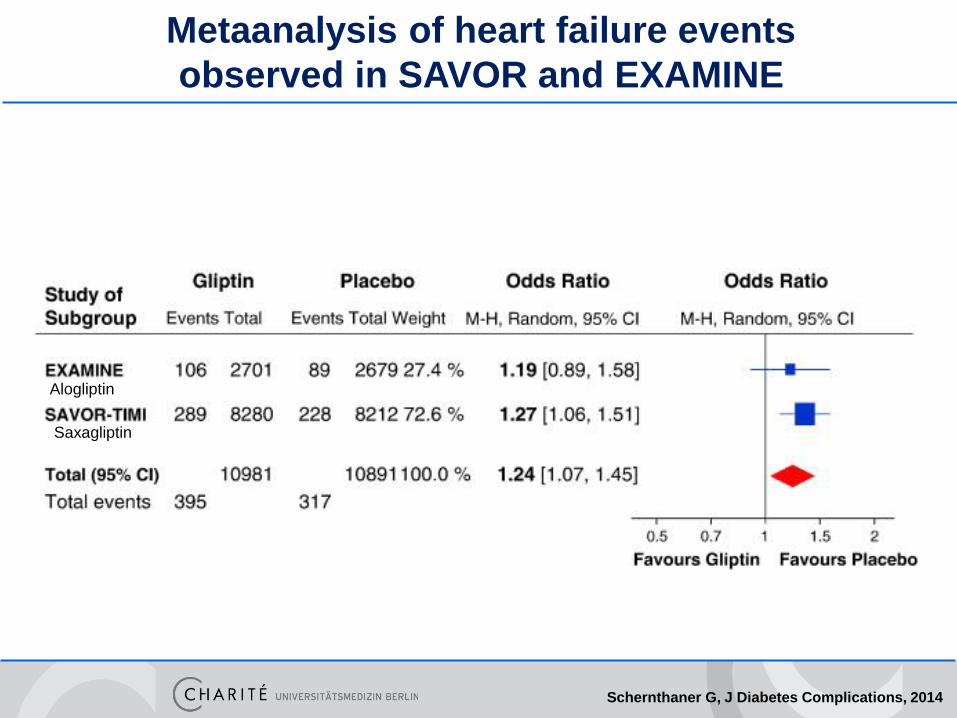
Metaanalysis of heart failure events
observed in SAVOR and EXAMINE
Schernthaner G, J Diabetes Complications, 2014
Alogliptin
Saxagliptin
Primary Objective
To demonstrate that the risk of cardiovascular events
in patients treated with sitagliptin in addition to usual
care was non-inferior to that in patients treated
without sitagliptin in addition to usual care.
Green JB et al. NEJM 2015
Primary Composite Cardiovascular Outcome
Time to first occurrence of:
• Cardiovascular-related death
• Nonfatal myocardial infarction
• Nonfatal stroke
• Hospitalization for unstable angina
A Clinical Endpoints Committee, blinded to therapy allocation, reviewed all potential CVD endpoints independently.
Green JB et al. NEJM 2015
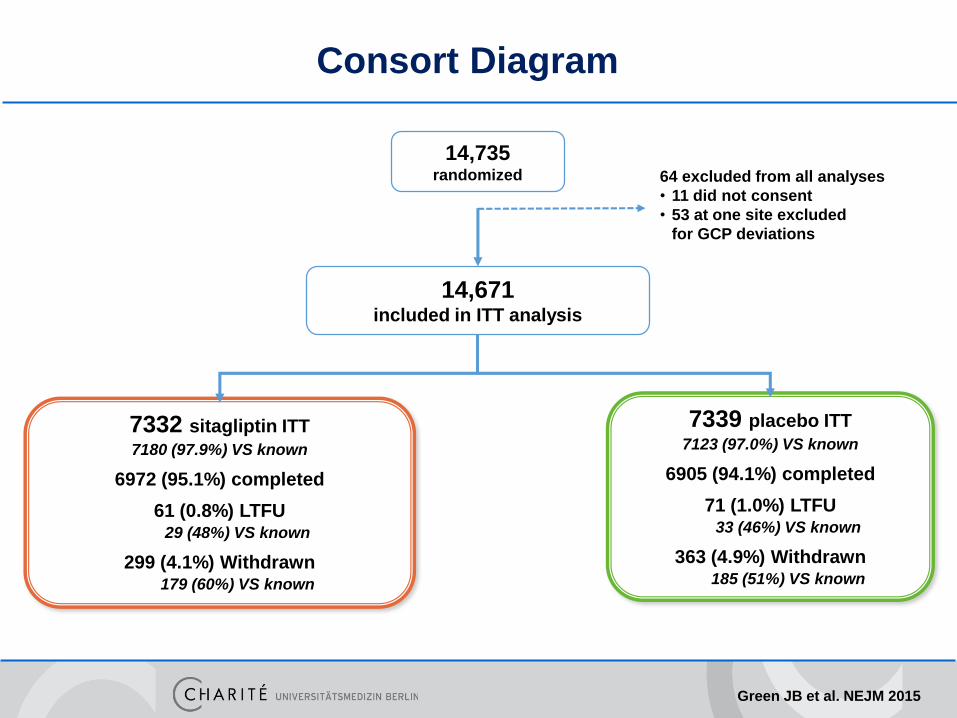
Consort Diagram
14,735randomized 64 excluded from all analyses
• 11 did not consent
• 53 at one site excluded
for GCP deviations
14,671included in ITT analysis
7332 sitagliptin ITT
7180 (97.9%) VS known
6972 (95.1%) completed
61 (0.8%) LTFU29 (48%) VS known
299 (4.1%) Withdrawn179 (60%) VS known
7339 placebo ITT
7123 (97.0%) VS known
6905 (94.1%) completed
71 (1.0%) LTFU33 (46%) VS known
363 (4.9%) Withdrawn185 (51%) VS known
Green JB et al. NEJM 2015
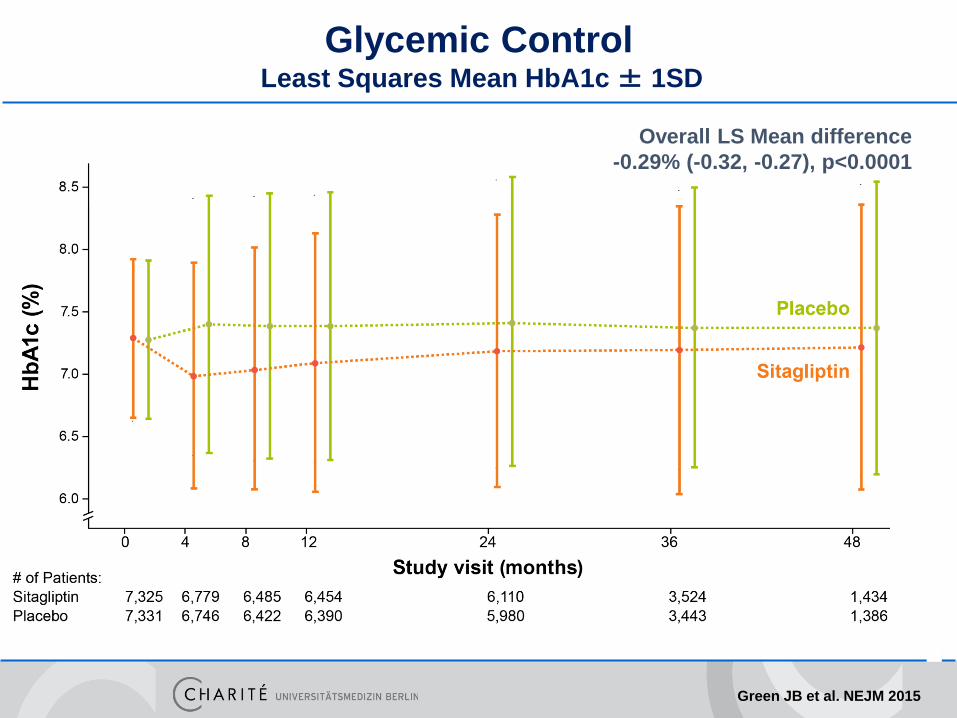
Glycemic ControlLeast Squares Mean HbA1c ± 1SD
Overall LS Mean difference
-0.29% (-0.32, -0.27), p<0.0001
Green JB et al. NEJM 2015
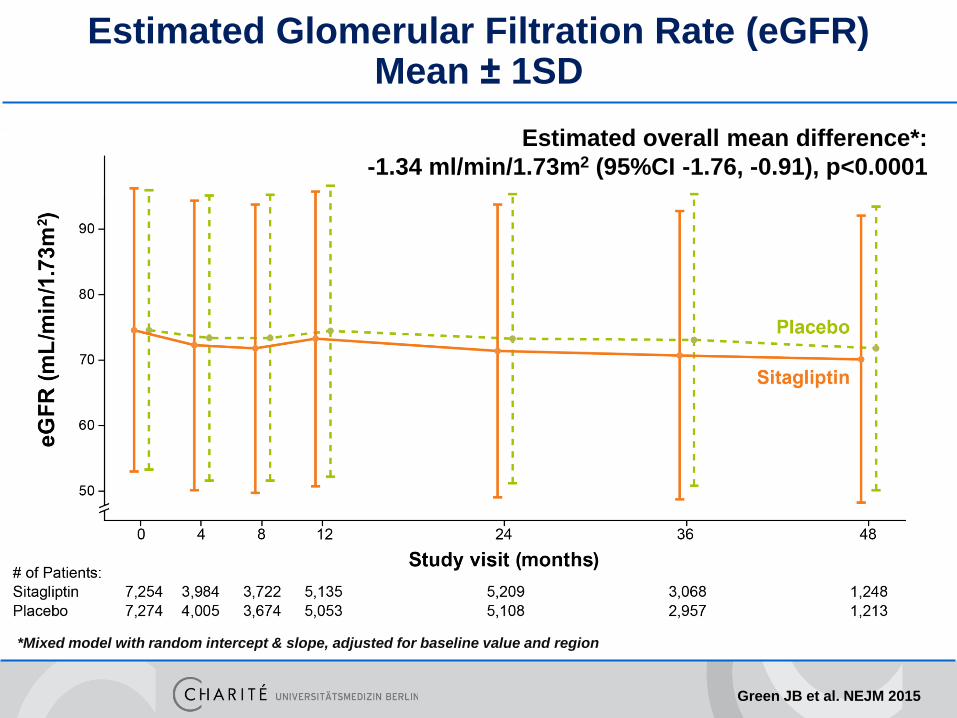
Estimated Glomerular Filtration Rate (eGFR)Mean ± 1SD
*Mixed model with random intercept & slope, adjusted for baseline value and region
Estimated overall mean difference*:
-1.34 ml/min/1.73m2 (95%CI -1.76, -0.91), p<0.0001
Green JB et al. NEJM 2015
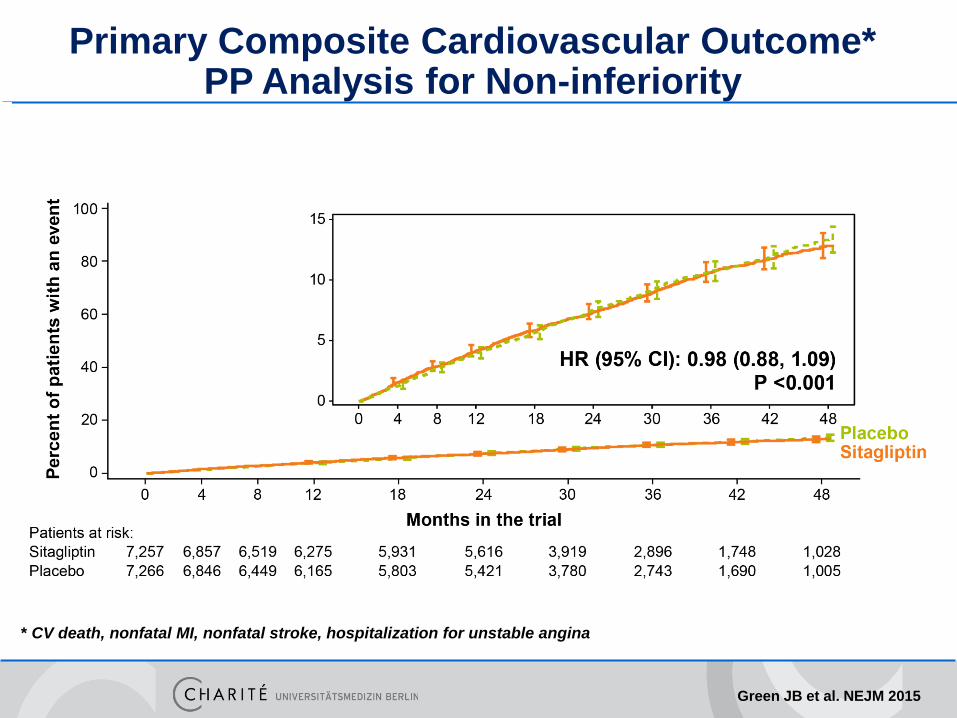
Primary Composite Cardiovascular Outcome* PP Analysis for Non-inferiority
* CV death, nonfatal MI, nonfatal stroke, hospitalization for unstable angina
Green JB et al. NEJM 2015
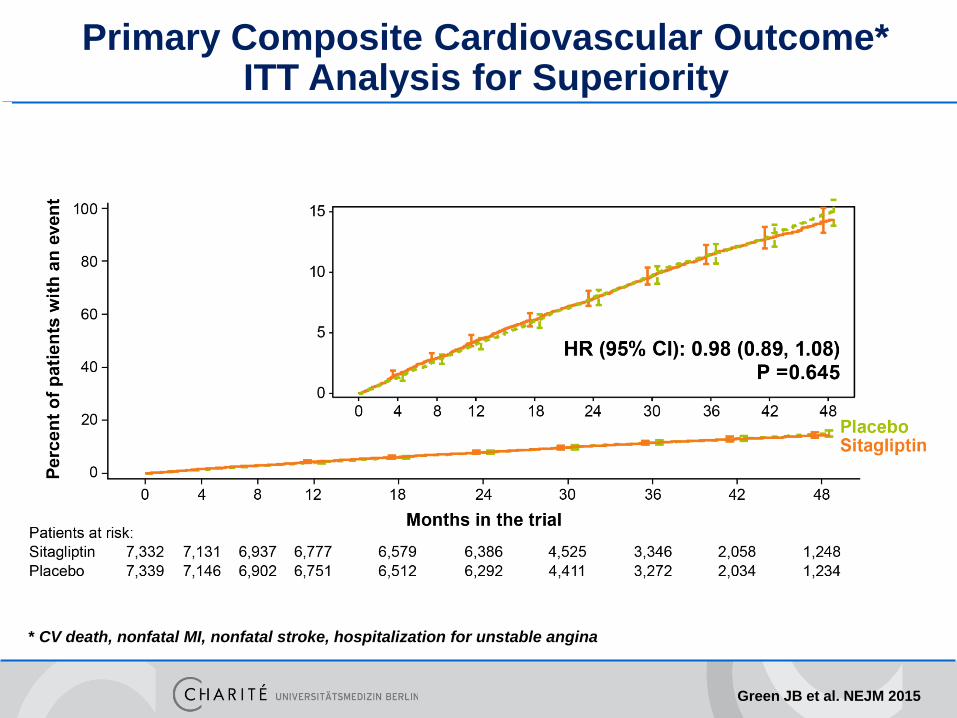
Primary Composite Cardiovascular Outcome* ITT Analysis for Superiority
* CV death, nonfatal MI, nonfatal stroke, hospitalization for unstable angina
Green JB et al. NEJM 2015
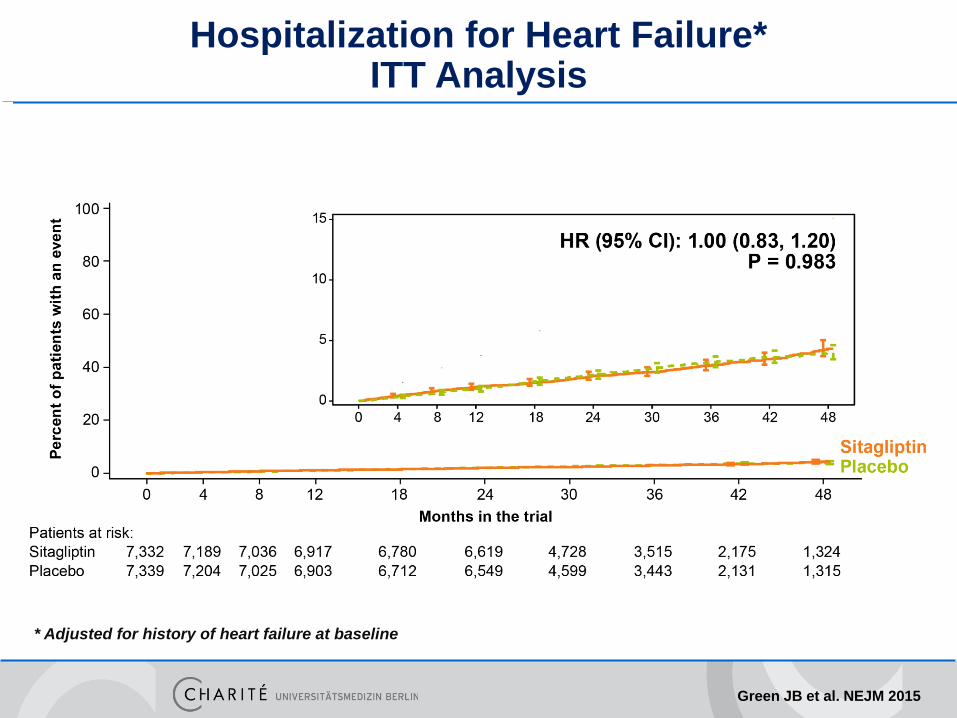
Hospitalization for Heart Failure*ITT Analysis
* Adjusted for history of heart failure at baseline
Green JB et al. NEJM 2015
Summary of Results (1)
• For the primary composite cardiovascular outcome(CV death, nonfatal MI, nonfatal stroke, or hospitalization for unstable angina) sitagliptin, compared with placebo, was noninferior, and not superior
• For the secondary composite cardiovascular outcome(CV death, nonfatal MI, or nonfatal stroke) sitagliptin, compared with placebo, was noninferior, and not superior
• The rate of hospitalization for heart failure did not differ between sitagliptin and placebo treatment groups
• The incidence of severe hypoglycemia did not differ between sitagliptin and placebo treatment groups
Green JB et al. NEJM 2015
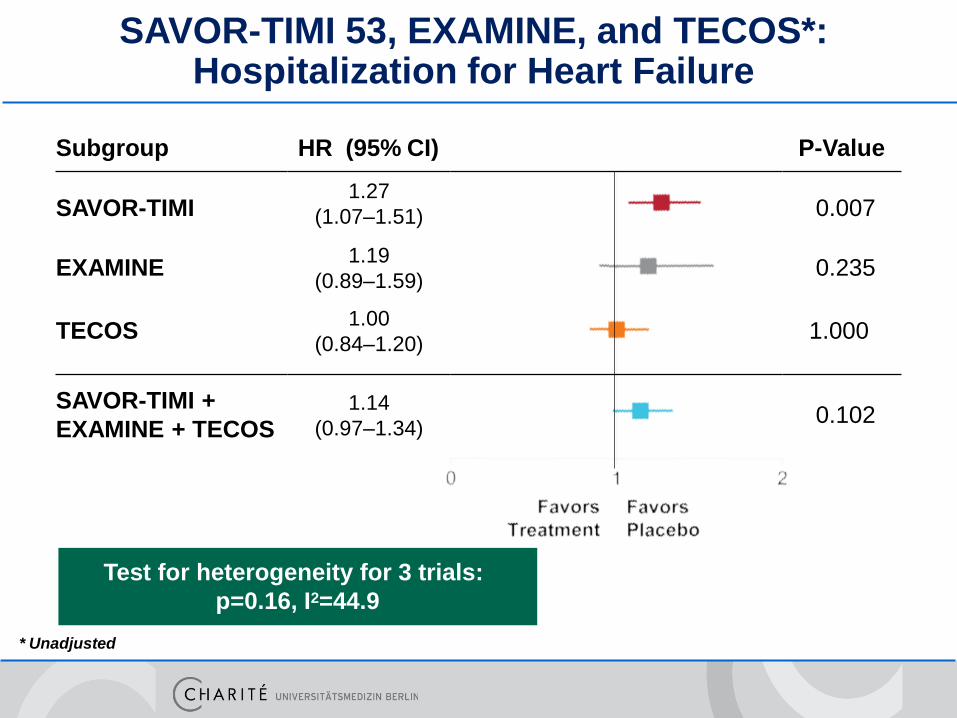
Subgroup HR (95% CI) P-Value
SAVOR-TIMI 0.007
EXAMINE 0.235
TECOS
1.27
(1.07–1.51)
1.19
(0.89–1.59)
1.00
(0.84–1.20)1.000
SAVOR-TIMI +
EXAMINE + TECOS1.14
(0.97–1.34)0.102
SAVOR-TIMI 53, EXAMINE, and TECOS*:Hospitalization for Heart Failure
* Unadjusted
Test for heterogeneity for 3 trials:
p=0.16, I2=44.9
• TECOS -> Sitagliptin
• ELIXA -> Lixisenatide
• EMPARG -> Empagliflozin
• ALBATROS -> Aldosteron Inhibition
• ARTS-HF -> Finerenone
• BACC -> Troponin bei ACS
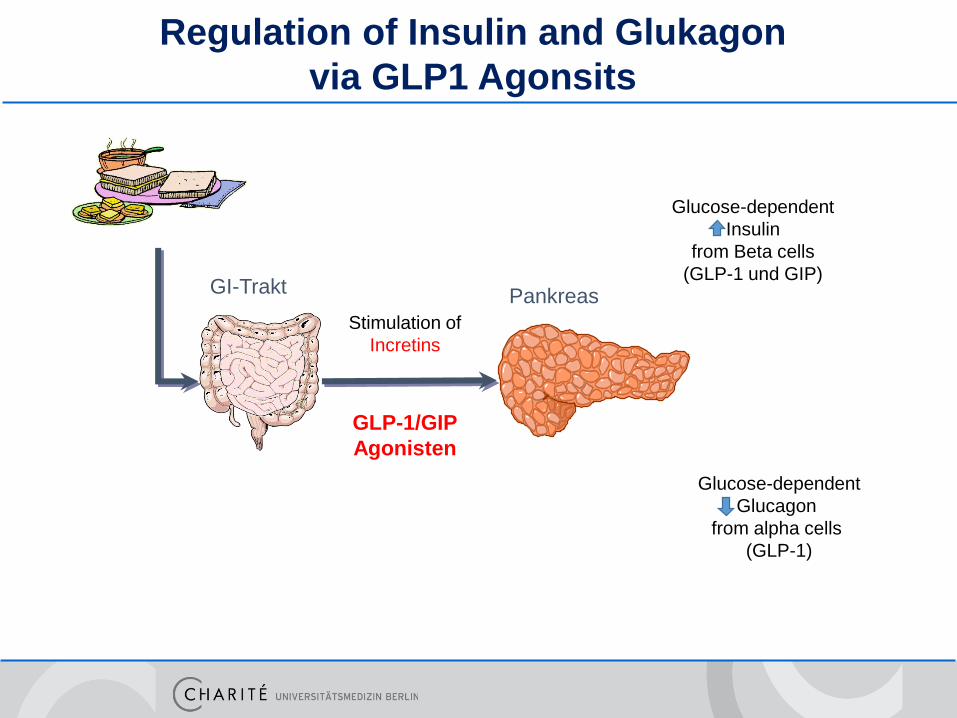
GLP-1/GIP
Agonisten
Stimulation of
Incretins
PankreasGI-Trakt
Glucose-dependent
Glucagon
from alpha cells
(GLP-1)
Glucose-dependent
Insulin
from Beta cells
(GLP-1 und GIP)
Regulation of Insulin and Glukagon
via GLP1 Agonsits
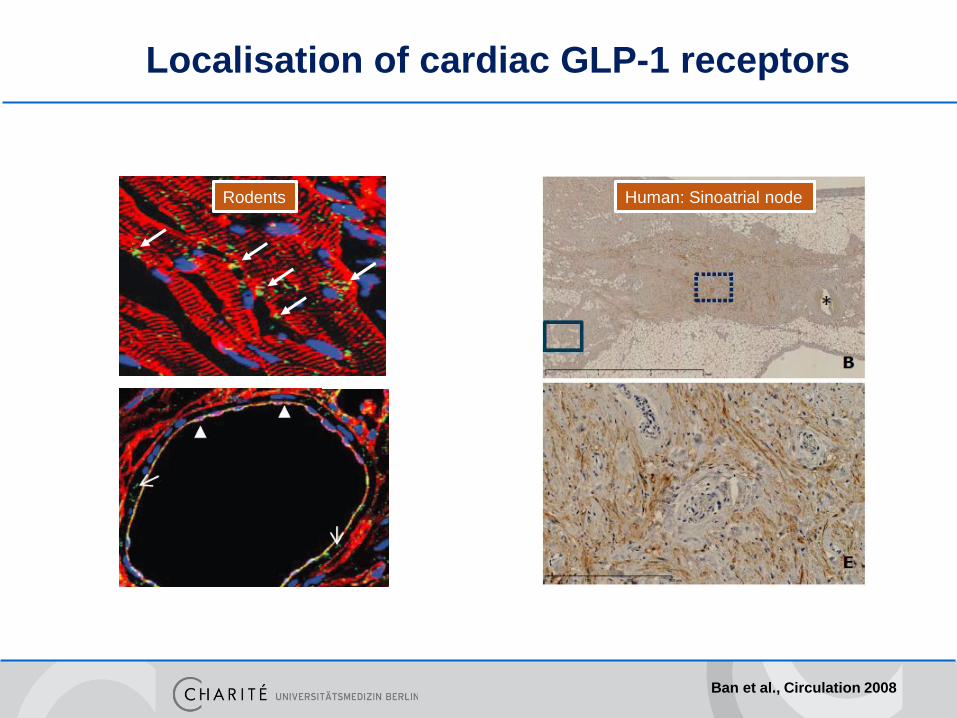
Localisation of cardiac GLP-1 receptors
Pyke et al., Endocrinology 2014
Human: Sinoatrial node
Ban et al., Circulation 2008
Rodents
Ussher, Circ Res 2014
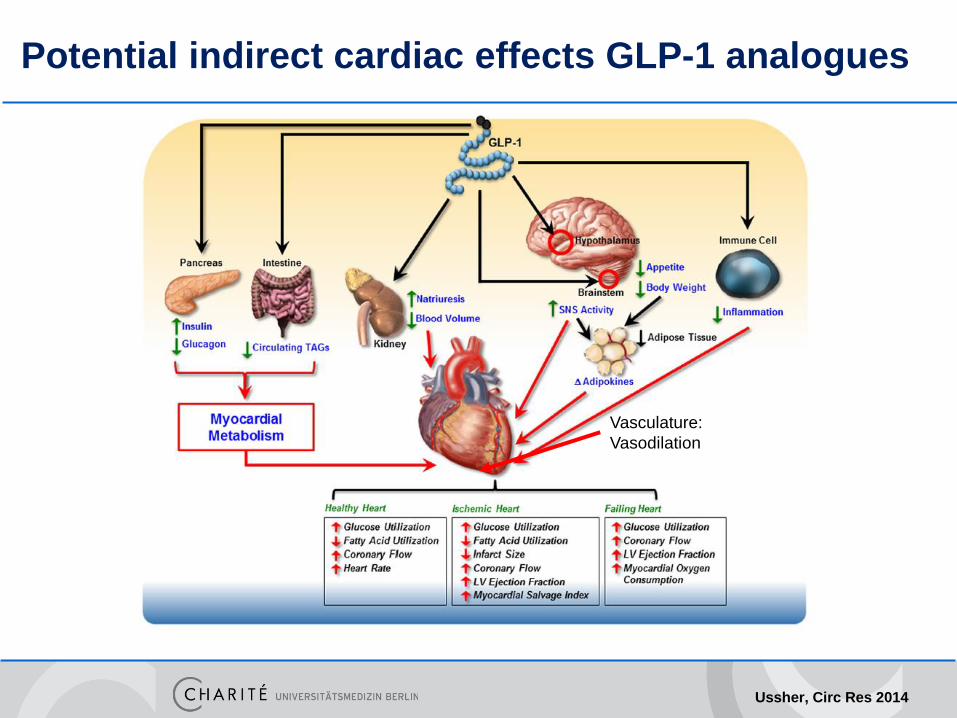
Potential indirect cardiac effects GLP-1 analogues
Vasculature:
Vasodilation
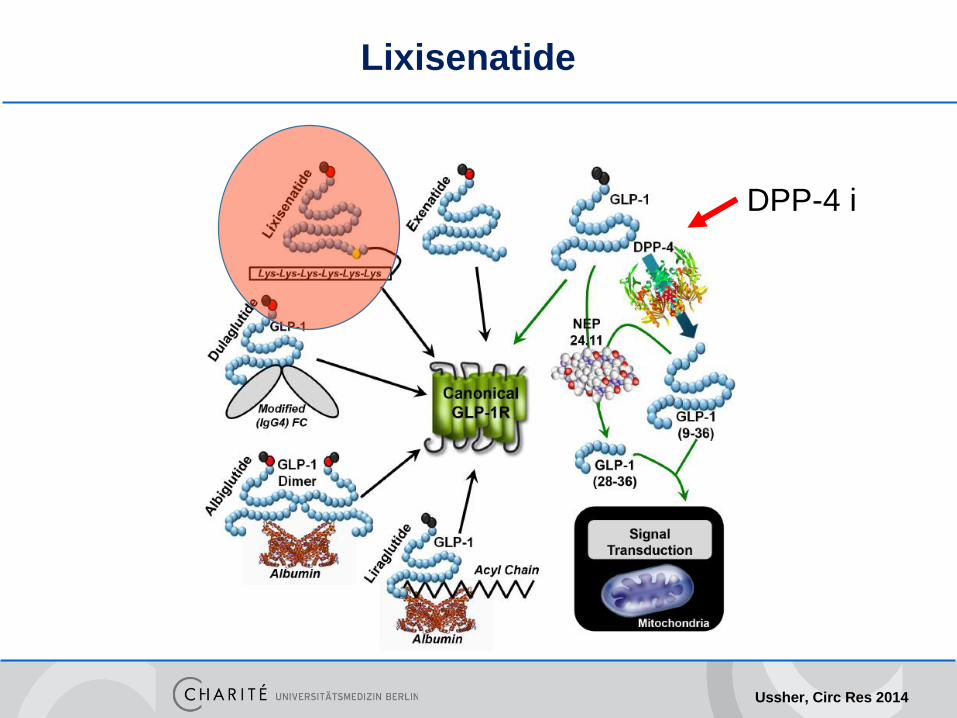
DPP-4 i
Lixisenatide
Ussher, Circ Res 2014
Evaluation of LIXisenatide in
Acute Coronary Syndrome (ELIXA)
ESC 31 August 2015 Hot Line III -Diabetes mellitus/Pharmacology
Eldrin F. Lewis, MD, MPH Associate Professor of Medicine Harvard
Medical School Brigham and Women’s Hospital
ELIXA Trial Executive Committee:
Rafael Diaz, Kenneth Dickstein, Hertzel Gerstein, Lars Køber, Eldrin Lewis, Aldo
Maggioni, John McMurray, Marc Pfeffer (Chair),
Jeffrey Probstfield, Matthew Riddle, Scott Solomon, Jean-Claude Tardif
on behalf of the ELIXA Investigators
Trial Design
• Randomized, double-blind, placebo-controlled event-driven trial
• Patients with Type 2 DM within 180 days of ACS
• Run-in period of 7 days; trained in self-administration of daily SC
volume-matched placebo
• Lixisenatide or matching placebo (1:1)
– Initial dose 10 µg/day
– Down- or up-titration permitted to maximum of 20 µg/day
• Glucose control managed by site investigators’ judgment
AHJ 2015
Endpoints
• Primary (Composite)
- CV death, Non-fatal MI, Non-fatal stroke, Hospitalization for
unstable angina (UA)
• Secondary and Other
- Primary endpoint + hospitalization for HF
- Primary endpoint + hospitalization for HF + coronary
revascularizatio
- All-cause death
- HF hospitalization
- CV death + HF hospitalization
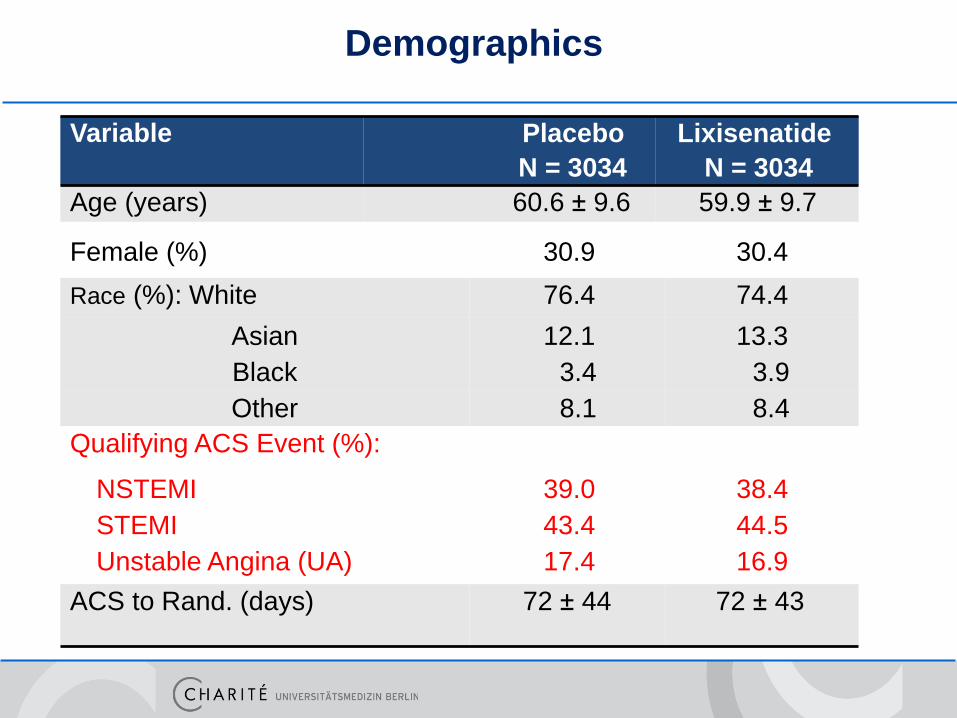
Variable Placebo
N = 3034
Lixisenatide
N = 3034
Age (years) 60.6 ± 9.6 59.9 ± 9.7
Female (%) 30.9 30.4
Race (%): White 76.4 74.4
Asian 12.1 13.3
Black 3.4 3.9
Other 8.1 8.4
Qualifying ACS Event (%):
NSTEMI 39.0 38.4
STEMI 43.4 44.5
Unstable Angina (UA) 17.4 16.9
ACS to Rand. (days) 72 ± 44 72 ± 43
Demographics
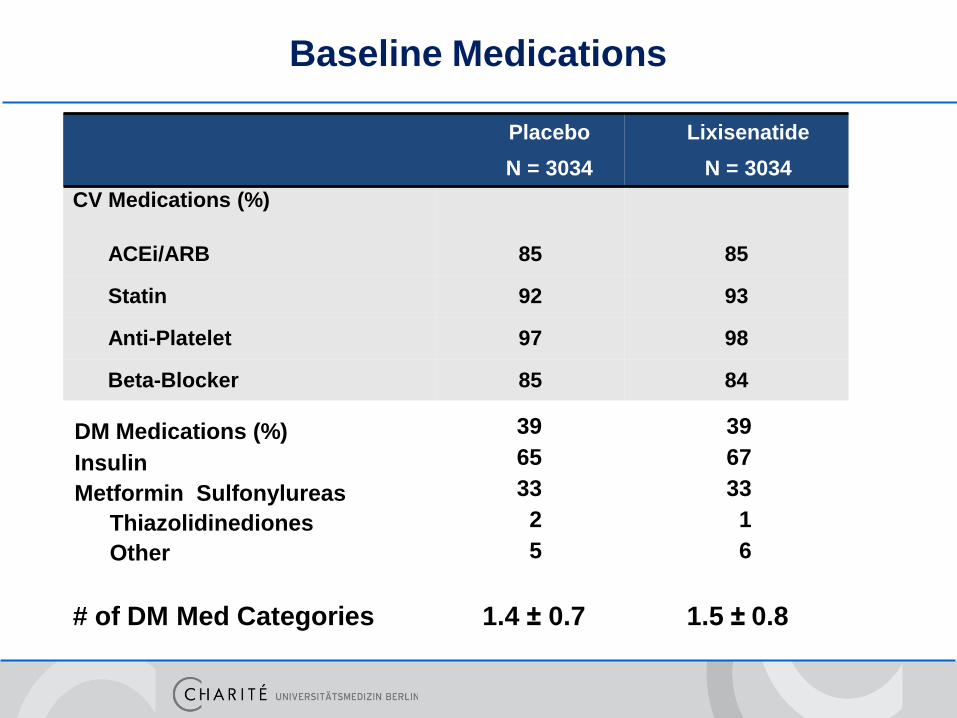
Placebo
N = 3034
Lixisenatide
N = 3034
CV Medications (%)
ACEi/ARB 85 85
Statin 92 93
Anti-Platelet 97 98
Beta-Blocker 85 84
DM Medications (%)
Insulin
Metformin Sulfonylureas
Thiazolidinediones
Other
39
65
33
2
5
39
67
33
1
6
# of DM Med Categories 1.4 ± 0.7 1.5 ± 0.8
Baseline Medications
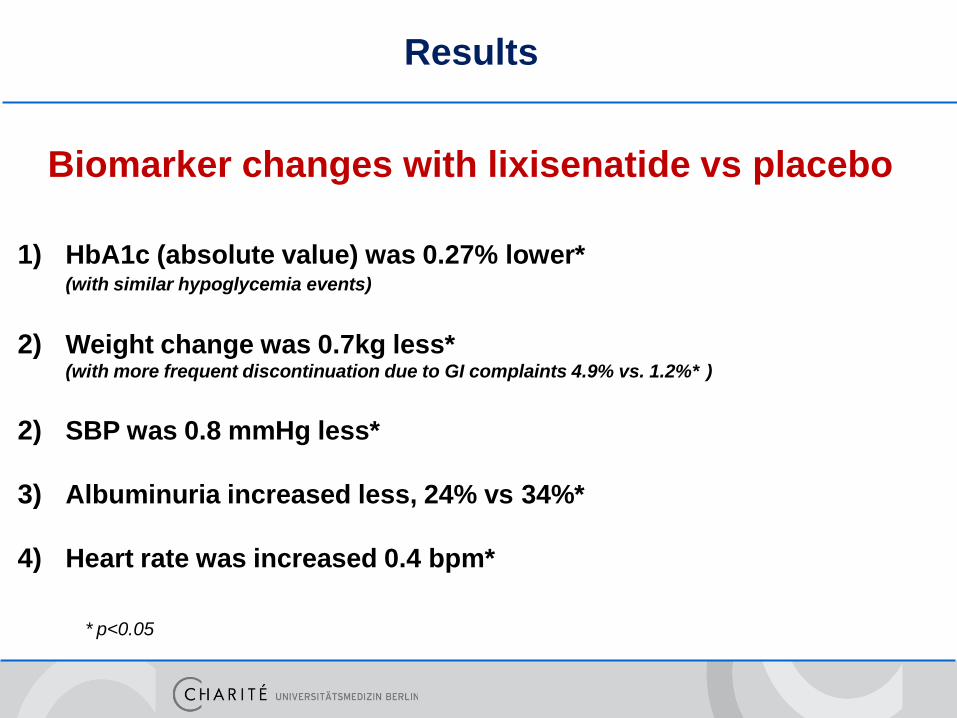
Results
Biomarker changes with lixisenatide vs placebo
1) HbA1c (absolute value) was 0.27% lower*(with similar hypoglycemia events)
2) Weight change was 0.7kg less*(with more frequent discontinuation due to GI complaints 4.9% vs. 1.2%* )
2) SBP was 0.8 mmHg less*
3) Albuminuria increased less, 24% vs 34%*
4) Heart rate was increased 0.4 bpm*
* p<0.05
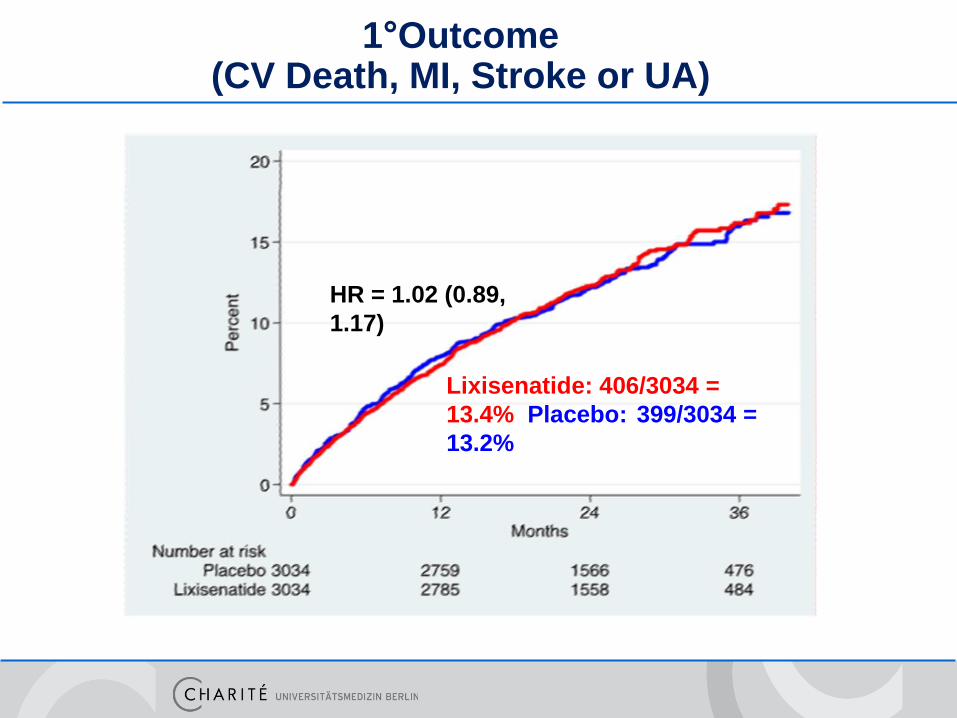
1°Outcome (CV Death, MI, Stroke or UA)
Lixisenatide: 406/3034 =
13.4% Placebo: 399/3034 =
13.2%
HR = 1.02 (0.89,
1.17)
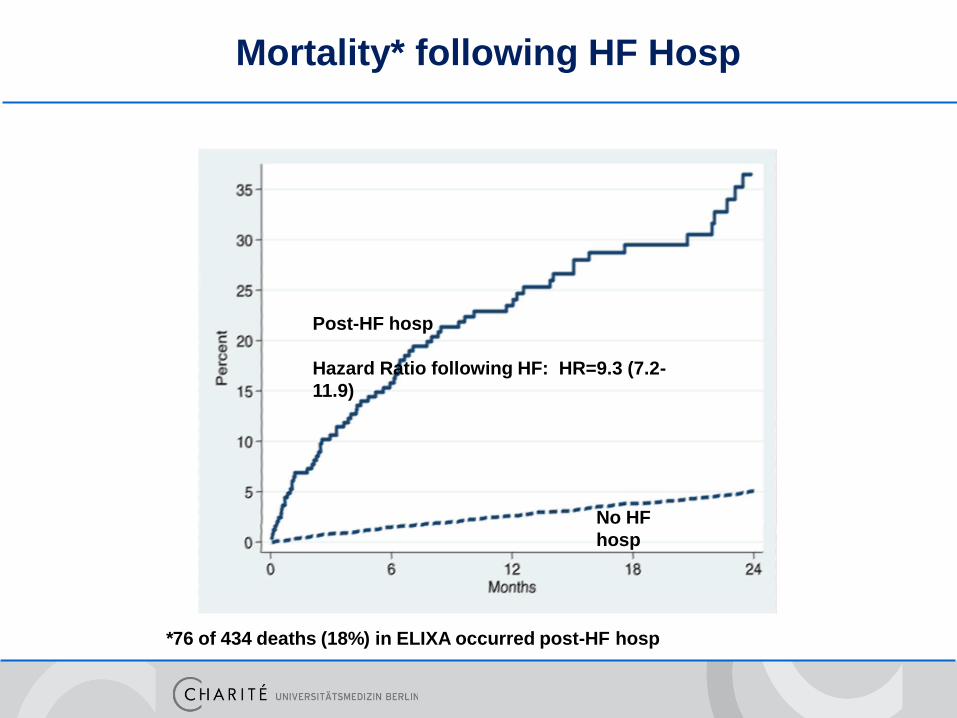
No HF
hosp
Post-HF hosp
Hazard Ratio following HF: HR=9.3 (7.2-
11.9)
*76 of 434 deaths (18%) in ELIXA occurred post-HF hosp
Mortality* following HF Hosp
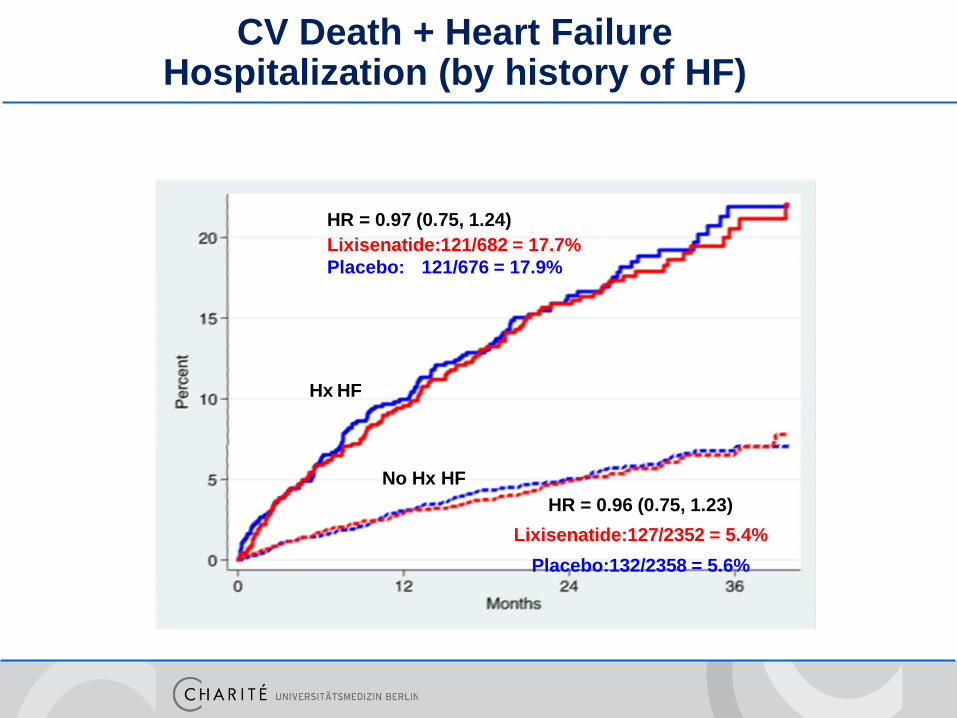
CV Death + Heart Failure Hospitalization (by history of HF)
HR = 0.97 (0.75, 1.24)
Lixisenatide:121/682 = 17.7%
Placebo: 121/676 = 17.9%
Hx HF
No Hx HF
HR = 0.96 (0.75, 1.23)
Lixisenatide:127/2352 = 5.4%
Placebo:132/2358 = 5.6%
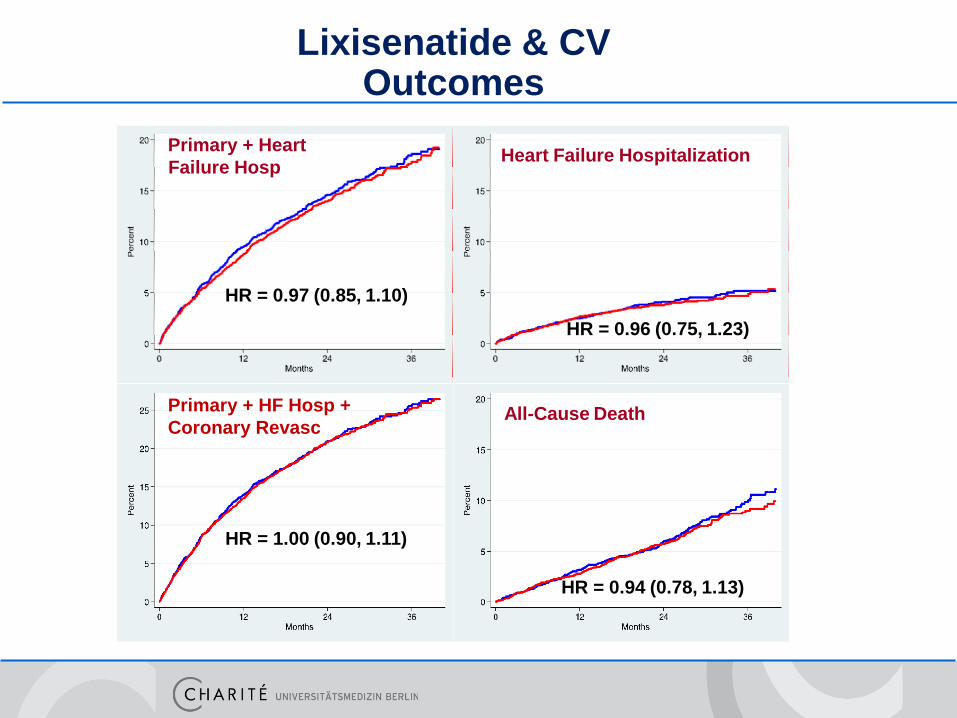
Lixisenatide & CVOutcomes
Primary + Heart
Failure Hosp
HR = 0.97 (0.85, 1.10)
Heart Failure Hospitalization
HR = 0.96 (0.75, 1.23)
HR = 0.94 (0.78, 1.13)
All-Cause DeathPrimary + HF Hosp +
Coronary Revasc
HR = 1.00 (0.90, 1.11)
ELIXA Summary
• Demonstrates CV safety of lixisenatide (as defined by FDA
Guidance), but not superiority in reducing CV events
• Additional analyses indicate safety with respect to heart
failure events as well as death
• Neutral effects seen across wide spectrum of heart failure
risk
ELIXA: what does it mean ?
• CV safety of lixisenatide in post ACS patients appears
excellent
• No signal of increase in risk of HF
• Probably does not rule out a genuine CV benefit
– Diabetes is long standing
– Follow up is too short
0 5 10 15 20 25
Years since randomization
Pro
po
rtio
nw
ith
even
t
1.0
0.8
0.6
0.4
0.2
0
Conventional (n = 1138)
Sulfonylurea/Insulin (n = 2729)
0 5 10 15 20 25
Years since randomization
Pro
po
rtio
nw
ith
even
t
1.0
0.8
0.6
0.4
0.2
0
33% reduction
P = 0.005
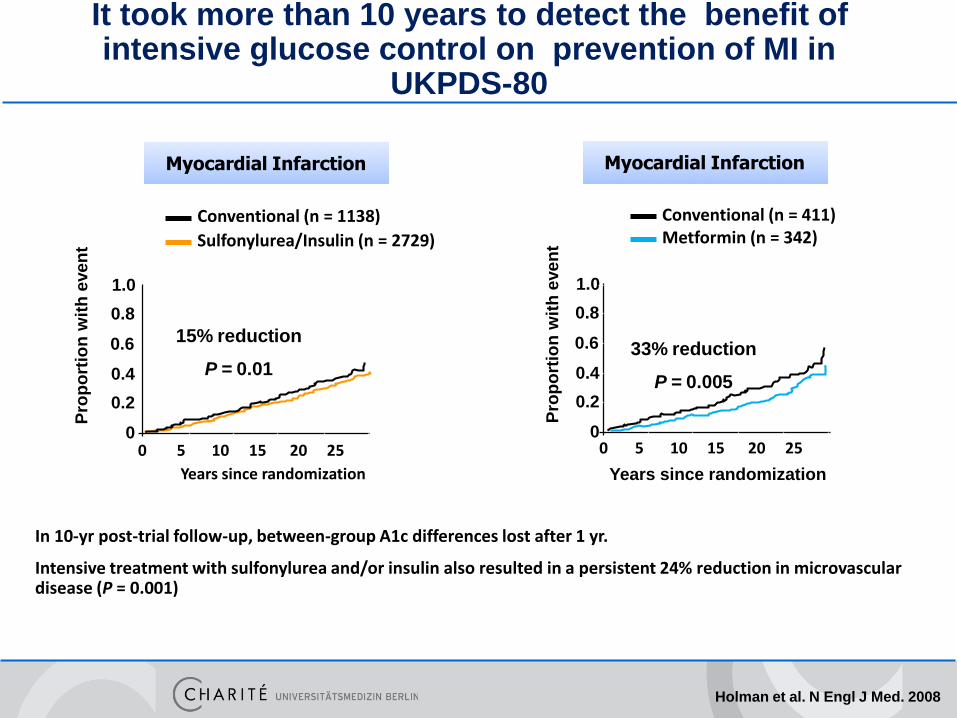
Holman et al. N Engl J Med. 2008
15% reduction
P = 0.01
In 10-yr post-trial follow-up, between-group A1c differences lost after 1 yr.
Intensive treatment with sulfonylurea and/or insulin also resulted in a persistent 24% reduction in microvascular disease (P = 0.001)
Conventional (n = 411) Metformin (n = 342)
It took more than 10 years to detect the benefit of intensive glucose control on prevention of MI in
UKPDS-80
Myocardial Infarction Myocardial Infarction
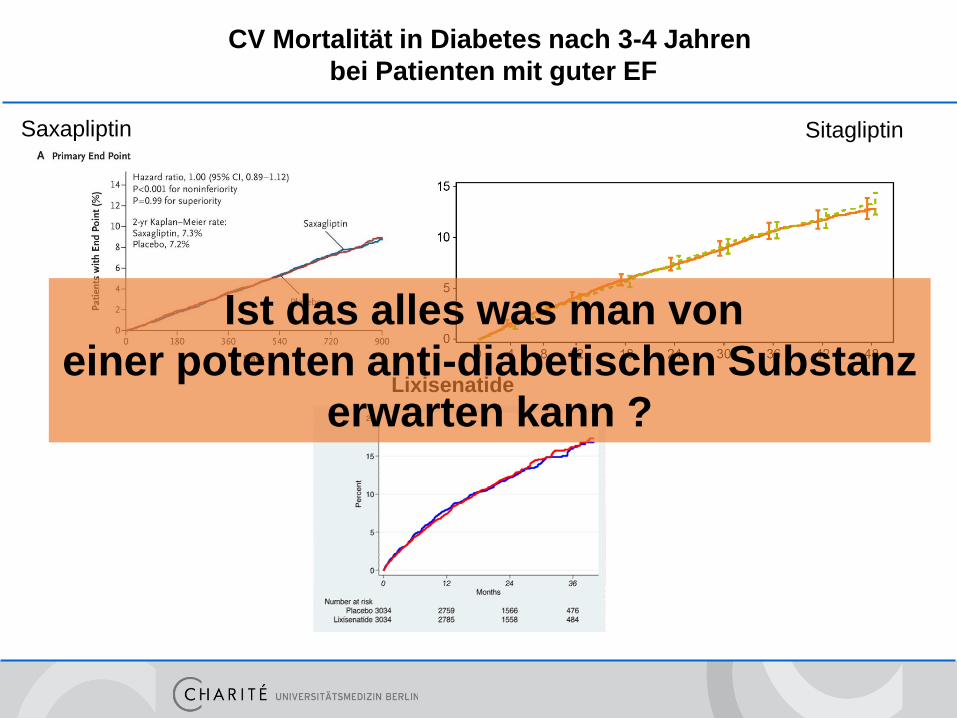
CV Mortalität in Diabetes nach 3-4 Jahren
bei Patienten mit guter EF
Saxapliptin Sitagliptin
Lixisenatide
Ist das alles was man von
einer potenten anti-diabetischen Substanz
erwarten kann ?
• TECOS -> Sitagliptin
• ELIXA -> Lixisenatide
• EMPARG -> Empagliflozin
• ALBATROS -> Aldosteron Inhibition
• ARTS-HF -> Finerenone
• BACC -> Troponin bei ACS
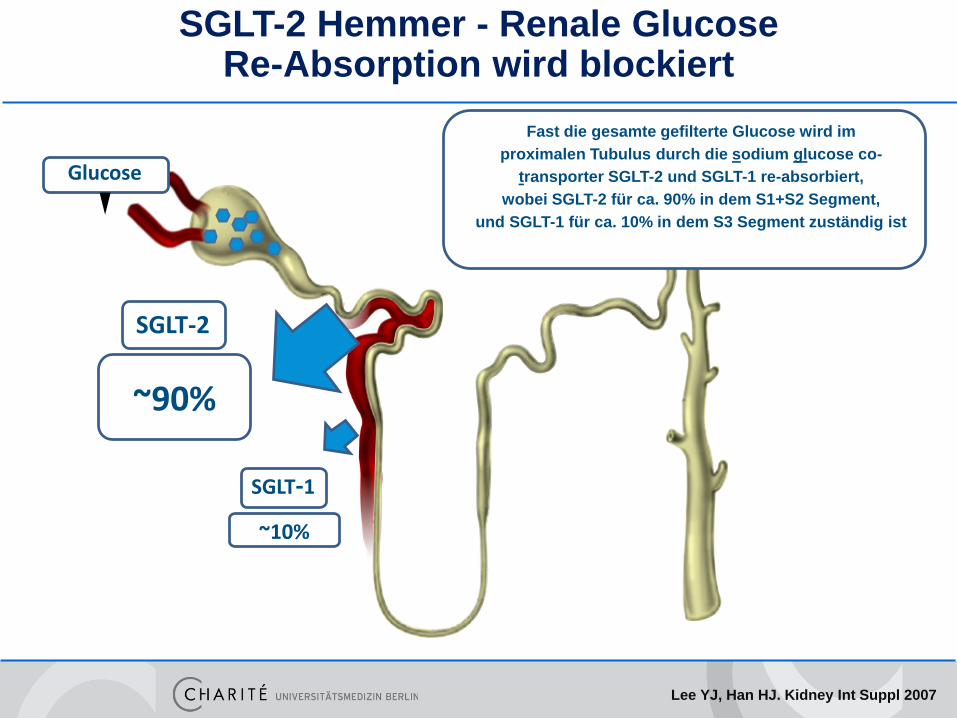
SGLT-2 Hemmer - Renale Glucose Re-Absorption wird blockiert
Lee YJ, Han HJ. Kidney Int Suppl 2007
Glucose
SGLT-1
SGLT-2
~10%
~90%
In gesunden Individuen filtern die Glomeruli ca. 180 g Glucose pro Tag
Fast die gesamte gefilterte Glucose wird im
proximalen Tubulus durch die sodium glucose co-
transporter SGLT-2 und SGLT-1 re-absorbiert,
wobei SGLT-2 für ca. 90% in dem S1+S2 Segment,
und SGLT-1 für ca. 10% in dem S3 Segment zuständig ist
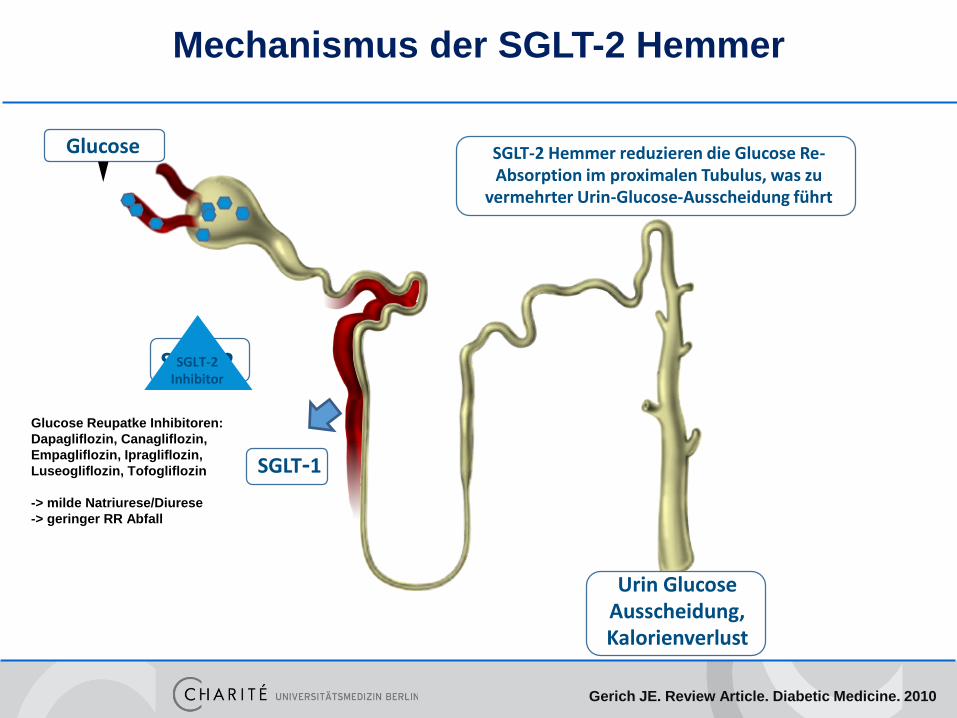
Mechanismus der SGLT-2 Hemmer
Gerich JE. Review Article. Diabetic Medicine. 2010
SGLT-2 Hemmer reduzieren die Glucose Re-Absorption im proximalen Tubulus, was zu
vermehrter Urin-Glucose-Ausscheidung führt
SGLT-2SGLT-2Inhibitor
SGLT-1
Glucose
Urin Glucose Ausscheidung, Kalorienverlust
Glucose Reupatke Inhibitoren:
Dapagliflozin, Canagliflozin,
Empagliflozin, Ipragliflozin,
Luseogliflozin, Tofogliflozin
-> milde Natriurese/Diurese
-> geringer RR Abfall
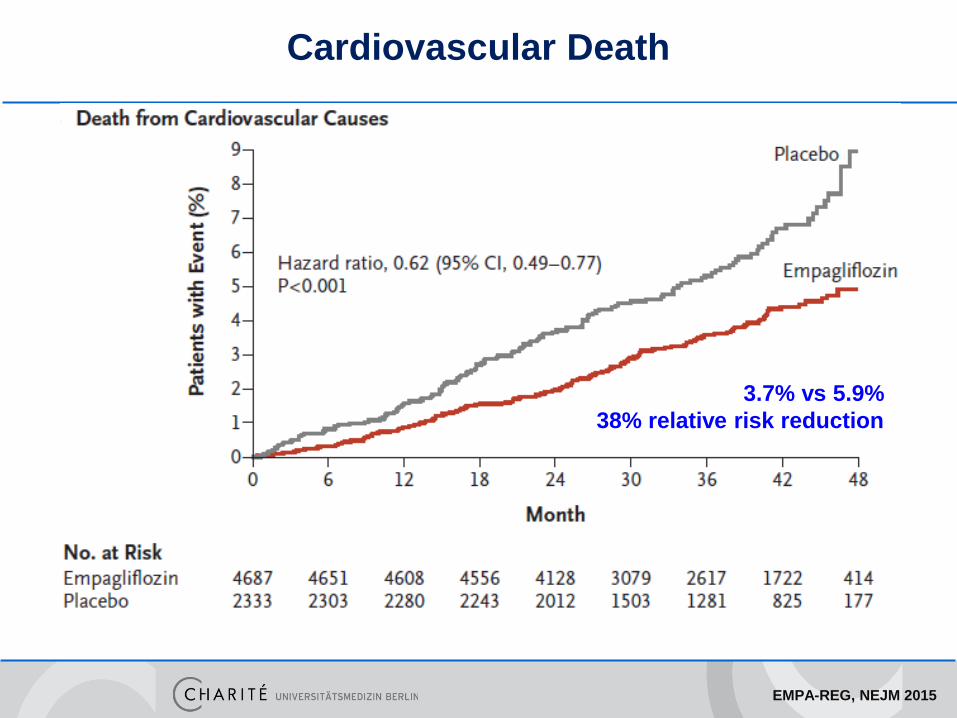
Zinman et al, NEJM. 2015
Empagliflozin, inhibitor of sodium–glucose co-transporter 2
N= 7020, type 2 diabetes at high cardiovascular risk;
3.1 years; primary composite outcome: CV death, MI, stroke
EMPA-REG, NEJM 2015
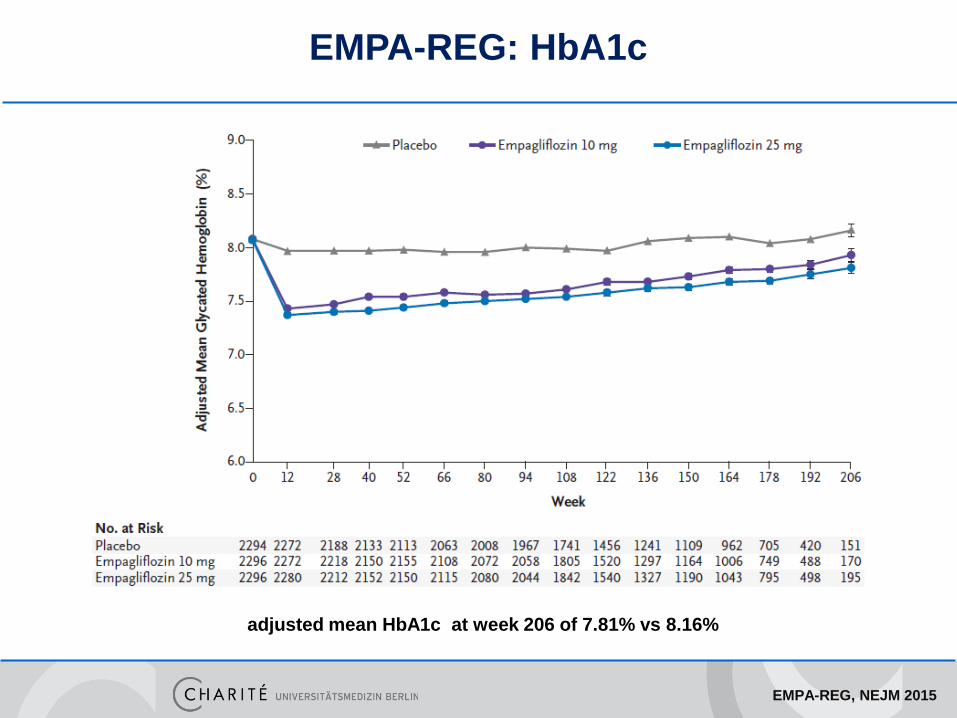
EMPA-REG: HbA1c
adjusted mean HbA1c at week 206 of 7.81% vs 8.16%
EMPA-REG, NEJM 2015
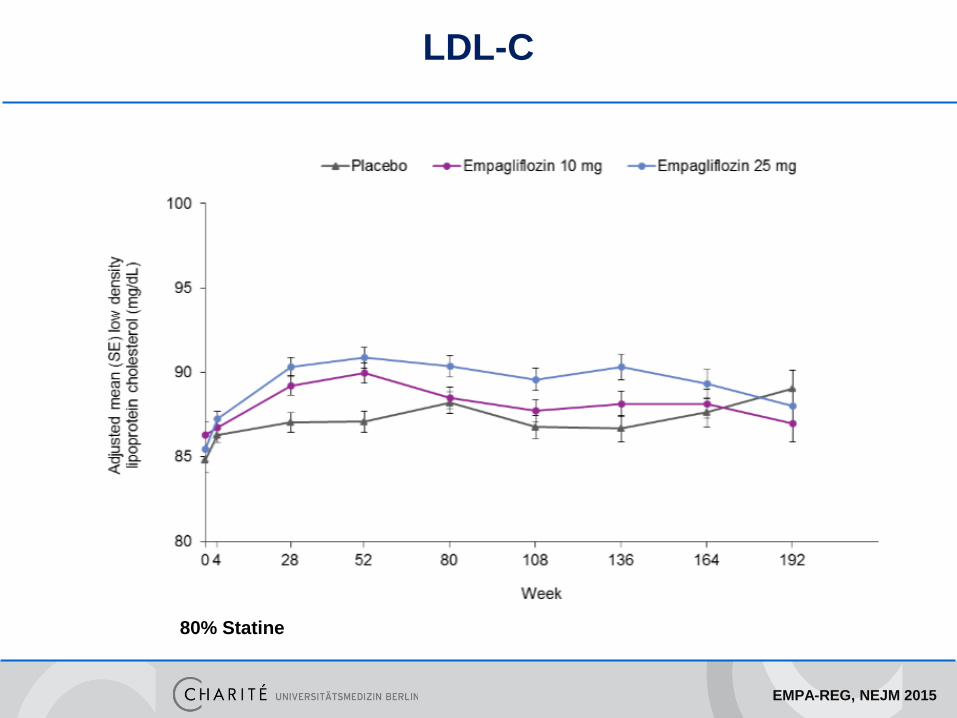
LDL-C
80% Statine
EMPA-REG, NEJM 2015
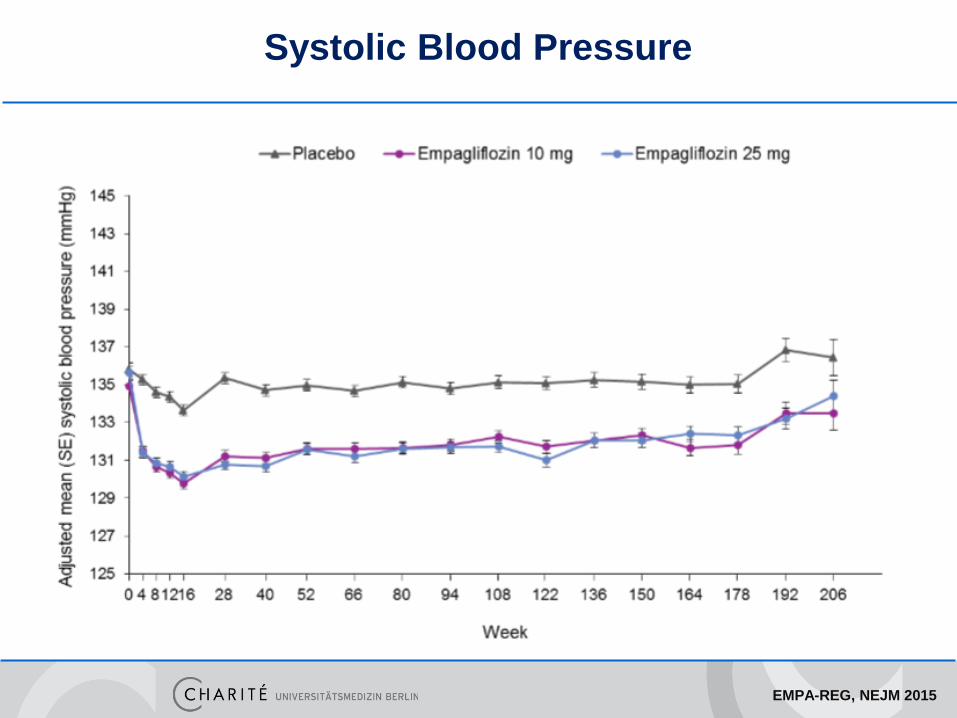
Systolic Blood Pressure
EMPA-REG, NEJM 2015
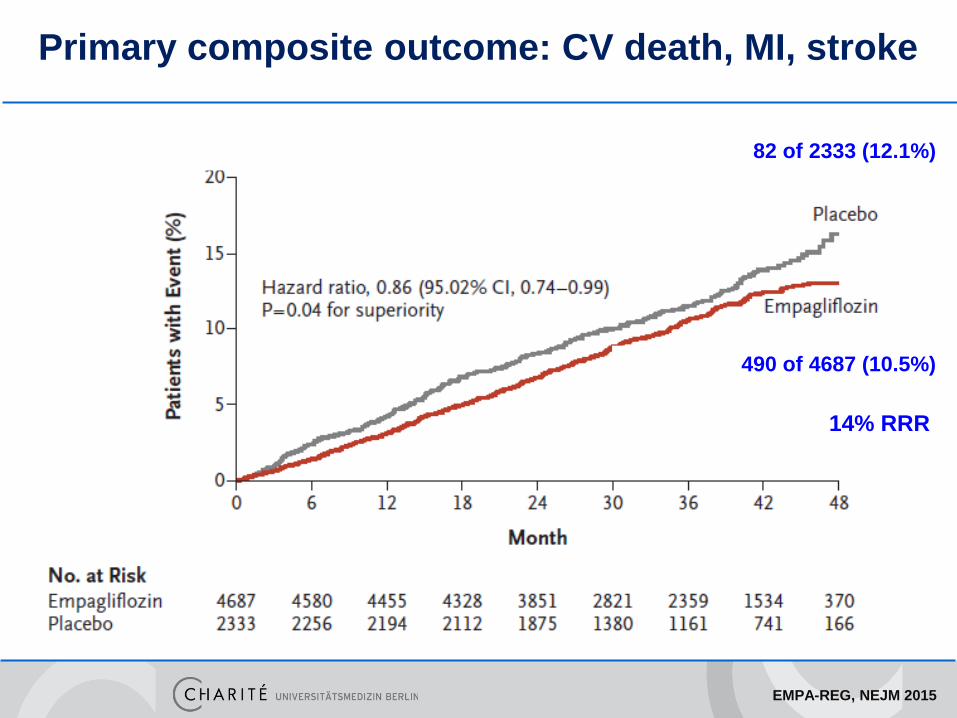
Primary composite outcome: CV death, MI, stroke
490 of 4687 (10.5%)
82 of 2333 (12.1%)
14% RRR
EMPA-REG, NEJM 2015
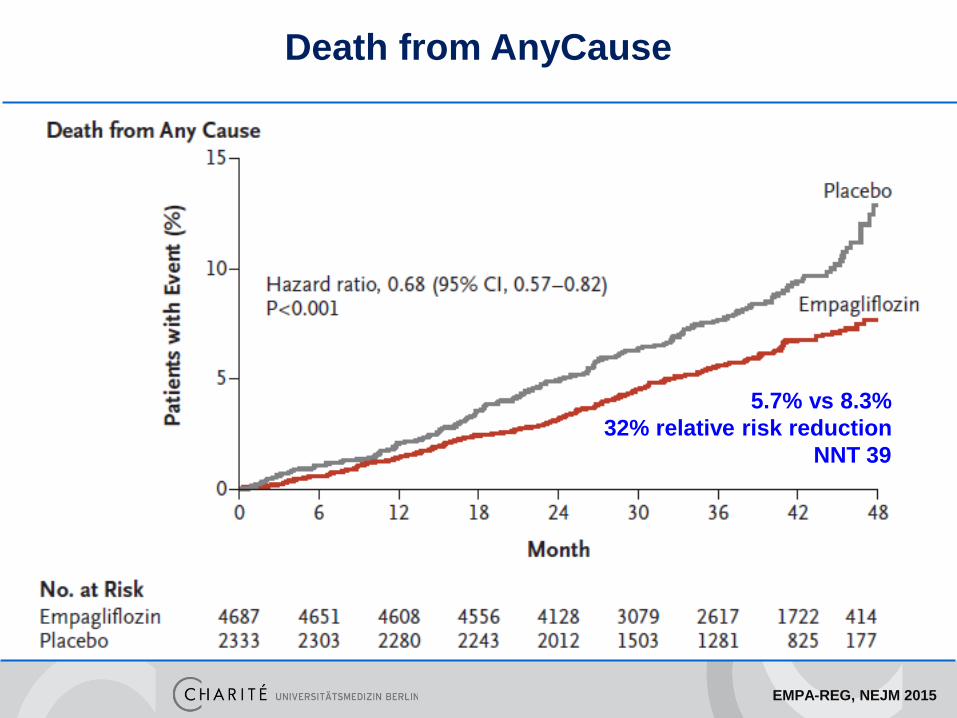
5.7% vs 8.3%
32% relative risk reduction
NNT 39
Death from AnyCause
EMPA-REG, NEJM 2015
3.7% vs 5.9%
38% relative risk reduction
Cardiovascular Death
EMPA-REG, NEJM 2015
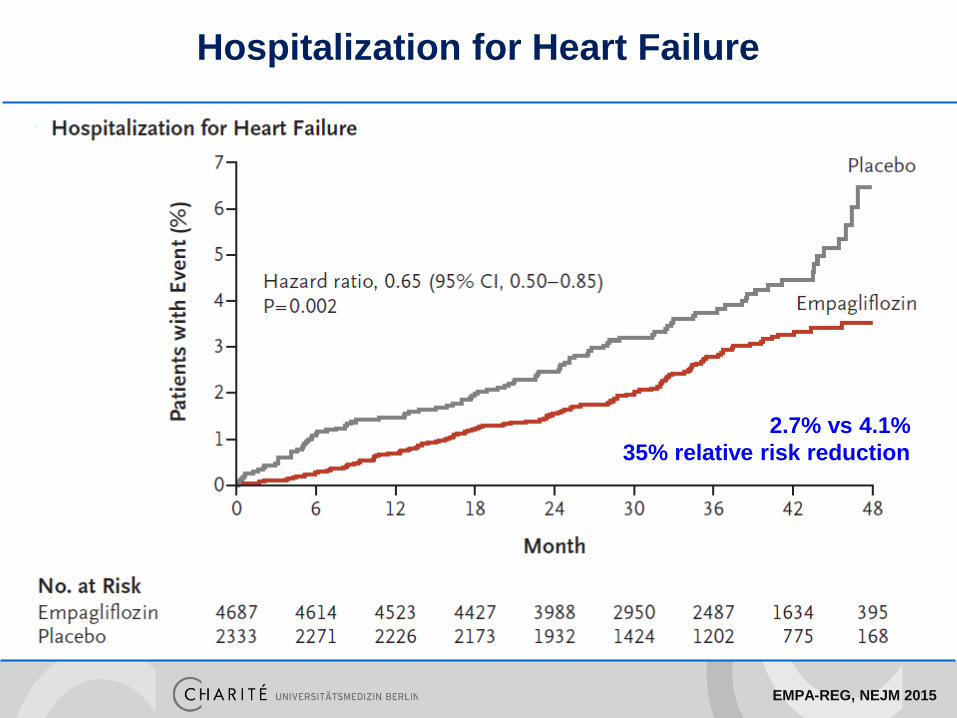
2.7% vs 4.1%
35% relative risk reduction
Hospitalization for Heart Failure
EMPA-REG, NEJM 2015
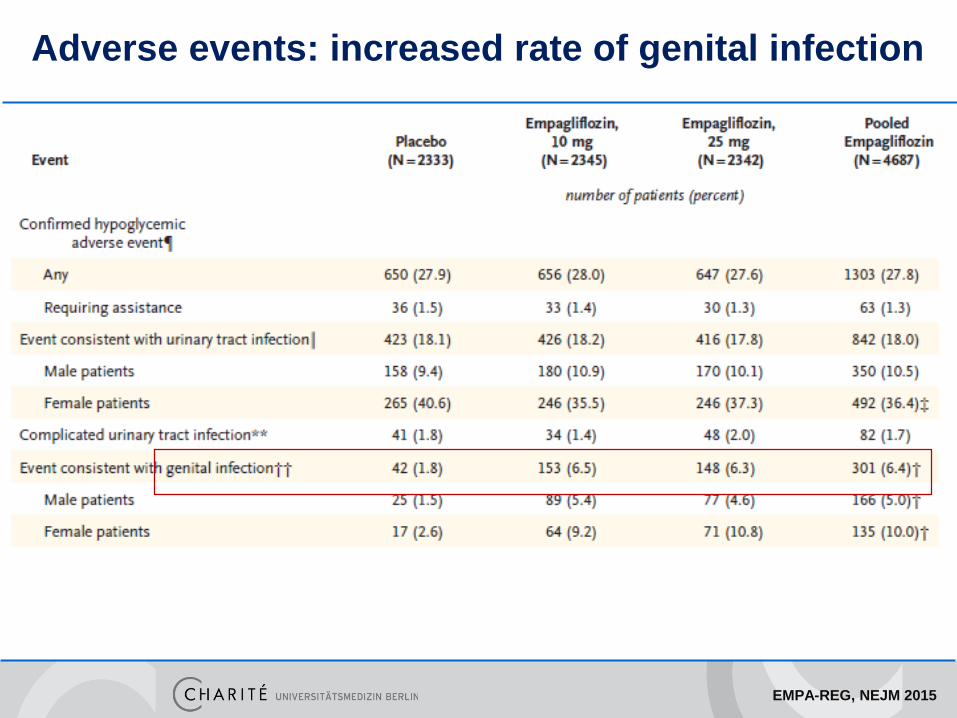
Adverse events: increased rate of genital infection
• TECOS -> Sitagliptin
• ELIXA -> Lixisenatide
• EMPARG -> Empagliflozin
• ALBATROS -> Aldosteron Inhibition
• ARTS-HF -> Finerenone
• BACC -> Troponin bei ACS
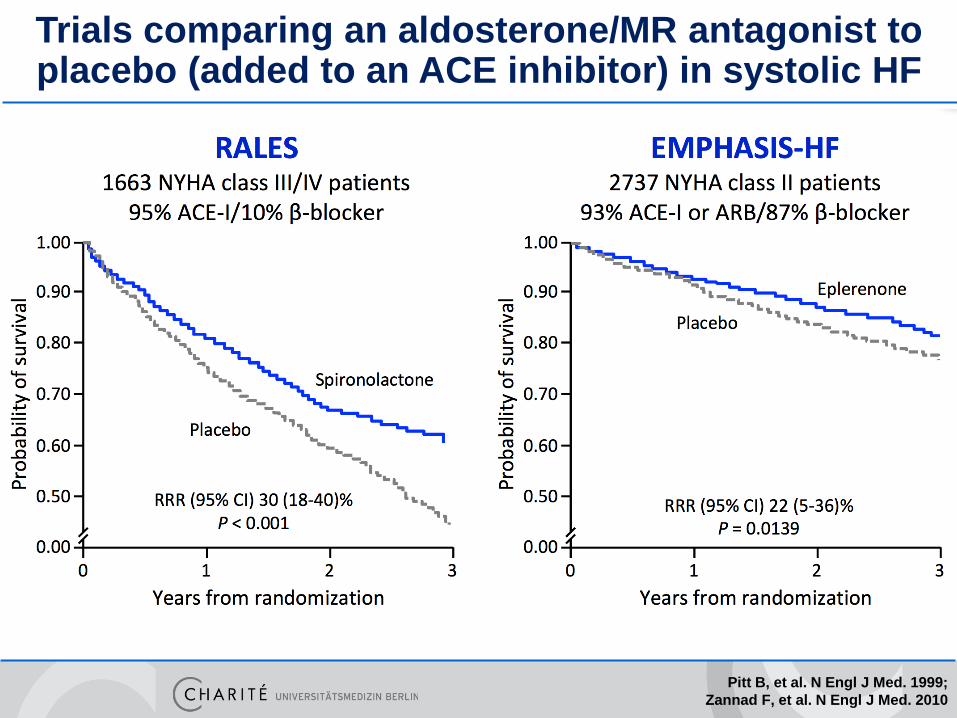
Pitt B, et al. N Engl J Med. 1999;
Zannad F, et al. N Engl J Med. 2010
Trials comparing an aldosterone/MR antagonist to placebo (added to an ACE inhibitor) in systolic HF
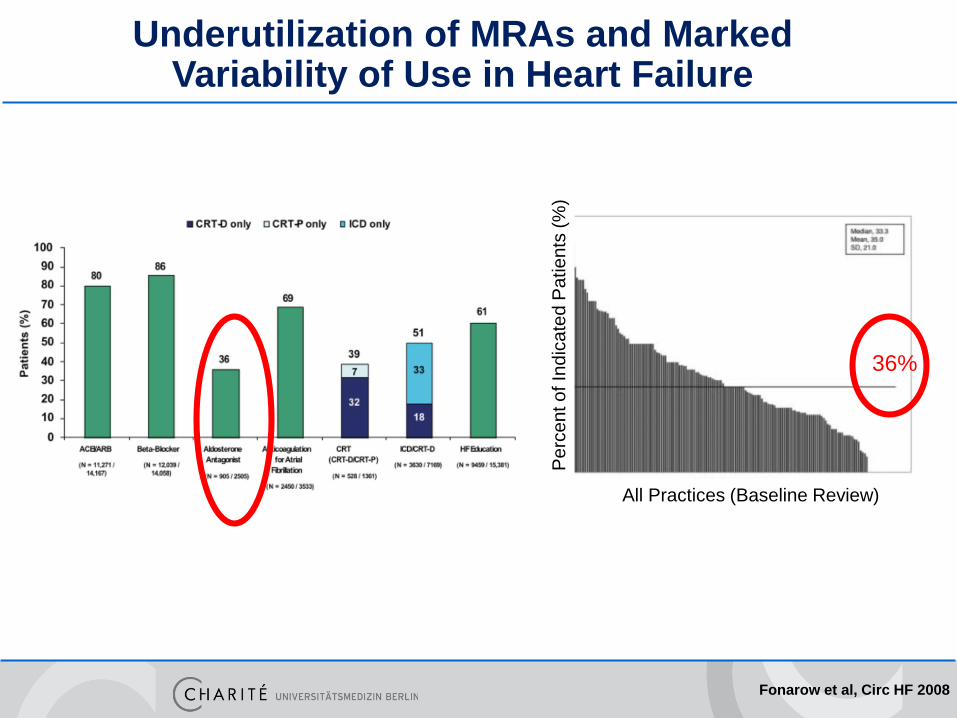
Underutilization of MRAs and Marked Variability of Use in Heart Failure
All Practices (Baseline Review)
Pe
rce
nt o
f In
dic
ate
d P
atie
nts
(%
)
36%
Fonarow et al, Circ HF 2008
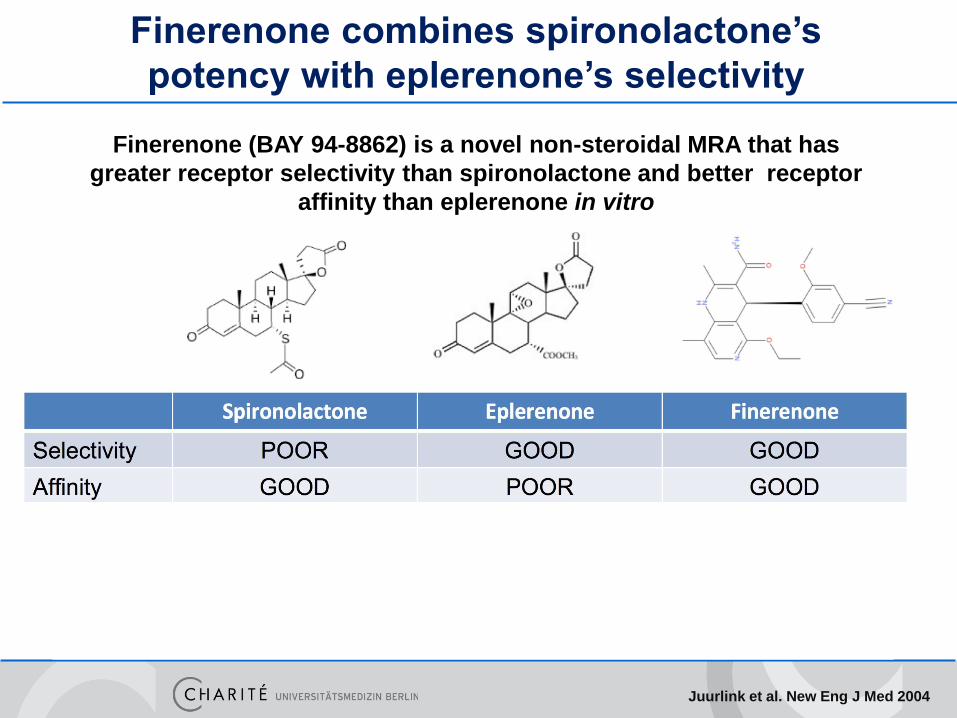
Finerenone combines spironolactone’s
potency with eplerenone’s selectivity
Juurlink et al. New Eng J Med 2004
Finerenone (BAY 94-8862) is a novel non-steroidal MRA that has
greater receptor selectivity than spironolactone and better receptor
affinity than eplerenone in vitro
Results of ARTS-HF:
finerenone versus eplerenone in patients with
worsening chronic heart failure and diabetes
and/or chronic kidney disease
Gerasimos FilippatosStefan D Anker, Michael Böhm, Mihai Gheorghiade, Lars Køber,
Henry Krum, Aldo P Maggioni, Piotr Ponikowski, Adriaan A Voors, Faiez Zannad, So-Young Kim, Christina Nowack, Giovanni Palombo, Peter Kolkhof, Nina Kimmeskamp-
Kirschbaum, Alexander Pieper and Bertram Pitt,
for the MinerAlocorticoid Receptor AnTagonist Study In Heart Failure(ARTS-HF) Committees and Investigators
Study objective
Study objective: to compare the safety and efficacy of different once-
daily oral doses of finerenone with eplerenone in patients who
presented in emergency departments with worsening chronic HFrEF
with type 2 diabetes mellitus and/or chronic kidney disease (CKD)
Pitt B et al. Eur Heart J 2013
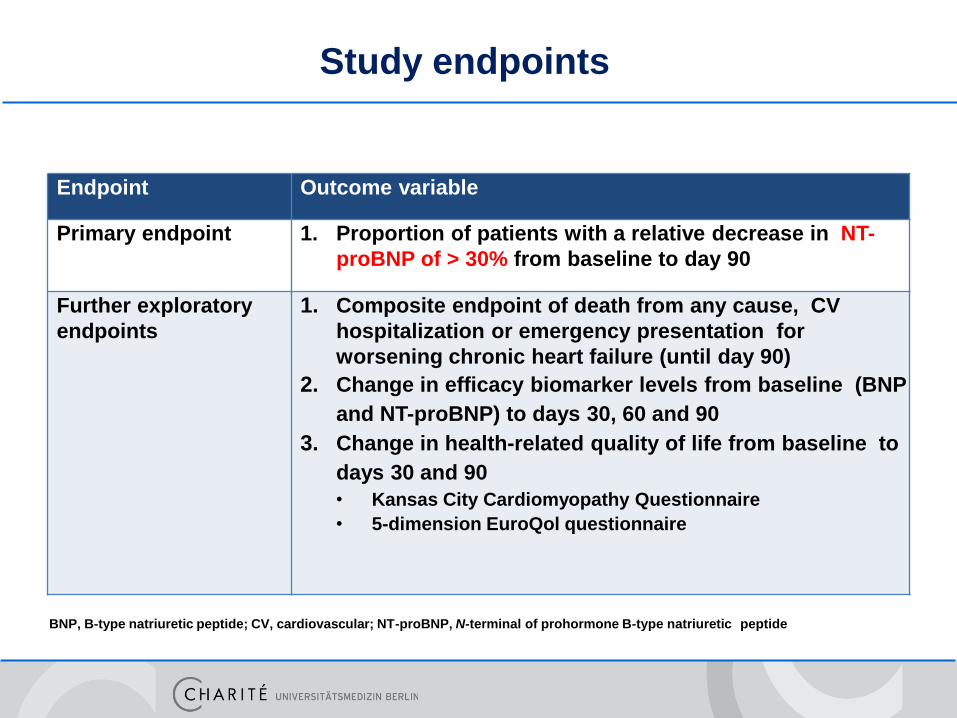
Study endpoints
Endpoint Outcome variable
Primary endpoint 1. Proportion of patients with a relative decrease in NT-
proBNP of > 30% from baseline to day 90
Further exploratory
endpoints
1. Composite endpoint of death from any cause, CV
hospitalization or emergency presentation for
worsening chronic heart failure (until day 90)
2. Change in efficacy biomarker levels from baseline (BNP
and NT-proBNP) to days 30, 60 and 90
3. Change in health-related quality of life from baseline to
days 30 and 90
• Kansas City Cardiomyopathy Questionnaire
• 5-dimension EuroQol questionnaire
BNP, B-type natriuretic peptide; CV, cardiovascular; NT-proBNP, N-terminal of prohormone B-type natriuretic peptide
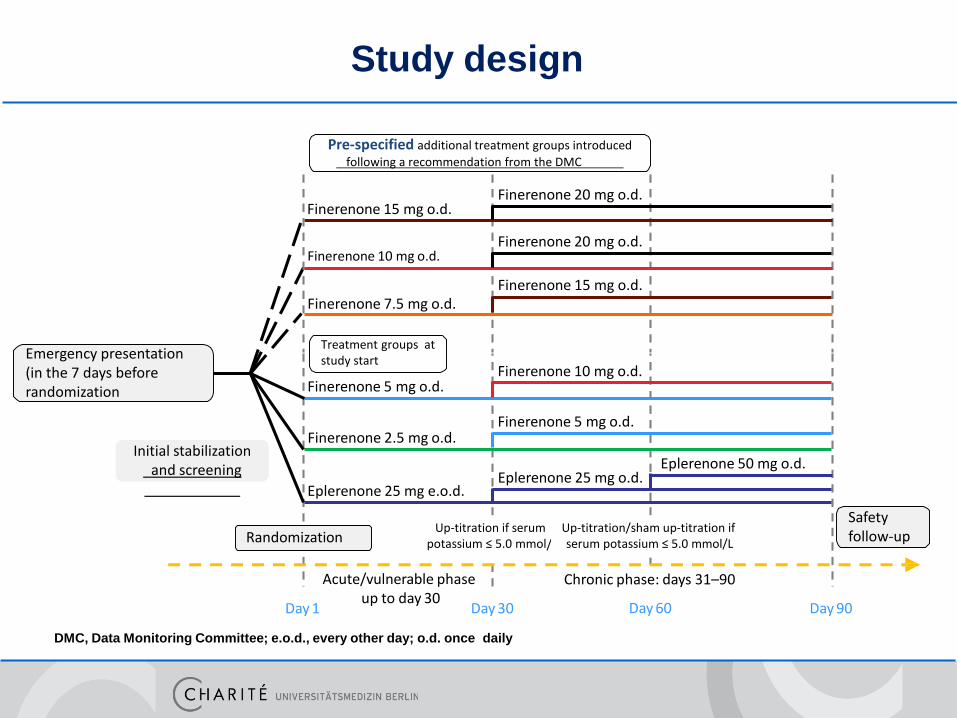
Study design
DMC, Data Monitoring Committee; e.o.d., every other day; o.d. once daily
Pre-specified additional treatment groups introduced
following a recommendation from the DMC
Treatment groups at study start
Initial stabilizationand screening
Safety follow-up
Emergency presentation (in the 7 days before randomization
Finerenone 20 mg o.d.
Finerenone 20 mg o.d.
Finerenone 10 mg o.d.
Finerenone 5 mg o.d.
Eplerenone 25 mg o.d.
Finerenone 15 mg o.d.
Finerenone 10 mg o.d.
Finerenone 15 mg o.d.Finerenone 7.5 mg o.d.
Finerenone 5 mg o.d.
Finerenone 2.5 mg o.d.
Eplerenone 25 mg e.o.d.
Eplerenone 50 mg o.d.
Acute/vulnerable phaseup to day 30
Chronic phase: days 31–90
Up-titration if serum potassium ≤ 5.0 mmol/L
Up-titration/sham up-titration if serum potassium ≤ 5.0 mmol/LRandomization
Day 1 Day 30 Day 90Day 60
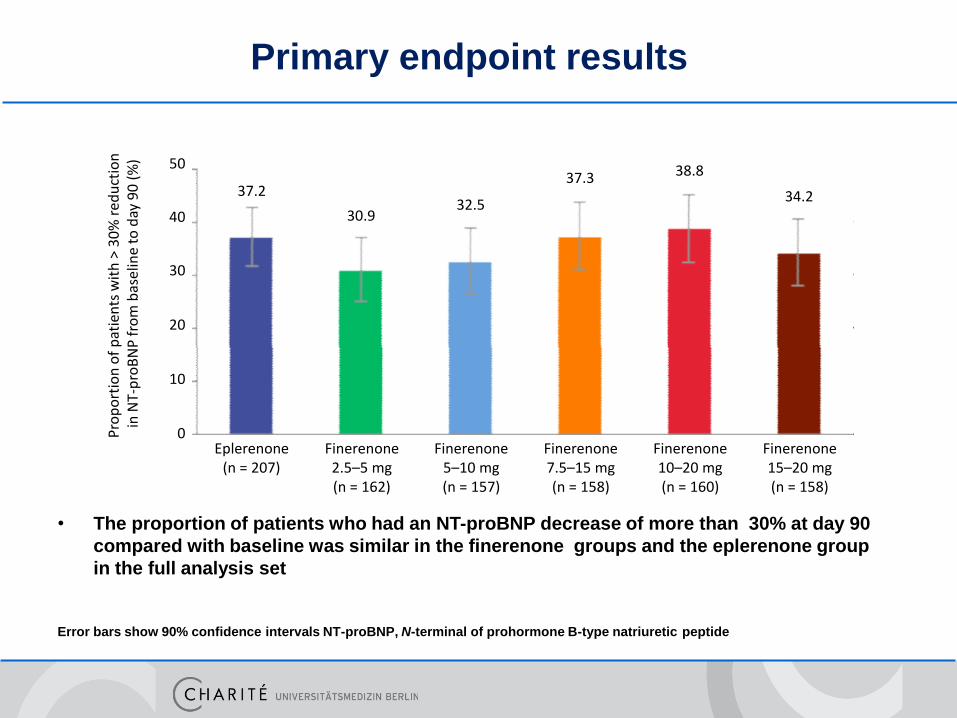
Primary endpoint results
• The proportion of patients who had an NT-proBNP decrease of more than 30% at day 90
compared with baseline was similar in the finerenone groups and the eplerenone group
in the full analysis set
Error bars show 90% confidence intervals NT-proBNP, N-terminal of prohormone B-type natriuretic peptide
Pro
po
rtio
n o
f p
atie
nts
wit
h >
30
% r
edu
ctio
nin
NT-
pro
BN
P f
rom
bas
elin
e to
day
90
(%
) 50
30
20
10
0Eplerenone
(n = 207)Finerenone 2.5–5 mg(n = 162)
Finerenone 5–10 mg(n = 157)
Finerenone 7.5–15 mg(n = 158)
Finerenone 10–20 mg(n = 160)
Finerenone 15–20 mg(n = 158)
37.2
30.932.5
37.3 38.8
34.2
40
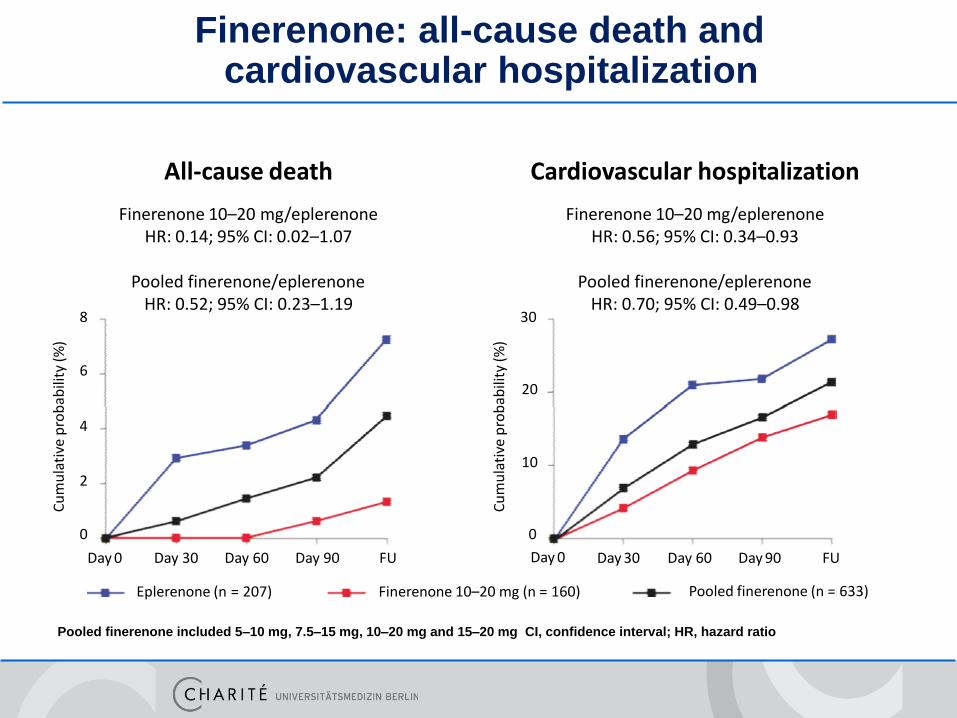
Cardiovascular hospitalization
Finerenone 10–20 mg/eplerenoneHR: 0.56; 95% CI: 0.34–0.93
Pooled finerenone/eplerenone HR: 0.70; 95% CI: 0.49–0.98
Finerenone: all-cause death and cardiovascular hospitalization
Pooled finerenone included 5–10 mg, 7.5–15 mg, 10–20 mg and 15–20 mg CI, confidence interval; HR, hazard ratio
All-cause death
Finerenone 10–20 mg/eplerenoneHR: 0.14; 95% CI: 0.02–1.07
Pooled finerenone/eplerenone HR: 0.52; 95% CI: 0.23–1.19
Cu
mu
lati
ve p
rob
abili
ty (
%)
8
0
Cu
mu
lati
ve p
rob
abili
ty (
%)
620
4
102
30
Day 0
0
Day 0 Day 30 Day 60 Day 90 FUDay 30 Day 60 Day 90 FU
Eplerenone (n = 207) Finerenone 10–20 mg (n = 160) Pooled finerenone (n = 633)
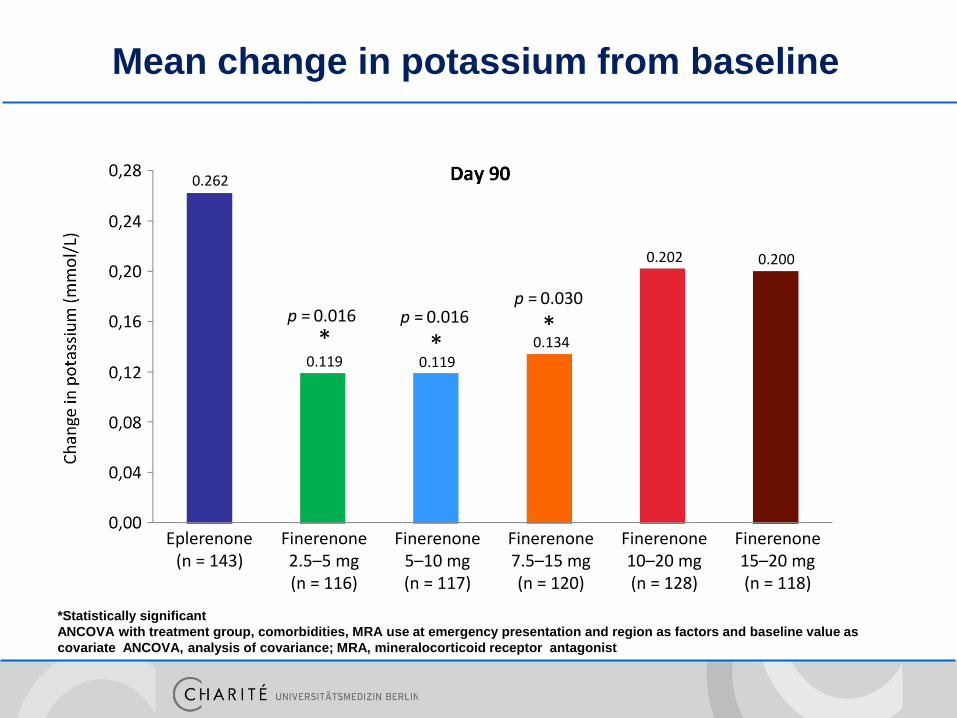
Mean change in potassium from baseline
*Statistically significant
ANCOVA with treatment group, comorbidities, MRA use at emergency presentation and region as factors and baseline value as
covariate ANCOVA, analysis of covariance; MRA, mineralocorticoid receptor antagonist
**p = 0.016 p = 0.016
p = 0.030
Eplerenone (n = 143)
Finerenone 2.5–5 mg(n = 116)
Finerenone 5–10 mg(n = 117)
Finerenone 7.5–15 mg(n = 120)
Finerenone 10–20 mg(n = 128)
Finerenone 15–20 mg(n = 118)
0.262
*0.119 0.119
0.134
0.202 0.200
Summary I
• In patients hospitalized for worsening chronic HFrEF with type 2
diabetes mellitus and/or CKD, the proportion of patients with a
relative decrease in NT-proBNP of more than 30% from baseline to
day 90 was similar in the eplerenone group and the finerenone
groups
• The incidence of the clinical composite endpoint (all-cause death,
cardiovascular hospitalization or emergency presentation for
worsening chronic heart failure) at day 90 was lower with all
finerenone doses (except 2.5–5 mg) than with eplerenone, with the
lowest incidence observed in the finerenone 10–20 mg dose group
Summary II
• All doses of finerenone were well tolerated, with a similar
incidence of treatment-emergent adverse events in the
eplerenone group and finerenone groups
• Hyperkalaemia (serum potassium ≥ 5.6 mmol/L) was observed
in 44 patients (4.3%) at any time post-baseline
• FINESSE-HF (3600 Pts. with reduced EF and Diabetes and/or CKD)
• FIGARO-DKD (6400 Pts. With diabetic kidney disease UACR <300mg/g)
• FIDELIO-DKD (4800 Pts. With diabetic kidney disease UACR> 300mg/g)
FINERENONE - Zukunft
Phase III Studienprogramm:
• TECOS -> Sitagliptin
• ELIXA -> Lixisenatide
• EMPARG -> Empagliflozin
• ALBATROS -> Aldosteron Inhibition
• ARTS-HF -> Finerenone
• BACC -> Troponin bei ACS
Accurate and Rapid Diagnosis of Myocardial Infarction Using a
High-Sensitivity Troponin I 1-Hour Algorithm
Johannes Tobias Neumann1, Nils Arne Sörensen1, Tjark Schwemer1, Francisco Ojeda1, Rafael Bourry1, Vanessa Sciacca1, Sarina Schäfer1,2, Christoph Waldeyer1, Christoph Sinning1, Thomas Renné3, Martin Than5, Will Parsonage4, Karin Wildi6, Nataliya Makarova1,2, Renate B. Schnabel1,2, Ulf Landmesser7, Christian Mueller6,
Louise Cullen4, Jaimi Greenslade4, Tanja Zeller1,2, Stefan Blankenberg1,2, MahirKarakas1,2, Dirk Westermann1,2
1 Department of General and Interventional Cardiology, University Heart Center Hamburg Eppendorf, Hamburg, Germany2 German Center for Cardiovascular Research (DZHK), Partner Site Hamburg/Kiel/Lübeck, Hamburg, Germany3 Institute of Clinical Chemistry and Laboratory Medicine, University Medical Center Hamburg-Eppendorf, Hamburg, Germany4 Royal Brisbane and Women's Hospital, Department of Emergency Medicine, Brisbane 4006, Australia5 Christchurch Hospital, Christchurch, New Zealand6 Department of Cardiology and Cardiovascular Research Institute Basel (CRIB), University Hospital Basel, Switzerland7 Department of Cardiology, Charite Universitätsmedizin Berlin, Campus Benjamin Franklin, Berlin, Germany
BACC
Background
There is clinical need to rapidly and safely rule-in or rule-out acute myocardial
infarction (AMI) in patients with acute chest pain in order to
1. initiate fast evidence based treatment for patients with AMI
2. limit overuse of scarce medical resources in the emergency room (ER)
discharging patients without acute cardiac conditions.
Guidelines recommend1,2 measuring high sensitivity assayed troponins directly after
admission and after 3 hours detecting elevated levels based on the 99th percentile of
the specific assays together with an increase/decrease.
Recent studies (ADAPT (2-hour)3 and APACE (1- hour)4 cohort) challenge current
guidelines with intervals shorter than 3 hours.
1 Hamm et al. EHJ 2011 2 Thygesen et al. EHJ 2012;
3 Than et al. JACC 2012; 4 Reichlin et al. CMAJ 2015
Aim of the study
To investigate the application of
high sensitivity assayed troponin I (TnI) for
a) a rapid 1-hour rule-out and rule-in compared to a 3-hours
approach
b) a lower and more sensitive cut-off value compared to the 99th
percentile
in the Biomarkers in Acute Cardiovascular Care (BACC) cohort
investigating 1,045 patients with acute chest pain.
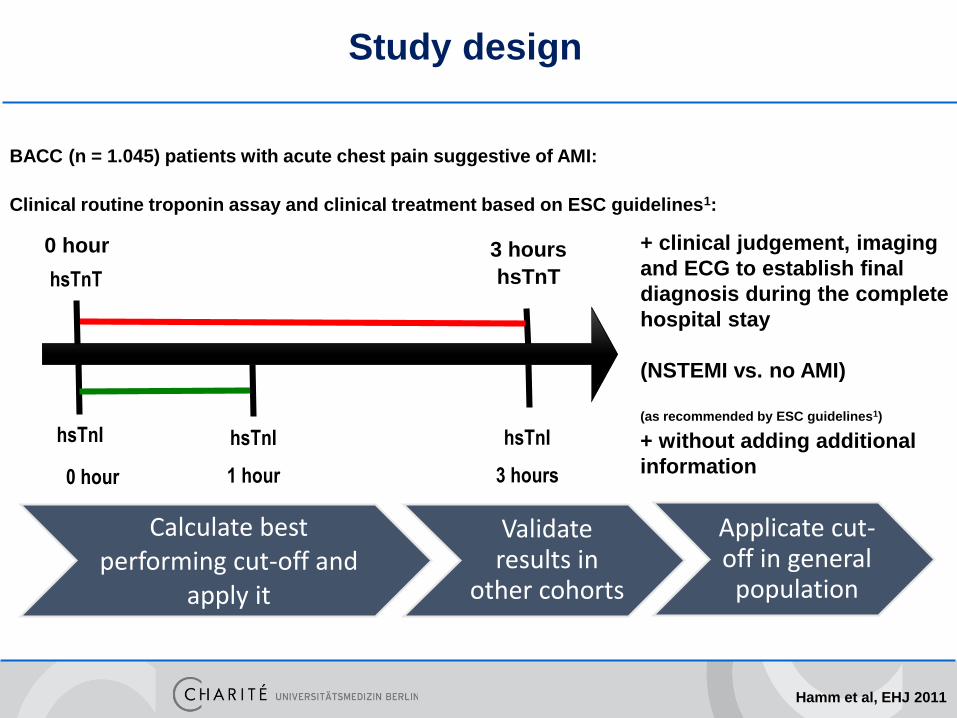
0 hour 3 hours
hsTnT hsTnT
BACC (n = 1.045) patients with acute chest pain suggestive of AMI:
Study design
Calculate bestperforming cut-off and
apply it
Validateresults in
other cohorts
Applicate cut-off in general
population
Clinical routine troponin assay and clinical treatment based on ESC guidelines1:
1 hour0 hour
hsTnI hsTnI
3 hours
hsTnI + without adding additional
information
+ clinical judgement, imaging
and ECG to establish final
diagnosis during the complete
hospital stay
(NSTEMI vs. no AMI)
(as recommended by ESC guidelines1)
Hamm et al, EHJ 2011
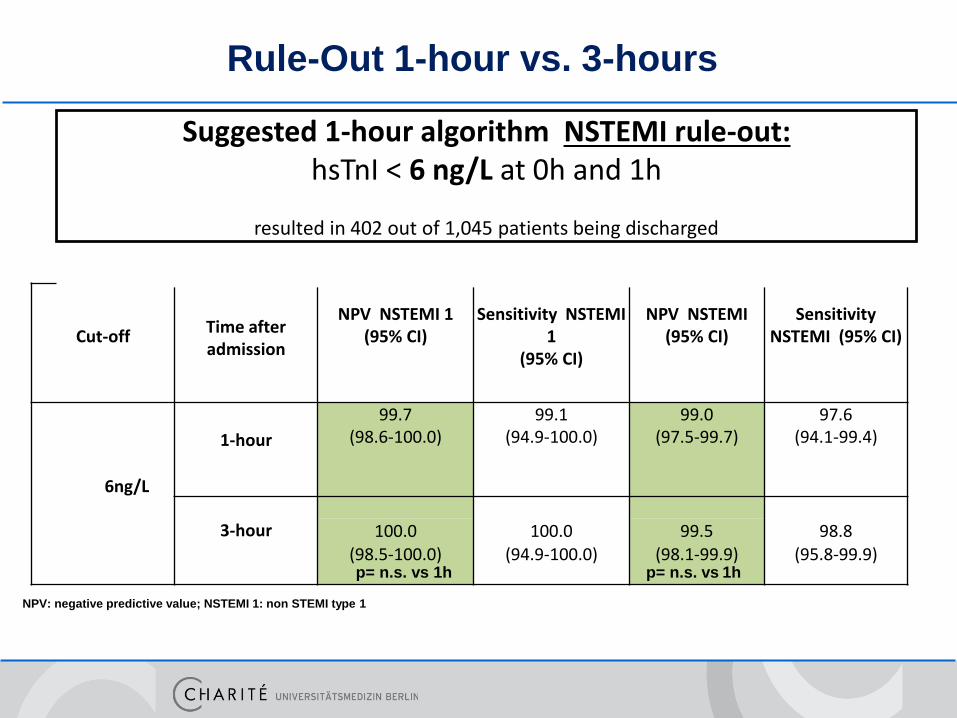
Cut-offTime after admission
NPV NSTEMI 1(95% CI)
Sensitivity NSTEMI 1
(95% CI)
NPV NSTEMI (95% CI)
Sensitivity NSTEMI (95% CI)
1-hour
99.7(98.6-100.0)
99.1(94.9-100.0)
99.0(97.5-99.7)
97.6(94.1-99.4)
6ng/L
3-hour 100.0(98.5-100.0)
100.0(94.9-100.0)
99.5(98.1-99.9)
98.8(95.8-99.9)
Rule-Out 1-hour vs. 3-hours
p= n.s. vs 1hp= n.s. vs 1h
NPV: negative predictive value; NSTEMI 1: non STEMI type 1
Suggested 1-hour algorithm NSTEMI rule-out:hsTnI < 6 ng/L at 0h and 1h
resulted in 402 out of 1,045 patients being discharged
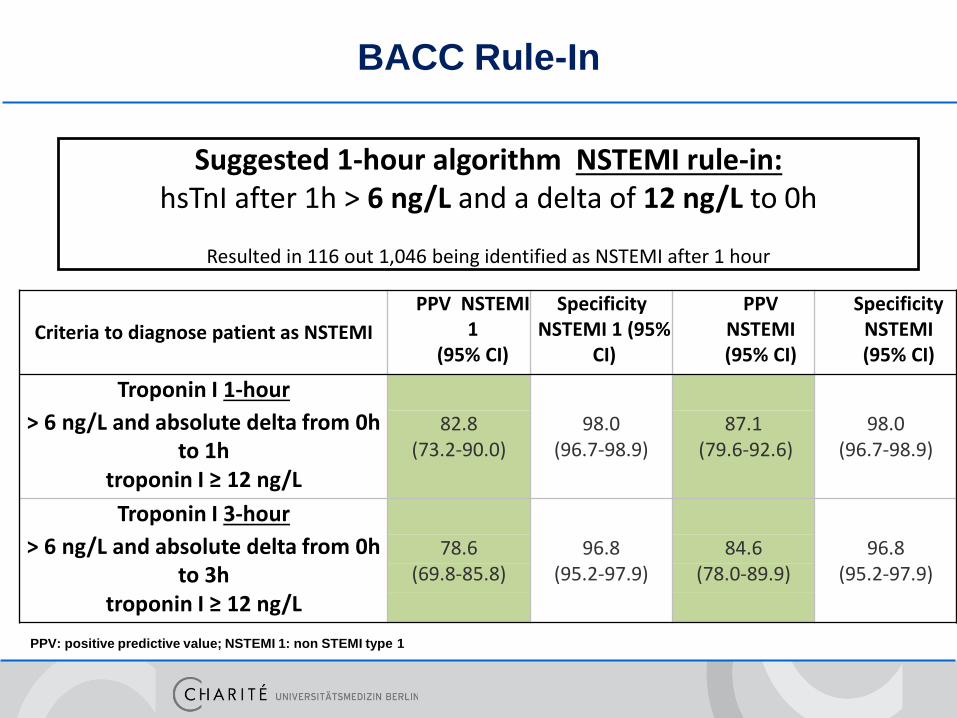
Criteria to diagnose patient as NSTEMI
PPV NSTEMI 1
(95% CI)
Specificity NSTEMI 1 (95%
CI)
PPV NSTEMI (95% CI)
Specificity NSTEMI (95% CI)
Troponin I 1-hour
> 6 ng/L and absolute delta from 0h 82.8 98.0 87.1 98.0
to 1h (73.2-90.0) (96.7-98.9) (79.6-92.6) (96.7-98.9)
troponin I ≥ 12 ng/L
Troponin I 3-hour
> 6 ng/L and absolute delta from 0h 78.6 96.8 84.6 96.8
to 3h (69.8-85.8) (95.2-97.9) (78.0-89.9) (95.2-97.9)
troponin I ≥ 12 ng/L
BACC Rule-In
PPV: positive predictive value; NSTEMI 1: non STEMI type 1
Suggested 1-hour algorithm NSTEMI rule-in:hsTnI after 1h > 6 ng/L and a delta of 12 ng/L to 0h
Resulted in 116 out 1,046 being identified as NSTEMI after 1 hour
A 1-hour algorithm is safe to rule-out AMI.
A sensitive troponin I cut-off (6 ng/L) performed better compared to
the 99th percentile (27 ng/L) in view of lower follow-up mortality.
Low troponin I values predict mortality in the general population.
Further studies are needed to test the best cut-off for each troponin
assay and to validate a 1-hour algorithm prospectively.
Conclusion

Carsten Tschöpe
Vielen Dank !





























