Embed Size (px)
Citation preview

Epilepsy in children |Classification and aetiology
Michael Carter | ACF3, paediatrics, King’s College Hospital and UCL
April 2012

Classification
Manifestations • Generalised: Arising within and rapidly engaging
bilaterally distributed networks• Focal: Originating within networks limited to one
hemisphere• Unknown (e.g. infantile spasms)
Electroclinical syndromes• Syndromic epilepsy (often categorised by age of onset,
see later)• Constellations of symptoms (e.g. mesial temporal lobe
sclerosis)• Non-syndromic epilepsy (e.g. post-stroke, perinatal
insults etc.)
Aetiology• Genetic• Structural-metabolic• Unknown


Manifestations | Generalised
Manifestation Example Investigations Treatment
Tonic-clonic (or tonic or clonic alone)
Valproate Lamotrigine
Absence EthosuxamideValproate
Atonic ValproateLamotrigine
Myoclonic Valproate

Generalised epilepsies | Drugs and SEs
Drug Mechanism Side effects
Valproate Inhibitor of GABA transaminase
GI upset, low PLTs, hepatitis, hair loss, tremor, teratogenic
Lamotrigine Na+ channel blockade
Rash including SJS, aseptic meningitis, double vision, dizziness, anxiety, GI upset (CI myoclonus)
Ethosuxamide Na+ or Ca2+ channel blockade
Anxiety and psychiatric disorders, pancytopaenia, GI upset, SJS
Note: carbamazepine worsens absence seizures; lamotrigine worsens myoclonic seizures
Fetal valproate syndrome: neural tube defects, coloboma, limb defects. Also, cardiac defects, dysmorphic features and occasional global developmental delay

Manifestations | Focal
Originate within networks limited to one hemisphere• Are described with specific reference to the symptoms
involved, such as:• Subjective sensations (e.g. auras)• Motor (e.g. twitching)• Autonomic (e.g. sweating)• Dyscognitive features (e.g. impaired consciousness –
note replaces “partial”)
And may:• Evolve to a bilateral convulsive seizure (note replaces “secondarily generalised”)
Usually denote a focal lesion within the brain, e.g. mesial temporal sclerosis, stroke etc.
The most common cause of acquired epilepsy, globally is …
(Emedicine)

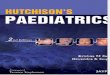
Manifestations | Focal
T2-weighted magnetic resonance images reveal the increased signal and volume loss of the left hippocampus: mesial temporal sclerosis (Emedicine)
First-line drugs for focal seizure SE effects
Carbamazepine (Na+ channel blockade)
Drowsiness, headaches, pancytopaenia, hypothyroidism, cerebellar syndrome (CI absences)
Lamotrigine Rash including SJS, aseptic meningitis, double vision, dizziness, anxiety, GI upset (CI myoclonus)
Alternatives: leviracetam, valproate, oxcarbazepine
Adjuncts: clobazam, gabapentin, topiramate
Alternatives: surgical intervention for a focal lesion

Manifestations | Unknown
For example, epilepsy syndromes in infancy
Infantile spasms:

Electroclinical syndromes
An electroclinical syndromes is:
“A complex of clinical features, signs, and symptoms that together define a distinctive, recognizable clinical disorder…
Identifiable on the basis of a typical age onset, specific EEG characteristics, seizure types, and often other features which, when taken together, permit a specific diagnosis.
The diagnosis in turn often has implications for treatment, management, and prognosis.”


Electroclinical syndromes | Neonatal
• Neonatal: benign neonatal seizures, others
Syndrome Symptoms Management Note
Benign neonatal seizures
Repetitive clonic seizures. Often unilateral. Ictal EEG with Rolandic spikes and waves
None Diagnosis of exclusion. By definition, excellent prognosis
Ohtahara, early myoclonic epilepsy
Continuing, tonic-clonic seizures. Hypsarrhythmia in EME
None Prognosis poor, onset to death within short months

Electroclinical syndromes | Infancy
Syndrome Symptoms Management Notes
Febrile seizures
Generalised T-C seizure with fever in children 6 months to 6 years of age
Usually none Atypical febrile seizures: Early onset, >15 mins, focal, focal deficit, repeated same day
Benign infantile epilepsy
Infancy-20 months. Focal seizures clusters for 1-3 days
Usually none Usually benign and relents. Atypical if no family history
West syndrome
Onset usually 5 months. Clusters of infantile spasms, hypsarrythmia
Vigabatrin Progressive encephalopathy
Dravet syndrome
Early febrile T-C seizures, myoclonus, atypical absences, focal (dyscognitive) seizures
ValproateTopiramate
Initially progressive encephalopathy that finally relents but with severe global delay

Electroclinical syndromes | Childhood
Syndrome Symptoms Management Notes
Childhood absence Brief impairment of consciousness
EthosuxamideValproate
Spike, slow-wave discharges 3-4 Hz
Panayiotopoulos syndrome
Prolonged autonomic seizures (vomiting). Focal
Carbamazepine Lamotrigine
Synonym: Early-onset occipital (misnomer)
Late-onset occipital (Gastaut)
Carbamazepine Lamotrigine
Benign epilepsy with centro-temporal spikes
Oro-pharngeal symptoms, facial sensorimotor. Focal
Carbamazepine Lamotrigine
Benign Rolandic epilepsy former name
Lennox-Gastaut Polymorphic intractable seizures
ValproateEarly referral to 3ary
EEG: generalised spike and wave

Electroclinical syndromes | Adolescence
These are also known as idiopathic generalised epilepsies, and categorised by their manifestations
Syndrome Symptoms Management Notes
Juvenile absences Brief impairment of consciousness
EthosuxamideValproate
Spike, slow-wave discharges 3-4 Hz
Juvenile generalised T-C
Generalised T-C. Preceding myo-clonus. No aura
Valproate Lamotrigine
Consider triggers (sleep deprivation, photic etc.)
Juvenile myoclonic epilepsy
Myoclonic jerks. May be subtle.
Valproate Consider triggers (sleep deprivation, photic etc.)

Aetiology
Genetic Structural-metabolic Unknown
Genetic defect directly contributes to the epilepsy and seizures are the main symptom of the disorder
Caused by a structural or metabolic disorder of the brain (formerly “symptomatic”)
Other epilepsy for whom genetic studies are currently negative
E.g. channelopathies E.g. tuberous sclerosis, stroke, tumours

Investigations in children
EEG• Indications: after second seizure (occasionally first
seizure)• Issues: Low sensitivity (useful to support a diagnosis
only)• Other: If normal, consider sleep EEG (with melatonin),
photic stimulation, hyperventilation or telemetry
MRI• Indications: <2 years of age, adults, focal onset,
resistance to first-line medication
Other • Routine biochemistry (including magnesium) and ECG in
all patients

Criteria for onward referral to 3ary
Epilepsy nursesTo be involved in the care of all children with epilepsy
Syndromes and manifestations• All children with infantile spasms• All children with suspected Dravet syndrome• All children with suspected Lennox-Gastaut syndrome• All children <2 years• All children with unilateral structural lesion• All children with drug-resistant epilepsy (after 2 drugs
with breakthrough)• All children with diagnostic doubt

Conclusions
Classification of epilepsies• By manifestation: generalised, focal, unknown• By electroclinical syndrome: usually also by typical age
of onset• By aetiology: genetic, structural-metabolic, unknown
Management• EEG (+/- MRI) after second seizure unless focal deficits
or unwell• Epilepsy nurses• Generally: valproate first-line for any generalised
epilepsy• Generally: carbamazepine (CI absences) or lamotrigine
(CI myoclonus) for focal epilepsy• Importance of explaining side-effects

References
NICE (2012) The epilepsies: the diagnosis and management of the epilepsies in adults and children in primary and secondary care. NICE Clinical Guideline 137
Berg et al. (2010) Revised terminology and concepts for organisation of seizures and the epilepsies: report of the ILAE commission on classification and terminology, 2005-2009. Epilepsia 51(4): 676-685
Panayiotopoulos (2005) The Epilepsies: seizures, syndromes and management. Bladon Medical, Oxford