Embed Size (px)
Citation preview

EP Show – Aug 2003
ICDs – Primary prevention
The EP Show: Which ICD for which patient? Part 2: Primary preventionEric Prystowsky MD
Director, Clinical Electrophysiology Laboratory St Vincent Hospital
Indianapolis, IN
Helmut Klein MD Head of Division of CardiologyOtto-von-Guericke Universität MagdeburgMagdeburg, Germany
Paul Dorian MD Professor of MedicineDivision of cardiologySt Michael's HospitalToronto, ON

EP Show – Aug 2003
ICDs – Primary prevention
Major trials
Primary prevention patients
MUSTT:• CAD • EF <40%
MADIT I: • CAD • EF <35%
MADIT II:• CAD • EF <30%

EP Show – Aug 2003
ICDs – Primary prevention
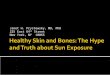
Control
ICD
ICD benefit
0
10
20
30
40
MADIT II
2-y
ear
all-c
au
se m
ort
ality
(%
)
31%
MUSTT MADIT I
54%51%
Relative reduction

EP Show – Aug 2003
ICDs – Primary prevention
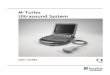
• EF <40% • CAD • Spontaneous nonsustained ventricular tachycardia (VT-NS)
MUSTT
ICDs (n=161)
Drug therapy (n=153)
p
24% 55% <0.001
Buxton et al. N Engl J Med 1999;341(25):1882-90.
Entry Criteria
Total mortality (5 years)

EP Show – Aug 2003
ICDs – Primary prevention
Control
ICD
ICD benefit
0
10
20
30
40
MADIT II
2-y
ear
all-c
au
se m
ort
ality
(%
)
31%
MUSTT MADIT
54%51%
Relative reduction

EP Show – Aug 2003
ICDs – Primary prevention
Nonischemic
0
2
4
6
8
10
12
14
All-c
ause m
ort
ality
(%
)
CAT AMIOVERT
Control ICD

EP Show – Aug 2003
ICDs – Primary prevention
Two questions
Why has it not been possible to show a survival benefit with ICDs for nonischemic cardiomyopathy patients?
Why haven't more ICDs been used in primary prevention in light of the positive data from trials?
Prystowsky

EP Show – Aug 2003
ICDs – Primary prevention
Nonischemic sudden death
The mechanism for sudden death may not be the same in nonischemic patients; they are less likely to have a new ischemic event
The intermediate term prognosis for nonischemic patients seems to be better
• Arrhythmia mechanisms may be different
• Beta blockers may be more effective
• ICDs may give less "bang for the buck"
Dorian

EP Show – Aug 2003
ICDs – Primary prevention
Jury is still out
"We have to be very careful to remember that absence of proof is not the same as proof of absence."
It is not yet proven that patients with dilated cardiomyopathy benefit from ICDs as primary prophylaxis, but [there is] also no proof ICDs are useless in this population
Numerous upcoming trials may shed further light on the issue
Dorian

EP Show – Aug 2003
ICDs – Primary prevention
Primary prevention
"Clearly we don't know everything we need to know about the magnitude of benefit from implanted defibrillators"
Few doubt ICDs are effective
The question is the likelihood of a patient actually suffering sudden death
• If small, the overall benefit is small
• If large, the overall benefit is large
Dorian

EP Show – Aug 2003
ICDs – Primary prevention
Insurance metaphor
A wood house heated by coal or wood needs good fire insurance, while a brick house not heated often doesn't need fire insurance
"How likely do we think it is that patients at potential risk for sudden death will actually have ventricular defibrillation or VT and be rescued by their defibrillator?"
Dorian

EP Show – Aug 2003
ICDs – Primary prevention
CMS decision
CMS did a subgroup analysis of MADIT II to give only partial coverage of ICDs—similar to the house metaphor
With limited resources one must pick the patients who clearly will get the most benefit
"If defibrillators cost a buck a piece, we wouldn't have the argument."
Prystowsky

EP Show – Aug 2003
ICDs – Primary prevention
ICDs in Europe
Why are there different approaches to ICDs in Germany and France?
"It's more a philosophic issue than a medical issue."
"It doesn't make sense that there is a difference between France and
Germany and Italy; I cannot explain this."
Klein

EP Show – Aug 2003
ICDs – Primary prevention
Nonischemic cardiomyopathy
The progress of nonischemic cardiomyopathy is very difficult to predict
Patients with long-lasting nonsustained VT have a worse prognosis
We tend to give long-lasting nonsustained VT patients ICDs, even when they are nonischemic
• A personal opinion
Klein

EP Show – Aug 2003
ICDs – Primary prevention
Need more parameters
More parameters [are needed] to judge risk in nonischemic patients because they have a high risk of sudden death
There is the parameter of nonsustained VT indicating higher risk
Klein

EP Show – Aug 2003
ICDs – Primary prevention
Primary prevention
So far in Germany, any patient meeting the criteria have received an ICD, but this is changing toward a more careful husbanding of resources
"We have had no problems so far, but it's getting worse and we will probably be forced to do so."
Klein

EP Show – Aug 2003
ICDs – Primary prevention
CMS coverage
CMS decided to provide reimbursement for patients with MADIT II criteria but only those with a QRS duration of >120 ms
"Frankly, having reviewed the data in the literature so far, that does seem to at least be the wood house. It doesn't mean we shouldn't be protecting the
nonwooden houses."
Prystowsky

EP Show – Aug 2003
ICDs – Primary prevention
Optimal therapy
"We believe strongly that patients should be considered for prophylactic ICD if and only if their other therapies have been absolutely optimized."
In a practical sense, this means many patients recommended for ICDs are ruled out by this more stringent approach
Dorian

EP Show – Aug 2003
ICDs – Primary prevention
MIRACLE
End point Control group
95% CI CRT group
95% CI p
Quality-of-life score
-11.0 -16 to -7 -17.5 -21 to -14 0.02
NYHA class 0 -1 to 0 -1 -1 to –1 0.007
Change in 6-minute walk distance (m)
53 43 to 75 55 44 to 79 0.36
Young JB et al. JAMA 2003; 289:2685-2694.

EP Show – Aug 2003
ICDs – Primary prevention
COMPANION
Measure CRT (%) CRT-ICD (%)Mortality and hospitalization
19 19
Mortality 23.9 43.4
Relative reduction at 12 months:compared with control arm
ACC 2003

EP Show – Aug 2003
ICDs – Primary prevention
Biventricular ICD
COMPANION showed that resynchronization improves quality of life and performance, but only the defibrillator improves the survival
"You cannot prevent sudden death by just improving ventricular function. . . . And if I have to make the choice, I certainly would use the combined device in coronary artery disease patients."
Klein

EP Show – Aug 2003
ICDs – Primary prevention
Biventricular pacemakers
"I have yet to implant a biventricular pacemaker [for this group of people]."
The data showing an advantage in preventing sudden death with the ICD function are very clear
"Am I just being too aggressive?"
Prystowsky

EP Show – Aug 2003
ICDs – Primary prevention
Changing approach
"Our thinking has evolved in this topic."
We started doing a number of pacemaker-only devices, but evidence is mounting that improving ventricular function has only modest effects in preventing arrhythmia
The extra risks and costs of adding the ICD function are not dramatic, and we are implanting more biventricular ICDs
Dorian

EP Show – Aug 2003
ICDs – Primary prevention
Choosing patients
Patients who clearly are in severe heart failure despite optimal medical treatment we tend to give biventricular ICDs
Those who have QRS of 120 or so but no severe heart failure might not get the ICD function
Klein

EP Show – Aug 2003
ICDs – Primary prevention
The broader view
"It's important to not just see the data as they are published but also to be
able to put them in context with a world of experience."
Prystowsky

EP Show – Aug 2003
ICDs – Primary prevention
Secondary prevention
Patients with documented cardiac arrest, sustained VT, syncope in the EP lab
Randomized trials point toward ICDs as therapy for these patients
DAVID trial suggests not pacing the ventricle, selecting which device is left to the physician
Prystowsky

EP Show – Aug 2003
ICDs – Primary prevention
Primary prevention
Randomized trials show that in ischemic heart disease ICDs are the best choice for therapy
For the nonischemic patients, the data are still not in and more data are needed
Depending on your budget, how narrow your selection process is will vary
Prystowsky

EP Show – Aug 2003
ICDs – Primary prevention
Biventricular devices
The biventricular ICD prolongs life, not just a biventricular pacemaker
The selection for a given patient will depend on multiple factors
There are still situations where a doctor or investigator may pick a biventricular pacemaker only
Prystowsky

EP Show – Aug 2003
ICDs – Primary prevention
The EP Show: Which ICD for which patient? Part 2: Primary preventionEric Prystowsky MD
Director, Clinical Electrophysiology Laboratory St Vincent Hospital
Indianapolis, IN
Helmut Klein MD Head of Division of CardiologyOtto-von-Guericke Universität MagdeburgMagdeburg, Germany
Paul Dorian MD Professor of MedicineDivision of cardiologySt Michael's HospitalToronto, ON