-
8/12/2019 enuresis data
1/9
REVIEW
Lower urinary tract function in childhood; normaldevelopment and
common functional disturbances
T. Neve us1
and U. Sille n2
1 Department of Womens and Childrens Health, Uppsala University,
Uppsala, Sweden2 Paediatric Urology Unit, Queen Silvias Childrens
Hospital, Goteborg, Sweden
Received 22 November 2011,revision requested 2 April
2012,revision received 28 May 2012,accepted 10 September
2012Correspondence: T. Neve us, MD,PhD, Department of Womensand
Childrens Health, UppsalaUniversity Childrens Hospital,Uppsala
University, 751 85 Upp-sala, Sweden.E-mail:
[email protected]
AbstractThis review aims to provide researchers and clinicians
involved with theadult lower urinary tract with background
knowledge regarding the earlydevelopment of bladder function and
its most common disturbances in
childhood. Bladder development begins in weeks 4 6 and the
detrusormuscle is formed during weeks 9 12 of gestation. Higher CNS
centres areinvolved in micturition at birth, and the infant usually
wakes up, at leastbriey, to void. Voiding during the rst years of
life is often incomplete,owing to detrusor-sphincter
dyscoordination, but this disappears whenbladder control is
attained. Approximately 5 10% of 7-year-old childrensuffer from
daytime incontinence and/or nocturnal enuresis, and a few percent
of them will not outgrow it. Daytime incontinence in childhood
isusually attributable to detrusor overactivity, although it is
unclear to whatextent it is the detrusor or the micturition reex
per se that is overactive.Enuresis nocturnal incontinence is caused
by either nocturnal polyuria
and/or nocturnal detrusor overactivity, in both cases combined
with higharousal thresholds. Bladder problems in childhood
constitute a risk factorfor the development or persistence of
bladder problems in adulthood.Keywords children, enuresis, foetal
development, incontinence, infants,lower urinary tract,
urodynamics.
This review is a brief overview of the normal evolu-tion of
lower urinary tract (LUT) function from foetallife until the age
when bladder control is attained.The most common disturbances of
this function, thatis, urge incontinence and nocturnal enuresis,
are alsodescribed. The pathogenic mechanisms behind theseconditions
are discussed but space does not permit usto go into the clinical
management here. Neither willwe be able to provide information
regarding otherimportant types of LUT dysfunction such as
dysfunc-tional voiding, neurogenic bladder or malformations.
Throughout this document, we will use globallyaccepted
paediatric LUT terminology as described bythe International
Childrens Continence Society (ICCS;Neveus et al. 2006).
Foetal development of the LUT and function
The bladder begins to develop early, in gestationalweeks 4 6,
from the urogenital sinus, which, in turn,is formed through
demarcation from the cloaca. Theureter and the vesicoureteral
junction are formedfrom the ureteric bud, an outgrowth on the
Wolfanduct. The ureteric bud also elongates and grows intothe
metanephros the kidney-forming mesenchyme and makes contact with
the nephrons. An abnor-mally high position of the ureteric bud on
theWolfan duct is thought to be responsible forprimary
vesico-ureteric reux (VUR), with a lateral-ized ureteral insertion
in the bladder. This displace-ment of the ureteric bud can also
cause renal
2012 The AuthorsActa Physiologica 2012 Scandinavian
Physiological Society, doi: 10.1111/apha.12015 85
Acta Physiol 2013, 207, 8592
-
8/12/2019 enuresis data
2/9
dysplasia, which is often seen together with VUR(Murer et al.
2007).
In studies of the human foetus, scattered muscle cellsare seen
in the bladder as early as the 9th week of gesta-tion, in the 12th
week the three-layered wall structure isevident and the bladder
wall thickness then increases in
a linear fashion throughout foetal life (Koerner et al.2006).
The external sphincter appears rst as a horse-shoe-shaped structure
around the urethra (Ludwikow-ski et al. 2001). Development of a
circular muscularstructure at the bladder neck has also been noted.
Thislatter structure has been shown to be hypertrophic inthe male
foetus towards the end of gestation, whichmay be one of the
explanations for the difference inbladder function variables
between male and femaleneonates (Oswald et al. 2006).
Regarding development of LUT function during foe-tal life,
changes in the intrinsic properties of thesmooth muscle and
peripheral neurotransmission haveto be considered. In animal
studies, it has been shownthat compliance in the bladder wall is
poor duringearly gestation when urine production starts,
butincreases during the second half of foetal life, anevolution
partly due to a gradual switch from collagenIII to I (Sze ll et al.
2003, Oswald et al. 2006).Increased tone as well as increased
spontaneous activ-ity in the detrusor has also been documented as
thefoetus evolves. This activity is not nerve mediated andmay be
necessary to promote voiding when the neuro-nal control is
incomplete and storage capacity minimal(Ekman et al. 2009). The
human bladder has some
reservoir capacity at 16 weeks of gestation. A decreasein
spontaneous detrusor activity and tone, concomi-tant with increased
activity in the bladder outlet, bothcontribute to an enhanced
storage function as the foe-tus matures (Sze ll et al. 2003).
It has also been shown in animal studies that theneonatal
detrusor has an increased or different reactiv-ity to stimuli.
Stimulation with a cholinergic agonistleads to multi-phasic
contraction in the neonatal blad-der and uni-phasic contractions in
the adult. Thisresemblance between the neonatal pattern and
detrusoroveractivity made the authors speculate about
delayedmaturation as an explanation for the latter condition(Ekman
et al. 2009).
Bladder function in neonates and infants
Most studies of the normal infant bladder rely on the4-h voiding
observation, which is non-invasive andgives information regarding
storage and emptyingcapacity (Holmdahl et al. 1996), but a limited
numberof cystometric studies have also been performed.
Less than 10% of healthy neonates and infants
havecystometrically detectable detrusor overactivity, a
nding that contradicts the above suggestion of detru-sor
overactivity as an immaturity phenomenon (Yeunget al. 1995, Jansson
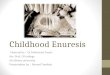
et al. 2005). On the other hand,an increased reactivity of the
detrusor muscle duringthe rst months of life has been detected
whencomparing cystometric versus free voiding studies;
catheter-based investigations can induce voiding con-tractions
at much lower bladder volumes (Fig. 1;Bachelard et al. 1999). This
nding might be a paral-lel to the increased spontaneous activity
seen in thefoetal and neonatal detrusor in experimental animals,as
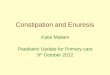
discussed above. The phenomenon probably alsoexplains the lower
voided volumes seen in cystometricinvestigations in the neonatal
period and during therst couple of months as compared with the
volumesobserved in free voiding studies (Fig. 2; Sillen 2004).After
infancy, the picture is reversed: the children voidsmaller volumes
than their cystometric bladdercapacity (Sille n 2004). This latter
relation betweencatheter-based and free voiding volumes remains
duringchildhood and is probably explained by voluntary
post-ponement of voiding in catheter-based investigations.
In both cystometric and free voiding studies,
detru-sor-sphincter dyscoordination has been shown to be anormal
part of the voiding pattern in neonates andinfants. In free voiding
studies, it is recognized asinterrupted voiding dened as two
voidings within5 10 min, with the lowest residual after the
secondvoiding. This is clearly an immaturity phenomenon as itis
seen in 60% of premature infants but then decreasesand disappears
when voluntary bladder control is
achieved (Jansson et al. 2000). In cystometric investiga-tions,
dyscoordination at voiding has been found in anumber of
investigations of neonates and infants as anintermittent increase
in sphincter electromyography(EMG) during the voiding contraction
and a concomi-tant uctuation in voiding pressure and the
urinarystream (Fig. 1; Jansson et al. 2005, Olsen et al. 2010).An
interrupted ow pattern was also observed in younginfant boys, in
studies where urinary ow was recordedwith an ultrasound probe
(Olsen et al. 2010). It isunknown whether this physiological
dyscoordination isonly an expression of immature nervous control or
if the increased excitability of the detrusor, discussedabove, is
also responsible. Support for the latter theory,however, is
provided by the fact that infants withknown overactivity during
lling, such as boys withposterior urethral valves, are especially
prone to inter-rupted voiding (Holmdahl et al. 1998).
Neonates and infants do not empty their bladdercompletely every
time they void, but usually at leastonce per four hours there is no
residual urine (Holm-dahl et al. 1996). The dyscoordination at
voidingabove discussed is probably responsible for the incom-plete
emptying, which is in accord with the fact that
2012 The AuthorsActa Physiologica 2012 Scandinavian
Physiological Society, doi: 10.1111/apha.1201586
The paediatric lower urinary tract T Neve us and U Sille n Acta
Physiol 2013, 207, 8592
-
8/12/2019 enuresis data
3/9
emptying becomes complete when bladder control is
achieved, that is, when coordination becomes normal(Jansson et
al. 2000).Sexual differences in neonatal and infantile bladder
function have been observed, mainly regarding voidingpressure
that is higher in male infants (median120 cm H 2 O; Fig. 1; Jansson
et al. 2000, 2005). Theexplanation for this is probably the
dyscoordinationthat effectively closes the outow during detrusor
con-traction. The high pressure levels, however, are onlygenerated
when bladder capacity is low. Therefore,the increased reactivity of
the detrusor musclediscussed above might inuence the generation of
highpressure by inducing contractions at low bladder vol-ume. But
this does not in itself explain the differencebetween the sexes, as
dyscoordination and increasedexcitability have also been found in
female neonates.The most obvious difference is the longer urethra
inmales, which is probably responsible for increasedoutow
resistance. The more pronounced bladderneck muscles in the male
foetus at the end of gesta-tion, mentioned above, might have the
same effect(Oswald et al. 2006).
It has traditionally been assumed that micturition inthe neonate
occurs as a purely spinal reex, without
involvement of the pontine micturition centre and the
frontal cortex. This assumption has now been chal-lenged. One
reason to believe that higher CNS centresare involved is the fact
that most term neonates andinfants wake up, or at least show signs
of arousal,before voiding (Yeung et al. 1995, Jansson et al.2005).
This awakening and arousal mechanism onlyfunctions in a minority
preterm children, on the otherhand (Sille n et al. 2000). This
difference indicates thatthe CNS connections involved in the
voiding reex aresufciently mature in full-term neonates to
inuencecentres of importance for arousal, when activated by afull
bladder. Furthermore, neither preterm nor full-term infants void at
constant bladder volumes (Sille n2004), an observation that also
supports the conceptof the voiding reex as associated with the
brain asearly as in the neonatal period.
Summary of immature bladder function characteris-tics
(1) Free voiding studies.(a) Interrupted voiding.(b) Incomplete
emptying.(c) Voiding once or twice every 2 h.(d) The child wakes up
or shows signs of arousal
at voiding.
Premature voiding Voiding(BC 15 mL)
Bachelard et al, 1999
Figure 1 Urodynamic study in 1 monthold boy showing premature
voiding con-traction and voiding at low bladder vol-ume. Note
dyscoordination at voidingwith increased EMG signal.
Fullterminfants
0
20
40
60
80
100
120
140
4 2 0 2 4 6
Age (months)
B l a d d e r c a p a c i
t y ( m L )
Prematureinfants
Cystometric
Free voiding
Expected
Figure 2 Cystometric and free voidingbladder capacity in
premature (19) andfull-term (12) infants. Formula for esti-mation
of expected bladder capacityaccording to International
ChildrensContinence Society standarisation (1).
2012 The AuthorsActa Physiologica 2012 Scandinavian
Physiological Society, doi: 10.1111/apha.12015 87
Acta Physiol 2013, 207, 8592 T Neve us and U Sille n The
paediatric lower urinary tract
-
8/12/2019 enuresis data
4/9
(2) Cystometry.(a) Increased excitability of detrusor with
voiding
contraction at low volume.(b) Overactive contractions rarely
seen (10%).(c) Cystometric capacity lower as compared with
free voiding.
(d) Dyscoordination at voiding.(e) High voiding pressure in
males.
Normal development in childhood
Both maturation of the CNS and adequate social cir-cumstances
are necessary for the development of vol-untary bladder control.
Potty training can be verybenecial, provided it is kind and not
forceful. Ideally,it should be initiated when the child starts to
be inter-ested in what is happening. The childs interest
usuallystarts at about 18 months of age, when he or shereports I
have voided. The next step is when thechild recognizes I am
starting to void, followed bythe ability to postpone voiding for a
few moments. Atthis stage, the child is able to reach the toilet in
timefor voiding. Before reaching complete continence, thechild must
be able to start voiding at any bladder vol-ume and also to
interrupt voiding voluntary. Beingsocially continent means that the
child takes care of the whole voiding situation from start to nish,
a skillthat is usually achieved at 5 6 years of age (Janssonet al.
2005).
As mentioned above, the immature detrusor-sphinc-ter
dyscoordination disappears at the age when blad-
der control is achieved. Furthermore, bladder capacityhas been
found to increase stepwise during toilettraining, a fact that is
probably attributable to theability to hold urine voluntarily. The
voidingfrequency is decreased from approximately once perhour in
the neonatal period to 7 8 times per day inthe toddler.
It should be noted that it is possible to make thechild dry much
earlier if he or she is regularly put onthe potty by a parent who
has learned to recognizethe childs signs of imminent voiding. The
degree of maturation for such training to be possible is
presentalready in the rst year of life. This type of trainingwas
used in Western countries before the era of super-absorbable
diapers and is still practiced in countrieswith other traditions
and nancial standards. Suchearly training has been shown to improve
the childsability to empty the bladder completely and
shouldprobably be encouraged in children with recurrenturinary
tract infections (Duong et al. 2010).
Summary of bladder function at toilet-training age(1) Free
voiding studies.
(a) Emptying complete.(b) Voiding 7 8 times a day.
(c) Stepwise increase in voided volumes.(d) The child takes an
interest in his/her own toi-
leting.(2) Cystometry.
(a) Cystometric capacity higher than voided vol-umes.
(b) Urethral sphincter relaxed during voiding.(c) Voiding
detrusor pressure decreased to adultlevels.
Common functional disturbances:epidemiology and comorbidity
It is obvious that the complex maturation processdescribed above
does not always go smoothly. Chil-dren become socially continent at
different ages, andin some cases, bladder control is not achieved
or isachieved only temporarily. The most common LUTdisturbances by
far are nocturnal enuresis anddaytime incontinence owing to
detrusor overactivity.
According to the ICCS standardization document,the word enuresis
, synonymous with nocturnal incon-tinence, is used to denote the
involuntary leakage of urine during sleep in discrete portions (as
opposed tocontinuous dribbling) in a child aged 5 years or more.If
the enuretic child also exhibits daytime LUTsymptoms such as
urgency, frequency or daytimeincontinence, the enuresis is
subspecied as non-monosymptomatic enuresis. The term diurnal
enure-sis should be avoided, instead speaking of
daytimeincontinence . Urge incontinence simply means daytime
incontinence in a child who also experiences urgency(Neveus et
al. 2006).
The prevalence of enuresis and daytime inconti-nence across the
paediatric age span is illustrated inTable 1 (Hellstro m et al.
1990, Hirasing et al. 1997,Bakker et al. 2002, So derstro m et al.
2004). As canbe noted, these are very common conditions and theymay
persist for many years or even into adulthood. Ithas also been
shown that for the enuretic child whowets his or her bed every
night, the chance of sponta-neous resolution before adulthood is
signicantlylower than for children with more sporadic
enuresis(Yeung et al. 2006). Enuresis is more common among
Table 1 Prevalence of daytime incontinence and enuresis
indifferent ages
5 years 7 years 10 yearsTeenage Adults
Daytimeincontinence (%)
10 15 5 10 3 8 2 5 1 3
Nocturnalenuresis (%)
10 15 5 10 3 7 1 4 0.5 2
2012 The AuthorsActa Physiologica 2012 Scandinavian
Physiological Society, doi: 10.1111/apha.1201588
The paediatric lower urinary tract T Neve us and U Sille n Acta
Physiol 2013, 207, 8592
-
8/12/2019 enuresis data
5/9
boys than girls, while for daytime incontinence the sit-uation
is the reverse (Hellstro m et al. 1990, Bakkeret al. 2002).
There is a considerable epidemiologic overlapbetween daytime
incontinence and nocturnal enuresis(Hellstro m et al. 1990, Bakker
et al. 2002), reecting
their overlapping pathogenetic mechanisms. It shouldalso be
mentioned that constipation, with or withoutfaecal incontinence, is
often part of the picture,especially in children with daytime
incontinence(So derstro m et al. 2004). These children are also
athigher than normal risk at developing urinary tractinfections
(Loening-Baucke 1997).
Daytime incontinence
The typical child with daytime incontinence is a girl(although
boys are certainly no rarities) who alsoexperiences some degree of
urgency symptoms. Shemay have to run to the toilet very often or
has made ahabit of postponing micturition as long as possibleusing
various holding manoeuvres such as standingon tiptoe or squatting
with her heel pressed againstthe perineum. Urinary tract infections
are quitecommon in these children, as is constipation
(Loening-Baucke 1997). Only very little research has been car-ried
out on the inheritability of the condition, butrecent work suggests
that it does indeed often run infamilies (von Gontard et al.
2011).
It may be safely assumed that the most commonmechanism
underlying paediatric daytime incontinence
is detrusor overactivity (Cisternino &
Passerini-Glazel1995). These children do not suffer from stress
incon-tinence. But what underlies the detrusor overactivity ismuch
more difcult to determine. Far too much spec-ulation regarding
pathogenesis has relied on researchcarried out in adults.
Detrusor overactivity during bladder lling isbelieved to be the
central cause of urge incontinence.Studies in adults, however,
indicate that involuntarydetrusor contractions are often preceded
by involun-tary sphincter relaxation more or less as in the nor-mal
micturition indicating that in these cases it isthe micturition
reex per se, not the detrusor contrac-tion, that is pathologically
easy to elicit (Artibani1997, McLennan et al. 2001). The
explanation for theincreased detrusor and/or sphincter excitability
is notknown. As it is seen in a relatively large number of young
children and as increased excitability is seen inthe neonatal
detrusor, a delayed maturation can beput forward as a possibility.
Connections betweendetrusor overactivity and delayed maturation are
alsosupported by the involvement of afferent unmyeli-nated C-bres
in detrusor overactivity (Yokoyamaet al. 2004), bres which are
involved in foetal and
neonatal micturition but not in the mature reex.A positive
bladder cooling reex in up to 50% of these children points in the
same pathogenetic direc-tion (Gladh et al. 2004), as this reex has
been shownto be positive in healthy infants, but after 2 4 yearsof
age is considered to be a sign of spinal damage.
If the micturition reex as such is not disturbed butdetrusor
contractions appear without warning, oneexplanation could be that
the excitation contractioncoupling to the detrusor is disturbed.
Animal researchand research in adults have implicated a large
numberof neurotransmitters and other factors as causative.The
purinergic contribution to detrusor (over-)activitydeserves special
mention here, as the pattern of ATP-specic receptors in the
detrusor of adults with urgeincontinence both differ from that of
controls and hassimilarities with that of small children (Moore et
al.2001). These results again suggest that detrusor over-activity
has similarities with early developmentalphases of bladder
function.
Urge incontinence in childhood can also be second-ary to other
problems. There is a well-documentedassociation between
constipation and incontinence(Loening-Baucke 1997). The theory
behind thisconnection is that the distended bowel compressingthe
bladder may lead to an interruption of the normalperipheral
inhibition of micturition provided by thesphincter and pelvic
oor.
In conclusion, detrusor overactivity in childhoodcan be assumed
to be pathogenetically multifactorial.The disturbance may be
centrally or peripherally med-
iated, owing to motor or sensory disturbance, of amyogenic or
perhaps a psychogenic nature. Mecha-nisms active at an earlier
developmental phase of bladder function may be of aetiological
importance.
Enuresis
The typical enuretic child is otherwise healthy and ismore often
a boy than a girl. There may be concomi-tant daytime symptoms such
as urgency or inconti-nence. Psychiatric symptoms are contrary to
earlierbeliefs usually not present, but many enuretic chil-dren
have low self-esteem because of their condition(Ha gglo f et al.
1997), and there is an overrepresenta-tion of children with
hyperactivity and/or attentiondifculties in the bedwetting group
(Duel et al. 2003).
Enuresis often runs in the family (Devlin 1991).This observation
is, however, of little clinical use, as ithas been found that no
predictions regarding progno-sis or therapeutic outcome can be
extracted from fam-ily history.
The main pathogenic mechanism is the inability towake up in
response to activation of the micturitionreex. As most neonates
already have the ability to
2012 The AuthorsActa Physiologica 2012 Scandinavian
Physiological Society, doi: 10.1111/apha.12015 89
Acta Physiol 2013, 207, 8592 T Neve us and U Sille n The
paediatric lower urinary tract
-
8/12/2019 enuresis data
6/9
wake up at voiding (Yeung et al. 1995), the disturbancecan be
suggested to be an early developmental errorrather than immaturity.
Beside this evident cause,research in recent decades has
established two patho-genic mechanisms as crucial to nocturnal
enuresis: noc-turnal polyuria and nocturnal detrusor
overactivity.
Many bedwetting children produce disproportion-ately large
amounts of urine at night, and this noctur-nal polyuria may often,
but not always, be explainedby a lack of the normal nocturnal peak
in the releaseof vasopressin from the pituitary (Rittig et al.
1989).These children wet their beds because their urine pro-duction
is greater than what can safely be stored intheir bladders. More
support for the polyuria hypothe-sis is derived from the
observation that bedwettingcan be provoked in some non-enuretic
children just byhaving them drink lots of water before bedtime
(Ras-mussen et al. 1996) and the fact that the vasopressinanalogue
desmopressin makes many bedwetters dry
especially ones with polyuria (Hunsballe et al. 1995).There are,
however, some modications to the
hypothesis. First, not all bedwetting children havepolyuria at
night (Hunsballe et al. 1995). Second,some dry children are
polyuric (and have nocturia;Mattsson & Lindstro m 1994). Third,
the polyuriadoes not explain why the child does not wake up.Fourth,
it is conceivable that in some cases the poly-uria may be the
effect rather than the cause of theenuresis as lack of bladder
distension, or sleepdisturbance per se, may increase urine
production(Mahler et al. 2012).
Soon after the polyuria explanation was launchedand
corroborated, other researchers discovered thatsome enuretic
children wet their beds not because theirbladders are full but
because they contract too easily.Ambulatory cystometric
examinations of children withtherapy-resistant enuresis conrmed
that nocturnaldetrusor overactivity is indeed common in this
group(Yeung et al. 1999). Further albeit indirect evidence isthe
epidemiological overlap between nocturnal enuresisand urge
incontinence, the fact that enuretic children especially the
non-polyuric ones void with smallervolumes than dry children (Neve
us et al. 2001) and theexperience that anticholinergics may
help.
Yet still, not all bedwetting children have
detrusoroveractivity, many non-bedwetters have symptoms of detrusor
overactivity i.e. urgency and we still needto explain why the
children do not wake up.
It is often stated that the nocturnal bladder volume isreduced
in enuretic children. This statement is in a waytrue but also quite
misleading. The bladder is not ana-tomically small, but it tends to
contract before it is full.
Both bladder distension and detrusor contractionsare strong
arousal stimuli (Page & Valentino 1994).The bedwetting child
can thus be regarded as a deep
sleeper almost by denition. This accords well withthe almost
universal parental observation of enureticchildren being difcult to
wake up at night and is alsosupported by studies on objective
arousal thresholds(Wolsh et al. 1997). This does not, however,
meanthat the sleep EEG of enuretic children is necessarily
different from that of dry children. Sleep stage distri-bution
and other polysomnographical parameters donot consistently differ
between enuretic and dry chil-dren (Bader et al. 2002), but they
are more difcult toarouse from sleep at night.
The disorder of arousal in enuretic children mayhave underlying
brainstem explanations, or it may,paradoxically, be caused by the
arousal stimuli them-selves. If someone (or in this case the
bladder) isalways knocking at the door, you end up ignoring itor
even installing an extra lock. This mechanism mayexplain the
observation that some enuretic childrenwith sleep apnoeas
attributable to enlarged tonsils ornasal adenoids will become dry
at night when theirupper airway obstruction is surgically
removed(Weider et al. 1991).
In summary, the enuretic child wets his/her bedbecause either
(i) bladder distention due to nocturnalpolyuria fails to wake
him/her up or (ii) uninhibiteddetrusor contractions fail to wake
him/her up, orboth. This is illustrated graphically in Figure
3.
There is now an increasing body of evidence indi-cating that all
three pathogenetic disturbances may becaused by an underlying
brainstem disturbance. Thelocus coeruleus (LC) in the upper pons is
crucial for
arousal from sleep (Kayama & Koyama 1993) andoverlaps
(functionally and anatomically) with the pon-tine micturition
centre (Holstege et al. 1986). It is alsothe main nucleus of the
central sympathetic nervoussystem and has direct and indirect
axonal connectionswith the vasopressin-producing hypothalamic
supraop-tic nucleus (Lightman et al. 1984).
Experiments measuring the startle blink reex(a test assessing
brainstem contribution to alertness;
Nocturnal
polyuria
Detrusor
overactivity
High arousal thresholds
Day-timeincontinence
Urgency
Nocturia
Enuresis Enuresis
Enuresis
Sound,undisturbedsleep
Suspected major pathogenetic factors in nocturnal enuresis
Figure 3 Suspected major pathogenetic factors in
nocturnalenuresis.
2012 The AuthorsActa Physiologica 2012 Scandinavian
Physiological Society, doi: 10.1111/apha.1201590
The paediatric lower urinary tract T Neve us and U Sille n Acta
Physiol 2013, 207, 8592
-
8/12/2019 enuresis data
7/9
Ornitz et al. 1999), overnight measurements of sym-pathetic and
parasympathetic tone (using heart ratevariability analysis;
Fujiwara et al. 2001) and theobservation that the antienuretic
activity of imipra-mine is dependent on its main metabolite binding
tothe LC (Danysz et al. 1985) all contribute to support-
ing the hypothesis that enuresis may be caused by adisturbance
in this region.
Adulthood consequences of disturbances inchildhood
As mentioned above, not all incontinent or bedwettingchildren
grow out of their condition. A schoolchildwith severe enuresis has
a very real risk of continuingto wet the bed into adulthood if we
are unable to curehim or her. The prevalence of enuresis in
adulthood isapprox. 0.5% (Hirasing et al. 1997). It has also
beenshown that micturition problems in childhood aresignicant risk
factors for developing micturitionproblems in adulthood. More
specically, adults withurge incontinence (as opposed to stress
incontinence)have often suffered from enuresis or daytime
inconti-nence as children (Kuh et al. 1999). This may reectan
overexcitability of the detrusor or of the micturi-tion reex that
does not disappear even when or if the child becomes dry.
Enuresis and/or daytime incontinence causes low self-esteem in
the aficted children (or adults; Ha gglo f et al.1997). The
psychosocial consequences of this areunknown, butprobably not
trivial. Reports about enure-
sis being common among criminals, previously taken asevidence to
the enuresis being caused by early trauma orpsychiatric regression
(Stein & Susser 1965), probablyreect both the consequences of
poor self-esteem and theoverrepresentation of children with
neuropsychiatricdisorders such as attention decit hyperactivity
disorder(ADHD) in the enuretic population.
Finally, the detrusor overactivity that underlies mostcases of
daytime incontinence and many cases of enuresis is per se a risk
factor for urinary tract infec-tions, VUR and kidney damage. There
is thus everyreason for adult and paediatric urologists,
nephrolo-gists and researchers to unite in their efforts to
helpmake these children dry !
Conict of interest
The authors have no present or conceivable conictsof interest to
report.
References
Artibani, W. 1997. Diagnosis and signicance of
idiopathicoveractive bladder. Urology 50 , 25 32.
Bachelard, M., Sille n, U., Hansson, S., Hermansson, G., Jod-al,
U. & Jacobsson, B. 1999. Urodynamic pattern inasymptomatic
infants: siblings of children with vesicouret-eral reux. J Urol 162
, 1733 1738.
Bader, G., Neve us, T., Kruse, J. & Sille n, U. 2002. Sleep
of primary enuretic children and controls. Sleep 25 , 579 583.
Bakker, E., van Sprundel, M., van der Auwera, J.C., van
Gool,
J.D. & Wyndaele, J.J. 2002. Voiding habits and wetting in
apopulation of 4,332 Belgian schoolchildren aged between 10and 14
years. Scand J Urol Nephrol 36 , 354 362.
Cisternino, A. & Passerini-Glazel, G. 1995. Bladder
dysfunc-tion in children. Scand J Urol Nephrol 2 , 5 29.
Danysz, W., Kostowski, W. & Hauptmann, M. 1985. Evi-dence
for the locus coeruleus involvement in desipramineaction in animal
models of depression. Pol J Pharmacol Pharm 37 , 855 864.
Devlin, J.B. 1991. Prevalence and risk factors for
childhoodnocturnal enuresis. Ir Med J 84 , 118 120.
Duel, B.P., Steinberg-Epstein, R., Hill, M. & Lerner, M.
2003.A survey of voiding dysfunction in children with
attentiondecit-hyperactivity disorder. J Urol 170 , 1521 1524.
Duong, T.H., Jansson, U.B., Holmdahl, G., Sille n , U.
&Hellstro m, A.-L. 2010. Development of bladder control inthe
rst year of life in children who are potty trained early. J Pediatr
Urol 6 , 501 505.
Ekman, M., Andersson, K.E. & Arner, A. 2009.
Receptor-induced phasic activity of newborn mouse bladders
isinhibited by protein kinase C and involves T-type Ca 2+
channels. BJU Int 104 , 690 697.Fujiwara, J., Kimura, S.,
Tsukayama, H., Nakahara, S., Hai-
bara, S., Fujita, M., Isobe, N. & Tamura, K. 2001.
Evalua-tion of the autonomic nervous system function in
childrenwith primary monosymptomatic nocturnal enuresis
powerspectrum analysis of heart rate variability using 24-hour
Holter electrocardiograms. Scand J Urol Nephrol 35 ,350 356.
Gladh, G., Mattsson, S. & Lindstro m, S. 2004. Outcome of
the bladder cooling test in children with nonneurogenicbladder
problems. J Urol 172 , 1095 1098.
von Gontard, A., Heron, J. & Joinson, C. 2011. Family
historyof nocturnal enuresis and urinary incontinence: results
froma large epidemiological study. J Urol 185 , 2303 2306.
Ha gglo f, B., Andre n, O., Bergstro m, E., Marklund, L.
&Wendelius, M. 1997. Self-esteem before and after treat-ment in
children with nocturnal enuresis and urinaryincontinence. Scand J
Urol Nephrol 31 , 79 82.
Hellstro m, A.-L., Hansson, E., Hansson, S., Hja lmas, K. &
Jod-al, U. 1990. Incontinence and micturition habits in
7-year-oldSwedish school entrants. Eur J Pediatr 149 , 434 437.
Hirasing, R.A., van Leerdam, F.J., Bolk-Bennink, L. &
Jank-negt, R.A. 1997. Enuresis nocturna in adults. Scand J Urol
Nephrol 31 , 533 536.
Holmdahl, G., Hanson, E., Hanson, M., Hellstro m, A.-L.,Hja
lmas, K. & Sille n, U. 1996. Four-hour voiding observa-tion in
healthy infants. J Urol 156 , 1809 1812.
Holmdahl, G., Hanson, E., Hanson, M., Hellstro m, A.-L.,Sille n,
U. & So lsnes, E. 1998. Four-hour voiding observa-tion in young
boys with posterior urethral valves. J Urol 160 , 1477 1481.
2012 The AuthorsActa Physiologica 2012 Scandinavian
Physiological Society, doi: 10.1111/apha.12015 91
Acta Physiol 2013, 207, 8592 T Neve us and U Sille n The
paediatric lower urinary tract
-
8/12/2019 enuresis data
8/9
Holstege, G., Grifths, D., De Wall, H. & Dalm, E.
1986.Anatomical and physiological observations on
supraspinalcontrol of bladder and urethral sphincter muscles in
thecat. J Comp Neurol 250 , 449 461.
Hunsballe, J.M., Hansen, T.K., Rittig, S., Nrgaard,
J.P.,Pedersen, E.B. & Djurhuus, J.C. 1995. Polyuric and
non-polyuric bedwetting pathogenetic differences in nocturnal
enuresis. Scand J Urol Nephrol S173 , 77 79. Jansson, U.-B.,
Hanson, M., Hanson, E., Hellstro m, A.-L. &
Sille n, U. 2000. Voiding pattern in healthy children 0 to3
years old: a longitudinal study. J Urol 164 , 2050 2054.
Jansson, U.-B., Hanson, M., Sille n, U. & Hellstro m,
A.-L.2005. Voiding pattern and acquisition of bladder controlfrom
birth to age 6 years a longitudinal study. J Urol 174 ,289 293.
Kayama, Y. & Koyama, Y. 1993. Brain stem mechanisms of sleep
and wakefulness. J Physiol Soc Jpn 55 , 1 14.
Koerner, I., Deibi, M., Oswald, J., Schwentner, C., Lunacek,A.,
Fritsch, H., Bartsch, G. & Radmayr, C. 2006. Genderspecic
chronological and morphometric assessment of fetal bladder wall
development. J Urol 176 , 2674 2678.
Kuh, D., Cardozo, L. & Hardy, R. 1999. Urinary inconti-nence
in middle aged women: childhood enuresis and otherlifetime risk
factors in a British prospective cohort. J Epi-demiol Community
Health 53 , 453 458.
Lightman, S.L., Todd, K. & Everitt, B.J. 1984.
Ascendingnoradrenergic projections from the brainstem: evidence
fora major role in the regulation of blood pressure and
Vaso-pressin secretion. Exp Brain Res 55 , 145 151.
Loening-Baucke, V. 1997. Urinary incontinence and urinarytract
infection and their resolution with treatment of
chronicconstipation of childhood. Pediatrics 100 , 228 232.
Ludwikowski, B., Oesch Hayward, I., Brenner, E. & Fritsch,H.
2001. The development of the external urethral sphinc-
ter in humans. BJU Int 87 , 565 568.Mahler, B.T., Kamperis, K.,
Schroeder, M., Frkier, J., Djur-
huus, J.C. & Rittig, S. 2012. Sleep deprivation
inducesexcess diuresis and natriuresis in healthy children. Am J
Physiol Renal Physiol 302 , F236 F243.
Mattsson, S. & Lindstro m, S. 1994. Diuresis and
voidingpattern in healthy schoolchildren. Br J Urol 76 , 783
789.
McLennan, M.T., Melick, C. & Bent, A.E. 2001.
Urethralinstability: clinical and urodynamic characteristics.
Neuro-urol Urodyn 20 , 653 660.
Moore, K.H., Ray, F.R. & Barden, J.A. 2001. Loss of
puriner-gic P2X3 and P2X 5 receptor innervation in human
detrusorfrom adults with urge incontinence. J Neurosci 21 , 1
6.
Murer, L., Benetti, E. & Artifoni, L. 2007. Embryology
andgenetics of primary vesico-ureteric reux and associatedrenal
dysplasia. Pediatr Nephrol 22 , 788 797.
Neve us, T., Tuvemo, T., La ckgren, G. & Stenberg, A.
2001.Bladder capacity and renal concentrating ability in enuresis
pathogenic implications. J Urol 165 , 2022 2025.
Neve us, T., von Gontard, A., Hoebeke, P., Hja lmas, K.,
Bauer,S., Bower, W., Jrgensen, T.M., Rittig, S., Vande Walle,
J.,Yeung, C.K. & Djurhuus, J.C. 2006. The standardization of
terminology of lower urinary tract function in children
andadolescents: report from the standardisation committee of
the International Childrens Continence Society (ICCS). J Urol
176 , 314 324.
Olsen, L.H., Grothe, I., Ravashdeh, Y. & Jrgensen, T.M.2010.
Urinary ow pattern in rst year of life. J Urol 193 ,694 698.
Ornitz, E.M., Russell, A.T., Hanna, G.L., Gabikian, P.,
Geh-ricke, J.G., Song, D. & Guthrie, D. 1999. Prepulse
inhibi-
tion of startle and the neurobiology of primary
nocturnalenuresis. Biol Psychiatry 45 , 1455 1466.
Oswald, J., Schwentner, C., Lunacek, A., Fritsch, H., Longa-to,
S., Sergi, C., Bartsch, G. & Radmayr, C. 2006. Reeval-uation of
the fetal muscle development of the vesicaltrigone. J Urol 176 ,
1166 1170.
Page, M.E. & Valentino, R.J. 1994. Locus coeruleus
activationby physiological challenges. Brain Res Bull 35 , 557
560.
Rasmussen, P.V., Kirk, J., Borup, K., Nrgaard, J.P. &
Djur-huus, J.C. 1996. Enuresis nocturna can be provoked innormal
healthy children by increasing the nocturnal urineoutput. Scand J
Urol Nephrol 30 , 57 61.
Rittig, S., Knudsen, U.B., Nrgaard, J.P., Pedersen, E.B.
&Djurhuus, J.C. 1989. Abnormal diurnal rhythm of
plasmaVasopressin and urinary output in patients with enuresis.Am J
Physiol 256 , F664 F671.
Sille n, U. 2004. Bladder function in infants. Scand J Urol
Nephrol Suppl 215 , 69 74.
Sille n, U., Solsnes, E., Hellstro m, A.-L. & Sandberg,
K.2000. The voiding pattern of healthy preterm neonates. J Urol 163
, 278 281.
So derstro m, U., Hoelcke, M., Alenius, L., So derling, A.-C.
&Hjern, A. 2004. Urinary and faecal incontinence: a
popula-tion-based study. Acta Paediatr 93 , 386 389.
Stein, Z. & Susser, M.W. 1965. Socio-medical study of
enuresis among delinquent boys. Br J Prev Soc Med 19 ,174 181.
Szell, E.A., Somogyi, G.T., de Groat, W.C. & Szigeti,
G.P.2003. Developmental changes in spontaneous smooth mus-cle
activity in the neonatal rat urinary bladder. Am J Phys-iol Regul
Integr Comp Physiol 285 , R809 R816.
Weider, D.J., Sateia, M.J. & West, R.P. 1991.
Nocturnalenuresis in children with upper airway obstruction.
Otolar-yngol Head Neck Surg 105 , 427 432.
Wolsh, N.M., Pivik, R.T. & Busby, K.A. 1997. Elevatedsleep
arousal thresholds in enuretic boys: clinical implica-tions. Acta
Paediatr 86 , 381 384.
Yeung, C.K., Godley, M.L., Ho, C.K.W., Duffy, P.G.,
Ransley,R.G., Chen, C.N. & Li, A.K.C. 1995. Some new
insightsinto bladder function in infancy. Br J Urol 76 , 235
240.
Yeung, C.K., Chiu, H.N. & Sit, F.K. 1999. Bladder
dysfunc-tion in children with refractory monosymptomatic
primarynocturnal enuresis. J Urol 162 , 1049 1055.
Yeung, C.K., Sreedhar, B., Sihoe, J.D., Sit, F.K. & Lau,
J.2006. Differences in characteristics of nocturnal enuresisbetween
children and adolescents: a critical appraisal froma large
epidemiological study. BJU Int 97 , 1069 1073.
Yokoyama, T., Nozaki, K., Fujita, O., Nose, H., Inoue, M.&
Kumon, H. 2004. Role of C afferent bers and monitor-ing of
intravesical resiniferatoxin therapy for patients withidiopathic
detrusor overactivity. J Urol 172 , 596 600.
2012 The AuthorsActa Physiologica 2012 Scandinavian
Physiological Society, doi: 10.1111/apha.1201592
The paediatric lower urinary tract T Neve us and U Sille n Acta
Physiol 2013, 207, 8592
-
8/12/2019 enuresis data
9/9
Copyright of Acta Physiologica is the property of
Wiley-Blackwell and its content may not be copied or
emailed to multiple sites or posted to a listserv without the
copyright holder's express written permission.
However, users may print, download, or email articles for
individual use.










![Practical consensus guidelines for the management of enuresis · monosymptomatic enuresis (MNE) [31], empirical evi- dence, and discussions of leading experts in pediatric urol- ogy](https://img.pdfslide.us/doc/110x75/5bdbed9309d3f2e0298cf9d2/practical-consensus-guidelines-for-the-management-of-enuresis-monosymptomatic.jpg)