Embed Size (px)
Citation preview

1
Clinical Decision Support System (CDSS)
Yoon KimAssistant ProfessorDepartment of Social MedicineE-mail: [email protected]: 031-299-6301
Two approaches: atomic vs. molecular
Molecular (=pre-coordinated =enumerative ) A single name/code and value
Left patellar deep tendon reflex intensity is 2 +Advantage
Concise in data storage Easy to execute decision support logic Don’t allow non-sensical statement
Atomic (=post-coordinated =compositional) Deep tendon reflex intensity is 2 +
Anatomic site is patellaLaterality is left
Advantage Better domain coverage & compositional flexibility (expressivity)
Requirement for compositional rules to avoid Combinational explosion, and anatomically implausible occurrence
RecommendationSystem should allow conversion: Atomic Molecular
Medical Injuries
As many as 44,000 to 98,000 Americans die each year from medical errors
More people die from medical injuries than from Breast Cancer or AIDS or Motor Vehicle Accidents
Direct health care costs totaling $9 - 15 billion per yearA systems approach utilizing information technology (clinical decision support systems) is needed
http://www.nap.edu/catalog/9728.html
Current Practice of Medicine
•Exploding Medical Knowledge
•Complexity of Medical System
•Exploding Medical Knowledge
•Complexity of Medical System
CurrentMedical Knowledge
Definition: Medical Informatics Medicine is fundamentally an information science
Clinicians and researchers spend a great deal of time acquiring and analyzing itThere is evidence it is not used optimally
e.g., misuse of services, medical errors, etc.There are scientific ways to determine how to use information better
The scientific field that deals with biomedical information, data, and knowledge ―their storage, retrieval, and optimal use for problem solving and decision-making.
Shortliff EH, Perreault LE. (eds) Medical Informatics: Computer Applications in Health Care and Biomedicine. New York: Springer-Verlag, 2000.

2
Fundamental Theorem of Medical Informatics
An intelligent practitioner working in combination with information resources/technology is “better” than the practitioner without such support.
Creating an environment of “supported practice”
Adapted from Hersh WR. Health/Medical/Biomedical Informatics: A general Introduction. 2003
Clinical informaticsapplications
Can classify by the type of information they usePatient-specific
The core application: the electronic medical recordAnother application: telemedicine
Knowledge-based Information retrieval systems
Combining the twoDecision-support systems
Decision Support System: Antibiotics Prescription Management
Patient Information: Coded Data• Culture results• Sensitivity• Ampicillin
Knowledge base: Decision Logic
•Machine-readable•Explicit & Detail•Update
DefinitionsClinical decision support system
Any computer program designed to help health professionals make clinical decisions
Tools for information management: information retrieval Tools for focusing attention: alerts, remindersTools for providing patient-specific recommendations: diagnostic system
Warner HR. et al(1997). Knowledge engineering in Health Informatics. Springer. 1997
Expert system A model of decision processTo represent, in an approximate form that is executable by a computer, the logical processes employed by an expert in a particular subject area to decide among 2 or more alternative conclusions
Munsen MA. et al. Chapter 16. Clinical decision-support systems. In Medical Informatics: Computer Applications in Health Care and Biomedicine. New York: Springer-Verlag, 2000.
Classical Expert System
InferenceEngine
InferenceEngine
KnowledgeBase
KnowledgeBase
DataData DecisionsDecisions
A computer program that, given case description, uses the information in the KB to generate new information about the case
Collection of encoded knowledge required to solve problems
Users Users
Warner HR. et al(1997). Knowledge engineering in Health Informatics. Springer
Domain experts
Knowledge Engineer
Fundamental problems in designing medical expert system
Knowledge acquisitionHow to translate human knowledge (e.g. textbook, journal, clinical database etc) into abstract representations in a computer
Knowledge representationHow to represent human knowledge in terms of data structures that can be processed by a computer
Inference generation How to use the abstract data structures to generate useful information in the context of a specific case
3
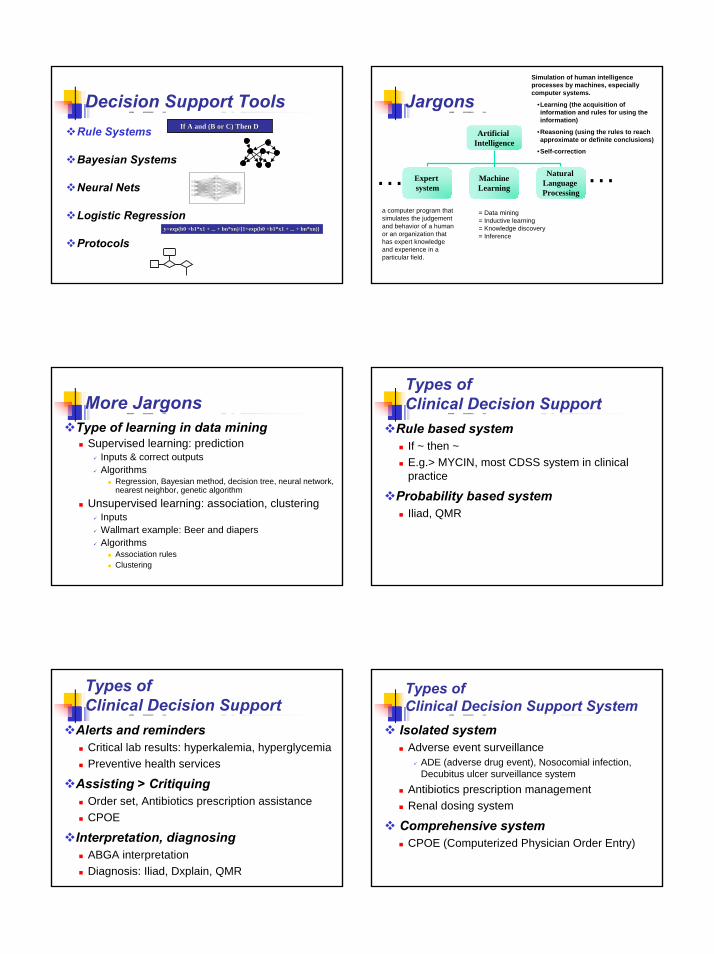
Decision Support ToolsRule Systems
Bayesian Systems
Neural Nets
Logistic Regression
Protocols
If A and (B or C) Then DIf A and (B or C) Then D
y=exp(b0 +b1*x1 + ... + y=exp(b0 +b1*x1 + ... + bnbn*xn)/{1+exp(b0 +b1*x1 + ... + *xn)/{1+exp(b0 +b1*x1 + ... + bnbn**xnxn)})}
Simulation of human intelligence processes by machines, especially computer systems.
•Learning (the acquisition of information and rules for using the information)
•Reasoning (using the rules to reach approximate or definite conclusions)
•Self-correction
Jargons Artificial
Intelligence
Expert system
MachineLearning
Natural Language Processing
= Data mining = Inductive learning= Knowledge discovery= Inference
a computer program that simulates the judgementand behavior of a human or an organization that has expert knowledge and experience in a particular field.
……
More Jargons Type of learning in data mining
Supervised learning: predictionInputs & correct outputsAlgorithms
Regression, Bayesian method, decision tree, neural network, nearest neighbor, genetic algorithm
Unsupervised learning: association, clusteringInputs Wallmart example: Beer and diapers Algorithms
Association rules Clustering
Types of Clinical Decision Support
Rule based system If ~ then ~E.g.> MYCIN, most CDSS system in clinical practice
Probability based systemIliad, QMR
Types of Clinical Decision Support
Alerts and remindersCritical lab results: hyperkalemia, hyperglycemiaPreventive health services
Assisting > CritiquingOrder set, Antibiotics prescription assistanceCPOE
Interpretation, diagnosingABGA interpretationDiagnosis: Iliad, Dxplain, QMR
Types of Clinical Decision Support System
Isolated system Adverse event surveillance
ADE (adverse drug event), Nosocomial infection, Decubitus ulcer surveillance system
Antibiotics prescription management Renal dosing system
Comprehensive system CPOE (Computerized Physician Order Entry)

4
Architecture of Clinical Decision Support System
Alert/Reminder
Clinical Workstation
BeeperFaxE-mailDatabase
Trigger
Rules Engine
Common Data Repository
Gather data
Event Monitor
• Select patient • Record
observation • Enter order
Access to KnowledgebaseCustomized & Organized information
Baorto DM et al.An "Infobutton" for Enabling Patients to Interpret On-line Pap Smear Reports.
Display of abnormal lab values with customizable threshold
CLAS (critical laboratory alerting system)
Goal Notify as rapidly as possible health-care personnel of laboratory values
System descriptionAlert logic: 11 alerting conditions (high/low/falling) developed by a medical panelAlerts were generated when test results transferred form the lab to the EMRAlerts were sent to health care personnel via pager, EMR, or fax
Evaluation (before and after)Appropriate treatment for alerting condition: 68.1% 83.8%Time spent in life threatening condition: 30.4hrs 15.7hrs
CLAS (critical laboratory alerting system)
Goal Notify as rapidly as possible health-care personnel of laboratory values
System descriptionAlert logic: 11 alerting conditions (high/low/falling) developed by a medical panelAlerts were generated when test results transferred form the lab to the EMR
Evaluation (before and after)Appropriate treatment for alerting condition: 68.1% 83.8%Time spent in life threatening condition: 30.4hrs 15.7hrs
Alerting Criteria for CLASData Used: Laboratory Results, Blood Gases
Alerting Condition Criteria
Hyponatremia (NAL) Na+ < 120 mEq/l
Falling Sodium (NAF) Na+ fallen 15+ mEq/l in 24 hr. and Na + < 130 mEq/l
Hypernatremia (NAH) Na+ > 155 mEq/l
Hypokalemia (KL) K+ < 2.7 mEq/l
Falling Potassium (KLF) K+ fallen 1+ mEq/l in 24 hr. and K + < 3.2 mEq/l
Hypokalemia, patient on digoxin
(KLD)
K+ < 3.3 mEq/l and patient on digoxin
Hyperkalemia (KH) K+ > 6.0 mEq/l
Metabolic acidosis (CO 2L) CO2 < 15 and BUN < 50 or CO 2 < 18 and BUN < 50 or CO 2 < 18 (BUN unknown) or CO 2 fallen 10+ in 24 hr. and CO 2 < 25
Hypoglycemia (GL) Glucose < 45 mg%
Hyperglycemia (GH) Glucose > 500 mg%
5
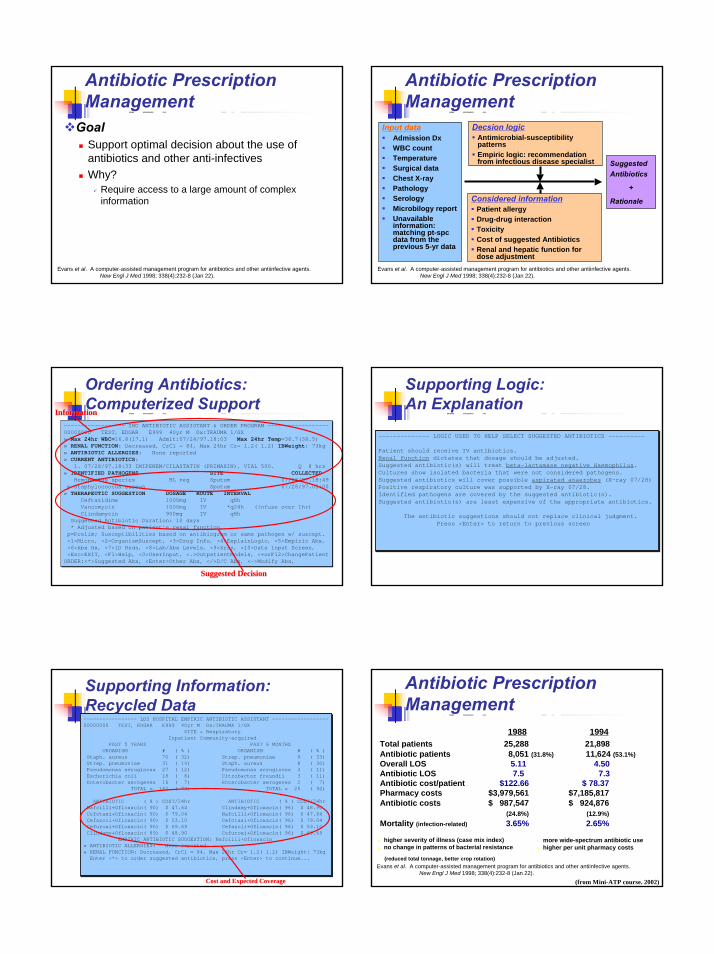
Antibiotic Prescription Management
Evans et al. A computer-assisted management program for antibiotics and other antiinfective agents.New Engl J Med 1998; 338(4):232-8 (Jan 22).
GoalSupport optimal decision about the use of antibiotics and other anti-infectivesWhy?
Require access to a large amount of complex information
Antibiotic Prescription Management
Input dataAdmission DxWBC countTemperatureSurgical dataChest X-rayPathologySerologyMicrobilogy reportUnavailable information: matching pt-spcdata from the previous 5-yr data
Evans et al. A computer-assisted management program for antibiotics and other antiinfective agents.New Engl J Med 1998; 338(4):232-8 (Jan 22).
Suggested Antibiotics
+
Rationale
Decsion logicAntimicrobial-susceptibility patternsEmpiric logic: recommendation from infectious disease specialist
Considered informationPatient allergyDrug-drug interactionToxicityCost of suggested AntibioticsRenal and hepatic function for dose adjustment
------------------ IHC ANTIBIOTIC ASSISTANT & ORDER PROGRAM ------------------00000000 TEST, EDGAR E999 40yr M Dx:TRAUMA 1/GX » Max 24hr WBC=16.8(17.1) Admit:07/24/97.18:03 Max 24hr Temp=38.7(38.5) » RENAL FUNCTION: Decreased, CrCl = 84, Max 24hr Cr= 1.2( 1.2) IBWeight: 73kg» ANTIBIOTIC ALLERGIES: None reported » CURRENT ANTIBIOTICS:
1. 07/28/97.18:33 IMIPENEM/CILASTATIN (PRIMAXIN), VIAL 500. Q 8 hrs » IDENTIFIED PATHOGENS SITE COLLECTED
Hemophilus species BL neg Sputum 07/28/97.18:49p Staphylococcus aureus Sputum 07/28/97.05:00
» THERAPEUTIC SUGGESTION DOSAGE ROUTE INTERVALCeftazidime 1000mg IV q8h Vancomycin 1000mg IV *q24h (infuse over 1hr) Clindamycin 900mg IV q8h
Suggested Antibiotic Duration: 10 days * Adjusted based on patient's renal function.
p=Prelim; Susceptibilities based on antibiogram or same pathogen w/ suscept. <1>Micro, <2>OrganismSuscept, <3>Drug Info, <4>ExplainLogic, <5>Empiric Abx, <6>Abx Hx, <7>ID Rnds, <8>Lab/Abx Levels, <9>Xray, <10>Data Input Screen, <Esc>EXIT, <F1>Help, <0>UserInput, <.>OutpatientModels, <+orF12>ChangePatient
ORDER:<*>Suggested Abx, <Enter>Other Abx, </>D/C Abx, <->Modify Abx,
------------------ IHC ANTIBIOTIC ASSISTANT & ORDER PROGRAM ------------------00000000 TEST, EDGAR E999 40yr M Dx:TRAUMA 1/GX » Max 24hr WBC=16.8(17.1) Admit:07/24/97.18:03 Max 24hr Temp=38.7(38.5) » RENAL FUNCTION: Decreased, CrCl = 84, Max 24hr Cr= 1.2( 1.2) IBWeight: 73kg» ANTIBIOTIC ALLERGIES: None reported » CURRENT ANTIBIOTICS:
1. 07/28/97.18:33 IMIPENEM/CILASTATIN (PRIMAXIN), VIAL 500. Q 8 hrs » IDENTIFIED PATHOGENS SITE COLLECTED
Hemophilus species BL neg Sputum 07/28/97.18:49p Staphylococcus aureus Sputum 07/28/97.05:00
» THERAPEUTIC SUGGESTION DOSAGE ROUTE INTERVALCeftazidime 1000mg IV q8h Vancomycin 1000mg IV *q24h (infuse over 1hr) Clindamycin 900mg IV q8h
Suggested Antibiotic Duration: 10 days * Adjusted based on patient's renal function.
p=Prelim; Susceptibilities based on antibiogram or same pathogen w/ suscept. <1>Micro, <2>OrganismSuscept, <3>Drug Info, <4>ExplainLogic, <5>Empiric Abx, <6>Abx Hx, <7>ID Rnds, <8>Lab/Abx Levels, <9>Xray, <10>Data Input Screen, <Esc>EXIT, <F1>Help, <0>UserInput, <.>OutpatientModels, <+orF12>ChangePatient
ORDER:<*>Suggested Abx, <Enter>Other Abx, </>D/C Abx, <->Modify Abx,
InformationInformation
Suggested DecisionSuggested Decision
Ordering Antibiotics: Computerized Support
-------------- LOGIC USED TO HELP SELECT SUGGESTED ANTIBIOTICS ----------
Patient should receive IV antibiotics. Renal function dictates that dosage should be adjusted. Suggested antibiotic(s) will treat beta-lactamase negative Haemophilus. Cultures show isolated bacteria that were not considered pathogens. Suggested antibiotics will cover possible aspirated anaerobes (X-ray 07/28) Positive respiratory culture was supported by X-ray 07/28. Identified pathogens are covered by the suggested antibiotic(s).Suggested antibiotic(s) are least expensive of the appropriate antibiotics.
The antibiotic suggestions should not replace clinical judgment. Press <Enter> to return to previous screen
-------------- LOGIC USED TO HELP SELECT SUGGESTED ANTIBIOTICS ----------
Patient should receive IV antibiotics. Renal function dictates that dosage should be adjusted. Suggested antibiotic(s) will treat beta-lactamase negative Haemophilus. Cultures show isolated bacteria that were not considered pathogens. Suggested antibiotics will cover possible aspirated anaerobes (X-ray 07/28) Positive respiratory culture was supported by X-ray 07/28. Identified pathogens are covered by the suggested antibiotic(s).Suggested antibiotic(s) are least expensive of the appropriate antibiotics.
The antibiotic suggestions should not replace clinical judgment. Press <Enter> to return to previous screen
Supporting Logic: An Explanation
----------------- LDS HOSPITAL EMPIRIC ANTIBIOTIC ASSISTANT ------------------00000000 TEST, EDGAR E999 40yr M Dx:TRAUMA 1/GX
SITE = Respiratory Inpatient Community-acquired
PAST 5 YEARS PAST 6 MONTHS ORGANISM # ( % ) ORGANISM # ( % )
Staph. aureus 70 ( 32) Strep. pneumoniae 9 ( 33) Strep. pneumoniae 31 ( 14) Staph. aureus 8 ( 30) Pseudomonas aeruginosa 27 ( 12) Pseudomonas aeruginosa 3 ( 11) Escherichia coli 18 ( 8) Citrobacter freundii 3 ( 11) Enterobacter aerogenes 16 ( 7) Enterobacter aerogenes 2 ( 7)
TOTAL = 162 ( 73) TOTAL = 25 ( 92)
ANTIBIOTIC ( % ) COST/24hr ANTIBIOTIC ( % ) COST/24hr Nafcilli+Ofloxacin( 90) $ 47.64 Clindamy+Ofloxacin( 96) $ 48.90 Cefotaxi+Ofloxacin( 90) $ 79.04 Nafcilli+Ofloxacin( 96) $ 47.64 Cefazoli+Ofloxacin( 90) $ 53.10 Cefotaxi+Ofloxacin( 96) $ 79.04 Cefuroxi+Ofloxacin( 90) $ 69.69 Cefazoli+Ofloxacin( 96) $ 53.10 Clindamy+Ofloxacin( 89) $ 48.90 Cefuroxi+Ofloxacin( 96) $ 69.69
EMPIRIC ANTIBIOTIC SUGGESTION: Nafcilli+Ofloxacin» ANTIBIOTIC ALLERGIES: None reported » RENAL FUNCTION: Decreased, CrCl = 84, Max 24hr Cr= 1.2( 1.2) IBWeight: 73kgEnter <*> to order suggested antibiotics, press <Enter> to continue...
----------------- LDS HOSPITAL EMPIRIC ANTIBIOTIC ASSISTANT ------------------00000000 TEST, EDGAR E999 40yr M Dx:TRAUMA 1/GX
SITE = Respiratory Inpatient Community-acquired
PAST 5 YEARS PAST 6 MONTHS ORGANISM # ( % ) ORGANISM # ( % )
Staph. aureus 70 ( 32) Strep. pneumoniae 9 ( 33) Strep. pneumoniae 31 ( 14) Staph. aureus 8 ( 30) Pseudomonas aeruginosa 27 ( 12) Pseudomonas aeruginosa 3 ( 11) Escherichia coli 18 ( 8) Citrobacter freundii 3 ( 11) Enterobacter aerogenes 16 ( 7) Enterobacter aerogenes 2 ( 7)
TOTAL = 162 ( 73) TOTAL = 25 ( 92)
ANTIBIOTIC ( % ) COST/24hr ANTIBIOTIC ( % ) COST/24hr Nafcilli+Ofloxacin( 90) $ 47.64 Clindamy+Ofloxacin( 96) $ 48.90 Cefotaxi+Ofloxacin( 90) $ 79.04 Nafcilli+Ofloxacin( 96) $ 47.64 Cefazoli+Ofloxacin( 90) $ 53.10 Cefotaxi+Ofloxacin( 96) $ 79.04 Cefuroxi+Ofloxacin( 90) $ 69.69 Cefazoli+Ofloxacin( 96) $ 53.10 Clindamy+Ofloxacin( 89) $ 48.90 Cefuroxi+Ofloxacin( 96) $ 69.69
EMPIRIC ANTIBIOTIC SUGGESTION: Nafcilli+Ofloxacin» ANTIBIOTIC ALLERGIES: None reported » RENAL FUNCTION: Decreased, CrCl = 84, Max 24hr Cr= 1.2( 1.2) IBWeight: 73kgEnter <*> to order suggested antibiotics, press <Enter> to continue...
Cost and Expected CoverageCost and Expected Coverage
Supporting Information: Recycled Data
Antibiotic Prescription Management
Evans et al. A computer-assisted management program for antibiotics and other antiinfective agents.New Engl J Med 1998; 338(4):232-8 (Jan 22).
1988 1994
higher severity of illness (case mix index)no change in patterns of bacterial resistance
more wide-spectrum antibiotic usehigher per unit pharmacy costs
(reduced total tonnage, better crop rotation)
Total patients 25,288 21,898Antibiotic patients 8,051 (31.8%) 11,624 (53.1%)Overall LOS 5.11 4.50Antibiotic LOS 7.5 7.3Antibiotic cost/patient $122.66 $ 78.37Pharmacy costs $3,979,561 $7,185,817Antibiotic costs $ 987,547 $ 924,876
(24.8%) (12.9%)Mortality (infection-related) 3.65% 2.65%
(from Mini-ATP course. 2002)
6
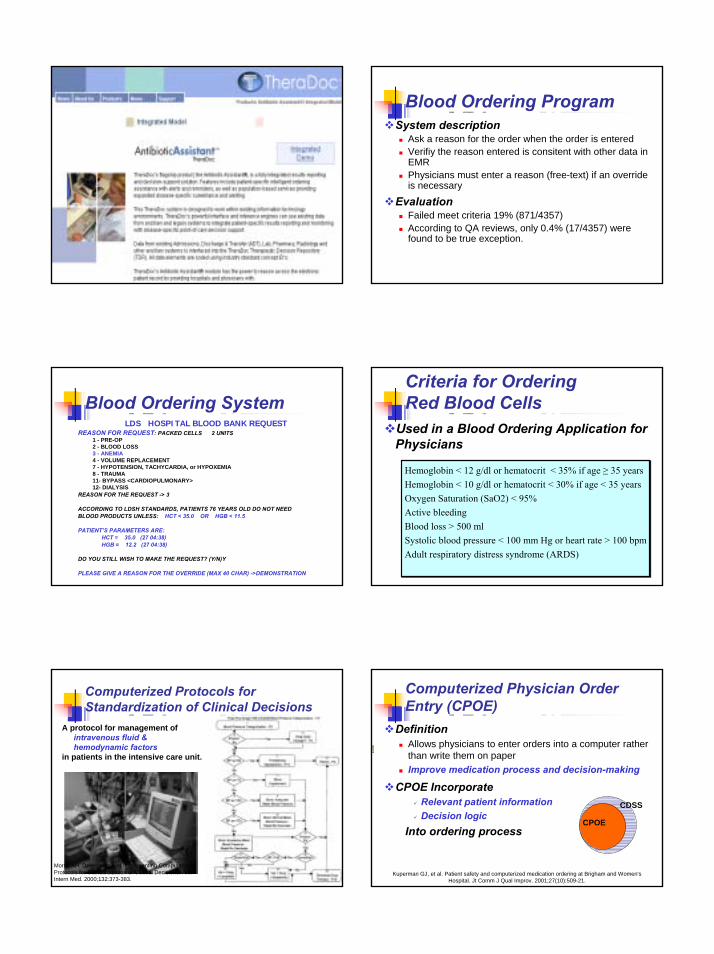
Blood Ordering ProgramSystem description
Ask a reason for the order when the order is enteredVerifiy the reason entered is consitent with other data in EMRPhysicians must enter a reason (free-text) if an override is necessary
EvaluationFailed meet criteria 19% (871/4357) According to QA reviews, only 0.4% (17/4357) were found to be true exception.
Blood Ordering SystemLDS HOSPITAL BLOOD BANK REQUEST
REASON FOR REQUEST: PACKED CELLS 2 UNITS1 - PRE-OP2 - BLOOD LOSS3 - ANEMIA4 - VOLUME REPLACEMENT7 - HYPOTENSION, TACHYCARDIA, or HYPOXEMIA8 - TRAUMA11- BYPASS <CARDIOPULMONARY>12- DIALYSIS
REASON FOR THE REQUEST -> 3
ACCORDING TO LDSH STANDARDS, PATIENTS 76 YEARS OLD DO NOT NEEDBLOOD PRODUCTS UNLESS: HCT < 35.0 OR HGB < 11.5
PATIENT’S PARAMETERS ARE:HCT = 35.0 (27 04:38)HGB = 12.2 (27 04:38)
DO YOU STILL WISH TO MAKE THE REQUEST? (Y/N)Y
PLEASE GIVE A REASON FOR THE OVERRIDE (MAX 40 CHAR) ->DEMONSTRATION
Criteria for Ordering Red Blood Cells
Used in a Blood Ordering Application for Physicians
Hemoglobin < 12 g/dl or hematocrit < 35% if age ≥ 35 yearsHemoglobin < 10 g/dl or hematocrit < 30% if age < 35 yearsOxygen Saturation (SaO2) < 95%Active bleedingBlood loss > 500 mlSystolic blood pressure < 100 mm Hg or heart rate > 100 bpmAdult respiratory distress syndrome (ARDS)
Hemoglobin < 12 g/dl or hematocrit < 35% if age ≥ 35 yearsHemoglobin < 10 g/dl or hematocrit < 30% if age < 35 yearsOxygen Saturation (SaO2) < 95%Active bleedingBlood loss > 500 mlSystolic blood pressure < 100 mm Hg or heart rate > 100 bpmAdult respiratory distress syndrome (ARDS)
Computerized Protocols forStandardization of Clinical Decisions
Morris AH. Developing and Implementing Computerized Protocols for Standardization of Clinical Decisions. Ann Intern Med. 2000;132:373-383.
A protocol for management of intravenous fluid & hemodynamic factors
in patients in the intensive care unit.
Computerized Physician Order Entry (CPOE)
DefinitionAllows physicians to enter orders into a computer rather than write them on paperImprove medication process and decision-making
CPOE Incorporate Relevant patient information Decision logic
Into ordering process
Kuperman GJ, et al. Patient safety and computerized medication ordering at Brigham and Women's Hospital. Jt Comm J Qual Improv. 2001;27(10):509-21.
CDSS
CPOE

7
CPOE Application Features Structured Orders: Dose List
Structured Orders: Dose Frequency List
Screen Display of Brigham Integrated Computing System's Renal Dosing
Chertow GM, Lee J, Kuperman GJ, et al. Guided medication dosing for inpatients with renal insufficiency. JAMA 2001;286:2839-2844.
Drug Allergy CheckingAlert review and therapeutic action screen
Kuperman GJ, et al. Improving response to critical laboratory results with automation: results of a randomized controlled trial. J Am Med Inform Assoc 1999;6:512-522

8
Drug Knowledgebase
Computerized ADE Surveillance System
Incidence of ADE19% of medical errors (Harvard Medical Practice Study)
2~5 ADEs per 100 admissions
Not recognized by clinician: ~80%
Kohn et al. To err is human: building a safer health system. Washington, DC. National Academy Press, 1999.
Leape et al. The nature of adverse events in hospitalized patients. Results of the Harvard Medical Practice Study II. NEJM 1991; 324:377-84.
Voluntary Reporting vs. Computerized ADE Surveillance
Evans RS et al. Development of a computerized adverse drug event monitor. Proc Annu Symp Comput Appl Med Care. 1991;:23-7.
9
401
0
100
200
300
400
500
Voluntary Reporting Computerized ADEsurveillance
Logic of Computerized ADE Surveillance
Knowledge-based As an antidote, vitamin K is given when a patient has bleeding tendency due to warfarinmedication
Patient-specificE.g> Vitamin K order stored in EMR
Computerized ADE surveillance: Combining the two
E.g> Vitamin K order can be used as a signal to detect ADEs
Computerized ADE Surveillance System (CSS)
ADE surveillance system
Independent Verificationby Clinical Pharmacist or Trained Nurse
Pharm-acyData
LabData
ClinicalDocumen-
tation
Create Daily
Report(8 am)
Pt. nameDiagnosisADE signalDrugs given
DataSources
ADEAlert
Generate ADE alerts
Trigger Condition
Met
Verified ADEDB
StoreInformation
Inform Clinician

9
ADE Signals: Core of CSSImproving PPV ADE Signals:Rules Behind Signals
12.5
46.0
0
20
40
60
Vitamin K Vitamin K +Warfarin
PositivePredictive Value
Computerized ADE Surveillance System (CSS)
ADE surveillance system
Independent Verificationby Clinical Pharmacist or Trained Nurse
Pharm-acyData
LabData
ClinicalDocumen-
tation
Create Daily
Report(8 am)
Pt. nameDiagnosisADE signalDrugs given
DataSources
ADEAlert
Generate ADE alerts
Trigger Condition
Met
Verified ADEDB
StoreInformation
Inform Clinician
ADE Verification: Review & Data Collection
Review methodsReviewing the chartTalking with the clinicians caring for the patient Interviewing the patient, when possible
Causality AssessmentNaranjo Score
SeverityRelevant data for verified ADEs
Type of ADEDrug causing ADEADE signalOthers: diagnosis, number of drugs given, ADE symptom, Time of ADE first noticed
Gold Standard for ADE Detection?:Chart Review vs. Computerized ADE Surveillance
ADE surveillance methods
Voluntary reportingChart reviewComputerized ADE Surveillance system
Detect more severe ADEs than chart review (51% vs. 42%)
Computer-assisted
Pharmacist-verified
ADE45%
Chart Review65%
12%
Jha AK, et al. Identifying ADE: development of a computer-based monitor and comparison with chart review and stimulated voluntary report. JAMIA. 1999;5(3):305-14
Voluntary Reporting4%
1%
Computerized Surveillance System:Gold Standard for ADE Detection?Senario(1)
Hives to radio-contrast dye were developed and fixed with Benadryl.The CSS was particularly good at identifying events associated with quantitative changes.
Senario(2)Patient became drowsy due to Benzodiazepine, and it was resolved when Benzodiazepine was discontinued.Chart review was better at identifying events associated only with symptoms.
There is no single “Gold Standard” in ADE detection.
10
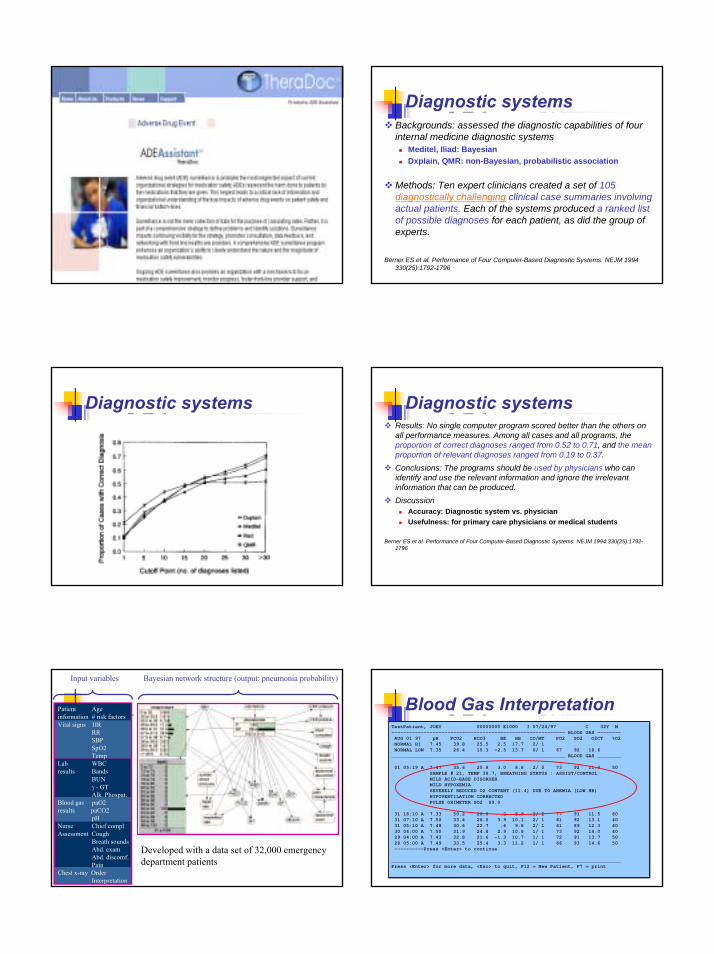
Diagnostic systemsBackgrounds: assessed the diagnostic capabilities of four internal medicine diagnostic systems
Meditel, Iliad: BayesianDxplain, QMR: non-Bayesian, probabilistic association
Methods: Ten expert clinicians created a set of 105 diagnostically challenging clinical case summaries involving actual patients. Each of the systems produced a ranked list of possible diagnoses for each patient, as did the group of experts.
Berner ES et al. Performance of Four Computer-Based Diagnostic Systems. NEJM 1994 330(25):1792-1796
Diagnostic systems Diagnostic systemsResults: No single computer program scored better than the others on all performance measures. Among all cases and all programs, the proportion of correct diagnoses ranged from 0.52 to 0.71, and the mean proportion of relevant diagnoses ranged from 0.19 to 0.37. Conclusions: The programs should be used by physicians who can identify and use the relevant information and ignore the irrelevant information that can be produced. Discussion
Accuracy: Diagnostic system vs. physicianUsefulness: for primary care physicians or medical students
Berner ES et al. Performance of Four Computer-Based Diagnostic Systems. NEJM 1994 330(25):1792-1796
Patient Ageinformation # risk factorsVital signs HR
RRSBPSpO2Temp
Lab WBCresults Bands
BUN γ - GTAlk. Phospat.
Blood gas paO2results paCO2
pH Nurse Chief complAssessment Cough
Breath soundsAbd. examAbd. discomf.Pain
Chest x-ray OrderInterpretation
Input variables Bayesian network structure (output: pneumonia probability)
Developed with a data set of 32,000 emergency department patients
TestPatient, JOEY 00000000 E1000 I 07/24/97 C 32Y M----------------------------------------------------------- BLOOD GAS --------AUG 01 97 pH PCO2 HCO3 BE HB CO/MT PO2 SO2 O2CT %O2NORMAL HI 7.45 39.8 25.5 2.5 17.7 2/ 1 NORMAL LOW 7.35 26.4 15.3 -2.5 13.7 0/ 1 67 92 18.6
___________________________________________________________ BLOOD GAS ________
01 05:19 A 7.47 35.6 25.8 3.0 8.8 2/ 0 73 92 11.4 50 SAMPLE # 21, TEMP 38.7, BREATHING STATUS : ASSIST/CONTROL MILD ACID-BASE DISORDER MILD HYPOXEMIA SEVERELY REDUCED O2 CONTENT (11.4) DUE TO ANEMIA (LOW HB) HYPOVENTILATION CORRECTED PULSE OXIMETER SO2 89.0
31 18:10 A 7.33 50.2 26.0 .2 8.9 2/ 2 77 91 11.5 60 31 07:10 A 7.50 33.4 26.0 3.9 10.1 2/ 1 61 92 13.1 40 31 05:10 A 7.48 30.6 22.7 .6 9.8 2/ 1 61 89 12.3 40 30 04:00 A 7.50 31.9 24.8 2.9 10.8 1/ 1 73 92 14.0 40 29 04:00 A 7.43 32.8 21.6 -1.3 10.7 1/ 1 72 91 13.7 50 28 05:00 A 7.49 33.5 25.4 3.3 11.2 1/ 1 66 93 14.6 50 ----------Press <Enter> to continue
______________________________________________________________________________Press <Enter> for more data, <Esc> to quit, F12 = New Patient, F7 = print
TestPatient, JOEY 00000000 E1000 I 07/24/97 C 32Y M----------------------------------------------------------- BLOOD GAS --------AUG 01 97 pH PCO2 HCO3 BE HB CO/MT PO2 SO2 O2CT %O2NORMAL HI 7.45 39.8 25.5 2.5 17.7 2/ 1 NORMAL LOW 7.35 26.4 15.3 -2.5 13.7 0/ 1 67 92 18.6
___________________________________________________________ BLOOD GAS ________
01 05:19 A 7.47 35.6 25.8 3.0 8.8 2/ 0 73 92 11.4 50 SAMPLE # 21, TEMP 38.7, BREATHING STATUS : ASSIST/CONTROL MILD ACID-BASE DISORDER MILD HYPOXEMIA SEVERELY REDUCED O2 CONTENT (11.4) DUE TO ANEMIA (LOW HB) HYPOVENTILATION CORRECTED PULSE OXIMETER SO2 89.0
31 18:10 A 7.33 50.2 26.0 .2 8.9 2/ 2 77 91 11.5 60 31 07:10 A 7.50 33.4 26.0 3.9 10.1 2/ 1 61 92 13.1 40 31 05:10 A 7.48 30.6 22.7 .6 9.8 2/ 1 61 89 12.3 40 30 04:00 A 7.50 31.9 24.8 2.9 10.8 1/ 1 73 92 14.0 40 29 04:00 A 7.43 32.8 21.6 -1.3 10.7 1/ 1 72 91 13.7 50 28 05:00 A 7.49 33.5 25.4 3.3 11.2 1/ 1 66 93 14.6 50 ----------Press <Enter> to continue
______________________________________________________________________________Press <Enter> for more data, <Esc> to quit, F12 = New Patient, F7 = print
Blood Gas Interpretation
11
Problems limiting development and use of CDSS
Cost-benefit of CDSS system Accuracy and reliability of CDSSDevelopment time and cost Lack of large, reliable, clinical databases (especially containing sign & symptom)
Significant “physician resistance”Questions regarding usefulness and cost-effectivenessNatural resistance to change, general computer ignorance, lack of time necessary to interact with computerIncentive: financial, non-financial
Inherent complexity of medicinePoorly understood pathophysiological process Notoriously idiosyncratic Lack of objective gold standard
Decision support and Safety from Informatics Review
Martin Luther King Jr./Drew Medical Center Patient Monitors Shut Off Following 2 DeathsThe Medical Center is disconnecting a new $411,000 patient monitoring system whose alarms failed to alert nurses this summer that two patients needed urgent attention. The patients ultimately died. The system was set up so that a central station received information from wireless bedside monitors tracking the blood pressure, heart rate, blood oxygen level and temperature of up to 60 patients. Typically, nurses depended on audible alarms to alert them of patients in distress. In its investigation of the first incident, the monitoring system's maker, Welch Allyn Inc., found that the alarm at the central station failed to sound because the incorrect identification code had been entered on the patient making it appear that another patient's vital signs were hers. In the second incident, the central alarm may not have sounded because of damage to the main console, a Welch Allyn spokesman said. The company says that damage occurred after installation.
Hospital computer crash a lesson to the industry (Boston Globe, 11/19/2002)
Beth Israel Deaconess Medical Center's computer system crashed repeatedly over 31/2 days last week, periodically blocking access to patient records, prescriptions, laboratory reports, and other information, and forcing the hospital to revert to the paper-based systems of what one executive called ''the hospital of the 1970s.'' Hospital and public health officials are calling the incident a wake-up call for hospitals across the country, whose computer systems may not be able to keep up with their growing workload. At Beth Israel, the systems handle 40 terabytes of information daily - or 40 times the information in the Library of Congress.Although computer systems have allowed hospitals to work with more speed and flexibility, executives said, last week's events showed how frightening it can be when they fail.The crisis began when a researcher installed software to analyze data, and a large amount of information started flowing over the network. Doctors noticed intermittent problems with e-mail and data entry. But at 4 p.m. on Wednesday, most of the the systems - from e-mail to accessing patient records to entering laboratory data - slowed or stopped and stayed down for two hours.The emergency room shut down for most of Friday, and the hospital decided to refuse all transfers except in life-threatening emergencies. Some lab tests that normally took 45 minutes to complete took closer to two hours, so doctors reverted to lower-tech methods of diagnosis. All hospitals were required to put in disaster plans for Y2K. Beth Israel has such a plan in place, but because systems evolve so quickly, it was already outdated.
Two ApproachesSoftware Oversight Committee (SOC)
To make sure there is ongoing monitoring to detect adverse events, address them, and to insure that the overall system performs as designed
(Miller RA, Gardener RM. Summary recommendations for responsible monitoring and regulation of clinical software committee. Ann Intern Med 1997 127:842-845)
FDA regulation1976 medical device act1995 FDA regulates blood bank software2002 General principle of software validation
Policy Issues: Barriers, Incentive & Mandate
Important barriersCost of EMR vs. Demonstrated benefits Attitude of clinical leaders on EMR
Payment system and dissemination of EMRCPOE: who pays and who harvests? Result of CBA
Fee-for-service << Case payment (DRG) << Capitation (HMO)
Incentives Federal government
External funding for the investment in acquiring an EMRCMS (Center for Medicare &Medicaid)
Quality and payment rate LeapFrog Group
Proposes an incentive bonus for providers having and using CPOE in hospital
California’s legislative mandateTo Implement CPOE system for urban hospitals by 2005
Leapfrog survey finds limited use of CPOE in U.S. hospitals January 18, 2002
The Leapfrog Group yesterday released the results of a survey, conducted last spring, that assessed hospitals’ use of computerized physician order entry (CPOE) and two other patient-safety practices considered important by the organization. Of 241 hospitals that answered the survey, just 3.3% reported that they had CPOE systems in place. Nearly 30%, however, said they planned to implement CPOE systems by 2004.
The survey also asked whether hospitals staffed their intensive care units with trained intensivists and whether they used evidence-based hospital referrals for certain high-risk surgeries and neonatal conditions. The survey was offered to more than 500 hospitals in Atlanta, California, East Tennessee, Minnesota, Seattle-Tacoma-Everett, and St. Louis. Complete results of the survey are available on the Leapfrog Group’s Web site (NewsRounds/Reuters, 1/18).
The Leapfrog Group is a coalition of 96 large health care purchasers that aims to reduce medical errors and health care costs by steering its members’ employees to hospitals that implement the three patient safety practices. The group plans to extend the survey to an additional 1,000 hospitals this year (Martinez, Wall Street Journal, 1/17).

12
"배합 금기 약품" 점검 시스템 도입(2003년 9월25일)
(서울=연합뉴스) 건강보험심사평가원은 함께 투약할 경우 심각한 부작용이 나타나 배합해서는 안 되는 의약품을 자동 점검할 수 있는 시스템을빠르면 올 연말 도입할 계획이라고 25일 밝혔다. 이 시스템이 도입되면 함께 투약되는 것이 금기된 약물이 처방될 경우 심평원 시스템에서 자동 점검돼 약국에 조제료와 투약비가 지급되지 않게되며, 의사가 처방전을 발행할 때도 경고 메시시가 나타나게 된다. 심평원이 숙명여대 의약정보연구소에 연구를 의뢰해 미국의 약물사용평가 기준을 적용, 지난해 9월 1~15일 서울과 수원에서 청구된 3천200만건의 의약품을 조사한 결과 4.87%(156만건)가 용법, 용량 기준을 벗어났으며 이 가운데 배합 금기 약품은 0.02%(5천583건)였다. 조사대상 의약품 가운데 식품의약품안전청의 성인 용량 기준을 벗어난 경우는6.59%(211만건)였다. 심각한 부작용 사례로는 항히스타민제 `테페나딘'과 항진균제 `케도코나졸'을 함께 투여한 39세 여성에게서 심근경색, 심장부정맥 등의 심장 독성이 나타났다는 보고가 있었다.
Decision Support Standards: Arden Syntax
Arden Syntax-RationaleArose from the need to make medical knowledge available for decision making at the point-of-care
Make knowledgeMake knowledge explicit
Allow knowledge sharing within and between institutionsStandardize the way medical knowledge is integrated into hospital information systemsInventors
Columbia Presbyterian RegenstriefLDS
Medical Logic ModuleA Medical Logic Module (MLM) is an independent unit in a health knowledge base.
Each MLM contains maintenance information, link to other sources of knowledge, and enough logic to make a single health decision
The MLM is an stream of text stored in and ASCII file in statements called slots.
Maintenance:Title: Simple MI Rule;;MLMname: simple_MI_rule;;Arden: ASTM-E1460-1995;;Version: 2.00;;Institution: LDS Hospital;;Author: Peter Haug M.D.;;Specialist: ;;Date: 2000-11-10;;Validation: Testing;; Library: ;;Purpose: Demonstrate a simple MLM;;Explanation: This MLM applies a simple rule to detect MI from a few data elements;;Keywords: MI, Myocardial Infarct;;Citations: ;;Links: ;;Knowledge:Type: data-driven;;Data: Let Chest_Pain be read {Chest Pain from the CDR} where Chest_Pain occurred within the last 1 day;Let ECG_Result be read {Value of ECG from the CDR} where ECG_Result occurred within the last 1 day;Let CK-MB be read {Last Last CK-MB from the CDR} where CK-MB occurred within the last 1 day;Let Troponin be read {Last Troponin from the CDR} where Troponin occurred within the last 1 day;;;Evoke: ;;Logic:
If Chest_Pain is present and (ECG_Result = Acute_MI or CK-MB is greater than 5% or Troponin is greater than 2)Then conclude true;;;Action:
Write “Acute MI is present”;;;End:
Simple MLM
Logic:
If Chest_Pain is present and (ECG_Result = Acute_MI or CK-MB is greater than 5% or Troponin is greater than 2)
Then conclude true;;;Action:
Write “Acute MI is present”;
Decision Support StandardsHL7 Standards
Arden Syntax
Guideline Interchange Format
InferenceEngine
InferenceEngine
KnowledgeBase
KnowledgeBase
Data Decisions
Maintenance: Title: Temperature under 38 for 24 hours;; MLMname: normal_temp_24_hr;; Arden: ASTM-E1460-1995;; Version: 2.00;; Institution: LDS Hospital;; Author: Peter Haug M.D.;; Specialist: ;; Date: 1998-11-20;; Validation: Testing;; Library: ;; Purpose:
Test the patients data to determine if the temperature has been less than 38 degrees for 24 hrs;;
Explanation: This MLM evaluates information in the database to determine if the patients temperature has been less than 38 degrees for 24 hours or more. At least two temperatures are required more than 4 hours apart. Called by discharge application at specific times;;
Keywords: Temperature, discharge;;
Citations: ;; Links: ;;
Knowledge: Type: data-driven;; Data:
Let temperature be read {all temperatures from the HELP system} where temperature occurred within the last 1 day;
;; Evoke: ;; Logic: ;; Action:
If COUNT of temperature is less than 2 Then
Write “Less than two temperatures in the last 24 hours”; ElseIf Time of Latest temperature – Time of Earliest temperature is less than 4 hours Then
Write “Temperatures gathered too close together.” ElseIf Any temperature greater than or equal to 38 Write “Elevated temperature in the last 24 hours” Else Write “Temperature less than 38 degrees for the last 24 hours; Endif; ;;
End:
GlifGlif
ArdenArden

13
MLM: Structure (Categories and Slots)
Maintenance categoryTitle, mlmname, version, institution, author, date, validation
Library categoryPurpose, explanation, keywords, citation, link
Knowledge categoryType, data, priority, evoke, logic, action, urgency
Knowledge: Data SlotPurpose
Terms in MLM must be mapped into a databaseUse of curly braces { } allows flexibility in mapping to the institution’s local database“Curly brace problem” also hinders sharing of knowledge
ExampleLast_creatinine:=read last {select “OBSER_VALUE” from “LCR” where qualifier in “creatinine”}
Knowledge: Logic slotIncludes
Set of medical criteriaEnd with a “conclude statement”Logical algorithm: If ~ then~conclude true;
ExampleIf last_creatinine is not present then
alert text:=“No recent creatinine available. consider ordering creatinine before giving IV contrast.”;
conclude true; else conclude false;endif;
Knowledge: Action slotFunctions
Carry out actions if logic slot concludes trueExamples of action
Write a message to screenStore a message in a fileCall another MLM
ExampleAction:
write “Last creatinine:” ||last_creat|| “on:” ||time of last_creatinine||
Appears as Last creatinine: 2.36 on: 2003-09-23T06:30:00
http://cslxinfmtcs.csmc.edu/hl7/arden/
Arden syntax sampleLibrary:
purpose:Warn the health care provider of hypokalemia in the setting of digoxin therapy.;;
explanation:Whenever a serum or whole blood potassium value is stored, it is checked for hypokalemia (less than 3.3). If hypokalemia is present, then if the patient has a non-zero serum digoxin level within the 3 months or an active order for digoxin administration, then an alert is generated (using the later of the level or the order). It warns that hypokalemia may potentiate digoxin arrhythmias. Repeat alerts are not generated if there has not been a new digoxin level or order since the last alert.;;
keywords: hypokalemia; digoxin; arrhythmia;;
citations: ;;
14
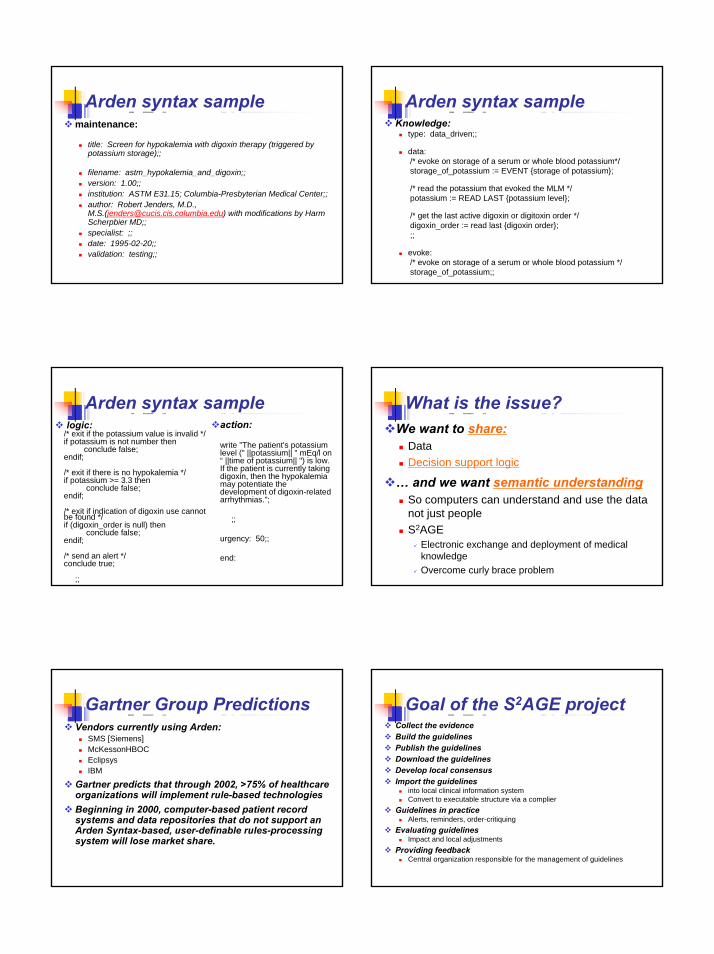
Arden syntax samplemaintenance:
title: Screen for hypokalemia with digoxin therapy (triggered by potassium storage);;
filename: astm_hypokalemia_and_digoxin;;version: 1.00;;institution: ASTM E31.15; Columbia-Presbyterian Medical Center;;author: Robert Jenders, M.D., M.S.([email protected]) with modifications by Harm Scherpbier MD;;specialist: ;;date: 1995-02-20;;validation: testing;;
Arden syntax sampleKnowledge:
type: data_driven;;
data:/* evoke on storage of a serum or whole blood potassium*/storage_of_potassium := EVENT {storage of potassium};
/* read the potassium that evoked the MLM */potassium := READ LAST {potassium level};
/* get the last active digoxin or digitoxin order */digoxin_order := read last {digoxin order};;;
evoke:/* evoke on storage of a serum or whole blood potassium */storage_of_potassium;;
Arden syntax samplelogic:
/* exit if the potassium value is invalid */if potassium is not number then
conclude false;endif;
/* exit if there is no hypokalemia */if potassium >= 3.3 then
conclude false;endif;
/* exit if indication of digoxin use cannot be found */if (digoxin_order is null) then
conclude false;endif;
/* send an alert */conclude true;
;;
action:
write "The patient's potassium level (" ||potassium|| " mEq/l on “ ||time of potassium|| ") is low. If the patient is currently taking digoxin, then the hypokalemiamay potentiate the development of digoxin-related arrhythmias.";
;;
urgency: 50;;
end:
What is the issue?We want to share:
DataDecision support logic
… and we want semantic understandingSo computers can understand and use the data not just peopleS2AGE
Electronic exchange and deployment of medical knowledgeOvercome curly brace problem
Gartner Group PredictionsVendors currently using Arden:
SMS [Siemens]McKessonHBOCEclipsysIBM
Gartner predicts that through 2002, >75% of healthcare organizations will implement rule-based technologiesBeginning in 2000, computer-based patient record systems and data repositories that do not support an Arden Syntax-based, user-definable rules-processing system will lose market share.
Goal of the S2AGE project Collect the evidenceBuild the guidelinesPublish the guidelines Download the guidelinesDevelop local consensusImport the guidelines
into local clinical information systemConvert to executable structure via a complier
Guidelines in practice Alerts, reminders, order-critiquing
Evaluating guidelines Impact and local adjustments
Providing feedbackCentral organization responsible for the management of guidelines

15
Selected Bibliography of CDSS: Reading AssignmentEvans RS, Pestotnik SL, Classen DC et al. A computer-assisted management program for antibiotics and other antiinfective agents. N Engl J Med 1998;338(4):232-238Johnston ME, Langton KB, Haynes RB, Mathieu A. Effects of computer-based clinical decision support systems on clinician performance and patient outcome. A critical appraisal of research. Ann Intern Med 1994;120:135-142.McDonald CJ, Overhage JM, Tierney WM, Abernathy GR, Dexter PR. The promise of computerized feedback systems for diabetes care. Ann Intern Med 1996;124(1 pt 2):170-174.Pestonik SL, Classen DC, Evans RS, Burke JP. Implementing antibiotic practice guidelines through computer-assisted decision support: clinical and financial outcomes. Ann Intern Med 1996;124:884-890.Rind DM, Safran C, Phillips RS, Wang Q, Calkins DR, Delbanco TL, Bleich HL, Slack WV. Effect of computer-based alerts on the treatment and outcomes of hospitalized patients. Arch Intern Med 1994;154:1511-1517.Shea S, DuMouchel W, Bahamonde L. A meta-analysis of 16 randomized controlled trials to evaluate computer-based clinical reminder systems for preventive care in the ambulatory setting. J Am Med Inform Assoc 1996;3(6):399-409.Shea S, Sideli RV, DuMouchel W, Pulver G, Arons RR, Clayton PD. Computer-generated informational messages directed to physicians: effect on length of hospital stay. J Am Med Informatics Assoc 1995;2:58-64.Somkin CP, Hiatt RA, Hurley LB, Gruskin E, Ackerson L, Larson P. The effect of patient and provider reminders on mammography and Papanicolaou smear screening in a large health maintenance organization. Arch Intern Med 1997;157:1658-1664.Weingarten SR, Riedinger MS, Conner L, Lee TH, Hoffman I, Johnson B, Ellrodt AG. Practice guidelines and reminders to reduce duration of hospital stay for patients with chest pain. An interventional trial. Ann Intern Med 1994;120:257-263.
Questions?





























