Embed Size (px)
Citation preview

J. clin; Path. (1961), 14, 552
Renal enlargement in chronic cor pulmonaleP. A. ELLIS
From the Department ofPathology, Newcastle General Hospital
SYNOPSIS Examination of the post-mortem records of 1,391 unselected cases showed that thecommonest condition associated with excessive diffuse enlargement of the kidneys was chroniccor pulmonale. A less striking enlargement was found in some cases of chronic rheumatic heartdisease.A hypothesis is put forward in which the renal enlargement is regarded as a work hypertrophy
brought about by the kidneys' efforts to compensate for a chronic respiratory acidosis.
Very little is to be found in the literature on thesubject of structural kidney changes in chronic corpulmonale. Black and Stanbury (1958) comment onthis lack of information and describe two patientswith cor pulmonale in both of whom the last illnesswas associated with renal failure. Simpson (1957)also described renal failure as occurring, along withliver damage, in patients suffering from severe anoxia.Anatomical changes were present in one of Blackand Stanbury's cases and were interpreted as beingthe earliest changes of tubular necrosis. Their othercase also showed some enlargement of the kidneyas a whole (combined weight 420 g.) and a smalltuberculous focus was present. Simpson states thatno anatomical lesions were present to account forthe renal failure associated with anoxia.The present investigations were undertaken as the
result of an impression gained while performingroutine post-mortem examinations that very largekidneys are often found in cases of chronic corpulmonale.
MATERIAL
The records of 1,391 necropsies were examined.This total was made up of all the necropsies per-formed at Newcastle General Hospital in 1956 and1957 (1,197) and 194 personal cases examined in1958 and 1959.Cases were admitted to the series when chronic
lung disease was present along with enlargement ofthe right ventricle. All those with left ventricularenlargement or valvular disease were excluded.
RESULTS
Thirty-seven cases satisfied these criteria and Fig. 1Received for publication 15 February 1961.
S
4
3
2
U,wU)
U
0cc
z
7.
6-
5.
A
I ILFfIB
KIDNEY WTS (9.)
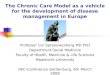
FIG. 1. A Histogram showing distribution of the com-bined weights of the kidneys in 37 cases of cor pulmonale;B In 42 cases with right ventricular hypertrophy fromcauses other than pulmonary disease (all rheumatic exceptfor one case of A.S.D.). Interval 25 grams.
shows the distribution of their combined kidneyweights. It will be seen that there were eight exceed-
552
. . . .
on July 28, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.14.5.552 on 1 S
eptember 1961. D
ownloaded from

Renal enlargement in chronic cor pulmonale
ing 500 g., the modal value being about 310 g. In therest of the 1,391 necropsies the kidney weighed morethan 500 g. in 28 cases and in 22 of these the enlarge-ment was due to purely local renal disease, includingpolycystic disease, pyogenic infections, solitarycysts, hypernephroma, secondary carcinoma, leuk-aemic infiltration, tubular necrosis, and amyloidosis.In the remaining six no acceptable local lesion waspresent. Of these, death was due to cardiac in-farction in four, to cerebral tumour in one, and tohead injury in one.
It is evident from these figures that enlargment ofthe kidneys to a combined weight of more than500 g. occurs more often in chronic cor pulmonalethan in any other condition, when purely local renaldisease is excluded.
chronic cardiac failure from other causes. Mitralstenosis was chosen for comparison because thiscondition commonly produces pure right ventricularhypertrophy associated with repeated episodes ofcongestive cardiac failure as does cor pulmonale.
In Fig. 3, 16 cases of pure mitral stenosis, all withenlargement of the right but with normal leftventricles, are similarly plotted. While there is somecorrelation between heart and kidney weight in Fig.3 it appears that cases of mitral stenosis with heartsof a given weight have smaller kidneys than cases ofcor pulmonale; and though the kidneys of one casereach 500 g. none exceed it. The numbers, of course,are smaller.A large number of cases of rheumatic heart
disease were excluded from the graph because the
CORRELATION OF HEART AND KIDNEY WEIGHTS InFig. 2 kidney weights are plotted against heartweights. Any increase in heart weights in these casesis, because of the criteria for inclusion in the series,the result of right ventricular hypertrophy. Thecorrelation which is shown between heart and kidneyweights, therefore, suggests a correlation betweenright ventricular weight and kidney weight, andconsequently between kidney weight and the degreeand duration of pulmonary disease.The first mechanism that suggests itself as respon-
sible for the renal enlargement is back pressure dueto chronic congestive cardiac failure. If this werethe only mechanism, one would expect to find asimilar degree of renal enlargement in cases of
sO5
400
A
, 300wz0
0
200-
,oo-
200 300 400 50'0HEART WTS (9.)
FIG. 3. Scatter diagram showing kidney weights plottedagainst heart weights in 16 cases ofpure mitral stenosis allhaving enlarged right, but normal left ventricles.
500
- 400
3c
wza 300-
200
100-
-f-200 300 400 500 600
HEART WTS (g.)700 800
FIG. 2. Scatter diagram showing kidney weights plottedagainst heart weights in 37 cases of cor pulmonale allhaving enlarged right, but normal left, ventricles.
left ventricle was enlarged, due as a rule to aorticvalve disease or to mitral incompetence. Figure lbshows the distribution of kidney weights in all casesof rheumatic heart disease in which the rightventricle was enlarged, irrespective of other lesions.A single case of congenital heart disease with rightventricular enlargement was also included. Com-parison of the two histograms clearly shows thatthere is a greater tendency to diffuse renal enlarge-ment in chronic cor pulmonale.A significant but less extreme degree of renal'
enlargement sometimes occurs in rheumatic heartdisease (three cases with kidneys weighing between475 and 500 g.).
MORBID ANATOMY OF THE ENLARGED KIDNEYS To thenaked eye, except for their size, the intact kidneysappeared normal. They were firm to the touch incommon with kidneys of chronic congestive failure
600
600 700 8000
IE w
553
.
*.
* :a
0 *11
0 0 00 0
0 0
on July 28, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.14.5.552 on 1 S
eptember 1961. D
ownloaded from

FIG. 5
, I~~~~~~~~~~~~~~~~~~~~PT
FIG. 6 FIG. 7
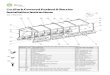
FIGS. 4, 5, 6, AND 7. Figs. 4 and 5 show cortex from two cases of cor pulinonale, Fig. 6 is a normal control, andFig. 7 shows the cortex of a kidney hypertrophi?d (weight 320 g.) because of removal of its fellow many years beforetlhe patient's deoth. All x 75.
on July 28, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.14.5.552 on 1 S
eptember 1961. D
ownloaded from

Renal enlargement in chronic cor pulmonale
in general. On cross section the cortex appearedbroad (up to 1 cm. in thickness) and there was, as arule, some degree of congestion.
Histological material was available from six casesin which the kidneys had weighed more than 500 g.and examination showed a striking and consistentincrease in the diameter of the glomeruli (Figs. 4 to7). In all six the diameters of 50 glomeruli weremeasured and the mean diameter and standarddeviation calculated. Similar measurements werealso taken from six normal kidneys and from theremaining kidney from a patient who died manyyears after a nephrectomy (see Table I). Detailed
TABLE I
DIAMETERS OF 50 GLOMERULI
255244224218232263181184167172182158205
32303324303829232424241928
Diagnosis
Cor pulmonaleCor pulmonaleCor pulmonaleCor pulmonaleCor pulmonaleCor pulmonaleNormalNormalNormalNormalNormalNormalAfter nephrectomy
histological assessment of the tubules was notpossible because of post-mortem autolysis whichwas advanced in some cases and present to someextent in all.
In none of the six cases was there a significantdegree of nephron loss, though in all of themoccasional glomeruli were hyalinized or fibrosed.Measurement of tubular diameters was not attemptedas it appeared that a very large number of measure-ments would have to be taken to make the figurerepresentative of the whole kidney and it was feltthat the increase in tubular diameter could best beappreciated by means of photomicrographs (Figs. 4,5, 6, and 7).
INCIDENTAL FINDINGS In the present 37 cases ofcor pulmonale active chronic peptic ulcers occurredin no fewer than 10 and a healed chronic ulcer inone. Three patients had given a past history ofgastrointestinal haemorrhage. The ulcers weremultiple in three of the ten.
DISCUSSION
It might be argued that this increase in renal weight
is entirely the result of congestion from chronic rightventricular failure. If this were so, the degree of renalenlargement should be approximately the same incases with equal degrees of right ventricular enlarge-ment, whether due to mitral stenosis or to primarylung disease. Figs. 2 and 3 were constructed in anattempt to refute this argument.Kidney weights were available in only two patients
dying of constrictive pericarditis, a condition inwhich passive venous congestion is prolonged andintense. The first, a man aged 51 years, had kidneysweighing 290 g., and in the second, a woman aged62 years, the kidneys weighed 300 g. These figuresargue against chronic congestion as the operativefactor in the renal enlargement of cor pulmonale.The following hypothesis is put forward as a
possible mechanism. It is well known that when thetotal bulk of renal tissue is reduced, for instance bynephrectomy or by widespread nephron loss inchronic nephritis, the remaining nephrons becomehypertrophied. That such hypertrophy is advanta-geous to the body's economy is obvious but themechanism whereby it is brought about is obscure.Presumably it results from the accumulation of somesubstance or substances excreted or detoxicated bythe kidney.
In chronic pulmonary disease associated withcarbon dioxide retention the kidney is required toexcrete an increased amount of acid; this it does bymeans of two mechanisms:
1 An increase in hydrogen ion output results inan increase in the titratable acidity of the urine.The hydrogen ion is produced in the reactionCO2 + H20 = H2CO3 = H + + HCO3, the first partof which is accelerated by the carbonic anhydrase ofthe renal tubular cells (Pitts and Alexander 1945;Pitts, Lotspeich, Schiess, and Ayer, 1948). One mightexpect this reaction to be pushed to the right by anincrease in carbon dioxide tension in accord with thelaw of mass action. 2 An increase in ammoniaexcretion, ammonia being formed in the tubule cellsfrom glutamine andcertain amino-acids by the actionofspecific enzymes. Byaccepting a hydrogen ion eachmolecule of ammonia becomes an ammonium ion(NH4 +). Once formed, the ammonium and hydrogenions within the tubular cells change places withfiltered sodium in the tubular lumen (Van SlykePhilips, Hamilton, Archibald, Futcher, and Hiller,1943). The net result is a loss of hydrogen ion, eitherfree, or in combination with ammonia as ammoniumion; an increase in the concentration of plasmabicarbonate ion HCO3 (formed in the above re-action); and sodium reabsorption to balance theincrease in bicarbonate.An increase in the plasmabicarbonate raises thepH
according to the Henderson-Hasselbalch equation
Name Mean (I) Deviation(d )
WADAIRREYHODMGUBARMELDODCGITBELFAIESMMAC
555
on July 28, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.14.5.552 on 1 S
eptember 1961. D
ownloaded from

pH = 6-1 + Log BHCO3
Stated in another way, an increase in concentrationof the bicarbonate ion causes a decrease in hydrogenion concentration by pushing the reaction H+ +HCO3 = H2CO3 to the right, i.e., it retards theionization of carbonic acid (law of mass action).
It is known that in subjects made acidotic by theadministration of NH4C1 by mouth, NH+4 outputin the urine rises rapidly in the first few hours as theurine becomes more acidic (Ferguson, 1951), afterwhich it rises more gradually over several days.Davies and Yudkin (1952) rendered rats acidotic forperiods of up to 30 weeks by giving N/20 HCI asdrinking water. By means of studies on kidneyslices they were able to demonstrate an increase inrenal glutaminase, glycine oxidase and L. amino-acid oxidase, enzymes responsible for the formationof ammonia from glutamine, glycine, and L. leucinerespectively. The gradual rise in ammonia output inchronic acidosis is thought to be due to this enzymeincrease.These observations indicate that the kidney
tubule is able to respond to the stimulus of acidosisby increasing its content of those enzymes wherebythe acidosis may be reduced, and, while in none ofthe experiments quoted above was renal hypertrophymentioned, it is perhaps not entirely unjustifiable tosuggest that it might occur, provided that the stimulusof an increased acid load were sufficiently prolonged.The mechanism whereby glomerular enlargement
is brought about cannot so easily be explained.Presumably it results in an enhanced rate ofglomerular filtration in the presence of a fallingcardiac output. In this connexion Davies andKilpatrick (1951) have shown that in cor pulmonalewith congestive failure, and in congestive failurefrom other causes, the effective renal plasma flow isreduced. The glomerular filtration rate is alsodecreased but not to the same extent, the filtrationfraction (glomerular filtration rate/effective renalplasma flow) being raised.
It is possible that the above hypothesis mayexplain not only the renal enlargement of cor
pulmonale but also the less striking enlargementseen in some of the cases of rheumatic heart disease.Gaseous exchange in the rigid lung of severe, long-
standing mitral stenosis is known to be inefficientwith regard to oxygen: however, the handling of themore diffusible carbon dioxide is said to be un-affected (Wood, 1956).
Several writers have commented on the associationbetween chronic chest disease and peptic ulceration,the latter being present in about 20% of cases(Green and Dundee, 1952; Latts, Cummins, andZieve, 1956). Flint and Warrack (1958) have shownthat acute peptic ulceration can be found in a higherproportion of necropsies on cases of cor pulmonaleif the lesions are looked for carefully. This is inagreement with the findings in the three casesdescribed above.The incidence of multiple chronic ulcer is remark-
ably high (four out of 10) but in so small a seriesthis might be due to chance. The frequency ofulceration is probably related to a high acid outputby the stomach. The hydrogen ions secreted bythe parietal cells are believed to be produced in thereaction CO2 + H20 = H2CO3 = H + + HCO3, thefirst part of which is catalysed by gastric carbonicanhydrase. As postulated above, for the samereaction occurring in the kidneys a high carbondioxide tension would push this reaction to the rightand increase acid production (Latts et al., 1956).Though the exact relationship between hyper-secretion of gastric hydrochloric acid and pepticulceration is not yet clear, it is widely recognizedthat an association exists.
My thanks are due to Miss Georgina Hunt for preparingthe sections and to Mr. E. Manns for the photomicro-graphs. I also wish to thank Dr. B. E. Tomlinson foradvice and criticism while the paper was in preparation.
REFERENCES
Black, D. A. K., ana Stanbury, S. W. (1958). Brit. med. J., 1, 872.Davies, B. M. A., and Yudkin, J. (1952). Biochem. J., 52, 407.Davies, C. E., and Kilpatrick, J. A. (1951). Clin. Sci., 10, 53.Ferguson, E. B. (1951). J. Physiol. (Lond.), 112, 420.Flint, F. J., and Waffack, A. J. N. (1958). Lancet, 2, 178.Green, P. T., and Dundee, J. C. (1952). Canad. med. Ass. J., 67, 438.Latts, E. M., Cummins, J. F., and Zieve, L. (1956). A.M.A. Arch.
intern. Med., 97, 576.Pitts, R. F., and Alexander, R. S. (1945). Amer. J. Physiol., 144, 239.
Lotspeich, W D, Schiess, W A., and Ayer, J. L. (1948). J.clin. Invest., 27, 48.
Simpson, T. (1957). Lancet, 2, 105.Van Slyke, D. D., Philips, R. A., Hamilton, P. B., Archibald, R. M.,
Futcher, P. H., and Hiller, A. (1943). J. biol. Chem., 150, 481.Wood, P. (1956). Diseases of the Heart and Circulation, 2nd ed.,
p. 540. Eyre & Spottiswoode, London.
556 P. A. Ellis
on July 28, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.14.5.552 on 1 S
eptember 1961. D
ownloaded from