Embed Size (px)
Citation preview

American Journal of Gastroenterology ISSN 0002-9270C© 2008 by Am. Coll. of Gastroenterology doi: 10.1111/j.1572-0241.2007.01588.xPublished by Blackwell Publishing
Endoscopic Management of Early Upper GastrointestinalHemorrhage Following Laparoscopic Roux-En-YGastric BypassLaith H. Jamil, M.D.,1 Kevin R. Krause, M.D.,2 David L. Chengelis, M.D.,2 Robert P. Jury, M.D.,2
Clara M. Jackson, M.D., Ph.D.,3 Michael E. Cannon, M.D.,1 and Michael C. Duffy, M.D.11Division of Gastroenterology/Hepatology, 2Department of Surgery, 3Department of Medicine/Pediatrics,William Beaumont Hospital, Royal Oak, Michigan
BACKGROUND Upper gastrointestinal hemorrhage (UGIH) is an infrequent complication (1–3.8%) followingAND AIMS: laparoscopic Roux-en-Y gastric bypass (LRYGB). The safety and efficacy of endoscopic management
of immediate postoperative bleeding is unknown. We sought to determine how frequently UGIHcomplicates LRYGB and whether endoscopic management is successful in controlling hemorrhage.
METHODS: Retrospective chart review of all patients who developed UGIH following LRYGB from November2001 to July 2005 at a large suburban teaching hospital.
RESULTS: Of 933 patients who underwent LRYGB, 30 (3.2%) developed postoperative UGIH. An endoscopicesophagogastroduodenoscopy (EGD) was performed in 27/30 patients (90%). All were found tohave bleeding emanating from the gastrojejunostomy (GJ) staple line. Endoscopic intervention wasperformed in 24/30 (80%) with epinephrine injection and heater probe cautery being used mostcommonly. Endoscopic therapy was ultimately successful in controlling all hemorrhage, with 5patients (17%) requiring a second EGD for rebleeding. No patient required surgery to controlhemorrhage. One patient aspirated during the endoscopic procedure with subsequent anoxicencephalopathy and died 5 days postoperatively. Twenty-one patients (70%) developed UGIH in theintraoperative or immediate postoperative period (<4 h postoperative). The mean length of stay wassignificantly longer in these patients (2.84 vs 4.1, P = 0.001).
CONCLUSIONS: (a) UGIH complicates LRYGB in a small but significant number of patients. (b) Bleeding usuallyoccurs at the GJ site. (c) EGD is safe and effective in controlling hemorrhage with standardendoscopic techniques. (d) UGIH occurs most commonly in the immediate postoperative period andmay be best managed in the operating room with the patient intubated to prevent aspiration.
(Am J Gastroenterol 2008;103:86–91)
INTRODUCTION
Roux-en-Y gastric bypass (RYGB) was developed as atreatment for extreme obesity in the 1960s (1). In 1994,Drs. Wittgrove and Clark reported the first case series oflaparoscopic RYGB (LRYGB) (2). In the United States, ap-proximately 140,000 RYGB procedures were performed in2005, far outnumbering the LAP-BAND�, duodenal switch,and vertical banded gastroplasty procedures (3).
The incidence of upper gastrointestinal hemorrhage(UGIH) complicating bariatric procedures ranges from 0.9%to 4.4% (4–9). In a meta-analysis, the bleeding rate variedfrom 1 to 3.8% with an average of 1.93% (10). This is statis-tically more than bleeding rates seen in open gastric bypassprocedures (0.6%, P = 0.008) (10). There has been hesi-tation to perform an esophagogastroduodenoscopy (EGD)in the immediate postoperative period because of concernfor disruption of the anastamosis with subsequent perfora-
tion (6). Endoscopic therapy for early postoperative bleed-ing at the gastric remnant and gastrojejunostomy (GJ) site inLRYGB has been proposed (11), while others have suggestedthat an operative approach would be safer (12). Previous re-ports of endoscopic therapy in early UGIH following LRYGBhave been limited to case reports and small case series, with-out detailed description of the endoscopic techniques (4, 13,14). We report the largest case series to date of endoscopicmanagement of early UGIH following LRYGB surgery withan emphasis on techniques, bleeding sites, and clinicaloutcomes.
METHODS
A retrospective chart review of all patients who developedUGIH in the postoperative period following LRYGB atWilliam Beaumont Hospital, Royal Oak, Michigan, a 1,061
86

Endoscopic Management of Early Upper Gastrointestinal Hemorrhage 87
bed tertiary care hospital, from November 2001 to July 2005was conducted. Patients were identified using hemorrhage asa complication identified by standard coding criteria. UGIHwas defined as patients presenting with hematemesis and/ormelena and/or hematochezia with significant hemodynamicchanges (increase in heart rate >20 bpm, or a decrease insystolic blood pressure >20 mmHg) and/or significant dropin hemoglobin (>2 g/dL) and/or signs of active or recentbleeding from the surgical site during an EGD. Charts werereviewed twice for accuracy of data. Human InvestigationCommittee approval was obtained prior to initiation of thestudy. The following data were collected: demographics,relevant medical history, clinical presentation and evalua-tion, transfusion requirements, and endoscopic managementtechniques.
Two experienced laparoscopic surgeons specializing inbariatric surgery performed all surgical procedures. A stan-dard operative approach using six laparoscopic ports (four5 mm, one 12 mm, and one 15 mm) was employed for allprocedures. A 15–30 cc gastric pouch was created by se-quential linear stapling. An antecolic Roux limb of either75–100 cm (BMI <50) or 150 cm (BMI >50) in length wascreated. The GJ was created using a stapled EEA (25 mm)stapler, and the jejunojejunstomy was created with a linearstapler with the resultant enterostomy closed with a linear sta-pler as well. A transgastric technique was used to place theanvil. The mesenteric defect was closed with a running su-ture. Peterson’s defect is not closed. No staple lines were over-sewn. The pouch was routinely tested for leaks using air andmethylene blue prior to completion of the case. Routine in-traoperative EGDs were not performed. All patients received5,000 IU of heparin subcutaneously 1 h before the procedureand had been advised to discontinue the use of aspirin and allnonsteroidal anti-inflammatory (NSAID) medication for atleast 1 wk prior to surgery. Gastroenterologists and surgeonswho are experienced in endoscopy and endoscopic control ofhemorrhage performed all EGDs.
RESULTS
Thirty patients (3.2%) developed postoperative UGIH out ofa total of 933 LRYGBs performed during the study period.Demographics, comorbidities, and relevant medications ofthese thirty patients are shown in Table 1. The mean age ofpatients was 49 yr (range 27–63). The majority were women(80%), were morbidly obese, and had a mean body massindex (BMI) of 47.06 kg/m2 (range 36–66 kg/m2). Despitebeing requested to stop aspirin and NSAIDs prior to surgery,5 patients were taking aspirin, 9 were taking NSAIDs, andone patient was taking both at the time of surgery. One patientwas taking coumadin for a mechanical aortic valve. One dayafter admission, his INR was 1.3 and he was started on anintravenous heparin drip prior to surgery. Five patients weretaking cox-2 inhibitors. No patient gave a history of signifi-cant alcohol abuse.
Table 1. Patient Demographics, Comorbidities, and Relevant Med-ications
Patient Characteristics Number (%N = 30 Where Applicable)
Mean age (range) 49 yr (27–63)Sex M:F 6:24BMI (range) 47.06 kg/m2 (36–66 kg/m2)Diabetes mellitus (%) 12 (40)Hypertension (%) 17 (57)Hyperlipidemia (%) 13 (43)Renal insufficiency (%) 1 (3.3)Degenerative joint disease (%) 28 (93)Dyspnea on exertion (%) 20 (67)Sleep apnea (%) 10 (33)GERD (%) 18 (60)Lower extremity edema 18 (60)Depression (%) 15 (50)Hypothyroidism (%) 5 (17)Smoking (%) 11 (37)Aspirin (%) 5 (17)NSAIDs (%) 9 (30)SSRI (%) 7 (23)
Of the 30 patients who developed postoperative UGIH,14 had 1 episode, 13 patients had 2 bleeding episodes, and3 patients had 3 bleeding episodes, for a total of 49 bleed-ing episodes. The majority of these bleeding episodes weremanifested by hematemesis (36 episodes [73%]) with theother presentations being distinctly less common (melena[3 episodes], hematochezia [7 episodes], and hypotensionwithout overt bleeding in one patient). A total of 32 EGDswere performed, with 23 of these (72%) being performed inthe operating room, 5 in the endoscopy unit, 3 in the post-operative recovery unit, and one in the intensive care unit.Table 2 shows the clinical and endoscopic characteristics ofthese bleeding episodes. Twenty-three of these procedures(72%) were performed with the patients intubated.
First Bleeding EpisodeFive patients (16%) were noted to have bleeding intraopera-tively (in four, bleeding was noted from the open Roux limbor from the GJ site following firing of the stapler) and onewas noted to have blood in the orogastric tube during theprocedure. Twenty patients developed hematemesis alone inthe postoperative period. Other presentations included var-ious combinations of hematemesis, melena, hematochezia,hemodynamic changes, and abnormal UGI series.
Bleeding generally was noted early, with the average timefrom completion of the operation to the first bleeding episodeof 6.5 h (range 0–43), and 7.83 h when excluding the 5 in-traoperative bleeders. Twenty-one patients (70%) developedUGIH in the intraoperative or immediate postoperative period(defined as <4 h).
An EGD was generally performed quickly upon recogni-tion of the bleeding. Excluding 5 intraoperative EGDs, theaverage time to endoscopy was 1.33 h from the evidence offirst bleed (range 15 min to 5 1/2 h depending on the clinical
88 Jamil et al.
Table 2. Clinical and Endoscopic Characteristics of Bleeding Episodes
Bleedings EpisodesClinical andEndoscopic First Episode Second Episode Third EpisodeCharacteristics (N = 30) N (%) (N = 16) N (%) (N = 3) N (%)
PresentationHematemesis 21 (70) 12 (75) 3 (100)Other 9 (30) 4 (25) 0
ManagementEGD 27 (90) 5 (31) 0Observation 3 (10) 11 (69) 3 (100)
Blood transfusion 9 (30) 9 (56) 1 (33)Location of EGD N = 27 N = 5
Operating room 20 (74) 3 (60)Recovery area 3 (11)Endoscopy suite 3 (11) 2 (40)Other 1 (4)
Patients intubated during EGD 19/27 (70.3%) 4/5 (80%)Prominent findings on EGD
Active blood oozing 13 (48) 4 (80)Bleeding vessel 7 (26)Adherent clot 7 (26)Other findings (visible vessel, 1 (20)
red streaks, etc.)Endoscopic therapy 23/27 (85) 5/5 (100)
Epinephrine injection 19 (70) 5 (100)Heater probe 18 (67) 4 (80)Clip 2 (7) 0
presentation). In general, most bleeding episodes within thefirst 4 h of surgery underwent an EGD within an hour of theonset of hemorrhage. The mean estimated blood loss duringthe first episode (when reported) was 211 mL (range 20–800mL).
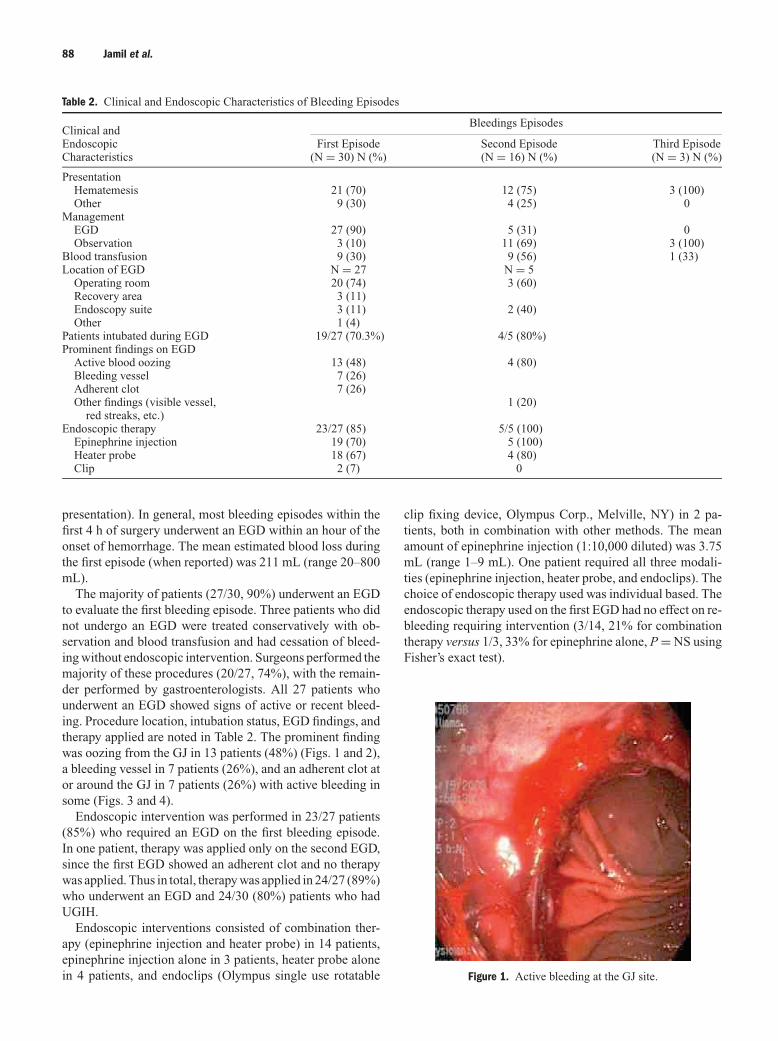
The majority of patients (27/30, 90%) underwent an EGDto evaluate the first bleeding episode. Three patients who didnot undergo an EGD were treated conservatively with ob-servation and blood transfusion and had cessation of bleed-ing without endoscopic intervention. Surgeons performed themajority of these procedures (20/27, 74%), with the remain-der performed by gastroenterologists. All 27 patients whounderwent an EGD showed signs of active or recent bleed-ing. Procedure location, intubation status, EGD findings, andtherapy applied are noted in Table 2. The prominent findingwas oozing from the GJ in 13 patients (48%) (Figs. 1 and 2),a bleeding vessel in 7 patients (26%), and an adherent clot ator around the GJ in 7 patients (26%) with active bleeding insome (Figs. 3 and 4).
Endoscopic intervention was performed in 23/27 patients(85%) who required an EGD on the first bleeding episode.In one patient, therapy was applied only on the second EGD,since the first EGD showed an adherent clot and no therapywas applied. Thus in total, therapy was applied in 24/27 (89%)who underwent an EGD and 24/30 (80%) patients who hadUGIH.
Endoscopic interventions consisted of combination ther-apy (epinephrine injection and heater probe) in 14 patients,epinephrine injection alone in 3 patients, heater probe alonein 4 patients, and endoclips (Olympus single use rotatable
clip fixing device, Olympus Corp., Melville, NY) in 2 pa-tients, both in combination with other methods. The meanamount of epinephrine injection (1:10,000 diluted) was 3.75mL (range 1–9 mL). One patient required all three modali-ties (epinephrine injection, heater probe, and endoclips). Thechoice of endoscopic therapy used was individual based. Theendoscopic therapy used on the first EGD had no effect on re-bleeding requiring intervention (3/14, 21% for combinationtherapy versus 1/3, 33% for epinephrine alone, P = NS usingFisher’s exact test).
Figure 1. Active bleeding at the GJ site.

Endoscopic Management of Early Upper Gastrointestinal Hemorrhage 89
Figure 2. After endoscopic therapy with epinephrine injection andheater probe therapy.
Second Bleeding EpisodeSixteen patients experienced a second episode of bleeding,with the mean time for rebleeding following the first en-doscopy of 38.67 h (range 0.5–136 h). Since there was cessa-tion of bleeding at the end of the first endoscopic procedures,these bleeding episodes where considered separate. The mostcommon clinical presentation was hematemesis alone (10 pa-tients). Other presentations included various combinations ofhematemesis, melena, hematochezia, hemodynamic changes,and a decrease in hemoglobin. The estimated blood loss dur-ing the second bleeding episodes was 115.5 mL (20–500 mL)where information was available.
Five of these sixteen patients (31%) required a repeat EGD.Three were performed in the operating room and two in theendoscopy unit. Endoscopic therapy, intubation status, and
Figure 3. Adherent clot with active oozing of blood.
Figure 4. Post epinephrine and heater probe therapy.
rebleeding status of these 5 patients are noted in Table 3. Ac-tive bleeding consisted of blood oozing from the GJ site infour patients. The fifth patient was noted to have red bloodstreaks at the GJ site without actual bleeding. One patient alsohad a gastric ulcer on the second postoperative day with a vis-ible vessel. Patients were treated with epinephrine injectionalone (one patient) or with epinephrine injection and heaterprobe (4 patients), with complete cessation of bleeding in allpatients without complications.
Third Bleeding EpisodeThree patients had a third discrete bleeding episode. Themean time for rebleeding following the second endoscopywas 4 h (range 0.5–8 h) with 387 mL average (130–530),with no significant hemodynamic changes. It was felt to be oldblood from previous bleeding episodes. All of these ceasedspontaneously without endoscopic intervention.
Heater Probe SettingsThe Olympus HPU heater probe was utilized with a settingvarying from 30 J to 15 J, with the higher settings used morecommonly.
Blood Transfusion RequirementsDuring the initial bleeding episode, nine patients requiredtransfusion, including three patients who did not undergo anEGD. The mean number of units of PRBC was 2.4 (range 1–6 U PRBC). During the second bleeding episode, 9 patientsrequired blood transfusion (mean 2 U PRBC/patient, range1–4 U PRBC). Six of those patients did not undergo an EGD.One patient who had been taking aspirin was given a platelettransfusion. Thus 47% of all patients with hemorrhage re-quired blood transfusion, with a mean 2.86 U/patient (range1–6 U).

90 Jamil et al.
Table 3. Endoscopic Therapy, Intubation Status, and Rebleeding Status in 5 Patients Who Underwent a Repeat EGD for UGIB
Patient # 1 2 3 4 5
Therapy on 1st EGD Epin∗/HP† Epin/HP None Epin/HP EpinPatient intubated on 1st EGD, yes/no Yes Yes Yes No YesTherapy on 2nd EGD Epin Epin/HP Epin/HP Epin/HP Epin/HPPatient intubated on 2nd EGD, yes/no Yes Yes Yes No YesPatient developed 3rd bleeding No Yes Yes Yes No
episode (none required an EGD)
∗Epin, 1:10,000 epinephrine solution.†HP = heater probe therapy.
Length of StayThe mean length of stay among patients with UGIH waslonger (4.1 days, range 2–10 days, SD 1.94) than for thosewho did not have UGIH (2.84 days, range 1–45 days, SD2.11). This difference was statistically significant (P =0.001)
ComplicationsThere were two endoscopic procedure-related complications.One patient undergoing an EGD in the endoscopy unit expe-rienced massive hematemesis with aspiration requiring in-tubation and CPR. Once the patient was stabilized, EGDwas successfully completed with endoscopic control of hem-orrhage. However, the patient sustained irreversible severeanoxic brain damage with coma and died several days later af-ter the family agreed to the withdrawal of ventilatory support.An autopsy showed saddle emboli in the pulmonary arteriesextending into the smaller arteries with multiple thrombi inmultiple veins in both legs which was determined to be theimmediate cause of death. The anoxic/ischemic damage tothe brain was difficult to assess.
One patient was found to have a perforation at the GJsite 1 wk postoperatively. She had undergone treatment withepinephrine, heater probe, and endoclip placement to treatbleeding from the GJ anastamosis. After discharge, she re-turned 2 days later with abdominal pain and was found to havefree intraperitoneal air and a small loculated fluid collectionadjacent to the GJ site on CT scan. No extravasation of gas-trograffin was noted on a UGI series. At laparotomy, she wasfound to have fibrinous debris around the GJ, but no actualleak. Thus, it is thought that the patient had sustained a smallpostoperative leak, which sealed spontaneously. Whether theinsufflation and therapy applied was the cause is difficult todetermine, since leaks are reported to be a complication inLRYGP (10).
DISCUSSION
This is the largest study published to date that demonstratesthat upper endoscopy is generally safe and efficacious inthe management of intraoperative and early postoperativeUGIH complicating LRYGB. No patient required reopera-tion for control of bleeding, thus avoiding major surgery withits potential morbidity in this high-risk group of morbidly
obese patients. Most UGIH (70%) developed in the intra-operative or immediate postoperative period (defined as <4h). Endoscopic therapy was applied in 24/27 patients (89%)who underwent an EGD and in 24/30 (80%) patients whohad a UGIH. The use of standard hemostatic endoscopictechniques, such as heater probe, epinephrine injection, andhemoclips, either alone or in various combinations, resultedin control of bleeding in all patients. Bleeding emanated fromthe GJ site in all our patients. No patient experienced a perfo-ration related directly to the EGD, although one patient hada late complication of a small leak and abscess, which hadsealed spontaneously.
Hematemesis was the most common clinical presentation(73%), probably because of the creation of a small gastricpouch with a limited gastric reservoir. This may also placethis patient population at a higher risk of aspiration fromUGIH because of the small gastric pouch created. In one pa-tient, aspiration and subsequent death complicated massivehematemesis. The single mortality in this series was felt torepresent a direct consequence of UGIH and aspiration duringthe endoscopic exam under conscious sedation. As a resultof this experience, early in the series it has become our pref-erence to perform endoscopic procedures for postoperativeUGIH under general anesthesia with endotracheal intubationin the operating room setting. This approach affords the mosteffective opportunity for difficult airway management in thishigh-risk group of patients, avoiding aspiration, as well asthe opportunity to proceed directly to operative interventionin the situation where endoscopic control proved ineffective.
Blood transfusion was required in 47% of all patients withhemorrhage, with a mean 2.86 U/patient. Length of stay issignificantly increased in patients with a UGIH complicatingLRYGB.
Other studies in the literature support a low rate of hemor-rhage following LRYGB. A recent literature review found 11reports of patients who had bleeding as a complication fol-lowing LRYGB in which management was discussed (15).Out of 2,895 patients, 89 (3.1%) developed acute postoper-ative hemorrhage. Of those, 20% underwent a reoperation(generally laparotomy), 55% required fluid and blood trans-fusion alone without an operation, and 20% did not requireany intervention. Therapeutic endoscopy was used in only 6patients (6.7%) in only three studies (4, 13, 14).
Performing an EGD immediately following the creationof the GJ appears to be safe with minimal risk to the

Endoscopic Management of Early Upper Gastrointestinal Hemorrhage 91
anastomosis. There is a potential role for intraoperative EGDin LRYGP (16), but given the low incidence of postoperativebleeding, we do not feel that its use is justified on a routinebasis. However, it might be considered in patients in whomthere is concern regarding the technical aspects of the gas-trojejunostomy.
In summary, UGIH complicates LRYGB in a small, butsignificant, number of patients. Most bleeding occurs eitherintraoperatively or within the first 4 h following the operationand is most commonly emanating from the GJ site. We feelmost patients with significant postoperative hemorrhage arebest managed in the operating room with the patient intubatedto prevent aspiration. In experienced hands, EGD is safe andeffective in controlling hemorrhage with standard endoscopictechniques, keeping in mind that some patients may require asecond procedure to control rebleeding. Aggressive therapeu-tic endoscopy should allow successful control of hemorrhageand avoid reoperation in this high-risk group.
STUDY HIGHLIGHTS
What Is Current Knowledge
� Upper gastrointestinal hemorrhage (UGIH) compli-cates laparoscopic Roux-en-Y gastric bypass (LRYGB)in a small but significant number of patients.
� There has been hesitation to perform an endoscopicesophagogastroduodenoscopy (EGD) in the immediatepostoperative period.
What Is New Here
� EGD is safe and effective in controlling hemorrhagewith standard endoscopic techniques.
� Bleeding usually occurs at the gastrojejunostomy (GJ)site.
� UGIH occurs most commonly in the immediate post-operative period
� UGIH best managed in the operating room with thepatient intubated.
Reprint requests and correspondence: Laith H. Jamil, M.D.,Mayo Clinic Jacksonville, Division of Gastroenterology, Davis Bldg6A, 4500 San Pablo Rd., Jacksonville, FL 32224.
Received April 29, 2007; accepted August 21, 2007.
REFERENCES
1. Mason EE, Ito C. Gastric bypass. Ann Surg 1969;170:329.2. Wittgrove AC, Clark GW, Tremblay LJ. Laparoscopic gas-
tric bypass, Roux-en-Y: Preliminary report of five cases.Obes Surg 1994;4:353–7.
3. American Society for Bariatric Surgery. Story for surgery
for obesity, chapter 3. Available at: http://www.asbs.org/htmL/patients/bypass.html. Accessed March 3, 2007.
4. Schauer PR, Ikramuddin S, Gourash W, et al. Outcomes afterlaparoscopic Roux-en-Y gastric bypass for morbid obesity.Ann Surg 2000;232:515–29.
5. Papasavas PK, Hayetian FD, Caushaj PF, et al. Outcomeanalysis of laparoscopic Roux-en-Y gastric bypass for mor-bid obesity. Surg Endosc 2002; 16:1653–7.
6. Nguyen NT, Rivers R, Wolfe BM. Early gastrointestinalhemorrhage after laparoscopic gastric bypass. Obes Surg2003;13:62–5.
7. Perugini RA, Mason R, Czerniach DR, et al. Predictors ofcomplication and suboptimal weight loss after laparoscopicRoux-en-Y gastric bypass: A series of 188 patients. ArchSurg 2003;138:541–5.
8. Kligman MD, Thomas C, Saxe J. Effect of the learning curveon the early outcome of laparoscopic Roux-en-Y gastricbypass. Am Surg 2003;69:304–10.
9. Livingston EH. Procedure incidence and in-house compli-cation rates of bariatric surgery in the United States. Am JSurg 2004;188:105–10.
10. Podnos YD, Jimenez JC, Wilson SE, et al. Complicationsafter laparoscopic gastric bypass. Arch Surg 2003;138:957–61.
11. Nguyen NT, Longoria M, Chalifoux S, et al. Gastrointestinalhemorrhage after laparoscopic gastric bypass. Obes Surg2004;14:1308–12.
12. Mehran A, Szomstein S, Zundel N, et al. Management ofacute bleeding after laparoscopic Roux-en-Y gastric bypass.Obes Surg 2003;13:842–7.
13. Steffen R. Early gastrointestinal hemorrhage after laparas-copic gastric bypass. Obes Surg 2003;13:466–7.
14. Lujan JA, Frutos MD, Hernandez Q, et al. Laparoscopic ver-sus open gastric bypass in the treatment of morbid obesity: Arandomized prospective study. Ann Surg 2004;239:433–7.
15. Spaw AT, Husted JD. Bleeding after laparoscopic gastricbypass: Case report and literature review. Surg Obes RelatDis 2005;1:99–103.
16. Champion JK, Hunt T, DeLisle N. Role of routine intra-operative endoscopy in laparoscopic bariatric surgery. SurgEndosc 2002;16:1663–5.
CONFLICT OF INTEREST
Guarantor of the article: Michael C. Duffy, M.D.Specific author contributions: Laith H. Jamil: data col-lection, data analysis, data entry, manuscript preparation,literature review. Kevin R. Krause: patient contribution,manuscript preparation and review. David L. Chengalis: pa-tient contribution, manuscript preparation and review. RobertP. Jury: patient contribution, manuscript preparation and re-view. Clara M. Jackson: literature review, data entry, dataanalysis, manuscript preparation and review. Michael E.Cannon: patient contribution, manuscript preparation andreview. Michael C. Duffy: mentor, patient contribution,manuscript preparation and review.Financial support: None.Potential competing interests: None.