Embed Size (px)
Citation preview

British Journal of Ophthalmology, 1985, 69, 29-31
Embolic retinopathy due to Corynebacteriumminutissimum endocarditisBRIAN J HERSCHORN AND ALEXANDER J BRUCKER
From the Department of Ophthalmology, University of Pennsylvania School of Medicine, and the Scheie EyeInstitute, Philadelphia, Pennsylvania 19104, USA
SUMMARY Infective embolic retinopathy as a sequela of bacterial endocarditis is described in a 31-year-old woman with mitral valve prolapse. The infective organism, Corynebacterium minutissimum,has not been previously found to cause ocular or multisystem diseases. It is a common muco-cutaneous inhabitant which causes erythrasma. In our case report both ocular involvement andsepticaemia were present. The infection was confirmed by positive serial blood cultures. Mitralvalve prolapse was confirmed by echocardiography. On clinical examination the retinopathyconsisted of white intraretinal lesions which resolved with antibiotic therapy. By fluoresceinangiography focal areas of hypofluorescence corresponding to the white fundus lesions werepresent. Optic disc oedema was also seen.
Corynebacterium minutissimum is a common muco-cutaneous inhabitant which causes erythrasma, amild, localised, superficial skin infection.' 2 Thiscommunication reports an unusual case of embolicretinopathy, bacterial endocarditis, mitral valve pro-lapse, and septicaemia due to C. minutissimum. Thespecies has not previously been implicated as thecause of ocular or multisystem infection.
Sterile emboli causing cerebral ischaemia3 andretinal vascular occlusions4 have been shown to havetheir origin from prolapsing mitral valves. In thepresent case vegetation on the prolapsing mitralvalves is believed to be the source of the emboli.
Case report
A 31-year-old woman was admitted to the Scheie EyeInstitute one day after the onset of decreased visionand photophobia of the left eye. During the pre-ceding week she noted metamorphopsia and spots inthat eye. For the last four months she had had feverand chills, frontal headaches, anorexia, weight loss,fatigue, intermittent migratory polyarthritis, andarthralgia. She had been placed on prophylactic anti-biotics after rheumatic fever at the age of 7 years; thismedication ceased three years prior to admissionto hospital. After tubal ligation one year before
admission echocardiography had shown prolapse ofthe mitral valve. In addition she had recently under-gone dental surgery.
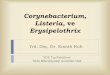
Visual acuity was 6/6 in each eye. Slit-lamp bio-microscopy showed 1 + flare and cells in the anteriorchamber and vitreous bilaterally. Intraocularpressures were normal. Ophthalmoscopic examina-tion of the right eye showed one white intraretinallesion with a fine rim of haemorrhage one disc
Corrcspondcncc to Alexander J Brucker, MD, Scheic Eye Insti- Fig. 1 Right macula. White intraretinal lesion with rim oftutc, 51 North 39th Strcct, Philadclphia, Pennsylvania 191(4, USA. haemorrhageprior to therapy (arrow).
29
on April 24, 2021 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.69.1.29 on 1 January 1985. D
ownloaded from

Brian J Herschorn and AlexanderJ Brucker
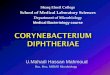
Fig. 2 Left macula. Discrete white intraretinal lesions seenprior to therapy. (Photographic artefact superotemporal tothefovea).
diameter temporal to the fovea (Fig. 1). A secondwhite intraretinal lesion was seen near the oraserrata. In the left eye a white intraretinal lesionof one-fifth disc diameter was seen in the papillo-macular bundle (Fig. 2). A zone of surroundingoedema extended to the nasal edge of the fovea. Asecond lesion was situated one and one half discdiameters temporal to the fovea (Fig. 2), with a thirdlesion located peripherally. Fluorescein angiography(Fig. 3) showed areas of hypofluorescence corre-sponding to the white lesions bilaterally. Fluoresceindye from the surrounding retinal capillaries filled
Fig. 3A Left macula. Fluorescein angiogram prior totherapy. Midvenous phaseshowing area ofhypofluorescencecorresponding to large white lesion seen clinically (Fig. 2).Smaller lesion (arrow) also appears hypofluorescent.
these areas and showed late staining of the retina.Leakage of dye from both the optic discs consistentwith papillitis was seen (Fig. 4). Cardiac auscultationrevealed a grade TI/VI apical, holosystolic, non-radiating murmur. The rest of the examination, in-cluding mucocutaneous tissues, was entirely normal.Blood cultures were 'positive for significant exclu-
sive growth of Corynebacterium minutissimum. Theorganism was sensitive to penicillin. Echocardio-graphy indicated vegetations on the anterior leaflet ofa prolapsing mitral valve consistent with bacterialendocarditis. Blood studies revealed a microcytic,hypochromic iron deficiency anaemia-. Serum IgMand IgG were elevated at 2451 mg/dl and 672 mg/dlrespectively (24-5 and 6-7 g/l).Treatment for subacute bacterial endocarditis was
initiated with 4 million units of aqueous penicillinintravenously every four hours for four weeks.Funduscopic examination during hospital ad-
mission showed rapid resolution of the peripherallesions, while the lesions in the posterior poleresolved slowly. Five weeks after therapy was in-itiated the lesion in the right fundus had disappearedand the lesions of the left fundus showed significantimprovement of both clinical and fluorescein angio-graphic appearances.
Discussion
Corynebacterium minutissimum has not been re-ported previously as a cause of endophthalmitis andendocarditis. Corynebacteria are frequent inhabi-tants of normal skin and mucous membranes5 6and frequently contaminate blood cultures.7 C.
Fig. 3B Latephase. Fluorescein dyefills area ofpreviouslydescribed hypofluorescence. Smaller lesion is essentiallyinapparent.
30
on April 24, 2021 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.69.1.29 on 1 January 1985. D
ownloaded from

Embolic retinopathy due to Corynebacterium minutissimum endocarditis
Fig. 4 Left eye. Diffuse leakage ofdyefrom the optic disclate in the angiogram.
minutissimum has been considered to be systemicallyharmless in humans. It is responsible, however, forerythrasma, a mild, chronic, localised, superficialinfection of body clefts and folds.' Cases of coryne-bacterial endocarditis constitute less than 0-3% of allcases of endocarditis5 and usually affected prostheticheart valves. None have been reported on an isolatedprolapsing mitral valve.6' -" Generally, the reportedincidence of bacterial endocarditis in mitral valveprolapse is 2 to 6%. "
In the present case C. minutissimum was confirmedby serial blood cultures. The mitral valve prolapse
may have served as a predisposing factor for theinfection. The ocular signs consisted exclusivelyof multiple, intraretinal white lesions sometimesassociated with a fine rim of haemorrhage. Byfluorescein angiography leakage of dye into the tissuesurrounding the lesions suggested an active inflam-matory process. Papillitis, which was not clinicallyapparent, was revealed by the angiographic study.The nature of the lesions is thought to be the accumu-lation of the inflammatory white cells surroundingthe sites of bacterial emboli.
References
1 Sarkany I, Taplin D, Blank H. The etiology and treatment oferythrasma. J Invest Dermatol 1961; 37: 282-90, 801-3.
2 Hoeprich PD, ed. infectious diseases, 2nd ed. Hagerstown:Harper and Row, 1977.
3 Barnett HJM, Jones MW, Boughner DR, Kostuk WJ. Cerebralischemic events associated with prolapsing mitral valves. ArchNeurol 1976; 33: 777-82.
4 Woldoff HS, Gerber M, Desser KB, Benchimol A. Retinalvascular lesions in two patients with prolapsed mitral valveleaflets. Am J Ophthalmol 1975; 79: 382-5.
5 Locatcher-Khorzao D, Segal BC. Microbiology of the eye. StLouis: Mosby, 1972.
6 Kaplan D, Weinstein L. Diphtheroid infections of man. AnnIntern Med 1969; 70: 919-29.
7 Washington JA II. Comparison of two commercially availablemedia for detection of bacteremia. Appi Microbiol 1971; 22:604-7.
8 Reid JD, Greenwood L. Corynebacterial endocarditis. ArchIntern Med 1967; 1 19: 106-10.
9 Blount JG. Bacterial endocarditis. Am J Med 1965; 38: 909-22.10 Gerry JL, Greenbough WB III. Diphtheroid endocarditis:
report of nine cases and review of the literature. Johns HopkinsMedJ 1976; 139:61-8.
11 Coker JE, Dworzack DL, Hodges GR, Petric SC, Pugh DM.The infected mitral valve. J Kaois Med Soc 1978; 79: 55t)-2.
31
on April 24, 2021 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.69.1.29 on 1 January 1985. D
ownloaded from