Embed Size (px)
Citation preview

BritishJournalofOphthalmology, 1992,76,332-335
Dapsone therapy for the acute inflammatory phase ofocular pemphigoid
Alasdair I Fern, Jeffrey L Jay, Hamish Young, Rona MacKie
Tennent Institute ofOphthalmology, WesternInfirmary, GlasgowGIl 6NTA I FernJ L Jay
University Department ofDermatology, WesternInfirmary, GlasgowH YoungR MacKieCorrespondence to:Jeffrey L Jay.Accepted for publication1 August 1991
AbstractOral dapsone was used to treat five patientswho presented in the acute inflammatory phaseofocular pemphigoid. The diagnosis was madeclinically by identifying cicatricial changeswhich were in some cases difficult to find. In allcases it was the inflammatory rather than thecicatricial features which responded to treat-ment. An initial dose of 100 mg/day waseffective without toxicity. When 150 mg/daywas used patients experienced side effects. Aclinical response was obtained after 1-4 weeksand could be maintained on a dose of between50 mg on alternate days and 100 mg/day.Therapy was withdrawn during remissionswhich lasted up to 32 weeks but all casesrequired continuing therapy which hasremained effective. Immunopathologicalexamination was carried out on two occasionsin all cases and although positive on at leastone occasion the results did not correlate withdisease activity or treatment. The inflam-matory phase of ocular. pemphigoid should beadded to the list of diseases responsive todapsone.
Cicatricial pemphigoid is a disease of unknownaetiology which results in chronic progressiveblistering and scarring of mucosal epithelium.The oral mucosa is most commonly affected withthe conjunctiva involved in 75% of cases and theskin in 21-30%. ' 23 The eye changes are charac-terised by subepithelial fibrosis with symble-pharon formation. There is also an acute inflam-
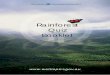
Figure I Early symblepharon in the lowerfornix (case 4). Thisfeature was often so mild as tobe overlooked on initial examination.
matory form of the disease with redness andswelling of the conjunctiva.4 In these cases offlorid inflammation the cicatricial changes maybe overlooked and the condition misdiagnosed.Dapsone and other drugs of the sulfone group
have been used for many years, particularly indermatological practice to treat a variety ofinflammatory conditions. Katz' lists 13 dapsoneresponsive conditions including dermatitisherpetiformis. Dermatological reports have sug-gested the drugmayhave an effecton a proportionof patients with cicatricial and bullous pemphi-goid67I but there is little information about itseffect on ocular disease. We describe the value ofdapsone in the treatment of the acute inflam-matory features of ocular pemphigoid.
Patients and methodsWe studied five consecutive patients between1984-1990who had ocular cicatricial pemphigoidin the acute inflammatory phase. None had ahistory ofother causes ofcicatricial conjunctivitissuch as chronic infection, chemical trauma, orStevens-Johnson syndrome.Whether or not there was a history of skin
lesions all patients were examined by a derma-tologist.The first two patients were commenced on
dapsone 150 mg/day but both developedhaemolysis and one became cyanosed. Subse-quent patients were therefore given a startingdose of 100 mg/day in divided doses and the dosewas reduced to the minimum required to main-tain a clinical response. Where possible treat-ment was discontinued but if the conditionrelapsed the drug was re-introduced at theprevious maintenance dose.While taking the drug each patient's blood was
examined regularly for evidence ofhaemolysis oranaemia.
Conjunctival and skin biopsies and serumsamples for immunological assay were takenfrom each patient while they were withouttreatment and the disease was active and whenthe condition was in remission during treatment.Conjunctival biopsies were taken by a snip ofupper bulbar conjunctiva elevated with forcepsunder topical anaesthesia with amethocaine 1%eye drops. Skin snip biopsy was taken fromnormal skin on the volar surface of the forearmafter subcutaneous injection of 1% lignocainewith adrenaline. The specimens were frozen inliquid nitrogen and direct immunofluorescencestaining performed with fluorescein-labelledantisera to human IgG, IgA, IgM, and C3.Indirect studies were performed for circulatingantibodies to conjunctival epithelium and itsbasement membrane zone.
332
on October 28, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.76.6.332 on 1 June 1992. D
ownloaded from

Dapsone, therapyfor the acute inflammatory phase ofocularpemphigoid
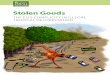
Figure 2 Advanced symblepharon with corneal pannus and scarmng identified atpresentation (case 2).
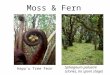
Figure 3 Inflamed conjunctiva prior to treatment (case 4).
Figure 4 Remission ofconjunctival inflammation I month after starting dapsone therapy.Same patient as Figure 3 (case 4).
ResultsThe mean age of the three male and two femalepatients was 60 years (range 40-72 years). Threeof the five cases presented with undiagnosedchronic conjunctivitis resistant to treatment.The diagnosis was eventually made clinicallywhen previously overlooked subconjunctivalfibrosis and symblepharon were identified(Fig 1). Selective involvement of the medial orlateral canthus was not present. In the other twopatients cicatricial changes were obvious onpresentation (Fig 2) allowing more rapid diag-nosis.Though there was cicatrisation in all cases the
main presenting problem was chronic conjunc-tival inflammation with discomfort and pain.Figure 3 shows the inflammed conjunctiva of onepatient and Figure 4 the same eye in remission ontherapy. While both eyes were involved in everycase there was often marked asymmetry. Onstopping the drug the latent period before recur-rence of the disease varied between patients andfor individual patients on different occasionsranging from 1 week to 8 months.
Patient 1 had required treatment for 20 yearsfor primary open angle glaucoma; formerly withtopical adrenaline and pilocarpine latterly topicalmetipiranolol and oral dichlorphenamide.Topical glaucoma therapy was stopped whenpemphigoid was diagnosed but the dichlor-phenamide was continued.The acute inflammatory element of ocular
pemphigoid responded to the drug in all caseswith a clinical response noted between 1-4 weeksafter starting dapsone (Table 1). The responsetime varied for different patients but was consis-tent for each patient on every occasion the drugwas recommenced. Some patients had initiallyreceived antibiotic and steroid drops but thesewere discontinued when the inflammation firstresponded to dapsone and could not account forthe improvement in the patients' conjunctivalappearance. Although the conjunctival inflam-mation was controlled by dapsone one caseneeded supplementary systemic steroid whensevere corneal and scleral involvement occurred.
Toxic reactions to dapsone occurred at dosesof 100 mg/day or more. There was one case ofmild jaundice and one of cyanosis and haemo-lysis. Both patients were able to continue effectivelong term therapy at reduced dose.
Dermatological examination identified onlyone patient with a skin disorder and this wasdescribed as psoriaform dermatitis after skinbiopsy and is inconsistent with cicatricial pem-phigoid. Two patients had oral signs suggestiveof pemphigoid.The immunofluorescent assay results are
shown in Table 2 and categorised according towhether the patient was taking dapsone or not.Conjunctival biopsy did not stimulate ocularinflammation or progression of conjunctivalfibrosis. No consistent pattern of immunologicalresults can be detected.
DiscussionThe cicatricial features of ocular pemphigoid arewell recognised but the acute manifestations ofthe disease are not. Mondino4 reports swollen
333
on October 28, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.76.6.332 on 1 June 1992. D
ownloaded from

Fern,jay, Young, MacKie
Table I Patient details and response to dapsone showingminimum maintenance dose and length ofasymptomaticremissions without treatment. All patients still require therapy
Duration ofResponse Maintenance remission off
Age time dose of dapsonePatient (yrs) sex (weeks) dapsone (weeks)
1 67 F 2 50 mg/day 6-322 63 M 2-4 50 mg/day 43 43 M 2 100 mg/day 10-164 72 F 3 50 mg/alternate days 1-165 59 M 1 50 mg/day 1
mounds of conjunctiva during episodes of acutedisease activity which interrupt and exacerbatethe conjunctival shrinkage. Wright9 includesconjunctival ulceration with fluorescein stainingin the clinical diagnostic criteria for ocularcicatricial pemphigoid. The patients reported inour paper illustrate the acute inflammatoryfeatures of conjunctival induration and vasculardilatation with chronic ocular irritation. It isthese aspects that responded to dapsone therapy.Although the condition is rare'0 the diagnosis
of ocular pemphigoid should be considered inany patient presenting with undiagnosed con-junctival inflammation. There is a condition withcicatricial conjunctivitis known as linear IgAdisease which is responsive to dapsone."I None ofour patients had any extraocular lesions consis-tent with linear IgA disease or dermatitis herpeti-formis.
Case 1 may represent pseudo-pemphigoidinitiated by 20 years of topical antiglaucomatherapy.'2 13 14 However the persistence of acuteconjunctival inflammation after discontinuingtopical medication makes the diagnosis lesslikely. The association ofpemphigoid and topicaltherapy for glaucoma has been described byTauber et allI who found that 26% of 111 cases ofocular cicatricial pemphigoid had a history ofmedical therapy for glaucoma for an average of11 years. Nearly all had this treatment before theonset of pemphigoid suggesting that glaucomamedication may be a causative factor. Whetherthis is a separate 'pseudo-pemphigoid' conditionor merely pemphigoid in which the usuallyidiopathic trigger factor has been identified it isknown they are histologically and immunologi-cally indistinguishable. 16 17 Both seem to respondequally to dapsone.
Cicatricial pemphigoid remains a clinical diag-nosis. Immunological tests may confirm thediagnosis when positive but do not exclude thediagnosis when negative. Only two patients inour study showed the diagnostic finding of linearimmunoglobulin deposition at the conjunctival
Table 2 Summary ofimmunofluorescent results. Tests were carried out both on and offtreatment in every case. Although positive on at least one occasion in each case the pattern did notcorrelate with either disease activity or treatment
On dapsone Offdapsone
Clinical ClinicalPatient state Conj Skin Serum state Conj Skin Serum
I Inactive ND -ve IgAi(C) Inactive ND ND IgA (C)2 Inactive ND ND -ve Active IgA!(L) -ve -ve3 Inactive IgA,(E) -ve IgGi(BM) and Inactive -ve -ve -ve
IgA (BM)4 Inactive -ve -ve -ve Inactive IgAi(L) -ve -veS Inactive IgAr(E) -ve -ve Active -ve -ve IgG,(C)
L=linear; E=intraepithelial; C=to conjunctiva; BM=to basement membrane; ND=not done.
basement membrane (cases 2 and 4) and thisdisappeared when the patients were takingdapsone. One other (case 3) had circulating IgGand IgA to conjunctival basement membrane butparadoxically the serum immunoglobulins wereonly present when the patient was taking dapsoneand disappeared when treatment was discon-tinued. Several patients had antibodies to con-junctival epithelium on direct and indirect testingbut this has been shown to be a non-specificfinding in several chronic conjunctival condi-tions.8 19 Immunological findings in pemphigoidare known to be inconsistent20 and do notcorrelate with extent or activity of disease.2'From our study it seems that an initial dose of
100 mg/day should be effective with little risk ofside effects. A maintenance dose of between50 mg/day and 50 mg on alternate days seemsadequate. In practice once control was achievedpatients were able to adjust their own main-tenance dose. This varied with the severity oftheir symptoms and at all times they remainedunder medical supervision. Rogers et al7 recom-mend an initial low dose and a gradual increaseover a 2 week period to the therapeutic level butthey found the ocular features ofpemphigoid lessresponsive to dapsone than mucosal ulcerationelsewhere. We observed remissions of variableduration but all patients eventually relapsed andthe fact that the relapsed patients were repeatedlybrought into remission again within 2 weeks ofrecommencing the drug was the most convincingclinical evidence that dapsone is effective in thiscondition. Side effects have been reported withdapsone principally haemolysis and methaemo-globinaemia. Doses of more than 50 mg/dayinvariably produce a degree of haemolysis whichseldom lowers the haemoglobin level by morethan 1 g but does elevate serum bilirubin. Unlesspatients have cardiopulmonary problems or pre-existing anaemia the drop in haemoglobin isusually well tolerated. Methaemoglobinaemia isnot a major problem and even in patients taking200 mg of dapsone per day the level does notusually exceed 12% of the total haemoglobin andis often less than 5%.5 This may give the patient agrey cyanosed appearance but is otherwiseasymptomatic. Dapsone is relatively non-toxicand particularly in an elderly population seemssafer to use than other possible means of treat-ment such as systemic steroids or immuno-suppressants.2223The mode of action of dapsone is unknown
despite considerable investigation. The drugappears to act by inhibiting the migration ofneutrophilic polymorphonuclear leucocytes.Whether this is achieved by inhibiting lysosomalenzyme activity,24 interfering with the leucocytes'cytotoxic system25 or preventing the cell res-ponding to chemotactic stimuli26 remains to beestablished.
1 Hardy KM, Perry HO, Pingree GC, Kirby TJ. Benign mucousmembrane pemphigoid. Arch Dermatol 1971; 104: 467-5.
2 Editorial. Pemphigoid. BrMedJ 1978; i: 64-5.3 Mondino BJ, Brown SI. Ocular cicatricial pemphigoid. Oph-
thalmology 1981; 88: 95-100.4 Mondino BJ, Brown SI, Lempert S, Jenkins MS. The acute
manifestations of ocular cicatricial pemphigoid. Diagnosisand treatment. Ophthalmology 1979; 86: 543-52.
5 Katz SI. Dapsone. In Fitzpatrick TB, et al, eds. Dermatology ingeneral medicine. London: McGraw-Hill, 1989; Chapter 218:2570-4.
334
on October 28, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.76.6.332 on 1 June 1992. D
ownloaded from

Dapsone therapyfor the acute inflammatory phase ofocularpemphigoid
6 Person JR, Rogers RS. Bullous pemphigoid responding tosulfapyridine and the sulfones. Arch Dermatol 1977; 113:610-5.
7 Rogers RS, Seehafer JR. Treatment of cicatricial (benignmucous membrane) pemphigoid with dapsone. J Am AcadDermatol 1982; 6: 215-23.
8 Venning VA, Millard PR, Woinarowska F. Dapsone as firstline therapy for bullous pemphigoid. Br J Dermatol 1989;120: 83-92.
9 Wright P. The enigma of ocular cicatricial pemphigoid. TransOphthalmol Soc UK 1979; 99: 141-5.
10 Duke-Elder S, ed. System of ophthalmology. Vol 8, Part 3.Diseases ofthe outer eye. London: Kimpton, 1965: 502-19.
11 Leonard JN, Haffenden GP, Ring NP, McMinn RMH,Sidgwick A, Mowbray JF, etal. Linear IgA disease in adults.BrJDernatol 1982; 107: 301-16.
12 Patten JJ, Cavanagh HD, Allansmith MR. Induced ocularpseudopemphigoid. Amj Ophthalmol 1976; 82: 272-6.
13 Hirst LW, Werblin T, Novak M, et al. Drug inducedcicatrizing conjunctivitis simulating ocular pemphigoid.Cornea 1982; 1: 121-8.
14 Norn MS. Pemphigoid related to epinephrine treatment(letter). AmJ Ophthalmol 1977; 83: 138.
15 Tauber J, Melamed S, Foster CD. Glaucoma in patients withocular cicatricial pemphigoid. Ophthalmology 1989; 96:33-7.
16 Foster CS. Cicatricial pemphigoid. Trans Am Ophthalmol Soc1986; 84:527-663.
17 Pouliquen Y, Patey A, Foster CS, Goichot L, Savoldelli M.
Drug-induced cicatricial pemphigoid affecting theconjunctiva light and electron microscopic features.Ophthalmology 1986; 93: 775-83.
18 Frith PA, Venning VA, Woinarowska F, Millard PR, BronAJ. Conjunctival involvement in cicatricial and bullouspemphigoid: a clinical and immunopathological study.BrJ7 Ophthalmol 1989; 73: 52-6.
19 Mondino BJ, Brown SI, Rabin BS. Autoimmune phenomenaof the external eye. Ophthalmology 1978; 85: 801-17.
20 Nieboer C, Roeleveld CG, Kalsbeek GL. Localised chronicpemphigoid. Report of a case, review of the literature anddiscussion of the relationship with cicatricial pemphigoid.Dermatologica 1978; 156: 24-33.
21 Ahmed AR, Maize JC, Provost TT. Bullous pemphigoid.Clinical and immunological follow-up after successfultherapy. Arch Dermatol 1977; 113: 1043-6.
22 Foster CS, Wilson LA, Ekins MB. Immunosuppressivetherapy for progressive ocular cicatricial pemphigoid. Oph-thalmology 1982; 89: 340-53.
23 Mondino BJ, Brown SI. Immunosuppressive therapy in ocularcicatricial pemphigoid. AmJ3 Ophthalmol 1983; 96: 453-59.
24 Mier PD, Van Den Hurk JJMA. Inhibition of lysosomalenzymes by dapsone. BrJ7 Dermatol 1975; 93: 471-2.
25 Stendahl 0, Edebo L, Magnusson KE, Tagesson C, Hjerten S.The inhibition of polymorphonuclear leukocyte cytotoxicityby dapsone: a possible mechanism in the treatment ofdermatitis herpetiformis. J Clin Invest 1978; 62: 214-20.
26 Harvath L, Yancey KB, Katz SI. Selective inhibition ofneutrophil chemotaxis by sulfones. Clin Res 1983; 31: 571A.
FIFTY YEARS AGOSyphilis
War brings many horrors in its train; not the least ofthese is an increase in syphilis.. I indicated at the outset that syphilis had shown adefinite annual decline in the years preceding thepresent war. I regret that the number of new acutecases is now beginning to show an alarming increase;this will not be seen in ophthalmology until later on,but unless the acute cases are properly treated it willsurely occur, it may be not for ten or fifteen years,when the congenital syphilitic children reach pubertyor the half treated cases arrive with lesions of thecentral nervous system.
BrJ' Ophthalmol 1942; 26: 23.
335
on October 28, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.76.6.332 on 1 June 1992. D
ownloaded from