Embed Size (px)
Citation preview
Eindhoven University of Technology
MASTER
Risk in healthcare real estate investment
Kosse, T.H.V.
Award date:2016
Link to publication
DisclaimerThis document contains a student thesis (bachelor's or master's), as authored by a student at Eindhoven University of Technology. Studenttheses are made available in the TU/e repository upon obtaining the required degree. The grade received is not published on the documentas presented in the repository. The required complexity or quality of research of student theses may vary by program, and the requiredminimum study period may vary in duration.
General rightsCopyright and moral rights for the publications made accessible in the public portal are retained by the authors and/or other copyright ownersand it is a condition of accessing publications that users recognise and abide by the legal requirements associated with these rights.
• Users may download and print one copy of any publication from the public portal for the purpose of private study or research. • You may not further distribute the material or use it for any profit-making activity or commercial gain
Utrecht, February 2016
Risk in Healthcare Real Estate Investment
by
T.H.V. (Tjeerd) Kosse
Student identity number: 0614493
In partial fulfillment of the requirements for the degree of
Master of Science
in Architecture, Building and Planning
Subject headings:
Real Estate Investment, Healthcare Real Estate, Medical Real Estate, Senior Housing, Skilled
Nursing Homes, Memory Homes, Investment Risk, Risk Factors, Determinants of the Cap
Rate, Hedonic Risk Model, Downside Risk.
Supervisors:
Ir. S.J.E. (Stephan) Maussen MRE, TU/e
Dr. Ir. P.E.W. (Pauline) van den Berg, TU/e
Drs. P. (Pim) Diepstraten, company supervisor
Department of the Built Environment
Master Architecture, Building and Planning

Risk in Healthcare Real Estate Investment ii
Colophon
Risk in Healthcare Real Estate Investment
In partial fulfillment of the requirements for the degree of Master of Science at
Eindhoven University of Technology
Department of the Built Environment
Master: Architecture, Building and Planning
Specialization: Real Estate Management and Development
Author
Ing. T.H.V. (Tjeerd) Kosse
Student ID: 0614993
Chairman Graduation Committee
Prof. Dr. T.A. (Theo) Arentze
Department of the Built Environment
Eindhoven University of Technology
Academic Supervisors
Ir. S.J.E. (Stephan) Maussen MRE
Department of the Built Environment
Eindhoven University of Technology
Dr. Ir. P.E.W. (Pauline) van den Berg
Department of the Built Environment
Eindhoven University of Technology
Company Supervisor
Drs. P. (Pim) Diepstraten
Partner & Senior Advisor
Finance Ideas
Date
16 February, 2016
Copyright © T.H.V. Kosse
Risk in Healthcare Real Estate Investment iii
Abstract
This master thesis investigates the risk of investing in healthcare real estate and in particular
skilled nursing and memory homes by finding and analyzing risk factors and their perceived
importance. Risk factors and their importance were found by reviewing the relevant literature
and analyzing data obtained during 22 interviews with experts on healthcare real estate
investment. A total of 75 risk factors and their importance were found offering investors an
instrument to analyze risk. Uncertainty over the risk of investing in healthcare real estate is
mitigated by using long-term rental contracts instead of requiring higher returns. Investors
manage the risk of long-term contracts by assessing the stability of the tenant. Two distinct
points of view were found on risk management in healthcare real estate investment; one
viewpoint is focused on tenant risks and the other viewpoint focuses on property risks. The
most common length of rental contracts is 15 years. In shorter rental contracts of 10 years
property risks are more important while tenant risks are more important when using rental
contracts of 20 years or longer. Markets with short contracts are more suitable for investors
who focus on property risks while markets with long contracts are more suitable for investors
who focus on tenant risks. Unwillingness of Dutch healthcare organizations to sign long-term
rental contracts could shift the focus of investors from tenant risks towards property risks.

Risk in Healthcare Real Estate Investment iv
Risk in Healthcare Real Estate Investment v
Table of Contents
Colophon ii
Abstract iii
Table of Contents v
Summary Article: Dutch vii
Summary Article: English xvii
Preface xxvii
RISK IN HEALTHCARE REAL ESTATE INVESTMENT 1
1. Research Context 1
1.1. Introduction 1
1.2. Research Objective and Questions 3
1.3. Scope 3
1.4. Research Design 5
1.5. Research Outline 6
2. Theoretical Background 9
2.1. The Real Estate System, the Asset Market and Market Value 9
2.2. Stages of Maturity of an Asset Market 10
2.3. The Current HCRE Investment Practice in The Netherlands 13
3. Literature Review: Risk in HCRE Investment 17
3.1. Risk in the Context of Real Estate Investment 17
3.2. Risks associated with Real Estate 22
3.3. Risks associated with Dutch HCRE 27
3.4. Synthesis of the Risk Factors Mentioned in the Literature Review 31
3.5. Brief Explanation of the Risk Factors 39
4. Methodology 43
4.1. Interview Guide 44
4.2. Interviewee Selection 44
4.3. Method of Analysis 46
4.4. Description of the Field Work 46
5. Results 49
5.1. Final List of Risk Factors 49
5.2. Importance of Risk Factors 66
5.3. Differences in Points of View between Interviewees 97
5.4. The Influence of the Length of Rental Contracts on the Risk 98
Risk in Healthcare Real Estate Investment vi
5.5. Chapter Conclusion 100
6. Conclusions and Discussion 101
6.1. Theoretical and Practical Implications 101
6.2. Recommendations on Managing the Risk Factors 103
6.3. Recommendations for Further Studies 104
6.4. Discussion 105
Reference List 107
List of Abbreviations 113
List of Figures 114
List of Tables 116
List of Equations 119
Appendix 1: Oversight of Risk Factors from the Literature Review 1
Appendix 2: Interview guide for Interviews with Experts 2
Appendix 3: The Evolution of the List of Risk Factors 14
Appendix 4: Descriptive Statistics of the Variables 29
Appendix 5: All Risk Factors Sorted on Average Rating 33
Appendix 6: All Risk Factors Sorted on Standard Deviation 35

Risk in Healthcare Real Estate Investment vii
Risico's bij beleggen in zorgvastgoed
Meer inzicht in het risico vanuit het perspectief van beleggers
Zorgvastgoed als beleggingscategorie is in opkomst in Nederland. Het wordt gezien als een
vastgoedcategorie die wordt gewaardeerd vanwege de stabiele kasstromen, hoge
rendementen en sterke demografische drivers. Ondanks de groeiende interesse is
zorgvastgoed nog een relatief onvolwassen markt. Vanwege de onduidelijkheid over de
risico's bij beleggen in zorgvastgoed zijn veel beleggers nog terughoudend bij het toetreden
tot deze markt. Er is een groeiende behoefte om de risico's bij beleggen in zorgvastgoed
goed in kaart te brengen.
Door ing. Tjeerd Kosse
isico's bij beleggen in vastgoed
zijn vaak onderzocht op basis van
kwantitatieve analyse. Recente
voorbeelden hiervan zijn onderzoeken die
gebruik maken van multifactor modellen
zoals die van Dale, Wolf & Yang (2015)
en Ho & Addae-Dapaah (2015). Daarnaast
zijn er vele onderzoeken geweest naar de
determinanten van de rendementseis,
waardonder door Sivitanidou & Sivitanides
(1999) en Wheaton et al. (2001). Ook op
micro-niveau zijn onderzoeken geweest
naar de determinanten van de
rendementseis. Hieronder valt onder
andere het onderzoek van McDonald &
Dermisi (2009). Wheaton et al.
concluderen dat de rendementseis sterk
samenhangt met onduidelijkheid over de
mate van risico. Omdat er nog geen
onderzoek is gedaan naar de risico's bij
beleggen in zorgvastgoed is er nog sprake
van grote onduidelijkheid. Dit onderzoek
biedt een kwalitatieve kijk op het risico bij
beleggen in zorgvastgoed.
De huidige praktijk
In de huidige praktijk gaat beleggen in
zorgvastgoed vaak gepaard met weinig
vertrouwen in de ontwikkeling van de
eindwaarde van het vastgoed. Omdat
beleggers lage verwachtingen hebben van
de eindwaarde proberen ze de
vastgoedgerelateerde risico's te mitigeren
door lange huurcontracten te tekenen. Op
deze wijze verplaatsen ze het risico van
een lage eindwaarde naar risico's
gerelateerd aan de stabiliteit van de
huurder. Huurders zijn echter niet altijd
bereid lange huurcontracten te tekenen
waardoor beleggers in het verleden
teleurgesteld zijn geraakt in de snelheid en
het gemak waarmee valt te beleggen in
zorgvastgoed. Zorgvastgoed is een
kennisintensief vastgoedtype waarbij
beleggers zowel rekening moeten houden
met vastgoedgerelateerde risico's als
huurdergerelateerde risico's. Uit de
resultaten van dit onderzoek blijkt welke
risico's dit zijn.
R
Risk in Healthcare Real Estate Investment viii
Methode
Dit onderzoek is gedaan aan de hand van
een literatuuronderzoek en 22 interviews
met experts op het gebied van beleggen in
zorgvastgoed. Onder de experts bevonden
zich 11 vertegenwoordigers van
vastgoedbeleggingsmaatschappijen en
woningcorporaties, 7 adviseurs en 4
overige experts. Op basis van de literatuur
is een lijst van risicofactoren opgesteld. De
risicofactoren op deze lijst zijn door de
geïnterviewden aangevuld en beoordeeld
op belangrijkheid op een 7-puntsschaal van
1 (helemaal niet belangrijk) tot 7 (extreem
belangrijk).
Resultaten
De resultaten laten zien dat bij beleggen in
zorgvastgoed zowel vastgoedgerelateerde
als huurdergerelateerde risicofactoren een
rol spelen. Bijlage 1 laat een vergelijking
zien van de risicofactoren verkregen uit
een synthese van de risicofactoren die
gevonden zijn in de literatuur en de
uiteindelijk lijst met risicofactoren uit dit
onderzoek. De vergelijking laat zien dat
vele risicofactoren niet genoemd zijn in de
literatuur. Vooral risicofactoren gerelateerd
aan de stabiliteit van de huurder komen
vrijwel niet voor in de bestaande literatuur.
Onder vastgoedgerelateerde risicofactoren
worden op hoofdniveau verstaan:
1.1 Volwassenheid van de assetmarkt;
1.2 Technische en functionele staat van
het object;
1.3 Fysieke locatie;
1.4 Veranderingen op de (lokale)
ruimtemarkt en;
1.5 Alternatieve aanwendbaarheid.
De huurdergerelateerde risicofactoren zijn
op hoofdniveau:
2.1 De verhouding tussen inkomsten
van de huurder gegenereerd in het
object en de huur van het object
(coverage ratio);
2.2 Invloed van veranderingen in
overheidsbeleid op huurder;
2.3 Kredietwaardigheid van de huurder;
2.4 Kwaliteit van het management van
de huurder;
2.5 Toekomstvisie van de huurder;
2.6 Concurrentie van andere
zorgverleners en;
2.7 Type contract.
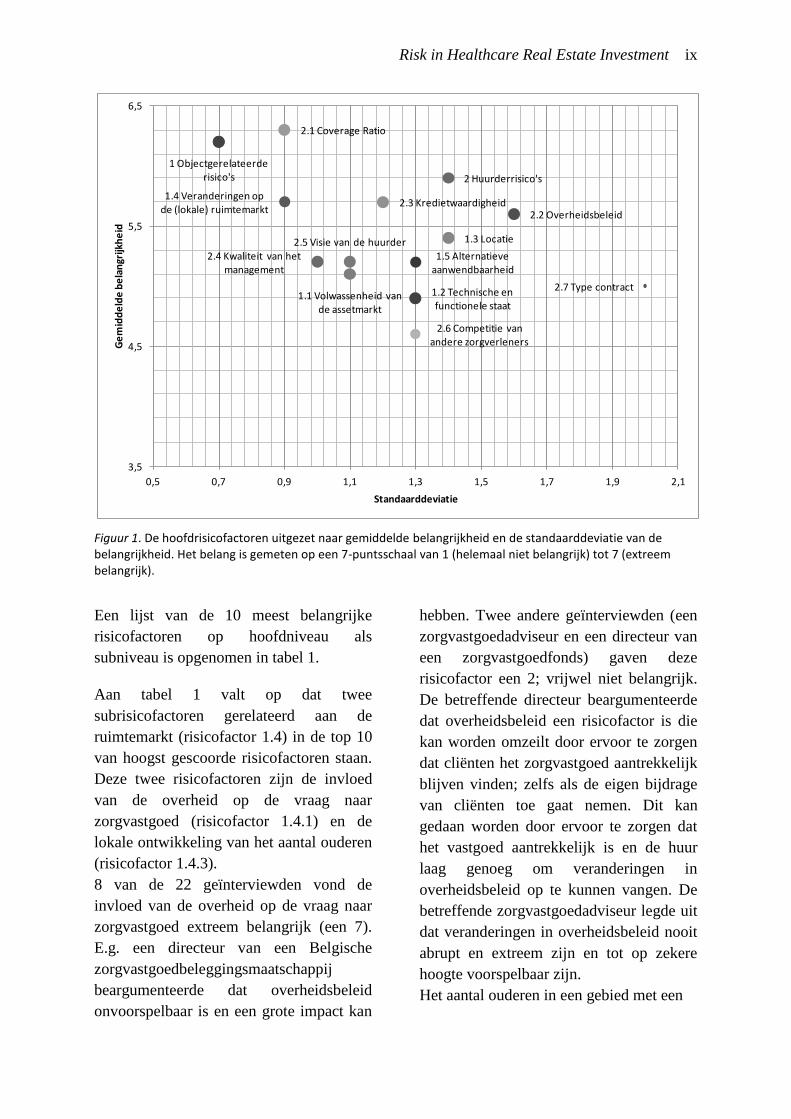
De mate van belangrijkheid van deze
risicofactoren is weergegeven in figuur 1.
In dit figuur is de gemiddelde score van de
risicofactoren uitgezet tegenover de
standaarddeviatie. Aan figuur 1 is te zien
dat de geïnterviewden het met elkaar eens
waren over dat objectgerelateerde risico's
(risicofactor 1) zeer belangrijk zijn terwijl
er meer onenigheid is over het belang van
huurdergerelateerde risico's (risicofactor
2). Verder valt op dat de coverage ratio
(risicofactor 2.1) gemiddeld het
belangrijkst wordt gevonden. Een directeur
van een Belgische zorgvastgoed-
beleggingsmaatschappij legde uit waarom
hij een hoge score gaf aan deze
risicofactor. Door het aanpassen van het
huurniveau aan het inkomen van de
huurder kan een groot deel van het
huurderrisico worden verminderd. Hij
voegde eraan toe dat het inkomen van
zorginstellingen sterk afhankelijk is van
overheidregulering, waardoor de meeste
zorginstellingen vrijwel hetzelfde
maximale inkomen kunnen genereren. Om
deze reden vrijwel alle geïnterviewden de
coverage ratio erg belangrijk.
Risk in Healthcare Real Estate Investment ix
Figuur 1. De hoofdrisicofactoren uitgezet naar gemiddelde belangrijkheid en de standaarddeviatie van de belangrijkheid. Het belang is gemeten op een 7-puntsschaal van 1 (helemaal niet belangrijk) tot 7 (extreem belangrijk).
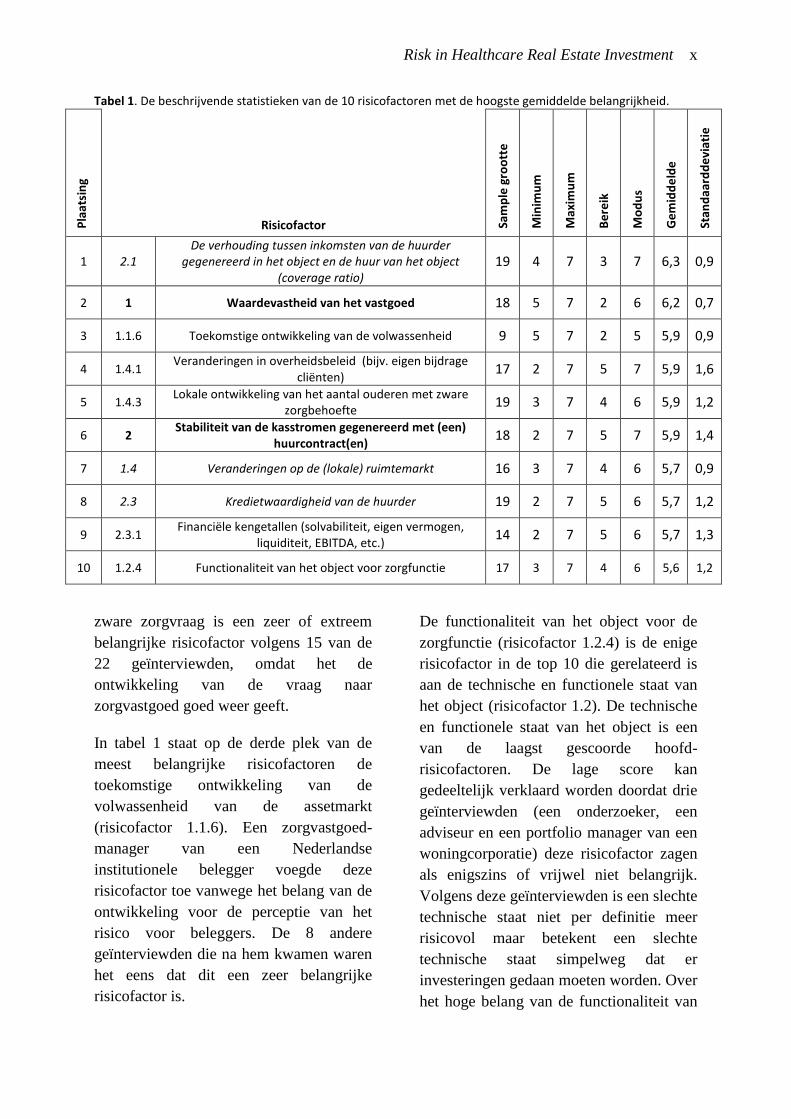
Een lijst van de 10 meest belangrijke
risicofactoren op hoofdniveau als
subniveau is opgenomen in tabel 1.
Aan tabel 1 valt op dat twee
subrisicofactoren gerelateerd aan de
ruimtemarkt (risicofactor 1.4) in de top 10
van hoogst gescoorde risicofactoren staan.
Deze twee risicofactoren zijn de invloed
van de overheid op de vraag naar
zorgvastgoed (risicofactor 1.4.1) en de
lokale ontwikkeling van het aantal ouderen
(risicofactor 1.4.3).
8 van de 22 geïnterviewden vond de
invloed van de overheid op de vraag naar
zorgvastgoed extreem belangrijk (een 7).
E.g. een directeur van een Belgische
zorgvastgoedbeleggingsmaatschappij
beargumenteerde dat overheidsbeleid
onvoorspelbaar is en een grote impact kan
hebben. Twee andere geïnterviewden (een
zorgvastgoedadviseur en een directeur van
een zorgvastgoedfonds) gaven deze
risicofactor een 2; vrijwel niet belangrijk.
De betreffende directeur beargumenteerde
dat overheidsbeleid een risicofactor is die
kan worden omzeilt door ervoor te zorgen
dat cliënten het zorgvastgoed aantrekkelijk
blijven vinden; zelfs als de eigen bijdrage
van cliënten toe gaat nemen. Dit kan
gedaan worden door ervoor te zorgen dat
het vastgoed aantrekkelijk is en de huur
laag genoeg om veranderingen in
overheidsbeleid op te kunnen vangen. De
betreffende zorgvastgoedadviseur legde uit
dat veranderingen in overheidsbeleid nooit
abrupt en extreem zijn en tot op zekere
hoogte voorspelbaar zijn.
Het aantal ouderen in een gebied met een
1 Objectgerelateerde risico's
1.1 Volwassenheid van de assetmarkt
1.2 Technische en functionele staat
1.3 Locatie
1.4 Veranderingen op de (lokale) ruimtemarkt
1.5 Alternatieve aanwendbaarheid
2 Huurderrisico's
2.1 Coverage Ratio
2.2 Overheidsbeleid2.3 Kredietwaardigheid
2.4 Kwaliteit van het management
2.5 Visie van de huurder
2.6 Competitie van andere zorgverleners
2.7 Type contract
3,5
4,5
5,5
6,5
0,5 0,7 0,9 1,1 1,3 1,5 1,7 1,9 2,1
Ge
mid
de
lde
be
lan
grijk
he
id
Standaarddeviatie
Risk in Healthcare Real Estate Investment x
Tabel 1. De beschrijvende statistieken van de 10 risicofactoren met de hoogste gemiddelde belangrijkheid.
Pla
atsi
ng
Risicofactor
Sam
ple
gro
ott
e
Min
imu
m
Max
imu
m
Be
reik
Mo
du
s
Ge
mid
de
lde
Stan
daa
rdd
evi
atie
1 2.1 De verhouding tussen inkomsten van de huurder
gegenereerd in het object en de huur van het object (coverage ratio)
19 4 7 3 7 6,3 0,9
2 1 Waardevastheid van het vastgoed 18 5 7 2 6 6,2 0,7
3 1.1.6 Toekomstige ontwikkeling van de volwassenheid 9 5 7 2 5 5,9 0,9
4 1.4.1 Veranderingen in overheidsbeleid (bijv. eigen bijdrage
cliënten) 17 2 7 5 7 5,9 1,6
5 1.4.3 Lokale ontwikkeling van het aantal ouderen met zware
zorgbehoefte 19 3 7 4 6 5,9 1,2
6 2 Stabiliteit van de kasstromen gegenereerd met (een)
huurcontract(en) 18 2 7 5 7 5,9 1,4
7 1.4 Veranderingen op de (lokale) ruimtemarkt 16 3 7 4 6 5,7 0,9
8 2.3 Kredietwaardigheid van de huurder 19 2 7 5 6 5,7 1,2
9 2.3.1 Financiële kengetallen (solvabiliteit, eigen vermogen,
liquiditeit, EBITDA, etc.) 14 2 7 5 6 5,7 1,3
10 1.2.4 Functionaliteit van het object voor zorgfunctie 17 3 7 4 6 5,6 1,2
zware zorgvraag is een zeer of extreem
belangrijke risicofactor volgens 15 van de
22 geïnterviewden, omdat het de
ontwikkeling van de vraag naar
zorgvastgoed goed weer geeft.
In tabel 1 staat op de derde plek van de
meest belangrijke risicofactoren de
toekomstige ontwikkeling van de
volwassenheid van de assetmarkt
(risicofactor 1.1.6). Een zorgvastgoed-
manager van een Nederlandse
institutionele belegger voegde deze
risicofactor toe vanwege het belang van de
ontwikkeling voor de perceptie van het
risico voor beleggers. De 8 andere
geïnterviewden die na hem kwamen waren
het eens dat dit een zeer belangrijke
risicofactor is.
De functionaliteit van het object voor de
zorgfunctie (risicofactor 1.2.4) is de enige
risicofactor in de top 10 die gerelateerd is
aan de technische en functionele staat van
het object (risicofactor 1.2). De technische
en functionele staat van het object is een
van de laagst gescoorde hoofd-
risicofactoren. De lage score kan
gedeeltelijk verklaard worden doordat drie
geïnterviewden (een onderzoeker, een
adviseur en een portfolio manager van een
woningcorporatie) deze risicofactor zagen
als enigszins of vrijwel niet belangrijk.
Volgens deze geïnterviewden is een slechte
technische staat niet per definitie meer
risicovol maar betekent een slechte
technische staat simpelweg dat er
investeringen gedaan moeten worden. Over
het hoge belang van de functionaliteit van
Risk in Healthcare Real Estate Investment xi
het object was meer consensus onder de
geïnterviewden.
De enige subrisicofactor die in de top 10
staat, en gerelateerd is aan de
huurderrisico, is de financiële kengetallen
van een huurder (risicofactor 2.3.1).
Financiële kengetallen tonen de
kredietwaardigheid van een huurder
(risicofactor 2.3) die door veel
geïnterviewden belangrijk wordt
gevonden. Een kredietwaardige huurder
betekent minder risico dat de huurder
vroegtijdig het contract moet opzeggen
vanwege een faillissement. Een
zorgvastgoedadviseur waarschuwde dat,
ook al is het analyseren van de
kredietwaardigheid een goede manier om
contractrisico te mitigeren, de
kredietwaardigheid van de zorginstelling
snel kan dalen als de zorginstelling slecht
management heeft of een slechte visie
heeft.
Verschillende zienswijzen beleggers
Tijdens de interviews werd het duidelijk
dat er twee verschillende manieren zijn om
naar beleggen in zorgvastgoed te kijken.
Sommige beleggers hebben de neiging om
risico te beheersen door zich te richten op
het risico van een instabiele huurder.
Andere beleggers proberen risico te
verminderen door alleen in objecten te
beleggen met een lage kans op
waardevermindering, zelfs als de huurder
failliet zou gaan. Het eerste perspectief
heeft overeenkomsten met
bedrijfsfinanciering, terwijl de het tweede
perspectief typerend is voor
vastgoedbeleggers.
Invloed van lengte huurcontract
De meest gebruikelijke lengte van
huurcontracten bij zorgvastgoed is 15 jaar.
Wanneer men korte huurcontracten
gebruikt van 10 jaar zijn objectgerelateerde
risico's belangrijker terwijl huurderrisico's
belangrijker zijn als men huurcontracten
gebruikt van langer dan 20 jaar. Markten
met kortere huurcontracten zijn meer
geschikt voor beleggers die zich richten op
objectgerelateerde risico's terwijl markten
met lange huurcontracten meer geschikt
zijn voor beleggers die zich richten op
huurderrisico's. Omdat zorginstellingen
niet altijd bereid zijn om lange
huurcontracten te tekenen kunnen zij een
verschuiving laten plaatsen waarbij
beleggers steeds meer aandacht besteden
aan objectgerelateerde risicofactoren in
plaats van huurdergerelateerde
risicofactoren.
Onzekerheid over het risico
De onderzoeksresultaten laten zien dat er
nog onzekerheid is over de mate van risico
bij beleggen in zorgvastgoed. De
risicofactoren hebben een
standaarddeviatie tussen de 0,7 en 2,0. Dit
suggereert dat meningen van experts over
de belangrijkheid van de risicofactoren
uiteen lopen. De gemiddelde score van 4,9
laat zien dat risicofactoren asymmetrisch
zijn gescoord. Een mogelijke verklaring
hiervoor zou kunnen zijn dat
geïnterviewden bij twijfel risicofactoren
belangrijker inschatten.
Conclusies
De bevindingen van dit onderzoek zijn van
toegevoegde waarde voor de bestaande
literatuur op een aantal manieren. Dit
onderzoek laat zien dat, naast macro-
economische risicofactoren, er ook
risicofactoren zijn op microniveau die de
risicoperceptie van beleggers beïnvloeden.
Het laat zien dat er verschillen zijn in
risicoperceptie tussen beleggers en dat er

Risk in Healthcare Real Estate Investment xii
verschillende manieren zijn om beleggen
in zorgvastgoed te benaderen. Bovendien
legt het de onzekerheden bloot die er zijn
bij beleggen in zorgvastgoed en toont dat
onzekerheid een rol speelt bij de
risicoperceptie bij beleggen in
zorgvastgoed.
De resultaten geven beleggers, taxateurs en
onderzoekers input voor een betere
benadering van risico. De risicofactoren en
hun belang kunnen gebruikt worden bij
beleggingsbeslissingen en bij het maken
van betere waardebepalingen. Door de
risicofactoren en hun belang in kaart te
brengen draagt dit onderzoek ook bij aan
de transparantie en volwassenheid van
zorgvastgoedmarkt.
Discussie
Dit onderzoek heeft enkele beperkingen.
Zo kunnen vraagtekens worden gezet bij
de onderzoeksmethode die heeft geleid tot
een te groot aantal risicofactoren. Een
selectie van de meest belangrijke
risicofactoren kunnen in
vervolgonderzoeken worden gebruikt om
het risico bij beleggen in zorgvastgoed
nader te bepalen. Ondanks deze
beperkingen heeft het onderzoek de kennis
over de risico's bij beleggen in
zorgvastgoed uitgebreid. Dit onderzoek is
het eerste kwalitatieve onderzoek naar
Nederlands zorgvastgoed dat zich volledig
richt op de risico's. Het biedt beleggers
nieuwe kennis die ze kunnen
implementeren in hun beslissingsproces en
geeft inzicht in de verschillende
zienswijzen van beleggers.
Bronnen
Dale, D., Wolf, R., & Yang, H.F. (2015).
An assessment of the risk and return of
residential real estate. Managerial
Finance, 41(6), 591 - 599.
Ho, D.K.H., & Addae-Dapaah, K. (2015).
International Direct Real Estate Risk
Premiums in a Multi-Factor Estimation
Model. Journal of Real Estate Financial
Economics, 52–85.
McDonald, J.F., & & Dermisi, S. (2009).
Office building capitalization rates: the
case of downtown Chicago. The Journal
of Real Estate Finance and Economics,
39(4), 472-485.
Sivitanidou, R.C., & Sivitanides, P.S.
(1999). Office Capitalization Rates: Real
Estate and Capital Market Influences.
Journal of Real Estate Finance and
Economics, (18)3, 297-322.
Wheaton, W.C., Torto, R.G., Sivitanides,
P.S., Southard, J.A., Hopkins, R.E., &
Costello, J.M. (2001). Real estate risk: a
forward-looking approach. Real Estate
Finance, 18(3), 20-28.
Risk in Healthcare Real Estate Investment xiii
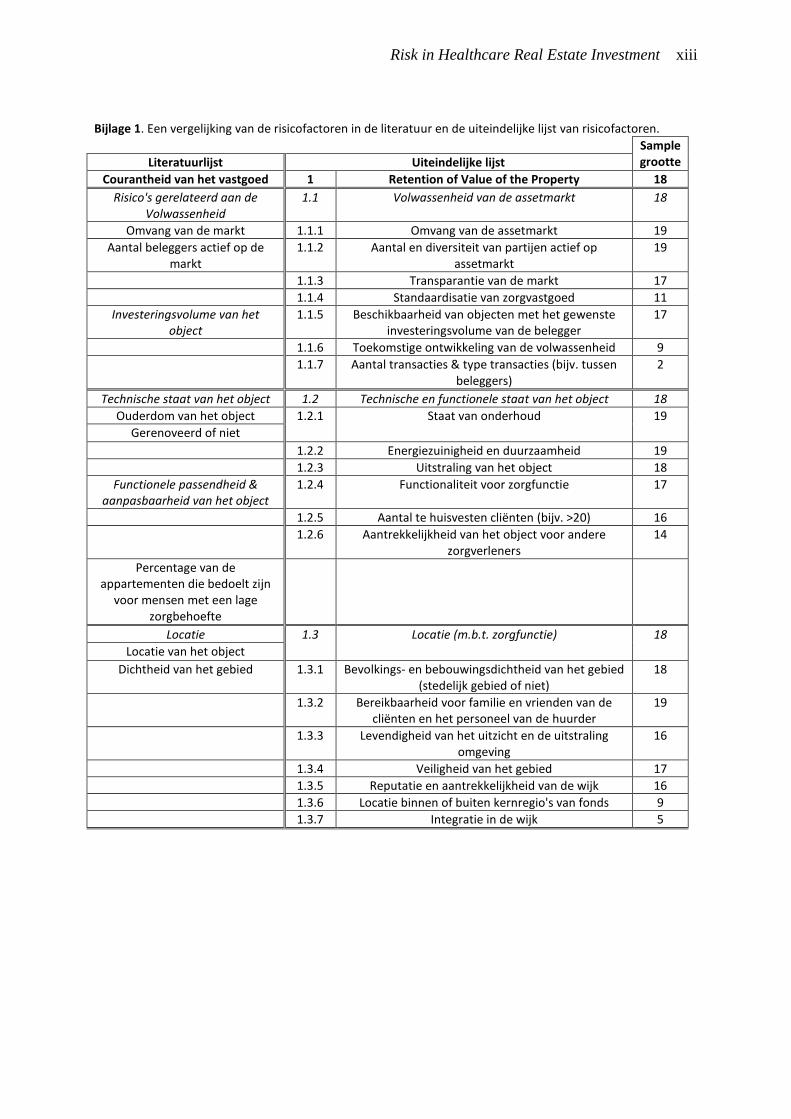
Bijlage 1. Een vergelijking van de risicofactoren in de literatuur en de uiteindelijke lijst van risicofactoren.
Sample grootte Literatuurlijst Uiteindelijke lijst
Courantheid van het vastgoed 1 Retention of Value of the Property 18
Risico's gerelateerd aan de Volwassenheid
1.1 Volwassenheid van de assetmarkt 18
Omvang van de markt 1.1.1 Omvang van de assetmarkt 19
Aantal beleggers actief op de markt
1.1.2 Aantal en diversiteit van partijen actief op assetmarkt
19
1.1.3 Transparantie van de markt 17
1.1.4 Standaardisatie van zorgvastgoed 11
Investeringsvolume van het object
1.1.5 Beschikbaarheid van objecten met het gewenste investeringsvolume van de belegger
17
1.1.6 Toekomstige ontwikkeling van de volwassenheid 9
1.1.7 Aantal transacties & type transacties (bijv. tussen beleggers)
2
Technische staat van het object 1.2 Technische en functionele staat van het object 18
Ouderdom van het object 1.2.1 Staat van onderhoud
19
Gerenoveerd of niet
1.2.2 Energiezuinigheid en duurzaamheid 19
1.2.3 Uitstraling van het object 18
Functionele passendheid & aanpasbaarheid van het object
1.2.4 Functionaliteit voor zorgfunctie 17
1.2.5 Aantal te huisvesten cliënten (bijv. >20) 16
1.2.6 Aantrekkelijkheid van het object voor andere zorgverleners
14
Percentage van de appartementen die bedoelt zijn
voor mensen met een lage zorgbehoefte
Locatie 1.3 Locatie (m.b.t. zorgfunctie)
18
Locatie van het object
Dichtheid van het gebied 1.3.1 Bevolkings- en bebouwingsdichtheid van het gebied (stedelijk gebied of niet)
18
1.3.2 Bereikbaarheid voor familie en vrienden van de cliënten en het personeel van de huurder
19
1.3.3 Levendigheid van het uitzicht en de uitstraling omgeving
16
1.3.4 Veiligheid van het gebied 17
1.3.5 Reputatie en aantrekkelijkheid van de wijk 16
1.3.6 Locatie binnen of buiten kernregio's van fonds 9
1.3.7 Integratie in de wijk 5

Risk in Healthcare Real Estate Investment xiv
Bijlage 1 (vervolg). Een vergelijking van de risicofactoren in de literatuur en de uiteindelijke lijst van risicofactoren.
Veranderingen op de ruimtemarkt
1.4 Veranderingen op de (lokale) ruimtemarkt 16
1.4.1 Veranderingen in overheidsbeleid (bijv. eigen bijdrage cliënten)
17
1.4.2 Medische ontwikkeling die invloed hebben op vraag 16
Aantal ouderen met zware zorgbehoefte
1.4.3 Lokale ontwikkeling van het aantal ouderen met zware zorgbehoefte
19
1.4.4 Uitstellen van moment van uit eigen huis gaan van cliënten
6
1.4.5 Vraag van andere zorgverleners op de huurmarkt 17
1.4.6 Kwalitatieve verandering in vraagbehoefte 17
1.4.7 De lengte van de wachtlijsten 19
Huurniveaus 1.4.8 Huurniveaus van concurrerend aanbod 17
Aanbod aan nieuwe ruimte 1.4.9 Concurrerend (nieuw) ruimteaanbod in omgeving 19
Leegstandspercentage 1.4.10 Leegstandspercentages van concurrerend zorgvastgoed
19
Mate van absorptie van ruimte
1.5 Alternatieve aanwendbaarheid (andere functie) 16
1.5.1 Lokale ontwikkeling van vraag en aanbod alternatieve functies (bijv. ontwikkeling lokale
woningmarkt)
17
1.5.2 Waarde van alternatieve aanwending (rendementsterugval)
9
1.5.2.1 Bouwtechnische flexibiliteit en passendheid voor alternatieve functie (o.a. percentage algemene
ruimtes)
17
1.5.2.2 Nabijheid van voorzieningen voor alternatieve functie
18
1.5.2.3 Veranderende bouwbesluit-eisen bij alternatieve functie
12
1.5.2.4 Bestemmingsbeleid gemeente (bijv. woonbestemming)
14
1.5.2.5 Voldoende parkeerplaatsen 17
Betrouwbaarheid van de huurder
2 Stabiliteit van de kasstromen gegenereerd met (een) huurcontract(en)
18
De verhouding tussen de inkomsten van de huurder en de
huur
2.1 De verhouding tussen inkomsten van de huurder gegenereerd in het object en de huur van het object
(coverage ratio)
19
Veranderingen in overheidsbeleid 2.2 Invloed van veranderingen in overheidsbeleid op huurder
19
2.2.1 Gevoeligheid van huurder voor beleidsveranderingen op nationaal- en
gemeenteniveau
17
2.2.2 Verhouding huur en de maximale huur op basis van het woningwaarderingsstelsel bij Scheiden Wonen
Zorg
14
2.2.3 Ontwikkeling van het beleid van zorgkantoren/zorgverzekeraars (bijv. toekenning
capaciteit)
14
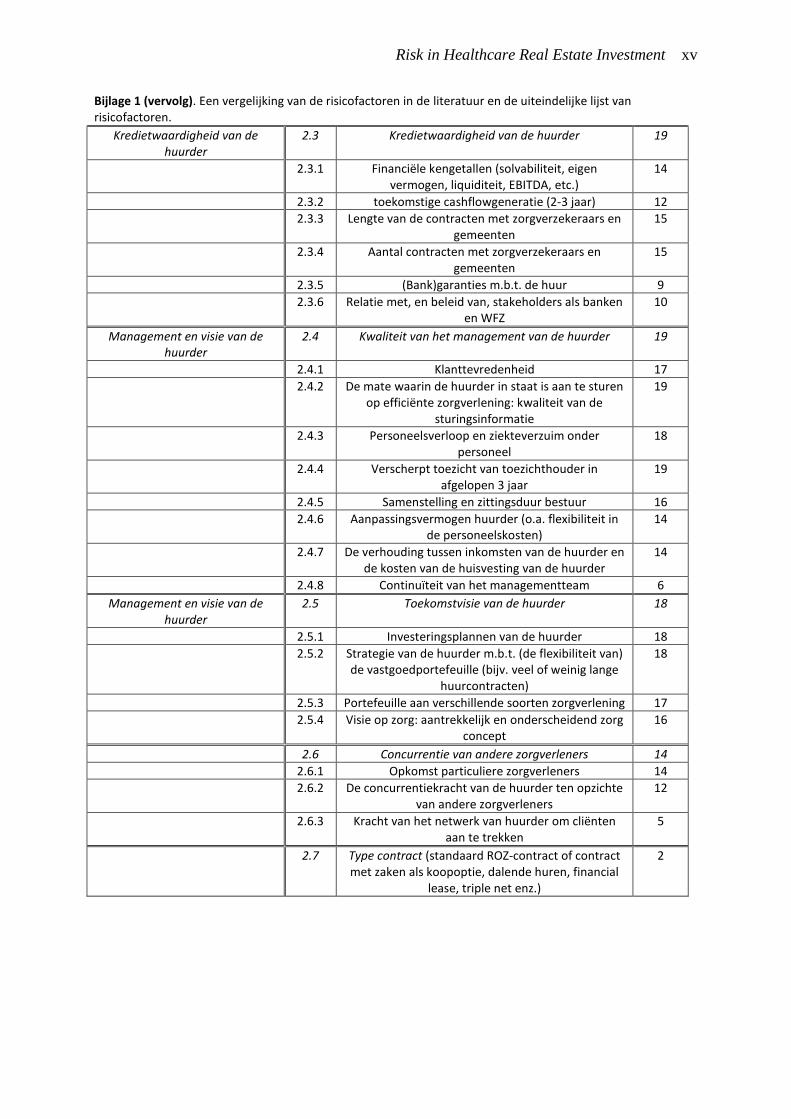
Risk in Healthcare Real Estate Investment xv
Bijlage 1 (vervolg). Een vergelijking van de risicofactoren in de literatuur en de uiteindelijke lijst van risicofactoren.
Kredietwaardigheid van de huurder
2.3 Kredietwaardigheid van de huurder 19
2.3.1 Financiële kengetallen (solvabiliteit, eigen vermogen, liquiditeit, EBITDA, etc.)
14
2.3.2 toekomstige cashflowgeneratie (2-3 jaar) 12
2.3.3 Lengte van de contracten met zorgverzekeraars en gemeenten
15
2.3.4 Aantal contracten met zorgverzekeraars en gemeenten
15
2.3.5 (Bank)garanties m.b.t. de huur 9
2.3.6 Relatie met, en beleid van, stakeholders als banken en WFZ
10
Management en visie van de huurder
2.4 Kwaliteit van het management van de huurder 19
2.4.1 Klanttevredenheid 17
2.4.2 De mate waarin de huurder in staat is aan te sturen op efficiënte zorgverlening: kwaliteit van de
sturingsinformatie
19
2.4.3 Personeelsverloop en ziekteverzuim onder personeel
18
2.4.4 Verscherpt toezicht van toezichthouder in afgelopen 3 jaar
19
2.4.5 Samenstelling en zittingsduur bestuur 16
2.4.6 Aanpassingsvermogen huurder (o.a. flexibiliteit in de personeelskosten)
14
2.4.7 De verhouding tussen inkomsten van de huurder en de kosten van de huisvesting van de huurder
14
2.4.8 Continuïteit van het managementteam 6
Management en visie van de huurder
2.5 Toekomstvisie van de huurder 18
2.5.1 Investeringsplannen van de huurder 18
2.5.2 Strategie van de huurder m.b.t. (de flexibiliteit van) de vastgoedportefeuille (bijv. veel of weinig lange
huurcontracten)
18
2.5.3 Portefeuille aan verschillende soorten zorgverlening 17
2.5.4 Visie op zorg: aantrekkelijk en onderscheidend zorg concept
16
2.6 Concurrentie van andere zorgverleners 14
2.6.1 Opkomst particuliere zorgverleners 14
2.6.2 De concurrentiekracht van de huurder ten opzichte van andere zorgverleners
12
2.6.3 Kracht van het netwerk van huurder om cliënten aan te trekken
5
2.7 Type contract (standaard ROZ-contract of contract met zaken als koopoptie, dalende huren, financial
lease, triple net enz.)
2

Risk in Healthcare Real Estate Investment xvi

Risk in Healthcare Real Estate Investment xvii
Risk in Healthcare Real Estate Investment
More insight into the risk from the perspective of investors
Healthcare real estate is an emerging investment category in The Netherlands. It is
appreciated as a real estate category for its stable cash flows, high returns and strong
demographic drivers. Despite the growing interest in healthcare real estate the healthcare
real estate market is still immature. Because of the uncertainty surrounding the risk of
healthcare real estate investment many investors are still reluctant to step into this market.
There is a growing need to map out the risks involved with investing in healthcare real
estate.
By ing. Tjeerd Kosse
isk in real estate investing has
been subject of many quantitative
studies. Recent examples are
studies in which multifactor models are
being used such as those by Dale, Wolf &
Yang (2015) en Ho & Addae-Dapaah
(2015). Moreover, there were many studies
on the determinants of the cap rate,
amongst others by Sivitanidou &
Sivitanides (1999) and Wheaton et al.
(2001). There have also been studies at
micro-level on the determinants of the cap
rate. One of these studies is a study by
McDonald & Dermisi (2009). Wheaton et
al. conclude that the cap rate is strong
related to uncertainty on the measure of
risk. Because there are yet no studies on
the risk of healthcare real estate investment
there is still uncertainty on the risk. This
study offers a quantitative view into the
risk of investing in healthcare real estate.
The Current Practice
In current practice investing in healthcare
real estate is coupled with little trust in the
development of the exit value of the
property. Because investors have low
expectations on the exit value they try to
mitigate the property related risks by
signing long-term rental contracts. In this
way they shift the risk of a low exit value
to risks related to the stability of the tenant.
Tenants are, however, not always willing
to sign long-term rental contracts which
has caused some disappointment amongst
investors in the speed and ease of investing
in healthcare real estate. Healthcare real
estate is knowledge intensive and investors
need to take into account both property as
tenant related risks. The results of this
study show which risks to take into
account.
R

Risk in Healthcare Real Estate Investment xviii
Method
This study is based on a literature review
and 22 interviews with experts on
investing in healthcare real estate. Among
the experts were 11 representatives of
(non-profit) real estate investment
companies, 7 consultants and 4 other
experts. On the basis of the literature a list
of risk factors was composed. Interviewees
completed this list with additional risk
factors and rated the risk factors on
importance on a 7-point scale from 1 (not
at all important) to 7 (extremely
important).
Results
The results show that in healthcare real
estate investment both property and tenant
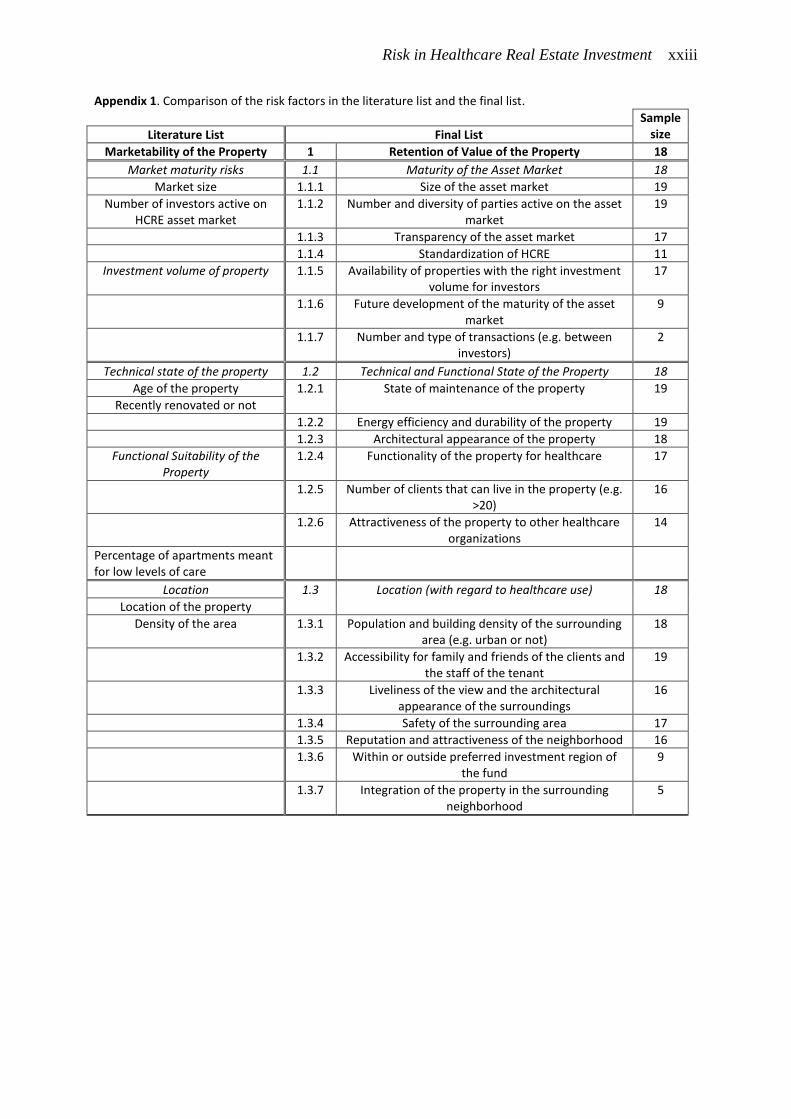
related risk factors play a role. Appendix 1
shows a comparison of the risk factors
obtained from a synthesis of the risk
factors found in a literature review with the
final list of risk factors found in this study.
The comparison shows that many risk
factors were not mentioned in the
literature. Especially risk factors related to
the reliability of the tenant are missing in
the existing literature.
The main risk factors related to property
are:
1.1 Maturity of the Asset Market;
1.2 Technical and Functional State of
the Property;
1.3 The Physical Location;
1.4 Local Space Market Changes and;
1.5 Alternative Use.
The tenant related risk factors are at main
level:
2.1 The Ratio between Income
Generated by the Tenant in the Property
and the Rent of the Property (Coverage
Ratio);
2.2 Influence of the Government on the
Stability of the Tenant;
2.3 Creditworthiness of the Tenant;
2.4 Quality of the Management of the
Tenant;
2.5 Vision of the Tenant;
2.6 Competition by Other Healthcare
Organizations and;
2.7 Type of Contract.
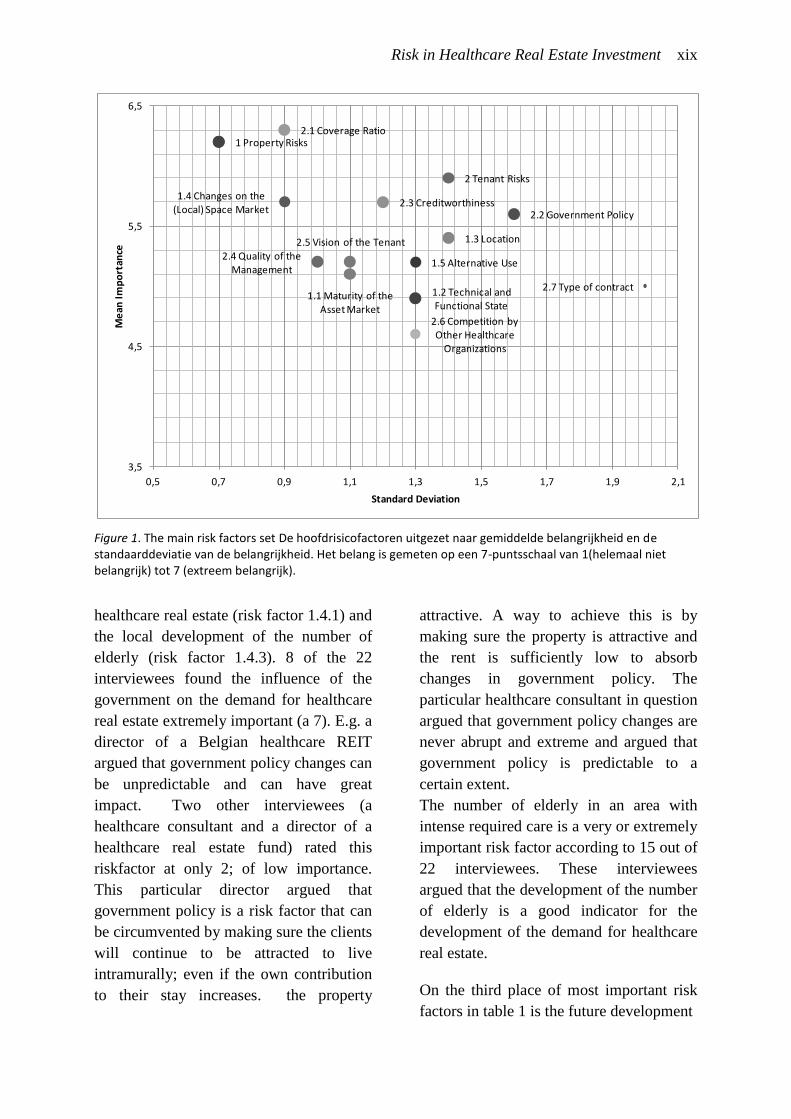
The importance of these risk factors are
shown in figure 1. In this figure the
average rating is set out against the
standard deviation. Figure 1 shows that
interviewees agreed that property related
risks (risk factor 1) are very important
while there is less consensus over the
importance of tenant related risks (risk
factor 2). It is noticeable that the coverage
ratio (risk factor 2.1) was found most
important on average. A director of a
Belgian healthcare REIT explained why he
gave a high rating to this risk factor. By
adjusting the rent level to the income of the
tenant a large part of the tenant risk can be
reduced. He added that the income of
healthcare organizations is strongly
dependent on government regulation so
that most healthcare organizations generate
roughly the same maximum income. For
this reasons most interviewees found this
risk factor very important.
A list of the 10 most important risk factors
at main level and sub level is shown in
table 1.
Table 1 shows that two sub-risk factors
related to the space market (risk factor 1.4)
are in the top 1 of highest rated risk
factors. These two risks are the influence
of the government on the demand for
Risk in Healthcare Real Estate Investment xix
Figure 1. The main risk factors set De hoofdrisicofactoren uitgezet naar gemiddelde belangrijkheid en de standaarddeviatie van de belangrijkheid. Het belang is gemeten op een 7-puntsschaal van 1(helemaal niet belangrijk) tot 7 (extreem belangrijk).
healthcare real estate (risk factor 1.4.1) and
the local development of the number of
elderly (risk factor 1.4.3). 8 of the 22
interviewees found the influence of the
government on the demand for healthcare
real estate extremely important (a 7). E.g. a
director of a Belgian healthcare REIT
argued that government policy changes can
be unpredictable and can have great
impact. Two other interviewees (a
healthcare consultant and a director of a
healthcare real estate fund) rated this
riskfactor at only 2; of low importance.
This particular director argued that
government policy is a risk factor that can
be circumvented by making sure the clients
will continue to be attracted to live
intramurally; even if the own contribution
to their stay increases. the property
attractive. A way to achieve this is by
making sure the property is attractive and
the rent is sufficiently low to absorb
changes in government policy. The
particular healthcare consultant in question
argued that government policy changes are
never abrupt and extreme and argued that
government policy is predictable to a
certain extent.
The number of elderly in an area with
intense required care is a very or extremely
important risk factor according to 15 out of
22 interviewees. These interviewees
argued that the development of the number
of elderly is a good indicator for the
development of the demand for healthcare
real estate.
On the third place of most important risk
factors in table 1 is the future development
1 Property Risks
1.1 Maturity of the Asset Market
1.2 Technical and Functional State
1.3 Location
1.4 Changes on the (Local) Space Market
1.5 Alternative Use
2 Tenant Risks
2.1 Coverage Ratio
2.2 Government Policy 2.3 Creditworthiness
2.4 Quality of the Management
2.5 Vision of the Tenant
2.6 Competition by Other Healthcare
Organizations
2.7 Type of contract
3,5
4,5
5,5
6,5
0,5 0,7 0,9 1,1 1,3 1,5 1,7 1,9 2,1
Me
an I
mp
ort
ance
Standard Deviation
Risk in Healthcare Real Estate Investment xx
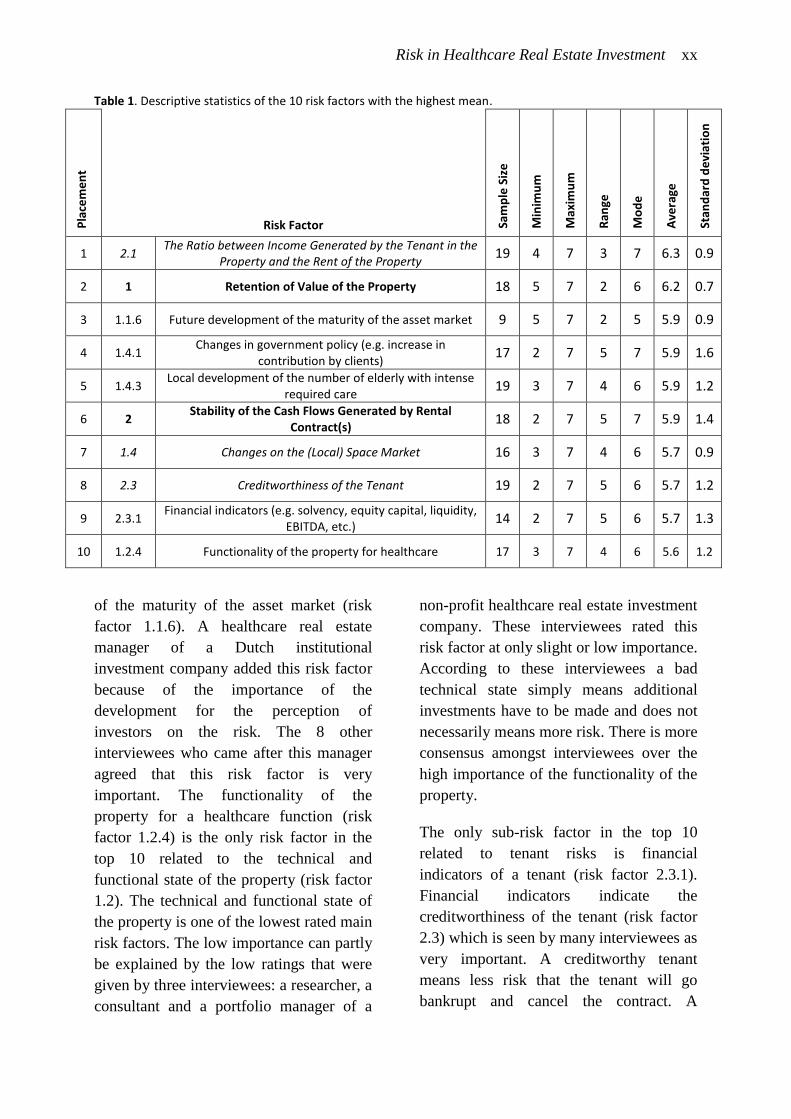
Table 1. Descriptive statistics of the 10 risk factors with the highest mean.
Pla
cem
en
t
Risk Factor
Sam
ple
Siz
e
Min
imu
m
Max
imu
m
Ran
ge
Mo
de
Ave
rage
Stan
dar
d d
evi
atio
n
1 2.1 The Ratio between Income Generated by the Tenant in the
Property and the Rent of the Property 19 4 7 3 7 6.3 0.9
2 1 Retention of Value of the Property 18 5 7 2 6 6.2 0.7
3 1.1.6 Future development of the maturity of the asset market 9 5 7 2 5 5.9 0.9
4 1.4.1 Changes in government policy (e.g. increase in
contribution by clients) 17 2 7 5 7 5.9 1.6
5 1.4.3 Local development of the number of elderly with intense
required care 19 3 7 4 6 5.9 1.2
6 2 Stability of the Cash Flows Generated by Rental
Contract(s) 18 2 7 5 7 5.9 1.4
7 1.4 Changes on the (Local) Space Market 16 3 7 4 6 5.7 0.9
8 2.3 Creditworthiness of the Tenant 19 2 7 5 6 5.7 1.2
9 2.3.1 Financial indicators (e.g. solvency, equity capital, liquidity,
EBITDA, etc.) 14 2 7 5 6 5.7 1.3
10 1.2.4 Functionality of the property for healthcare 17 3 7 4 6 5.6 1.2
of the maturity of the asset market (risk
factor 1.1.6). A healthcare real estate
manager of a Dutch institutional
investment company added this risk factor
because of the importance of the
development for the perception of
investors on the risk. The 8 other
interviewees who came after this manager
agreed that this risk factor is very
important. The functionality of the
property for a healthcare function (risk
factor 1.2.4) is the only risk factor in the
top 10 related to the technical and
functional state of the property (risk factor
1.2). The technical and functional state of
the property is one of the lowest rated main
risk factors. The low importance can partly
be explained by the low ratings that were
given by three interviewees: a researcher, a
consultant and a portfolio manager of a
non-profit healthcare real estate investment
company. These interviewees rated this
risk factor at only slight or low importance.
According to these interviewees a bad
technical state simply means additional
investments have to be made and does not
necessarily means more risk. There is more
consensus amongst interviewees over the
high importance of the functionality of the
property.
The only sub-risk factor in the top 10
related to tenant risks is financial
indicators of a tenant (risk factor 2.3.1).
Financial indicators indicate the
creditworthiness of the tenant (risk factor
2.3) which is seen by many interviewees as
very important. A creditworthy tenant
means less risk that the tenant will go
bankrupt and cancel the contract. A

Risk in Healthcare Real Estate Investment xxi
healthcare real estate consultant warned
that, although taking into account the
creditworthiness of the tenant is an
excellent way to mitigate contract risk, the
creditworthiness of a tenant can decline
rapidly if the healthcare organization has
bad management or a bad vision.
Different Points of View
During the interviewees it became evident
that there are two different points of view
on healthcare real estate investment. Some
investors have a tendency to manage risk
by focusing on the risk of an instable
tenant. Other investors try to reduce risk by
investing solely in properties with a low
chance of depreciation, even if the tenant
would go bankrupt. The first perspective
has similarities with corporate investment
while the second perspective is typical for
real estate investors.
Influence of the Length of Contracts
The most usual length of rental contracts is
15 years. When using short contracts of 10
years property related risk become more
important while tenant risks are more
important when using rental contracts
longer than 20 years. Markets with shorter
rental contracts are more suitable for
investors who focus on property related
risks factors while markets with longer
rental contracts are more suitable for
investors who focus on tenant risks.
Because healthcare organizations are not
always willing to sign long-term contracts
a shift can take place in which investors
are forced to focus more on property risks
instead of tenant risks.
Uncertainty over the Risk
The results show that there is still
uncertainty over the level of risk in
healthcare real estate investment. The risk
factors have a large standard deviation
between 0.7 and 2.0. This suggests that
opinions differ on the importance of the
risk factors. The average rating of 4.9
shows that the risk factors were rated
asymmetrically. A possible explanation is
that interviewees rated risk factors of
higher importance when in doubt.
Conclusions
The findings of this study are of added
value to the existing literature in a number
of ways. This study shows that, besides
macro-economic risk factors, there are
numerous risk factors at micro level that
influence the risk perception of investors.
It shows that there are differences in the
risk perception of investors and that there
are different ways to approach healthcare
real estate investment. Moreover, it
uncovers the uncertainties there are
surrounding healthcare real estate
investment and shows that uncertainty
places a role in risk perception in
healthcare real estate investment.
The results give investors, appraisers and
researchers input for a better
approximation for risk. The risk factors
and their importance can be used in the
investment decision process and to
appraise healthcare properties better. By
mapping out the risk factors and their
importance this study contributes to the
transparency and maturity of the healthcare
real estate market.
Discussion
This study has a couple of limitations. The
research method can be called into
question because it has resulted in too
many risk factors. A selection of the risk
factors can be used in follow up studies to
examine risk in healthcare real estate

Risk in Healthcare Real Estate Investment xxii
investment more closely. Despite these
limitations the study has contributed to the
knowledge on the risk of investing in
healthcare real estate. This study is the first
qualitative study on Dutch healthcare real
estate focusing solely on the risks. It offers
investors new knowledge they can
implement in their investment decision
process and gives insight in the different
points of view amongst investors.
Sources
Dale, D., Wolf, R., & Yang, H.F. (2015).
An assessment of the risk and return of
residential real estate. Managerial
Finance, 41(6), 591 - 599.
Ho, D.K.H., & Addae-Dapaah, K. (2015).
International Direct Real Estate Risk
Premiums in a Multi-Factor Estimation
Model. Journal of Real Estate Financial
Economics, 52–85.
McDonald, J.F., & & Dermisi, S. (2009).
Office building capitalization rates: the
case of downtown Chicago. The Journal
of Real Estate Finance and Economics,
39(4), 472-485.
Sivitanidou, R.C., & Sivitanides, P.S.
(1999). Office Capitalization Rates: Real
Estate and Capital Market Influences.
Journal of Real Estate Finance and
Economics, (18)3, 297-322.
Wheaton, W.C., Torto, R.G., Sivitanides,
P.S., Southard, J.A., Hopkins, R.E., &
Costello, J.M. (2001). Real estate risk: a
forward-looking approach. Real Estate
Finance, 18(3), 20-28.
Risk in Healthcare Real Estate Investment xxiii
Appendix 1. Comparison of the risk factors in the literature list and the final list.
Sample size Literature List Final List
Marketability of the Property 1 Retention of Value of the Property 18
Market maturity risks 1.1 Maturity of the Asset Market 18
Market size 1.1.1 Size of the asset market 19
Number of investors active on HCRE asset market
1.1.2 Number and diversity of parties active on the asset market
19
1.1.3 Transparency of the asset market 17
1.1.4 Standardization of HCRE 11
Investment volume of property 1.1.5 Availability of properties with the right investment volume for investors
17
1.1.6 Future development of the maturity of the asset market
9
1.1.7 Number and type of transactions (e.g. between investors)
2
Technical state of the property 1.2 Technical and Functional State of the Property 18
Age of the property 1.2.1 State of maintenance of the property 19
Recently renovated or not
1.2.2 Energy efficiency and durability of the property 19
1.2.3 Architectural appearance of the property 18
Functional Suitability of the Property
1.2.4 Functionality of the property for healthcare 17
1.2.5 Number of clients that can live in the property (e.g. >20)
16
1.2.6 Attractiveness of the property to other healthcare organizations
14
Percentage of apartments meant for low levels of care
Location 1.3 Location (with regard to healthcare use) 18
Location of the property
Density of the area 1.3.1 Population and building density of the surrounding area (e.g. urban or not)
18
1.3.2 Accessibility for family and friends of the clients and the staff of the tenant
19
1.3.3 Liveliness of the view and the architectural appearance of the surroundings
16
1.3.4 Safety of the surrounding area 17
1.3.5 Reputation and attractiveness of the neighborhood 16
1.3.6 Within or outside preferred investment region of the fund
9
1.3.7 Integration of the property in the surrounding neighborhood
5

Risk in Healthcare Real Estate Investment xxiv
Appendix 1 (continued). Comparison of the risk factors in the literature list and the final list.
Space market changes 1.4 Changes on the (Local) Space Market 16
1.4.1 Changes in government policy (e.g. increase in contribution by clients)
17
1.4.2 Medical developments that can influence the demand for HCRE space
16
Number of elderly with severe somatic and psycho-geriatric
conditions
1.4.3 Local development of the number of elderly with intense required care
19
1.4.4 Delay in the moment of moving out from their own house by future clients
6
1.4.5 Demand of other healthcare organizations on the space market (maturity of the space market)
17
1.4.6 Qualitative change in demand for space by clients 17
1.4.7 The length of the waiting lists 19
Rent levels 1.4.8 Rent levels of competing space 17
Supply of new space 1.4.9 Competing (new) supply of space in the vicinity 19
Vacancy rate 1.4.10 Vacancy rates of competing HCRE 19
Level of absorption of space
1.5 Alternative Use 16
1.5.1 Local development of demand and supply for alternative use (e.g. the development of the local
housing market)
17
1.5.2 Value of the alternative use (level of decline in return)
9
1.5.2.1 Technical flexibility of the property and suitability for alternative use (e.g. percentage of common
rooms)
17
1.5.2.2 Vicinity of services and facilities such as shops required for the alternative use
18
1.5.2.3 Changes in governmental technical requirements with regard to the alternative use
12
1.5.2.4 The measure of restrictions with regard to land use policy by the local government (e.g. whether
residential use is allowed)
14
1.5.2.5 The possibility of enough parking spots for the alternative use
17
Reliability of the Tenant 2 Stability of the Cash Flows Generated by Rental Contract(s)
18
Ratio between tenant earnings and rent
2.1 The Ratio between Income Generated by the Tenant in the Property and the Rent of the Property
19
Government policy changes 2.2 Influences of Government Policy Changes on the Stability of the Tenant
19
2.2.1 Sensitivity of the tenant to government policy changes on national and local level
17
2.2.2 Ratio of the rent and the regulated maximum rent if the separation between funding for healthcare and
housing would be implemented
14
2.2.3 Development of the policy of healthcare insurance companies (e.g. with regard to the allocation of the
capacity to different healthcare organizations)
14
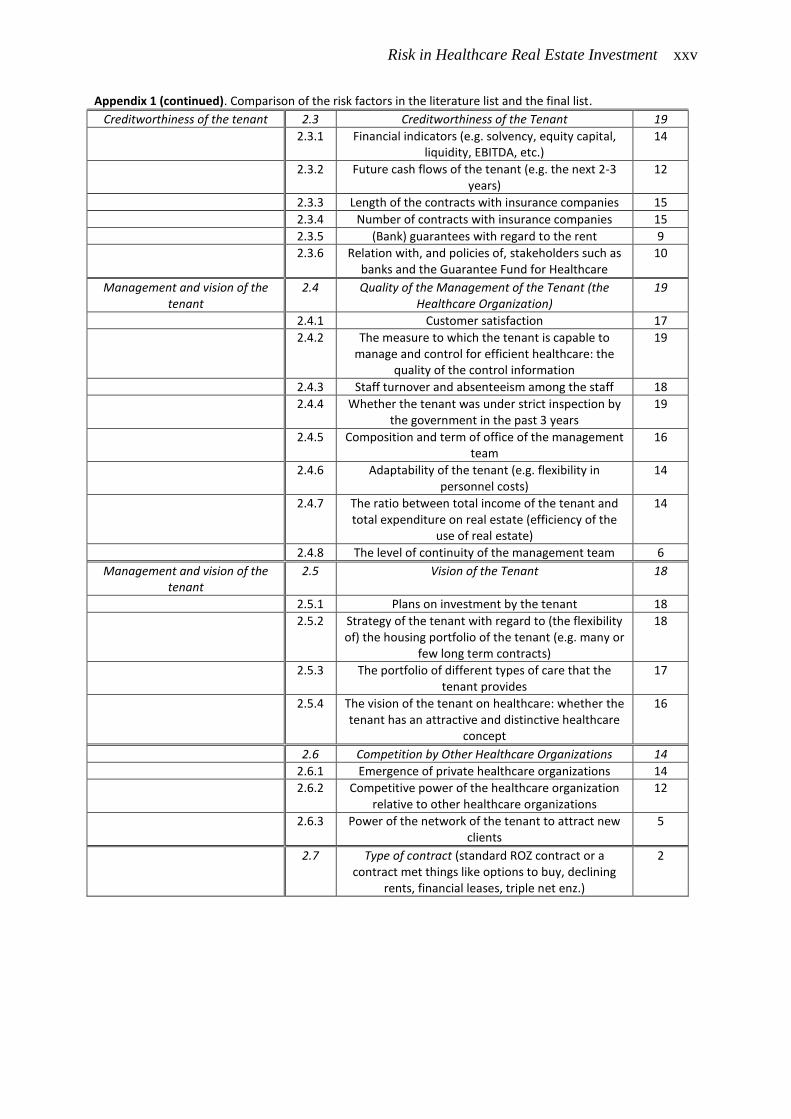
Risk in Healthcare Real Estate Investment xxv
Appendix 1 (continued). Comparison of the risk factors in the literature list and the final list.
Creditworthiness of the tenant 2.3 Creditworthiness of the Tenant 19
2.3.1 Financial indicators (e.g. solvency, equity capital, liquidity, EBITDA, etc.)
14
2.3.2 Future cash flows of the tenant (e.g. the next 2-3 years)
12
2.3.3 Length of the contracts with insurance companies 15
2.3.4 Number of contracts with insurance companies 15
2.3.5 (Bank) guarantees with regard to the rent 9
2.3.6 Relation with, and policies of, stakeholders such as banks and the Guarantee Fund for Healthcare
10
Management and vision of the tenant
2.4 Quality of the Management of the Tenant (the Healthcare Organization)
19
2.4.1 Customer satisfaction 17
2.4.2 The measure to which the tenant is capable to manage and control for efficient healthcare: the
quality of the control information
19
2.4.3 Staff turnover and absenteeism among the staff 18
2.4.4 Whether the tenant was under strict inspection by the government in the past 3 years
19
2.4.5 Composition and term of office of the management team
16
2.4.6 Adaptability of the tenant (e.g. flexibility in personnel costs)
14
2.4.7 The ratio between total income of the tenant and total expenditure on real estate (efficiency of the
use of real estate)
14
2.4.8 The level of continuity of the management team 6
Management and vision of the tenant
2.5 Vision of the Tenant 18
2.5.1 Plans on investment by the tenant 18
2.5.2 Strategy of the tenant with regard to (the flexibility of) the housing portfolio of the tenant (e.g. many or
few long term contracts)
18
2.5.3 The portfolio of different types of care that the tenant provides
17
2.5.4 The vision of the tenant on healthcare: whether the tenant has an attractive and distinctive healthcare
concept
16
2.6 Competition by Other Healthcare Organizations 14
2.6.1 Emergence of private healthcare organizations 14
2.6.2 Competitive power of the healthcare organization relative to other healthcare organizations
12
2.6.3 Power of the network of the tenant to attract new clients
5
2.7 Type of contract (standard ROZ contract or a contract met things like options to buy, declining
rents, financial leases, triple net enz.)
2

Risk in Healthcare Real Estate Investment xxvi
Risk in Healthcare Real Estate Investment xxvii
Preface
This report is the final product of my graduation thesis which serves to complete my master
Real Estate Management & Development at Eindhoven University of Technology. My
interest in real estate investment led me to the topic of healthcare real estate. Healthcare real
estate offers investors a new and growing real estate asset market, but investing in healthcare
real estate requires that investors gain new knowledge. With this study I hope to have
expanded on the currently underdeveloped knowledge on healthcare real estate investment.
I would like to thank several people for their involvement in this project. I would like
to thank Finance Ideas for offering me the opportunity to graduate on this interesting subject.
Furthermore, I would like to thank all the interviewees for sharing their knowledge so
enthusiastically. Your contribution has resulted in a deeper understanding of the healthcare
real estate market and the risks and uncertainties investors face. Thanks to your contribution
knowledge on healthcare real estate is greatly expanded and will result in a reduction in the
sense of uncertainty surrounding this new asset class.
I am grateful for my academic supervisors Stephan Maussen and Pauline van den
Berg, who gave excellent academic support and asked critical questions at the right moments.
I thank my company supervisor Pim Diepstraten for his practical input and support throughout
the entire process. Furthermore, I would like to thank Piet Eichholz for his support at decisive
moments, which has helped tremendously.
Last but not least, I would like to thank my family, friends and colleagues for their
support. You offered the conditions that made this study possible.
Tjeerd Kosse
Utrecht, February 2016

Risk in Healthcare Real Estate Investment xxviii
Risk in Healthcare Real Estate Investment 1
RISK IN HEALTHCARE REAL ESTATE INVESTMENT
1. Research Context
1.1. Introduction
The healthcare industry in The Netherlands has undergone big changes in recent years (Van
Ewijk, Van der Horst, & Besseling, 2013; Van der Wielen, 2014). These changes were mostly
caused by government policy changes in order to cut back the constant and alarming growth
of healthcare costs (Dantuma & Winkel, 2015; Van Ewijk et al., 2013; Ministerie van VWS,
2014; Van der Wielen, 2014). One of the ways to cut back costs was to change the way of
funding of healthcare real estate (HCRE) and to switch to performance oriented funding (Van
der Schaar, 2002; Nederlandse Zorgautoriteit, 2009; Nederlandse Zorgautoriteit, 2011). The
system of ex-post reimbursement is gradually changed to a performance oriented system
(Nederlandse Zorgautoriteit, 2011). In the performance oriented system funding will take
place entirely based on the number and type of clients the healthcare organizations receive
(Nederlandse Zorgautoriteit, 2011).
Because of this change it is evident that healthcare organizations have to adapt
themselves to the changing policies by making sure their real estate costs are covered based
on their performance. No longer is it financially viable to have high vacancy rates because
performance fees only cover the costs of most HCRE at an occupancy rate of 97%
(Nederlandse Zorgautoriteit, 2009). The policy changes have made healthcare organizations
responsible for the costs of real estate.
Because healthcare organizations are now funded based on their performance, lending
to an healthcare organization has become more risky (Van der Wielen, 2014; De Baaij, 2014,
2015; Postema, 2015). Banks have become more hesitant in providing funding for healthcare
organizations and set more strict terms on their loans to healthcare organizations (Van der
Wielen, 2014; Hermus, 2014; Postema, 2015). Housing associations are also retreating from
the HCRE asset market in order to focus on providing social housing (Van der Gijp, 2014;
Hermus, 2014, 2015; De Baaij, 2015) because government policy now encourages non-profit
housing associations to focus on their core purpose, which is to provide social housing
(Hermus, 2015; Scheijgrond, Anker, & Besier, 2015). This new situation has created the
incentive for healthcare organizations to search for alternative ways of financing their

Risk in Healthcare Real Estate Investment 2
operations and real estate (Van der Wielen, 2014; De Baaij, 2014; Hermus, 2014; Postema,
2015). One of these ways is by partnering up with real estate investors to rent (parts of) their
real estate instead of owning it (Hermus, 2014; 2015).
In foreign countries such as Belgium, the United Kingdom and the United States
investors have been investing in HCRE for several years (Van Elp & Konings, 2015; Berden
& Van de Velde, 2015; Hermus, 2015). Based on the positive experiences abroad, are
considering investing in Dutch HCRE (DTZ Zadelhoff, 2014; Schellens & De Bruijn, 2014).
HCRE is associated with diversification benefits, a hedge against an aging population, long
rental agreements, steady cash flows, growth perspectives, high availability of properties and
low risk with high returns (DTZ Zadelhoff, 2014; Van der Gijp, 2014; Van Elp & Konings,
2015; Hermus, 2014). Based on the prospect of adding a new asset class to their portfolio with
all these benefits, investors show clear signs of willingness to invest in HCRE (Berden & Van
de Velde, 2015; Hermus, 2014; Van Schie, 2014). Berden & Van de Velde (2015) argue that
HCRE is at the beginning of a boom which will lead to a mature and proper functioning asset
market. Van Elp & Konings (2015) estimate that the total volume of HCRE is 52 million
square meter (comparable to the size of the Dutch office market) and that it grows by roughly
0,8 million square meter per year. According to Van Elp & Konings the HCRE asset market
will be larger than the retail asset market by 2030. These findings are confirmed by DTZ
Zadelhoff (2014) who estimate that the amount of investment will have increased to € 825
million by 2017. This would mean a sevenfold increase in four years time (DTZ Zadelhoff,
2014). Because of this growth, DTZ Zadelhoff expects that by 2017 the demand will surpass
the supply of HCRE. However, in reality investors have not yet substantively invested in
HCRE (Schellens & De Bruijn, 2014). Investors are still unsure about the risks of investing in
HCRE. When they do wish to invest they often offer a lower price or require a higher return
than healthcare organizations are willing to accept (Van Schie, 2014; De Baaij, 2015). This is
caused by the phenomenon that as uncertainty over the risk of investing in real estate
increases the required cap rates increase (Wheaton et al., 2001). This leads to the following
problem statement.
Healthcare organizations are looking for alternative ways to finance their real estate.
Dutch real estate investors, on the other hand, show willingness to invest in HCRE but
hesitate because of uncertainty on the risk of investing in HCRE. HCRE is at the beginning
stage of becoming a new and substantial asset class on the Dutch real estate asset market
(Berden & Van de Velde, 2015; Van Elp & Konings, 2015). But the investment volume in
HCRE is still at a low level because investors are unsure of the risks and require a higher
Risk in Healthcare Real Estate Investment 3
return than healthcare organizations are willing to accept (Van Schie, 2014; De Baaij, 2015).
Wheaton et al. (2001) present support that as uncertainty over the risk of investing in real
estate increases the required cap rates increase. This phenomenon can be seen on the Dutch
HCRE market, where high risk premiums are required because of uncertainty on the risk of
investing in HCRE (Van Schie, 2014; De Baaij, 2015). To stimulate more investment more
knowledge is required on the risk of investing in HCRE to take away some of the uncertainty.
The supposition of this study is that by offering more clarity on the risks investors will
become less hesitant about investing in HCRE. In short the problem statement is:
There is a lack of knowledge on the level of risk of investing in HCRE properties.
1.2. Research Objective and Questions
The preceding introduction has shown a knowledge gap in the practice of HCRE investment.
In order to connect demand and supply on the HCRE property market new knowledge is
required on the risk of HCRE. This has resulted in the following research objective and
research questions.
1.2.1. Research Objective
The main objective of this thesis is to investigate the risks of investing in Dutch HCRE and
the importance of these different risks to real estate investors.
1.2.2. Research Question
What are the risks of investing in Dutch HCRE and the importance of these risks to real estate
investors?
I. What is the context of the current situation on the HCRE asset market?
II. What are the risks of investing in HCRE?
III. How important is each of these risks to investors?
1.3. Scope
The scope of this study is limited to only one category of HCRE. There is no unequivocal
definition of HCRE, although a generally accepted definition of HCRE is "real estate related
to healthcare". Because this definition is rather vague, more specific definitions have been
developed. The definition of HCRE used in this thesis is based on the broad definition used by
Van der Gijp (2014) and Van Elp & Konings (2015):
HCRE is real estate in which healthcare services are being provided.
Risk in Healthcare Real Estate Investment 4
HCRE is in more diverse in form and appearance than housing, offices or retail. Large
hospitals, worth of hundreds of millions, and housing at which inhabitants receive healthcare
services both fall into the same category. To simply limit the scope of this study only one
category is selected: intramural elderly HCRE. Intramural elderly HCRE are facilities for
elderly with high levels of required care. The real estate comes in the form of memory care
facilities and skilled nursing care facilities, or a combination of both. Besides elderly
intramural HCRE there are the following other seven categories of HCRE: life-cycle proof
housing; care at home; intramural mental HCRE; intramural handicap HCRE; and primary,
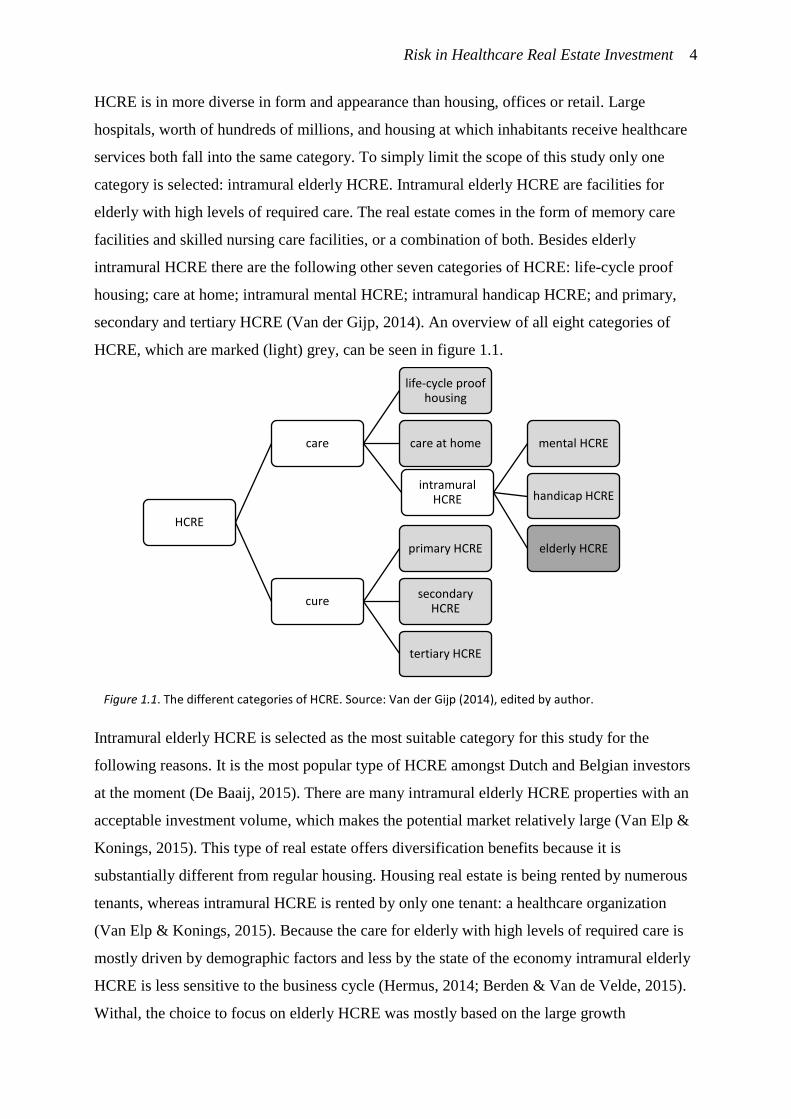
secondary and tertiary HCRE (Van der Gijp, 2014). An overview of all eight categories of
HCRE, which are marked (light) grey, can be seen in figure 1.1.
Intramural elderly HCRE is selected as the most suitable category for this study for the
following reasons. It is the most popular type of HCRE amongst Dutch and Belgian investors
at the moment (De Baaij, 2015). There are many intramural elderly HCRE properties with an
acceptable investment volume, which makes the potential market relatively large (Van Elp &
Konings, 2015). This type of real estate offers diversification benefits because it is
substantially different from regular housing. Housing real estate is being rented by numerous
tenants, whereas intramural HCRE is rented by only one tenant: a healthcare organization
(Van Elp & Konings, 2015). Because the care for elderly with high levels of required care is
mostly driven by demographic factors and less by the state of the economy intramural elderly
HCRE is less sensitive to the business cycle (Hermus, 2014; Berden & Van de Velde, 2015).
Withal, the choice to focus on elderly HCRE was mostly based on the large growth
HCRE
care
life-cycle proof housing
care at home
intramural HCRE
mental HCRE
handicap HCRE
elderly HCRE
cure
primary HCRE
secondary HCRE
tertiary HCRE
Figure 1.1. The different categories of HCRE. Source: Van der Gijp (2014), edited by author.

Risk in Healthcare Real Estate Investment 5
perspective. It is expected that the amount of people in need of elderly healthcare will grow
because the population is ageing (Van Elp & Konings, 2015; Van der Gijp, 2014). This might
seem contradictory to recent events because recent policy changes have temporarily reduced
the total number of elderly residing in intramural HCRE (Van Galen, Willems, & Poulus,
2012). Elderly with low levels of required care are no longer eligible for intramural
healthcare, which has temporarily resulted in a decrease of demand for this target group
(Regeling langdurige zorg, 2015; Van Galen, Willems, & Poulus, 2012). However, elderly
with severe somatic and psycho-geriatric health problems, who require more intense care,
continue to receive intramural healthcare (Regeling langdurige zorg, 2015; Van Galen,
Willems, & Poulus, 2012). The number of people with this high level of required care is
expected to grow substantially (Van Galen, Willems, & Poulus, 2012). This can be seen in
figure 1.2.
Figure 1.2. Development of demand for intramural elderly HCRE. The number of people with high levels of required care, categorized by type of required care. Source: Van Galen, Willems, & Poulus (2012), edited by author.
Figure 1.2 shows that the demand for memory care will continue to rise particularly rapidly.
Because of the aging population dementia will grow explosively the coming years; by over
100% by 2040 (Alzheimer Nederland, 2014). Alzheimer Nederland (2014) expects that the
number of dementia patients will peak in 2055 at 690.000 people. These numbers show that
there are strong demographic drivers for intramural elderly HCRE.
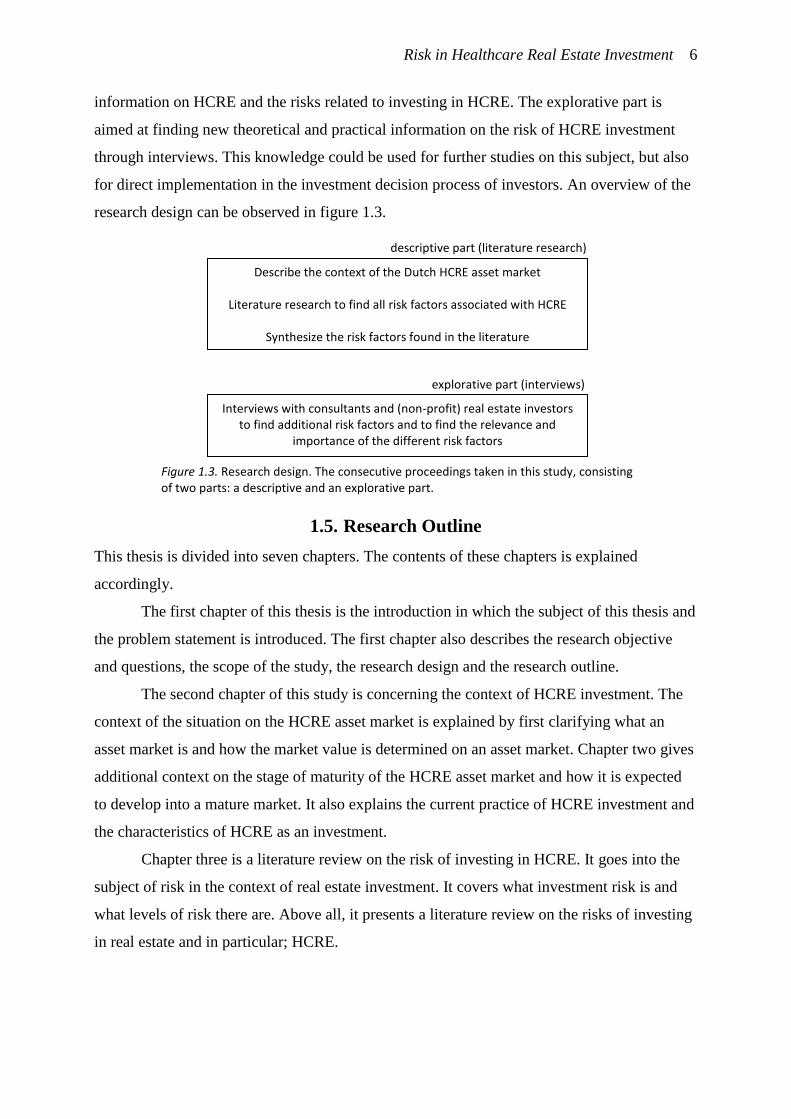
1.4. Research Design
This study is divided into two parts: a descriptive part, which consists mostly of literature
research, and an explorative part. The literature research is aimed at collecting all relevant
0
10.000
20.000
30.000
40.000
50.000
60.000
70.000
80.000
20
12
20
13
20
14
20
15
20
16
20
17
20
18
20
19
20
20
20
21
20
22
20
23
20
24
20
25
20
26
20
27
20
28
20
29
20
30
Memory Care Skilled Nursing
Specific Memory Care Specific Skilled Nursing Care
Risk in Healthcare Real Estate Investment 6
information on HCRE and the risks related to investing in HCRE. The explorative part is
aimed at finding new theoretical and practical information on the risk of HCRE investment
through interviews. This knowledge could be used for further studies on this subject, but also
for direct implementation in the investment decision process of investors. An overview of the
research design can be observed in figure 1.3.
1.5. Research Outline
This thesis is divided into seven chapters. The contents of these chapters is explained
accordingly.
The first chapter of this thesis is the introduction in which the subject of this thesis and
the problem statement is introduced. The first chapter also describes the research objective
and questions, the scope of the study, the research design and the research outline.
The second chapter of this study is concerning the context of HCRE investment. The
context of the situation on the HCRE asset market is explained by first clarifying what an
asset market is and how the market value is determined on an asset market. Chapter two gives
additional context on the stage of maturity of the HCRE asset market and how it is expected
to develop into a mature market. It also explains the current practice of HCRE investment and
the characteristics of HCRE as an investment.
Chapter three is a literature review on the risk of investing in HCRE. It goes into the
subject of risk in the context of real estate investment. It covers what investment risk is and
what levels of risk there are. Above all, it presents a literature review on the risks of investing
in real estate and in particular; HCRE.
Interviews with consultants and (non-profit) real estate investors to find additional risk factors and to find the relevance and
importance of the different risk factors
Describe the context of the Dutch HCRE asset market
Literature research to find all risk factors associated with HCRE
Synthesize the risk factors found in the literature
descriptive part (literature research)
explorative part (interviews)
Figure 1.3. Research design. The consecutive proceedings taken in this study, consisting of two parts: a descriptive and an explorative part.

Risk in Healthcare Real Estate Investment 7
Chapter four explains the methodology this study and covers the way the interviews
were carried out. Furthermore, it contains information on the interviewee selection, method of
analysis and contains a description of the fieldwork.
In Chapter five the results of this study are presented.
In Chapter six the practical and theoretical implications of the results are discussed as
well as recommendations and a discussion.

Risk in Healthcare Real Estate Investment 8
Risk in Healthcare Real Estate Investment 9
2. Theoretical Background
The introduction already stated that in the current HCRE asset market there is lack of
knowledge on the risk. This chapter goes more into detail on how this leads to higher return
requirements, longer rental agreements or a lower market value. Furthermore this chapter
gives a frame of reference to the stage of maturity the HCRE property market currently is in.
Lastly, it explains current practice in HCRE investment and clarifies the characteristics of
HCRE as an investment.
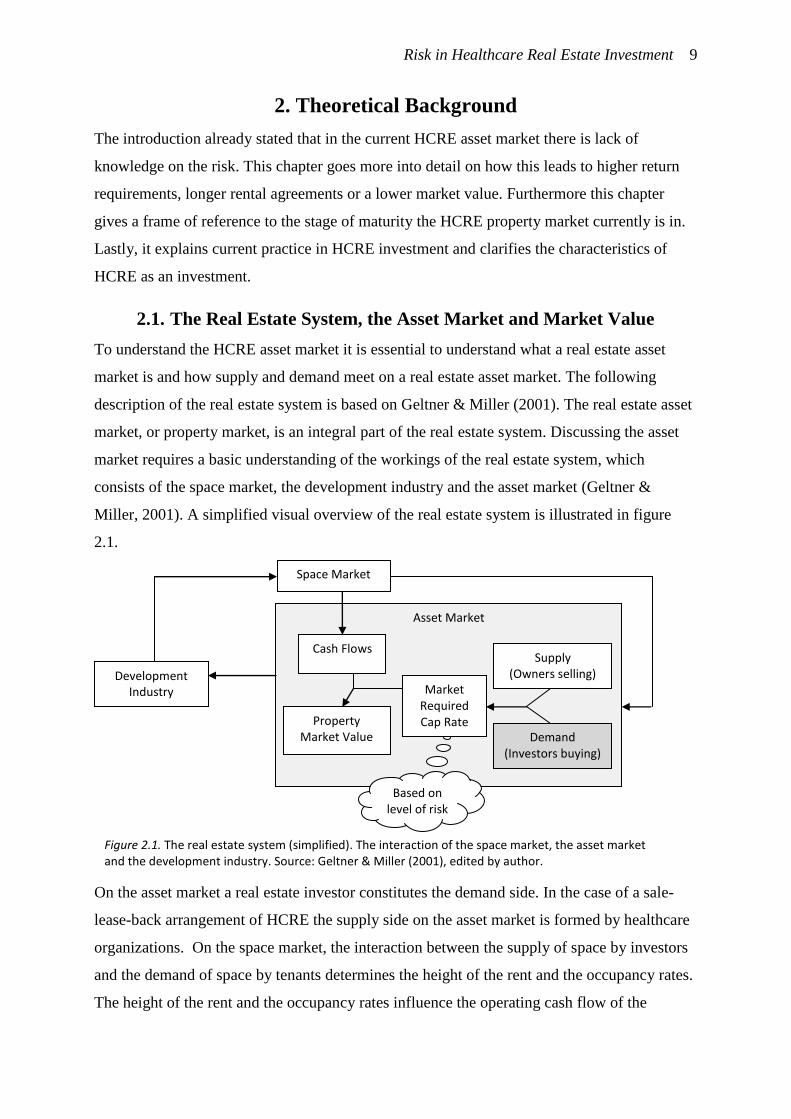
2.1. The Real Estate System, the Asset Market and Market Value
To understand the HCRE asset market it is essential to understand what a real estate asset
market is and how supply and demand meet on a real estate asset market. The following
description of the real estate system is based on Geltner & Miller (2001). The real estate asset
market, or property market, is an integral part of the real estate system. Discussing the asset
market requires a basic understanding of the workings of the real estate system, which
consists of the space market, the development industry and the asset market (Geltner &
Miller, 2001). A simplified visual overview of the real estate system is illustrated in figure
2.1.
On the asset market a real estate investor constitutes the demand side. In the case of a sale-
lease-back arrangement of HCRE the supply side on the asset market is formed by healthcare
organizations. On the space market, the interaction between the supply of space by investors
and the demand of space by tenants determines the height of the rent and the occupancy rates.
The height of the rent and the occupancy rates influence the operating cash flow of the
Asset Market
Based on level of risk
Development Industry
Space Market
Cash Flows
Property Market Value
Market Required Cap Rate
Supply (Owners selling)
Demand (Investors buying)
Figure 2.1. The real estate system (simplified). The interaction of the space market, the asset market and the development industry. Source: Geltner & Miller (2001), edited by author.
Risk in Healthcare Real Estate Investment 10
property. Since the operating cash flow is one of the elements used to determine the market
value of a property on the asset market the space market is inseparably connected to the asset
market.
In the asset market supply and demand consists of owners selling and investors
buying. The market value of the property is determined by both the cash flows of the property
and the market required cap rate. Investors ideally determine the market required cap rate
based on their perceptions on risk1.
On the HCRE asset market real estate investors are undecided on the risk of investing
in HCRE. When they do wish to invest they often require a high cap rate (Van Schie, 2014;
De Baaij, 2015). Wheaton et al. (2001) present support that as uncertainty over the risk of
investing in real estate increases the required cap rates increase. This phenomenon is
exemplified on the Dutch HCRE market, where high risk premiums are required by investors
because of a lack of consensus on the risk (Van Schie, 2014; De Baaij, 2015). Because market
required cap rates are high on the HCRE asset market the market value of the properties on
this market are low. This is due to the way cap rates influence the market value; when cash
flows remain equal and the market required cap rate rises, the market value of properties
depreciates. Because investors require a high cap rate the appraised market value is below the
acceptance levels of most healthcare organizations (Van Schie, 2014; De Baaij, 2015). Some
investors are willing to accommodate an acceptable return if the healthcare organization
agrees to sign a long-term contract. This epitomizes the predicament on the HCRE asset
market at its current stage; the beginning stage.
2.2. Stages of Maturity of an Asset Market
HCRE is at the onset of becoming a new and substantial asset class on the Dutch real estate
asset market (Van Elp & Konings, 2015; Berden & Van de Velde, 2015; Hermus, 2015). An
asset market goes through certain stages as it matures. Although these stages are gradual and
inadmissible to define, three stages are distinguished in the literature: the emerging market,
the developing market and the mature market (Keogh & D'Arcy, 1994; Chin, Dent, &
Roberts, 2006). Keogh & D'Arcy (1994) and Chin et al. (2006) studied the maturity of real
1 Apart from the risk, the cap rate is in fact also influenced by the opportunity cost of capital. Investors have a set amount of
capital available to allocate to several potential types of assets. The allocation of investment depends on the relative attractiveness of an asset class; as other types of assets become less attractive, real estate can become relatively more attractive to invest in. Thus, the performance of
other assets, such as stocks and bonds, will influence the attractiveness of real estate. E.g. if bonds and stocks become less attractive for
investment because they offer lower returns, investing in real estate becomes more attractive, and subsequently the height of the market required cap rate for real estate will drop. Another important factor investors take into consideration has a strong influence on the risk: the
growth expectations of the future cash flows. As the growth expectations rise, the risk of receiving lower than expected returns lowers.
Subsequently the market required cap rates will lower as well.

Risk in Healthcare Real Estate Investment 11
estate asset markets. Maturity, according to Chin et al. (2006), is defined as "an intrinsically
desirable set of market features" (p. 51). Many of the desirable characteristics they mention
are concerning real estate asset markets of entire countries and not specific sectors within
those countries. Some of the factors Chin et al. mention, also influence the maturity of Dutch
HCRE. To begin with the "existence of a sophisticated property profession with its associated
institutions and networks" (p. 51). As Dutch HCRE is a relatively new category, previously
unavailable for investment until recent government policy changes, investors are now at the
stage of orienting themselves on this new market (Berden & Van de Velde, 2015). Because
HCRE is quite knowledge intensive (Hermus, 2014), these activities have not yet resulted in
substantial investment. This demonstrates that the institutions and networks are still under
development. Chin et al. also stress the importance of the existence of "extensive information
flows and research activity" (p. 51). Information availability improves the transparency of the
market and reduces unexpected outcomes. Statistical analysis on the risk and return is
restricted by a lack of transactions which ensues in a lack of transparency (Hermus & Veuger,
2015). Although data on transactions is accumulating as more transactions occur every year,
the lack of statistical evidence shows the immaturity of the HCRE asset market.
A recent example, useful in the context of this thesis, of how a market can mature is
the Belgian HCRE asset market. The following paragraph is based on Berden & Van de Velde
(2015). The Belgian HCRE asset market was still an emerging market at the turn of the
century. By now Belgian investors such as Cofinimmo, AG Real Estate and Aedifica have
collectively invested over € 1,6 billion in Belgian HCRE. An example of the growth of the
HCRE portfolio of Belgian investors is depicted in figure 2.2.
Figure 2.2. The development of the portfolio of the Belgian HCRE investor Aedifica. The volume of investment by property type, in million euro. Source: Aedifica (2015), edited by author.
Figure 2.2 shows that the investment volume in elderly care facilities by Aedifica has
gradually increased (Aedifica, 2015). This gradual increase is related to the development of
0
200
400
600
800
1000
2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
Elderly Care Facilities Apartments Hotels

Risk in Healthcare Real Estate Investment 12
the maturity of the Belgian HCRE asset market. When the investment firm Cofinimmo
decided to start investing in HCRE in the early 2000s, the market was still underdeveloped.
The Belgian healthcare industry was unprepared for the growing demand for HCRE, and was
not able to finance the development of new HCRE. In this environment larger healthcare
organizations thrived as they were able to expand and reap the benefits of economies of scale.
To be able to expand they focused their capital on their core business (to provide healthcare)
by partnering up with investors. The investors provided funding for the development of new
HCRE. These partnerships laid the foundation for the Belgian HCRE asset market. Both
investors and healthcare organizations had to come to an understanding on the kind of
agreements they would devise regarding the duration of the rental agreement, the maintenance
of the properties, the entrusted duties of both parties etc. Because of the success of these early
transactions the popularity of HCRE grew among other investors. As other investors started to
invest the market size and maturity grew until the Belgian HCRE became commonly known
as a mature market. This example demonstrates that as the knowledge on the Belgian HCRE
market increased, the size and transparency of the market increased alongside with it, and vice
versa. Berden & Van de Velde (2015) suggest that the Dutch HCRE market will go through a
similar development.
A similar comparison was made by Hermus (2015) between the British and Dutch
HCRE market. The following explanation is based on Hermus (2015). The government policy
changes that recently occurred in The Netherlands are similar to policy changes in the United
Kingdom some years ago. Like in Belgium, British healthcare organizations decided to focus
their capital on their core business, entrusting investors with opportunities for investment. By
turning over their real estate they were able to improve their solvency. In The Netherlands
healthcare organizations have been renting their real estate likewise, admittedly from non-
profit housing associations. But housing associations are retrieving from the HCRE asset
market to be able to focus on providing social housing. These circumstances accommodate an
opening for investors to offer healthcare organizations the opportunity to sell a part of their
portfolio with a sale-and-leaseback arrangement to improve their solvency. Hermus expects
that in the coming years the number of investors active on the Dutch HCRE market will
increase, resulting in a more mature and transparent asset market. For healthcare
organizations this has the additional benefit of more competition among investors which will
drive up the market value.
Risk in Healthcare Real Estate Investment 13
2.3. The Current HCRE Investment Practice in The Netherlands
HCRE investment is still at the beginning stage in The Netherlands. The practice of HCRE
investment in this stage is significantly different from other types of real estate. HCRE has
several advantages and disadvantages in comparison to other types of real estate. The
advantages and disadvantages mentioned by Hermus (2014) and Berden & Van de Velde
(2015) are shown in table 2.1.
Table 2.1. The advantages and disadvantages of investing in HCRE. Source: Hermus (2014) and Berden & Van de Velde (2015), edited by author.
Advantages Disadvantages
Long rental agreements 1,2
The market is not (yet) transparent 1
Hedge against inflation 1,2
Political risk 1
Strong demographic drivers 1,2
Knowledge intensive 1
Low influence of the business cycle 1,2
Availability of high quality properties 1,2
Social impact on society 1
Hedge against the aging population 3
1: mentioned by Hermus (2014) 2: mentioned by Berden & Van de Velde (2015) 3: mentioned by Van der Gijp (2014)
One of the advantages mentioned is the length of the rental agreements. In HCRE rental
agreements have historically been long. Rental agreements of over 10 years are still very
common today. In HCRE investment long rental contracts with reliable partners ensures
stable cash flows that are indexed for inflation (Van der Gijp, 2014; Hermus & Veuger,
2015).
Because the rental contracts are indexed for inflation they offers a hedge against the inflation.
HCRE experiences strong demographic drivers caused by the aging of the population.
Because the demand for HCRE is mostly demographically driven it is less susceptible to
economic recessions. In the UK periodic returns show less volatility and seem to be less
susceptible to the negative impact of the business cycle than other types of commercial real
estate (Van der Gijp, 2014). Another advantage mentioned by Hermus and Berden & Van de
Velde is that the availability of properties is still high because investment in HCRE still needs
to regain.
Hermus also mentions three disadvantages. The developing HCRE asset market is not
yet transparent. Some of the causes hereof are a lack of references and difficulties in valuating
HCRE. Another disadvantage is political risk. Because the healthcare industry is heavily
regulated and depended on government policy, each change in government policy can have
far-reaching effects on HCRE. Another disadvantage is the high level of required knowledge
to be able to invest in HCRE. Some investors might adjourn investing in HCRE for this
Risk in Healthcare Real Estate Investment 14
reason but others might see investing in a knowledge intensive real estate type as a
competitive advantage.
Although Berden & Van de Velde (2015) and Hermus seem to agree on most
advantages, Hermus (2014) sees a disadvantage in the limited possibilities for diversification
within HCRE. Berden & Van de Velde suggest that by partnering up with a healthcare
organization an investor can achieve diversification by means of spreading investment over
several locations. When trying to achieve diversification in this way the strategy of the partner
is a key element. If the strategy of the partnering healthcare organization is to expand and to
provide healthcare in a range of different locations the investor can provide rental properties
and in that way diversify his portfolio geographically (Berden & Van de Velde, 2015).
Whether HCRE can offer diversification within a portfolio of different types of real estate
remains undisputed.
HCRE has another specific benefit not seen in other real estate types. Pension funds
and insurance companies can benefit by investing in HCRE indirectly by benefiting from the
improved functioning of healthcare organizations (Van der Gijp, 2014). The aging of the
population will result in more pensioners and more expenditure for the care of elderly. By
investing in HCRE pension funds and insurance companies can hedge against the aging
population because the demand for HCRE will rise as the population ages. Moreover,
investing in HCRE can offer investors the benefit of having social impact (Hermus, 2014).
Besides different advantages and disadvantages HCRE investment has other typical
characteristics. Typical about the current practice of HCRE investment in The Netherlands is
an emphasis on long and stable rental agreements brought about by low expectations on the
exit values and little faith in the functioning of the HCRE space market. In a properly
functioning space market tenants compete with each other for space through pricing. An
example of a properly functioning space market is the housing market. If the tenant of an
apartment cancels his rental contract the property is expected to be rented out to one of the
many potential tenants at a price resembling demand and supply on the space market. Such
confidence in finding a tenant is lacking on the HCRE space market. Once the rental contract
of a HCRE property ends, the investor expects that the chance of finding a healthcare
organization willing to rent the property at a reasonable price is low (Hermus & Veuger,
2015). The lack of confidence in being able to find a tenant is at the root of low expected exit
values (Van der Gijp, 2014). Because HCRE is specifically aimed at a much smaller pool of
potential tenants the market value is strongly dependent on the company-specific commercial
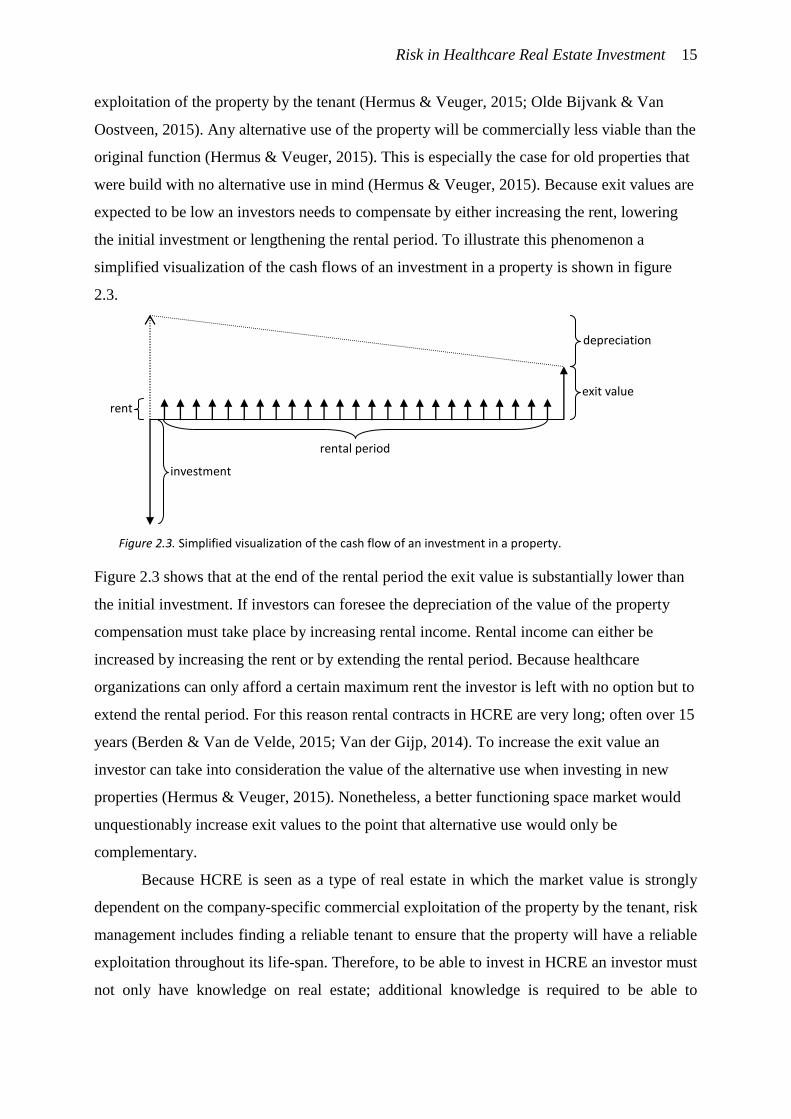
Risk in Healthcare Real Estate Investment 15
exploitation of the property by the tenant (Hermus & Veuger, 2015; Olde Bijvank & Van
Oostveen, 2015). Any alternative use of the property will be commercially less viable than the
original function (Hermus & Veuger, 2015). This is especially the case for old properties that
were build with no alternative use in mind (Hermus & Veuger, 2015). Because exit values are
expected to be low an investors needs to compensate by either increasing the rent, lowering
the initial investment or lengthening the rental period. To illustrate this phenomenon a
simplified visualization of the cash flows of an investment in a property is shown in figure
2.3.
Figure 2.3 shows that at the end of the rental period the exit value is substantially lower than
the initial investment. If investors can foresee the depreciation of the value of the property
compensation must take place by increasing rental income. Rental income can either be
increased by increasing the rent or by extending the rental period. Because healthcare
organizations can only afford a certain maximum rent the investor is left with no option but to
extend the rental period. For this reason rental contracts in HCRE are very long; often over 15
years (Berden & Van de Velde, 2015; Van der Gijp, 2014). To increase the exit value an
investor can take into consideration the value of the alternative use when investing in new
properties (Hermus & Veuger, 2015). Nonetheless, a better functioning space market would
unquestionably increase exit values to the point that alternative use would only be
complementary.
Because HCRE is seen as a type of real estate in which the market value is strongly
dependent on the company-specific commercial exploitation of the property by the tenant, risk
management includes finding a reliable tenant to ensure that the property will have a reliable
exploitation throughout its life-span. Therefore, to be able to invest in HCRE an investor must
not only have knowledge on real estate; additional knowledge is required to be able to
rent
depreciation
exit value
investment
rental period
Figure 2.3. Simplified visualization of the cash flow of an investment in a property.
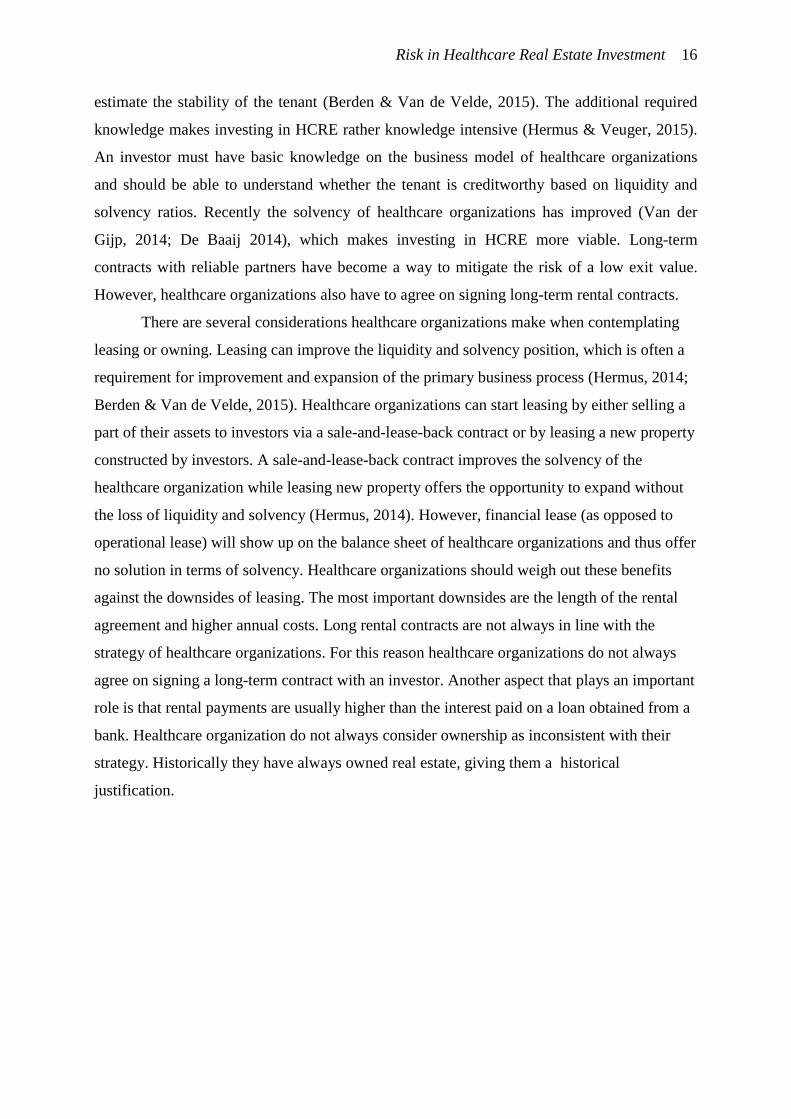
Risk in Healthcare Real Estate Investment 16
estimate the stability of the tenant (Berden & Van de Velde, 2015). The additional required
knowledge makes investing in HCRE rather knowledge intensive (Hermus & Veuger, 2015).
An investor must have basic knowledge on the business model of healthcare organizations
and should be able to understand whether the tenant is creditworthy based on liquidity and
solvency ratios. Recently the solvency of healthcare organizations has improved (Van der
Gijp, 2014; De Baaij 2014), which makes investing in HCRE more viable. Long-term
contracts with reliable partners have become a way to mitigate the risk of a low exit value.
However, healthcare organizations also have to agree on signing long-term rental contracts.
There are several considerations healthcare organizations make when contemplating
leasing or owning. Leasing can improve the liquidity and solvency position, which is often a
requirement for improvement and expansion of the primary business process (Hermus, 2014;
Berden & Van de Velde, 2015). Healthcare organizations can start leasing by either selling a
part of their assets to investors via a sale-and-lease-back contract or by leasing a new property
constructed by investors. A sale-and-lease-back contract improves the solvency of the
healthcare organization while leasing new property offers the opportunity to expand without
the loss of liquidity and solvency (Hermus, 2014). However, financial lease (as opposed to
operational lease) will show up on the balance sheet of healthcare organizations and thus offer
no solution in terms of solvency. Healthcare organizations should weigh out these benefits
against the downsides of leasing. The most important downsides are the length of the rental
agreement and higher annual costs. Long rental contracts are not always in line with the
strategy of healthcare organizations. For this reason healthcare organizations do not always
agree on signing a long-term contract with an investor. Another aspect that plays an important
role is that rental payments are usually higher than the interest paid on a loan obtained from a
bank. Healthcare organization do not always consider ownership as inconsistent with their
strategy. Historically they have always owned real estate, giving them a historical
justification.
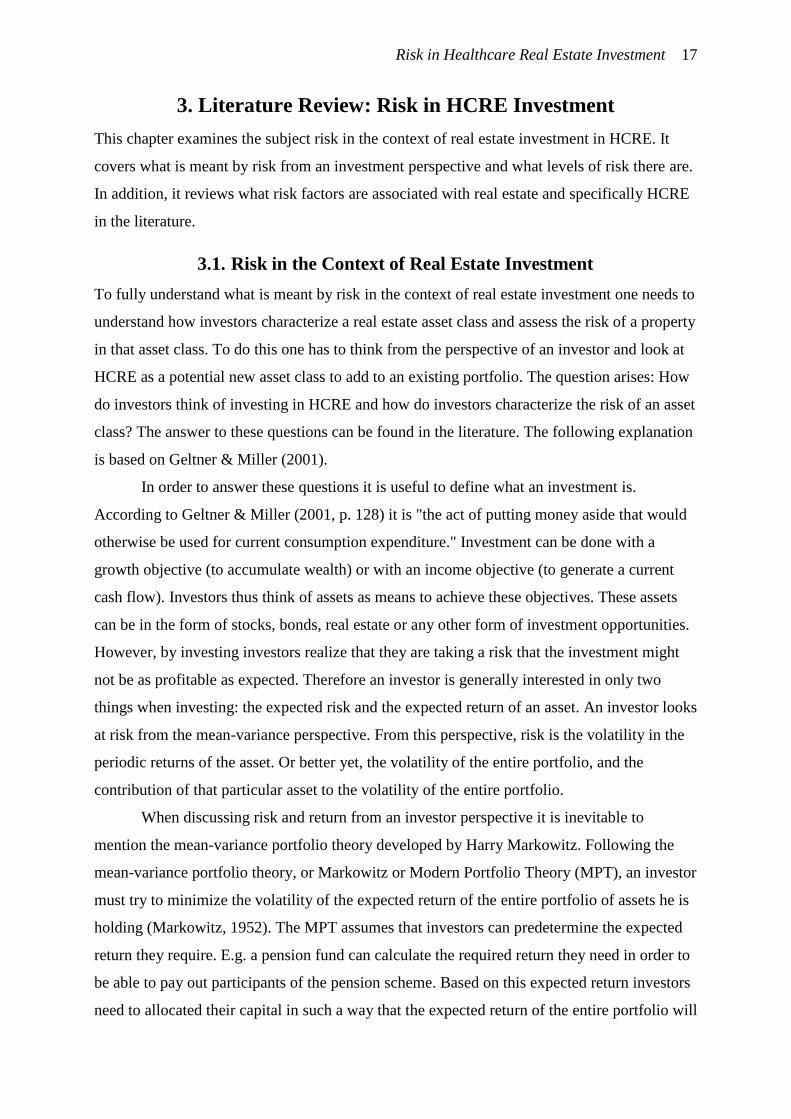
Risk in Healthcare Real Estate Investment 17
3. Literature Review: Risk in HCRE Investment
This chapter examines the subject risk in the context of real estate investment in HCRE. It
covers what is meant by risk from an investment perspective and what levels of risk there are.
In addition, it reviews what risk factors are associated with real estate and specifically HCRE
in the literature.
3.1. Risk in the Context of Real Estate Investment
To fully understand what is meant by risk in the context of real estate investment one needs to
understand how investors characterize a real estate asset class and assess the risk of a property
in that asset class. To do this one has to think from the perspective of an investor and look at
HCRE as a potential new asset class to add to an existing portfolio. The question arises: How
do investors think of investing in HCRE and how do investors characterize the risk of an asset
class? The answer to these questions can be found in the literature. The following explanation
is based on Geltner & Miller (2001).
In order to answer these questions it is useful to define what an investment is.
According to Geltner & Miller (2001, p. 128) it is "the act of putting money aside that would
otherwise be used for current consumption expenditure." Investment can be done with a
growth objective (to accumulate wealth) or with an income objective (to generate a current
cash flow). Investors thus think of assets as means to achieve these objectives. These assets
can be in the form of stocks, bonds, real estate or any other form of investment opportunities.
However, by investing investors realize that they are taking a risk that the investment might
not be as profitable as expected. Therefore an investor is generally interested in only two
things when investing: the expected risk and the expected return of an asset. An investor looks
at risk from the mean-variance perspective. From this perspective, risk is the volatility in the
periodic returns of the asset. Or better yet, the volatility of the entire portfolio, and the
contribution of that particular asset to the volatility of the entire portfolio.
When discussing risk and return from an investor perspective it is inevitable to
mention the mean-variance portfolio theory developed by Harry Markowitz. Following the
mean-variance portfolio theory, or Markowitz or Modern Portfolio Theory (MPT), an investor
must try to minimize the volatility of the expected return of the entire portfolio of assets he is
holding (Markowitz, 1952). The MPT assumes that investors can predetermine the expected
return they require. E.g. a pension fund can calculate the required return they need in order to
be able to pay out participants of the pension scheme. Based on this expected return investors
need to allocated their capital in such a way that the expected return of the entire portfolio will
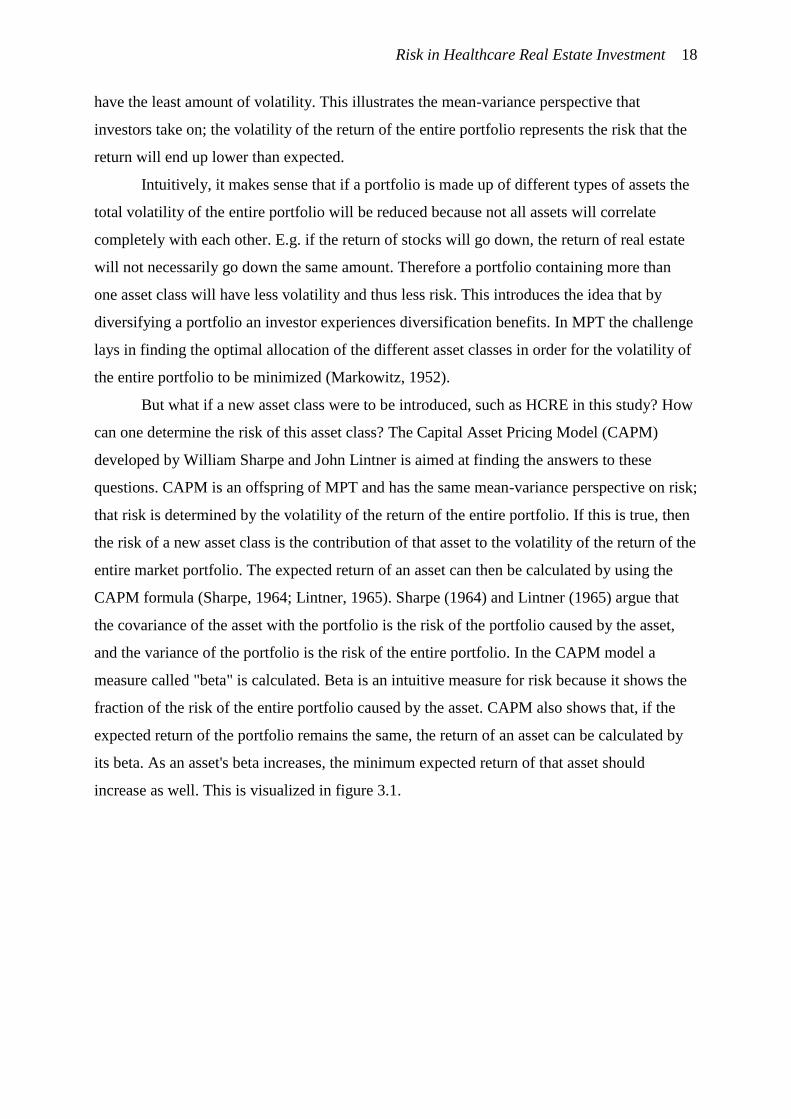
Risk in Healthcare Real Estate Investment 18
have the least amount of volatility. This illustrates the mean-variance perspective that
investors take on; the volatility of the return of the entire portfolio represents the risk that the
return will end up lower than expected.
Intuitively, it makes sense that if a portfolio is made up of different types of assets the
total volatility of the entire portfolio will be reduced because not all assets will correlate
completely with each other. E.g. if the return of stocks will go down, the return of real estate
will not necessarily go down the same amount. Therefore a portfolio containing more than
one asset class will have less volatility and thus less risk. This introduces the idea that by
diversifying a portfolio an investor experiences diversification benefits. In MPT the challenge
lays in finding the optimal allocation of the different asset classes in order for the volatility of
the entire portfolio to be minimized (Markowitz, 1952).
But what if a new asset class were to be introduced, such as HCRE in this study? How
can one determine the risk of this asset class? The Capital Asset Pricing Model (CAPM)
developed by William Sharpe and John Lintner is aimed at finding the answers to these
questions. CAPM is an offspring of MPT and has the same mean-variance perspective on risk;
that risk is determined by the volatility of the return of the entire portfolio. If this is true, then
the risk of a new asset class is the contribution of that asset to the volatility of the return of the
entire market portfolio. The expected return of an asset can then be calculated by using the
CAPM formula (Sharpe, 1964; Lintner, 1965). Sharpe (1964) and Lintner (1965) argue that
the covariance of the asset with the portfolio is the risk of the portfolio caused by the asset,
and the variance of the portfolio is the risk of the entire portfolio. In the CAPM model a
measure called "beta" is calculated. Beta is an intuitive measure for risk because it shows the
fraction of the risk of the entire portfolio caused by the asset. CAPM also shows that, if the
expected return of the portfolio remains the same, the return of an asset can be calculated by
its beta. As an asset's beta increases, the minimum expected return of that asset should
increase as well. This is visualized in figure 3.1.
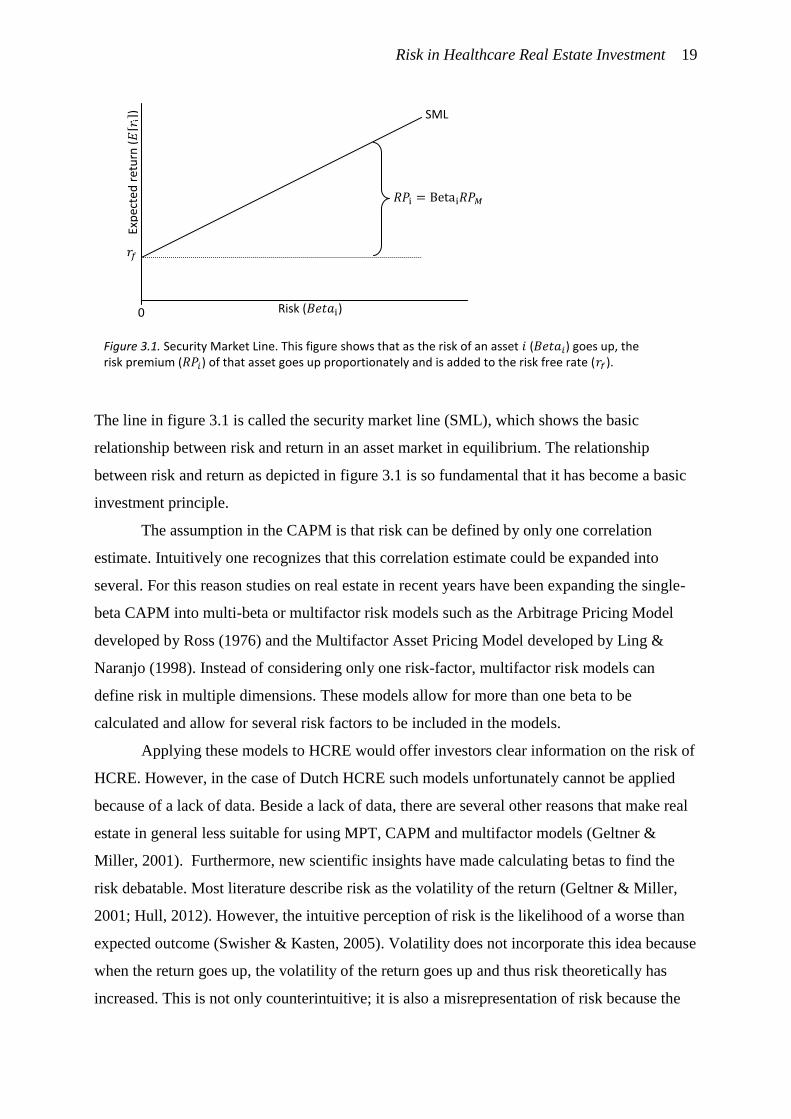
Risk in Healthcare Real Estate Investment 19
The line in figure 3.1 is called the security market line (SML), which shows the basic
relationship between risk and return in an asset market in equilibrium. The relationship
between risk and return as depicted in figure 3.1 is so fundamental that it has become a basic
investment principle.
The assumption in the CAPM is that risk can be defined by only one correlation
estimate. Intuitively one recognizes that this correlation estimate could be expanded into
several. For this reason studies on real estate in recent years have been expanding the single-
beta CAPM into multi-beta or multifactor risk models such as the Arbitrage Pricing Model
developed by Ross (1976) and the Multifactor Asset Pricing Model developed by Ling &
Naranjo (1998). Instead of considering only one risk-factor, multifactor risk models can
define risk in multiple dimensions. These models allow for more than one beta to be
calculated and allow for several risk factors to be included in the models.
Applying these models to HCRE would offer investors clear information on the risk of
HCRE. However, in the case of Dutch HCRE such models unfortunately cannot be applied
because of a lack of data. Beside a lack of data, there are several other reasons that make real
estate in general less suitable for using MPT, CAPM and multifactor models (Geltner &
Miller, 2001). Furthermore, new scientific insights have made calculating betas to find the
risk debatable. Most literature describe risk as the volatility of the return (Geltner & Miller,
2001; Hull, 2012). However, the intuitive perception of risk is the likelihood of a worse than
expected outcome (Swisher & Kasten, 2005). Volatility does not incorporate this idea because
when the return goes up, the volatility of the return goes up and thus risk theoretically has
increased. This is not only counterintuitive; it is also a misrepresentation of risk because the
SML
0
Exp
ecte
d r
etu
rn (
)
Risk ( )
Figure 3.1. Security Market Line. This figure shows that as the risk of an asset ( ) goes up, the risk premium ( ) of that asset goes up proportionately and is added to the risk free rate ( ).
Risk in Healthcare Real Estate Investment 20
periodic returns of an asset often do not follow a normal distribution (Swisher & Kasten,
2005; Mamoghli & Daboussi, 2010). Therefore, when calculating beta using CAPM the
perception of risk could be too optimistic or too pessimistic (Chong, Jin, & Phillips, 2013).
An alternative would be to use downside risk instead of volatility, which is aimed at the
probability that the return is lower than expected (Roy, 1952, cited in Chong, Jin & Phillips,
2013). Mamoghli & Daboussi (2010) provide support that downside risk is a better measure
for risk than CAPM's beta because of skewness and kurtosis in the probability distribution of
returns. They compared CAPM with downside-CAPM; a model developed by Estrada (2002,
cited in Momoghli & Daboussi, 2010), which allows for the investor to set an expected return
in order to calculate the chance that the return will be lower than expected based on the
volatility of the periodic returns of that asset. The downside-CAPM is based on the asset 's
downside standard deviation of returns; in short the semideviation (Estrada, 2007).
Downside risk and semideviation is still under development and for several reasons it
is not yet regular practice in the investment world (Swisher & Kasten, 2005). In this study the
concept behind downside risk, that risk is represented by the probability of a lower than
expected return, is used as the definition of what risk is in the eye of investors. It is a more
intuitive measure of risk and allows for a better focus on what really matters to an investor.
In the practice of real estate investment the assessment of risk is incorporated into the
valuation method. When investing in a property, first the value of the property is estimated
using a valuation method. The most common and most advised method is the discounted cash
flow method [DCF] (Lusht, 2001; Geltner & Miller, 2001). In this method the cash flows are
used in combination with the required internal rate of return [IRR] in order to determine the
value of the property (Lusht, 2001; Geltner & Miller, 2001). In this setting the meaning of risk
is the probability that the value of the property is lower than expected (downside risk). The
higher the probability that the value will be lower than expected the higher the IRR must be in
order to compensate for the risk.
Investors translate risk into a higher expected return by using surcharges on expected
return that investors require (Buffing, Achterveld, & Conijn, 2015). This is called the buildup
method (Chong, Jin, & Phillips, 2013), in which the expected return is based on the risk free
rate plus several risk premiums depending on the type of investment. This can be seen in the
following formula:
(1)

Risk in Healthcare Real Estate Investment 21
in which the expected return is based on the risk free rate and the risk premiums for
real estate general risks ( ), property type specific risks ( ) and property specific
risks ( ) (Buffing et al., 2015). Real estate general risks are risks that apply to all types of
real estate. Property type specific risks apply specifically to the entire type of properties and
property specific risks are risks that are specific for each individual property. This means that
one particular property shares the same real estate and property type risks with other
properties in the same type but has specific risks at property level. In order to illustrate this a
model was developed: the Hedonic Risk Model (HRM). The HRM is based on the concepts of
the hedonic value model or hedonic pricing model introduced by Rosen (1974), that uses the
characteristics of the building, renter and the environment to find the price of real estate. If the
same hedonic approach would be applied to the risk of a good, the hypothesis would be that
risk is determined by the risk-bearing characteristics of that good. In a formula risk
(semideviation of asset : ) can then be expressed as the function of the implicit risk-
bearing characteristics ( in the formula . This is the
HRM introduced in this study. Unfortunately, in this study risk is unknown and
therefore it is impossible to use statistical analysis to find the individual values for
. This study can, however, offer insight into the characteristics (
. A visualization of the HRM can be seen in figure 3.2.
The idea that the level of risk of real estate can be estimated by examining the characteristics
of real estate has been subject of many studies in which attempts have been made in
investigating which characteristics ( determine the risk. These risk-bearing
Figure 3.2. The HRM: Hedonic Risk Model. The risk of investing in real estate can be broken down into several risk factors based on the notion of the hedonic hypothesis. The risk can be divided into three levels of risk: real estate general risks, property type specific risks and property specific risks.
Risk:
Real estate general risks
Property type specific risks
Property specific risks
risk factors: characteristic t/m
risk factors: characteristic t/m
risk factors: characteristics t/m

Risk in Healthcare Real Estate Investment 22
characteristics are called: risk factors. The following literature review will reveal some of the
different risk factors that were found in the literature.
3.2. Risks associated with Real Estate
Because there are few sources on the risk of HCRE investment scientific works on other real
estate types are included in this literature review. HCRE is strongly correlated to other real
estate types, as shown by Van Elp & Konings (2015). This can partly be explained by real
estate general risk factors such as large macro-economic effects which influence all real estate
types. Another explanation is that some of the property type specific risks and property
specific risks for other real estate types could be similar to those of HCRE.
There have been several studies on the risk factors of real estate using CAPM and multifactor
models of which some of the more recent are described hereafter. Dale, Wolf & Yang (2015)
investigated risk in investing in residential real estate. They observe that the betas for
residential real estate, as calculated in several studies using CAPM models, portray residential
real estate as an asset class with an exceptional high return to risk ratio (Dale et al., 2015).
According to Dale et al. the risk calculated using CAPM does not reflect the true underlying
risk of residential real estate. Dale et al. add two risk factors to the CAPM: liquidity risk and
leverage risk, and find that by adding these risk factors the betas they find are more realistic.
Pavlov, Steiner & Wachter (2015) tested the relationship between macroeconomic risk
factors and the returns on international real estate. They find support for their hypothesis that
there is a relation between returns and the global stock market; foreign exchange rate
fluctuations, inflation and country governance.
Ho & Addae-Dapaah (2015) studied office, residential and retail real estate in Asia
and the United States. They conducted a literature review to find the risk factors associated
with investing in real estate. They describe the following risk factors in their literature review
which consist of references to studies such as those by Ling & Naranjo (1998) and Pai and
Geltner (2007, cited in Ho & Addae-Dapaah, 2015): stock market; bond market; Gross
National Product (GDP); supply of new stock; prime lending rate; vacancy rate; consumption;
location; the law system of the country; the size of the property and; the real estate class (Ho
& Addae-Dapaah, 2015).
There have also been several studies on the determinants of the cap rate in real estate
investment. Investors ideally determine the cap rate based on the level of risk the investment
Risk in Healthcare Real Estate Investment 23
represents (Geltner & Miller, 2001). As the risk of an asset increases, so does the expected
return as visualized in figure 7 of this chapter: the security market line. Several studies have
been devoted to finding the risk factors that are related to the height of the cap rates.
Froland (1987) finds the determinants of the cap rate to be: the mortgage contract rate;
the spread between Treasury bills and; the corporate earnings-to-price ratio. Ambrose &
Nourse (1993) note that Froland's study did not take into consideration the property types,
while the results by Dokko, Edelstein, Pomer and Urdang (1991) indicate that cap rates differ
among property types. Ambrose & Nourse used property specific variables, location variables
and financial characteristics variables to examine the determinants of commercial and
industrial properties. Their results indicate that property type characteristics are important
when explaining the cap rates.
Sivitanidou & Sivitanides (1999) investigated cap rates in the office market. The
results of their study suggests that the following factors are the most important determinants
of the cap rates in office real estate: the level of concentration of offices in a central business
district (CBD); the level of diversity of different types of tenants on the demand side of the
office space market; the ratio of government tenants versus other office tenants and; the level
of absorption of the office space by new tenants (Sivitanidou & Sivitanides, 1999).
Wheaton et al. (2001) make a more general observation on risk in real estate
investment. They argue that the level of uncertainty when forecasting cap rates is the most
important factor when estimating risk in real estate investment. The reasoning is that in real
estate investment, unlike in other asset classes such as stocks and bonds, cap rates can (to
some extent) be statistically predicted based on forecasts (Wheaton et al., 2001). The level of
predictability largely determines the height of the cap rate because as the predictability
increases cap rates go down because predictability is associated with lower risk. The model
used by Wheaton et al. shows strong statistical significance, which, according to Wheaton et
al. suggests that it is possible to make predictions on the height of the cap rates in real estate
investment using statistical analysis on forecasts of market rents and interest rates.
Furthermore, they argue that local market factors are the most important factors in explaining
cap rates. That real estate cap rates can largely be predicted using statistical analysis is further
underlined by Sivitanides, Southard, Torto, & Wheaton (2001). The two local market factors
used by Sivitanides et al. are: the ratio between current rent levels and the historical average
level and; the change in rent levels. Sivitanides et al. hereby capture some of the indicators of
cyclical movements as they predict that an upwards trend in rent levels results in lowering cap
rates and a downward trend results in rising cap rates.
Risk in Healthcare Real Estate Investment 24
D'Argensio & Laurin (2009) listed variables related to the height of cap rates based on
a literature review and own insights. The list consists of variables that capture the growth of
cash flows (rent index; vacancy rate; GDP growth and; inflation rate), real estate variables
(the size of the space market divided by the size of the population [the 'depth' of the market];
the size of the space market divided by the size of the area [the 'density' of the market] and;
the existence of real estate investment trusts [REITs] in that particular asset market) and
qualitative variables (the quality of the bureaucracy; the strength and impartiality of law and
order and; an index by the ICRG/PRS Group that combines three kinds of investment risk).
Furthermore, they investigate the relation between government bonds and the cap rates of real
estate. They find that real estate cap rates are largely related to government bonds. The
variables mentioned earlier also play a role, but only to a lesser extent (D'Argensio & Laurin,
2009). The 'depth' and 'density' of the market are significant factors, because according to
D'Argensio & Laurin investors prefer to operate in larger markets. The other real estate
variables have less explanatory power (D'Argensio & Laurin, 2009).
The previous studies were conducted at macro level. The following studies are micro-level;
they focus on only one local real estate market. Saderion, Smith & Smith (1994) analyzed the
apartment market in Houston, Texas, by analyzing 500 transactions between 1978 and 1988.
They conclude that variations in cap rates can be explained by the size, age and location of the
apartment complexes.
A similar study was done by McDonald & Dermisi (2009) on the cap rates of
transactions of 132 offices in downtown Chicago in the period 1996 to 2007. According to
this study a low cap rate is associated with a low risk-free rate, a lower borrowing rate, class-
A buildings, newer buildings, buildings that had been renovated, lowering vacancy rates in
the local office market and an increase in employment in the financial sector in the
metropolitan area.
Hendershott & Turner (1999) use data on 403 transactions in Stockholm in the period
1990 to 1992 to analyze the determinants of the cap rates. They conclude that cap rates are
lower for those properties that are used for residential purposes as opposed to commercial
purposes. Furthermore, low cap rates are associated with good locations, below-market
financing and low density land plots.
Netzell (2009, cited in Chaney & Hoesli, 2012) continued on a study by Gunnelin,
Hendershott, Hoesli & Söderberg (2004, cited in Chaney & Hoesli, 2012) on 599 properties in
Stockholm. They extended the period of observation; from a period of just the year 2000 to
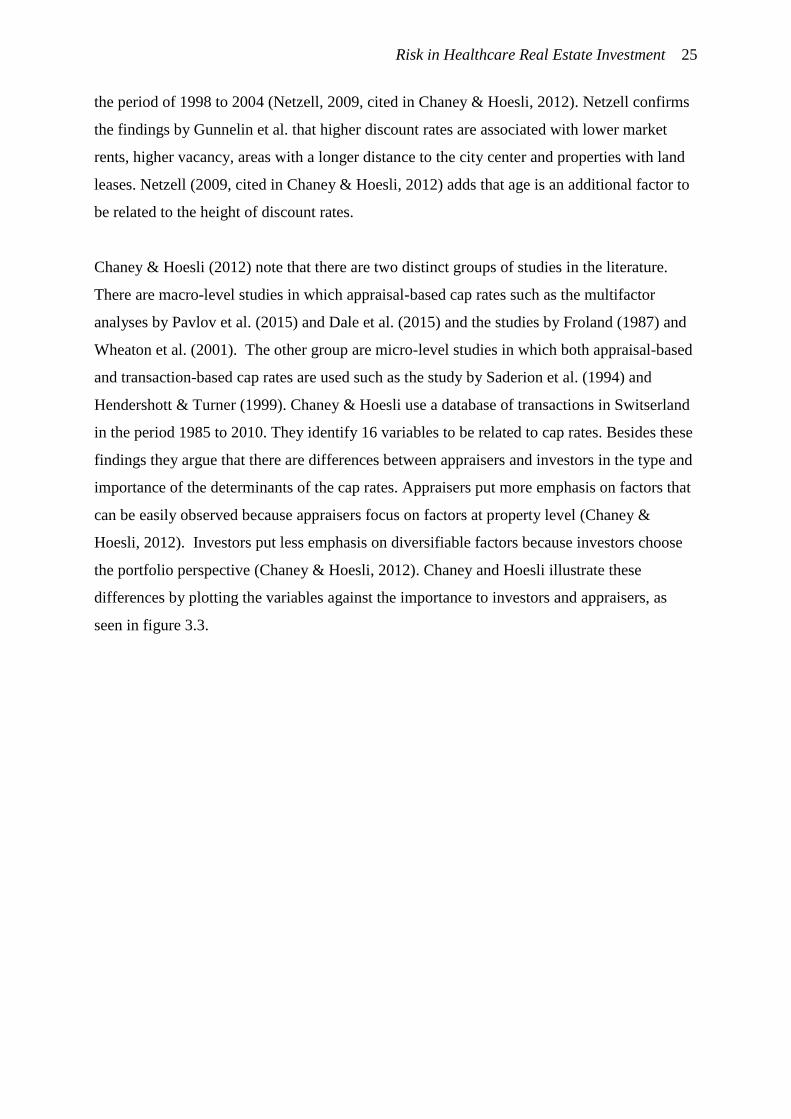
Risk in Healthcare Real Estate Investment 25
the period of 1998 to 2004 (Netzell, 2009, cited in Chaney & Hoesli, 2012). Netzell confirms
the findings by Gunnelin et al. that higher discount rates are associated with lower market
rents, higher vacancy, areas with a longer distance to the city center and properties with land
leases. Netzell (2009, cited in Chaney & Hoesli, 2012) adds that age is an additional factor to
be related to the height of discount rates.
Chaney & Hoesli (2012) note that there are two distinct groups of studies in the literature.
There are macro-level studies in which appraisal-based cap rates such as the multifactor
analyses by Pavlov et al. (2015) and Dale et al. (2015) and the studies by Froland (1987) and
Wheaton et al. (2001). The other group are micro-level studies in which both appraisal-based
and transaction-based cap rates are used such as the study by Saderion et al. (1994) and
Hendershott & Turner (1999). Chaney & Hoesli use a database of transactions in Switserland
in the period 1985 to 2010. They identify 16 variables to be related to cap rates. Besides these
findings they argue that there are differences between appraisers and investors in the type and
importance of the determinants of the cap rates. Appraisers put more emphasis on factors that
can be easily observed because appraisers focus on factors at property level (Chaney &
Hoesli, 2012). Investors put less emphasis on diversifiable factors because investors choose
the portfolio perspective (Chaney & Hoesli, 2012). Chaney and Hoesli illustrate these
differences by plotting the variables against the importance to investors and appraisers, as
seen in figure 3.3.
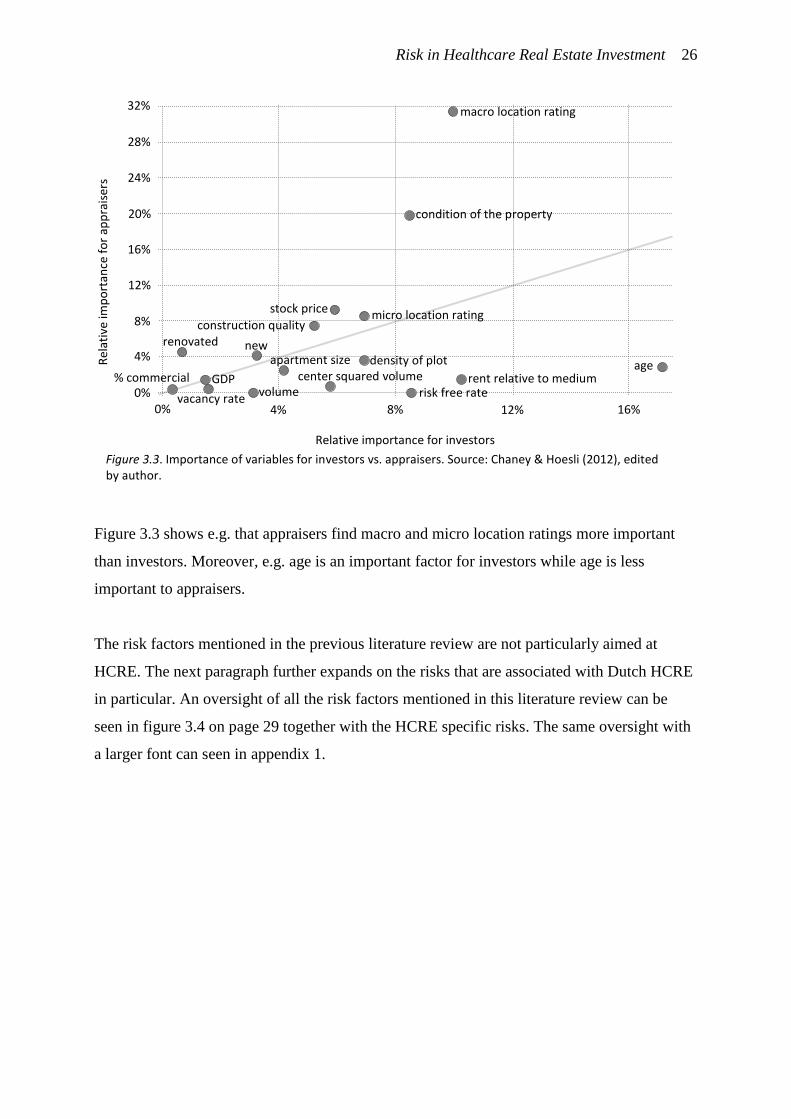
Risk in Healthcare Real Estate Investment 26
Figure 3.3 shows e.g. that appraisers find macro and micro location ratings more important
than investors. Moreover, e.g. age is an important factor for investors while age is less
important to appraisers.
The risk factors mentioned in the previous literature review are not particularly aimed at
HCRE. The next paragraph further expands on the risks that are associated with Dutch HCRE
in particular. An oversight of all the risk factors mentioned in this literature review can be
seen in figure 3.4 on page 29 together with the HCRE specific risks. The same oversight with
a larger font can seen in appendix 1.
macro location rating
age
condition of the property
micro location rating stock price
construction quality renovated new
rent relative to medium risk free rate
density of plot center squared volume
apartment size
vacancy rate
GDP % commercial
Figure 3.3. Importance of variables for investors vs. appraisers. Source: Chaney & Hoesli (2012), edited by author.
Rel
ativ
e im
po
rtan
ce f
or
app
rais
ers
Relative importance for investors
0% 4% 8% 12% 16%
32%
28%
24%
16%
8%
4%
0%
20%
12%
volume
Risk in Healthcare Real Estate Investment 27
3.3. Risks associated with Dutch HCRE
There are only limited a number of articles and books available on Dutch HCRE. Relevant
works on the risk of HCRE investment are described below in a brief literature review.
Van Elp & Konings (2015) conducted a study on HCRE investment in The
Netherlands as a result of growing interest in HCRE. They found the standard deviation of the
returns of Dutch HCRE. These standard deviations should give an indication of the risk
involved with investing in HCRE. They also calculated the Sharpe ratios for different real
estate asset classes in The Netherlands. The Sharpe ratio is in essence a way to approximate
the ratio between risk and return by dividing the risk premium (approximated by Van Elp &
Konings by taking the average return over 2003-2013 minus the risk free premium of 3,5%)
by the risk (the volatility of the return; approximated by the standard deviation). The greater
the Sharpe ratio, the better the investor is compensated for the risk. The return, standard
deviation, Sharpe ratio and the correlation of the different real estate classes with Care HCRE
can be seen in table 3.1.
Table 3.1. Return, standard deviation, and Sharpe ratios for different kinds of Dutch real estate, and the correlation of care HCRE with the different kinds of real estate. Source: Van Elp & Konings (2015), edited by author.
Average Return 2003-2013
Standard deviation
Sharpe ratio Correlation with Care HCRE
All Dutch HCRE 5.6 5.7 0.4 0.86
Care HCRE 4.8 5.8 0.2 1
Cure HCRE 6.2 4.3 0.6 0.47
All Dutch real estate 5.8 4.3 0.5 0.79
Residential real estate 5.0 4.5 0.3 0.77
Office real estate 4.1 4.8 0.1 0.79
Retail real estate 8.2 4.4 1.1 0.81
Industrial 6.3 4.3 0.6 0.62
Other 8.5 3.3 1.5 n/a
Shares 3.4 24.9 n/a n/a
JP Morgan Bonds 6.4 6.4 0.5 0.40
Table 3.1 shows that Care HCRE has a low Sharpe ratio and is correlated with other asset
classes. This would mean that Care HCRE offers slight diversification benefits and does not
offer as much return in comparison to the risk relative to other types of real estate. Van Elp &
Konings add to these findings that they are not completely representative because 82% of the
properties investigated were owned by non-profit housing associations who typically require a
lower return than regular investors (Van Elp & Konings, 2015). Therefore there was very
little data available on asset owned by for-profit institutional investment companies.
Furthermore, most real estate in the dataset could not be considered investment grade (Van
Elp & Konings, 2015). De Baaij (2015) notices that a large part of the investigated real estate
Risk in Healthcare Real Estate Investment 28
was old. Furthermore he notices that most of the HCRE in the study is not interesting for
investors (De Baaij, 2015). Van Elp & Konings (2015) argue that the reason the average
return for Care HCRE was so low because after 2007 the indirect return on the investigated
real estate was negative, which was caused by government policy changes. They also argue
that investing in HCRE can offer low risk and high return as it does in the United States, the
United Kingdom, Belgium and Australia. However, HCRE in The Netherlands is a new
investment market and therefore clearly not without risk (Van Elp & Konings, 2015). One of
the risks already mentioned is the risk of political interference, which in the case of the study
by Van Elp & Konings resulted in a low indirect return. The risks that are associated with
investing in Dutch HCRE will be described hereafter.
Van Elp & Konings mention four factors that can cause investors concerns about the risk of
investing in HCRE. One of these is the question whether the market of HCRE is sufficiently
large and liquid. The second risk factor they mention is political risk as policy changes by the
government can have far-reaching effects on risk and return. The third factor is the
creditworthiness of healthcare organizations as tenants and the fourth risk factor they mention
is concerning the height of the exit value and the likelihood of vacancy. In addition, Van Elp
& Konings discuss what HCRE is suitable for investment. They explain this by using a four
quadrant matrix in which 2 different variables are set out against each other; the
creditworthiness of the tenant and the marketability of the real estate. The four quadrants are
as follows (Van Elp & Konings, 2015):
Quadrant I: creditworthy tenant in marketable real estate: investment grade;
Quadrant II: creditworthy tenant in unmarketable real estate: question mark;
Quadrant III: credit-unworthy tenant in unmarketable real estate: not investment grade;
Quadrant IV: credit-unworthy tenant in unmarketable real estate: question mark.
The way Van Elp & Konings (2015) set up their four quadrant model shows an
underlying reasoning that the measure to which HCRE is investible is dependant on two
variables: the creditworthiness of the tenant and the marketability of the real estate. These two
variables actually are risk factors as the level of risk increases as creditworthiness and
marketability decreases. The understanding that the creditworthiness of the tenant and the
marketability of the real estate are two important risk factors is further underlined by De Baaij
(2015, 2014). De Baaij considers the creditworthiness of the tenant as an important factor that
influences the stability of the cash flows. He argues that if the tenant is incapable of meeting
his obligations to pay the rent the next risk factor to take into account is the measure to which

Risk in Healthcare Real Estate Investment 29
the building be used for an alternative function. In other words; if the creditworthiness of the
tenant proofs to be low and the tenant is unable to pay the rent investors must make sure the
property does not lose value by means of ensuring there is an alternative use.
Berden & Van de Velde (2015) also mention the creditworthiness of the tenant, but
add that the creditworthiness is not the only aspect when investigating the future tenant of the
property. They argue that besides screening on creditworthiness the healthcare organization
should be screened on track record, strategic vision and having a strong and structured
management team (Berden & Van de Velde, 2015).
Van der Gijp (2014) mentions four different risk factors: political risk, space market
risk, asset market risk and partner risk. By political risk is meant the risk of government
policy changes which can have an effect on the HCRE market. This is similar to the findings
of Van Elp & Konings (2015) and Berden & Van de Velde (2015) who all argue that political
interference in the healthcare industry is an important risk factor. By space market risk is
meant the extent to which there is sufficient demand for space in comparison to the supply of
HCRE space. If demand for space remains significantly higher than supply the risk of
investing in HCRE will be lower. The third factor mentioned, asset market risk, is the risk that
the HCRE asset market will not truly develop into a mature market with sufficient investors.
If the market will not go through mayor changes, the transparency and liquidity of the market
will remain poor. The fourth factor, partner risk, is the risk that the partner, the healthcare
organization, proves to have insufficient solvency and liquidity to pay the rent. This risk is
similar to the chance that the healthcare organization goes bankrupt; in other words: the
creditworthiness of the tenant, as mentioned by Van Elp & Konings (2015).
In the previous literature review several risk factors were identified. Most were retrieved from
scientific literature on other real estate classes and some were retrieved from literature on
Dutch HCRE. An oversight of the different risk factors can be seen in figure 3.4. The same
oversight can be seen in appendix 1 with a larger font.

Risk in Healthcare Real Estate Investment 30
Figure 3.4. The oversight of all risk factors mentioned in the literature review and their sources.
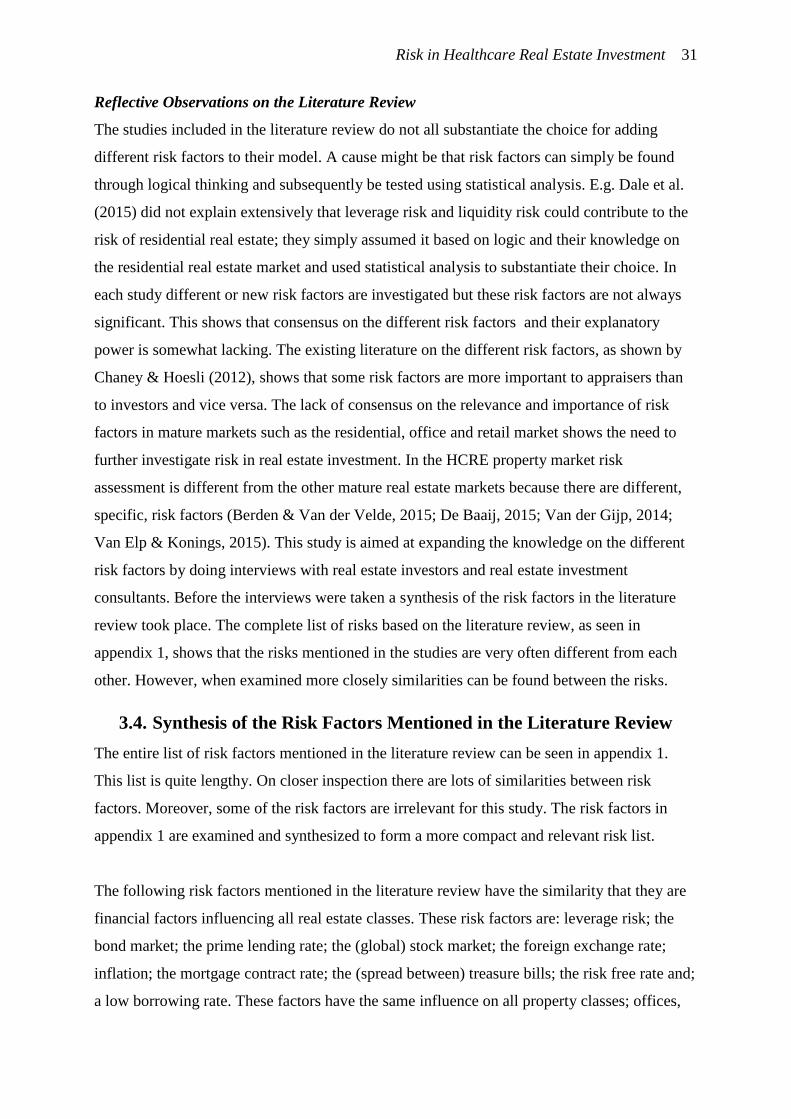
Risk in Healthcare Real Estate Investment 31
Reflective Observations on the Literature Review
The studies included in the literature review do not all substantiate the choice for adding
different risk factors to their model. A cause might be that risk factors can simply be found
through logical thinking and subsequently be tested using statistical analysis. E.g. Dale et al.
(2015) did not explain extensively that leverage risk and liquidity risk could contribute to the
risk of residential real estate; they simply assumed it based on logic and their knowledge on
the residential real estate market and used statistical analysis to substantiate their choice. In
each study different or new risk factors are investigated but these risk factors are not always
significant. This shows that consensus on the different risk factors and their explanatory
power is somewhat lacking. The existing literature on the different risk factors, as shown by
Chaney & Hoesli (2012), shows that some risk factors are more important to appraisers than
to investors and vice versa. The lack of consensus on the relevance and importance of risk
factors in mature markets such as the residential, office and retail market shows the need to
further investigate risk in real estate investment. In the HCRE property market risk
assessment is different from the other mature real estate markets because there are different,
specific, risk factors (Berden & Van der Velde, 2015; De Baaij, 2015; Van der Gijp, 2014;
Van Elp & Konings, 2015). This study is aimed at expanding the knowledge on the different
risk factors by doing interviews with real estate investors and real estate investment
consultants. Before the interviews were taken a synthesis of the risk factors in the literature
review took place. The complete list of risks based on the literature review, as seen in
appendix 1, shows that the risks mentioned in the studies are very often different from each
other. However, when examined more closely similarities can be found between the risks.
3.4. Synthesis of the Risk Factors Mentioned in the Literature Review
The entire list of risk factors mentioned in the literature review can be seen in appendix 1.
This list is quite lengthy. On closer inspection there are lots of similarities between risk
factors. Moreover, some of the risk factors are irrelevant for this study. The risk factors in
appendix 1 are examined and synthesized to form a more compact and relevant risk list.
The following risk factors mentioned in the literature review have the similarity that they are
financial factors influencing all real estate classes. These risk factors are: leverage risk; the
bond market; the prime lending rate; the (global) stock market; the foreign exchange rate;
inflation; the mortgage contract rate; the (spread between) treasure bills; the risk free rate and;
a low borrowing rate. These factors have the same influence on all property classes; offices,

Risk in Healthcare Real Estate Investment 32
housing, retail and also HCRE. Although studies show that these risk factors are relevant, they
play a role at macro level. These risks influence the real estate general risk premium (
in equation 1 on page 19), which is similar for all real estate types. Also the risk factors GDP,
consumption and land lease influence the real estate general risk premium and are not HCRE
specific. Therefore these risk factors are removed from the risk list. The same can be said
about the risk factor real estate type, because the real estate type is already limited to only
one; HCRE. The concentration of offices in a CBD is seen as irrelevant because this risk
factor applies only to office real estate classes and is thus removed from the risk list.
Also the risk factor 'uncertainty in forecasting cap rates' is removed. The notion that
risk increases as it is harder to forecast future changes shows the need to make sure future
forecasts on risk become more accurate. The risk factor itself does not offer a means to
determine the level of risk to reduce uncertainty.
An overview of all the removed risk factors and the reason for their irrelevance is seen
in table 3.2.
Table 3.2. The risk factors that were removed from the synthesized risk list and the reason they were deemed irrelevant.
Risk Factors Reasons for Irrelevance
leverage risk
financial factors that influence all real estate classes
the bond market
the prime lending rate
the (global) stock market
the foreign exchange rate
inflation
the mortgage contract rate
the (spread between) treasury bills
the risk free rate
a low borrowing rate
GDP
influences all real estate classes consumption
land lease
real estate type the real estate type is known to be HCRE
concentration of offices in a CBD this risk factor is related to offices
uncertainty in forecasting cap rates
the risk factor shows that when there is uncertainty on the level of risk this results in higher cap rates. The
risk factor is not useful in actually determining the level of risk
In the literature marketability was mentioned by Van Elp & Konings (2015), Berden & Van
de Velde (2015), De Baaij (2015) and Van der Gijp (2014) as an important risk factor in
HCRE together with the reliability or creditworthiness of the tenant. These sources
specifically mention these two risk factors because from the perspective of the investor risk
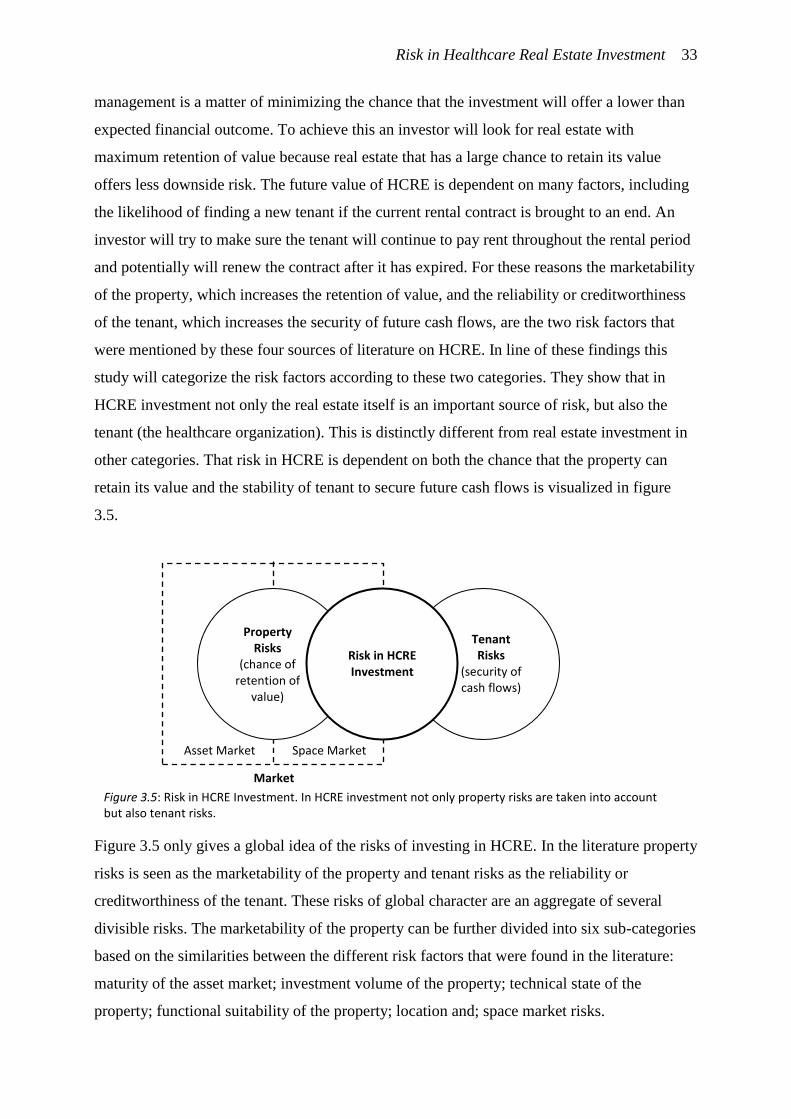
Risk in Healthcare Real Estate Investment 33
management is a matter of minimizing the chance that the investment will offer a lower than
expected financial outcome. To achieve this an investor will look for real estate with
maximum retention of value because real estate that has a large chance to retain its value
offers less downside risk. The future value of HCRE is dependent on many factors, including
the likelihood of finding a new tenant if the current rental contract is brought to an end. An
investor will try to make sure the tenant will continue to pay rent throughout the rental period
and potentially will renew the contract after it has expired. For these reasons the marketability
of the property, which increases the retention of value, and the reliability or creditworthiness
of the tenant, which increases the security of future cash flows, are the two risk factors that
were mentioned by these four sources of literature on HCRE. In line of these findings this
study will categorize the risk factors according to these two categories. They show that in
HCRE investment not only the real estate itself is an important source of risk, but also the
tenant (the healthcare organization). This is distinctly different from real estate investment in
other categories. That risk in HCRE is dependent on both the chance that the property can
retain its value and the stability of tenant to secure future cash flows is visualized in figure
3.5.
Figure 3.5 only gives a global idea of the risks of investing in HCRE. In the literature property
risks is seen as the marketability of the property and tenant risks as the reliability or
creditworthiness of the tenant. These risks of global character are an aggregate of several
divisible risks. The marketability of the property can be further divided into six sub-categories
based on the similarities between the different risk factors that were found in the literature:
maturity of the asset market; investment volume of the property; technical state of the
property; functional suitability of the property; location and; space market risks.
Market
Asset Market Space Market
Risk in HCRE Investment
Property Risks
(chance of retention of
value)
Tenant Risks
(security of cash flows)
Figure 3.5: Risk in HCRE Investment. In HCRE investment not only property risks are taken into account but also tenant risks.

Risk in Healthcare Real Estate Investment 34
The following risk factors found in the literature are all related to the maturity of the market:
market size and liquidity; marketability of the real estate; asset market risk; liquidity risk and;
existence of REITs. By asset market risk Van der Gijp (2014) meant the risk that the HCRE
asset market would remain underdeveloped. When an asset market is more developed the
marketability of the property increases. As the market size grows the maturity of the market
increases and the property becomes more easily marketable. Another risk factor mentioned in
the literature is the risk factor existence of REITs. The existence of REITs shows a certain
level of development of the asset market. This risk factor was included in the synthesized list
in the form of the number of investors active on the HCRE asset market. As more investors
are active on the asset market the maturity of the market increases and the property becomes
more easily marketable. The risk factors that resulted from this synthesis can be seen in table
3.3.
Table 3.3. On the left the risks from the literature related to maturity of the market and on the right the synthesized list of risk related to the maturity of the market.
Risks related to the Maturity of the Market
→
1.1 Maturity of the Market
market size and liquidity
1.1.1 market size asset market risk
liquidity risk
existence of REITs 1.1.2 number of real estate investors active on
HCRE asset market
Another two risk factors mentioned in the literature, size of the property and volume of
investment, both influence the marketability of the property. As the volume and size of the
investment is either too small or too big the property is harder to transfer to another investor.
The risk factor the volume of the investment is related to the risk factor the size of the
property. These two factors can be merged into one, as from an investors' perspective the
volume of the investment is the most important factor. The risk factors that resulted from this
synthesis can be seen in table 3.4.
Table 3.4. On the left the risks from the literature related to the investment volume of the property and on the right the synthesized list of risk related to marketability.
Risks related to investment volume of the property
→ 1.2 Investment Volume of the Property size of the property
volume of investment
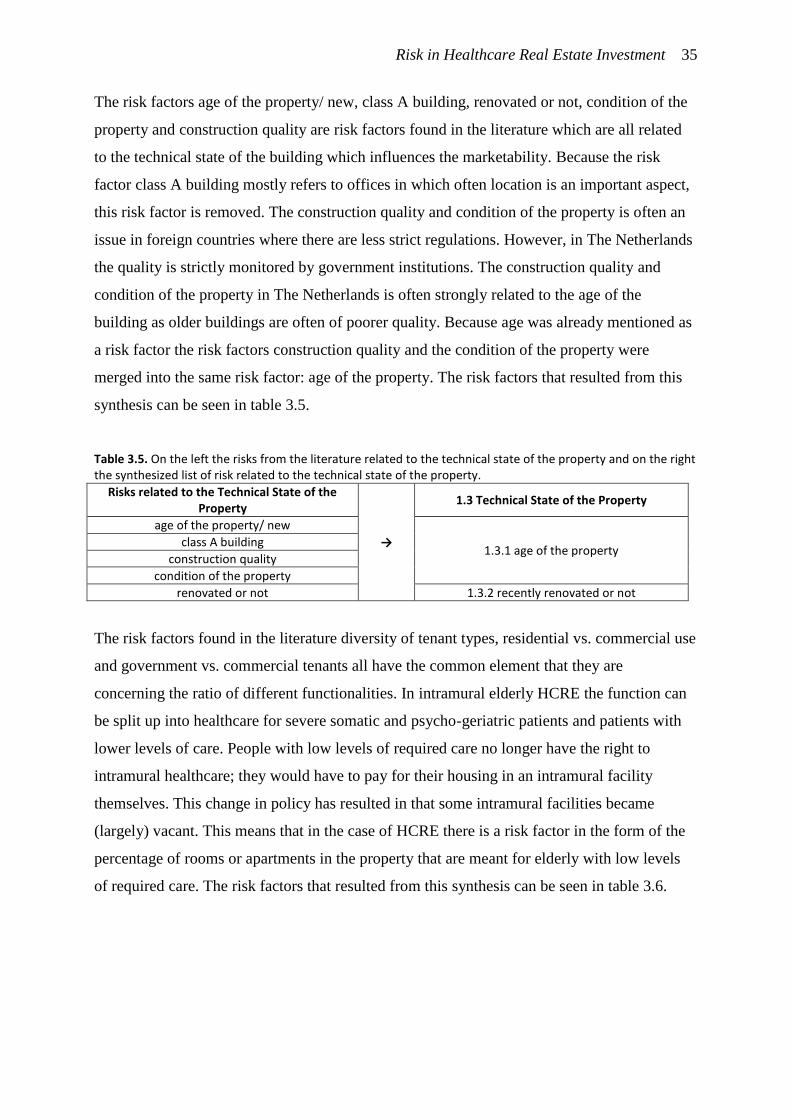
Risk in Healthcare Real Estate Investment 35
The risk factors age of the property/ new, class A building, renovated or not, condition of the
property and construction quality are risk factors found in the literature which are all related
to the technical state of the building which influences the marketability. Because the risk
factor class A building mostly refers to offices in which often location is an important aspect,
this risk factor is removed. The construction quality and condition of the property is often an
issue in foreign countries where there are less strict regulations. However, in The Netherlands
the quality is strictly monitored by government institutions. The construction quality and
condition of the property in The Netherlands is often strongly related to the age of the
building as older buildings are often of poorer quality. Because age was already mentioned as
a risk factor the risk factors construction quality and the condition of the property were
merged into the same risk factor: age of the property. The risk factors that resulted from this
synthesis can be seen in table 3.5.
Table 3.5. On the left the risks from the literature related to the technical state of the property and on the right the synthesized list of risk related to the technical state of the property.
Risks related to the Technical State of the Property
→
1.3 Technical State of the Property
age of the property/ new
1.3.1 age of the property class A building
construction quality
condition of the property
renovated or not 1.3.2 recently renovated or not
The risk factors found in the literature diversity of tenant types, residential vs. commercial use
and government vs. commercial tenants all have the common element that they are
concerning the ratio of different functionalities. In intramural elderly HCRE the function can
be split up into healthcare for severe somatic and psycho-geriatric patients and patients with
lower levels of care. People with low levels of required care no longer have the right to
intramural healthcare; they would have to pay for their housing in an intramural facility
themselves. This change in policy has resulted in that some intramural facilities became
(largely) vacant. This means that in the case of HCRE there is a risk factor in the form of the
percentage of rooms or apartments in the property that are meant for elderly with low levels
of required care. The risk factors that resulted from this synthesis can be seen in table 3.6.
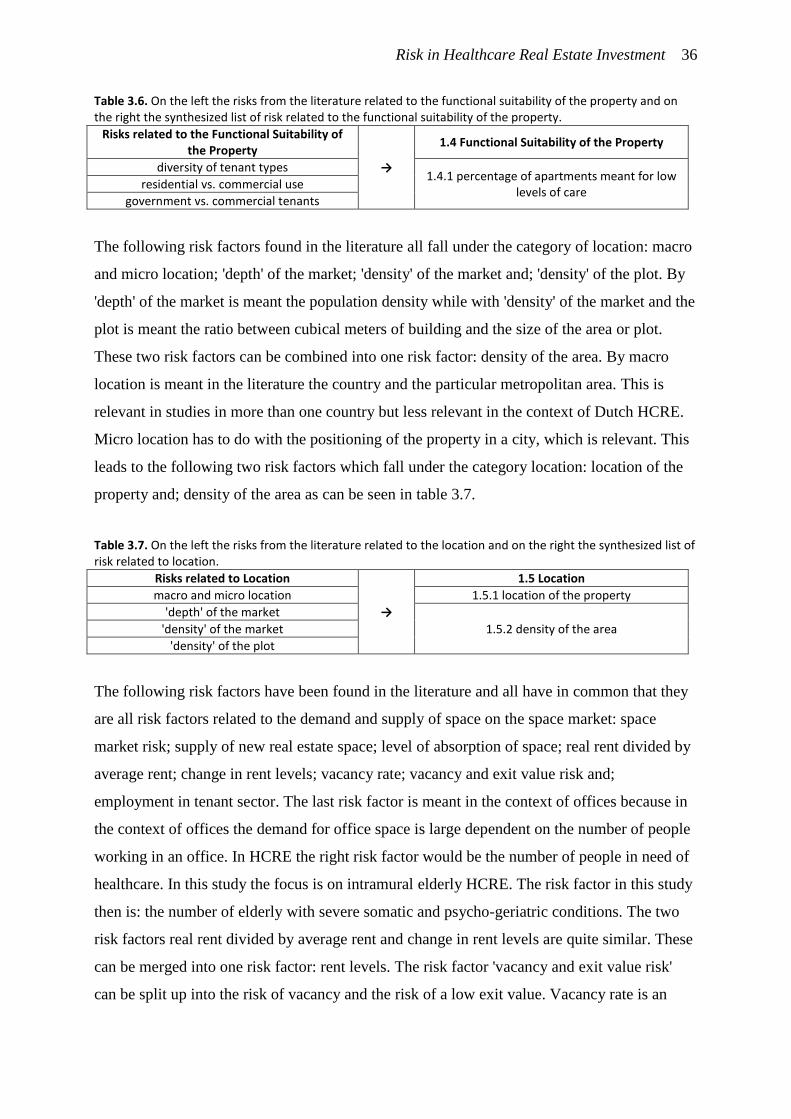
Risk in Healthcare Real Estate Investment 36
Table 3.6. On the left the risks from the literature related to the functional suitability of the property and on the right the synthesized list of risk related to the functional suitability of the property.
Risks related to the Functional Suitability of the Property
→
1.4 Functional Suitability of the Property
diversity of tenant types 1.4.1 percentage of apartments meant for low
levels of care residential vs. commercial use
government vs. commercial tenants
The following risk factors found in the literature all fall under the category of location: macro
and micro location; 'depth' of the market; 'density' of the market and; 'density' of the plot. By
'depth' of the market is meant the population density while with 'density' of the market and the
plot is meant the ratio between cubical meters of building and the size of the area or plot.
These two risk factors can be combined into one risk factor: density of the area. By macro
location is meant in the literature the country and the particular metropolitan area. This is
relevant in studies in more than one country but less relevant in the context of Dutch HCRE.
Micro location has to do with the positioning of the property in a city, which is relevant. This
leads to the following two risk factors which fall under the category location: location of the
property and; density of the area as can be seen in table 3.7.
Table 3.7. On the left the risks from the literature related to the location and on the right the synthesized list of risk related to location.
Risks related to Location
→
1.5 Location
macro and micro location 1.5.1 location of the property
'depth' of the market
1.5.2 density of the area 'density' of the market
'density' of the plot
The following risk factors have been found in the literature and all have in common that they
are all risk factors related to the demand and supply of space on the space market: space
market risk; supply of new real estate space; level of absorption of space; real rent divided by
average rent; change in rent levels; vacancy rate; vacancy and exit value risk and;
employment in tenant sector. The last risk factor is meant in the context of offices because in
the context of offices the demand for office space is large dependent on the number of people
working in an office. In HCRE the right risk factor would be the number of people in need of
healthcare. In this study the focus is on intramural elderly HCRE. The risk factor in this study
then is: the number of elderly with severe somatic and psycho-geriatric conditions. The two
risk factors real rent divided by average rent and change in rent levels are quite similar. These
can be merged into one risk factor: rent levels. The risk factor 'vacancy and exit value risk'
can be split up into the risk of vacancy and the risk of a low exit value. Vacancy rate is an
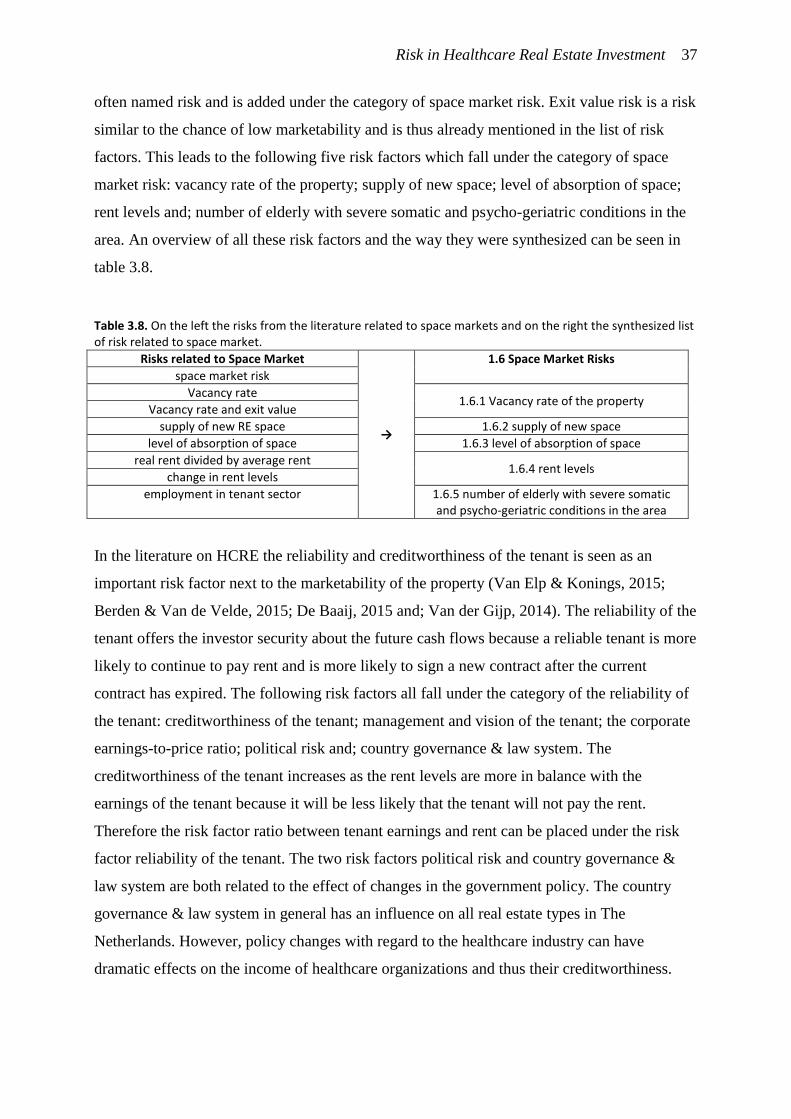
Risk in Healthcare Real Estate Investment 37
often named risk and is added under the category of space market risk. Exit value risk is a risk
similar to the chance of low marketability and is thus already mentioned in the list of risk
factors. This leads to the following five risk factors which fall under the category of space
market risk: vacancy rate of the property; supply of new space; level of absorption of space;
rent levels and; number of elderly with severe somatic and psycho-geriatric conditions in the
area. An overview of all these risk factors and the way they were synthesized can be seen in
table 3.8.
Table 3.8. On the left the risks from the literature related to space markets and on the right the synthesized list of risk related to space market.
Risks related to Space Market
→
1.6 Space Market Risks
space market risk
Vacancy rate 1.6.1 Vacancy rate of the property
Vacancy rate and exit value
supply of new RE space 1.6.2 supply of new space
level of absorption of space 1.6.3 level of absorption of space
real rent divided by average rent 1.6.4 rent levels
change in rent levels
employment in tenant sector 1.6.5 number of elderly with severe somatic and psycho-geriatric conditions in the area
In the literature on HCRE the reliability and creditworthiness of the tenant is seen as an
important risk factor next to the marketability of the property (Van Elp & Konings, 2015;
Berden & Van de Velde, 2015; De Baaij, 2015 and; Van der Gijp, 2014). The reliability of the
tenant offers the investor security about the future cash flows because a reliable tenant is more
likely to continue to pay rent and is more likely to sign a new contract after the current
contract has expired. The following risk factors all fall under the category of the reliability of
the tenant: creditworthiness of the tenant; management and vision of the tenant; the corporate
earnings-to-price ratio; political risk and; country governance & law system. The
creditworthiness of the tenant increases as the rent levels are more in balance with the
earnings of the tenant because it will be less likely that the tenant will not pay the rent.
Therefore the risk factor ratio between tenant earnings and rent can be placed under the risk
factor reliability of the tenant. The two risk factors political risk and country governance &
law system are both related to the effect of changes in the government policy. The country
governance & law system in general has an influence on all real estate types in The
Netherlands. However, policy changes with regard to the healthcare industry can have
dramatic effects on the income of healthcare organizations and thus their creditworthiness.

Risk in Healthcare Real Estate Investment 38
Therefore the two risk factors, political risk and country governance & law system, are added
as a risk factor in the form of 'government policy changes'.
The arguments above leads to the following list of risk factors related to the reliability
of the tenant: ratio between tenant earnings and rent; government policy changes;
creditworthiness of the tenant and; management and vision of the tenant.
An overview of all the risk factors and the way they were synthesized can be seen in
table 3.9.
Table 3.9. On the left the risks from the literature related to the reliability of the tenant and on the right the synthesized list of risk related to reliability of the tenant.
Risks related to Reliability of the Tenant
→
2 Reliability of the Tenant
creditworthiness of the tenant 2.1 creditworthiness of the tenant
the corporate earnings-to-price ratio 2.2 ratio between tenant earnings and rent
political risk 2.3 government policy changes
country governance & law system
management and vision of the tenant 2.4 management and vision of the tenant
The synthesis of the risk factors in the literature has reduced the number of risk factors to 24
risk factors distributed over 2 categories: marketability of the property and reliability of the
tenant. The marketability of the property has four sub-categories: market maturity risks;
technical state of the property; location and; space market changes. The entire synthesized
risk list can be seen in table 3.10.
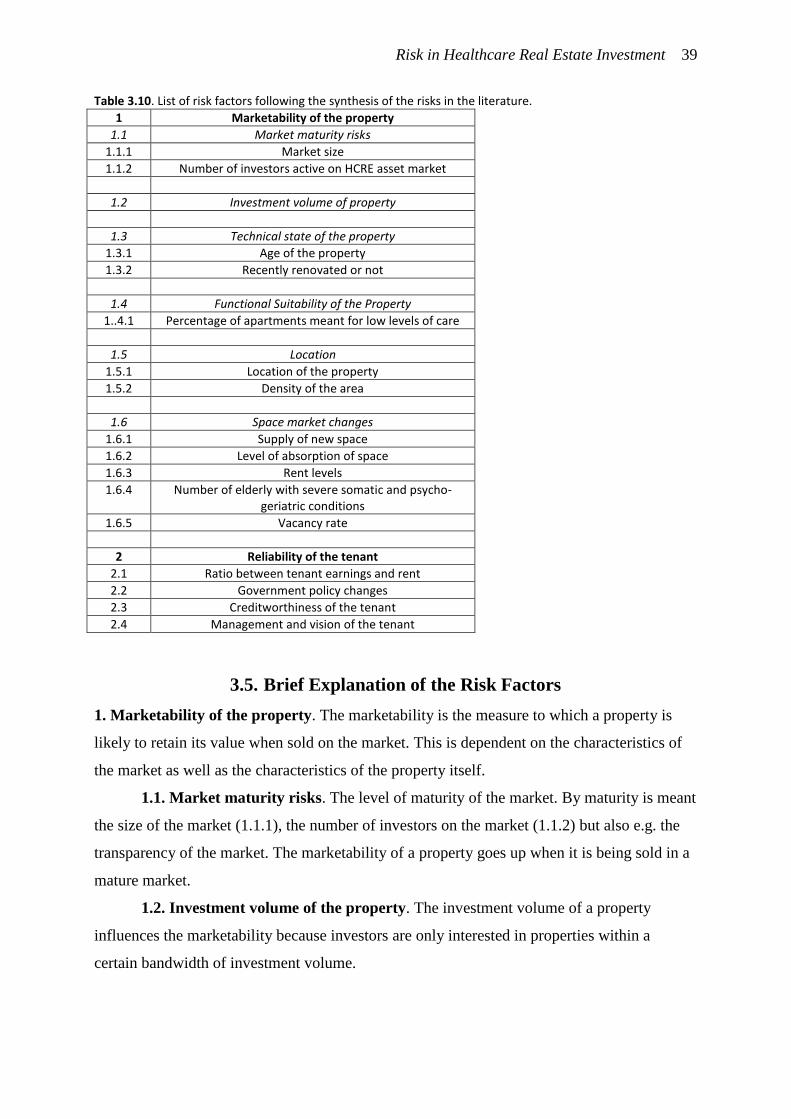
Risk in Healthcare Real Estate Investment 39
Table 3.10. List of risk factors following the synthesis of the risks in the literature.
1 Marketability of the property
1.1 Market maturity risks
1.1.1 Market size
1.1.2 Number of investors active on HCRE asset market
1.2 Investment volume of property
1.3 Technical state of the property
1.3.1 Age of the property
1.3.2 Recently renovated or not
1.4 Functional Suitability of the Property
1..4.1 Percentage of apartments meant for low levels of care
1.5 Location
1.5.1 Location of the property
1.5.2 Density of the area
1.6 Space market changes
1.6.1 Supply of new space
1.6.2 Level of absorption of space
1.6.3 Rent levels
1.6.4 Number of elderly with severe somatic and psycho-geriatric conditions
1.6.5 Vacancy rate
2 Reliability of the tenant
2.1 Ratio between tenant earnings and rent
2.2 Government policy changes
2.3 Creditworthiness of the tenant
2.4 Management and vision of the tenant
3.5. Brief Explanation of the Risk Factors
1. Marketability of the property. The marketability is the measure to which a property is
likely to retain its value when sold on the market. This is dependent on the characteristics of
the market as well as the characteristics of the property itself.
1.1. Market maturity risks. The level of maturity of the market. By maturity is meant
the size of the market (1.1.1), the number of investors on the market (1.1.2) but also e.g. the
transparency of the market. The marketability of a property goes up when it is being sold in a
mature market.
1.2. Investment volume of the property. The investment volume of a property
influences the marketability because investors are only interested in properties within a
certain bandwidth of investment volume.
Risk in Healthcare Real Estate Investment 40
1.3 Technical state of the property. The marketability of a property goes up as the
technical state of the building gets better because investors are usually only willing to invest
in new properties. The technical state of the property is largely influenced by the age of the
property (1.3.1) and whether the property was recently renovated or not (1.3.2).
1.4 Functional suitability of the property. This risk factor represents the risk that the
property is, or will become, partly unsuitable for the kind of function it needs to fulfill. The
kind of function it needs to fulfill can change over time, e.g. when the current tenant contract
ends and an alternative function needs to be found for the property. The measure to which the
property is flexible in its function increases the retention of value. In the case of HCRE
properties with the function of providing intramural care for people with low levels of
required care (1.4.1) are often partly vacant because low levels of care are no longer provided
intramurally; people with low levels of required care now receive services at home.
1.5 Location. The location influences the marketability of the property as properties in
a location with a small local market can only be offered to a small number of tenants. The
location of the property (1.5.1) is strongly related to the accessibility by for instance family
members who wish to visit the elderly in the intramural care facility. Furthermore, location
determines in what space market the property is situated and the density of the area (1.5.2).
1.6 Space market changes. This risk factor represents the chance that the demand for
space on the (local) market becomes lower than expected. This is dependent on the supply of
new space (1.6.1) by real estate developers and the absorption levels of space (1.6.2). A
changing equilibrium on the space market by changes in supply and demand will also result in
changing rent levels (1.6.3). In intramural elderly HCRE the demand for space is mostly
driven by the number of elderly with severe somatic and psycho-geriatric conditions (1.6.4).
Because the government regulates who is eligible for intramural elderly HCRE the
government also has an influence on the number of patients and thus the demand of space.
The risk factor vacancy rate (1.6.5) is another indicator for the shifts in the balance between
demand and supply on the space market. IF vacancy increases the balance will shift towards a
market with more supply than demand. In such market the value of property is likely to go
down.
2. Reliability of the tenant. The reliability of the tenant is the measure to which a tenant is
likely to continue to pay rent. From an investors perspective this factor determines the
stability and security of the future cash flows.
Risk in Healthcare Real Estate Investment 41
2.1 Ratio between tenant earnings and rent. This ratio shows to what extent the
tenant can withstand loss of earnings while still being able to pay rent. This is especially the
case when the government cuts costs on healthcare and healthcare organizations are forced to
offer the same services for less money.
2.2 Government policy changes. The government can make changes in the policies
related to healthcare funding. In the past this has resulted in less income for healthcare
organizations. Government policy changes thus influence the likelihood that the tenant will be
able to continue to pay rent.
2.3 Creditworthiness of the tenant. The creditworthiness of a tenant is the measure
of likelihood that the tenant will be able to pay off credit payments. This measure is similar to
the likelihood the tenant will be able to continue to pay rent.
2.4 Management and vision of the tenant. Besides creditworthiness an investor
should also look at the business plan and the quality of the management of the healthcare
organization. The creditworthiness of the tenant might be good at the moment, but with bad
management and vision this can easily change in the future.

Risk in Healthcare Real Estate Investment 42
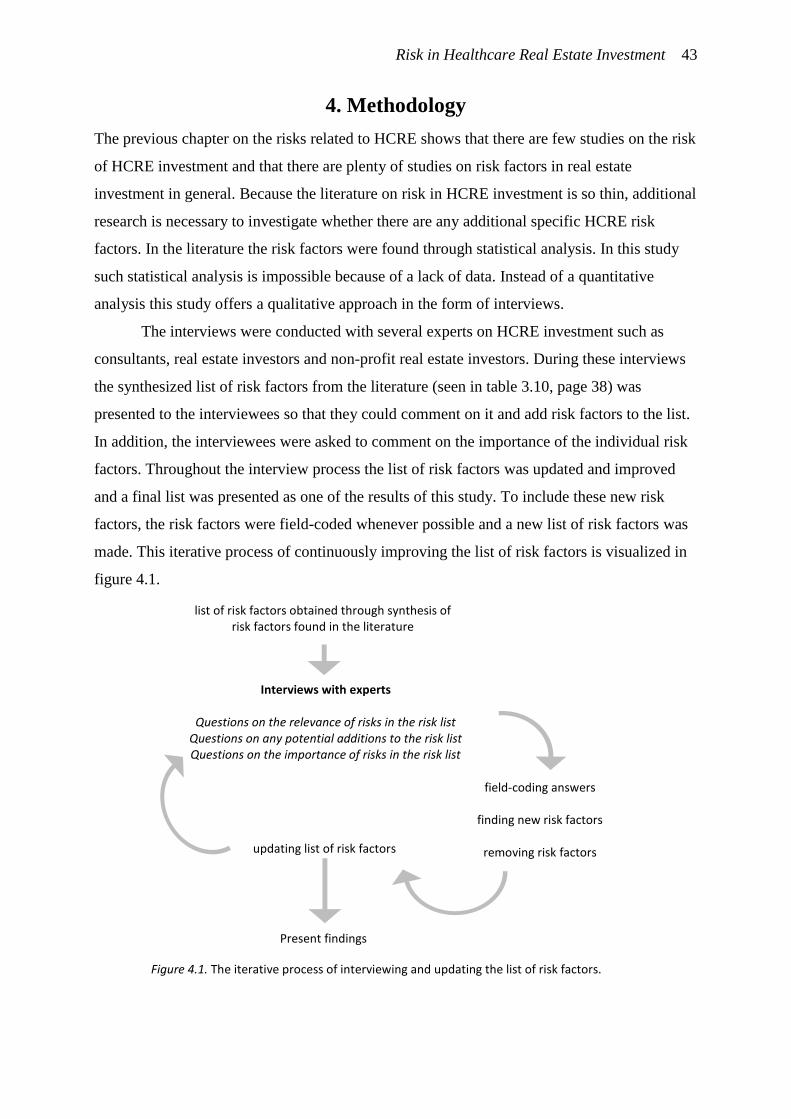
Risk in Healthcare Real Estate Investment 43
4. Methodology
The previous chapter on the risks related to HCRE shows that there are few studies on the risk
of HCRE investment and that there are plenty of studies on risk factors in real estate
investment in general. Because the literature on risk in HCRE investment is so thin, additional
research is necessary to investigate whether there are any additional specific HCRE risk
factors. In the literature the risk factors were found through statistical analysis. In this study
such statistical analysis is impossible because of a lack of data. Instead of a quantitative
analysis this study offers a qualitative approach in the form of interviews.
The interviews were conducted with several experts on HCRE investment such as
consultants, real estate investors and non-profit real estate investors. During these interviews
the synthesized list of risk factors from the literature (seen in table 3.10, page 38) was
presented to the interviewees so that they could comment on it and add risk factors to the list.
In addition, the interviewees were asked to comment on the importance of the individual risk
factors. Throughout the interview process the list of risk factors was updated and improved
and a final list was presented as one of the results of this study. To include these new risk
factors, the risk factors were field-coded whenever possible and a new list of risk factors was
made. This iterative process of continuously improving the list of risk factors is visualized in
figure 4.1.
Figure 4.1. The iterative process of interviewing and updating the list of risk factors.
list of risk factors obtained through synthesis of risk factors found in the literature
Present findings
updating list of risk factors
Interviews with experts
Questions on the relevance of risks in the risk list Questions on any potential additions to the risk list Questions on the importance of risks in the risk list
field-coding answers
finding new risk factors
removing risk factors
Risk in Healthcare Real Estate Investment 44
Figure 4.1 shows that throughout the interviews the list of risk factors was updated and at the
end of all the interviews the list was presented in this thesis. The interviews were done using
an interview guide.
4.1. Interview Guide
The interviews with the experts were conducted in the following manner. The experts were
asked to look at the list of risks, comment on it and perhaps remove or add any additional
risks. When an interviewee wished to add any risk factors the risk factor was first examined
and compared to the existing list in cooperation with the interviewee. If the risk factor was
similar to one of the existing ones it was not added. The interviewees were then asked to give
their opinion on the risk list with regard to the relevance and importance of the different risk
factors. The level of importance was measured using the following 7-point Likert scale based
on Vagias (2006): 1 – Not at all important; 2 – Low importance; 3 – Slightly important; 4 –
Neutral; 5 – Moderately important; 6 – Very important and; 7 – Extremely important. The
level of relative importance between the property risks and tenant risks were measured on a 9-
point scale as used in the Analytical Hierarchy Process (AHP) by Saaty (1990): 1 – equal; 3 –
moderately more; 5 – strongly more; 7 – very strongly more and; 9 – extremely more
important.
The interview guide was based on Emans (2002). The interview guide was tested on a
test respondent, using the cognitive interviewing technique of going through the entire
interview and at the same time evaluating the questions from the perspective of the
interviewee. Using the information obtained from this test a final version of the interview
guide was made, which can be seen in Appendix 2. Appendix 2 also includes a detailed
description of the way the interview guide was designed to improve objectivity during the
interviews.
4.2. Interviewee Selection
The experts that were interviewed consisted of 12 (non-profit) real estate investors, 7
consultants and 4 other experts. Both Dutch and Belgian investors were included in the
selection. There were 4 non-profit real estate investment organizations among the Dutch
investors. The exact characteristics of the different investors and consultants will remain
classified to ensure anonymity. An overview of the experts and, if applicable, the volume of
the fund they manage can be seen in table 4.1.
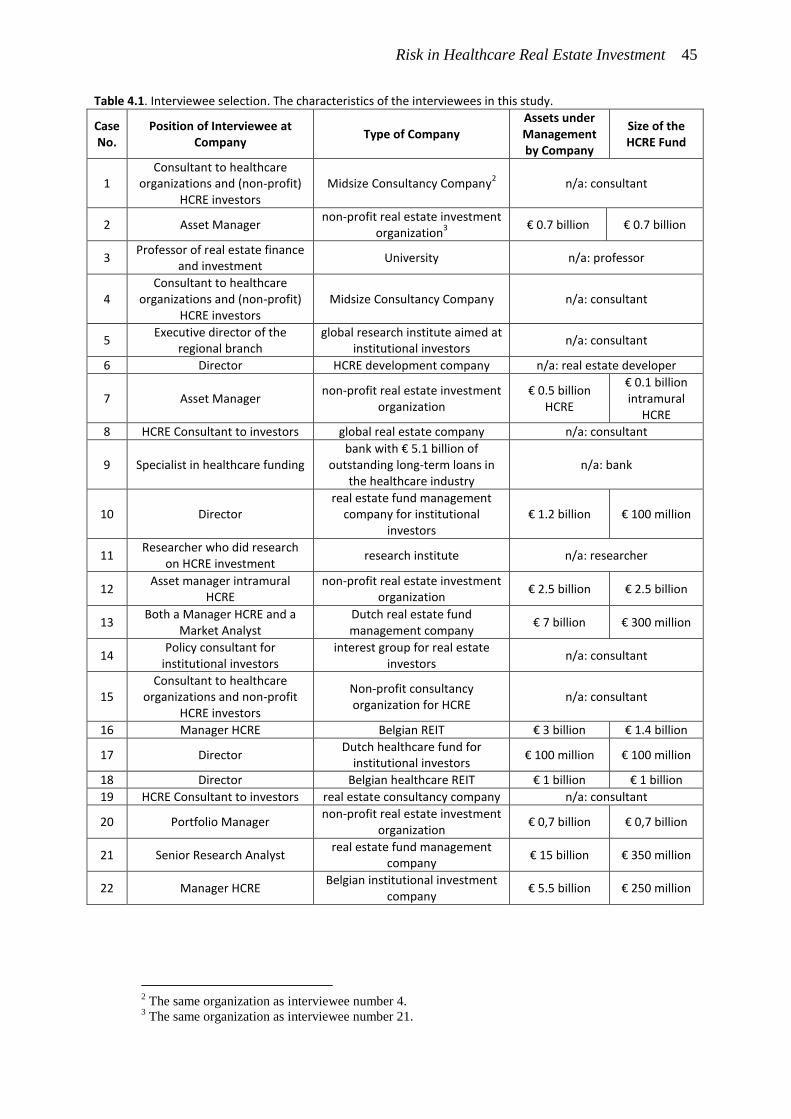
Risk in Healthcare Real Estate Investment 45
Table 4.1. Interviewee selection. The characteristics of the interviewees in this study.
Case No.
Position of Interviewee at Company
Type of Company Assets under Management by Company
Size of the HCRE Fund
1 Consultant to healthcare
organizations and (non-profit) HCRE investors
Midsize Consultancy Company2 n/a: consultant
2 Asset Manager non-profit real estate investment
organization3
€ 0.7 billion € 0.7 billion
3 Professor of real estate finance
and investment University n/a: professor
4 Consultant to healthcare
organizations and (non-profit) HCRE investors
Midsize Consultancy Company n/a: consultant
5 Executive director of the
regional branch global research institute aimed at
institutional investors n/a: consultant
6 Director HCRE development company n/a: real estate developer
7 Asset Manager non-profit real estate investment
organization € 0.5 billion
HCRE
€ 0.1 billion intramural
HCRE
8 HCRE Consultant to investors global real estate company n/a: consultant
9 Specialist in healthcare funding bank with € 5.1 billion of
outstanding long-term loans in the healthcare industry
n/a: bank
10 Director real estate fund management
company for institutional investors
€ 1.2 billion € 100 million
11 Researcher who did research
on HCRE investment research institute n/a: researcher
12 Asset manager intramural
HCRE non-profit real estate investment
organization € 2.5 billion € 2.5 billion
13 Both a Manager HCRE and a
Market Analyst Dutch real estate fund management company
€ 7 billion € 300 million
14 Policy consultant for
institutional investors interest group for real estate
investors n/a: consultant
15 Consultant to healthcare
organizations and non-profit HCRE investors
Non-profit consultancy organization for HCRE
n/a: consultant
16 Manager HCRE Belgian REIT € 3 billion € 1.4 billion
17 Director Dutch healthcare fund for
institutional investors € 100 million € 100 million
18 Director Belgian healthcare REIT € 1 billion € 1 billion
19 HCRE Consultant to investors real estate consultancy company n/a: consultant
20 Portfolio Manager non-profit real estate investment
organization € 0,7 billion € 0,7 billion
21 Senior Research Analyst real estate fund management
company € 15 billion € 350 million
22 Manager HCRE Belgian institutional investment
company € 5.5 billion € 250 million
2 The same organization as interviewee number 4.
3 The same organization as interviewee number 21.
Risk in Healthcare Real Estate Investment 46
Table 4.1 shows a wide variety of different experts. The experts were selected based on their
expertise on HCRE investment and their position at a company. To improve the spread of
viewpoints several different companies and organizations were included in the selection.
Virtually all companies who were invited for an interview agreed to participate in the study;
only one Dutch fund management company did not respond. Considering the small number of
investment companies active in HCRE the interviewees reflect a large part of the total
population.
4.3. Method of Analysis
Throughout the interviews and especially after the interviews the gathered qualitative and
quantitative data was analyzed using a systematic method: thematic analysis. After each
interview the data was examined to find patterns and themes. The large number of 22
interviews allowed for a strong development of pattern recognition. As the interviews
progressed the themes that were recognized could be familiarized and a deeper understanding
of the themes could be developed. During and after each interview the data was studied
carefully to become familiarized with it. At first it seemed the data did not show any patterns,
but as the interviews progressed similarities between interviews were found. During the
interviews short notes were made once new information was revealed or when a pattern
seemed to emerge. New themes and patterns that were discovered were noted or memorized
in order to analyze the most important themes in more detail at a later point. Once all
interviews were conducted and all data was collected the data was examined more closely on
several important themes. The themes that were found to have a meaningful scientific or
practical contribution and could be supported with enough proof were included in the results
of this study.
4.4. Description of the Field Work
The interviews were conducted on the basis of an interview guide which was designed for
interviews of roughly 30 minutes. In reality the interviews lasted vastly longer because most
interviewees were willing to invest extra time in sharing their knowledge and to provide
meaningful context to their answers. On average the interviews lasted 1 hour, excluding
introductory talks. In total over 20 hours were spend on detailed discussions on the subject
matter with 23 experts on HCRE.
The enthusiasm of the interviewees was shown at the moment they were addressed by
email to ask for their permission to conduct an interview. Only one company declined by not
Risk in Healthcare Real Estate Investment 47
responding while the other 23 experts agreed within three weeks to plan a meeting. All
interviews were planned in a period of five-and-a-half weeks. One interview had to be
rescheduled by three weeks because the interviewee was hindered.
The interviews went according to expectations with some exceptions. It was expected
that interviewees were able to come up with several risk factors and that risk factors that were
added by previous interviewees were recognized as such by the consecutive interviewees. The
list of risk factors grew longer as more interviews took place, indicating that interviewees at
the beginning of the process either forgot some risk factors or that risk factors that were added
at a later point in time were not relevant to them. In general it can be concluded from the data
that once a risk factor was added it was seen by others as relevant and that adding it to the list
was justifiable. Only a few risk factors were removed at a later point if an interviewee could
argue clearly the irrelevance. In total 66 risk factors were added by interviewees, 14 were
changed, 8 were synthesized or merged, 6 were removed and 2 were moved on the list. The
precise evolution of the list of risk factors can be found in appendix 3. In appendix 3 shows
which interviewee suggested to add, change or remove which risk factor.
During the interviews it became clear that interviewees were hesitant in calling a risk
factor irrelevant or less important. For this reason the risk factors tend to be asymmetrically
rated for importance with a tendency towards considering risk factors more important as
opposed to less important. Although this was in line with expectations, the Likert scale that
was used was symmetrical. The results suggest that all risk factors are often moderately
important or very important. Therefore a qualitative analysis of the data was necessary to find
indicators of the importance of the risk factors.
Some interviews did not go entirely as expected. One interviewee was able to discuss
the relevance of the risk factors and was able to add risk factors but due to a lack of time was
unable to rate the importance of the risk factors. Some interviewees had difficulty filling in
the scores because of indecisiveness. However, most interviewees were able to express their
standpoints very clearly. Only one interviewee (a specialist at a bank) was unable to respond
to the questions of the interview guide because he was unable to take on the perspective of a
real estate investor. As a specialist on healthcare working at a bank he could only take on the
perspective of a bank. Nonetheless, this interview was very helpful because it gave insight in
the perspective of banks on funding healthcare organizations. The interviewee explained how
banks fund healthcare organizations and how risk management of banks has similarities with
some real estate investors.

Risk in Healthcare Real Estate Investment 48
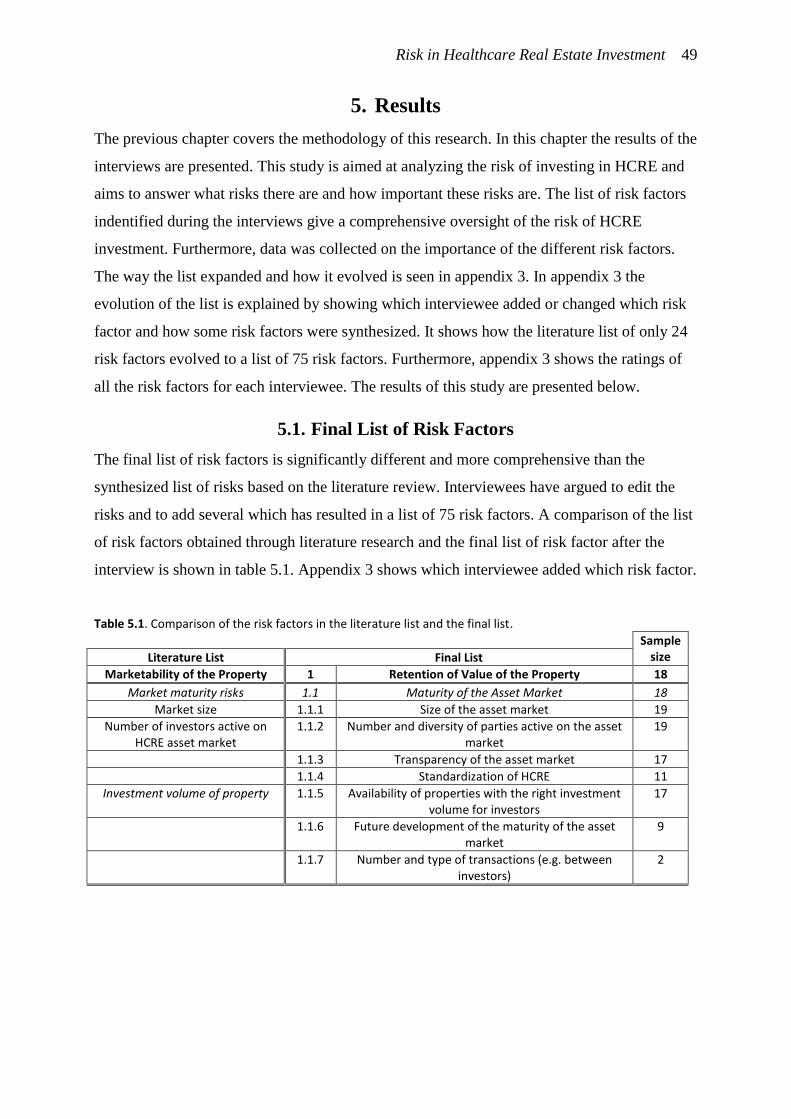
Risk in Healthcare Real Estate Investment 49
5. Results
The previous chapter covers the methodology of this research. In this chapter the results of the
interviews are presented. This study is aimed at analyzing the risk of investing in HCRE and
aims to answer what risks there are and how important these risks are. The list of risk factors
indentified during the interviews give a comprehensive oversight of the risk of HCRE
investment. Furthermore, data was collected on the importance of the different risk factors.
The way the list expanded and how it evolved is seen in appendix 3. In appendix 3 the
evolution of the list is explained by showing which interviewee added or changed which risk
factor and how some risk factors were synthesized. It shows how the literature list of only 24
risk factors evolved to a list of 75 risk factors. Furthermore, appendix 3 shows the ratings of
all the risk factors for each interviewee. The results of this study are presented below.
5.1. Final List of Risk Factors
The final list of risk factors is significantly different and more comprehensive than the
synthesized list of risks based on the literature review. Interviewees have argued to edit the
risks and to add several which has resulted in a list of 75 risk factors. A comparison of the list
of risk factors obtained through literature research and the final list of risk factor after the
interview is shown in table 5.1. Appendix 3 shows which interviewee added which risk factor.
Table 5.1. Comparison of the risk factors in the literature list and the final list.
Sample size Literature List Final List
Marketability of the Property 1 Retention of Value of the Property 18
Market maturity risks 1.1 Maturity of the Asset Market 18
Market size 1.1.1 Size of the asset market 19
Number of investors active on HCRE asset market
1.1.2 Number and diversity of parties active on the asset market
19
1.1.3 Transparency of the asset market 17
1.1.4 Standardization of HCRE 11
Investment volume of property 1.1.5 Availability of properties with the right investment volume for investors
17
1.1.6 Future development of the maturity of the asset market
9
1.1.7 Number and type of transactions (e.g. between investors)
2
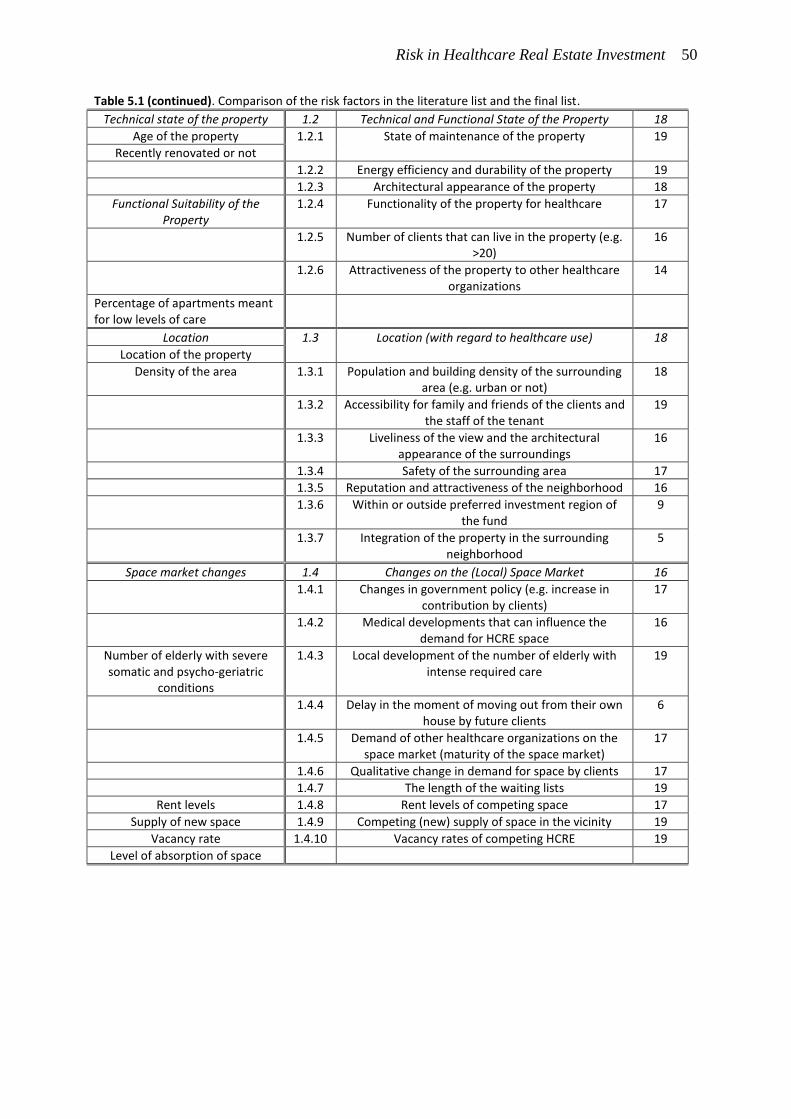
Risk in Healthcare Real Estate Investment 50
Table 5.1 (continued). Comparison of the risk factors in the literature list and the final list.
Technical state of the property 1.2 Technical and Functional State of the Property 18
Age of the property 1.2.1 State of maintenance of the property 19
Recently renovated or not
1.2.2 Energy efficiency and durability of the property 19
1.2.3 Architectural appearance of the property 18
Functional Suitability of the Property
1.2.4 Functionality of the property for healthcare 17
1.2.5 Number of clients that can live in the property (e.g. >20)
16
1.2.6 Attractiveness of the property to other healthcare organizations
14
Percentage of apartments meant for low levels of care
Location 1.3 Location (with regard to healthcare use) 18
Location of the property
Density of the area 1.3.1 Population and building density of the surrounding area (e.g. urban or not)
18
1.3.2 Accessibility for family and friends of the clients and the staff of the tenant
19
1.3.3 Liveliness of the view and the architectural appearance of the surroundings
16
1.3.4 Safety of the surrounding area 17
1.3.5 Reputation and attractiveness of the neighborhood 16
1.3.6 Within or outside preferred investment region of the fund
9
1.3.7 Integration of the property in the surrounding neighborhood
5
Space market changes 1.4 Changes on the (Local) Space Market 16
1.4.1 Changes in government policy (e.g. increase in contribution by clients)
17
1.4.2 Medical developments that can influence the demand for HCRE space
16
Number of elderly with severe somatic and psycho-geriatric
conditions
1.4.3 Local development of the number of elderly with intense required care
19
1.4.4 Delay in the moment of moving out from their own house by future clients
6
1.4.5 Demand of other healthcare organizations on the space market (maturity of the space market)
17
1.4.6 Qualitative change in demand for space by clients 17
1.4.7 The length of the waiting lists 19
Rent levels 1.4.8 Rent levels of competing space 17
Supply of new space 1.4.9 Competing (new) supply of space in the vicinity 19
Vacancy rate 1.4.10 Vacancy rates of competing HCRE 19
Level of absorption of space
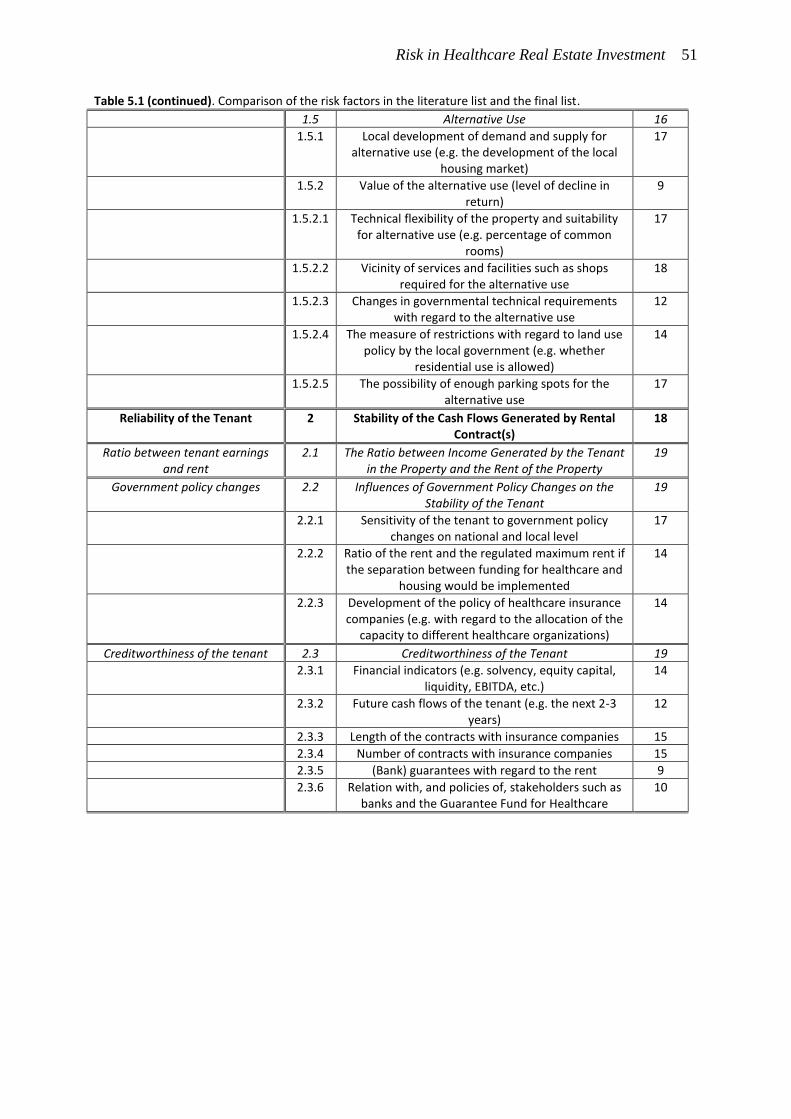
Risk in Healthcare Real Estate Investment 51
Table 5.1 (continued). Comparison of the risk factors in the literature list and the final list.
1.5 Alternative Use 16
1.5.1 Local development of demand and supply for alternative use (e.g. the development of the local
housing market)
17
1.5.2 Value of the alternative use (level of decline in return)
9
1.5.2.1 Technical flexibility of the property and suitability for alternative use (e.g. percentage of common
rooms)
17
1.5.2.2 Vicinity of services and facilities such as shops required for the alternative use
18
1.5.2.3 Changes in governmental technical requirements with regard to the alternative use
12
1.5.2.4 The measure of restrictions with regard to land use policy by the local government (e.g. whether
residential use is allowed)
14
1.5.2.5 The possibility of enough parking spots for the alternative use
17
Reliability of the Tenant 2 Stability of the Cash Flows Generated by Rental Contract(s)
18
Ratio between tenant earnings and rent
2.1 The Ratio between Income Generated by the Tenant in the Property and the Rent of the Property
19
Government policy changes 2.2 Influences of Government Policy Changes on the Stability of the Tenant
19
2.2.1 Sensitivity of the tenant to government policy changes on national and local level
17
2.2.2 Ratio of the rent and the regulated maximum rent if the separation between funding for healthcare and
housing would be implemented
14
2.2.3 Development of the policy of healthcare insurance companies (e.g. with regard to the allocation of the
capacity to different healthcare organizations)
14
Creditworthiness of the tenant 2.3 Creditworthiness of the Tenant 19
2.3.1 Financial indicators (e.g. solvency, equity capital, liquidity, EBITDA, etc.)
14
2.3.2 Future cash flows of the tenant (e.g. the next 2-3 years)
12
2.3.3 Length of the contracts with insurance companies 15
2.3.4 Number of contracts with insurance companies 15
2.3.5 (Bank) guarantees with regard to the rent 9
2.3.6 Relation with, and policies of, stakeholders such as banks and the Guarantee Fund for Healthcare
10
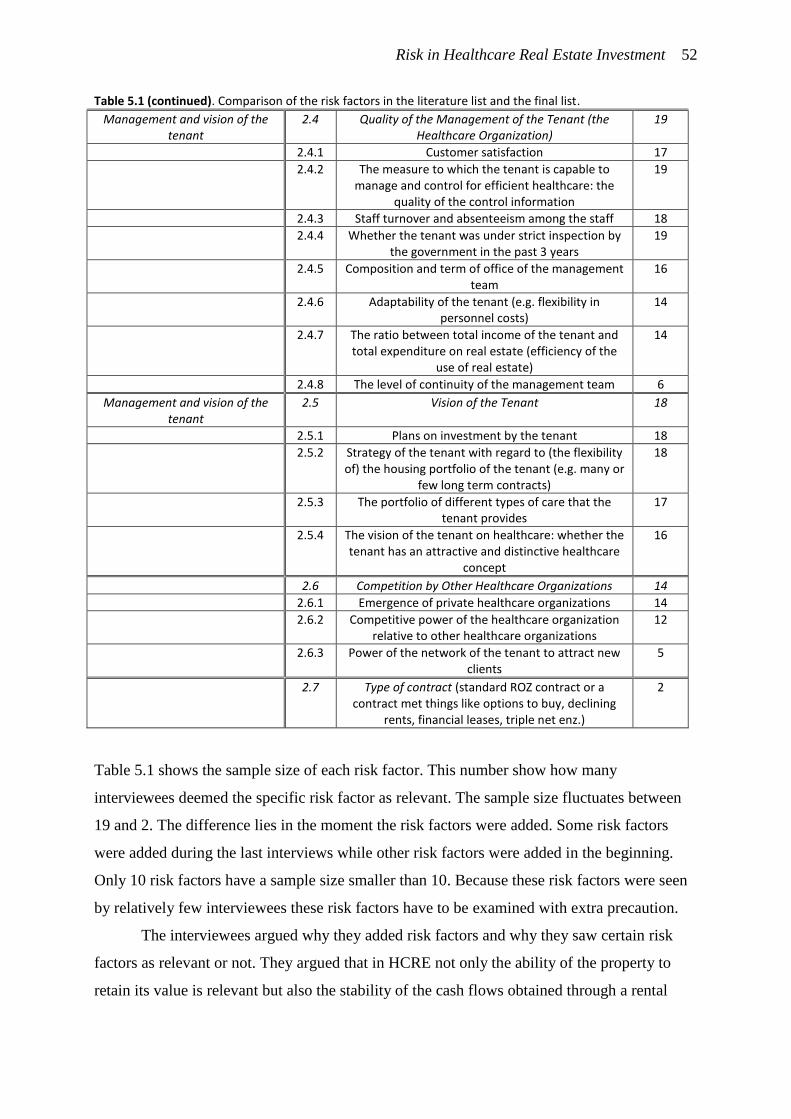
Risk in Healthcare Real Estate Investment 52
Table 5.1 (continued). Comparison of the risk factors in the literature list and the final list.
Management and vision of the tenant
2.4 Quality of the Management of the Tenant (the Healthcare Organization)
19
2.4.1 Customer satisfaction 17
2.4.2 The measure to which the tenant is capable to manage and control for efficient healthcare: the
quality of the control information
19
2.4.3 Staff turnover and absenteeism among the staff 18
2.4.4 Whether the tenant was under strict inspection by the government in the past 3 years
19
2.4.5 Composition and term of office of the management team
16
2.4.6 Adaptability of the tenant (e.g. flexibility in personnel costs)
14
2.4.7 The ratio between total income of the tenant and total expenditure on real estate (efficiency of the
use of real estate)
14
2.4.8 The level of continuity of the management team 6
Management and vision of the tenant
2.5 Vision of the Tenant 18
2.5.1 Plans on investment by the tenant 18
2.5.2 Strategy of the tenant with regard to (the flexibility of) the housing portfolio of the tenant (e.g. many or
few long term contracts)
18
2.5.3 The portfolio of different types of care that the tenant provides
17
2.5.4 The vision of the tenant on healthcare: whether the tenant has an attractive and distinctive healthcare
concept
16
2.6 Competition by Other Healthcare Organizations 14
2.6.1 Emergence of private healthcare organizations 14
2.6.2 Competitive power of the healthcare organization relative to other healthcare organizations
12
2.6.3 Power of the network of the tenant to attract new clients
5
2.7 Type of contract (standard ROZ contract or a contract met things like options to buy, declining
rents, financial leases, triple net enz.)
2
Table 5.1 shows the sample size of each risk factor. This number show how many
interviewees deemed the specific risk factor as relevant. The sample size fluctuates between
19 and 2. The difference lies in the moment the risk factors were added. Some risk factors
were added during the last interviews while other risk factors were added in the beginning.
Only 10 risk factors have a sample size smaller than 10. Because these risk factors were seen
by relatively few interviewees these risk factors have to be examined with extra precaution.
The interviewees argued why they added risk factors and why they saw certain risk
factors as relevant or not. They argued that in HCRE not only the ability of the property to
retain its value is relevant but also the stability of the cash flows obtained through a rental
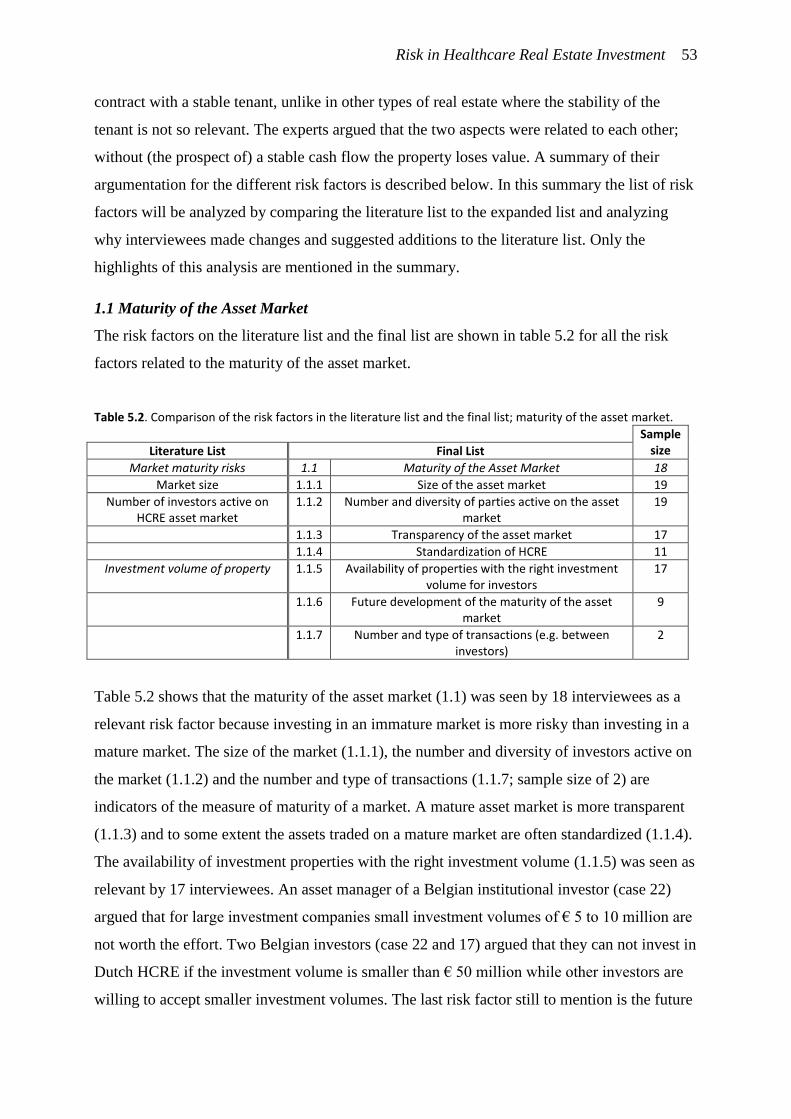
Risk in Healthcare Real Estate Investment 53
contract with a stable tenant, unlike in other types of real estate where the stability of the
tenant is not so relevant. The experts argued that the two aspects were related to each other;
without (the prospect of) a stable cash flow the property loses value. A summary of their
argumentation for the different risk factors is described below. In this summary the list of risk
factors will be analyzed by comparing the literature list to the expanded list and analyzing
why interviewees made changes and suggested additions to the literature list. Only the
highlights of this analysis are mentioned in the summary.
1.1 Maturity of the Asset Market
The risk factors on the literature list and the final list are shown in table 5.2 for all the risk
factors related to the maturity of the asset market.
Table 5.2. Comparison of the risk factors in the literature list and the final list; maturity of the asset market.
Sample size Literature List Final List
Market maturity risks 1.1 Maturity of the Asset Market 18
Market size 1.1.1 Size of the asset market 19
Number of investors active on HCRE asset market
1.1.2 Number and diversity of parties active on the asset market
19
1.1.3 Transparency of the asset market 17
1.1.4 Standardization of HCRE 11
Investment volume of property 1.1.5 Availability of properties with the right investment volume for investors
17
1.1.6 Future development of the maturity of the asset market
9
1.1.7 Number and type of transactions (e.g. between investors)
2
Table 5.2 shows that the maturity of the asset market (1.1) was seen by 18 interviewees as a
relevant risk factor because investing in an immature market is more risky than investing in a
mature market. The size of the market (1.1.1), the number and diversity of investors active on
the market (1.1.2) and the number and type of transactions (1.1.7; sample size of 2) are
indicators of the measure of maturity of a market. A mature asset market is more transparent
(1.1.3) and to some extent the assets traded on a mature market are often standardized (1.1.4).
The availability of investment properties with the right investment volume (1.1.5) was seen as
relevant by 17 interviewees. An asset manager of a Belgian institutional investor (case 22)
argued that for large investment companies small investment volumes of € 5 to 10 million are
not worth the effort. Two Belgian investors (case 22 and 17) argued that they can not invest in
Dutch HCRE if the investment volume is smaller than € 50 million while other investors are
willing to accept smaller investment volumes. The last risk factor still to mention is the future
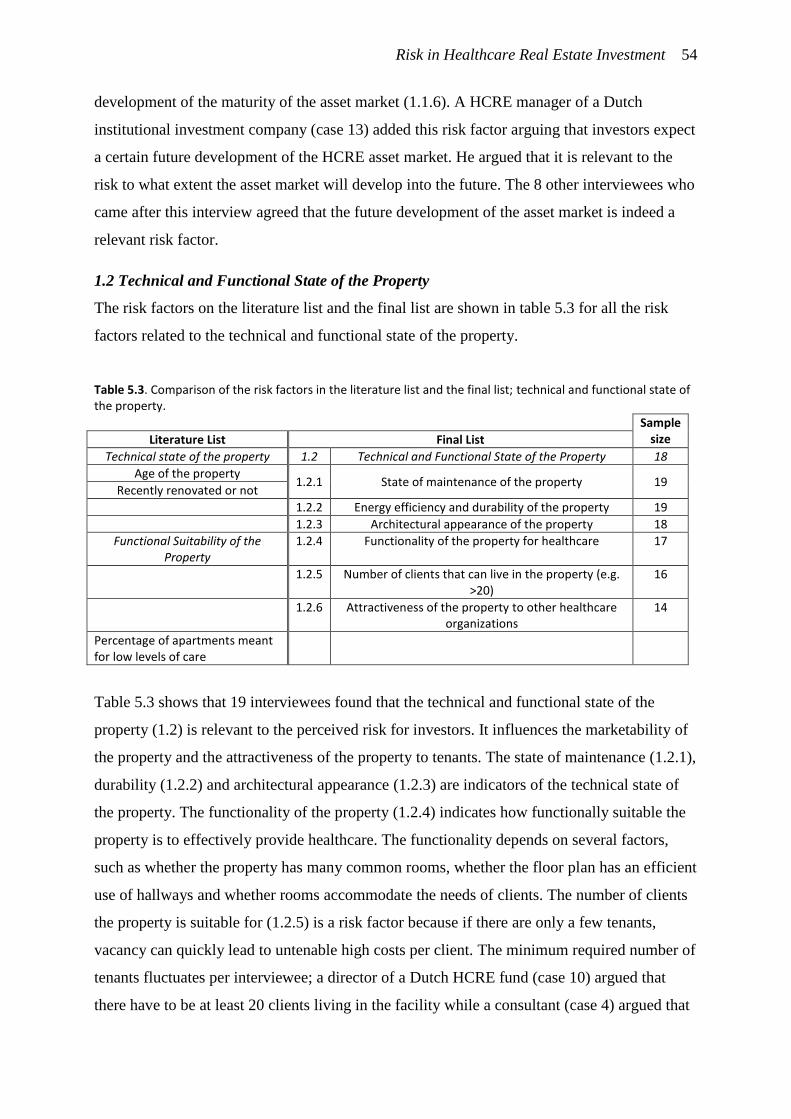
Risk in Healthcare Real Estate Investment 54
development of the maturity of the asset market (1.1.6). A HCRE manager of a Dutch
institutional investment company (case 13) added this risk factor arguing that investors expect
a certain future development of the HCRE asset market. He argued that it is relevant to the
risk to what extent the asset market will develop into the future. The 8 other interviewees who
came after this interview agreed that the future development of the asset market is indeed a
relevant risk factor.
1.2 Technical and Functional State of the Property
The risk factors on the literature list and the final list are shown in table 5.3 for all the risk
factors related to the technical and functional state of the property.
Table 5.3. Comparison of the risk factors in the literature list and the final list; technical and functional state of the property.
Sample size Literature List Final List
Technical state of the property 1.2 Technical and Functional State of the Property 18
Age of the property 1.2.1 State of maintenance of the property 19
Recently renovated or not
1.2.2 Energy efficiency and durability of the property 19
1.2.3 Architectural appearance of the property 18
Functional Suitability of the Property
1.2.4 Functionality of the property for healthcare 17
1.2.5 Number of clients that can live in the property (e.g. >20)
16
1.2.6 Attractiveness of the property to other healthcare organizations
14
Percentage of apartments meant for low levels of care
Table 5.3 shows that 19 interviewees found that the technical and functional state of the
property (1.2) is relevant to the perceived risk for investors. It influences the marketability of
the property and the attractiveness of the property to tenants. The state of maintenance (1.2.1),
durability (1.2.2) and architectural appearance (1.2.3) are indicators of the technical state of
the property. The functionality of the property (1.2.4) indicates how functionally suitable the
property is to effectively provide healthcare. The functionality depends on several factors,
such as whether the property has many common rooms, whether the floor plan has an efficient
use of hallways and whether rooms accommodate the needs of clients. The number of clients
the property is suitable for (1.2.5) is a risk factor because if there are only a few tenants,
vacancy can quickly lead to untenable high costs per client. The minimum required number of
tenants fluctuates per interviewee; a director of a Dutch HCRE fund (case 10) argued that
there have to be at least 20 clients living in the facility while a consultant (case 4) argued that

Risk in Healthcare Real Estate Investment 55
at least 120 clients would be enough for the property to function properly. The preferred
number of clients lies above 50 in most cases. The last risk factor that was added is the
attractiveness of the property to other potential tenants (1.2.6). As an asset manager for
intramural HCRE at a non-profit investment company (case 12) argued: some properties are
specifically designed for one particular healthcare organization. Such a property is less
attractive for other potential tenants, resulting in an increase in risk. In the original literature
list there is a risk factor (percentage of apartments meant for low levels of care) who was
removed immediately after the first interview with a consultant (case 1). This risk refers to
existing properties in which both intense care (skilled nursing and memory care) and low
levels of care are offered to the clients. Recent policy changes have made intramural HCRE
for low levels of care more risky because it lead to vacancy. The interviewed consultant could
argue why this risk factor was no longer relevant. He argued that the changes in the healthcare
industry already took place and that this risk factor is no longer relevant.
1.3 Location
The risk factors on the literature list and the final list are shown in table 5.4 for all the risk
factors related to the location.
Table 5.4. Comparison of the risk factors in the literature list and the final list; location.
Sample size Literature List Final List
Location 1.3 Location (with regard to healthcare use) 18
Location of the property
Density of the area 1.3.1 Population and building density of the surrounding area (e.g. urban or not)
18
1.3.2 Accessibility for family and friends of the clients and the staff of the tenant
19
1.3.3 Liveliness of the view and the architectural appearance of the surroundings
16
1.3.4 Safety of the surrounding area 17
1.3.5 Reputation and attractiveness of the neighborhood 16
1.3.6 Within or outside preferred investment region of the fund
9
1.3.7 Integration of the property in the surrounding neighborhood
5
Table 5.4 shows that location (1.3) is seen by 18 interviewees as a risk factor for the obvious
reason that the location determines local market conditions, alternative use options and
whether the property is suitable for its original intent; to provide healthcare services in. The
choice was made to split up the local market conditions, alternative use and location in the list
of risk, although these risk factors are interconnected. The interviewees added several sub-risk
Risk in Healthcare Real Estate Investment 56
factors related to the physical location of the property. Whether the location is in an urban
setting or a rural setting (1.3.1) was seen as a relevant risk factor by 18 interviewees. A HCRE
manager of an institutional investment company (case 13) argued that a higher density is less
risky and less volatile while an asset manager of a Belgian institutional investment company
(case 22) argued that the density of the area is less relevant and that elderly care facilities in
rural areas can attract clients from over a larger distances because people in rural areas are
willing to travel further. Furthermore, several attributes of the location were added as risk
factors such as accessibility (1.3.2), safety (1.3.4) and reputation and attractiveness of the area
(1.3.5). The liveliness of the view and the attractiveness of the surroundings (1.3.3) were
argued to be relevant by 16 interviewees because it represents value to clients and thereby
decreases the risk of vacancy. Integration of the care facility in the neighborhood (1.3.7) was
added by a director of a Dutch HCRE fund (case 17) arguing that it ensures a more lively
view and more attractive surroundings. He and a consultant (case 4) added that a lively view
is valuable for clients, who most often stay inside. Furthermore, many interviewees (such as a
consultant [case 4] and a director of a Belgian REIT [case 18]) argued that the children of the
clients are an important stakeholder in the decision making process when a new client moves
to a care facility. Some investors, as argued by a HCRE manager at an institutional investment
company (case 13) and a senior research analyst at an other institution fund management
company (case 21) consider whether the location fits within the core regions of the fund plan
of the investment company (1.3.6) a relevant risk factor, while others (such as a director of a
Dutch HCRE fund [case 17]), who do not work with core regions, see this risk factor as
irrelevant. Investors who work with core regions argue that core regions represent a general
selection of locations with less risk. Core regions represent regions with better alternative use
options and a stable and growing demand for HCRE.
1.4 Changes on the (Local) Space Market
The risk factors on the literature list and the final list are shown in table 5.5 for all the risk
factors related to the (local) space market.
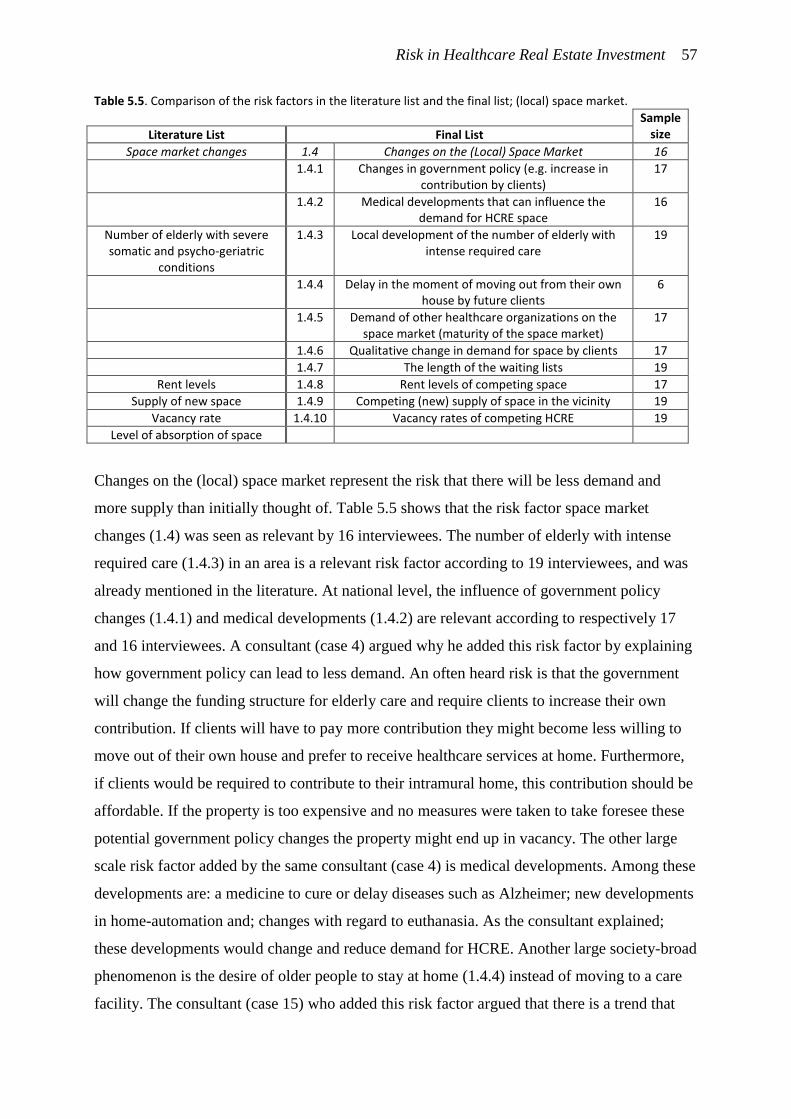
Risk in Healthcare Real Estate Investment 57
Table 5.5. Comparison of the risk factors in the literature list and the final list; (local) space market.
Sample size Literature List Final List
Space market changes 1.4 Changes on the (Local) Space Market 16
1.4.1 Changes in government policy (e.g. increase in contribution by clients)
17
1.4.2 Medical developments that can influence the demand for HCRE space
16
Number of elderly with severe somatic and psycho-geriatric
conditions
1.4.3 Local development of the number of elderly with intense required care
19
1.4.4 Delay in the moment of moving out from their own house by future clients
6
1.4.5 Demand of other healthcare organizations on the space market (maturity of the space market)
17
1.4.6 Qualitative change in demand for space by clients 17
1.4.7 The length of the waiting lists 19
Rent levels 1.4.8 Rent levels of competing space 17
Supply of new space 1.4.9 Competing (new) supply of space in the vicinity 19
Vacancy rate 1.4.10 Vacancy rates of competing HCRE 19
Level of absorption of space
Changes on the (local) space market represent the risk that there will be less demand and
more supply than initially thought of. Table 5.5 shows that the risk factor space market
changes (1.4) was seen as relevant by 16 interviewees. The number of elderly with intense
required care (1.4.3) in an area is a relevant risk factor according to 19 interviewees, and was
already mentioned in the literature. At national level, the influence of government policy
changes (1.4.1) and medical developments (1.4.2) are relevant according to respectively 17
and 16 interviewees. A consultant (case 4) argued why he added this risk factor by explaining
how government policy can lead to less demand. An often heard risk is that the government
will change the funding structure for elderly care and require clients to increase their own
contribution. If clients will have to pay more contribution they might become less willing to
move out of their own house and prefer to receive healthcare services at home. Furthermore,
if clients would be required to contribute to their intramural home, this contribution should be
affordable. If the property is too expensive and no measures were taken to take foresee these
potential government policy changes the property might end up in vacancy. The other large
scale risk factor added by the same consultant (case 4) is medical developments. Among these
developments are: a medicine to cure or delay diseases such as Alzheimer; new developments
in home-automation and; changes with regard to euthanasia. As the consultant explained;
these developments would change and reduce demand for HCRE. Another large society-broad
phenomenon is the desire of older people to stay at home (1.4.4) instead of moving to a care
facility. The consultant (case 15) who added this risk factor argued that there is a trend that
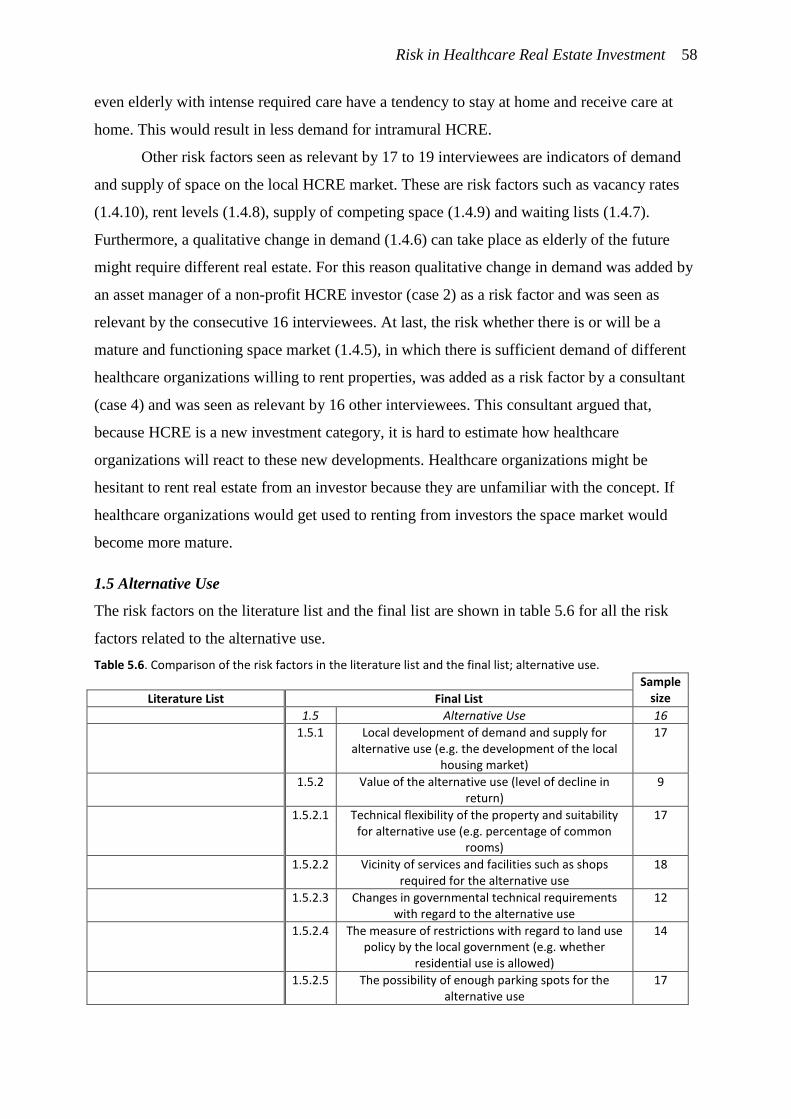
Risk in Healthcare Real Estate Investment 58
even elderly with intense required care have a tendency to stay at home and receive care at
home. This would result in less demand for intramural HCRE.
Other risk factors seen as relevant by 17 to 19 interviewees are indicators of demand
and supply of space on the local HCRE market. These are risk factors such as vacancy rates
(1.4.10), rent levels (1.4.8), supply of competing space (1.4.9) and waiting lists (1.4.7).
Furthermore, a qualitative change in demand (1.4.6) can take place as elderly of the future
might require different real estate. For this reason qualitative change in demand was added by
an asset manager of a non-profit HCRE investor (case 2) as a risk factor and was seen as
relevant by the consecutive 16 interviewees. At last, the risk whether there is or will be a
mature and functioning space market (1.4.5), in which there is sufficient demand of different
healthcare organizations willing to rent properties, was added as a risk factor by a consultant
(case 4) and was seen as relevant by 16 other interviewees. This consultant argued that,
because HCRE is a new investment category, it is hard to estimate how healthcare
organizations will react to these new developments. Healthcare organizations might be
hesitant to rent real estate from an investor because they are unfamiliar with the concept. If
healthcare organizations would get used to renting from investors the space market would
become more mature.
1.5 Alternative Use
The risk factors on the literature list and the final list are shown in table 5.6 for all the risk
factors related to the alternative use.
Table 5.6. Comparison of the risk factors in the literature list and the final list; alternative use.
Sample size Literature List Final List
1.5 Alternative Use 16
1.5.1 Local development of demand and supply for alternative use (e.g. the development of the local
housing market)
17
1.5.2 Value of the alternative use (level of decline in return)
9
1.5.2.1 Technical flexibility of the property and suitability for alternative use (e.g. percentage of common
rooms)
17
1.5.2.2 Vicinity of services and facilities such as shops required for the alternative use
18
1.5.2.3 Changes in governmental technical requirements with regard to the alternative use
12
1.5.2.4 The measure of restrictions with regard to land use policy by the local government (e.g. whether
residential use is allowed)
14
1.5.2.5 The possibility of enough parking spots for the alternative use
17
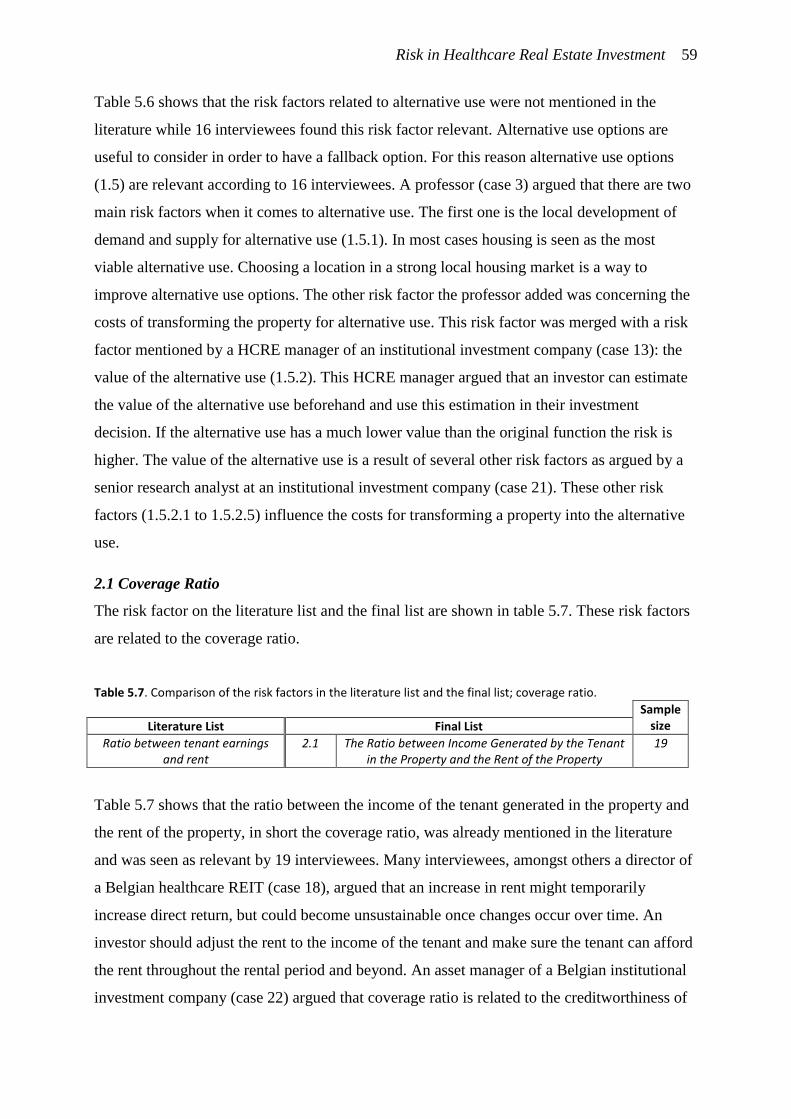
Risk in Healthcare Real Estate Investment 59
Table 5.6 shows that the risk factors related to alternative use were not mentioned in the
literature while 16 interviewees found this risk factor relevant. Alternative use options are
useful to consider in order to have a fallback option. For this reason alternative use options
(1.5) are relevant according to 16 interviewees. A professor (case 3) argued that there are two
main risk factors when it comes to alternative use. The first one is the local development of
demand and supply for alternative use (1.5.1). In most cases housing is seen as the most
viable alternative use. Choosing a location in a strong local housing market is a way to
improve alternative use options. The other risk factor the professor added was concerning the
costs of transforming the property for alternative use. This risk factor was merged with a risk
factor mentioned by a HCRE manager of an institutional investment company (case 13): the
value of the alternative use (1.5.2). This HCRE manager argued that an investor can estimate
the value of the alternative use beforehand and use this estimation in their investment
decision. If the alternative use has a much lower value than the original function the risk is
higher. The value of the alternative use is a result of several other risk factors as argued by a
senior research analyst at an institutional investment company (case 21). These other risk
factors (1.5.2.1 to 1.5.2.5) influence the costs for transforming a property into the alternative
use.
2.1 Coverage Ratio
The risk factor on the literature list and the final list are shown in table 5.7. These risk factors
are related to the coverage ratio.
Table 5.7. Comparison of the risk factors in the literature list and the final list; coverage ratio.
Sample size Literature List Final List
Ratio between tenant earnings and rent
2.1 The Ratio between Income Generated by the Tenant in the Property and the Rent of the Property
19
Table 5.7 shows that the ratio between the income of the tenant generated in the property and
the rent of the property, in short the coverage ratio, was already mentioned in the literature
and was seen as relevant by 19 interviewees. Many interviewees, amongst others a director of
a Belgian healthcare REIT (case 18), argued that an increase in rent might temporarily
increase direct return, but could become unsustainable once changes occur over time. An
investor should adjust the rent to the income of the tenant and make sure the tenant can afford
the rent throughout the rental period and beyond. An asset manager of a Belgian institutional
investment company (case 22) argued that coverage ratio is related to the creditworthiness of
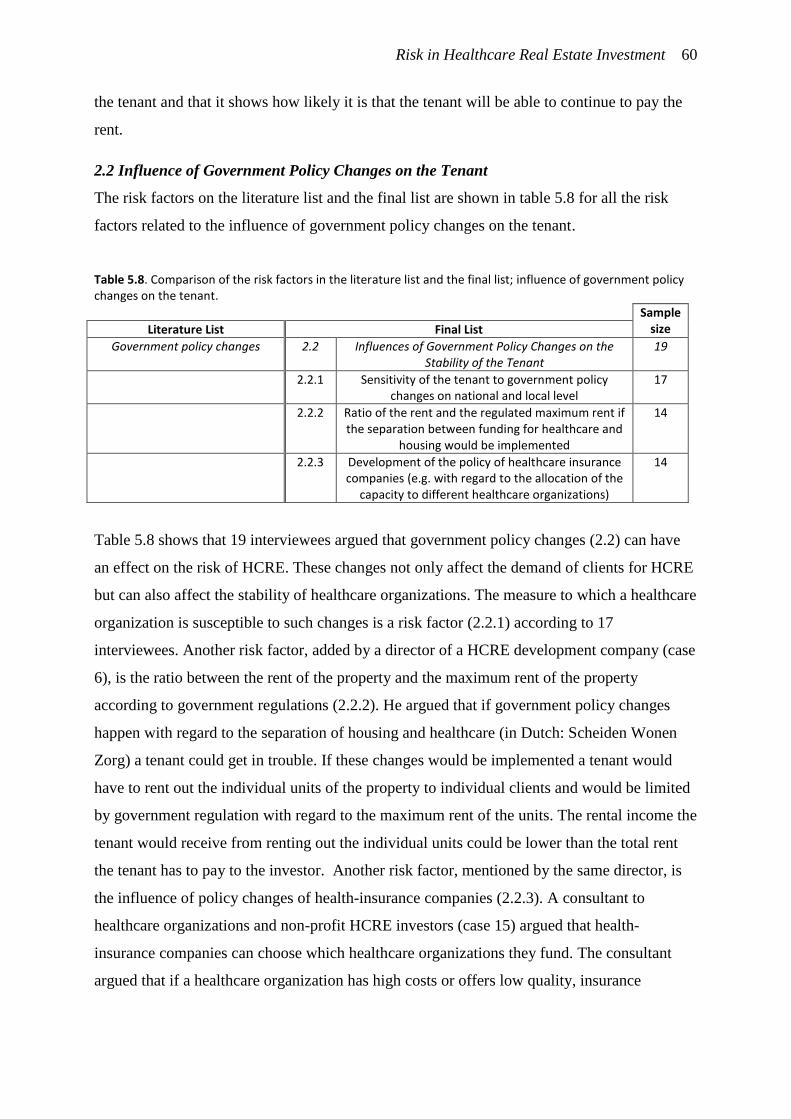
Risk in Healthcare Real Estate Investment 60
the tenant and that it shows how likely it is that the tenant will be able to continue to pay the
rent.
2.2 Influence of Government Policy Changes on the Tenant
The risk factors on the literature list and the final list are shown in table 5.8 for all the risk
factors related to the influence of government policy changes on the tenant.
Table 5.8. Comparison of the risk factors in the literature list and the final list; influence of government policy changes on the tenant.
Sample size Literature List Final List
Government policy changes 2.2 Influences of Government Policy Changes on the Stability of the Tenant
19
2.2.1 Sensitivity of the tenant to government policy changes on national and local level
17
2.2.2 Ratio of the rent and the regulated maximum rent if the separation between funding for healthcare and
housing would be implemented
14
2.2.3 Development of the policy of healthcare insurance companies (e.g. with regard to the allocation of the
capacity to different healthcare organizations)
14
Table 5.8 shows that 19 interviewees argued that government policy changes (2.2) can have
an effect on the risk of HCRE. These changes not only affect the demand of clients for HCRE
but can also affect the stability of healthcare organizations. The measure to which a healthcare
organization is susceptible to such changes is a risk factor (2.2.1) according to 17
interviewees. Another risk factor, added by a director of a HCRE development company (case
6), is the ratio between the rent of the property and the maximum rent of the property
according to government regulations (2.2.2). He argued that if government policy changes
happen with regard to the separation of housing and healthcare (in Dutch: Scheiden Wonen
Zorg) a tenant could get in trouble. If these changes would be implemented a tenant would
have to rent out the individual units of the property to individual clients and would be limited
by government regulation with regard to the maximum rent of the units. The rental income the
tenant would receive from renting out the individual units could be lower than the total rent
the tenant has to pay to the investor. Another risk factor, mentioned by the same director, is
the influence of policy changes of health-insurance companies (2.2.3). A consultant to
healthcare organizations and non-profit HCRE investors (case 15) argued that health-
insurance companies can choose which healthcare organizations they fund. The consultant
argued that if a healthcare organization has high costs or offers low quality, insurance
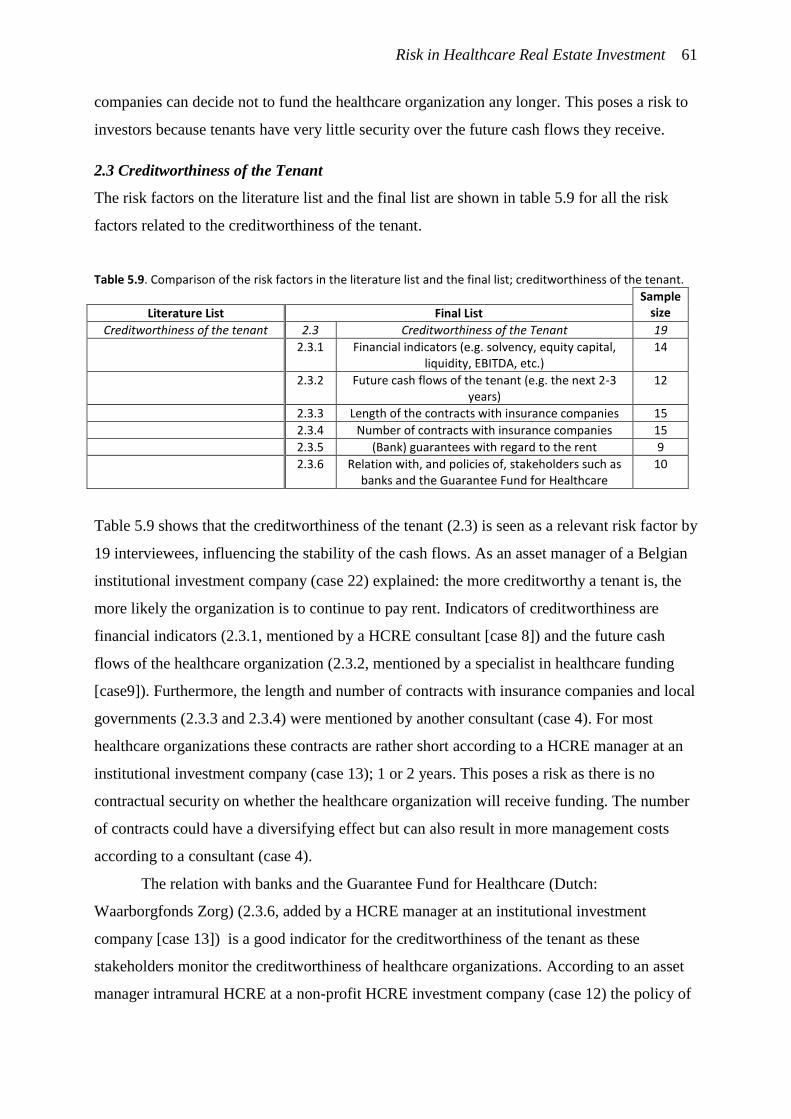
Risk in Healthcare Real Estate Investment 61
companies can decide not to fund the healthcare organization any longer. This poses a risk to
investors because tenants have very little security over the future cash flows they receive.
2.3 Creditworthiness of the Tenant
The risk factors on the literature list and the final list are shown in table 5.9 for all the risk
factors related to the creditworthiness of the tenant.
Table 5.9. Comparison of the risk factors in the literature list and the final list; creditworthiness of the tenant.
Sample size Literature List Final List
Creditworthiness of the tenant 2.3 Creditworthiness of the Tenant 19
2.3.1 Financial indicators (e.g. solvency, equity capital, liquidity, EBITDA, etc.)
14
2.3.2 Future cash flows of the tenant (e.g. the next 2-3 years)
12
2.3.3 Length of the contracts with insurance companies 15
2.3.4 Number of contracts with insurance companies 15
2.3.5 (Bank) guarantees with regard to the rent 9
2.3.6 Relation with, and policies of, stakeholders such as banks and the Guarantee Fund for Healthcare
10
Table 5.9 shows that the creditworthiness of the tenant (2.3) is seen as a relevant risk factor by
19 interviewees, influencing the stability of the cash flows. As an asset manager of a Belgian
institutional investment company (case 22) explained: the more creditworthy a tenant is, the
more likely the organization is to continue to pay rent. Indicators of creditworthiness are
financial indicators (2.3.1, mentioned by a HCRE consultant [case 8]) and the future cash
flows of the healthcare organization (2.3.2, mentioned by a specialist in healthcare funding
[case9]). Furthermore, the length and number of contracts with insurance companies and local
governments (2.3.3 and 2.3.4) were mentioned by another consultant (case 4). For most
healthcare organizations these contracts are rather short according to a HCRE manager at an
institutional investment company (case 13); 1 or 2 years. This poses a risk as there is no
contractual security on whether the healthcare organization will receive funding. The number
of contracts could have a diversifying effect but can also result in more management costs
according to a consultant (case 4).
The relation with banks and the Guarantee Fund for Healthcare (Dutch:
Waarborgfonds Zorg) (2.3.6, added by a HCRE manager at an institutional investment
company [case 13]) is a good indicator for the creditworthiness of the tenant as these
stakeholders monitor the creditworthiness of healthcare organizations. According to an asset
manager intramural HCRE at a non-profit HCRE investment company (case 12) the policy of
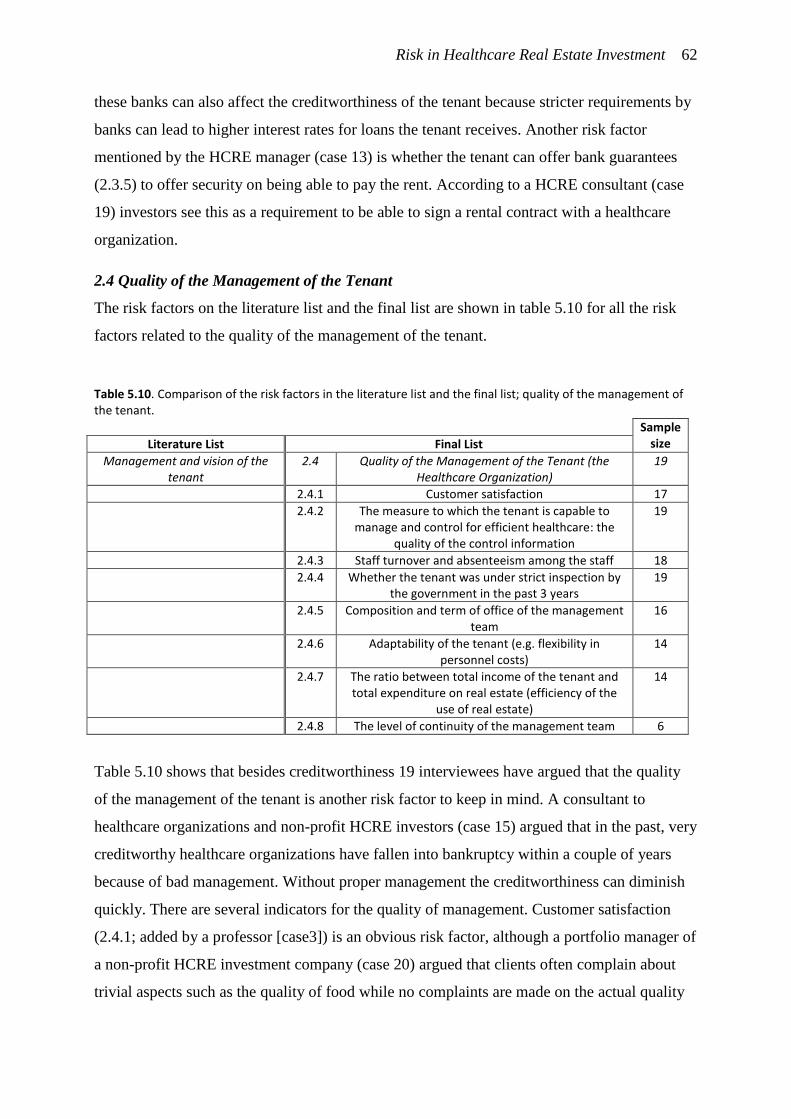
Risk in Healthcare Real Estate Investment 62
these banks can also affect the creditworthiness of the tenant because stricter requirements by
banks can lead to higher interest rates for loans the tenant receives. Another risk factor
mentioned by the HCRE manager (case 13) is whether the tenant can offer bank guarantees
(2.3.5) to offer security on being able to pay the rent. According to a HCRE consultant (case
19) investors see this as a requirement to be able to sign a rental contract with a healthcare
organization.
2.4 Quality of the Management of the Tenant
The risk factors on the literature list and the final list are shown in table 5.10 for all the risk
factors related to the quality of the management of the tenant.
Table 5.10. Comparison of the risk factors in the literature list and the final list; quality of the management of the tenant.
Sample size Literature List Final List
Management and vision of the tenant
2.4 Quality of the Management of the Tenant (the Healthcare Organization)
19
2.4.1 Customer satisfaction 17
2.4.2 The measure to which the tenant is capable to manage and control for efficient healthcare: the
quality of the control information
19
2.4.3 Staff turnover and absenteeism among the staff 18
2.4.4 Whether the tenant was under strict inspection by the government in the past 3 years
19
2.4.5 Composition and term of office of the management team
16
2.4.6 Adaptability of the tenant (e.g. flexibility in personnel costs)
14
2.4.7 The ratio between total income of the tenant and total expenditure on real estate (efficiency of the
use of real estate)
14
2.4.8 The level of continuity of the management team 6
Table 5.10 shows that besides creditworthiness 19 interviewees have argued that the quality
of the management of the tenant is another risk factor to keep in mind. A consultant to
healthcare organizations and non-profit HCRE investors (case 15) argued that in the past, very
creditworthy healthcare organizations have fallen into bankruptcy within a couple of years
because of bad management. Without proper management the creditworthiness can diminish
quickly. There are several indicators for the quality of management. Customer satisfaction
(2.4.1; added by a professor [case3]) is an obvious risk factor, although a portfolio manager of
a non-profit HCRE investment company (case 20) argued that clients often complain about
trivial aspects such as the quality of food while no complaints are made on the actual quality
Risk in Healthcare Real Estate Investment 63
of healthcare. Staff absenteeism (2.4.3; added by an asset manager of a non-profit HCRE
investment company [case 2]) is an indicator of satisfaction among staff. Because providing
healthcare services is labor intensive, staff absenteeism is seen by 18 interviewees as a
relevant risk factor. A consultant (case 1) argued that the quality of the control information
(2.4.2) is another indicator of the quality of the management. He argued that an effective
organization has information and data on the services they deliver and can monitor and steer
based on this information to make processes more effective. 18 other interviewees agreed on
the relevance of this risk factor. Furthermore, he argued that if a healthcare organization is
under strict inspection by the government (2.4.4) this would be an indication of bad
management.
Two risk factors that were mentioned interviewees are concerning the management
team itself (2.4.5; added by a consultant [case 4] and; 2.4.8; added by a HCRE manager of a
Belgian REIT [case 16]). An asset manager of a Belgian institutional investment company
(case 22) argued that a management team that changes composition continuously is
considered more risky while a management team that has not changed its members for years
is also seen as risky. The continuation of the management team is another aspect that 6
interviewees deem relevant as it provides stability into the future.
Furthermore, 14 interviewees also indicated that they see flexibility in the cost of staff
(2.4.6) an important risk factor. A HCRE manager at an investment company (case 13) argued
that if there is flexibility in the costs of staff a healthcare organization can adjust to changing
circumstances. A director of a real estate development company (case 6) argued that investors
should also look at whether a healthcare organization has relatively high or low housing costs
(2.4.7). This indicates whether the healthcare organization is able to make effective use of its
real estate.
2.5 Vision of the Tenant
The risk factors on the literature list and the final list are shown in table 5.11 for all the risk
factors related to the vision of the tenant.
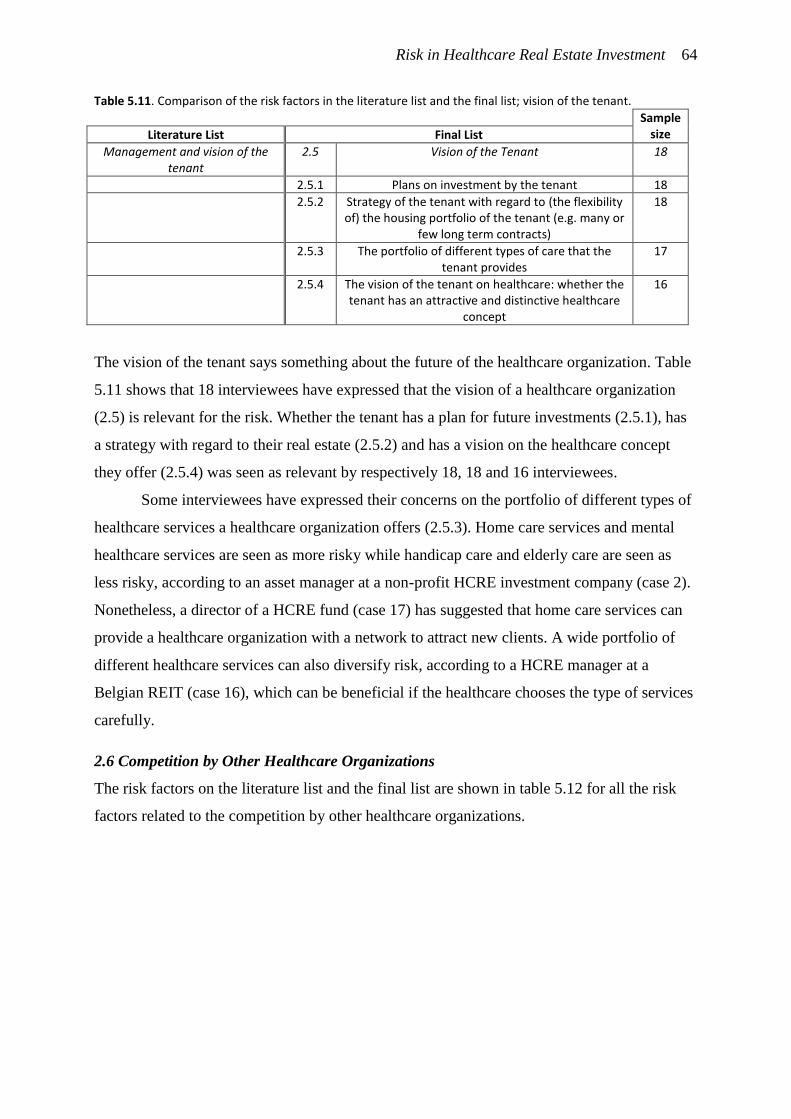
Risk in Healthcare Real Estate Investment 64
Table 5.11. Comparison of the risk factors in the literature list and the final list; vision of the tenant.
Sample size Literature List Final List
Management and vision of the tenant
2.5 Vision of the Tenant 18
2.5.1 Plans on investment by the tenant 18
2.5.2 Strategy of the tenant with regard to (the flexibility of) the housing portfolio of the tenant (e.g. many or
few long term contracts)
18
2.5.3 The portfolio of different types of care that the tenant provides
17
2.5.4 The vision of the tenant on healthcare: whether the tenant has an attractive and distinctive healthcare
concept
16
The vision of the tenant says something about the future of the healthcare organization. Table
5.11 shows that 18 interviewees have expressed that the vision of a healthcare organization
(2.5) is relevant for the risk. Whether the tenant has a plan for future investments (2.5.1), has
a strategy with regard to their real estate (2.5.2) and has a vision on the healthcare concept
they offer (2.5.4) was seen as relevant by respectively 18, 18 and 16 interviewees.
Some interviewees have expressed their concerns on the portfolio of different types of
healthcare services a healthcare organization offers (2.5.3). Home care services and mental
healthcare services are seen as more risky while handicap care and elderly care are seen as
less risky, according to an asset manager at a non-profit HCRE investment company (case 2).
Nonetheless, a director of a HCRE fund (case 17) has suggested that home care services can
provide a healthcare organization with a network to attract new clients. A wide portfolio of
different healthcare services can also diversify risk, according to a HCRE manager at a
Belgian REIT (case 16), which can be beneficial if the healthcare chooses the type of services
carefully.
2.6 Competition by Other Healthcare Organizations
The risk factors on the literature list and the final list are shown in table 5.12 for all the risk
factors related to the competition by other healthcare organizations.
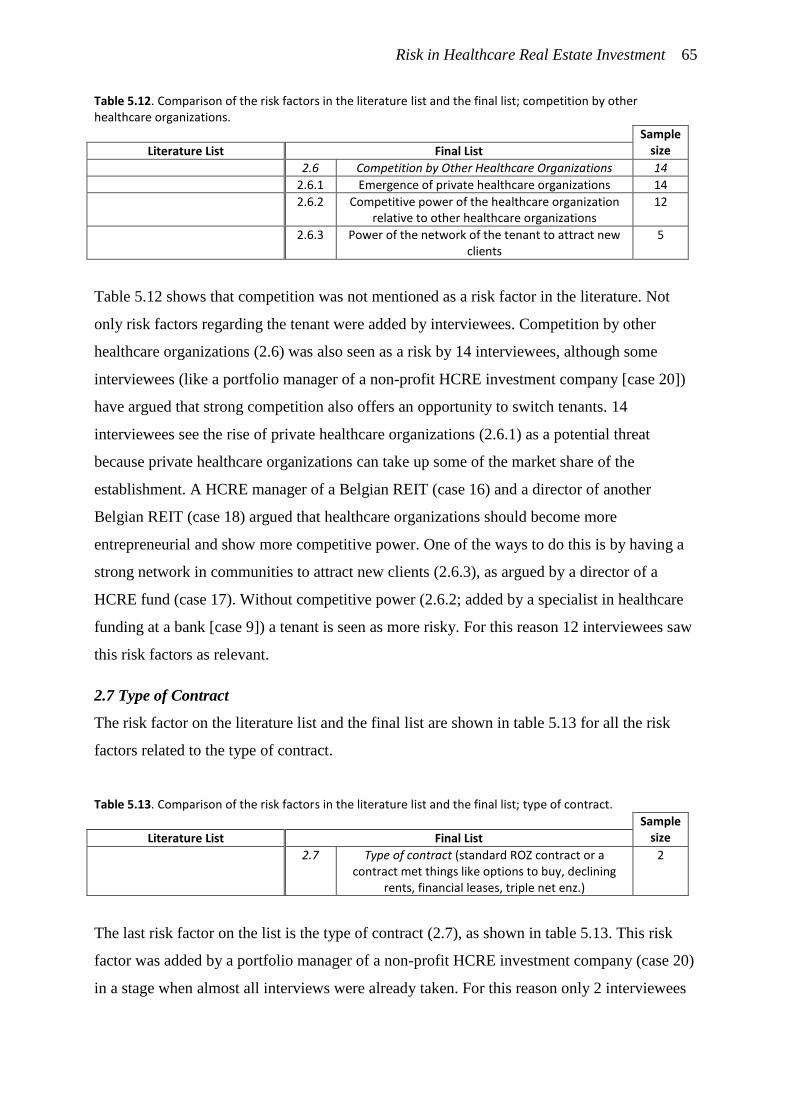
Risk in Healthcare Real Estate Investment 65
Table 5.12. Comparison of the risk factors in the literature list and the final list; competition by other healthcare organizations.
Sample size Literature List Final List
2.6 Competition by Other Healthcare Organizations 14
2.6.1 Emergence of private healthcare organizations 14
2.6.2 Competitive power of the healthcare organization relative to other healthcare organizations
12
2.6.3 Power of the network of the tenant to attract new clients
5
Table 5.12 shows that competition was not mentioned as a risk factor in the literature. Not
only risk factors regarding the tenant were added by interviewees. Competition by other
healthcare organizations (2.6) was also seen as a risk by 14 interviewees, although some
interviewees (like a portfolio manager of a non-profit HCRE investment company [case 20])
have argued that strong competition also offers an opportunity to switch tenants. 14
interviewees see the rise of private healthcare organizations (2.6.1) as a potential threat
because private healthcare organizations can take up some of the market share of the
establishment. A HCRE manager of a Belgian REIT (case 16) and a director of another
Belgian REIT (case 18) argued that healthcare organizations should become more
entrepreneurial and show more competitive power. One of the ways to do this is by having a
strong network in communities to attract new clients (2.6.3), as argued by a director of a
HCRE fund (case 17). Without competitive power (2.6.2; added by a specialist in healthcare
funding at a bank [case 9]) a tenant is seen as more risky. For this reason 12 interviewees saw
this risk factors as relevant.
2.7 Type of Contract
The risk factor on the literature list and the final list are shown in table 5.13 for all the risk
factors related to the type of contract.
Table 5.13. Comparison of the risk factors in the literature list and the final list; type of contract.
Sample size Literature List Final List
2.7 Type of contract (standard ROZ contract or a contract met things like options to buy, declining
rents, financial leases, triple net enz.)
2
The last risk factor on the list is the type of contract (2.7), as shown in table 5.13. This risk
factor was added by a portfolio manager of a non-profit HCRE investment company (case 20)
in a stage when almost all interviews were already taken. For this reason only 2 interviewees
Risk in Healthcare Real Estate Investment 66
considered this risk factor as relevant. This portfolio manager argued that standard contracts
are more easily marketable because some investors will not trade with properties with
contracts that are foreign to them. He added that these unusual contracts are most common
amongst non-profit investors.
The previous comparison shows that many risks were overlooked in the literature. No article
in scientific journals mentioned tenant risks while many interviewees argued the relevance of
tenant risks. This shows that the academic focus on macro-economic risk factors does not
entirely match the experiences of investors who examine both property risks and tenant risks
as micro-level.
5.2. Importance of Risk Factors
Besides expanding the existing knowledge in the literature on the risk factors of HCRE
investment, this study also gives insight on the importance of the individual risk factors. Data
was collected during the interviews on the importance of the risk factors. Although this is
predominantly a qualitative study the quantitative data obtained during the interviews was
analyzed using SPSS 23. The sample size of each of the 75 variables varies from 19 to 2
cases. As expected, tests showed no results with statistical significance. Although statistical
analysis is not possible with the sampled data, the descriptive statistics do give insight into the
importance of the different risk factors.
Importance of the Main Risk Factors
All of the descriptive statistics are shown in appendix 4. A selection of the descriptive
statistics of only the main risk factors is shown in Table 5.14.
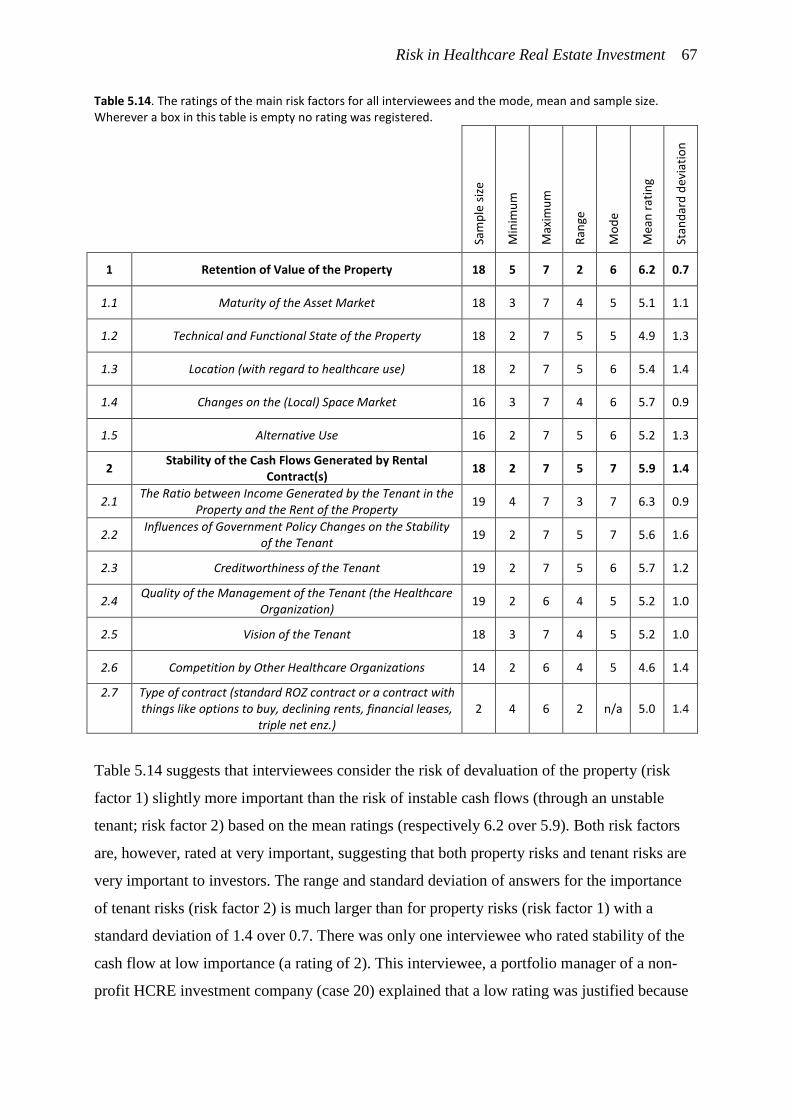
Risk in Healthcare Real Estate Investment 67
Table 5.14. The ratings of the main risk factors for all interviewees and the mode, mean and sample size. Wherever a box in this table is empty no rating was registered.
Sam
ple
siz
e
Min
imu
m
Max
imu
m
Ran
ge
Mo
de
Mea
n r
atin
g
Stan
dar
d d
evia
tio
n
1 Retention of Value of the Property 18 5 7 2 6 6.2 0.7
1.1 Maturity of the Asset Market 18 3 7 4 5 5.1 1.1
1.2 Technical and Functional State of the Property 18 2 7 5 5 4.9 1.3
1.3 Location (with regard to healthcare use) 18 2 7 5 6 5.4 1.4
1.4 Changes on the (Local) Space Market 16 3 7 4 6 5.7 0.9
1.5 Alternative Use 16 2 7 5 6 5.2 1.3
2 Stability of the Cash Flows Generated by Rental
Contract(s) 18 2 7 5 7 5.9 1.4
2.1 The Ratio between Income Generated by the Tenant in the
Property and the Rent of the Property 19 4 7 3 7 6.3 0.9
2.2 Influences of Government Policy Changes on the Stability
of the Tenant 19 2 7 5 7 5.6 1.6
2.3 Creditworthiness of the Tenant 19 2 7 5 6 5.7 1.2
2.4 Quality of the Management of the Tenant (the Healthcare
Organization) 19 2 6 4 5 5.2 1.0
2.5 Vision of the Tenant 18 3 7 4 5 5.2 1.0
2.6 Competition by Other Healthcare Organizations 14 2 6 4 5 4.6 1.4
2.7 Type of contract (standard ROZ contract or a contract with things like options to buy, declining rents, financial leases,
triple net enz.) 2 4 6 2 n/a 5.0 1.4
Table 5.14 suggests that interviewees consider the risk of devaluation of the property (risk
factor 1) slightly more important than the risk of instable cash flows (through an unstable
tenant; risk factor 2) based on the mean ratings (respectively 6.2 over 5.9). Both risk factors
are, however, rated at very important, suggesting that both property risks and tenant risks are
very important to investors. The range and standard deviation of answers for the importance
of tenant risks (risk factor 2) is much larger than for property risks (risk factor 1) with a
standard deviation of 1.4 over 0.7. There was only one interviewee who rated stability of the
cash flow at low importance (a rating of 2). This interviewee, a portfolio manager of a non-
profit HCRE investment company (case 20) explained that a low rating was justified because
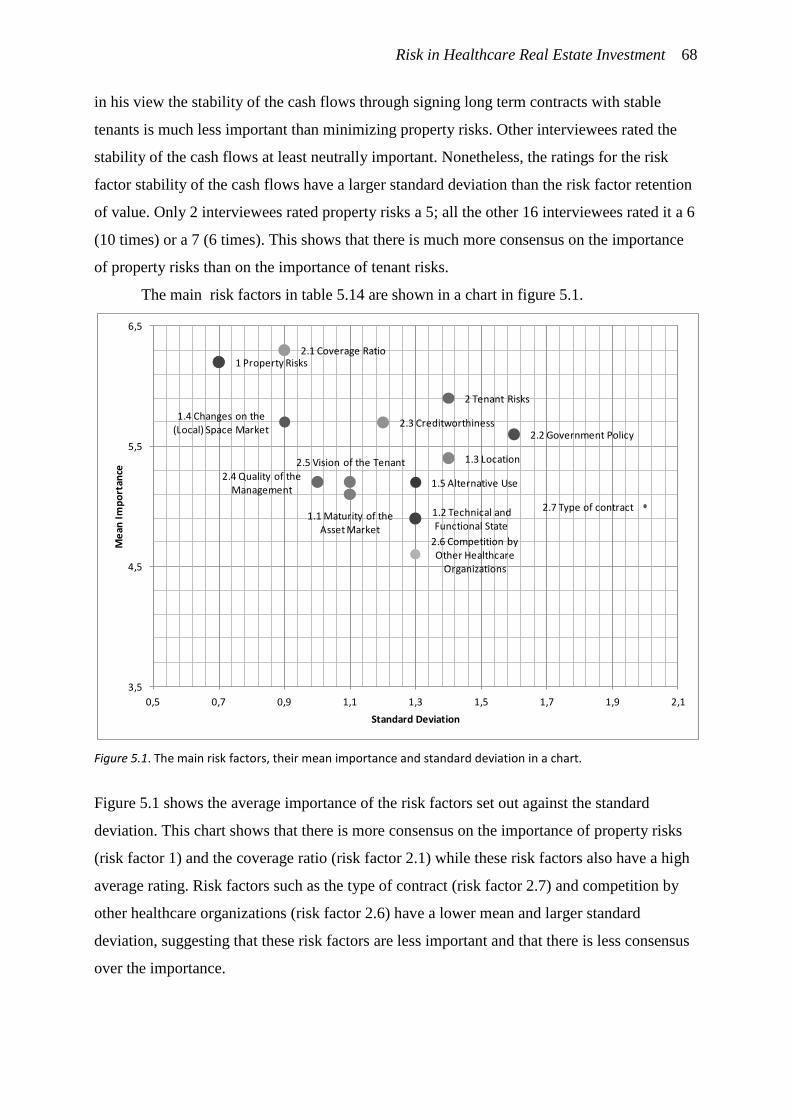
Risk in Healthcare Real Estate Investment 68
in his view the stability of the cash flows through signing long term contracts with stable
tenants is much less important than minimizing property risks. Other interviewees rated the
stability of the cash flows at least neutrally important. Nonetheless, the ratings for the risk
factor stability of the cash flows have a larger standard deviation than the risk factor retention
of value. Only 2 interviewees rated property risks a 5; all the other 16 interviewees rated it a 6
(10 times) or a 7 (6 times). This shows that there is much more consensus on the importance
of property risks than on the importance of tenant risks.
The main risk factors in table 5.14 are shown in a chart in figure 5.1.
Figure 5.1. The main risk factors, their mean importance and standard deviation in a chart.
Figure 5.1 shows the average importance of the risk factors set out against the standard
deviation. This chart shows that there is more consensus on the importance of property risks
(risk factor 1) and the coverage ratio (risk factor 2.1) while these risk factors also have a high
average rating. Risk factors such as the type of contract (risk factor 2.7) and competition by
other healthcare organizations (risk factor 2.6) have a lower mean and larger standard
deviation, suggesting that these risk factors are less important and that there is less consensus
over the importance.
1 Property Risks
1.1 Maturity of the Asset Market
1.2 Technical and Functional State
1.3 Location
1.4 Changes on the (Local) Space Market
1.5 Alternative Use
2 Tenant Risks
2.1 Coverage Ratio
2.2 Government Policy 2.3 Creditworthiness
2.4 Quality of the Management
2.5 Vision of the Tenant
2.6 Competition by Other Healthcare
Organizations
2.7 Type of contract
3,5
4,5
5,5
6,5
0,5 0,7 0,9 1,1 1,3 1,5 1,7 1,9 2,1
Me
an I
mp
ort
ance
Standard Deviation
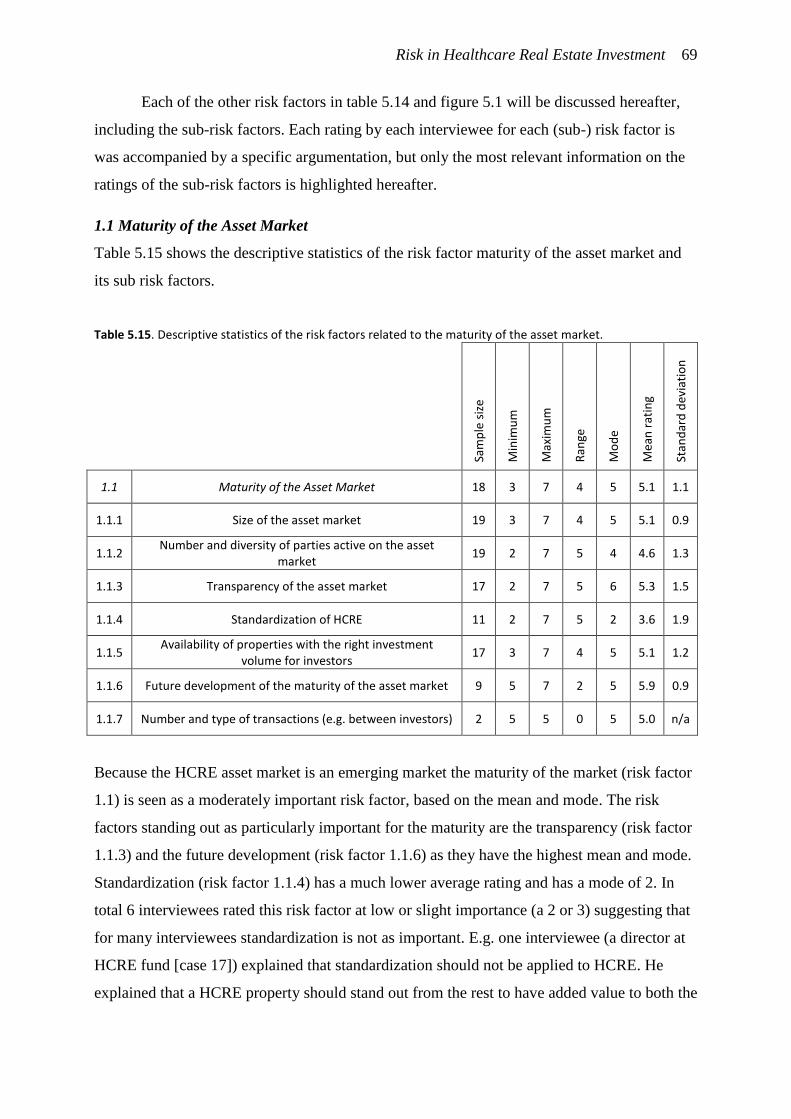
Risk in Healthcare Real Estate Investment 69
Each of the other risk factors in table 5.14 and figure 5.1 will be discussed hereafter,
including the sub-risk factors. Each rating by each interviewee for each (sub-) risk factor is
was accompanied by a specific argumentation, but only the most relevant information on the
ratings of the sub-risk factors is highlighted hereafter.
1.1 Maturity of the Asset Market
Table 5.15 shows the descriptive statistics of the risk factor maturity of the asset market and
its sub risk factors.
Table 5.15. Descriptive statistics of the risk factors related to the maturity of the asset market.
Sam
ple
siz
e
Min
imu
m
Max
imu
m
Ran
ge
Mo
de
Mea
n r
atin
g
Stan
dar
d d
evia
tio
n
1.1 Maturity of the Asset Market 18 3 7 4 5 5.1 1.1
1.1.1 Size of the asset market 19 3 7 4 5 5.1 0.9
1.1.2 Number and diversity of parties active on the asset
market 19 2 7 5 4 4.6 1.3
1.1.3 Transparency of the asset market 17 2 7 5 6 5.3 1.5
1.1.4 Standardization of HCRE 11 2 7 5 2 3.6 1.9
1.1.5 Availability of properties with the right investment
volume for investors 17 3 7 4 5 5.1 1.2
1.1.6 Future development of the maturity of the asset market 9 5 7 2 5 5.9 0.9
1.1.7 Number and type of transactions (e.g. between investors) 2 5 5 0 5 5.0 n/a
Because the HCRE asset market is an emerging market the maturity of the market (risk factor
1.1) is seen as a moderately important risk factor, based on the mean and mode. The risk
factors standing out as particularly important for the maturity are the transparency (risk factor
1.1.3) and the future development (risk factor 1.1.6) as they have the highest mean and mode.
Standardization (risk factor 1.1.4) has a much lower average rating and has a mode of 2. In
total 6 interviewees rated this risk factor at low or slight importance (a 2 or 3) suggesting that
for many interviewees standardization is not as important. E.g. one interviewee (a director at
HCRE fund [case 17]) explained that standardization should not be applied to HCRE. He
explained that a HCRE property should stand out from the rest to have added value to both the
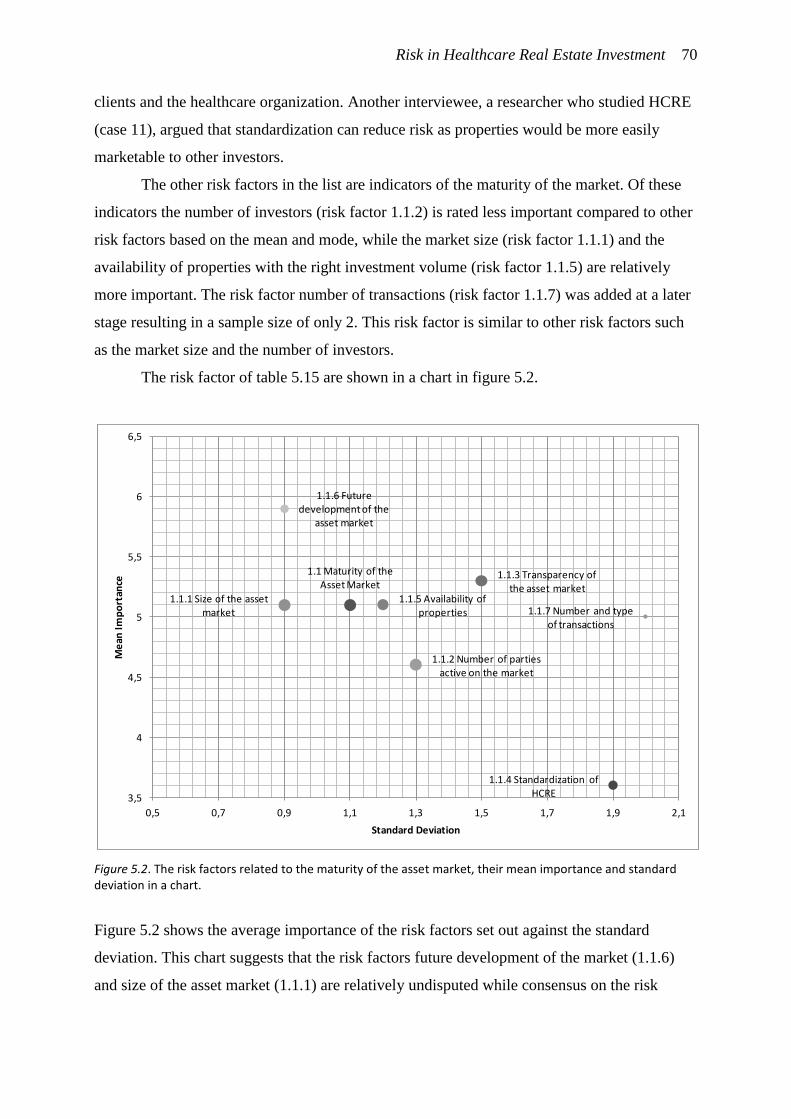
Risk in Healthcare Real Estate Investment 70
clients and the healthcare organization. Another interviewee, a researcher who studied HCRE
(case 11), argued that standardization can reduce risk as properties would be more easily
marketable to other investors.
The other risk factors in the list are indicators of the maturity of the market. Of these
indicators the number of investors (risk factor 1.1.2) is rated less important compared to other
risk factors based on the mean and mode, while the market size (risk factor 1.1.1) and the
availability of properties with the right investment volume (risk factor 1.1.5) are relatively
more important. The risk factor number of transactions (risk factor 1.1.7) was added at a later
stage resulting in a sample size of only 2. This risk factor is similar to other risk factors such
as the market size and the number of investors.
The risk factor of table 5.15 are shown in a chart in figure 5.2.
Figure 5.2. The risk factors related to the maturity of the asset market, their mean importance and standard deviation in a chart.
Figure 5.2 shows the average importance of the risk factors set out against the standard
deviation. This chart suggests that the risk factors future development of the market (1.1.6)
and size of the asset market (1.1.1) are relatively undisputed while consensus on the risk
1.1 Maturity of the Asset Market
1.1.1 Size of the asset market
1.1.2 Number of parties active on the market
1.1.3 Transparency of the asset market
1.1.4 Standardization of HCRE
1.1.5 Availability of properties
1.1.6 Future development of the
asset market
1.1.7 Number and type of transactions
3,5
4
4,5
5
5,5
6
6,5
0,5 0,7 0,9 1,1 1,3 1,5 1,7 1,9 2,1
Me
an I
mp
ort
ance
Standard Deviation
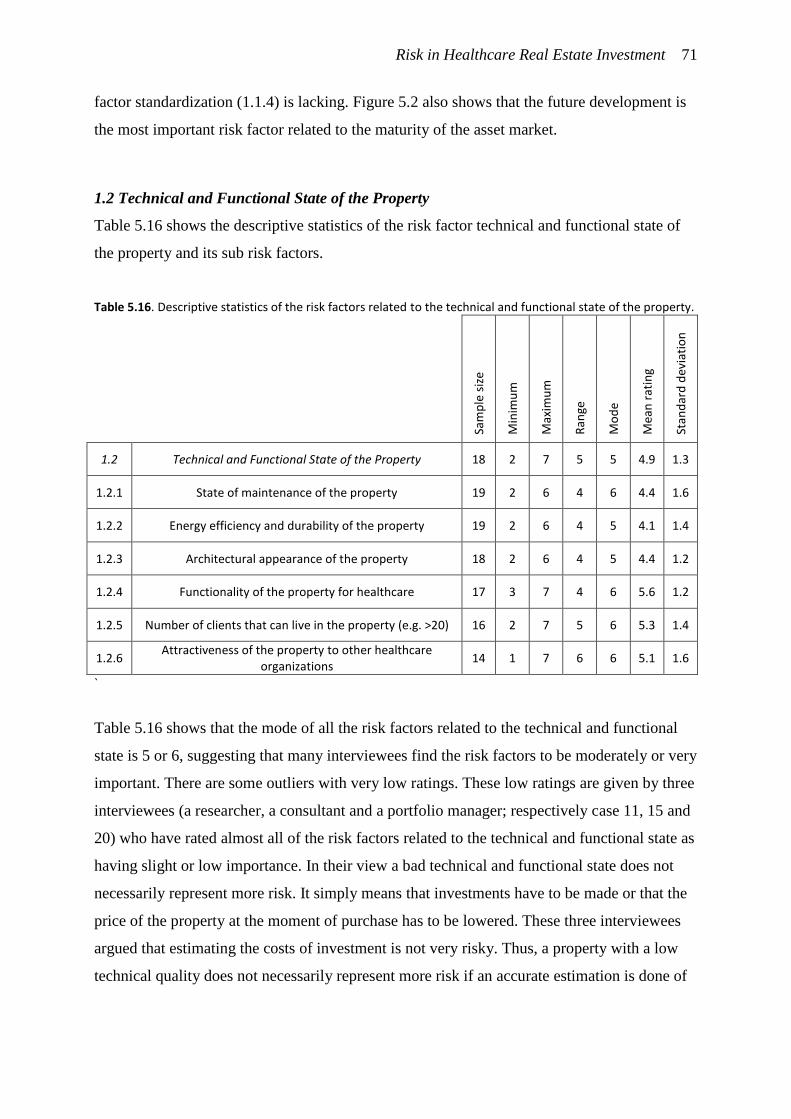
Risk in Healthcare Real Estate Investment 71
factor standardization (1.1.4) is lacking. Figure 5.2 also shows that the future development is
the most important risk factor related to the maturity of the asset market.
1.2 Technical and Functional State of the Property
Table 5.16 shows the descriptive statistics of the risk factor technical and functional state of
the property and its sub risk factors.
Table 5.16. Descriptive statistics of the risk factors related to the technical and functional state of the property.
Sam
ple
siz
e
Min
imu
m
Max
imu
m
Ran
ge
Mo
de
Mea
n r
atin
g
Stan
dar
d d
evia
tio
n
1.2 Technical and Functional State of the Property 18 2 7 5 5 4.9 1.3
1.2.1 State of maintenance of the property 19 2 6 4 6 4.4 1.6
1.2.2 Energy efficiency and durability of the property 19 2 6 4 5 4.1 1.4
1.2.3 Architectural appearance of the property 18 2 6 4 5 4.4 1.2
1.2.4 Functionality of the property for healthcare 17 3 7 4 6 5.6 1.2
1.2.5 Number of clients that can live in the property (e.g. >20) 16 2 7 5 6 5.3 1.4
1.2.6 Attractiveness of the property to other healthcare
organizations 14 1 7 6 6 5.1 1.6
`
Table 5.16 shows that the mode of all the risk factors related to the technical and functional
state is 5 or 6, suggesting that many interviewees find the risk factors to be moderately or very
important. There are some outliers with very low ratings. These low ratings are given by three
interviewees (a researcher, a consultant and a portfolio manager; respectively case 11, 15 and
20) who have rated almost all of the risk factors related to the technical and functional state as
having slight or low importance. In their view a bad technical and functional state does not
necessarily represent more risk. It simply means that investments have to be made or that the
price of the property at the moment of purchase has to be lowered. These three interviewees
argued that estimating the costs of investment is not very risky. Thus, a property with a low
technical quality does not necessarily represent more risk if an accurate estimation is done of

Risk in Healthcare Real Estate Investment 72
the additional investments. Because of these three interviewees the risk factors rate lower on
average than other risk factors on the list.
The risk factor regarding the attractiveness of the property to other healthcare
organizations (1.2.6) is considered very or extremely important by eight interviewees. As an
asset manager of intramural HCRE at a non-profit HCRE investment company (case 12)
explained: some properties are made suitable for only one healthcare organization, causing it
to become less attractive to other healthcare organizations. This phenomenon presents a risk
because it increases dependence on one healthcare organization. One interviewee (a director
at a HCRE fund [case 17]) has rated this risk factor a 1, meaning it is not at all important to
him. This interviewee has argued that in his opinion adjusting the property to the needs of a
healthcare organization makes it much more valuable to that healthcare organization. The
interviewee argued that by making sure the property performs optimally for the healthcare
organization, the healthcare organization also becomes dependent on the investor. In that way
a partnership can form with mutual dependence.
Based on the mean ratings and modes the most important risk factors with regard to
the technical and functional state are: the functionality of the property to healthcare
organizations (1.2.4); the number of clients that can live in the property (1.2.5) and; the
attractiveness of the property to other healthcare organizations (1.2.6). The least important
risk factor, based on the mean and mode, is the durability of the property (1.2.2).
The risk factor of table 5.16 are shown in a chart in figure 5.3.
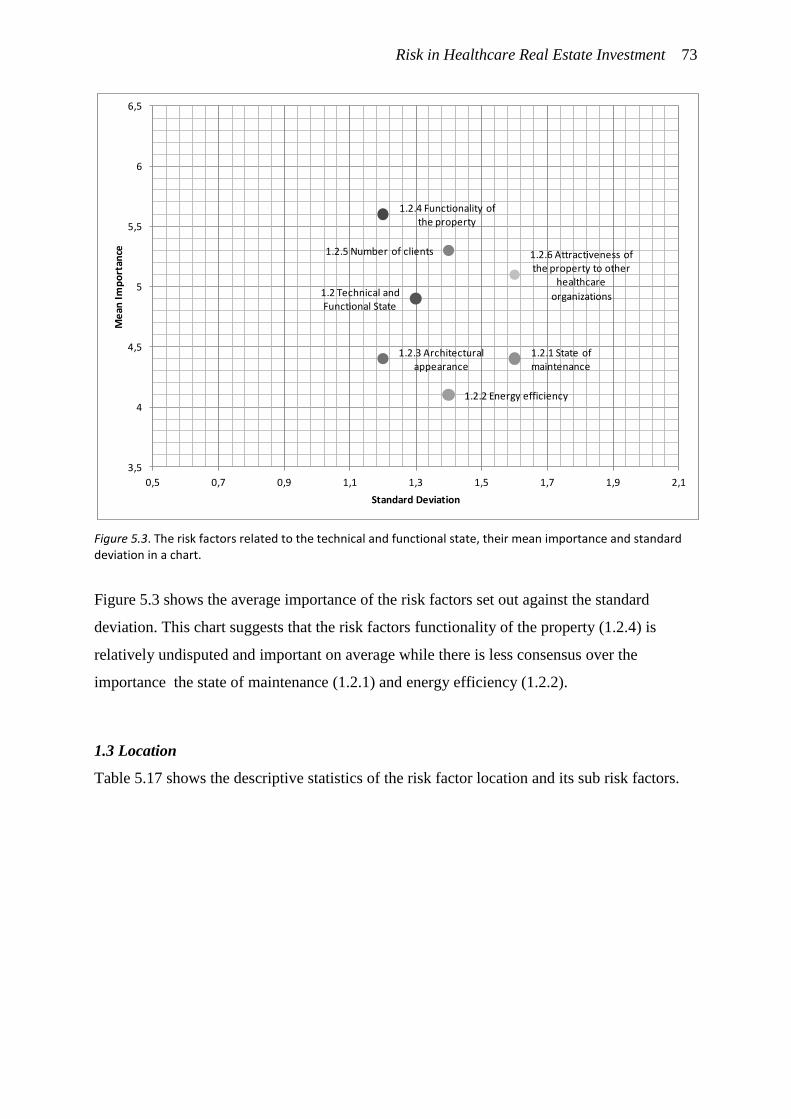
Risk in Healthcare Real Estate Investment 73
Figure 5.3. The risk factors related to the technical and functional state, their mean importance and standard deviation in a chart.
Figure 5.3 shows the average importance of the risk factors set out against the standard
deviation. This chart suggests that the risk factors functionality of the property (1.2.4) is
relatively undisputed and important on average while there is less consensus over the
importance the state of maintenance (1.2.1) and energy efficiency (1.2.2).
1.3 Location
Table 5.17 shows the descriptive statistics of the risk factor location and its sub risk factors.
1.2 Technical and Functional State
1.2.1 State of maintenance
1.2.2 Energy efficiency
1.2.3 Architectural appearance
1.2.4 Functionality of the property
1.2.5 Number of clients 1.2.6 Attractiveness of the property to other
healthcare
organizations
3,5
4
4,5
5
5,5
6
6,5
0,5 0,7 0,9 1,1 1,3 1,5 1,7 1,9 2,1
Me
an I
mp
ort
ance
Standard Deviation
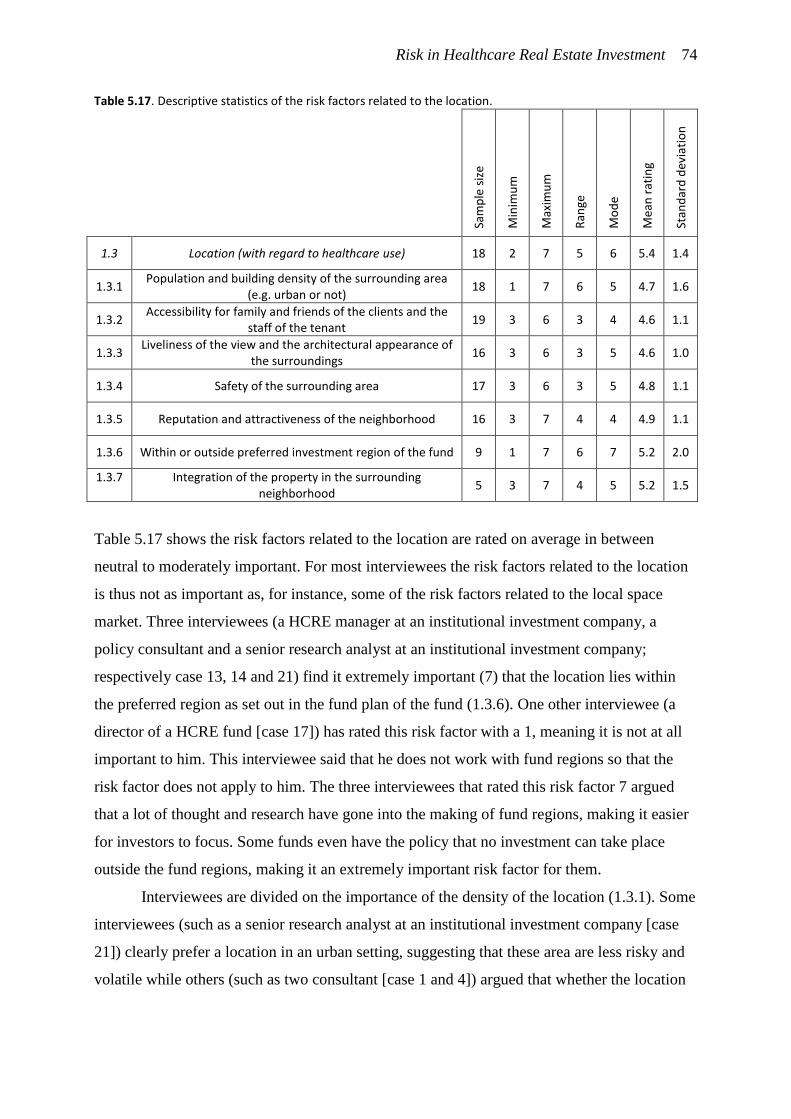
Risk in Healthcare Real Estate Investment 74
Table 5.17. Descriptive statistics of the risk factors related to the location.
Sam
ple
siz
e
Min
imu
m
Max
imu
m
Ran
ge
Mo
de
Mea
n r
atin
g
Stan
dar
d d
evia
tio
n
1.3 Location (with regard to healthcare use) 18 2 7 5 6 5.4 1.4
1.3.1 Population and building density of the surrounding area
(e.g. urban or not) 18 1 7 6 5 4.7 1.6
1.3.2 Accessibility for family and friends of the clients and the
staff of the tenant 19 3 6 3 4 4.6 1.1
1.3.3 Liveliness of the view and the architectural appearance of
the surroundings 16 3 6 3 5 4.6 1.0
1.3.4 Safety of the surrounding area 17 3 6 3 5 4.8 1.1
1.3.5 Reputation and attractiveness of the neighborhood 16 3 7 4 4 4.9 1.1
1.3.6 Within or outside preferred investment region of the fund 9 1 7 6 7 5.2 2.0
1.3.7 Integration of the property in the surrounding neighborhood
5 3 7 4 5 5.2 1.5
Table 5.17 shows the risk factors related to the location are rated on average in between
neutral to moderately important. For most interviewees the risk factors related to the location
is thus not as important as, for instance, some of the risk factors related to the local space
market. Three interviewees (a HCRE manager at an institutional investment company, a
policy consultant and a senior research analyst at an institutional investment company;
respectively case 13, 14 and 21) find it extremely important (7) that the location lies within
the preferred region as set out in the fund plan of the fund (1.3.6). One other interviewee (a
director of a HCRE fund [case 17]) has rated this risk factor with a 1, meaning it is not at all
important to him. This interviewee said that he does not work with fund regions so that the
risk factor does not apply to him. The three interviewees that rated this risk factor 7 argued
that a lot of thought and research have gone into the making of fund regions, making it easier
for investors to focus. Some funds even have the policy that no investment can take place
outside the fund regions, making it an extremely important risk factor for them.
Interviewees are divided on the importance of the density of the location (1.3.1). Some
interviewees (such as a senior research analyst at an institutional investment company [case
21]) clearly prefer a location in an urban setting, suggesting that these area are less risky and
volatile while others (such as two consultant [case 1 and 4]) argued that whether the location
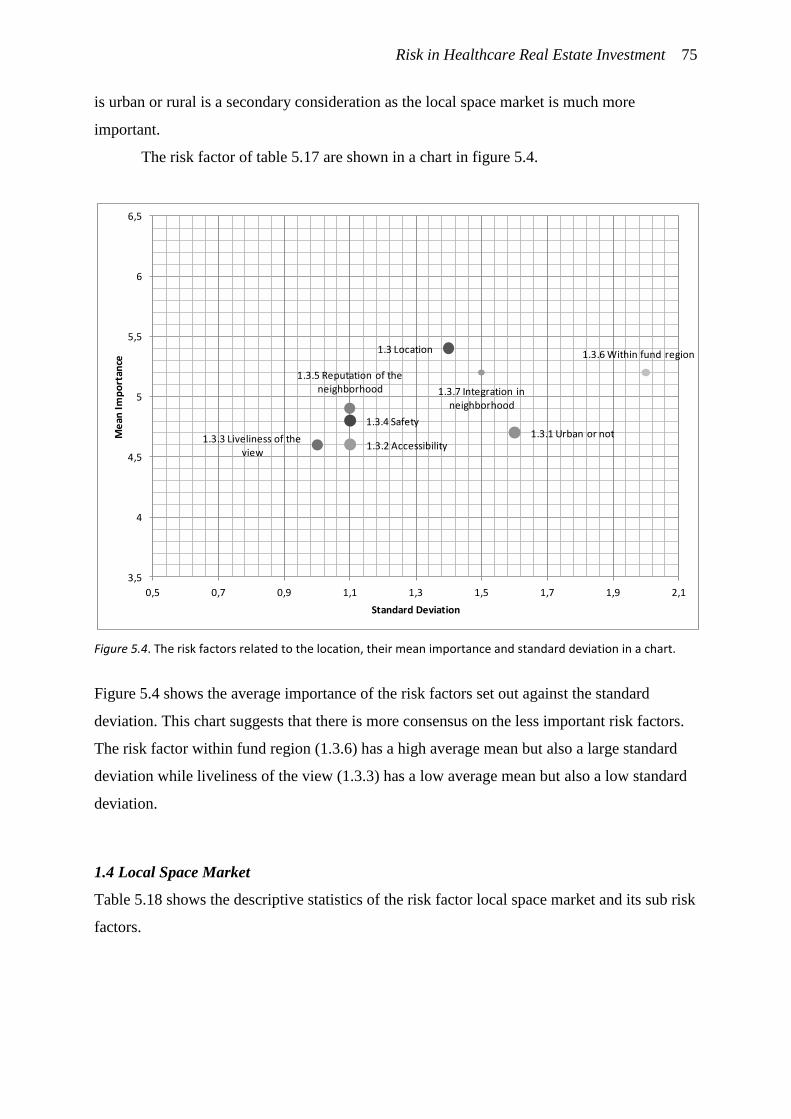
Risk in Healthcare Real Estate Investment 75
is urban or rural is a secondary consideration as the local space market is much more
important.
The risk factor of table 5.17 are shown in a chart in figure 5.4.
Figure 5.4. The risk factors related to the location, their mean importance and standard deviation in a chart.
Figure 5.4 shows the average importance of the risk factors set out against the standard
deviation. This chart suggests that there is more consensus on the less important risk factors.
The risk factor within fund region (1.3.6) has a high average mean but also a large standard
deviation while liveliness of the view (1.3.3) has a low average mean but also a low standard
deviation.
1.4 Local Space Market
Table 5.18 shows the descriptive statistics of the risk factor local space market and its sub risk
factors.
1.3 Location
1.3.1 Urban or not1.3.2 Accessibility
1.3.3 Liveliness of the view
1.3.4 Safety
1.3.5 Reputation of the neighborhood
1.3.6 Within fund region
1.3.7 Integration in neighborhood
3,5
4
4,5
5
5,5
6
6,5
0,5 0,7 0,9 1,1 1,3 1,5 1,7 1,9 2,1
Me
an I
mp
ort
ance
Standard Deviation
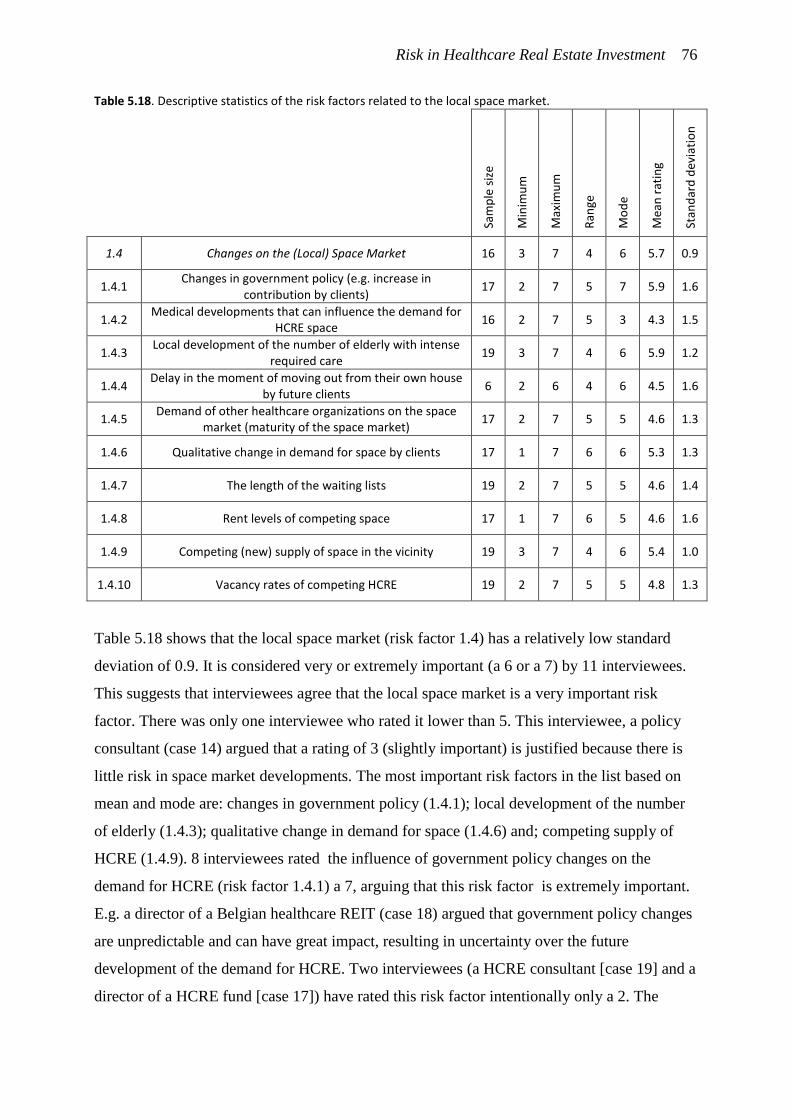
Risk in Healthcare Real Estate Investment 76
Table 5.18. Descriptive statistics of the risk factors related to the local space market.
Sam
ple
siz
e
Min
imu
m
Max
imu
m
Ran
ge
Mo
de
Mea
n r
atin
g
Stan
dar
d d
evia
tio
n
1.4 Changes on the (Local) Space Market 16 3 7 4 6 5.7 0.9
1.4.1 Changes in government policy (e.g. increase in
contribution by clients) 17 2 7 5 7 5.9 1.6
1.4.2 Medical developments that can influence the demand for
HCRE space 16 2 7 5 3 4.3 1.5
1.4.3 Local development of the number of elderly with intense
required care 19 3 7 4 6 5.9 1.2
1.4.4 Delay in the moment of moving out from their own house
by future clients 6 2 6 4 6 4.5 1.6
1.4.5 Demand of other healthcare organizations on the space
market (maturity of the space market) 17 2 7 5 5 4.6 1.3
1.4.6 Qualitative change in demand for space by clients 17 1 7 6 6 5.3 1.3
1.4.7 The length of the waiting lists 19 2 7 5 5 4.6 1.4
1.4.8 Rent levels of competing space 17 1 7 6 5 4.6 1.6
1.4.9 Competing (new) supply of space in the vicinity 19 3 7 4 6 5.4 1.0
1.4.10 Vacancy rates of competing HCRE 19 2 7 5 5 4.8 1.3
Table 5.18 shows that the local space market (risk factor 1.4) has a relatively low standard
deviation of 0.9. It is considered very or extremely important (a 6 or a 7) by 11 interviewees.
This suggests that interviewees agree that the local space market is a very important risk
factor. There was only one interviewee who rated it lower than 5. This interviewee, a policy
consultant (case 14) argued that a rating of 3 (slightly important) is justified because there is
little risk in space market developments. The most important risk factors in the list based on
mean and mode are: changes in government policy (1.4.1); local development of the number
of elderly (1.4.3); qualitative change in demand for space (1.4.6) and; competing supply of
HCRE (1.4.9). 8 interviewees rated the influence of government policy changes on the
demand for HCRE (risk factor 1.4.1) a 7, arguing that this risk factor is extremely important.
E.g. a director of a Belgian healthcare REIT (case 18) argued that government policy changes
are unpredictable and can have great impact, resulting in uncertainty over the future
development of the demand for HCRE. Two interviewees (a HCRE consultant [case 19] and a
director of a HCRE fund [case 17]) have rated this risk factor intentionally only a 2. The
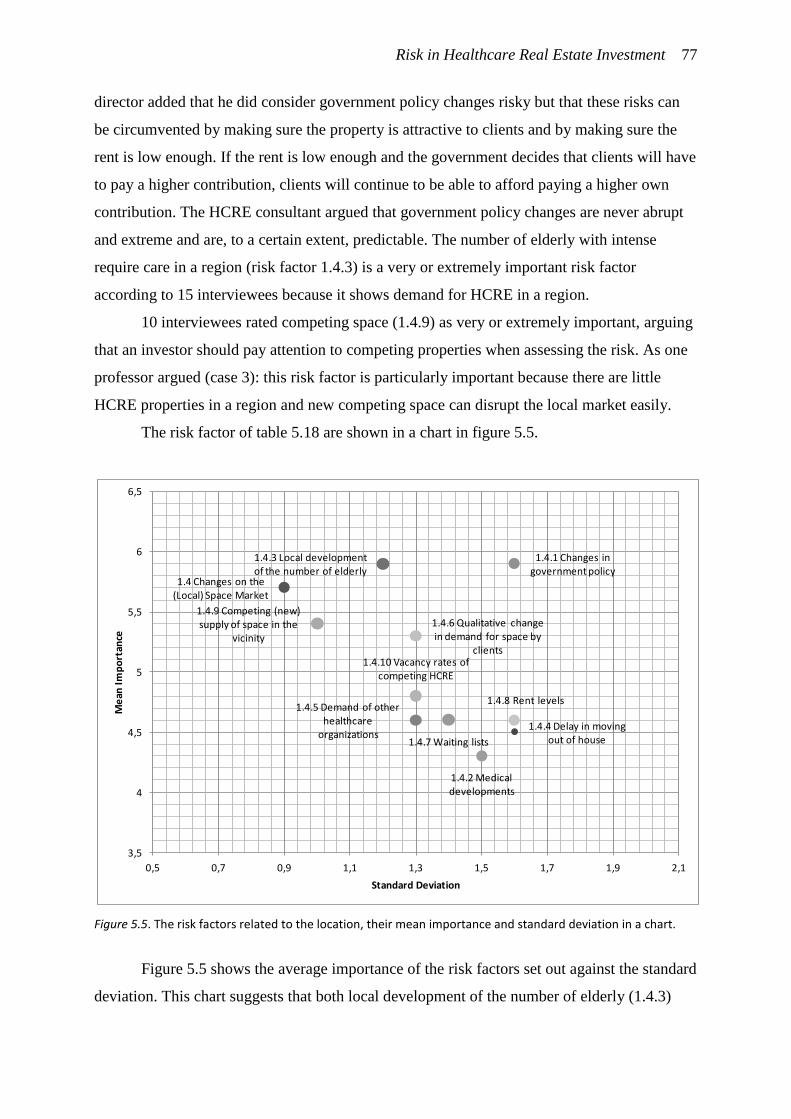
Risk in Healthcare Real Estate Investment 77
director added that he did consider government policy changes risky but that these risks can
be circumvented by making sure the property is attractive to clients and by making sure the
rent is low enough. If the rent is low enough and the government decides that clients will have
to pay a higher contribution, clients will continue to be able to afford paying a higher own
contribution. The HCRE consultant argued that government policy changes are never abrupt
and extreme and are, to a certain extent, predictable. The number of elderly with intense
require care in a region (risk factor 1.4.3) is a very or extremely important risk factor
according to 15 interviewees because it shows demand for HCRE in a region.
10 interviewees rated competing space (1.4.9) as very or extremely important, arguing
that an investor should pay attention to competing properties when assessing the risk. As one
professor argued (case 3): this risk factor is particularly important because there are little
HCRE properties in a region and new competing space can disrupt the local market easily.
The risk factor of table 5.18 are shown in a chart in figure 5.5.
Figure 5.5. The risk factors related to the location, their mean importance and standard deviation in a chart.
Figure 5.5 shows the average importance of the risk factors set out against the standard
deviation. This chart suggests that both local development of the number of elderly (1.4.3)
1.4 Changes on the (Local) Space Market
1.4.1 Changes in government policy
1.4.2 Medical developments
1.4.3 Local development of the number of elderly
1.4.4 Delay in moving out of house
1.4.5 Demand of other healthcare
organizations
1.4.6 Qualitative change in demand for space by
clients
1.4.7 Waiting lists
1.4.8 Rent levels
1.4.9 Competing (new) supply of space in the
vicinity
1.4.10 Vacancy rates of competing HCRE
3,5
4
4,5
5
5,5
6
6,5
0,5 0,7 0,9 1,1 1,3 1,5 1,7 1,9 2,1
Me
an I
mp
ort
ance
Standard Deviation
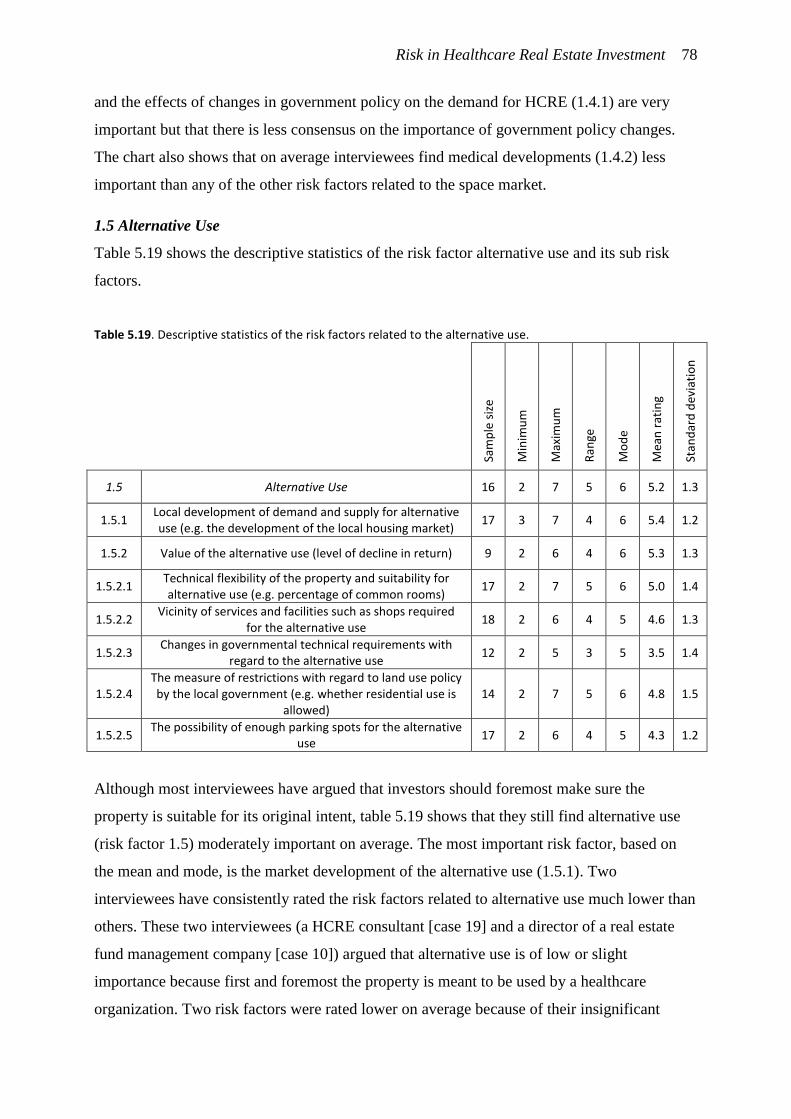
Risk in Healthcare Real Estate Investment 78
and the effects of changes in government policy on the demand for HCRE (1.4.1) are very
important but that there is less consensus on the importance of government policy changes.
The chart also shows that on average interviewees find medical developments (1.4.2) less
important than any of the other risk factors related to the space market.
1.5 Alternative Use
Table 5.19 shows the descriptive statistics of the risk factor alternative use and its sub risk
factors.
Table 5.19. Descriptive statistics of the risk factors related to the alternative use.
Sam
ple
siz
e
Min
imu
m
Max
imu
m
Ran
ge
Mo
de
Mea
n r
atin
g
Stan
dar
d d
evia
tio
n
1.5 Alternative Use 16 2 7 5 6 5.2 1.3
1.5.1 Local development of demand and supply for alternative use (e.g. the development of the local housing market)
17 3 7 4 6 5.4 1.2
1.5.2 Value of the alternative use (level of decline in return) 9 2 6 4 6 5.3 1.3
1.5.2.1 Technical flexibility of the property and suitability for alternative use (e.g. percentage of common rooms)
17 2 7 5 6 5.0 1.4
1.5.2.2 Vicinity of services and facilities such as shops required
for the alternative use 18 2 6 4 5 4.6 1.3
1.5.2.3 Changes in governmental technical requirements with
regard to the alternative use 12 2 5 3 5 3.5 1.4
1.5.2.4 The measure of restrictions with regard to land use policy by the local government (e.g. whether residential use is
allowed) 14 2 7 5 6 4.8 1.5
1.5.2.5 The possibility of enough parking spots for the alternative
use 17 2 6 4 5 4.3 1.2
Although most interviewees have argued that investors should foremost make sure the
property is suitable for its original intent, table 5.19 shows that they still find alternative use
(risk factor 1.5) moderately important on average. The most important risk factor, based on
the mean and mode, is the market development of the alternative use (1.5.1). Two
interviewees have consistently rated the risk factors related to alternative use much lower than
others. These two interviewees (a HCRE consultant [case 19] and a director of a real estate
fund management company [case 10]) argued that alternative use is of low or slight
importance because first and foremost the property is meant to be used by a healthcare
organization. Two risk factors were rated lower on average because of their insignificant
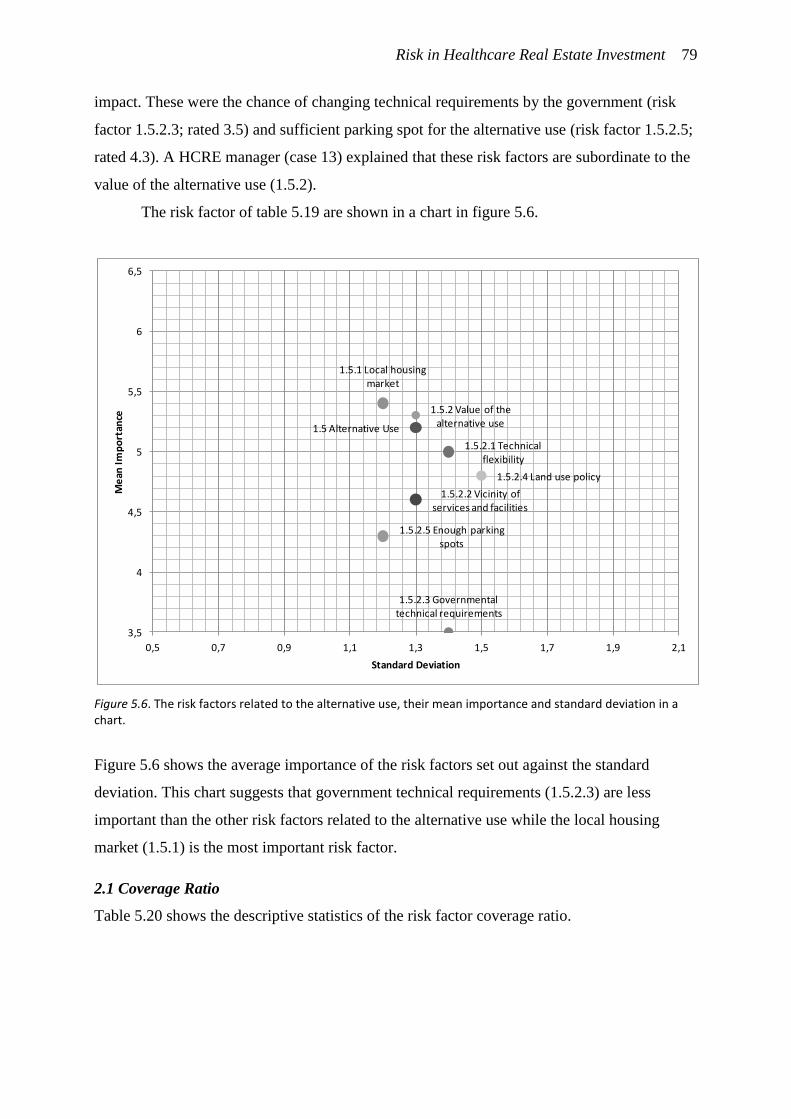
Risk in Healthcare Real Estate Investment 79
impact. These were the chance of changing technical requirements by the government (risk
factor 1.5.2.3; rated 3.5) and sufficient parking spot for the alternative use (risk factor 1.5.2.5;
rated 4.3). A HCRE manager (case 13) explained that these risk factors are subordinate to the
value of the alternative use (1.5.2).
The risk factor of table 5.19 are shown in a chart in figure 5.6.
Figure 5.6. The risk factors related to the alternative use, their mean importance and standard deviation in a chart.
Figure 5.6 shows the average importance of the risk factors set out against the standard
deviation. This chart suggests that government technical requirements (1.5.2.3) are less
important than the other risk factors related to the alternative use while the local housing
market (1.5.1) is the most important risk factor.
2.1 Coverage Ratio
Table 5.20 shows the descriptive statistics of the risk factor coverage ratio.
1.5 Alternative Use
1.5.1 Local housing market
1.5.2 Value of the alternative use
1.5.2.1 Technical flexibility
1.5.2.2 Vicinity of services and facilities
1.5.2.3 Governmental technical requirements
1.5.2.4 Land use policy
1.5.2.5 Enough parking spots
3,5
4
4,5
5
5,5
6
6,5
0,5 0,7 0,9 1,1 1,3 1,5 1,7 1,9 2,1
Me
an I
mp
ort
ance
Standard Deviation

Risk in Healthcare Real Estate Investment 80
Table 5.20. Descriptive statistics of the risk factor coverage ratio.
Sam
ple
siz
e
Min
imu
m
Max
imu
m
Ran
ge
Mo
de
Mea
n r
atin
g
Stan
dar
d d
evia
tio
n
2.1 The Ratio between Income Generated by the Tenant in the
Property and the Rent of the Property 19 4 7 3 7 6.3 0.9
Table 5.20 shows that the coverage ratio (risk factor 2.1) has an average rating of 6.3 and a
mode of 7. The mean rating of this risk factor is the highest of all risk factors, suggesting this
risk factor is the most important risk factor of all. Only 3 interviewees (an asset manager and
a portfolio manager of a non-profit HCRE investment company [case 2 and 20] and an
intramural HCRE asset manager of another non-profit HCRE investment company [case 12])
rated the coverage ratio lower than 6 (respectively 5, 4 and 5). The small range of 3 and the
standard deviation of 0.9 suggests that there is consensus on the importance of this risk factor.
A director of a Belgian healthcare REIT (case 18) argued that by adjusting the rent to the
income of the tenant the risk of the investment is largely reduced. He added that the income of
healthcare organizations is strictly dependent on government regulation so that all healthcare
organizations can generate roughly the same maximum income. On average interviewees
have rated this risk factor 6.3, suggesting that that setting the right rent level is very important.
2.2 Influence of Government Policy Changes on the Tenant
Table 5.21 shows the descriptive statistics of the risk factor influence of government policy
changes on the tenant and its sub risk factors.

Risk in Healthcare Real Estate Investment 81
Table 5.21. Descriptive statistics of the risk factors related to the influence of the government on the tenant.
Sam
ple
siz
e
Min
imu
m
Max
imu
m
Ran
ge
Mo
de
Mea
n r
atin
g
Stan
dar
d d
evia
tio
n
2.2 Influences of Government Policy Changes on the Stability
of the Tenant 19 2 7 5 7 5.6 1.6
2.2.1 Sensitivity of the tenant to government policy changes on
national and local level 17 2 7 5 6 5.6 1.5
2.2.2 Ratio of the rent and the regulated maximum rent if the separation between funding for healthcare and housing
would be implemented 14 2 6 4 5 4.9 1.2
2.2.3 Development of the policy of healthcare insurance companies (e.g. with regard to the allocation of the
capacity to different healthcare organizations) 14 2 7 5 5 4.9 1.6
Table 5.21 shows that on average the influence of government policy on a tenant (risk factor
2.2) was rated 5.6. Only 5 interviewees rated the importance of the influence of the
government on the stability of the tenant lower than very important while 14 interviewees
rated this risk factor very or extremely important. Those interviewees who rated this risk
factor as extremely important expressed their fear that government policy changes can lead to
bankruptcy of the tenant. E.g. an asset manager of a non-profit HCRE investment company
(case 7) argued that government policy changes have caused large vacancy in the past. Three
interviewees (a consultant [case 1], a researcher [case 11], a policy consultant [case 14] and a
portfolio manager of a non-profit HCRE investment company [case 20]) considered the
influence of the government on the tenant of low to neutral importance. The portfolio
manager argued that the individual tenant is less important because a tenant is replaceable. He
placed more importance on a strong space market, arguing that sufficient demand for a
property is more important than the individual tenant.
The risk factor of table 5.21 are shown in a chart in figure 5.7.
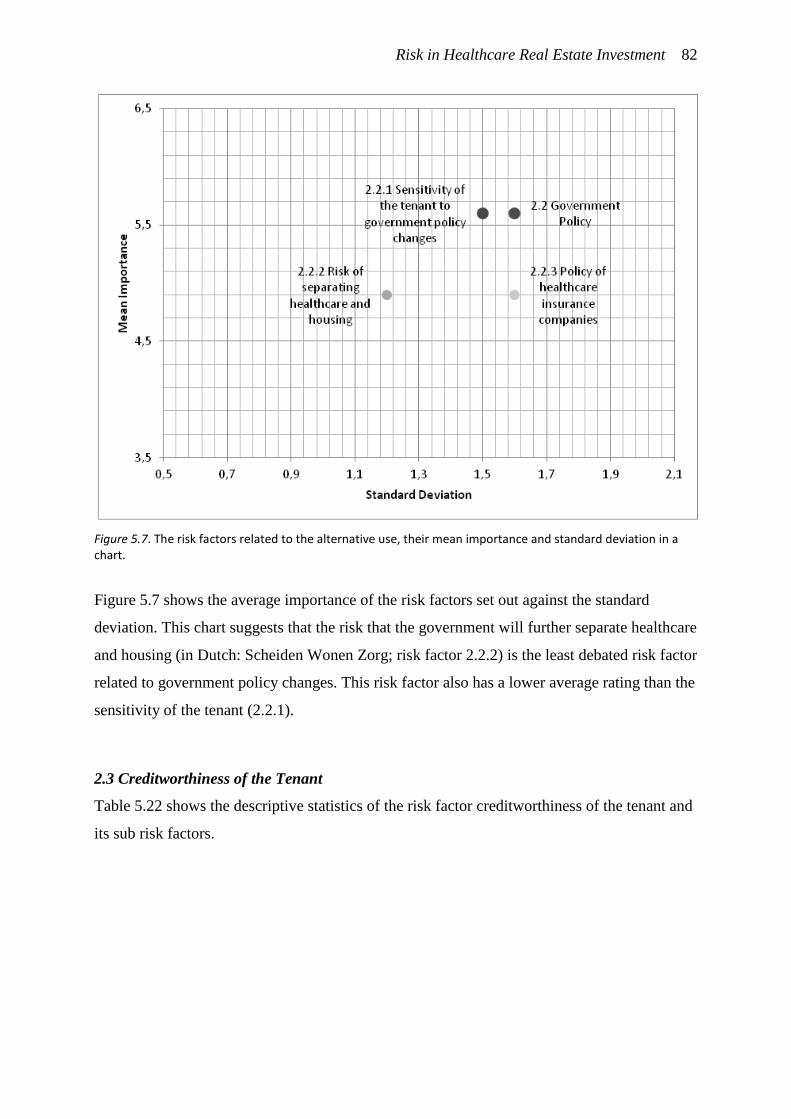
Risk in Healthcare Real Estate Investment 82
Figure 5.7. The risk factors related to the alternative use, their mean importance and standard deviation in a chart.
Figure 5.7 shows the average importance of the risk factors set out against the standard
deviation. This chart suggests that the risk that the government will further separate healthcare
and housing (in Dutch: Scheiden Wonen Zorg; risk factor 2.2.2) is the least debated risk factor
related to government policy changes. This risk factor also has a lower average rating than the
sensitivity of the tenant (2.2.1).
2.3 Creditworthiness of the Tenant
Table 5.22 shows the descriptive statistics of the risk factor creditworthiness of the tenant and
its sub risk factors.
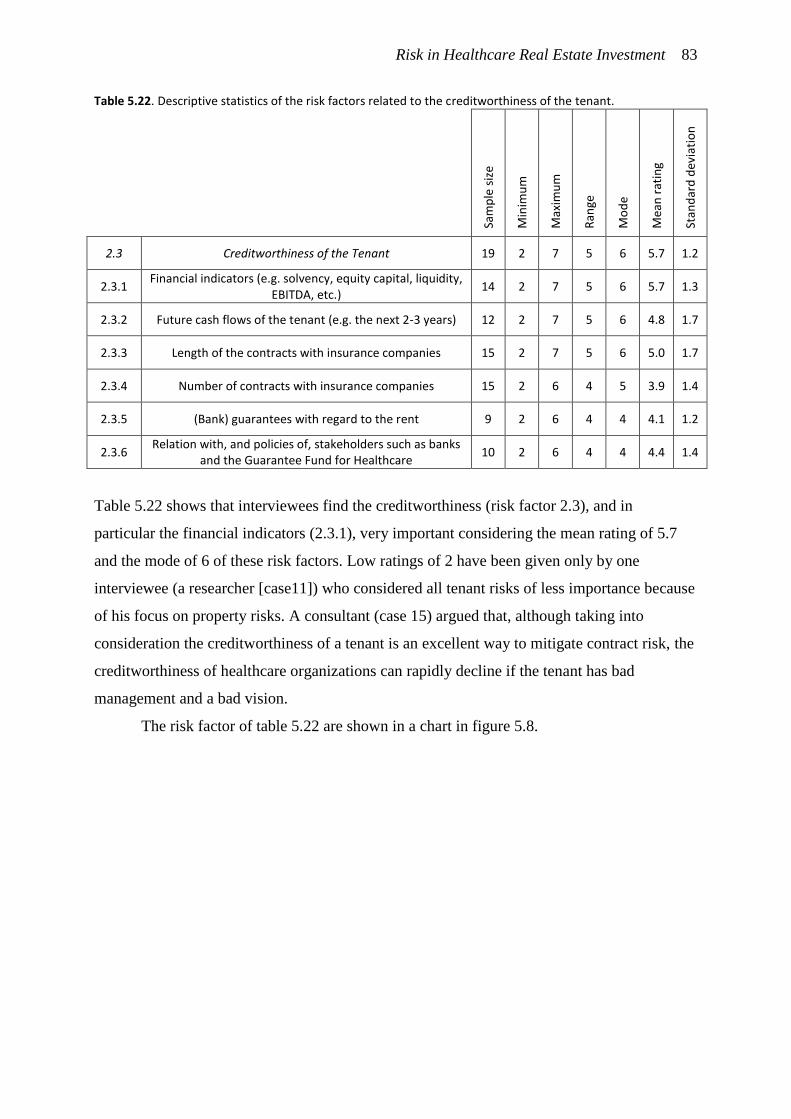
Risk in Healthcare Real Estate Investment 83
Table 5.22. Descriptive statistics of the risk factors related to the creditworthiness of the tenant.
Sam
ple
siz
e
Min
imu
m
Max
imu
m
Ran
ge
Mo
de
Mea
n r
atin
g
Stan
dar
d d
evia
tio
n
2.3 Creditworthiness of the Tenant 19 2 7 5 6 5.7 1.2
2.3.1 Financial indicators (e.g. solvency, equity capital, liquidity,
EBITDA, etc.) 14 2 7 5 6 5.7 1.3
2.3.2 Future cash flows of the tenant (e.g. the next 2-3 years) 12 2 7 5 6 4.8 1.7
2.3.3 Length of the contracts with insurance companies 15 2 7 5 6 5.0 1.7
2.3.4 Number of contracts with insurance companies 15 2 6 4 5 3.9 1.4
2.3.5 (Bank) guarantees with regard to the rent 9 2 6 4 4 4.1 1.2
2.3.6 Relation with, and policies of, stakeholders such as banks
and the Guarantee Fund for Healthcare 10 2 6 4 4 4.4 1.4
Table 5.22 shows that interviewees find the creditworthiness (risk factor 2.3), and in
particular the financial indicators (2.3.1), very important considering the mean rating of 5.7
and the mode of 6 of these risk factors. Low ratings of 2 have been given only by one
interviewee (a researcher [case11]) who considered all tenant risks of less importance because
of his focus on property risks. A consultant (case 15) argued that, although taking into
consideration the creditworthiness of a tenant is an excellent way to mitigate contract risk, the
creditworthiness of healthcare organizations can rapidly decline if the tenant has bad
management and a bad vision.
The risk factor of table 5.22 are shown in a chart in figure 5.8.
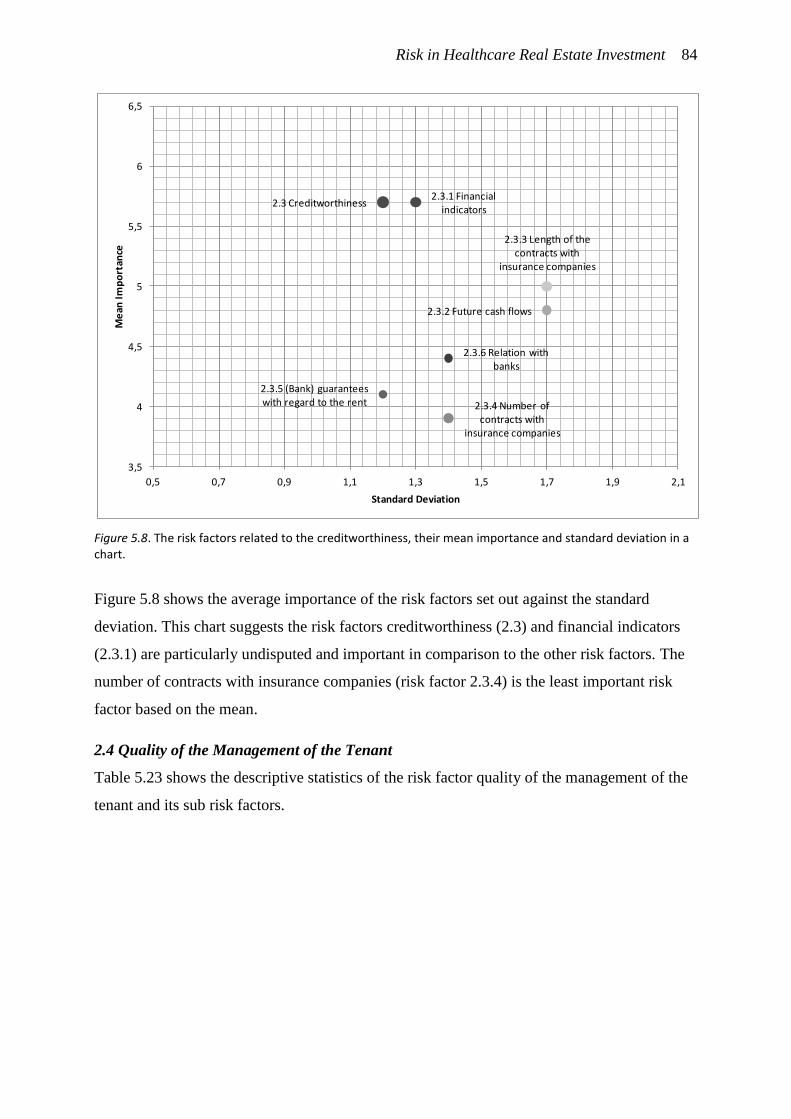
Risk in Healthcare Real Estate Investment 84
Figure 5.8. The risk factors related to the creditworthiness, their mean importance and standard deviation in a chart.
Figure 5.8 shows the average importance of the risk factors set out against the standard
deviation. This chart suggests the risk factors creditworthiness (2.3) and financial indicators
(2.3.1) are particularly undisputed and important in comparison to the other risk factors. The
number of contracts with insurance companies (risk factor 2.3.4) is the least important risk
factor based on the mean.
2.4 Quality of the Management of the Tenant
Table 5.23 shows the descriptive statistics of the risk factor quality of the management of the
tenant and its sub risk factors.
2.3.3 Length of the contracts with
insurance companies
2.3 Creditworthiness2.3.1 Financial
indicators
2.3.2 Future cash flows
2.3.4 Number of contracts with
insurance companies
2.3.5 (Bank) guarantees with regard to the rent
2.3.6 Relation with banks
3,5
4
4,5
5
5,5
6
6,5
0,5 0,7 0,9 1,1 1,3 1,5 1,7 1,9 2,1
Me
an I
mp
ort
ance
Standard Deviation
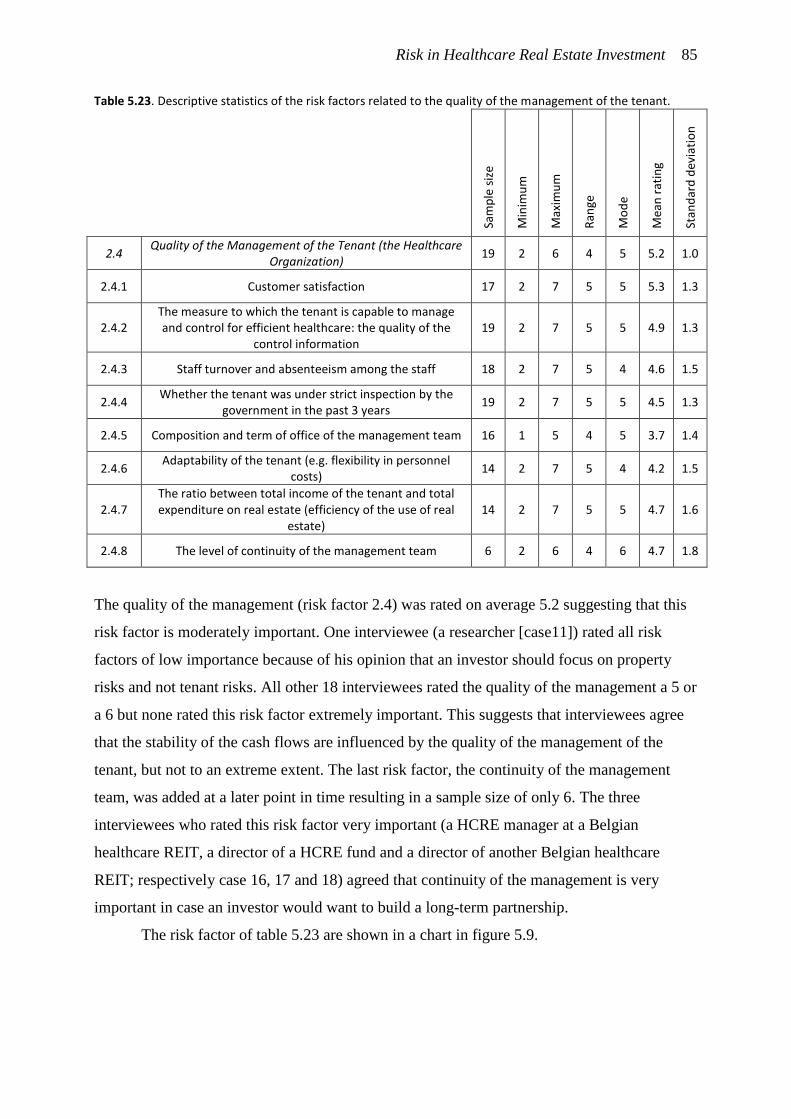
Risk in Healthcare Real Estate Investment 85
Table 5.23. Descriptive statistics of the risk factors related to the quality of the management of the tenant.
Sam
ple
siz
e
Min
imu
m
Max
imu
m
Ran
ge
Mo
de
Mea
n r
atin
g
Stan
dar
d d
evia
tio
n
2.4 Quality of the Management of the Tenant (the Healthcare
Organization) 19 2 6 4 5 5.2 1.0
2.4.1 Customer satisfaction 17 2 7 5 5 5.3 1.3
2.4.2 The measure to which the tenant is capable to manage and control for efficient healthcare: the quality of the
control information 19 2 7 5 5 4.9 1.3
2.4.3 Staff turnover and absenteeism among the staff 18 2 7 5 4 4.6 1.5
2.4.4 Whether the tenant was under strict inspection by the
government in the past 3 years 19 2 7 5 5 4.5 1.3
2.4.5 Composition and term of office of the management team 16 1 5 4 5 3.7 1.4
2.4.6 Adaptability of the tenant (e.g. flexibility in personnel
costs) 14 2 7 5 4 4.2 1.5
2.4.7 The ratio between total income of the tenant and total expenditure on real estate (efficiency of the use of real
estate) 14 2 7 5 5 4.7 1.6
2.4.8 The level of continuity of the management team 6 2 6 4 6 4.7 1.8
The quality of the management (risk factor 2.4) was rated on average 5.2 suggesting that this
risk factor is moderately important. One interviewee (a researcher [case11]) rated all risk
factors of low importance because of his opinion that an investor should focus on property
risks and not tenant risks. All other 18 interviewees rated the quality of the management a 5 or
a 6 but none rated this risk factor extremely important. This suggests that interviewees agree
that the stability of the cash flows are influenced by the quality of the management of the
tenant, but not to an extreme extent. The last risk factor, the continuity of the management
team, was added at a later point in time resulting in a sample size of only 6. The three
interviewees who rated this risk factor very important (a HCRE manager at a Belgian
healthcare REIT, a director of a HCRE fund and a director of another Belgian healthcare
REIT; respectively case 16, 17 and 18) agreed that continuity of the management is very
important in case an investor would want to build a long-term partnership.
The risk factor of table 5.23 are shown in a chart in figure 5.9.
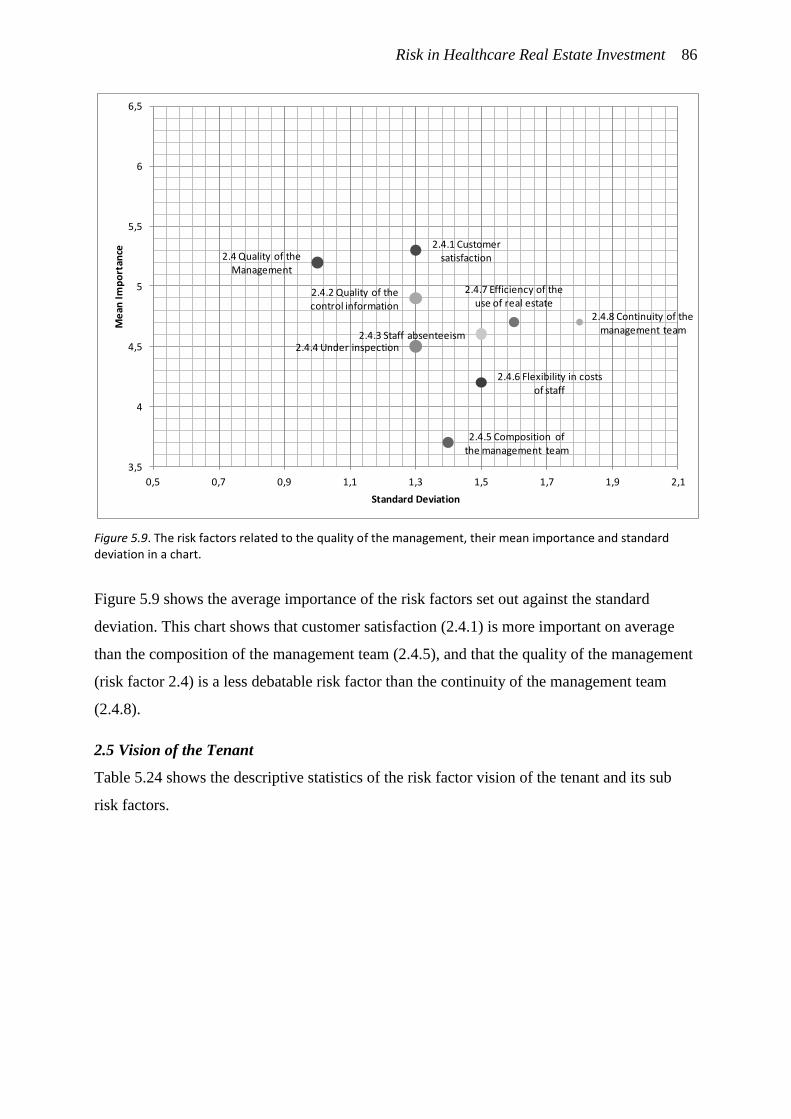
Risk in Healthcare Real Estate Investment 86
Figure 5.9. The risk factors related to the quality of the management, their mean importance and standard deviation in a chart.
Figure 5.9 shows the average importance of the risk factors set out against the standard
deviation. This chart shows that customer satisfaction (2.4.1) is more important on average
than the composition of the management team (2.4.5), and that the quality of the management
(risk factor 2.4) is a less debatable risk factor than the continuity of the management team
(2.4.8).
2.5 Vision of the Tenant
Table 5.24 shows the descriptive statistics of the risk factor vision of the tenant and its sub
risk factors.
2.4.3 Staff absenteeism
2.4 Quality of the Management
2.4.1 Customer satisfaction
2.4.2 Quality of the control information
2.4.4 Under inspection
2.4.5 Composition of the management team
2.4.6 Flexibility in costs of staff
2.4.7 Efficiency of the use of real estate
2.4.8 Continuity of the management team
3,5
4
4,5
5
5,5
6
6,5
0,5 0,7 0,9 1,1 1,3 1,5 1,7 1,9 2,1
Me
an I
mp
ort
ance
Standard Deviation
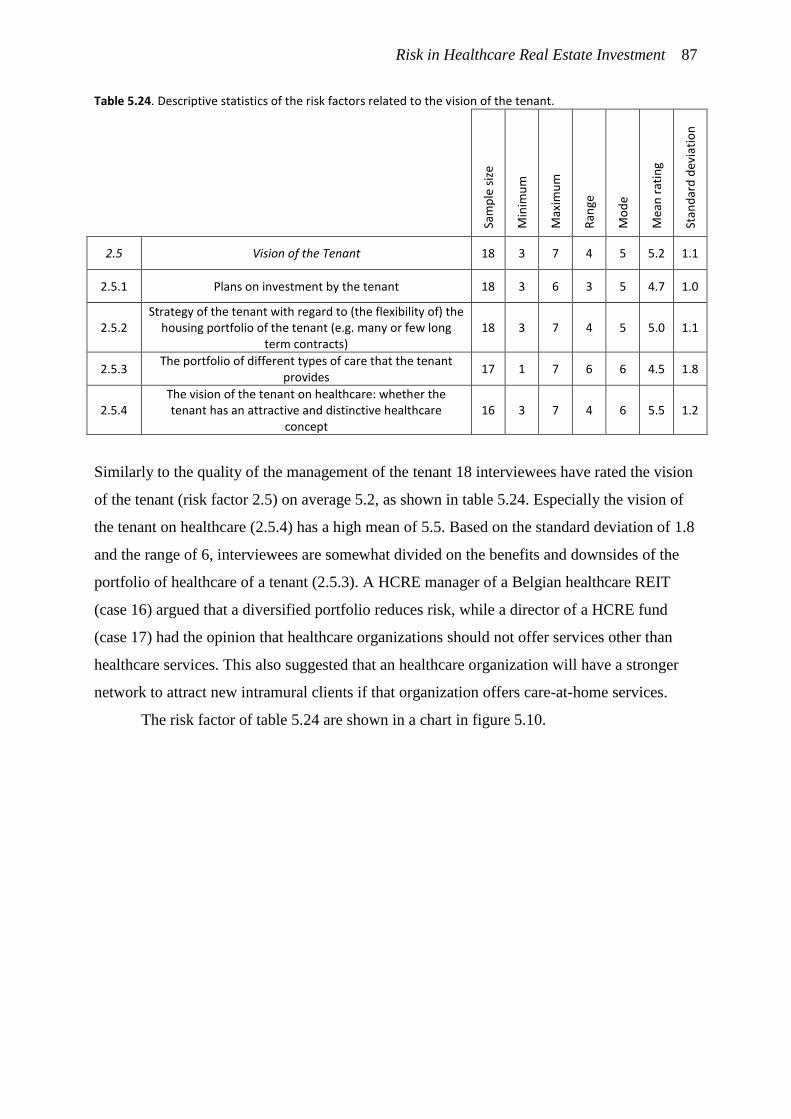
Risk in Healthcare Real Estate Investment 87
Table 5.24. Descriptive statistics of the risk factors related to the vision of the tenant.
Sam
ple
siz
e
Min
imu
m
Max
imu
m
Ran
ge
Mo
de
Mea
n r
atin
g
Stan
dar
d d
evia
tio
n
2.5 Vision of the Tenant 18 3 7 4 5 5.2 1.1
2.5.1 Plans on investment by the tenant 18 3 6 3 5 4.7 1.0
2.5.2 Strategy of the tenant with regard to (the flexibility of) the
housing portfolio of the tenant (e.g. many or few long term contracts)
18 3 7 4 5 5.0 1.1
2.5.3 The portfolio of different types of care that the tenant
provides 17 1 7 6 6 4.5 1.8
2.5.4 The vision of the tenant on healthcare: whether the tenant has an attractive and distinctive healthcare
concept 16 3 7 4 6 5.5 1.2
Similarly to the quality of the management of the tenant 18 interviewees have rated the vision
of the tenant (risk factor 2.5) on average 5.2, as shown in table 5.24. Especially the vision of
the tenant on healthcare (2.5.4) has a high mean of 5.5. Based on the standard deviation of 1.8
and the range of 6, interviewees are somewhat divided on the benefits and downsides of the
portfolio of healthcare of a tenant (2.5.3). A HCRE manager of a Belgian healthcare REIT
(case 16) argued that a diversified portfolio reduces risk, while a director of a HCRE fund
(case 17) had the opinion that healthcare organizations should not offer services other than
healthcare services. This also suggested that an healthcare organization will have a stronger
network to attract new intramural clients if that organization offers care-at-home services.
The risk factor of table 5.24 are shown in a chart in figure 5.10.
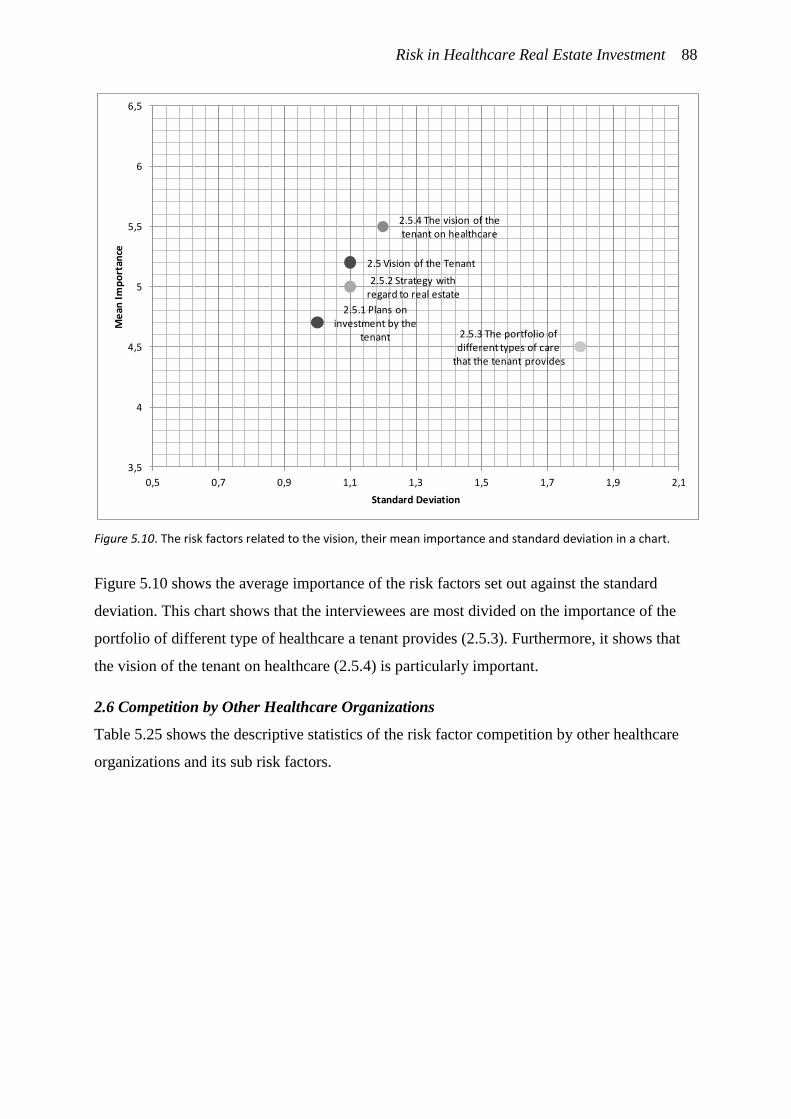
Risk in Healthcare Real Estate Investment 88
Figure 5.10. The risk factors related to the vision, their mean importance and standard deviation in a chart.
Figure 5.10 shows the average importance of the risk factors set out against the standard
deviation. This chart shows that the interviewees are most divided on the importance of the
portfolio of different type of healthcare a tenant provides (2.5.3). Furthermore, it shows that
the vision of the tenant on healthcare (2.5.4) is particularly important.
2.6 Competition by Other Healthcare Organizations
Table 5.25 shows the descriptive statistics of the risk factor competition by other healthcare
organizations and its sub risk factors.
2.5.3 The portfolio of different types of care
that the tenant provides
2.5 Vision of the Tenant
2.5.1 Plans on investment by the
tenant
2.5.2 Strategy with regard to real estate
2.5.4 The vision of the tenant on healthcare
3,5
4
4,5
5
5,5
6
6,5
0,5 0,7 0,9 1,1 1,3 1,5 1,7 1,9 2,1
Me
an I
mp
ort
ance
Standard Deviation
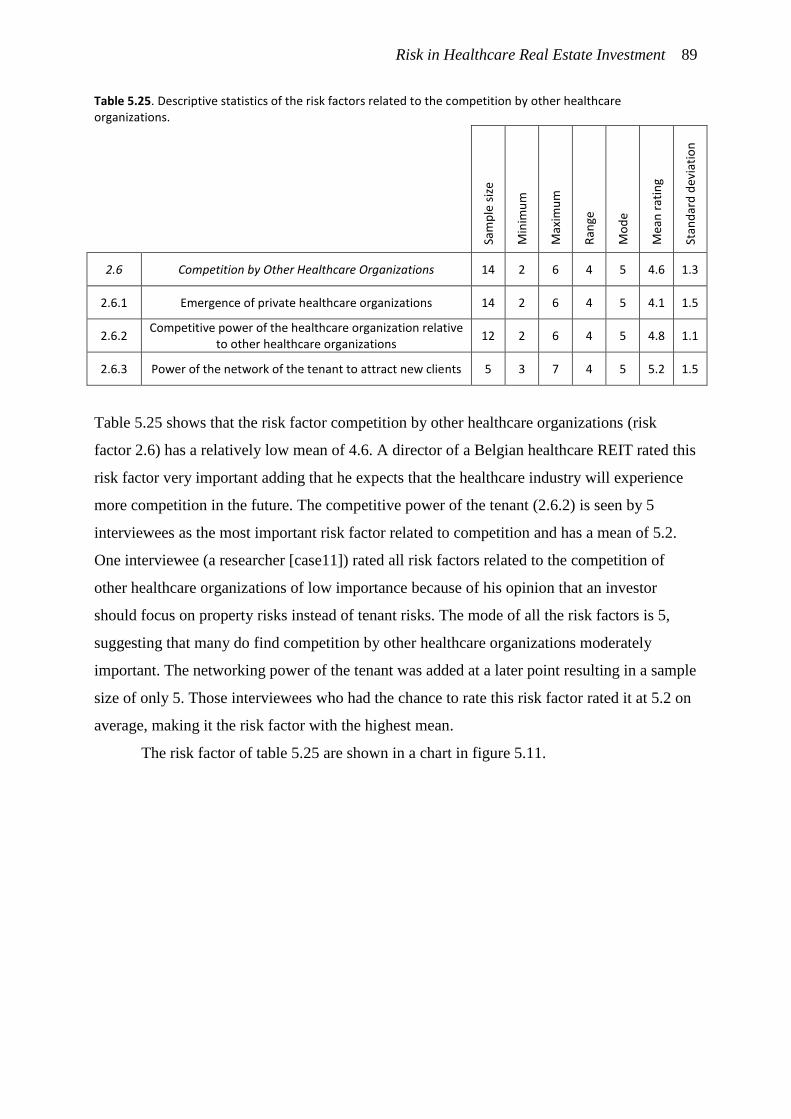
Risk in Healthcare Real Estate Investment 89
Table 5.25. Descriptive statistics of the risk factors related to the competition by other healthcare organizations.
Sam
ple
siz
e
Min
imu
m
Max
imu
m
Ran
ge
Mo
de
Mea
n r
atin
g
Stan
dar
d d
evia
tio
n
2.6 Competition by Other Healthcare Organizations 14 2 6 4 5 4.6 1.3
2.6.1 Emergence of private healthcare organizations 14 2 6 4 5 4.1 1.5
2.6.2 Competitive power of the healthcare organization relative
to other healthcare organizations 12 2 6 4 5 4.8 1.1
2.6.3 Power of the network of the tenant to attract new clients 5 3 7 4 5 5.2 1.5
Table 5.25 shows that the risk factor competition by other healthcare organizations (risk
factor 2.6) has a relatively low mean of 4.6. A director of a Belgian healthcare REIT rated this
risk factor very important adding that he expects that the healthcare industry will experience
more competition in the future. The competitive power of the tenant (2.6.2) is seen by 5
interviewees as the most important risk factor related to competition and has a mean of 5.2.
One interviewee (a researcher [case11]) rated all risk factors related to the competition of
other healthcare organizations of low importance because of his opinion that an investor
should focus on property risks instead of tenant risks. The mode of all the risk factors is 5,
suggesting that many do find competition by other healthcare organizations moderately
important. The networking power of the tenant was added at a later point resulting in a sample
size of only 5. Those interviewees who had the chance to rate this risk factor rated it at 5.2 on
average, making it the risk factor with the highest mean.
The risk factor of table 5.25 are shown in a chart in figure 5.11.
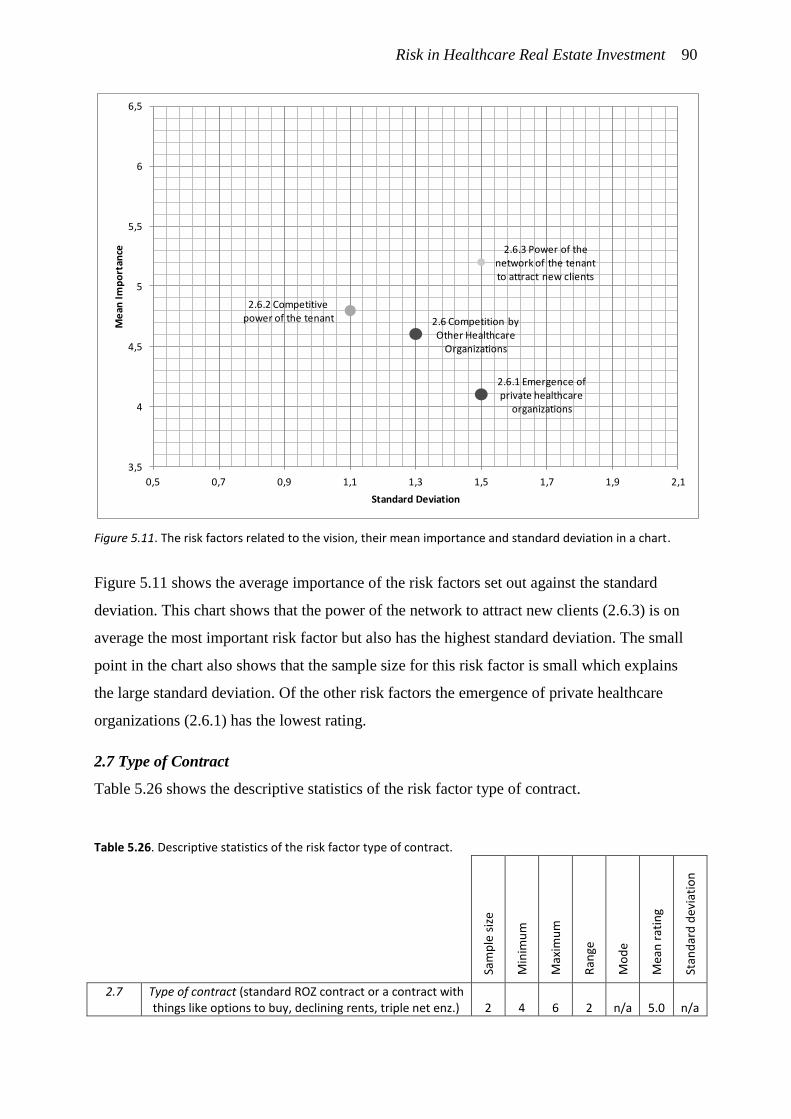
Risk in Healthcare Real Estate Investment 90
Figure 5.11. The risk factors related to the vision, their mean importance and standard deviation in a chart.
Figure 5.11 shows the average importance of the risk factors set out against the standard
deviation. This chart shows that the power of the network to attract new clients (2.6.3) is on
average the most important risk factor but also has the highest standard deviation. The small
point in the chart also shows that the sample size for this risk factor is small which explains
the large standard deviation. Of the other risk factors the emergence of private healthcare
organizations (2.6.1) has the lowest rating.
2.7 Type of Contract
Table 5.26 shows the descriptive statistics of the risk factor type of contract.
Table 5.26. Descriptive statistics of the risk factor type of contract.
Sam
ple
siz
e
Min
imu
m
Max
imu
m
Ran
ge
Mo
de
Mea
n r
atin
g
Stan
dar
d d
evia
tio
n
2.7 Type of contract (standard ROZ contract or a contract with things like options to buy, declining rents, triple net enz.) 2 4 6 2 n/a 5.0 n/a
2.6.3 Power of the network of the tenant to attract new clients
2.6 Competition by Other Healthcare
Organizations
2.6.1 Emergence of private healthcare
organizations
2.6.2 Competitive power of the tenant
3,5
4
4,5
5
5,5
6
6,5
0,5 0,7 0,9 1,1 1,3 1,5 1,7 1,9 2,1
Me
an I
mp
ort
ance
Standard Deviation
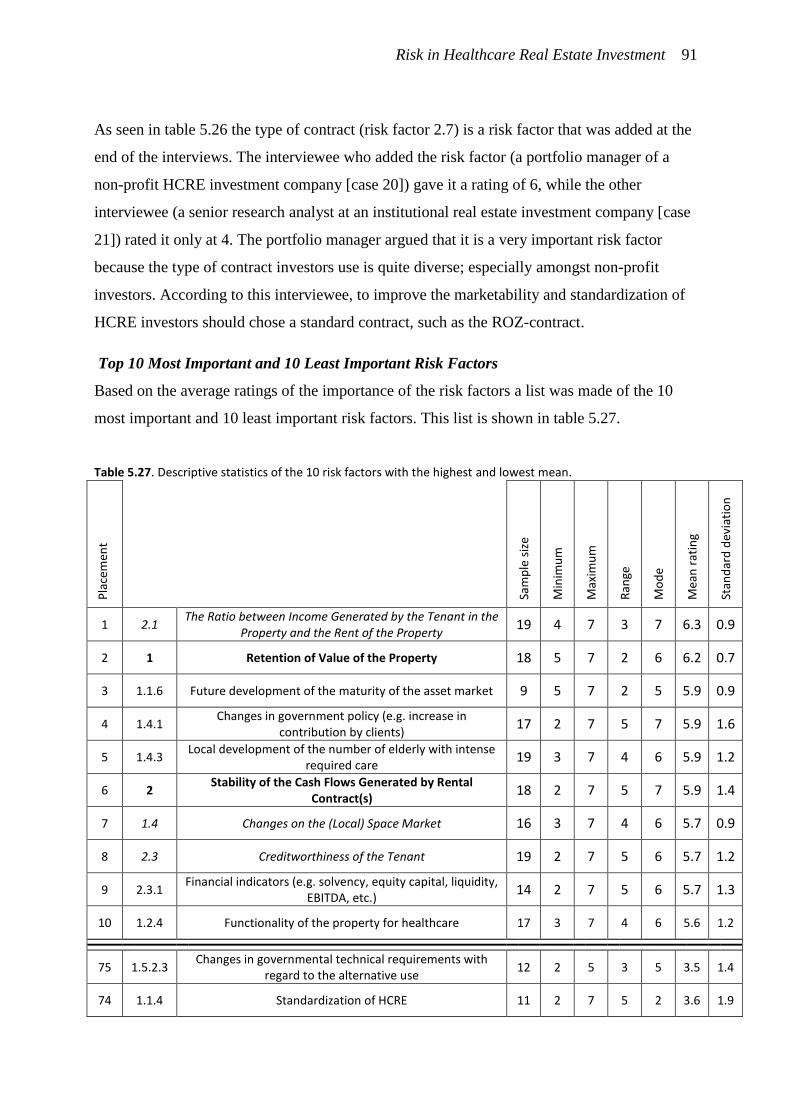
Risk in Healthcare Real Estate Investment 91
As seen in table 5.26 the type of contract (risk factor 2.7) is a risk factor that was added at the
end of the interviews. The interviewee who added the risk factor (a portfolio manager of a
non-profit HCRE investment company [case 20]) gave it a rating of 6, while the other
interviewee (a senior research analyst at an institutional real estate investment company [case
21]) rated it only at 4. The portfolio manager argued that it is a very important risk factor
because the type of contract investors use is quite diverse; especially amongst non-profit
investors. According to this interviewee, to improve the marketability and standardization of
HCRE investors should chose a standard contract, such as the ROZ-contract.
Top 10 Most Important and 10 Least Important Risk Factors
Based on the average ratings of the importance of the risk factors a list was made of the 10
most important and 10 least important risk factors. This list is shown in table 5.27.
Table 5.27. Descriptive statistics of the 10 risk factors with the highest and lowest mean.
Pla
cem
ent
Sam
ple
siz
e
Min
imu
m
Max
imu
m
Ran
ge
Mo
de
Mea
n r
atin
g
Stan
dar
d d
evia
tio
n
1 2.1 The Ratio between Income Generated by the Tenant in the
Property and the Rent of the Property 19 4 7 3 7 6.3 0.9
2 1 Retention of Value of the Property 18 5 7 2 6 6.2 0.7
3 1.1.6 Future development of the maturity of the asset market 9 5 7 2 5 5.9 0.9
4 1.4.1 Changes in government policy (e.g. increase in
contribution by clients) 17 2 7 5 7 5.9 1.6
5 1.4.3 Local development of the number of elderly with intense
required care 19 3 7 4 6 5.9 1.2
6 2 Stability of the Cash Flows Generated by Rental
Contract(s) 18 2 7 5 7 5.9 1.4
7 1.4 Changes on the (Local) Space Market 16 3 7 4 6 5.7 0.9
8 2.3 Creditworthiness of the Tenant 19 2 7 5 6 5.7 1.2
9 2.3.1 Financial indicators (e.g. solvency, equity capital, liquidity,
EBITDA, etc.) 14 2 7 5 6 5.7 1.3
10 1.2.4 Functionality of the property for healthcare 17 3 7 4 6 5.6 1.2
75 1.5.2.3 Changes in governmental technical requirements with
regard to the alternative use 12 2 5 3 5 3.5 1.4
74 1.1.4 Standardization of HCRE 11 2 7 5 2 3.6 1.9
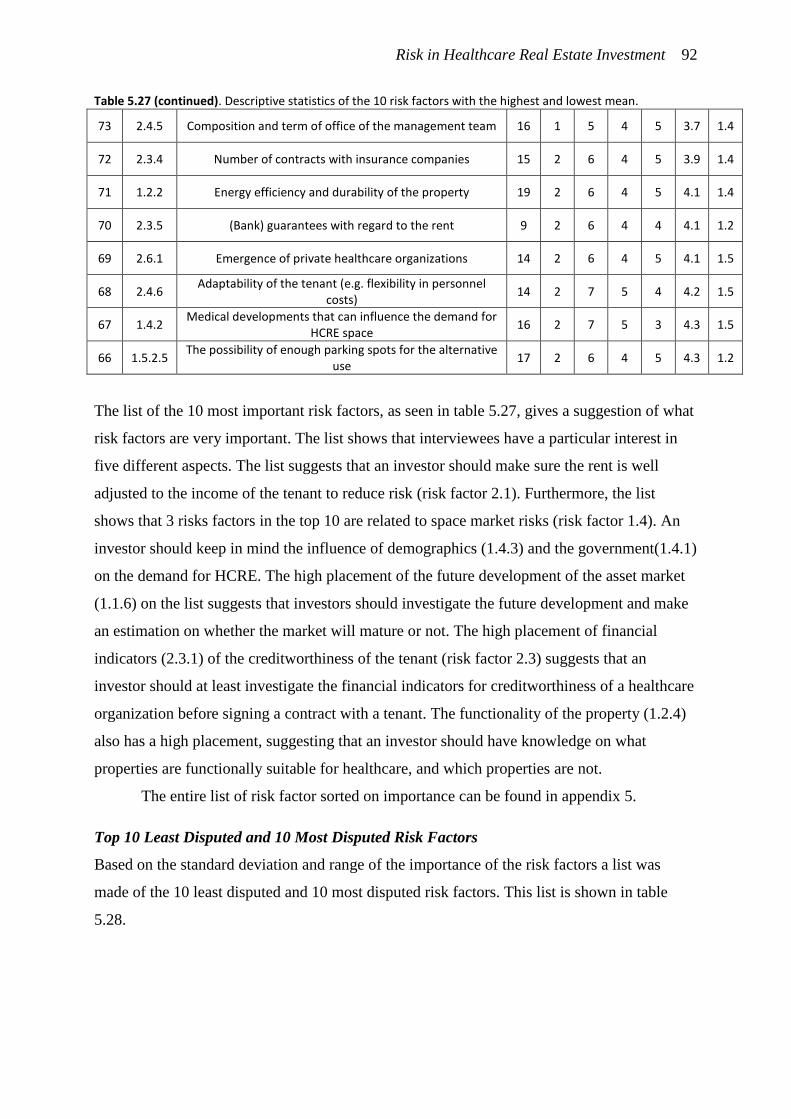
Risk in Healthcare Real Estate Investment 92
Table 5.27 (continued). Descriptive statistics of the 10 risk factors with the highest and lowest mean.
73 2.4.5 Composition and term of office of the management team 16 1 5 4 5 3.7 1.4
72 2.3.4 Number of contracts with insurance companies 15 2 6 4 5 3.9 1.4
71 1.2.2 Energy efficiency and durability of the property 19 2 6 4 5 4.1 1.4
70 2.3.5 (Bank) guarantees with regard to the rent 9 2 6 4 4 4.1 1.2
69 2.6.1 Emergence of private healthcare organizations 14 2 6 4 5 4.1 1.5
68 2.4.6 Adaptability of the tenant (e.g. flexibility in personnel
costs) 14 2 7 5 4 4.2 1.5
67 1.4.2 Medical developments that can influence the demand for
HCRE space 16 2 7 5 3 4.3 1.5
66 1.5.2.5 The possibility of enough parking spots for the alternative
use 17 2 6 4 5 4.3 1.2
The list of the 10 most important risk factors, as seen in table 5.27, gives a suggestion of what
risk factors are very important. The list shows that interviewees have a particular interest in
five different aspects. The list suggests that an investor should make sure the rent is well
adjusted to the income of the tenant to reduce risk (risk factor 2.1). Furthermore, the list
shows that 3 risks factors in the top 10 are related to space market risks (risk factor 1.4). An
investor should keep in mind the influence of demographics (1.4.3) and the government(1.4.1)
on the demand for HCRE. The high placement of the future development of the asset market
(1.1.6) on the list suggests that investors should investigate the future development and make
an estimation on whether the market will mature or not. The high placement of financial
indicators (2.3.1) of the creditworthiness of the tenant (risk factor 2.3) suggests that an
investor should at least investigate the financial indicators for creditworthiness of a healthcare
organization before signing a contract with a tenant. The functionality of the property (1.2.4)
also has a high placement, suggesting that an investor should have knowledge on what
properties are functionally suitable for healthcare, and which properties are not.
The entire list of risk factor sorted on importance can be found in appendix 5.
Top 10 Least Disputed and 10 Most Disputed Risk Factors
Based on the standard deviation and range of the importance of the risk factors a list was
made of the 10 least disputed and 10 most disputed risk factors. This list is shown in table
5.28.
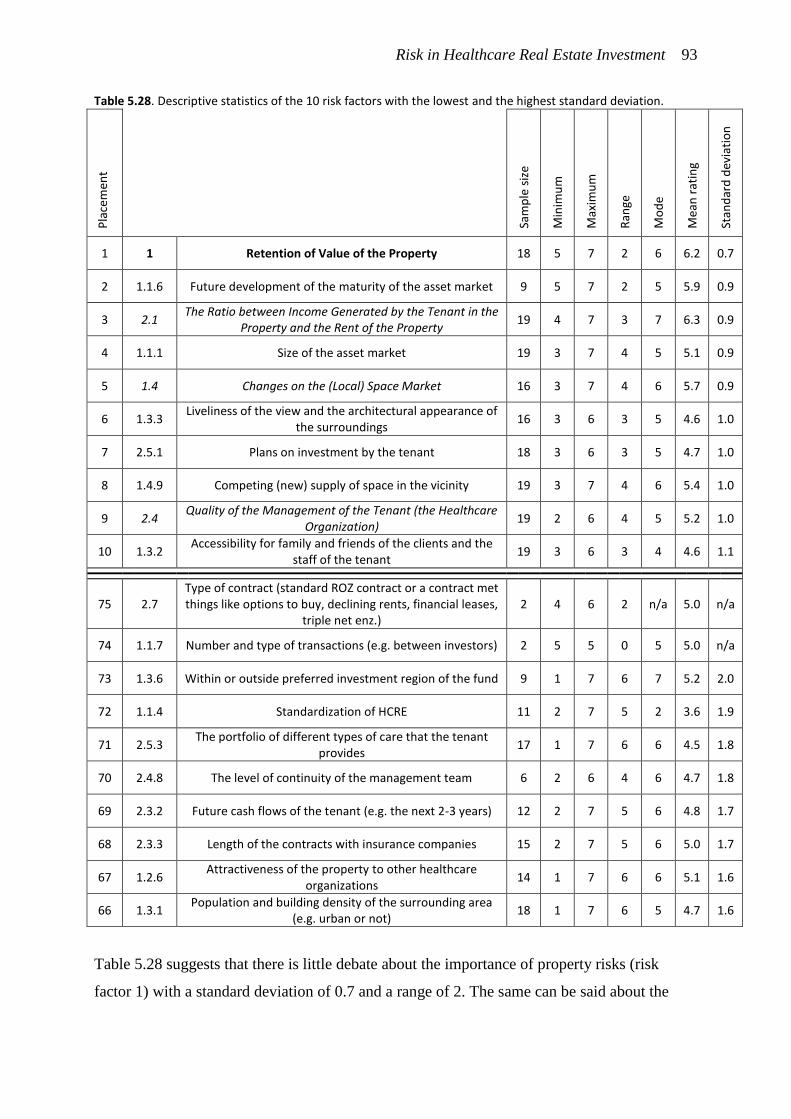
Risk in Healthcare Real Estate Investment 93
Table 5.28. Descriptive statistics of the 10 risk factors with the lowest and the highest standard deviation. P
lace
men
t
Sam
ple
siz
e
Min
imu
m
Max
imu
m
Ran
ge
Mo
de
Mea
n r
atin
g
Stan
dar
d d
evia
tio
n
1 1 Retention of Value of the Property 18 5 7 2 6 6.2 0.7
2 1.1.6 Future development of the maturity of the asset market 9 5 7 2 5 5.9 0.9
3 2.1 The Ratio between Income Generated by the Tenant in the
Property and the Rent of the Property 19 4 7 3 7 6.3 0.9
4 1.1.1 Size of the asset market 19 3 7 4 5 5.1 0.9
5 1.4 Changes on the (Local) Space Market 16 3 7 4 6 5.7 0.9
6 1.3.3 Liveliness of the view and the architectural appearance of
the surroundings 16 3 6 3 5 4.6 1.0
7 2.5.1 Plans on investment by the tenant 18 3 6 3 5 4.7 1.0
8 1.4.9 Competing (new) supply of space in the vicinity 19 3 7 4 6 5.4 1.0
9 2.4 Quality of the Management of the Tenant (the Healthcare
Organization) 19 2 6 4 5 5.2 1.0
10 1.3.2 Accessibility for family and friends of the clients and the
staff of the tenant 19 3 6 3 4 4.6 1.1
75 2.7 Type of contract (standard ROZ contract or a contract met things like options to buy, declining rents, financial leases,
triple net enz.) 2 4 6 2 n/a 5.0 n/a
74 1.1.7 Number and type of transactions (e.g. between investors) 2 5 5 0 5 5.0 n/a
73 1.3.6 Within or outside preferred investment region of the fund 9 1 7 6 7 5.2 2.0
72 1.1.4 Standardization of HCRE 11 2 7 5 2 3.6 1.9
71 2.5.3 The portfolio of different types of care that the tenant
provides 17 1 7 6 6 4.5 1.8
70 2.4.8 The level of continuity of the management team 6 2 6 4 6 4.7 1.8
69 2.3.2 Future cash flows of the tenant (e.g. the next 2-3 years) 12 2 7 5 6 4.8 1.7
68 2.3.3 Length of the contracts with insurance companies 15 2 7 5 6 5.0 1.7
67 1.2.6 Attractiveness of the property to other healthcare
organizations 14 1 7 6 6 5.1 1.6
66 1.3.1 Population and building density of the surrounding area
(e.g. urban or not) 18 1 7 6 5 4.7 1.6
Table 5.28 suggests that there is little debate about the importance of property risks (risk
factor 1) with a standard deviation of 0.7 and a range of 2. The same can be said about the
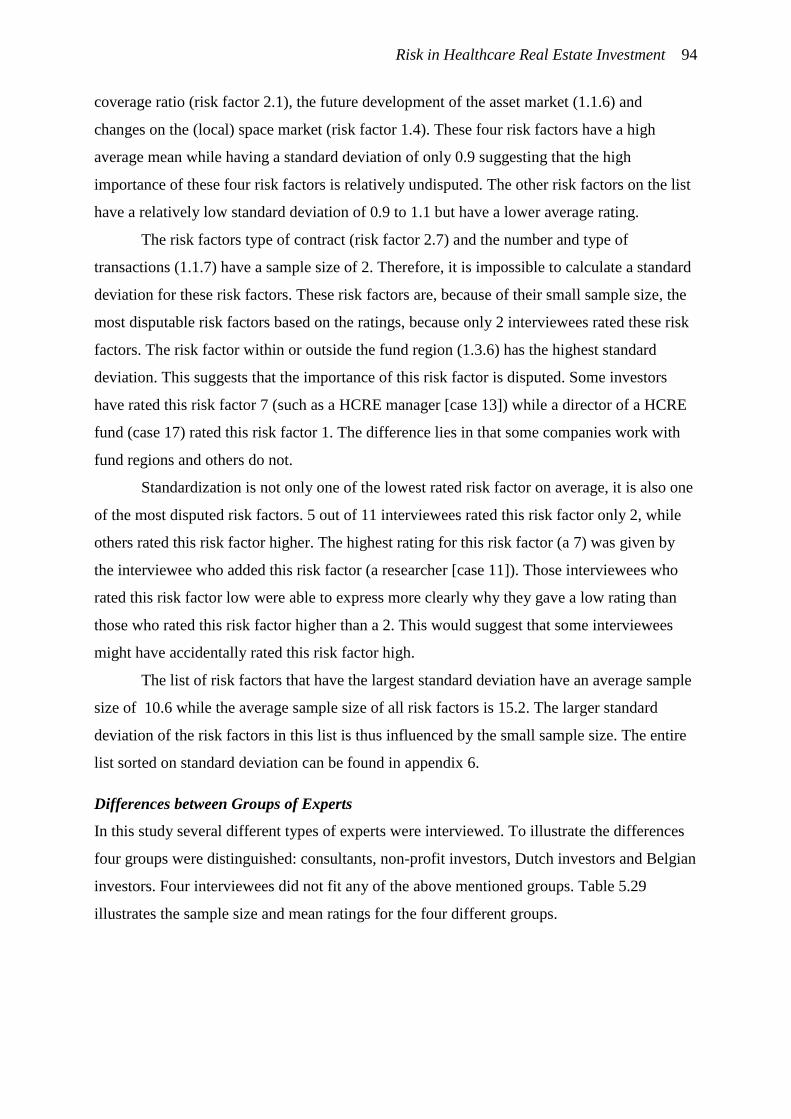
Risk in Healthcare Real Estate Investment 94
coverage ratio (risk factor 2.1), the future development of the asset market (1.1.6) and
changes on the (local) space market (risk factor 1.4). These four risk factors have a high
average mean while having a standard deviation of only 0.9 suggesting that the high
importance of these four risk factors is relatively undisputed. The other risk factors on the list
have a relatively low standard deviation of 0.9 to 1.1 but have a lower average rating.
The risk factors type of contract (risk factor 2.7) and the number and type of
transactions (1.1.7) have a sample size of 2. Therefore, it is impossible to calculate a standard
deviation for these risk factors. These risk factors are, because of their small sample size, the
most disputable risk factors based on the ratings, because only 2 interviewees rated these risk
factors. The risk factor within or outside the fund region (1.3.6) has the highest standard
deviation. This suggests that the importance of this risk factor is disputed. Some investors
have rated this risk factor 7 (such as a HCRE manager [case 13]) while a director of a HCRE
fund (case 17) rated this risk factor 1. The difference lies in that some companies work with
fund regions and others do not.
Standardization is not only one of the lowest rated risk factor on average, it is also one
of the most disputed risk factors. 5 out of 11 interviewees rated this risk factor only 2, while
others rated this risk factor higher. The highest rating for this risk factor (a 7) was given by
the interviewee who added this risk factor (a researcher [case 11]). Those interviewees who
rated this risk factor low were able to express more clearly why they gave a low rating than
those who rated this risk factor higher than a 2. This would suggest that some interviewees
might have accidentally rated this risk factor high.
The list of risk factors that have the largest standard deviation have an average sample
size of 10.6 while the average sample size of all risk factors is 15.2. The larger standard
deviation of the risk factors in this list is thus influenced by the small sample size. The entire
list sorted on standard deviation can be found in appendix 6.
Differences between Groups of Experts
In this study several different types of experts were interviewed. To illustrate the differences
four groups were distinguished: consultants, non-profit investors, Dutch investors and Belgian
investors. Four interviewees did not fit any of the above mentioned groups. Table 5.29
illustrates the sample size and mean ratings for the four different groups.
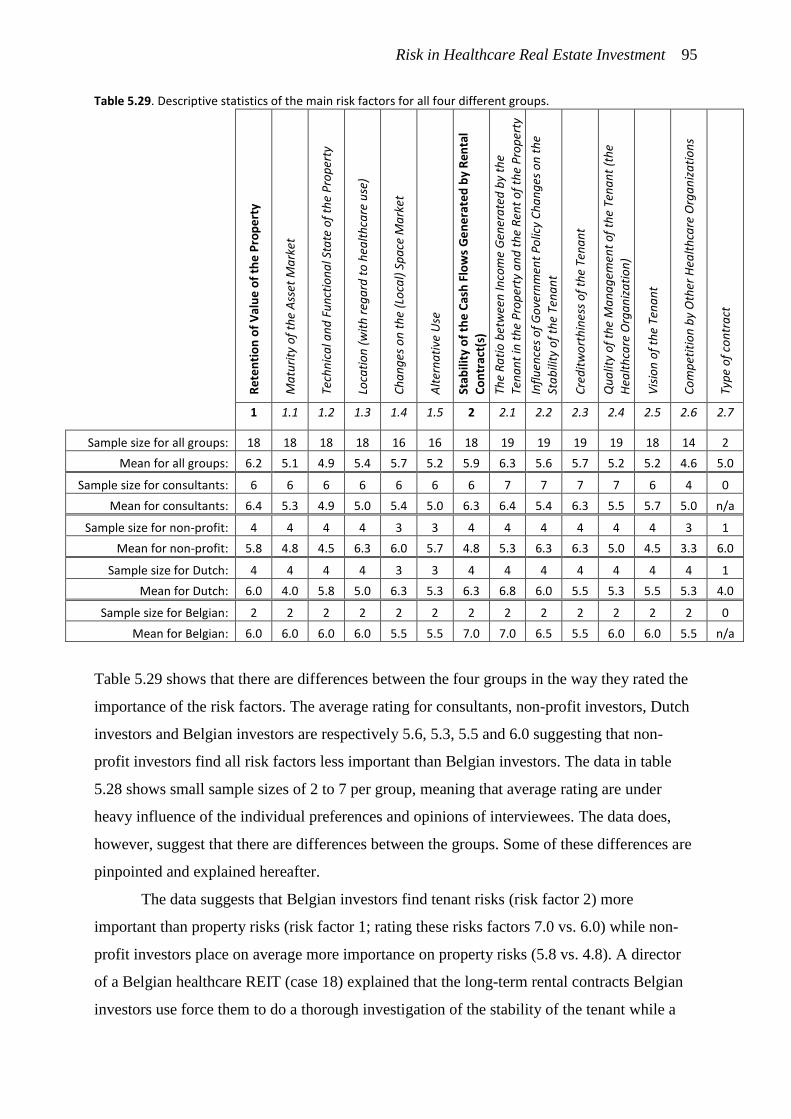
Risk in Healthcare Real Estate Investment 95
Table 5.29. Descriptive statistics of the main risk factors for all four different groups.
Re
ten
tio
n o
f V
alu
e o
f th
e P
rop
ert
y
Ma
turi
ty o
f th
e A
sset
Ma
rket
Tech
nic
al a
nd
Fu
nct
ion
al S
tate
of
the
Pro
per
ty
Loca
tio
n (
wit
h r
ega
rd t
o h
ealt
hca
re u
se)
Ch
an
ges
on
th
e (L
oca
l) S
pa
ce M
ark
et
Alt
ern
ati
ve U
se
Stab
ility
of
the
Cas
h F
low
s G
en
era
ted
by
Ren
tal
Co
ntr
act(
s)
The
Ra
tio
bet
wee
n In
com
e G
ener
ate
d b
y th
e
Ten
an
t in
th
e P
rop
erty
an
d t
he
Ren
t o
f th
e P
rop
erty
Infl
uen
ces
of
Go
vern
men
t P
olic
y C
ha
ng
es o
n t
he
Sta
bili
ty o
f th
e Te
na
nt
Cre
dit
wo
rth
ines
s o
f th
e Te
na
nt
Qu
alit
y o
f th
e M
an
ag
emen
t o
f th
e Te
na
nt
(th
e
Hea
lth
care
Org
an
iza
tio
n)
Vis
ion
of
the
Ten
an
t
Co
mp
etit
ion
by
Oth
er H
ealt
hca
re O
rga
niz
ati
on
s
Typ
e o
f co
ntr
act
1 1.1 1.2 1.3 1.4 1.5 2 2.1 2.2 2.3 2.4 2.5 2.6 2.7
Sample size for all groups: 18 18 18 18 16 16 18 19 19 19 19 18 14 2
Mean for all groups: 6.2 5.1 4.9 5.4 5.7 5.2 5.9 6.3 5.6 5.7 5.2 5.2 4.6 5.0
Sample size for consultants: 6 6 6 6 6 6 6 7 7 7 7 6 4 0
Mean for consultants: 6.4 5.3 4.9 5.0 5.4 5.0 6.3 6.4 5.4 6.3 5.5 5.7 5.0 n/a
Sample size for non-profit: 4 4 4 4 3 3 4 4 4 4 4 4 3 1
Mean for non-profit: 5.8 4.8 4.5 6.3 6.0 5.7 4.8 5.3 6.3 6.3 5.0 4.5 3.3 6.0
Sample size for Dutch: 4 4 4 4 3 3 4 4 4 4 4 4 4 1
Mean for Dutch: 6.0 4.0 5.8 5.0 6.3 5.3 6.3 6.8 6.0 5.5 5.3 5.5 5.3 4.0
Sample size for Belgian: 2 2 2 2 2 2 2 2 2 2 2 2 2 0
Mean for Belgian: 6.0 6.0 6.0 6.0 5.5 5.5 7.0 7.0 6.5 5.5 6.0 6.0 5.5 n/a
Table 5.29 shows that there are differences between the four groups in the way they rated the
importance of the risk factors. The average rating for consultants, non-profit investors, Dutch
investors and Belgian investors are respectively 5.6, 5.3, 5.5 and 6.0 suggesting that non-
profit investors find all risk factors less important than Belgian investors. The data in table
5.28 shows small sample sizes of 2 to 7 per group, meaning that average rating are under
heavy influence of the individual preferences and opinions of interviewees. The data does,
however, suggest that there are differences between the groups. Some of these differences are
pinpointed and explained hereafter.
The data suggests that Belgian investors find tenant risks (risk factor 2) more
important than property risks (risk factor 1; rating these risks factors 7.0 vs. 6.0) while non-
profit investors place on average more importance on property risks (5.8 vs. 4.8). A director
of a Belgian healthcare REIT (case 18) explained that the long-term rental contracts Belgian
investors use force them to do a thorough investigation of the stability of the tenant while a
Risk in Healthcare Real Estate Investment 96
portfolio manager of a non-profit investment company (case 20) explained that the tenant
risks are subordinate to property risks. The portfolio manager explained that in the long
history of their company they experienced that property risks are more important.
Dutch investors find the maturity of the asset market (risk factor 1.1) only neutrally
important on average while Belgian investors find it very important. One Belgian asset
manager (case 22) explained that an immature asset market results in higher cap rates while
Dutch investors, such as a director of a HCRE fund (case 10), explained that the low maturity
of the market also offers opportunities to those investors willing to take the lead.
The technical and functional state (risk factor 1.2) is more important to investors (both
Dutch and Belgian; respectively 5.8 and 6.0) than to consultants and non-profit investors
(respectively 4.9 and 4.5). A Dutch HCRE manager (case 13) explained that Dutch investors
prefer to invest in new properties and a director of a Belgian healthcare REIT (case 18)
argued that the properties should be in a good technical and functional state in support of the
tenants.
Location (risk factor 1.3) is on average less important to Dutch investors and
consultant (respectively 5.0 and 5.0) than to Belgian and non-profit investors (respectively 6.0
and 6.3). Dutch investors and consultants explained that to them the local HCRE space market
is more important than aspects like accessibility. E.g. a HCRE consultant (case 19) explained
that location is only of low importance while the number of elderly in a region (1.4.3) is
extremely important. It seems that Belgian and non-profit investors misunderstood that the
local space market and location were separated on the list of risk factors and accidentally
rated location high while meaning that the local space market is of high importance.
With regard to the importance of the local space market (risk factor 1.4) and
alternative use (risk factor 1.5) there are no large differences between the average rating of the
four groups. The small differences can be explained by differences in opinions of the
individual interviewees.
The coverage ratio (risk factor 2.1) is rated lower on average by non-profit investors
(only 5.3 as opposed to 6.4, 6.8 and 7.0). A portfolio manager of a non-profit investment
company (case 20) rated the coverage ratio only 4, explaining that in his experience
healthcare organizations can operate very differently resulting in a big differences in the
economic effectiveness of healthcare organizations.
The data suggests that the influence of the government (risk factor 2.2) is less
important according to consultants (5.4 on average) than to investors (6.2 on average). This
suggests that investors are more wary of government influences than consultants. According
Risk in Healthcare Real Estate Investment 97
to a policy consultant (case 14) and another consultant (case 1) the influence of the
government is overrated as a risk factor.
Interviewees from all four different groups seem to agree on the importance of the
creditworthiness (risk factor 2.3). Small differences in average importance can be explained
by slight differences in opinions of the individual interviewees.
The quality of the management (risk factor 2.4) and the vision of the tenant (risk factor
2.5) is on average more important to Belgian investors (6.0 and 6.0 on average) than to non-
profit investors (5.0 and 4.5 on average). Non-profit investors place more importance on
property risks than tenant risks while Belgian investors do the opposite. For this reason non-
profit investors seem to find the quality of the management and the vision of less importance.
The data also suggests that non-profit investors perceive less risk in competition by
other investors (risk factor 2.6) by rating it only 3.3 on average as opposed to 5.2 on average
by consultants and other investors. An asset manager of a non-profit investment company
(case 7) argued that there is no fierce competition between healthcare organizations. A
portfolio manager of another non-profit investment company (case 20) suggested that
competition can also offer opportunity to switch tenant.
Because of the small sample size of only 2 on the importance of the type of contract
(risk factor 2.7) no results are found on the differences between groups with regard to this risk
factor.
5.3. Differences in Points of View between Interviewees
During the interviews it became evident that there are two different points of view on HCRE
investment. One viewpoint held by some interviewees is that risk management in HCRE
investment predominantly is a matter of reducing risk with regard to the stability of the tenant.
These interviewees saw investment in HCRE as vastly different from investing in other types
of real estate. Other interviewees held the position that reducing risk when investing in HCRE
is predominantly a matter of investing in the right kind of property, similar to investing in
other types of real estate. In this study these two groups are called 'Corporate Investors' and
'Real Estate Investors'. Not all interviewees can be fitted into one of these categories but often
fit somewhere in between. There were no interviewees who disregarded all risk factors related
to the devaluation of the property and no interviewees who completely disregarded all risk
factors related to tenant stability.
Corporate Investors see investment in HCRE as a means to finance a healthcare
organization. Their focus is on finding a stable tenant with which they can start a partnership.
Risk in Healthcare Real Estate Investment 98
Often the goal of these partnerships is to take over a large part of the existing portfolio of the
healthcare organization and to invest in future properties rented by the same tenant. These
type of investors prefer contracts of over 25 years and expect that the value of the property at
the end of the contract will be reduced to near the value of the land. The risk factors Corporate
Investors find most important are similar to those that banks find important when providing
loans to a healthcare organization. One interview with a bank (case 9) showed that this
particular bank provided loans on the basis of a whole set of information on the healthcare
organization and did not consider property risks. Corporate Investors, however, do consider
property risks. However, they allow the risk of low marketability of a property to be balanced
out by having less risk over the cash flows of a property through long-term rental contracts
with a stable tenant. The focus of the Corporate Investor is thus on direct return whilst
accepting a negative indirect return on the property. This viewpoint is held predominantly by
Belgian investors and some non-profit investors. Investors with this viewpoint have proven in
the past that their way of investing results in stable and high returns but have difficulty
finding a tenant willing to agree on long-term rental contracts.
Real Estate Investors see investment in HCRE as investing in a new and upcoming
real estate investment category. Their focus lies on finding properties with low risk with
regard to their location, the local space market and the technical and functional state. These
investors believe that, like with other types of real estate, a properly functioning property on a
good location in a market with high demand should be able to attract a tenant. Therefore, the
stability of the tenant is of less importance because a bankrupt tenant should be replaceable by
another tenant. Real Estate Investors do look at the stability of the tenant because they realize
that the immaturity of the HCRE market requires compensation. They compensate by signing
rental contracts with a term of 15 years with a stable tenant, but expect that rental contracts
will become shorter (closer to 9 year years) as the market matures. Real Estate Investors
expect that healthcare organizations will not sign longer rental contracts than 15 years. They
expect both direct and indirect return; they think the property can retain its value even towards
the end of the rental contract. At the end of the rental contract they expect a new rental
contract of similar or even higher rent can be signed.
5.4. The Influence of the Length of Rental Contracts on the Risk
Interviewees were also asked about the influence of the length of the rental contract on the
risk. Interviewees were asked to rate the relative importance of property risks and tenant risks
at three different lengths of rental contracts (10, 20 and 30 years) using the following scale: 1
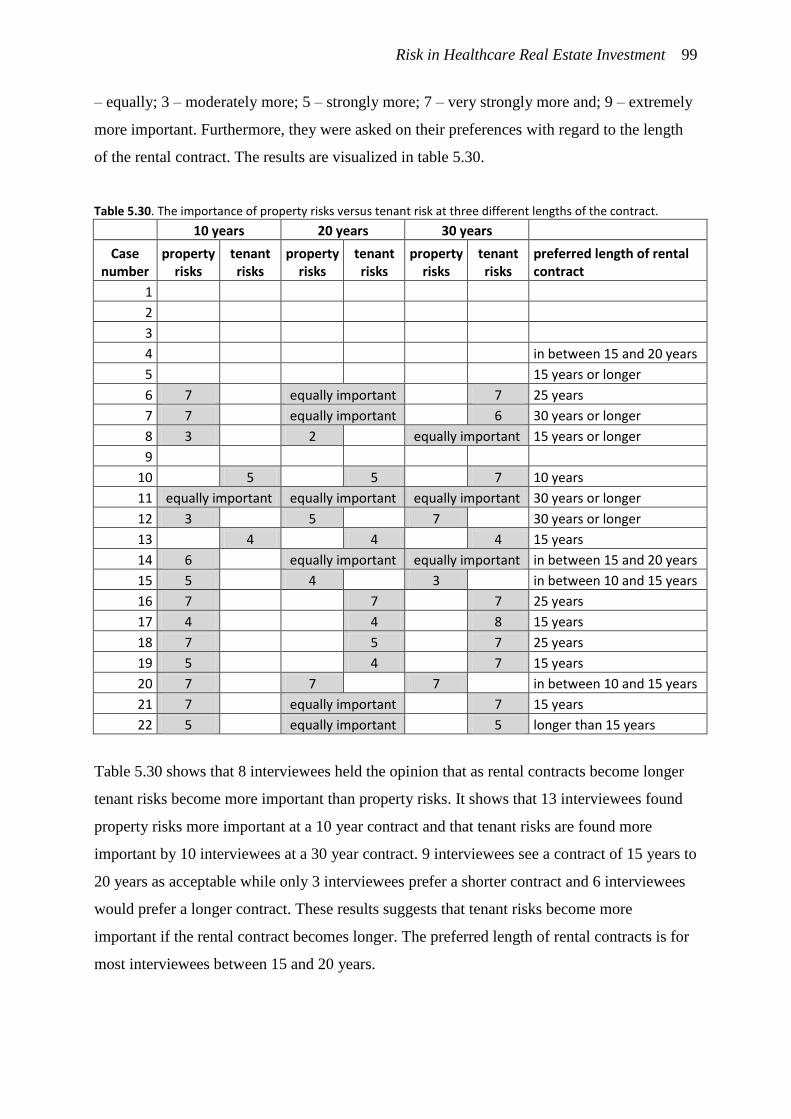
Risk in Healthcare Real Estate Investment 99
– equally; 3 – moderately more; 5 – strongly more; 7 – very strongly more and; 9 – extremely
more important. Furthermore, they were asked on their preferences with regard to the length
of the rental contract. The results are visualized in table 5.30.
Table 5.30. The importance of property risks versus tenant risk at three different lengths of the contract.
10 years 20 years 30 years
Case number
property risks
tenant risks
property risks
tenant risks
property risks
tenant risks
preferred length of rental contract
1 2 3 4
in between 15 and 20 years
5
15 years or longer
6 7
equally important
7 25 years
7 7
equally important
6 30 years or longer
8 3
2
equally important 15 years or longer
9 10
5
5
7 10 years
11 equally important equally important equally important 30 years or longer
12 3
5
7
30 years or longer
13
4
4
4 15 years
14 6
equally important equally important in between 15 and 20 years
15 5
4
3
in between 10 and 15 years
16 7
7
7 25 years
17 4
4
8 15 years
18 7
5
7 25 years
19 5
4
7 15 years
20 7
7
7
in between 10 and 15 years
21 7
equally important
7 15 years
22 5
equally important
5 longer than 15 years
Table 5.30 shows that 8 interviewees held the opinion that as rental contracts become longer
tenant risks become more important than property risks. It shows that 13 interviewees found
property risks more important at a 10 year contract and that tenant risks are found more
important by 10 interviewees at a 30 year contract. 9 interviewees see a contract of 15 years to
20 years as acceptable while only 3 interviewees prefer a shorter contract and 6 interviewees
would prefer a longer contract. These results suggests that tenant risks become more
important if the rental contract becomes longer. The preferred length of rental contracts is for
most interviewees between 15 and 20 years.
Risk in Healthcare Real Estate Investment 100
5.5. Chapter Conclusion
This chapter shows the results of this study. The attempt to analyze risk in HCRE investment
by finding the risk factors has resulted in an expansion of the list of risk factors. Several risks
that were mentioned during the interviews were added to the list of risk factors resulting in an
expansion from 24 to 75 risk factors. The list of risk factors obtained through literature
research was expanded by both quantifiable and qualitative risk factors at both property type
and property level.
Furthermore, data was collected in an attempt to analyze how important the individual
risk factors are on a 7-point scale from 1- not at all important to 7 - extremely important. The
data shows that risk factors have a standard deviation of 0.7 to 2.0, suggesting that there is
still a lot of uncertainty over the importance of the risk factors. The average rating of 4.9
shows that risk factors were asymmetrically rated. Interviewees more often found risk factors
more important than less important suggesting that interviewees had difficulty in prioritizing
which risk factors are more important than others. A possible explanation is that interviewees
have a tendency to find risk factors more important when they are uncertain over the
importance.
The results also show that there are two distinguishable points of view in HCRE
investment. Real Estate Investors make higher estimations of the height of the exit value than
Corporate Investors, suggesting that they perceive less uncertainty over the exit value.
Another explanation of this phenomenon could be that Real Estate Investors are less risk
adverse than Corporate Investors.
The data collected on the length of the rental contract and the importance of property
risks and tenant risks suggests that tenant risks become more important if the rental contract
becomes longer. The preferred length of rental contracts is for most interviewees in between
15 and 20 years.

Risk in Healthcare Real Estate Investment 101
6. Conclusions and Discussion
The goal of this study is to investigate risk in HCRE investment by finding the relevant risk
factors and their importance. The method to come to these results is by reviewing the
literature and doing 22 interviews with experts on HCRE investment. In the previous chapter
the results of the literature review and interviews were presented. These findings have both
theoretical and practical implications.
6.1. Theoretical and Practical Implications
Addition to Existing Literature
The results of this study have expanded the existing knowledge on the risk of investing in
HCRE with additional risk factors. The result is a more comprehensive list of risk factors
which includes risk mentioned in the literature and new risk which were added by experts on
HCRE investment. Furthermore, data was collected on the importance of the risk factors
showing which risk factors are particularly important and which risk factors are less
important. Differences in viewpoints were found on the importance of risk factors as well an
uncertainty over the importance resulting in a wider range of answers by different
interviewees and a tendency to find risk factor more important. These findings add to the
existing literature in a number of ways. This study is different from the existing literature
because it is a qualitative study on the risk factors at property type and property level. It
shows that besides macro-economic risk factors there are numerous micro-level risk factors
influencing the risk perception of investors. It shows differences in risk perception between
different types of investors and consultants and that there are different ways to approach
HCRE investment. Furthermore, it uncovers the uncertainties of investing in HCRE and
shows that uncertainty has a role in risk perception in HCRE investment. The results found in
this research can be used as a reference in future studies on HCRE investment.
Input for Improved Investment Decisions
The findings of this study offer input to make better investment decisions. The risk factors of
HCRE investment found in this study can be used by real estate investors to make a
comprehensive risk analysis by analyzing the property and the tenant on the 75 risk factors
that were found in this study. In current practice the value of properties is often determined
using the sales comparison method after which the IRR can be calculated. The investor can
then estimate whether the IRR is in line with the risk the investment holds. The findings offer
an investor information on the risks factors of HCRE investment and thereby offer the
Risk in Healthcare Real Estate Investment 102
investor the building blocks to make an analysis of the risk. An investor can use a risk
analysis to improve the adjustment of the return requirements to future investments and to
substantiate investment decisions.
Input for Better Estimations of Property Values
The list of risk factors and their importance offer input to improve appraising HCRE when the
income approach is used. The sales comparison method is not always applicable to HCRE due
to the lack of comparable transactions. For this reason HCRE has also been appraised using
the income approach. The difficulty with appraising using the income approach is to make
correct estimations on the return requirements. In the past appraisers used rough estimates of
the IRR or the gross initial yield. Because the correctness of return estimates are so vital for
the feasibility of valuation based on the income approach, the findings of this study can
further substantiate the choice of the return requirements. The results of this study can be used
in to improve risk analysis to come to a better understanding of return requirements in HCRE
investment.
Increase in Transparency and Maturity of the HCRE Asset Market
The results of this study will contribute to the maturity of the HCRE market in a number of
ways. It presents information investors can use to make better estimations of the risk of
HCRE investment. Furthermore, it takes away some of the uncertainty of investing in HCRE.
The comprehensive list of risk factors obtained through extensive literature research and 22
interview can give investors a sense of control over the management of risk in HCRE
investment. Investors will be able to use the information to manage the risk and to steer on
investment in properties that pose less risk. The insights and information of this study have
thus increased the transparency of the HCRE asset market and contributes to the maturity.
Implications of the Length of Rental Contracts on HCRE Risk Management
The results suggest that tenant risks become more important if the rental contract becomes
longer. The preferred length of rental contracts is for most interviewees between 15 and 20
years. This means that if rental contracts become longer investors need to pay more attention
to tenant risks and make sure the cash flows are stable. If rental contracts become shorter the
investor should pay more attention to property risks and make sure that the exit value is
higher. This can only be the case in properties with higher retention of value. Properties that
lose their value quickly can not be combined with short rental contracts unless the initial
investment is very low. Therefore, if rental contracts become shorter, risk management will
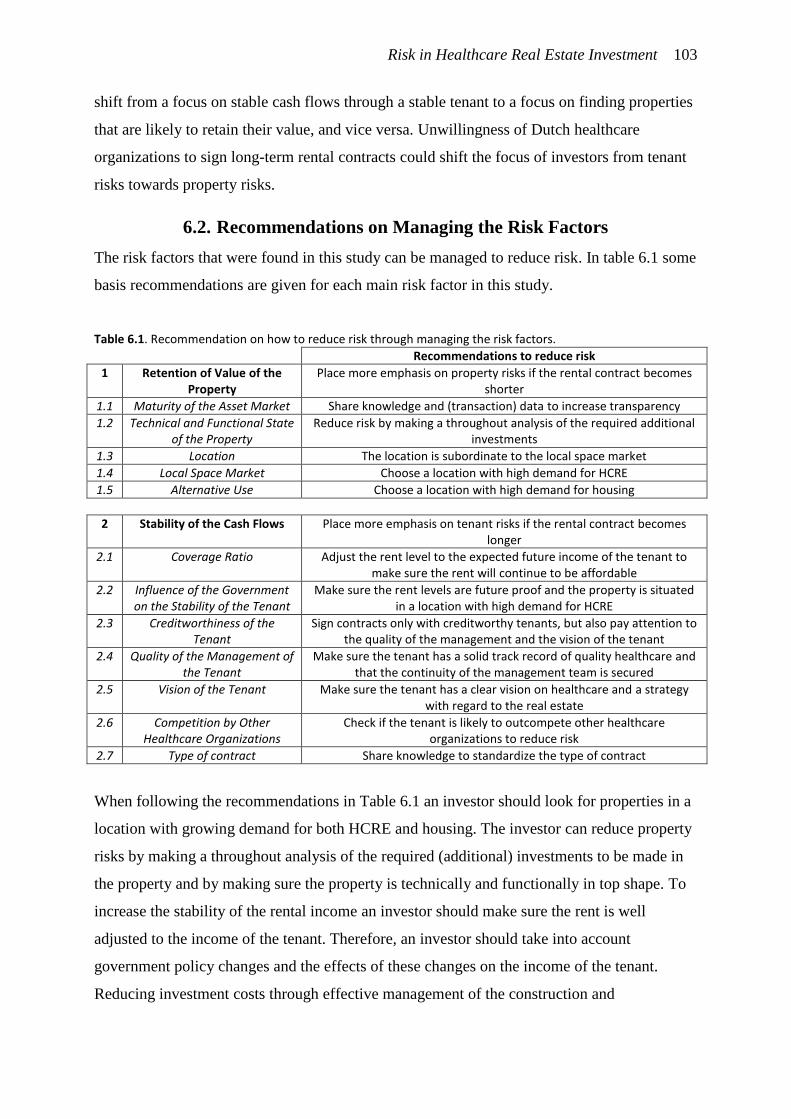
Risk in Healthcare Real Estate Investment 103
shift from a focus on stable cash flows through a stable tenant to a focus on finding properties
that are likely to retain their value, and vice versa. Unwillingness of Dutch healthcare
organizations to sign long-term rental contracts could shift the focus of investors from tenant
risks towards property risks.
6.2. Recommendations on Managing the Risk Factors
The risk factors that were found in this study can be managed to reduce risk. In table 6.1 some
basis recommendations are given for each main risk factor in this study.
Table 6.1. Recommendation on how to reduce risk through managing the risk factors.
Recommendations to reduce risk
1 Retention of Value of the Property
Place more emphasis on property risks if the rental contract becomes shorter
1.1 Maturity of the Asset Market Share knowledge and (transaction) data to increase transparency
1.2 Technical and Functional State of the Property
Reduce risk by making a throughout analysis of the required additional investments
1.3 Location The location is subordinate to the local space market
1.4 Local Space Market Choose a location with high demand for HCRE
1.5 Alternative Use Choose a location with high demand for housing
2 Stability of the Cash Flows Place more emphasis on tenant risks if the rental contract becomes longer
2.1 Coverage Ratio Adjust the rent level to the expected future income of the tenant to make sure the rent will continue to be affordable
2.2 Influence of the Government on the Stability of the Tenant
Make sure the rent levels are future proof and the property is situated in a location with high demand for HCRE
2.3 Creditworthiness of the Tenant
Sign contracts only with creditworthy tenants, but also pay attention to the quality of the management and the vision of the tenant
2.4 Quality of the Management of the Tenant
Make sure the tenant has a solid track record of quality healthcare and that the continuity of the management team is secured
2.5 Vision of the Tenant Make sure the tenant has a clear vision on healthcare and a strategy with regard to the real estate
2.6 Competition by Other Healthcare Organizations
Check if the tenant is likely to outcompete other healthcare organizations to reduce risk
2.7 Type of contract Share knowledge to standardize the type of contract
When following the recommendations in Table 6.1 an investor should look for properties in a
location with growing demand for both HCRE and housing. The investor can reduce property
risks by making a throughout analysis of the required (additional) investments to be made in
the property and by making sure the property is technically and functionally in top shape. To
increase the stability of the rental income an investor should make sure the rent is well
adjusted to the income of the tenant. Therefore, an investor should take into account
government policy changes and the effects of these changes on the income of the tenant.
Reducing investment costs through effective management of the construction and
Risk in Healthcare Real Estate Investment 104
maintenance of the property is an effective way to be able to lower the rent and make sure the
property will remain affordable.
To mitigate property risks an investor can choose to sign only long-term rental
contracts and in that way shift towards managing tenant risks. When investing in HCRE an
investor should always take into account the creditworthiness of the tenant. Although the
creditworthiness is important, an investor should also make sure the tenant has a solid track
record and a stable and reliable management team. The tenant should also have a clear vision
on healthcare and it should be clear that the decision to rent a property from the investor is in
line with their strategy.
To further reduce the overall risk of investing in HCRE investors can share their
knowledge an thereby increase transparency and improve the maturity of the HCRE market.
Because uncertainty has a big impact on HCRE investment, sharing knowledge can
significantly contribute to reducing risk and increase the investment volume.
6.3. Recommendations for Further Studies
The method of analysis of this study has resulted in a very long and comprehensive list of risk
factors because of the way the interview guide was set up. In the interview guide the list of
risks from the literature is presented which could offer the interviewee cognitions; a form of
directive questioning (Emans, 2002). In consultation with the supervisors of this thesis the
choice was made to accept this potential directive effect. The goal of the interviews was to
make the list of risks as comprehensive as possible. The idea was that if more risk factors
were mentioned the list of risk factors would become more comprehensive. In future research
this form of directive questioning should be avoided. Instead of offering interviewees
cognitions by giving examples of risk factors the interviewer should let the interviewees come
up with the risk factors themselves. In that way the interviewees will only mention the risk
factors that are relevant to them. Based on the answers of the interviewees a list of risk factors
could be made after which this synthesized list could be used to find the importance of the
risk factors.
The method of analysis to find the importance of the risk factors could also be
improved. Because of the small sample size a more suitable method would have been the
AHP method developed by Saaty (1990). Using this method the importance of the risk factors
can be found through pair-wise comparison. This method would have resulted in a better
estimation of the importance of the risk factors because the interviewees would be asked
about the relative importance of the risk factors. The AHP method cannot be applied to 75

Risk in Healthcare Real Estate Investment 105
risk factors because the number of questions to be able to pair-wise compare would exceed
the limits of any study. The results of this study can, however, be used in further studies by
selecting a small number of risk factors and use these risk factors to apply the AHP method.
In that way more accurate results with regard to the importance can be found. Selecting the
right risk factors can be based on the mean importance of the risk factors (e.g. selecting only
the 10 most important risk factors) or based on own insight.
This study can also be used as a reference for further studies on risk in HCRE. The risk
factors in this study could be quantified using a rating system and quantitative data.
Quantifying the risk factors allows researchers to construct a model to estimate risk at
property level. When these risk estimates would be plotted against return requirements of
investor the relation between risk and return in HCRE can be approximated and a
hypothesized risk-return pattern can appear.
Furthermore, the numerous risk factors found in this study could be the subject of
future studies on the individual risks. Further research could go into questions such as: What
is the ideal rent level an investor should ask? And what is the chance that an investor can find
another tenant at the same or higher rent level? What is technically and functionally 'good'
intramural HCRE? Further research could go into how senior housing facilities can contribute
to the quality of life of elderly in surrounding neighborhoods and how this can affect the value
and attractiveness of a senior housing facility.
6.4. Discussion
The study has a couple of limitations. The study does not offer statistical significant results
with regard to the importance of the risk factors. The Likert-scale that was used for this study
is symmetric while response was asymmetric. Furthermore, pair-wise comparison to find the
relative importance of the risk factors was not possible because of the large number of risk
factors.
Another limitation is that in this study a distinct difference was made between
intramural HCRE and other types of HCRE. In reality intramural HCRE is often combined
with extramural HCRE in one property. Further investigation should go into the multi-
functionality of some HCRE properties and the risk of multiple functions.
Furthermore, this study has been solely from the perspective of investors. Healthcare
organizations are left out in this study intentionally to limit the scope. However, healthcare
organizations are equally important in finding a match between demand and supply on the

Risk in Healthcare Real Estate Investment 106
HCRE asset market. In follow-up studies the findings of this study can be used to inform
healthcare organizations on the perspective of investors to familiarize healthcare
organizations with the views of investors on the risks of HCRE investment.
Despite these limitations this study has expanded the knowledge on risk in HCRE.
This study is the first qualitative study on Dutch HCRE focusing solely on the risks. It offers
investors a new knowledge they can implement directly in their decision process and gives
insight into the different investment perspectives among investors.

Risk in Healthcare Real Estate Investment 107
Reference List
Aedifica. (2015). Evolutie van de portefeuille. Retrieved from aedifica.be:
http://www.aedifica.be/nl/evolutie-van-de-portefeuille
Alzheimer Nederland. (2014). Hoeveel mensen lijden aan dementie? Amersfoort: Alzheimer
Nederland.
Ambrose, B.W., & Nourse, H.O. (1993). Factors influencing capitalization rates. Journal of
Real Estate Research, (8)2 , 221-237.
Berden, S., & Van de Velde, W. (2015). Beleggingen Cofinimmo in zorgvastgoed
uitgebouwd. In E. De Klerk, D. Kootstra, S. Roest, A. Tjeerdsma, & C. Worms, Barometer
Zorgvastgoed (pp. 127-132). Assen: Koninklijke Van Gorcum.
Buffing, S., Achterveld, W., & Conijn, J. (2015). Handboek modelmatig waarderen
marktwaarde in verhuurde staat. Rotterdam: Ortec Finance.
Chaney, A., & Hoesli, M. (2012). Transaction-based and appraisal-based capitalization rate
determinants. Swiss Finance Institute Research Paper, 12-28.
Chin, W., Dent, P., & Roberts, C. (2006). An Exploratory Analysis of Barriers to Investment
and Market Maturity in Southeast Asian Cities. Journal of Real Estate Portfolio Management,
12(1), 49-57.
Chong, J., Jin, Y., & Phillips, G.M. (2013). The Entrepreneur’s Cost of Capital: Incorporating
Downside Risk in the Buildup Method. MacroRisk Analytics Working Paper Series, 1-16.
Dale, D., Wolf, R., & Yang, H.F. (2015). An assessment of the risk and return of residential
real estate. Managerial Finance, 41(6), 591 - 599.
Dantuma, E., & Winkel, E. (2015). Update Gezondheidszorg: Bezuinigingen temperen groei
en vertrouwen. Amsterdam: ING Economisch Bureau.
D'Argensio, J.J., & Laurin, F. (2009). The real estate risk premium: A developed/emerging
country panel data analysis. Journal of Portfolio Management, 35(5), 118.
Risk in Healthcare Real Estate Investment 108
De Baaij, J. (2014). Stijgende lijn in financiële stabiliteit zorginstellingen. In J. Veuger, E. De
Klerk, A. Tjeerdsma, & S. Roest, Barometer Maatschappelijk Vastgoed (pp. 207-215). Assen:
Koninklijke Van Gorcum.
De Baaij, J. (2015). Zorgvastgoed internationaal volwassen beleggingsmarkt. In E. De Klerk,
D. Kootstra, S. Roest, A. Tjeerdsma, & C. Worms, Barometer Zorgvastgoed (pp. 133-138).
Assen: Koninklijke Van Gorcum.
Dokko, Y., Edelstein, R.H., Pomer, M., & Urdang, E.S. (1991). Determinants of the rate of
return for non-residential real estate: inflation expectations and market adjustment lags.
AREUEA Journal, (19)1, 52-69.
DTZ Zadelhoff. (2014). De opmars van zorgvastgoed. Amsterdam: DTZ Zadelhoff.
Emans, B. (2002). Interviewen: theorie, techniek en training. Groningen: Wolters-Noordhoff.
Estrada, J. (2002). Systematic Risk in Emerging Markets: The D-CAPM. Emerging Markets
Review, 3(4). 365-379. Cited in Mamoghli, C., & Daboussi, S. (2010). Capital Asset Pricing
Models and Performance Measures in the Downside Risk Framework. Journal of Emerging
Market Finance, 9(2), 95-130.
Estrada, J. (2007). Mean-semivariance behavior: Downside risk and capital asset pricing.
International Review of Economics and Finance 16, 169 – 185.
Froland, C. (1987). What determines cap rates on real estate. Journal of Portfolio
Management, 13, 77-83.
Geltner, D.N., & Miller, N.G. (2001). Commercial Real Estate Analysis and Investments.
Mason, OH: South-Western Publishing.
Gunnelin, A., Hendershott, P., Hoesli, M., & Söderberg, B. (2004). Determinants of Cross-
Sectional Variation in Discount Rates, Growth Rates and Exit Cap Rates, Real Estate
Economics, 32(2), 217–237. Cited in Chaney, A., & Hoesli, M. (2012). Transaction-based and
appraisal-based capitalization rate determinants. Swiss Finance Institute Research Paper, 12-
28.
Risk in Healthcare Real Estate Investment 109
Hendershott, P.H, & Turner, B. (1999). Estimating constant-quality capitalization rates and
capitalization effects of below market financing. Journal of Property Research, 16(2), 109-
122.
Hermus, J. (2015). Een vergelijking met de Engelse zorgvastgoedmarkt. In E. De Klerk, D.
Kootstra, S. Roest, A. Tjeerdsma, & C. Worms, Barometer Zorgvastgoed (pp. 71-75). Assen:
Koninklijke Van Gorcum.
Hermus, J., & Veuger, J. (2015) Waardering zorgvastgoed. In E. De Klerk, D. Kootstra, S.
Roest, A. Tjeerdsma, & C. Worms, Barometer Zorgvastgoed (pp. 79-99). Assen: Koninklijke
Van Gorcum.
Hermus, J. (2014). Zorgvastgoed biedt kansen voor zorginstellingen én marktpartijen. In J.
Veuger, E. De Klerk, A. Tjeerdsma, & S. Roest, Barometer Maatschappelijk Vastgoed (pp.
229-233). Assen: Koninklijke Van Gorcum.
Ho, D.K.H., & Addae-Dapaah, K. (2015). International Direct Real Estate Risk Premiums in a
Multi-Factor Estimation Model. Journal of Real Estate Financial Economics, 52–85.
Hull, J.C. (2012). Risk Management and Financial Institutions. Hoboken, NJ: John Wiley &
Sons.
Keogh, G., & D'Arcy, É. (1994). Market maturity and property market behaviour: a European
comparison of mature and emergent markets. Journal of Property Research, 11(3), 215-235.
Ling, D.C., & Naranjo, A. (1997). Economic Risk Factors and Commercial Real Estate
Returns. Journal of Real Estate Finance and Economics, 15(3), 283-307.
Lintner, J. (1965). The valuation of risk assets and the selection of risky investments in stock
portfolios and capital budgets. The review of economics and statistics, 13-37.
Lusht, K.M. (2001). Real estate valuation: principles and applications. State College, PA:
KML Publishing.
Netzell, O. (2009). A Study of Micro-Level Variation in Appraisal-Based Capitalisation
Rates, Journal of Property Research, 26(3), 235–263. Cited in Chaney, A., & Hoesli, M.
(2012). Transaction-based and appraisal-based capitalization rate determinants. Swiss Finance
Institute Research Paper, 12-28.
Risk in Healthcare Real Estate Investment 110
Mamoghli, C., & Daboussi, S. (2010). Capital Asset Pricing Models and Performance
Measures in the Downside Risk Framework. Journal of Emerging Market Finance, 9(2), 95-
130.
Markowitz, H. (1952). Portfolio Selection. Journal of Finance, 7, 77-91.
McDonald, J.F., & & Dermisi, S. (2009). Office building capitalization rates: the case of
downtown Chicago. The Journal of Real Estate Finance and Economics, 39(4), 472-485.
Ministerie van VWS. (2014). Hervorming langdurige zorg: naar goede zorg die bij ons past.
Den Haag: Ministerie van Volksgezondheid, Welzijn en Sport.
Nederlandse Zorgautoriteit. (2011). Invoering normatieve huisvestingscomponent (NHC)
bestaande zorgaanbieders. Utrecht: Nederlandse Zorgautoriteit.
Nederlandse Zorgautoriteit. (2009). Naar integrale tarieven in de AWBZ. Utrecht:
Nederlandse Zorgautoriteit.
Olde Bijvank, E., & Van Oostveen, R. (2015). Steeds strategischer omgang met zorgvastgoed.
In E. De Klerk, D. Kootstra, S. Roest, A. Tjeerdsma, & C. Worms, Barometer Zorgvastgoed
(pp. 33-39). Assen: Koninklijke Van Gorcum.
Pai, A., & Geltner, D.N. (2007). Stocks Are from mars, real estate is from venus—the cross-
section of long-run investment performance. Journal of Portfolio Management, 33(5), 134–
144. Cited in Ho, D.K.H., & Addae-Dapaah, K. (2015). International Direct Real Estate Risk
Premiums in a Multi-Factor Estimation Model. Journal of Real Estate Financial Economics,
52–85.
Pavlov, A., Steiner, E., & Wachter, S. (2015). Macroeconomic risk factors and the role of
mispriced credit in the returns from international real estate securities. Real Estate Economics,
43(1), 241-270.
Postema, D.J. (2015). Financierbaarheid van zorgvastgoed. In E. De Klerk, D. Kootstra, S.
Roest, A. Tjeerdsma, & C. Worms, Barometer Zorgvastgoed (pp. 119-125). Assen:
Koninklijke Van Gorcum.

Risk in Healthcare Real Estate Investment 111
Regeling langdurige zorg. (2015, August 25). Bijlage A. bij artikel 2.1 van de Regeling
langdurige zorg. Retrieved August 25, 2015, from wetten.overheid.nl:
http://wetten.overheid.nl/BWBR0036014/BijlageA/geldigheidsdatum_25-08-2015
Rosen, S. (1974). Hedonic Prices and Implicit Markets: Product Differentiationin Pure
Competition. Journal of Political Economy, 82(1), 34-55.
Ross, S. (1976). The Arbitrage Theory of Capital Asset Pricing. Journal of Economic Theory,
13, 341-360.
Roy, A.D. (1952). Safety first and the holding of assets. Econometrica 20(3), pp. 431-449.
Cited in Chong, J., Jin, Y., & Phillips, G.M. (2013) Incorporating Downside Risk in the
Buildup Method. MacroRisk Analytics Working Paper Series, 1-16.
Saaty, T.L. (1990). How to make a decision: The Analytical Hierarchy Process. European
Journal of Operational Research, 48, 9-26.
Saderion, Z., Smith, B., & Smith, C. (1994). An integrated approach to the evaluation of
commercial real estate. Journal of Real Estate Research, 9(2), 151-167.
Scheijgrond, E., Anker, G., & Besier, G. (2015). Stilte voor de storm met zorgvastgoed: Alle
hens aan dek! In E. De Klerk, D. Kootstra, S. Roest, A. Tjeerdsma, & C. Worms, Barometer
Zorgvastgoed (pp. 139-145). Assen: Koninklijke Van Gorcum.
Schellens, W., & De Bruijn, J. (2014, September 11). Zorgvastgoed wordt volwassen
beleggingscategorie. Retrieved September 9, 2015, from DTZ.nl: https://www.dtz.nl/nl/over-
dtz-zadelhoff/nieuws-en-agenda/overzicht-nieuwsberichten/2014/q3-2014/nieuwsberichten-
uit-het-derde-kwartaal-van-2014/zorgvastgoed-wordt-volwassen-
beleggingscategorie/?page=2
Sharpe, W. (1964). Capital Asset Prices: A Theory of Market Equilibrium Under Conditions
of Risk. Journal of Finance, 19, 425-442.
Sivitanides, P., Southard, J., Torto, R.G., & Wheaton, W.C. (2001). The Determinants of
Appraisal-Based Capitalization Rates. Boston, MA: Torto Wheaton Research.
Sivitanidou, R.C., & Sivitanides, P.S. (1999). Office Capitalization Rates: Real Estate and
Capital Market Influences. Journal of Real Estate Finance and Economics, (18)3, 297-322.
Risk in Healthcare Real Estate Investment 112
Swisher, P., & Kasten, G.W. (2005). Post-modern portfolio theory. Journal of Financial
Planning, 18(9), 74-85.
Vagias, W.M. (2006). Likert-type scale response anchors. Clemson, SC: Clemson University.
Van der Gijp, B. (2014). Investeren in zorgvastgoed: relatief onbekende assetclass. In J.
Veuger, E. De Klerk, A. Tjeerdsma, & S. Roest, Barometer Maatschappelijk Vastgoed (pp.
195-206). Assen: Koninklijke Van Gorcum.
Van der Schaar, J. (2002). Zorgvernieuwing Vast Goed: over facilitair vastgoedbeheer en
zorg. Den Haag: Ministerie van Volksgezondheid, Welzijn en Sport.
Van der Wielen, S. (2014). Alternatieve financieringsvormen voor zorgvastgoed
[afstudeerscriptie]. Amsterdam: Amsterdam School of Real Estate.
Van Elp, M., & Konings, P. (2015). Beleggen in zorgvastgoed. Amsterdam: Economisch
Instituut voor de Bouw (EIB).
Van Ewijk, C., Van der Horst, A., & Besseling, P. (2013). Gezondheid loont: tussen keuze en
solidariteit. Den Haag: Centraal Planbureau.
Van Galen, J., Willems, J., & Poulus, C. (2012). Monitor Investeren voor de Toekomst. Delft:
ABF Research.
Van Schie, M. (2014). Zorgvastgoed als volwaardige beleggingscategorie. In J. Veuger, E. De
Klerk, A. Tjeerdsma, & S. Roest, Barometer Maatschappelijk Vastgoed (pp. 235-238). Assen:
Koninklijke Van Gorcum.
Wheaton, W.C., Torto, R.G., Sivitanides, P.S., Southard, J.A., Hopkins, R.E., & Costello,
J.M. (2001). Real estate risk: a forward-looking approach. Real Estate Finance, 18(3), 20-28.
Risk in Healthcare Real Estate Investment 113
List of Abbreviations
AHP: Analytical Hierarchy Process
CAPM: Capital Asset Pricing Model
CBD: Central Business District
GDP: Gross Domestic Product
HCRE: Healthcare Real Estate
HRM: Hedonic Risk Model
IRR: Internal Rate of Return
MPT: Modern Portfolio Theory
REIT: Real Estate Investment Trust
Risk in Healthcare Real Estate Investment 114
List of Figures
Figure 1.1. The different categories of HCRE. Source: Van der Gijp (2014), edited by
author. Page 4.
Figure 1.2. Development of demand for intramural elderly HCRE. The number of
people with high levels of required care, categorized by type of required care. Source: Van
Galen, Willems, & Poulus (2012), edited by author. Page 5.
Figure 1.3. Research design. The consecutive proceedings taken in this study,
consisting of two parts: a descriptive and an explorative part. Page 6.
Figure 2.1. The real estate system (simplified). The interaction of the space market, the
asset market and the development industry. Source: Geltner & Miller (2001), edited by
author. Page 9.
Figure 2.2. The development of the portfolio of the Belgian HCRE investor Aedifica.
The volume of investment by property type, in million euro. Source: Aedifica (2015), edited
by author. Page 11.
Figure 2.3. Simplified visualization of the cash flow of an investment in a property.
Page 15.
Figure 3.1. Security Market Line. This figure shows that as the risk of an asset
( ) goes up, the risk premium ( ) of that asset goes up proportionately and is added to
the risk free rate ( ). Page 19.
Figure 3.2. The HRM: Hedonic Risk Model. The risk of investing in real estate can be
broken down into several risk factors based on the notion of the hedonic hypothesis. The risk
can be divided into three levels of risk: real estate general risks, property type specific risks
and property specific risks. Page 21.
Figure 3.3. Importance of variables for investors vs. appraisers. Source: Chaney &
Hoesli (2012), edited by author. Page 26.
Figure 3.4. The oversight of all risk factors mentioned in the literature review and their
sources. Page 30.
Figure 3.5: Risk in HCRE Investment. In HCRE investment not only property risks are
taken into account but also tenant risks. Page 33.
Figure 4.1. The iterative process of interviewing and updating the list of risk factors.
Page 43.
Figure 5.1. The main risk factors, their mean importance and standard deviation in a
chart. Page 68.
Risk in Healthcare Real Estate Investment 115
Figure 5.2. The risk factors related to the maturity of the asset market, their mean
importance and standard deviation in a chart. Page 70.
Figure 5.3. The risk factors related to the technical and functional state, their mean
importance and standard deviation in a chart. Page 73.
Figure 5.4. The risk factors related to the location, their mean importance and standard
deviation in a chart. Page 75.
Figure 5.5. The risk factors related to the location, their mean importance and standard
deviation in a chart. Page 77.
Figure 5.6. The risk factors related to the alternative use, their mean importance and
standard deviation in a chart. Page 79.
Figure 5.7. The risk factors related to the alternative use, their mean importance and
standard deviation in a chart. Page 82.
Figure 5.8. The risk factors related to the creditworthiness, their mean importance and
standard deviation in a chart. Page 84.
Figure 5.9. The risk factors related to the quality of the management, their mean
importance and standard deviation in a chart. Page 86.
Figure 5.10. The risk factors related to the vision, their mean importance and standard
deviation in a chart. Page 88.
Figure 5.11. The risk factors related to the vision, their mean importance and standard
deviation in a chart. Page 90.
Risk in Healthcare Real Estate Investment 116
List of Tables
Table 2.1. The advantages and disadvantages of investing in HCRE. Source: Hermus
(2014) and Berden & Van de Velde (2015), edited by author. Page 13.
Table 3.1. Return, standard deviation, and Sharpe ratios for different kinds of Dutch
real estate, and the correlation of care HCRE with the different kinds of real estate. Source:
Van Elp & Konings (2015), edited by author. Page 27.
Table 3.2. The risk factors that were removed from the synthesized risk list and the
reason they were deemed irrelevant. Page 32.
Table 3.3. On the left the risks from the literature related to maturity of the market and
on the right the synthesized list of risk related to the maturity of the market. Page 34.
Table 3.4. On the left the risks from the literature related to the investment volume of
the property and on the right the synthesized list of risk related to marketability. Page 34.
Table 3.5. On the left the risks from the literature related to the technical state of the
property and on the right the synthesized list of risk related to the technical state of the
property. Page 35.
Table 3.6. On the left the risks from the literature related to the functional suitability of
the property and on the right the synthesized list of risk related to the functional suitability of
the property. Page 36.
Table 3.7. On the left the risks from the literature related to the location and on the
right the synthesized list of risk related to location. Page 36.
Table 3.8. On the left the risks from the literature related to space markets and on the
right the synthesized list of risk related to space market. Page 37.
Table 3.9. On the left the risks from the literature related to the reliability of the tenant
and on the right the synthesized list of risk related to reliability of the tenant. Page 38.
Table 3.10. List of risk factors following the synthesis of the risks in the literature.
Page 39.
Table 4.1. Interviewee selection. The characteristics of the interviewees in this study.
Page 45.
Table 5.1. List of risk factors obtained through literature research and interviews. Risk
factors marked grey are risk factor that apply to the entire HCRE market. Other risk factors
are property related. Page 49.
Table 5.2. Comparison of the risk factors in the literature list and the final list;
maturity of the asset market. Page 53.

Risk in Healthcare Real Estate Investment 117
Table 5.3. Comparison of the risk factors in the literature list and the final list;
technical and functional state of the property. Page 54.
Table 5.4. Comparison of the risk factors in the literature list and the final list;
location. Page 55.
Table 5.5. Comparison of the risk factors in the literature list and the final list; (local)
space market. Page 57.
Table 5.6. Comparison of the risk factors in the literature list and the final list;
alternative use. Page 58.
Table 5.7. Comparison of the risk factors in the literature list and the final list;
coverage ratio. Page 59.
Table 5.8. Comparison of the risk factors in the literature list and the final list;
influence of government policy changes on the tenant. Page 60.
Table 5.9. Comparison of the risk factors in the literature list and the final list;
creditworthiness of the tenant. Page 61.
Table 5.10. Comparison of the risk factors in the literature list and the final list; quality
of the management of the tenant. Page 62.
Table 5.11. Comparison of the risk factors in the literature list and the final list; vision
of the tenant. Page 64.
Table 5.12. Comparison of the risk factors in the literature list and the final list;
competition by other healthcare organizations. Page 65.
Table 5.13. Comparison of the risk factors in the literature list and the final list; type of
contract. Page 65.
Table 5.14. The ratings of the main risk factors for all interviewees and the mode,
mean and sample size. Wherever a box in this table is empty no rating was registered. Page
67.
Table 5.15. Descriptive statistics of the risk factors related to the maturity of the asset
market. Page 69.
Table 5.16. Descriptive statistics of the risk factors related to the technical and
functional state of the property. Page 71.
Table 5.17. Descriptive statistics of the risk factors related to the location. Page 74.
Table 5.18. Descriptive statistics of the risk factors related to the local space market.
Page 76.
Table 5.19. Descriptive statistics of the risk factors related to the alternative use. Page
78.
Risk in Healthcare Real Estate Investment 118
Table 5.20. Descriptive statistics of the risk factor coverage ratio. Page 80.
Table 5.21. Descriptive statistics of the risk factors related to the influence of the
government on the tenant. Page 81.
Table 5.22. Descriptive statistics of the risk factors related to the creditworthiness of
the tenant. Page 83.
Table 5.23. Descriptive statistics of the risk factors related to the quality of the
management of the tenant. Page 85.
Table 5.24. Descriptive statistics of the risk factors related to the vision of the tenant.
Page 87.
Table 5.25. Descriptive statistics of the risk factors related to the competition by other
healthcare organizations. Page 89.
Table 5.26. Descriptive statistics of the risk factor type of contract. Page 90.
Table 5.27. Descriptive statistics of the 10 risk factors with the highest and lowest
mean. Page 91.
Table 5.28. Descriptive statistics of the 10 risk factors with the lowest and the highest
standard deviation. Page 93.
Table 5.29. Descriptive statistics of the main risk factors for all four different groups.
Page 95.
Table 5.30. The importance of property risks versus tenant risk at three different
lengths of the contract. Page 99.
Table 6.1. Recommendation on how to reduce risk through managing the risk factors.
Page 103.

Risk in Healthcare Real Estate Investment 119
List of Equations
Equation 1: . Page 20.

Risk in Healthcare Real Estate Investment: Appendices 1
Appendix 1: Oversight of Risk Factors from the Literature Review
Risk Factors
Rea
l Est
ate
Gen
era
l Ris
ks
Pro
per
ty C
lass
Sp
ecif
ic R
isks
Pro
per
ty S
pec
ific
Ris
ks
Van
Elp
& K
on
ings
(2
01
5)
Van
der
Gijp
(2
01
4)
Van
Baa
ij (2
01
4, 2
01
5)
Ber
den
& V
an d
e V
eld
e (2
01
5)
Dal
e et
al.
(20
15
)
Pav
lov
et a
l. (2
01
5)
Ho
& A
dd
ae-D
apaa
h (
20
15
)
Fro
lan
d (
19
87
)
Do
kko
et
al. (
19
91
) an
d A
mb
rose
& N
ou
rse
(19
93
)
Sivi
tan
ido
u &
Siv
itan
ides
(1
99
9)
Wh
eato
n e
t al
. (2
00
1)
Sivi
tan
idas
et
al. (
20
01
)
D'A
rgen
sio
& L
auri
n (
20
09
)
Sald
erio
n e
t al
. (1
99
4)
McD
on
ald
& D
erm
isi (
20
09
)
Hen
der
sho
tt &
Tu
rner
(1
99
9)
Net
zell
(20
09
) an
d H
end
ersh
ott
et
al. (
20
04
)
Ch
aney
& H
oes
li (2
01
2)
Risks associated with HCRE
Market size and liquidity ✓
Political risk ✓ ✓ ✓
Creditworthiness of the tenant ✓ ✓ ✓ ✓
Vacancy and exit value risk ✓
Marketability of real estate ✓ ✓
Space market risk ✓
Asset market risk ✓
Management and vision of tenant ✓
Risks associated with real estate
Liquidity risk ✓
Leverage risk ✓
(Global) stock market ✓ ✓ ✓
Foreign exchange rate ✓
Inflation ✓ ✓ ✓
Country governance & law system ✓ ✓ ✓
Bond market ✓ ✓
GDP ✓ ✓ ✓
Supply of new RE space ✓
Prime lending rate ✓
Vacancy rate ✓ ✓ ✓ ✓ ✓
Consumption ✓
Macro and micro location ✓ ✓ ✓ ✓ ✓
Size of the property ✓ ✓ ✓
Real estate class ✓ ✓
Mortgage contract rate ✓
(Spread between) T-bills and risk free rate ✓ ✓ ✓ ✓
Corporate earnings-to-price ratio ✓
Concentration of offices in a CBD ✓
Diversity of tenant types ✓
Government vs. commercial tenants ✓
Level of absorption of space ✓
Uncertainty in forecasting cap rates ✓
Real rent divided by average rent ✓ ✓ ✓ ✓ ✓
Change in rent levels ✓ ✓
'Depth' of the market ✓
'Density' of the market ✓
Existence of REITs ✓
Age of property/ new ✓ ✓ ✓ ✓
Low borrowing rate ✓ ✓
Class A buildings ✓
Renovated or not ✓ ✓
Employment in tenant sector ✓
Residential vs. commercial use ✓ ✓
'Density' of the plot ✓ ✓
Land lease ✓
Condition of the property ✓
Construction quality ✓
Volume of investment ✓
Risk in Healthcare Real Estate Investment: Appendices 2
Appendix 2: Interview guide for Interviews with Experts
The interview guide is based on Emans (2002) and was translated to Dutch for the interviews.
To increase the objectivity in interviews standardization can help to reduce the influence of
non-controlled situations. Emans therefore advises to use a standardized interview guide to
increase the predictability of the interview. By standardization all unwanted influences are
reduced to a minimum such as the presence of third parties and the influence of the age, sex
and status of the interviewee. To achieve standardization the interviewer needs to control for
situational influences, evaluate the informants' answers on correctness and completeness and
avoid to give own interpretations to the answers of the informants. The interview guide in this
study is structured, meaning it follows a sequence of questions, and makes use of both open
and closed questions. In some cases the answers in the open questions will be field-coded
when e.g. the risk factors mentioned by the interviewee strongly resemble risk factors already
mentioned earlier. Another form of a situational influence that can be avoided using
standardization is the influence of the interviewer on the conversation. To minimize this effect
the questions were set up in such a way to have a neutral attitude towards the subjects to
facilitate the interviewee with maximum space for personal expression. To further standardize
the interviews efforts were made to make sure there are as little deviations as possible with
regard to the presence of third parties. All interviewees were made anonymous, recorded and
will be in person with the author of this thesis.
The interview guide in this study incorporate the idea by Emans that the interviewer
has several (consecutive and iterative) tasks: to introduce the interview; to ask questions; to
evaluate the questions on usefulness; to ask for further explanations if necessary and; to note
the answers. The interviewee needs to be aware when asking a question that the questions
themselves do not direct the interviewee in a certain direction. Emans shows nine possible
forms of directing questions and how to avoid them. The questions in the interview guide
were corrected to minimize directive questioning e.g. by avoiding mentioning the sources on
which the interviewees comment; by avoiding giving examples of responses and by avoiding
offering cognitions as far as possible.
After the interviewee gives an answer the interviewer needs to evaluate the answer on
validity, comprehensiveness, relevance and clarity. To increase the validity of the answers
special attention was paid in the interview guide to avoid socially desirable answers and to
avoid e.g. that interviewees will try to come up with more risk factors than they initially
Risk in Healthcare Real Estate Investment: Appendices 3
thought of; not because they forgot some of the risk factors but simply to be friendly towards
the interviewer.
Some of the questions in the interview guide were inevitably directing the interviewee.
In the interview guide the list of risks from the literature is presented which could offer the
interviewee cognitions; a form of directive questioning. In consultation with the supervisors
of this thesis the choice was made to accept this potential directive effect. The goal of the
interviews is to make the list of risks as comprehensive as possible. If more risk factors are
mentioned by the interviewees the list of risks should become more comprehensive. By
showing the list of risks during the interview the interviewee should be able to recognize and
remember some of the risks he perhaps initially did not think of.
In order to set up the questions first the specific need for information was identified by
making a list of the variables, as advised by Emans (2002). The list of variables represent the
specified need for information obtain through the interviews. There are three different groups
of experts that are part of the interviews; consultants with a focus on HCRE, HCRE investors
and housing associations who invest in HCRE. The difference between a housing association
and an investor is that housing associations are non-profit and are under strict government
regulation. Although housing associations are non-profit, they effectively operate the same as
any other real estate investor when they invest in HCRE. The only difference is that they
sometimes require a lower return because they reduce the total expected return to include a
discount. This discount is the 'social return' that housing association give to society in order to
fulfill their social obligations. The list of variables is seen in table 1.
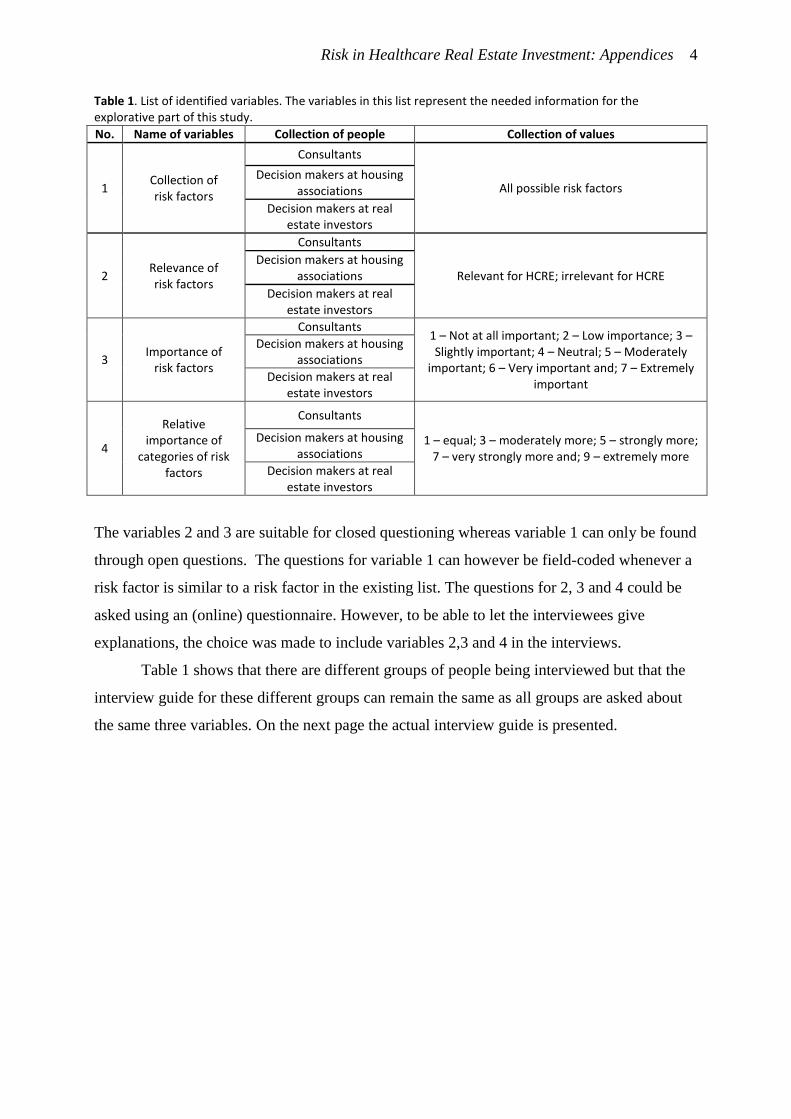
Risk in Healthcare Real Estate Investment: Appendices 4
Table 1. List of identified variables. The variables in this list represent the needed information for the explorative part of this study.
No. Name of variables Collection of people Collection of values
1 Collection of risk factors
Consultants
All possible risk factors Decision makers at housing
associations
Decision makers at real estate investors
2 Relevance of risk factors
Consultants
Relevant for HCRE; irrelevant for HCRE Decision makers at housing
associations
Decision makers at real estate investors
3 Importance of
risk factors
Consultants 1 – Not at all important; 2 – Low importance; 3 – Slightly important; 4 – Neutral; 5 – Moderately
important; 6 – Very important and; 7 – Extremely important
Decision makers at housing associations
Decision makers at real estate investors
4
Relative importance of
categories of risk factors
Consultants
1 – equal; 3 – moderately more; 5 – strongly more; 7 – very strongly more and; 9 – extremely more
Decision makers at housing associations
Decision makers at real estate investors
The variables 2 and 3 are suitable for closed questioning whereas variable 1 can only be found
through open questions. The questions for variable 1 can however be field-coded whenever a
risk factor is similar to a risk factor in the existing list. The questions for 2, 3 and 4 could be
asked using an (online) questionnaire. However, to be able to let the interviewees give
explanations, the choice was made to include variables 2,3 and 4 in the interviews.
Table 1 shows that there are different groups of people being interviewed but that the
interview guide for these different groups can remain the same as all groups are asked about
the same three variables. On the next page the actual interview guide is presented.
Risk in Healthcare Real Estate Investment: Appendices 5
Eindhoven University of Technology 2015
Expert-Interviews on the Risk Factors of HCRE Investment Page 1
Information on the interview guide
1. Follow the order of the questions strictly.
2. Questions that have been marked italic have to be read literally.
3. Check if the recording device is working.
4. Fill in the technical variables as far as possible before the interview.
5. Introduce yourself first and then continue with the information on the interview.
Information on the interview
I want to start mentioning the goal of this interview. This interview is part of my master
graduation research project at Eindhoven University of Technology to investigate the risks in
healthcare real estate investment. I'm conducting this research during my internship at
Finance Ideas. This interview is anonymous and will be recorded if you agree. The record will
only be available for the teachers at my university on request.
This interview is part of a series of interviews with other experts. The reason of
interviewing you is because of your knowledge on real estate investment in healthcare real
estate. These interviews will be used to find all the risks of investing in healthcare real
estate. The questions will thus be about the risks of investing in healthcare real estate.
The specific healthcare real estate in this interview is intramural elderly healthcare
real estate. This is intramural healthcare real estate for the nursing of older people with
severe somatic and psycho-geriatric conditions. All questions will be specifically about
intramural elderly healthcare real estate.
The interview is conducted based on a structured interview guide. There are 3
questions which I will ask in a consecutive order. The only thing you have to do is to answer
these questions as good, accurate and complete as possible. The whole interview will take
up to a maximum of 30 minutes.
Do you have any questions regarding what I just said before we start? [any questions
will be answered briefly and unrelated questions will be answered after the interview]. Then
I would like to first clarify a few thing before I start with the questions.
Risk in Healthcare Real Estate Investment: Appendices 6
Eindhoven University of Technology 2015
Expert-Interviews on the Risk Factors of HCRE Investment Page 2
Explanation of the questions
We assume that risk is determined by the risk-bearing attributes of a property. I've
constructed a Risk Model [show the Handout: Risk Model]. The idea behind this risk model is
that the characteristics of a property determine the level of risk. These characteristics are
the risk factors. There are real estate general risk factors; property class specific risk factors
and; property specific risk factors. The real estate general risk factors are factors that
influence the risk of all types of real estate. These are risk factors such as: the bond market;
GDP; stock market; inflation; etc. I'm only interested in the property class specific risk factors
and property specific risk factors. In office real estate changes in the number of office jobs is
for instance a risk factor that is property class specific, and the location of an office is a risk
factor that property specific. I am interested in the risk factors at property class level and
property level for HCRE. Do you have any question about what I just said? [Answer all
relevant questions. Any irrelevant questions can be answered after the interview.]
Before I started doing these interviews I conducted a literature review on the risk in HCRE
investment. Based on this literature review I've made a list of risk factors [show the
Handout: List of Risk Factors and the figure Relation Risk with Property, Tenant and Market].
This list is divided into marketability of the property and stability of the tenant. The
marketability influences the ability of the property to retain its value and influences the
indirect return. The stability of the tenant influences the security of the cash flows which
form the direct return. These two risk factors are influenced by all sorts of risk factors. These
[point at the list of risk factors] are the risk factors I've managed to obtain from the
literature. First I'm going to ask you to improve this list and after that I'm going to ask you
how important the different risk factors are. Do you have any question about what I just
said? [Answer all relevant questions. Any irrelevant questions can be answered after the
interview.] Then I will now start with the interview; starting with the first question.
(Note the time of the beginning of the interview.)
(Start the recording device.)
Risk in Healthcare Real Estate Investment: Appendices 7
Eindhoven University of Technology 2015
Expert-Interviews on the Risk Factors of HCRE Investment Page 3
Question 1
[Give the A3 format list of risk factors]. Can you explain for each risk factor on this list which
risk factor is relevant or not and which risk factor you would like to add to the list?
(Don't give examples. Try to let the informant mention as many risk factors he can think of.
Write all the risk factors down. Ask again if necessary in order to write down all risk factors.
Make sure to have detailed descriptions of all the risk factors. Don't assist by trying to
explain the risk factors yourself. Evaluate on validity, completeness, relevance and clarity
and if necessary ask further.)
Question 2
Can you explain for each of these risk factors how important they are when investing in
intramural elderly healthcare real estate on a 7-point scale from 1 – Not at all important to 7
– Extremely important [point at 7-point scale]?
(Explain the question if necessary. Make sure to all the risk factors are rated. Don't give
examples. Evaluate on validity, completeness, relevance and clarity and if necessary ask
further.)
Question 3
Can you say which of the two risk factors "marketability of the property" and "reliability of
the tenant" is more important and, if applicable, how much more important [point at answer
form question 3]?
(Explain the question if necessary. Make sure to all the risk factors are rated. Don't give
examples. Evaluate on validity, completeness, relevance and clarity and if necessary ask
further.)
Closing
These were all the questions I have. I want to thank you for your cooperation. Do you have
any questions? Do you want me to send you the results once I finish my research?
(Stop the recorder.)
(Fill in the technical variables.)
(Answer any questions.)

Risk in Healthcare Real Estate Investment: Appendices 8
Eindhoven University of Technology 2015
Expert-Interviews on the Risk Factors of HCRE Investment Appendix A
Technical variables
Case number:
Informant number:
Name of informant:
Date and time:
Duration of the interview:
Place of the interview:
What kind of investor or consultant?
Third parties attending the interview?
Noise and disruptions?
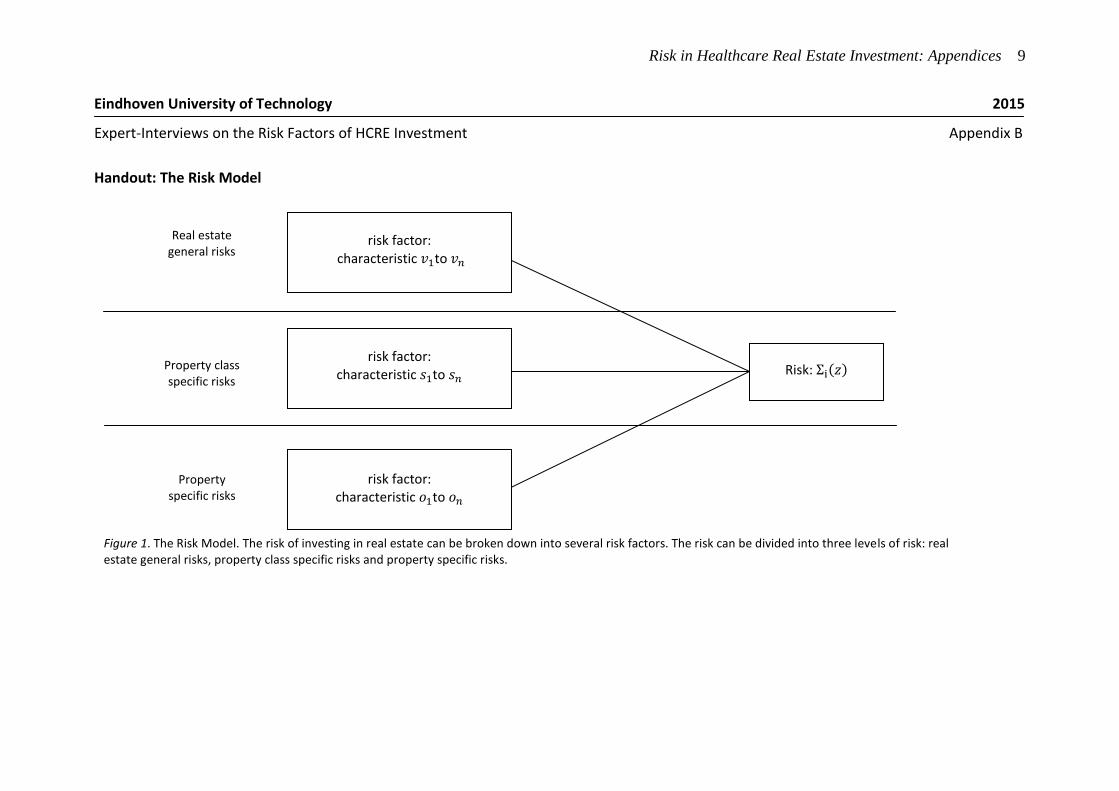
Risk in Healthcare Real Estate Investment: Appendices 9
Figure 1. The Risk Model. The risk of investing in real estate can be broken down into several risk factors. The risk can be divided into three levels of risk: real estate general risks, property class specific risks and property specific risks.
Risk:
Real estate general risks
Property class specific risks
Property
specific risks
risk factor: characteristic to
risk factor: characteristic to
risk factor: characteristic to
Eindhoven University of Technology 2015
Expert-Interviews on the Risk Factors of HCRE Investment Appendix B
Handout: The Risk Model
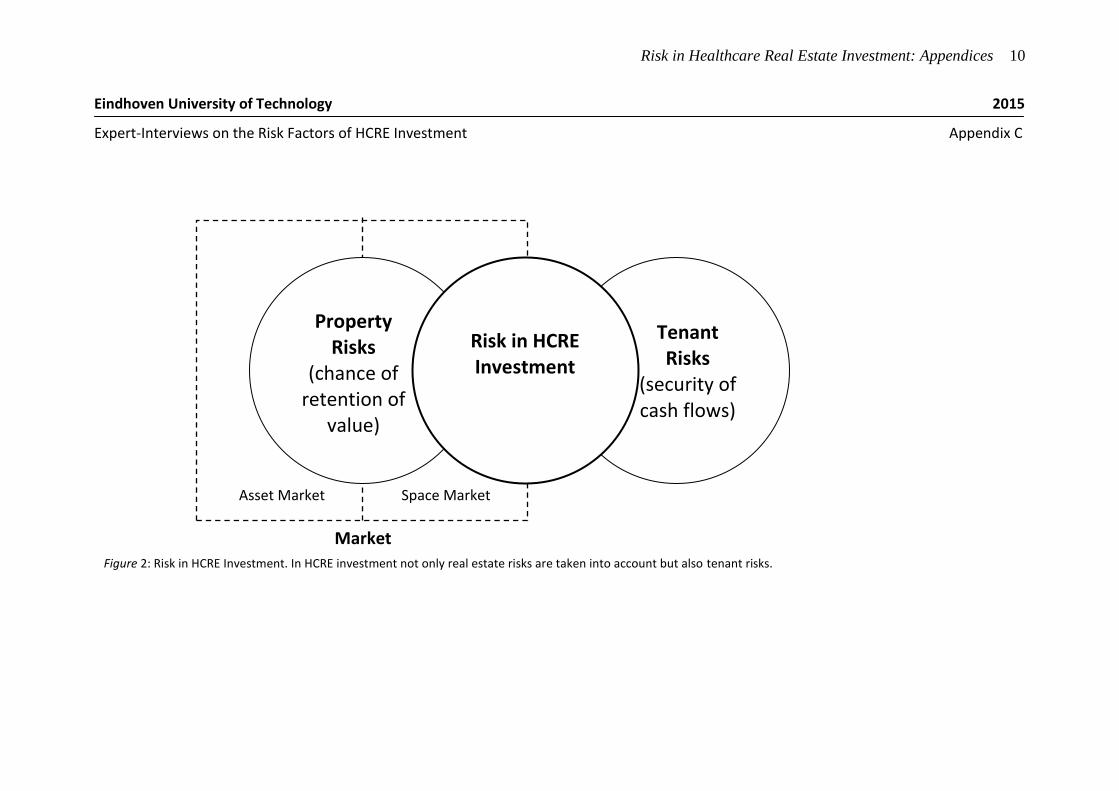
Risk in Healthcare Real Estate Investment: Appendices 10
Eindhoven University of Technology 2015
Expert-Interviews on the Risk Factors of HCRE Investment Appendix C
Market
Asset Market Space Market
Risk in HCRE Investment
Property Risks
(chance of retention of
value)
Tenant Risks
(security of cash flows)
Figure 2: Risk in HCRE Investment. In HCRE investment not only real estate risks are taken into account but also tenant risks.
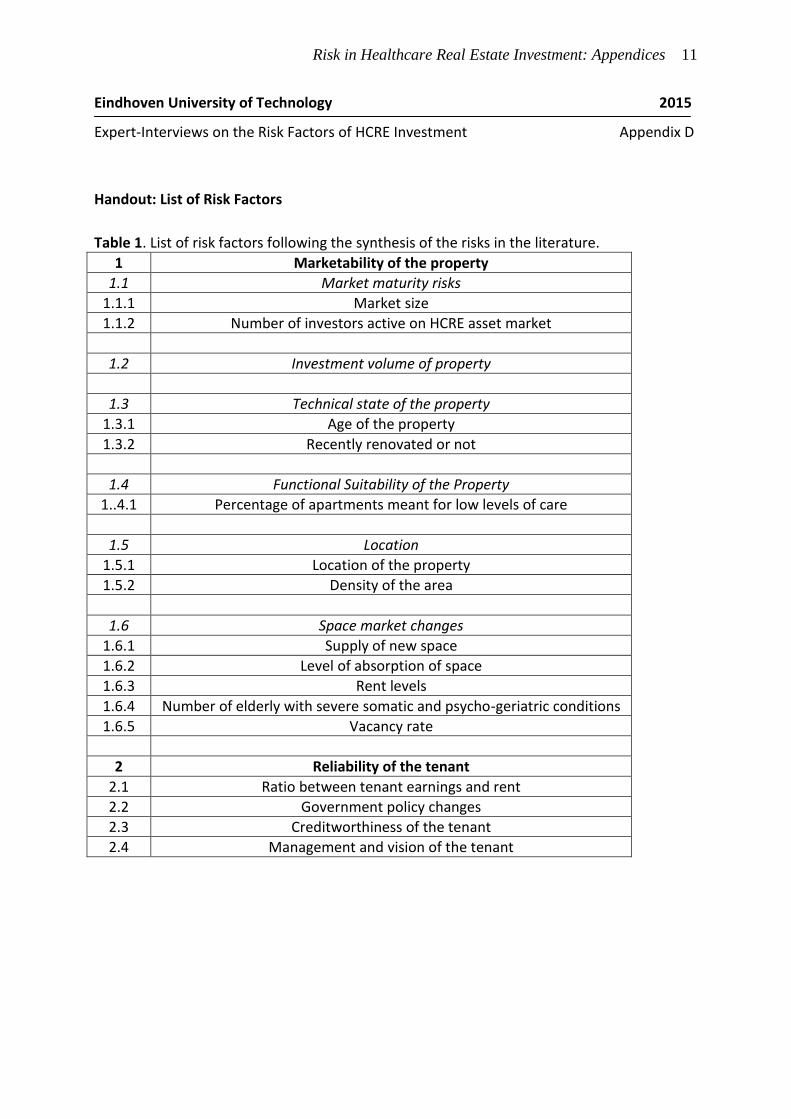
Risk in Healthcare Real Estate Investment: Appendices 11
Eindhoven University of Technology 2015
Expert-Interviews on the Risk Factors of HCRE Investment Appendix D
Handout: List of Risk Factors
Table 1. List of risk factors following the synthesis of the risks in the literature.
1 Marketability of the property
1.1 Market maturity risks
1.1.1 Market size
1.1.2 Number of investors active on HCRE asset market
1.2 Investment volume of property
1.3 Technical state of the property
1.3.1 Age of the property
1.3.2 Recently renovated or not
1.4 Functional Suitability of the Property
1..4.1 Percentage of apartments meant for low levels of care
1.5 Location
1.5.1 Location of the property
1.5.2 Density of the area
1.6 Space market changes
1.6.1 Supply of new space
1.6.2 Level of absorption of space
1.6.3 Rent levels
1.6.4 Number of elderly with severe somatic and psycho-geriatric conditions
1.6.5 Vacancy rate
2 Reliability of the tenant
2.1 Ratio between tenant earnings and rent
2.2 Government policy changes
2.3 Creditworthiness of the tenant
2.4 Management and vision of the tenant
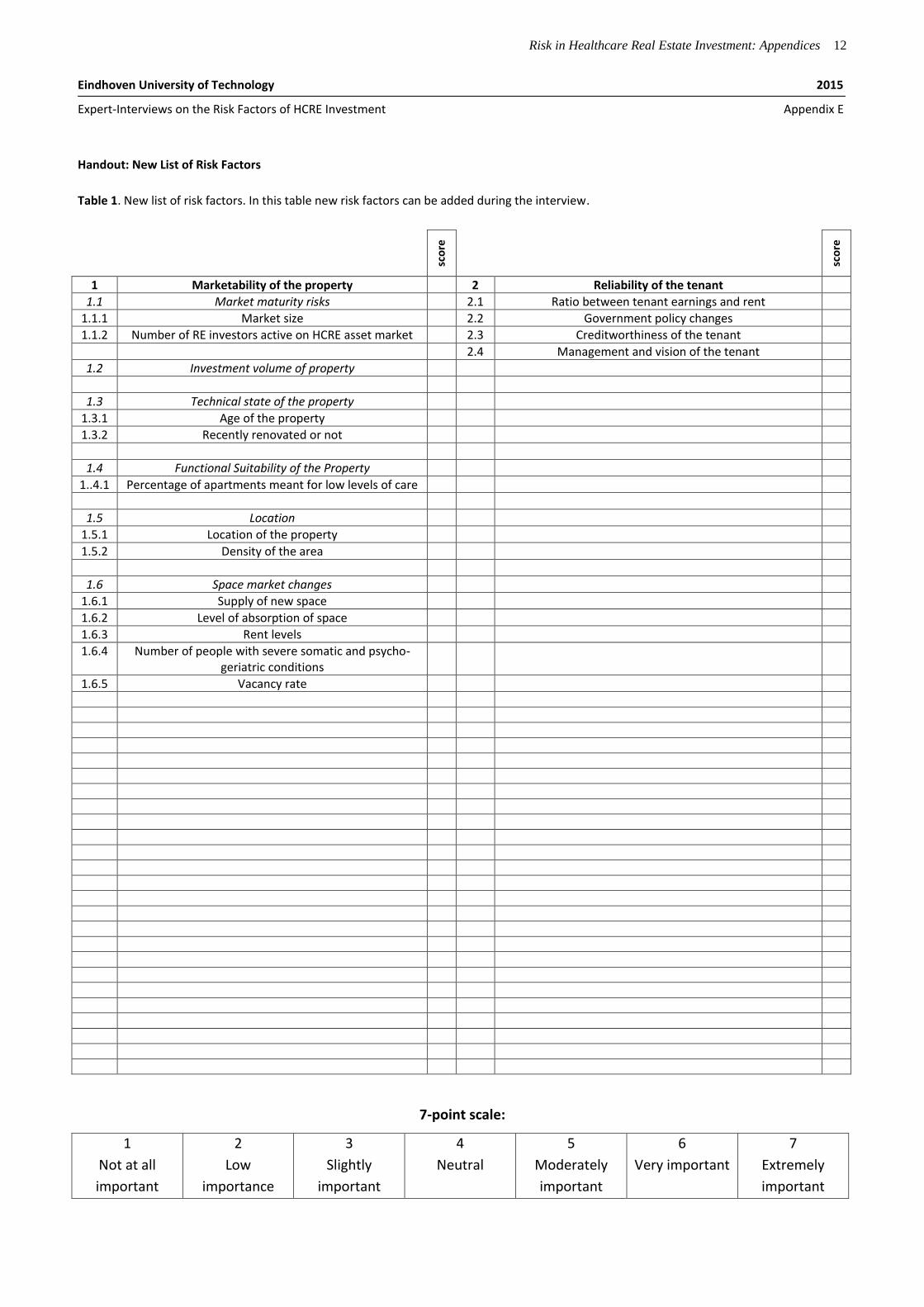
Risk in Healthcare Real Estate Investment: Appendices 12
Eindhoven University of Technology 2015
Expert-Interviews on the Risk Factors of HCRE Investment Appendix E
Handout: New List of Risk Factors
Table 1. New list of risk factors. In this table new risk factors can be added during the interview.
sco
re
sco
re
1 Marketability of the property 2 Reliability of the tenant
1.1 Market maturity risks 2.1 Ratio between tenant earnings and rent
1.1.1 Market size 2.2 Government policy changes
1.1.2 Number of RE investors active on HCRE asset market 2.3 Creditworthiness of the tenant
2.4 Management and vision of the tenant
1.2 Investment volume of property
1.3 Technical state of the property
1.3.1 Age of the property
1.3.2 Recently renovated or not
1.4 Functional Suitability of the Property
1..4.1 Percentage of apartments meant for low levels of care
1.5 Location
1.5.1 Location of the property
1.5.2 Density of the area
1.6 Space market changes
1.6.1 Supply of new space
1.6.2 Level of absorption of space
1.6.3 Rent levels
1.6.4 Number of people with severe somatic and psycho-geriatric conditions
1.6.5 Vacancy rate
7-point scale:
1
Not at all
important
2
Low
importance
3
Slightly
important
4
Neutral 5
Moderately
important
6
Very important 7
Extremely
important
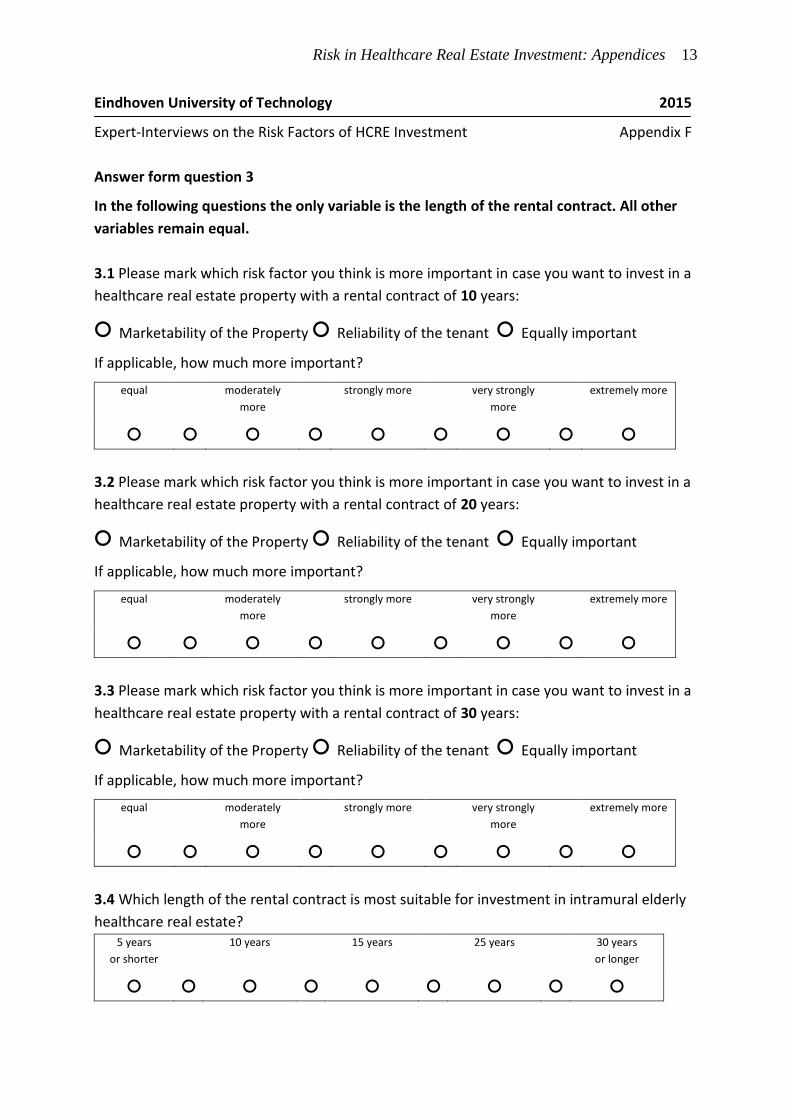
Risk in Healthcare Real Estate Investment: Appendices 13
Eindhoven University of Technology 2015
Expert-Interviews on the Risk Factors of HCRE Investment Appendix F
Answer form question 3
In the following questions the only variable is the length of the rental contract. All other
variables remain equal.
3.1 Please mark which risk factor you think is more important in case you want to invest in a
healthcare real estate property with a rental contract of 10 years:
○ Marketability of the Property ○ Reliability of the tenant ○ Equally important
If applicable, how much more important?
equal moderately
more
strongly more very strongly
more
extremely more
○ ○ ○ ○ ○ ○ ○ ○ ○
3.2 Please mark which risk factor you think is more important in case you want to invest in a
healthcare real estate property with a rental contract of 20 years:
○ Marketability of the Property ○ Reliability of the tenant ○ Equally important
If applicable, how much more important?
equal moderately
more
strongly more very strongly
more
extremely more
○ ○ ○ ○ ○ ○ ○ ○ ○
3.3 Please mark which risk factor you think is more important in case you want to invest in a
healthcare real estate property with a rental contract of 30 years:
○ Marketability of the Property ○ Reliability of the tenant ○ Equally important
If applicable, how much more important?
equal moderately
more
strongly more very strongly
more
extremely more
○ ○ ○ ○ ○ ○ ○ ○ ○
3.4 Which length of the rental contract is most suitable for investment in intramural elderly
healthcare real estate? 5 years
or shorter
10 years 15 years 25 years 30 years
or longer
○ ○ ○ ○ ○ ○ ○ ○ ○
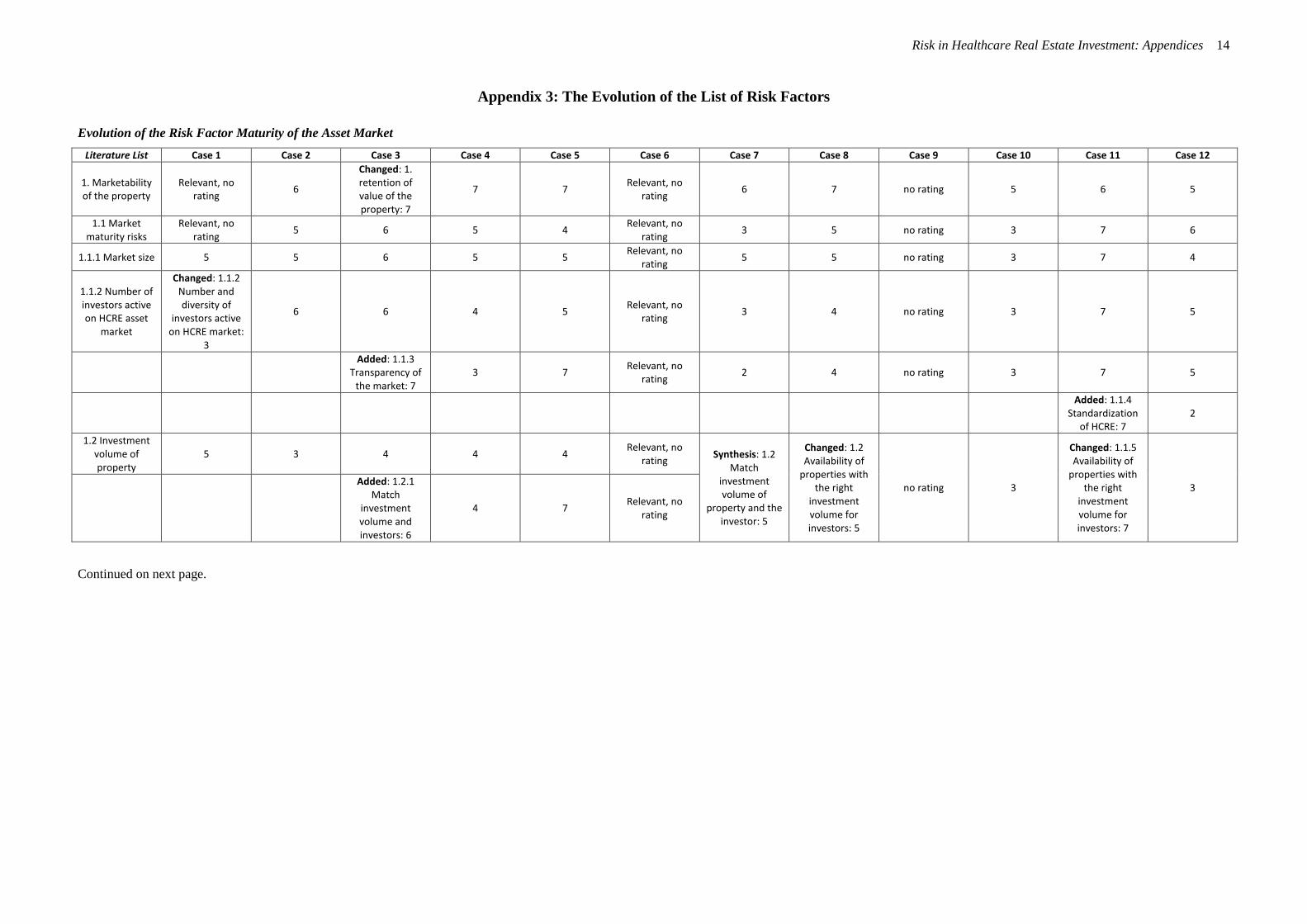
Risk in Healthcare Real Estate Investment: Appendices 14
Appendix 3: The Evolution of the List of Risk Factors
Evolution of the Risk Factor Maturity of the Asset Market
Literature List Case 1 Case 2 Case 3 Case 4 Case 5 Case 6 Case 7 Case 8 Case 9 Case 10 Case 11 Case 12
1. Marketability of the property
Relevant, no rating
6
Changed: 1. retention of value of the property: 7
7 7 Relevant, no
rating 6 7 no rating 5 6 5
1.1 Market maturity risks
Relevant, no rating
5 6 5 4 Relevant, no
rating 3 5 no rating 3 7 6
1.1.1 Market size 5 5 6 5 5 Relevant, no
rating 5 5 no rating 3 7 4
1.1.2 Number of investors active on HCRE asset
market
Changed: 1.1.2 Number and diversity of
investors active on HCRE market:
3
6 6 4 5 Relevant, no
rating 3 4 no rating 3 7 5
Added: 1.1.3
Transparency of the market: 7
3 7 Relevant, no
rating 2 4 no rating 3 7 5
Added: 1.1.4
Standardization of HCRE: 7
2
1.2 Investment volume of property
5 3 4 4 4 Relevant, no
rating Synthesis: 1.2
Match investment volume of
property and the investor: 5
Changed: 1.2 Availability of
properties with the right
investment volume for investors: 5
no rating 3
Changed: 1.1.5 Availability of
properties with the right
investment volume for investors: 7
3
Added: 1.2.1 Match
investment volume and investors: 6
4 7 Relevant, no
rating
Continued on next page.
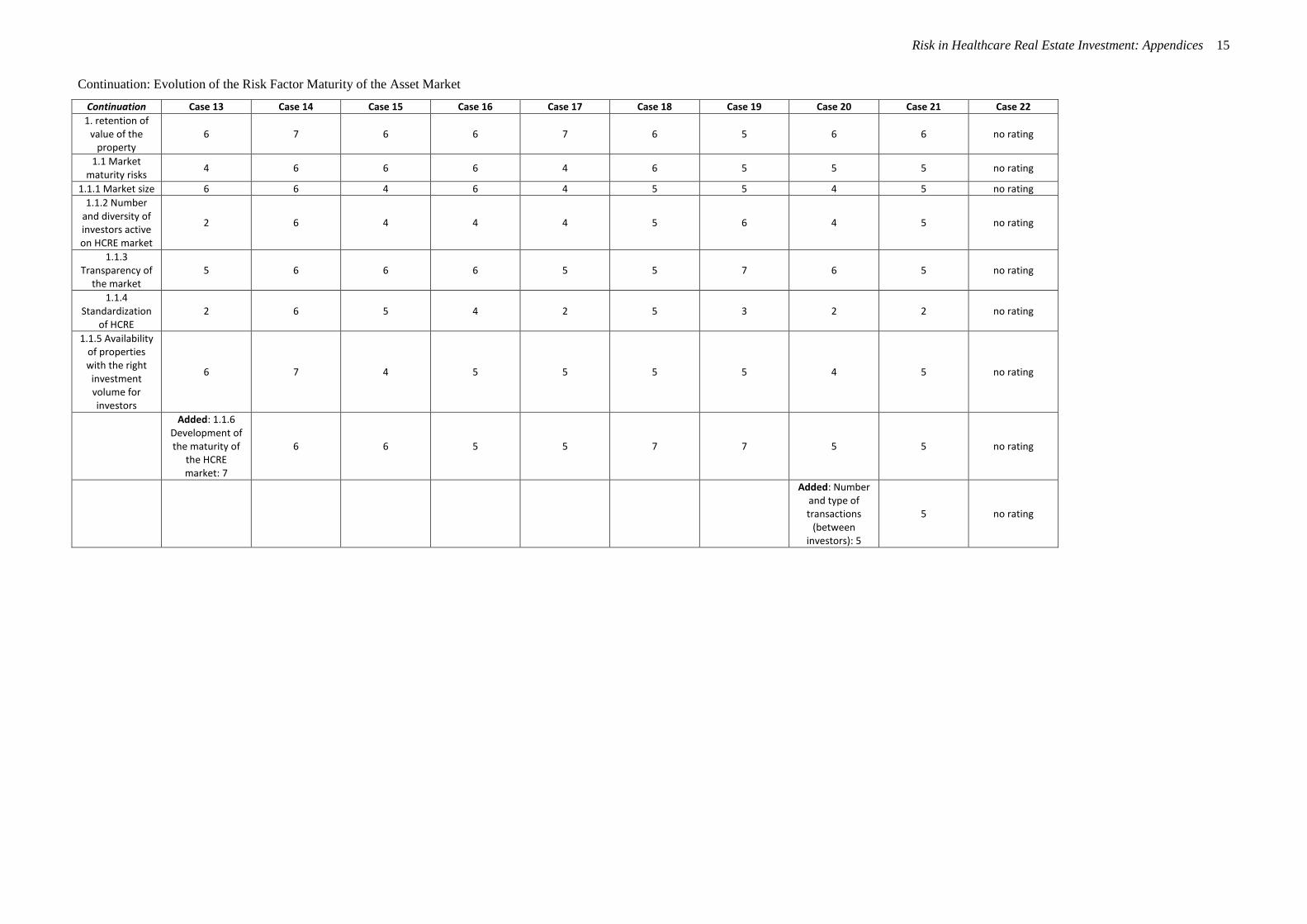
Risk in Healthcare Real Estate Investment: Appendices 15
Continuation: Evolution of the Risk Factor Maturity of the Asset Market
Continuation Case 13 Case 14 Case 15 Case 16 Case 17 Case 18 Case 19 Case 20 Case 21 Case 22
1. retention of value of the
property 6 7 6 6 7 6 5 6 6 no rating
1.1 Market maturity risks
4 6 6 6 4 6 5 5 5 no rating
1.1.1 Market size 6 6 4 6 4 5 5 4 5 no rating
1.1.2 Number and diversity of investors active on HCRE market
2 6 4 4 4 5 6 4 5 no rating
1.1.3 Transparency of
the market 5 6 6 6 5 5 7 6 5 no rating
1.1.4 Standardization
of HCRE 2 6 5 4 2 5 3 2 2 no rating
1.1.5 Availability of properties with the right
investment volume for investors
6 7 4 5 5 5 5 4 5 no rating
Added: 1.1.6 Development of the maturity of
the HCRE market: 7
6 6 5 5 7 7 5 5 no rating
Added: Number and type of transactions
(between investors): 5
5 no rating
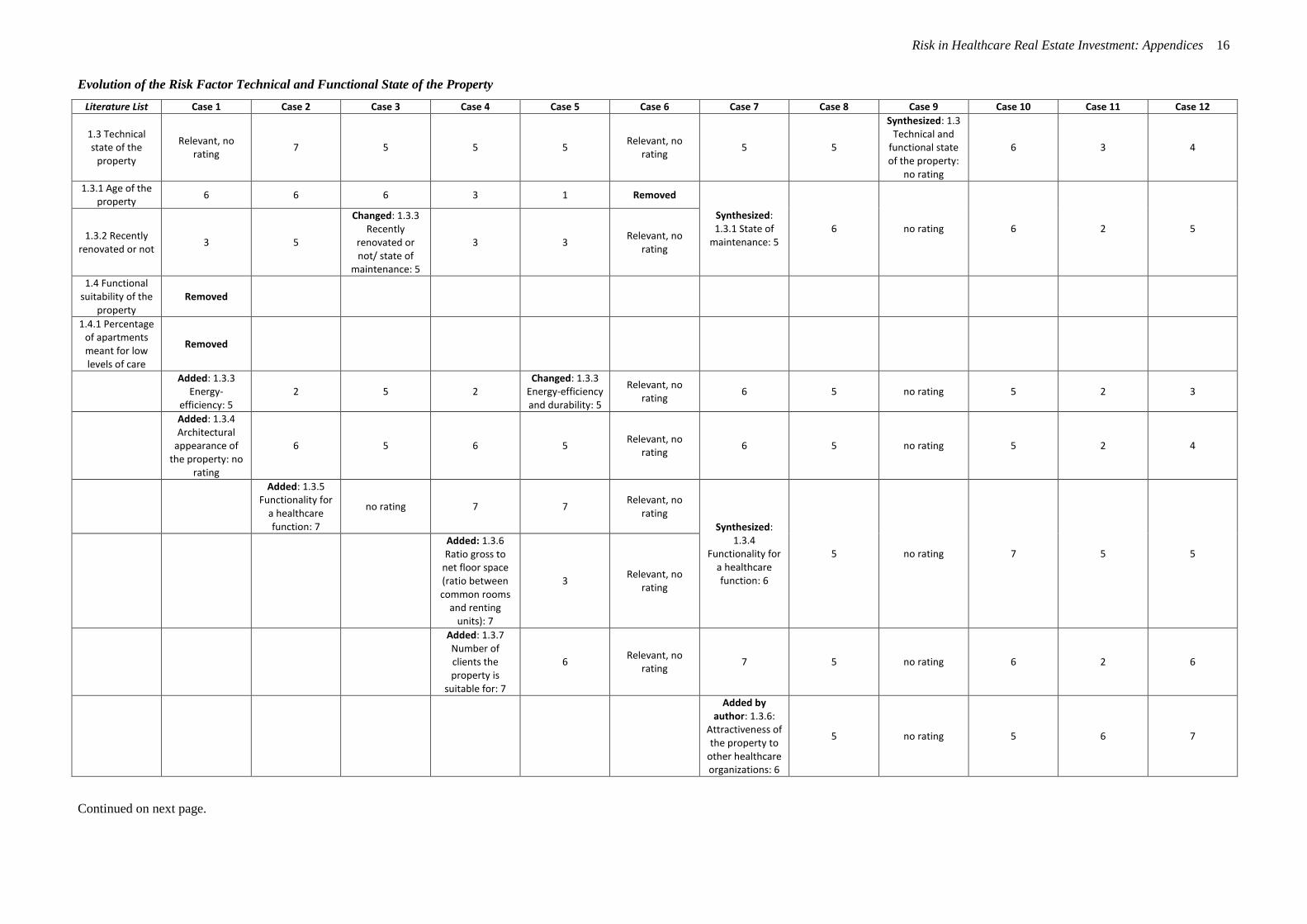
Risk in Healthcare Real Estate Investment: Appendices 16
Evolution of the Risk Factor Technical and Functional State of the Property
Literature List Case 1 Case 2 Case 3 Case 4 Case 5 Case 6 Case 7 Case 8 Case 9 Case 10 Case 11 Case 12
1.3 Technical state of the
property
Relevant, no rating
7 5 5 5 Relevant, no
rating 5 5
Synthesized: 1.3 Technical and
functional state of the property:
no rating
6 3 4
1.3.1 Age of the property
6 6 6 3 1 Removed
Synthesized: 1.3.1 State of
maintenance: 5 6 no rating 6 2 5
1.3.2 Recently renovated or not
3 5
Changed: 1.3.3 Recently
renovated or not/ state of
maintenance: 5
3 3 Relevant, no
rating
1.4 Functional suitability of the
property Removed
1.4.1 Percentage of apartments meant for low levels of care
Removed
Added: 1.3.3
Energy-efficiency: 5
2 5 2 Changed: 1.3.3
Energy-efficiency and durability: 5
Relevant, no rating
6 5 no rating 5 2 3
Added: 1.3.4 Architectural
appearance of the property: no
rating
6 5 6 5 Relevant, no
rating 6 5 no rating 5 2 4
Added: 1.3.5 Functionality for
a healthcare function: 7
no rating 7 7 Relevant, no
rating
Synthesized: 1.3.4
Functionality for a healthcare function: 6
5 no rating 7 5 5
Added: 1.3.6 Ratio gross to
net floor space (ratio between common rooms
and renting units): 7
3 Relevant, no
rating
Added: 1.3.7 Number of clients the property is
suitable for: 7
6 Relevant, no
rating 7 5 no rating 6 2 6
Added by author: 1.3.6:
Attractiveness of the property to
other healthcare organizations: 6
5 no rating 5 6 7
Continued on next page.
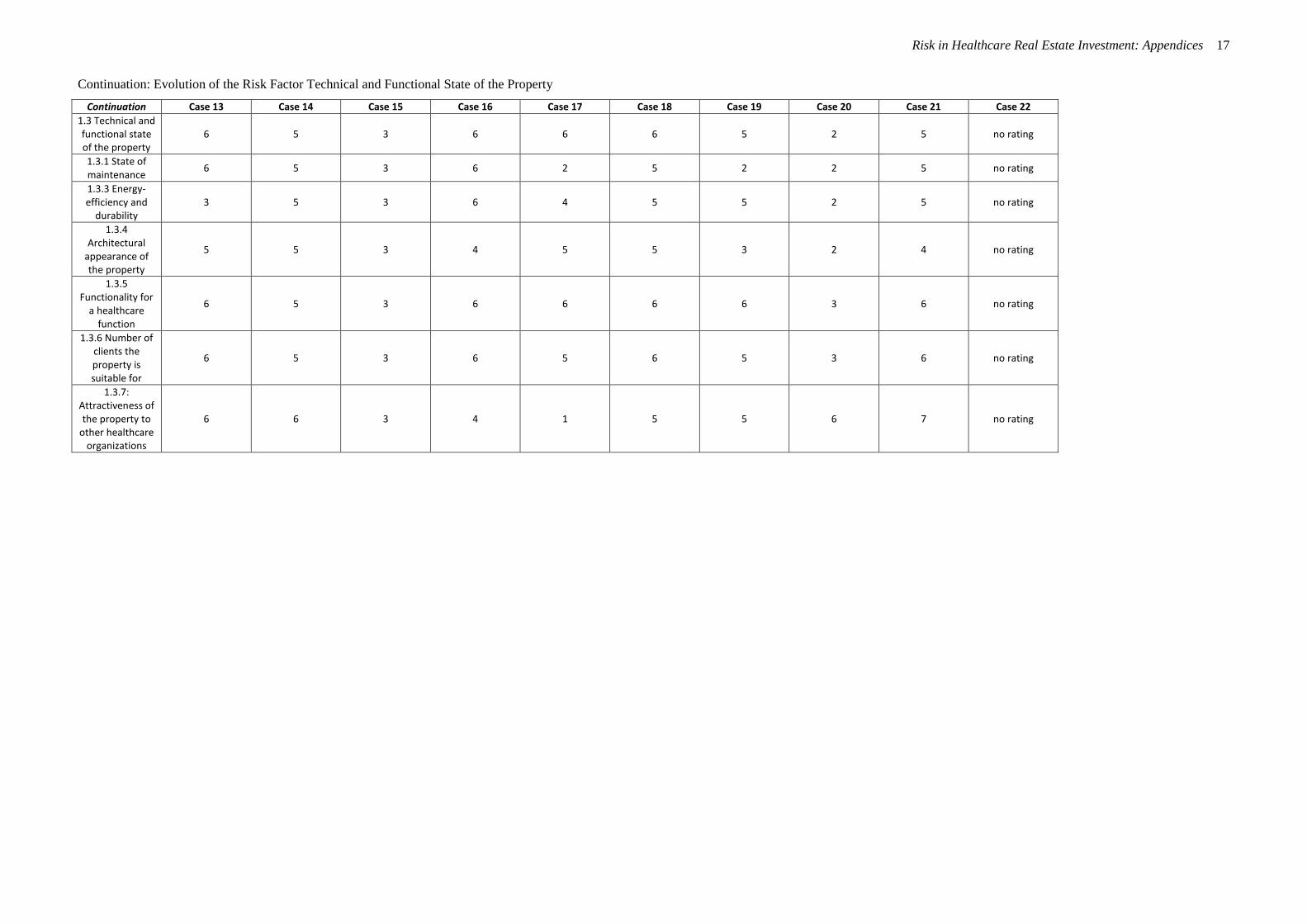
Risk in Healthcare Real Estate Investment: Appendices 17
Continuation: Evolution of the Risk Factor Technical and Functional State of the Property
Continuation Case 13 Case 14 Case 15 Case 16 Case 17 Case 18 Case 19 Case 20 Case 21 Case 22
1.3 Technical and functional state of the property
6 5 3 6 6 6 5 2 5 no rating
1.3.1 State of maintenance
6 5 3 6 2 5 2 2 5 no rating
1.3.3 Energy-efficiency and
durability 3 5 3 6 4 5 5 2 5 no rating
1.3.4 Architectural
appearance of the property
5 5 3 4 5 5 3 2 4 no rating
1.3.5 Functionality for
a healthcare function
6 5 3 6 6 6 6 3 6 no rating
1.3.6 Number of clients the property is suitable for
6 5 3 6 5 6 5 3 6 no rating
1.3.7: Attractiveness of the property to
other healthcare organizations
6 6 3 4 1 5 5 6 7 no rating
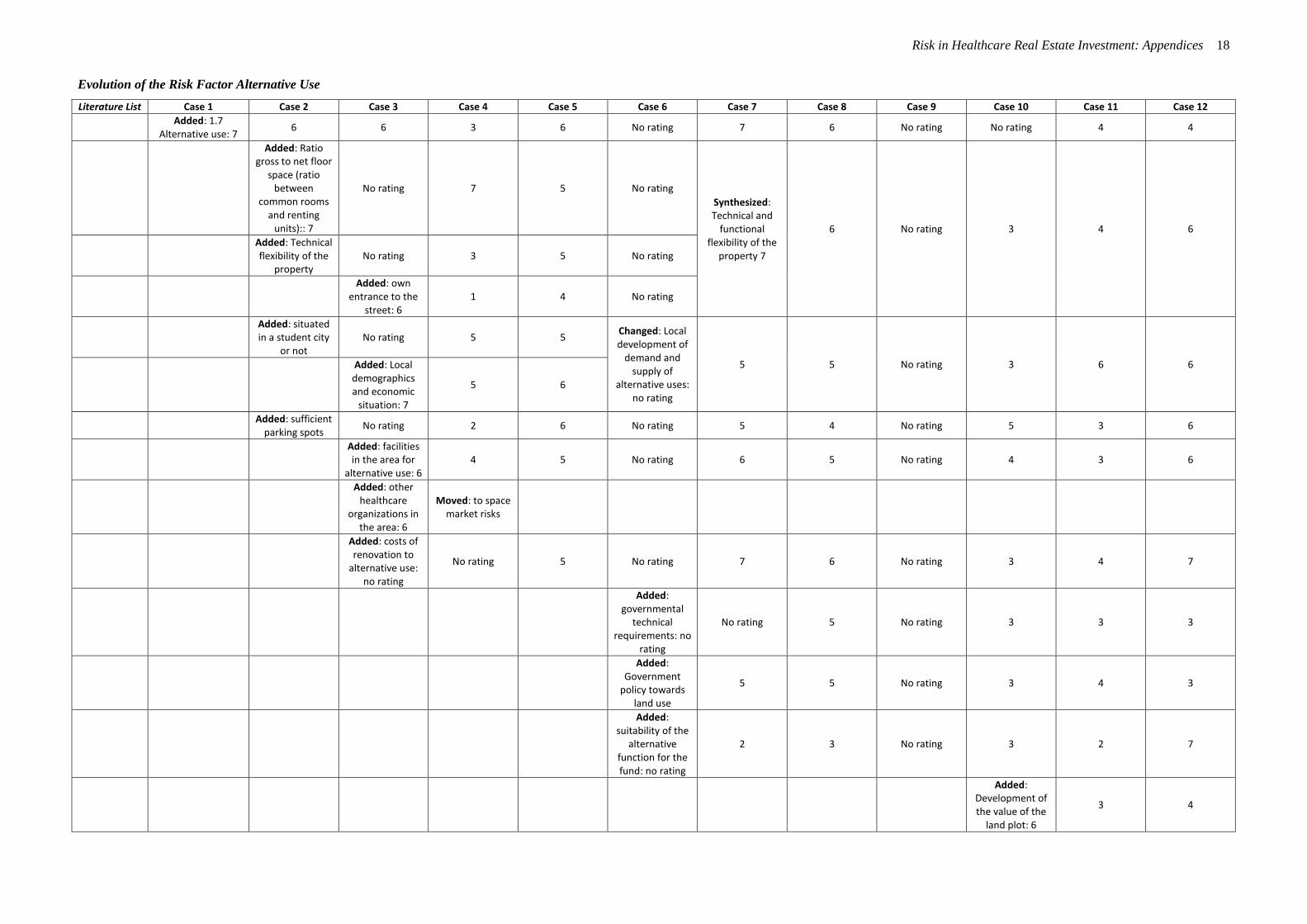
Risk in Healthcare Real Estate Investment: Appendices 18
Evolution of the Risk Factor Alternative Use
Literature List Case 1 Case 2 Case 3 Case 4 Case 5 Case 6 Case 7 Case 8 Case 9 Case 10 Case 11 Case 12
Added: 1.7
Alternative use: 7 6 6 3 6 No rating 7 6 No rating No rating 4 4
Added: Ratio gross to net floor
space (ratio between
common rooms and renting
units):: 7
No rating 7 5 No rating
Synthesized: Technical and
functional flexibility of the
property 7
6 No rating 3 4 6
Added: Technical flexibility of the
property No rating 3 5 No rating
Added: own
entrance to the street: 6
1 4 No rating
Added: situated in a student city
or not No rating 5 5
Changed: Local development of
demand and supply of
alternative uses: no rating
5 5 No rating 3 6 6
Added: Local demographics and economic
situation: 7
5 6
Added: sufficient
parking spots No rating 2 6 No rating 5 4 No rating 5 3 6
Added: facilities in the area for
alternative use: 6 4 5 No rating 6 5 No rating 4 3 6
Added: other healthcare
organizations in the area: 6
Moved: to space market risks
Added: costs of renovation to
alternative use: no rating
No rating 5 No rating 7 6 No rating 3 4 7
Added: governmental
technical requirements: no
rating
No rating 5 No rating 3 3 3
Added: Government
policy towards land use
5 5 No rating 3 4 3
Added: suitability of the
alternative function for the fund: no rating
2 3 No rating 3 2 7
Added: Development of the value of the
land plot: 6
3 4
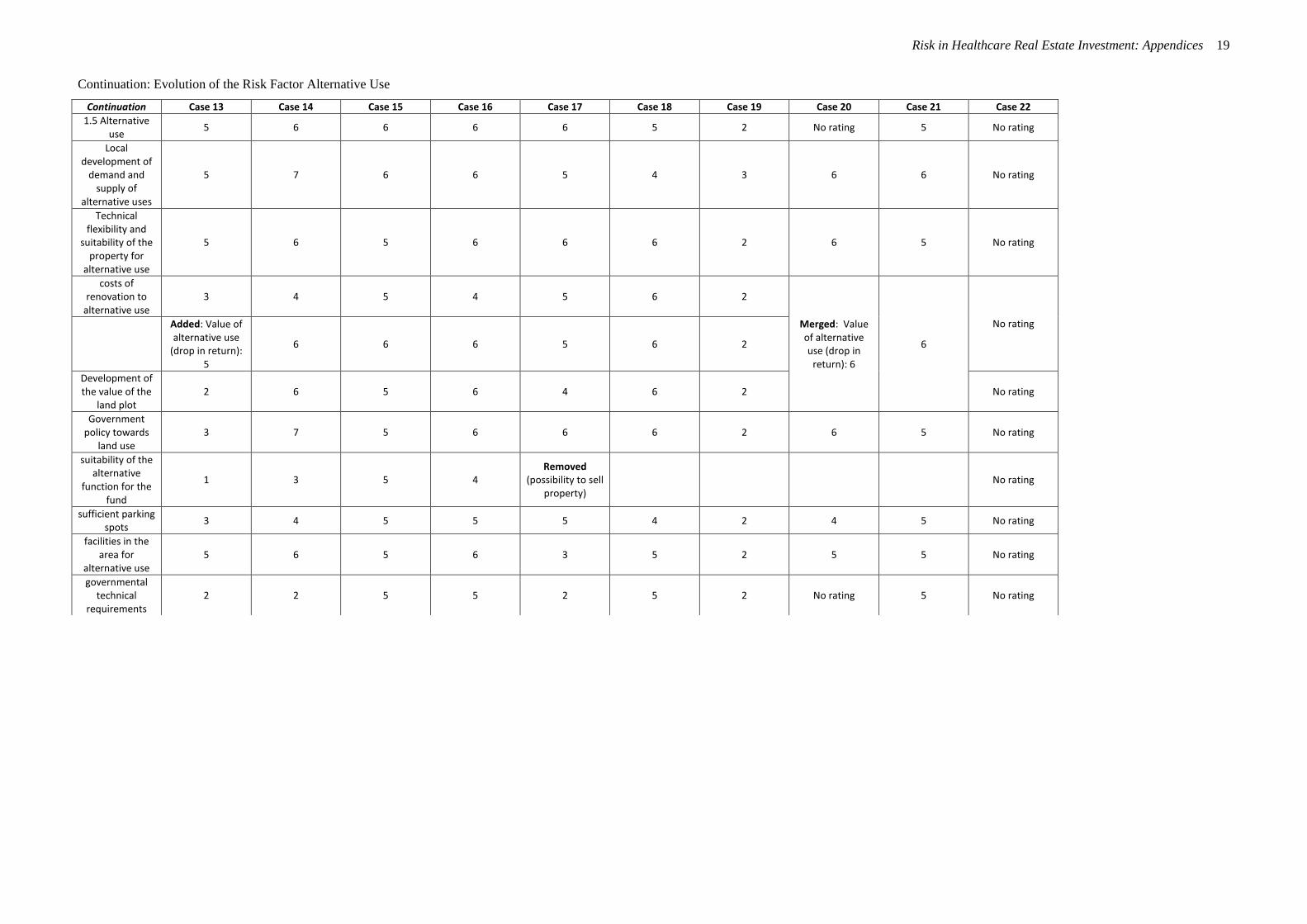
Risk in Healthcare Real Estate Investment: Appendices 19
Continuation: Evolution of the Risk Factor Alternative Use
Continuation Case 13 Case 14 Case 15 Case 16 Case 17 Case 18 Case 19 Case 20 Case 21 Case 22
1.5 Alternative use
5 6 6 6 6 5 2 No rating 5 No rating
Local development of
demand and supply of
alternative uses
5 7 6 6 5 4 3 6 6 No rating
Technical flexibility and
suitability of the property for
alternative use
5 6 5 6 6 6 2 6 5 No rating
costs of renovation to
alternative use 3 4 5 4 5 6 2
Merged: Value of alternative use (drop in
return): 6
6
No rating
Added: Value of alternative use
(drop in return): 5
6 6 6 5 6 2
Development of the value of the
land plot 2 6 5 6 4 6 2 No rating
Government policy towards
land use 3 7 5 6 6 6 2 6 5 No rating
suitability of the alternative
function for the fund
1 3 5 4 Removed
(possibility to sell property)
No rating
sufficient parking spots
3 4 5 5 5 4 2 4 5 No rating
facilities in the area for
alternative use 5 6 5 6 3 5 2 5 5 No rating
governmental technical
requirements 2 2 5 5 2 5 2 No rating 5 No rating
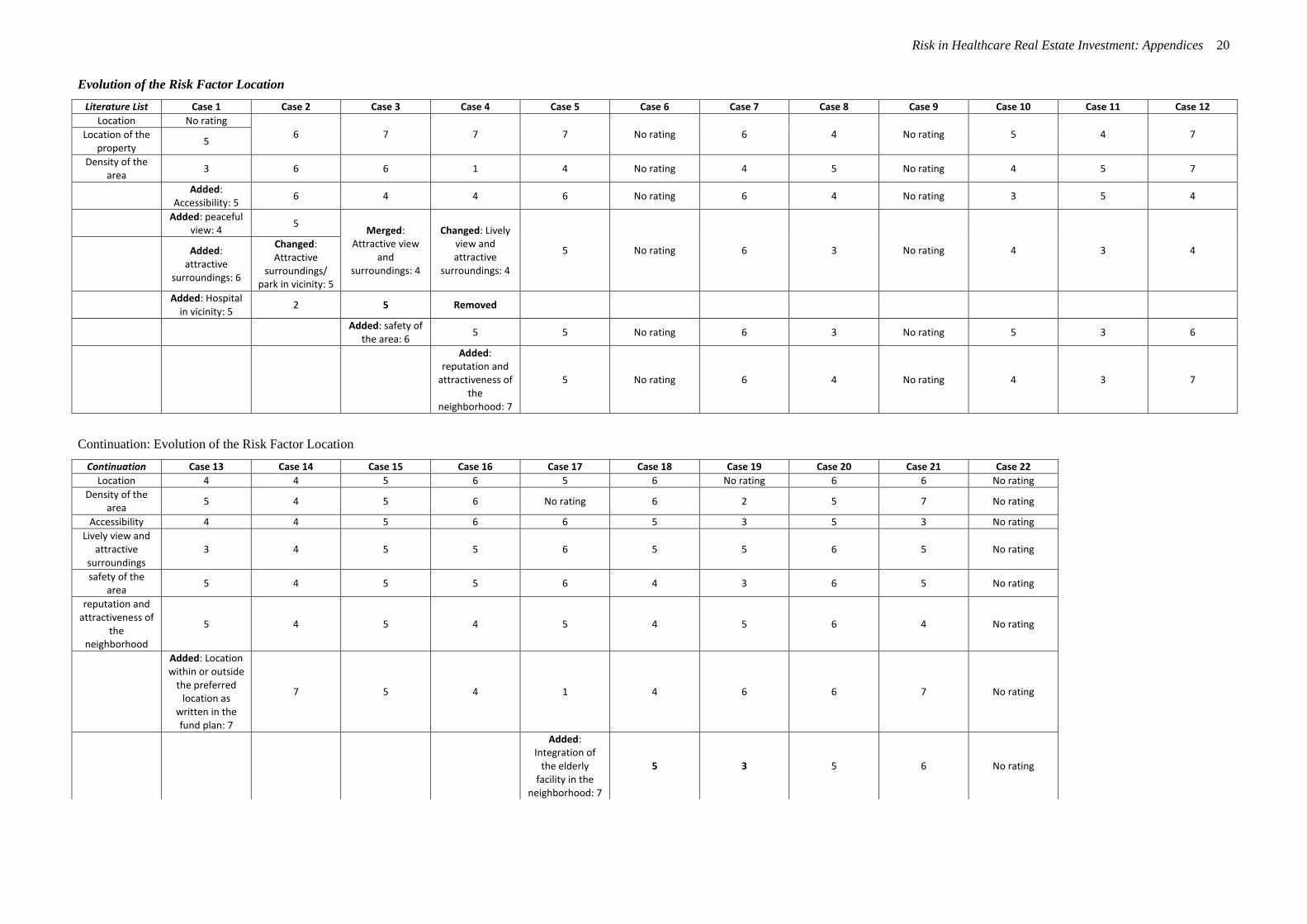
Risk in Healthcare Real Estate Investment: Appendices 20
Evolution of the Risk Factor Location
Literature List Case 1 Case 2 Case 3 Case 4 Case 5 Case 6 Case 7 Case 8 Case 9 Case 10 Case 11 Case 12
Location No rating
6 7 7 7 No rating 6 4 No rating 5 4 7 Location of the property
5
Density of the area
3 6 6 1 4 No rating 4 5 No rating 4 5 7
Added:
Accessibility: 5 6 4 4 6 No rating 6 4 No rating 3 5 4
Added: peaceful
view: 4 5
Merged: Attractive view
and surroundings: 4
Changed: Lively view and attractive
surroundings: 4
5 No rating 6 3 No rating 4 3 4
Added:
attractive surroundings: 6
Changed: Attractive
surroundings/ park in vicinity: 5
Added: Hospital
in vicinity: 5 2 5 Removed
Added: safety of
the area: 6 5 5 No rating 6 3 No rating 5 3 6
Added: reputation and
attractiveness of the
neighborhood: 7
5 No rating 6 4 No rating 4 3 7
Continuation: Evolution of the Risk Factor Location
Continuation Case 13 Case 14 Case 15 Case 16 Case 17 Case 18 Case 19 Case 20 Case 21 Case 22
Location 4 4 5 6 5 6 No rating 6 6 No rating
Density of the area
5 4 5 6 No rating 6 2 5 7 No rating
Accessibility 4 4 5 6 6 5 3 5 3 No rating
Lively view and attractive
surroundings 3 4 5 5 6 5 5 6 5 No rating
safety of the area
5 4 5 5 6 4 3 6 5 No rating
reputation and attractiveness of
the neighborhood
5 4 5 4 5 4 5 6 4 No rating
Added: Location within or outside
the preferred location as
written in the fund plan: 7
7 5 4 1 4 6 6 7 No rating
Added: Integration of
the elderly facility in the
neighborhood: 7
5 3 5 6 No rating
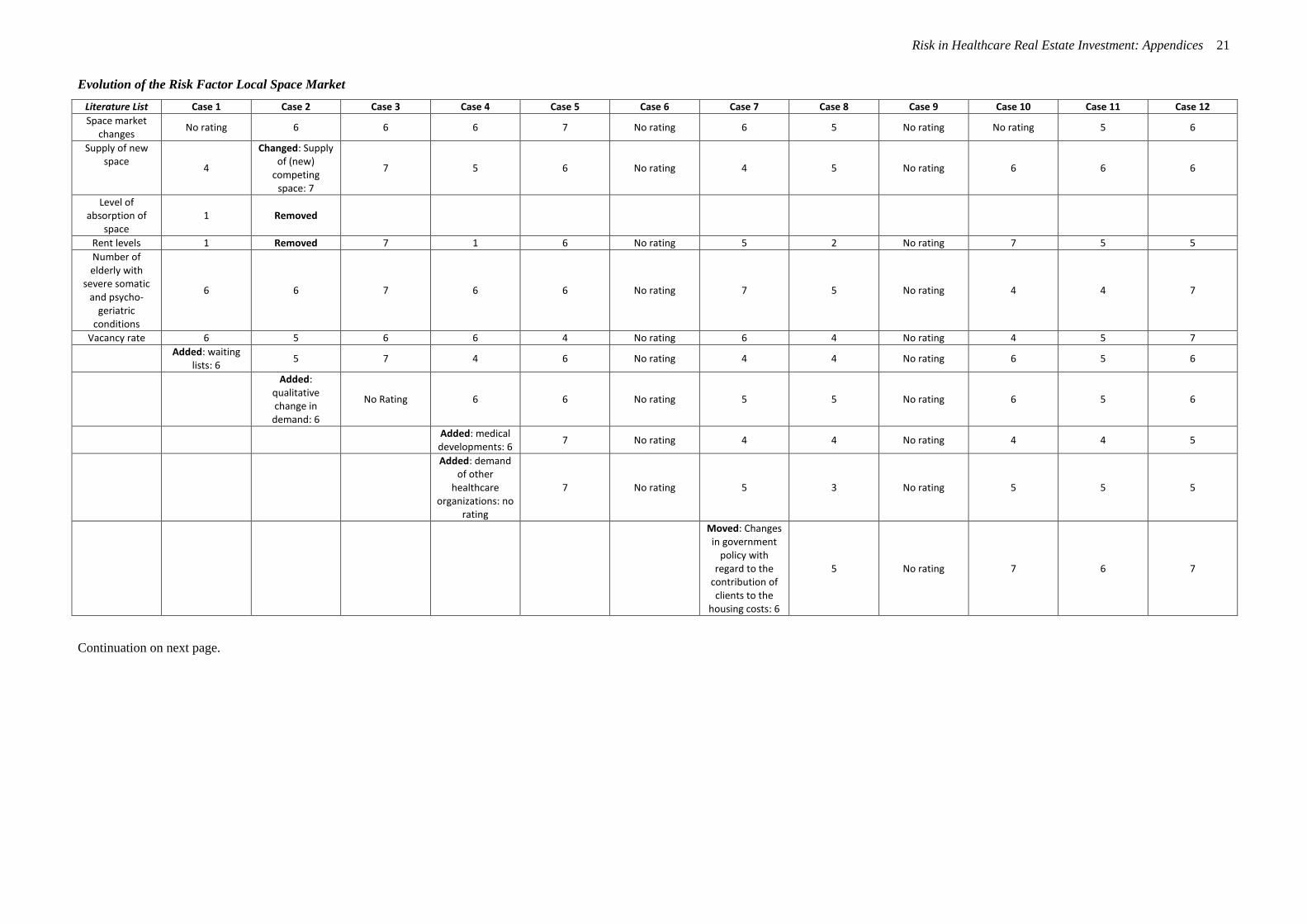
Risk in Healthcare Real Estate Investment: Appendices 21
Evolution of the Risk Factor Local Space Market
Literature List Case 1 Case 2 Case 3 Case 4 Case 5 Case 6 Case 7 Case 8 Case 9 Case 10 Case 11 Case 12
Space market changes
No rating 6 6 6 7 No rating 6 5 No rating No rating 5 6
Supply of new space
4
Changed: Supply of (new)
competing space: 7
7 5 6 No rating 4 5 No rating 6 6 6
Level of absorption of
space 1 Removed
Rent levels 1 Removed 7 1 6 No rating 5 2 No rating 7 5 5
Number of elderly with
severe somatic and psycho-
geriatric conditions
6 6 7 6 6 No rating 7 5 No rating 4 4 7
Vacancy rate 6 5 6 6 4 No rating 6 4 No rating 4 5 7
Added: waiting
lists: 6 5 7 4 6 No rating 4 4 No rating 6 5 6
Added: qualitative change in
demand: 6
No Rating 6 6 No rating 5 5 No rating 6 5 6
Added: medical developments: 6
7 No rating 4 4 No rating 4 4 5
Added: demand of other
healthcare organizations: no
rating
7 No rating 5 3 No rating 5 5 5
Moved: Changes in government
policy with regard to the
contribution of clients to the
housing costs: 6
5 No rating 7 6 7
Continuation on next page.

Risk in Healthcare Real Estate Investment: Appendices 22
Continuation: Evolution of the Risk Factor Local Space Market
Continuation Case 13 Case 14 Case 15 Case 16 Case 17 Case 18 Case 19 Case 20 Case 21 Case 22
Changes on the local space
market 7 3 6 6 6 5 5 No rating 6 No rating
Changes in government policy with
regard to the contribution of clients to the housing costs
7 6 7 7 2 7 2 6 6 No rating
medical developments
3 3 3 5 3 5 3 2 7 No rating
Supply of (new) competing space
5 3 5 5 6 6 6 6 5 No rating
Local development of
elderly with severe somatic
and psycho-geriatric
conditions
7 3 6 6 6 6 7 6 7 No rating
Vacancy rates of competing properties
2 3 5 4 5 5 3 6 5 No rating
waiting lists 5 3 5 4 2 5 3 2 5 No rating
qualitative change in demand
5 5 5 6 7 6 6 1 4 No rating
Rent levels of competing properties
3 3 5 5 4 5 5 6 5 No rating
demand of other healthcare
organizations 2 3 5 4 5 3 6 4 4 No rating
Added: Willingness of
elderly to move out of their own
home: 6
No rating 3 5 5 2 6 No rating
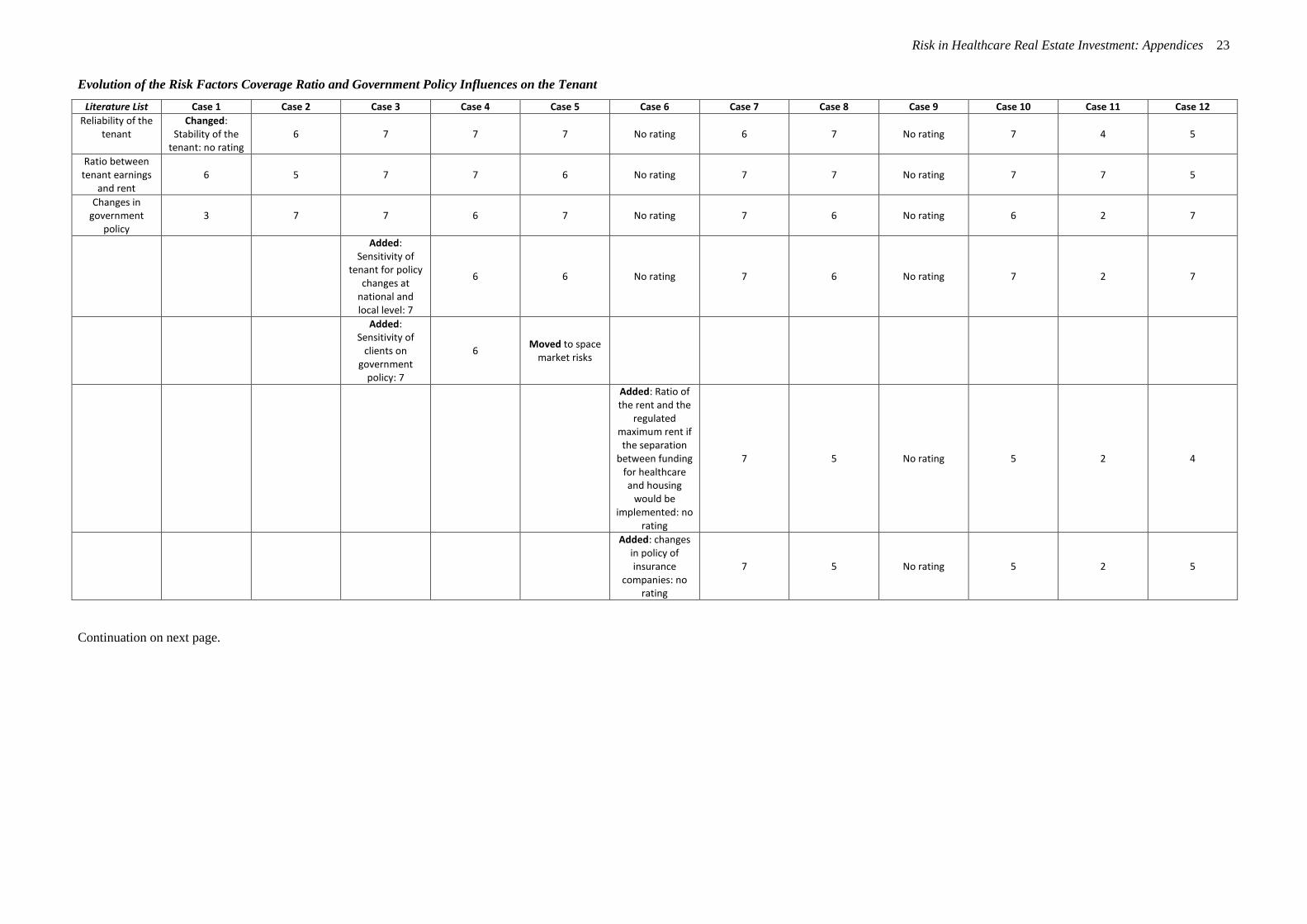
Risk in Healthcare Real Estate Investment: Appendices 23
Evolution of the Risk Factors Coverage Ratio and Government Policy Influences on the Tenant
Literature List Case 1 Case 2 Case 3 Case 4 Case 5 Case 6 Case 7 Case 8 Case 9 Case 10 Case 11 Case 12
Reliability of the tenant
Changed: Stability of the
tenant: no rating 6 7 7 7 No rating 6 7 No rating 7 4 5
Ratio between tenant earnings
and rent 6 5 7 7 6 No rating 7 7 No rating 7 7 5
Changes in government
policy 3 7 7 6 7 No rating 7 6 No rating 6 2 7
Added: Sensitivity of
tenant for policy changes at
national and local level: 7
6 6 No rating 7 6 No rating 7 2 7
Added: Sensitivity of
clients on government
policy: 7
6 Moved to space
market risks
Added: Ratio of the rent and the
regulated maximum rent if the separation
between funding for healthcare and housing
would be implemented: no
rating
7 5 No rating 5 2 4
Added: changes in policy of insurance
companies: no rating
7 5 No rating 5 2 5
Continuation on next page.
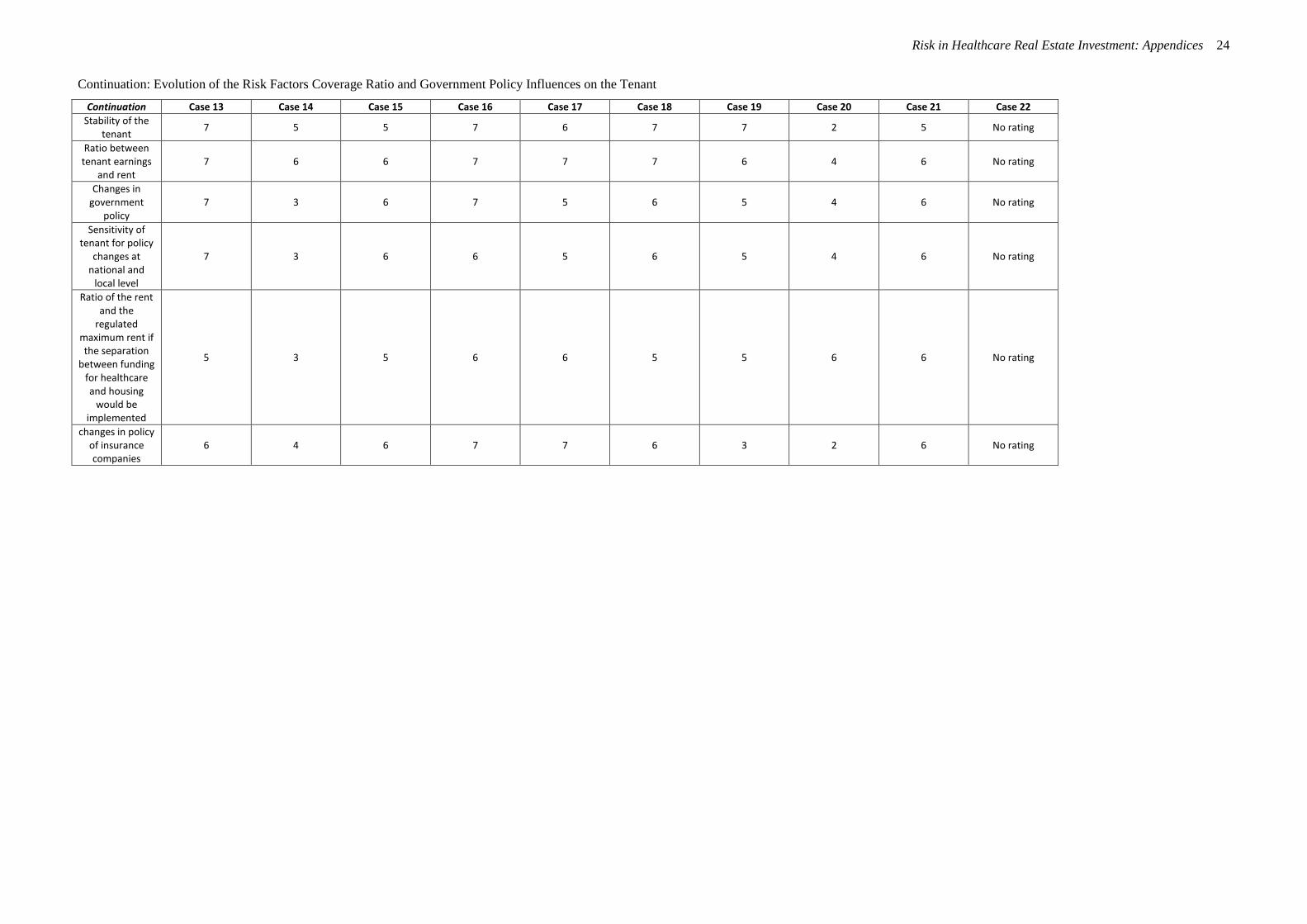
Risk in Healthcare Real Estate Investment: Appendices 24
Continuation: Evolution of the Risk Factors Coverage Ratio and Government Policy Influences on the Tenant
Continuation Case 13 Case 14 Case 15 Case 16 Case 17 Case 18 Case 19 Case 20 Case 21 Case 22
Stability of the tenant
7 5 5 7 6 7 7 2 5 No rating
Ratio between tenant earnings
and rent 7 6 6 7 7 7 6 4 6 No rating
Changes in government
policy 7 3 6 7 5 6 5 4 6 No rating
Sensitivity of tenant for policy
changes at national and
local level
7 3 6 6 5 6 5 4 6 No rating
Ratio of the rent and the
regulated maximum rent if the separation
between funding for healthcare and housing
would be implemented
5 3 5 6 6 5 5 6 6 No rating
changes in policy of insurance companies
6 4 6 7 7 6 3 2 6 No rating
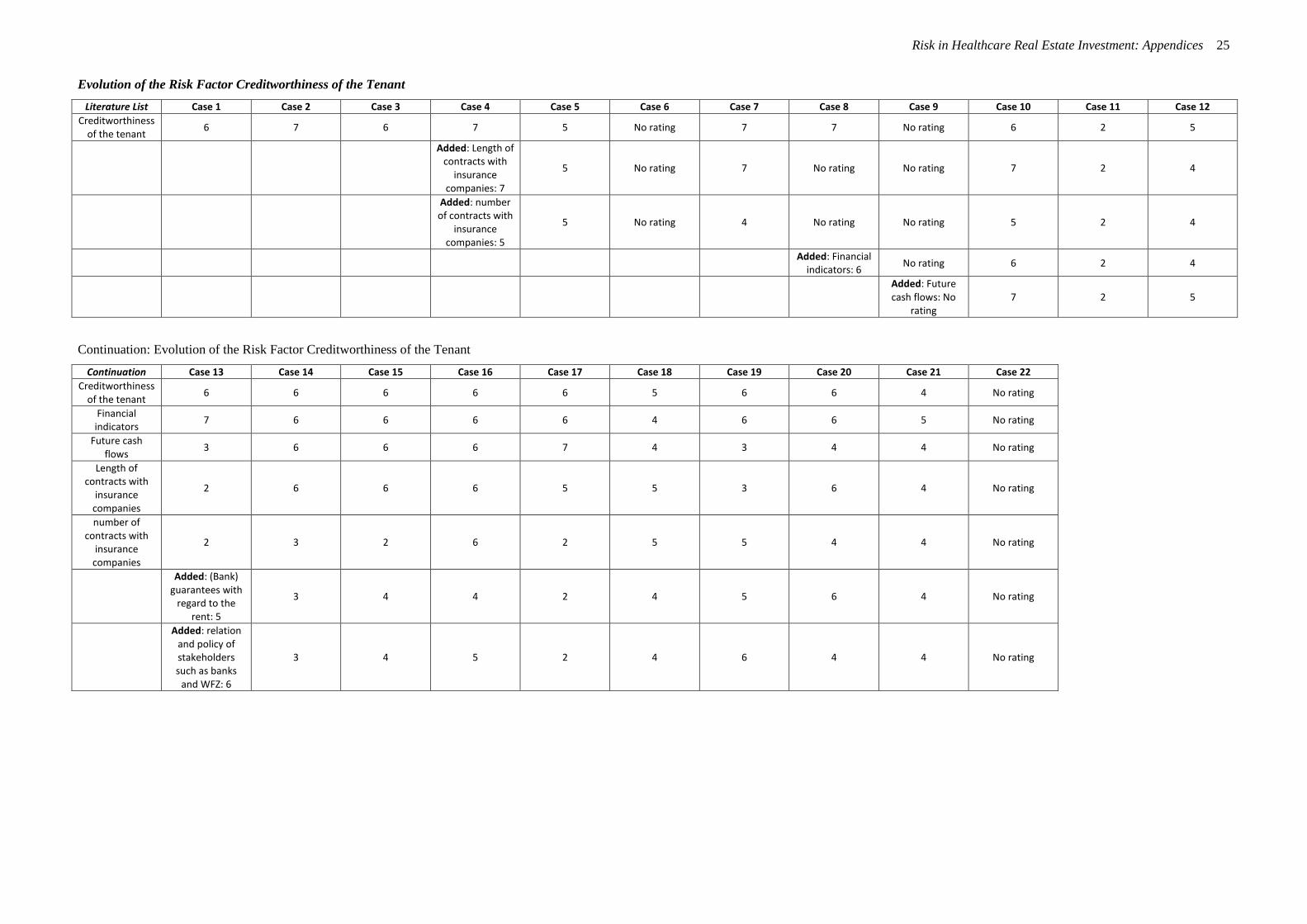
Risk in Healthcare Real Estate Investment: Appendices 25
Evolution of the Risk Factor Creditworthiness of the Tenant
Literature List Case 1 Case 2 Case 3 Case 4 Case 5 Case 6 Case 7 Case 8 Case 9 Case 10 Case 11 Case 12
Creditworthiness of the tenant
6 7 6 7 5 No rating 7 7 No rating 6 2 5
Added: Length of contracts with
insurance companies: 7
5 No rating 7 No rating No rating 7 2 4
Added: number of contracts with
insurance companies: 5
5 No rating 4 No rating No rating 5 2 4
Added: Financial indicators: 6
No rating 6 2 4
Added: Future cash flows: No
rating 7 2 5
Continuation: Evolution of the Risk Factor Creditworthiness of the Tenant
Continuation Case 13 Case 14 Case 15 Case 16 Case 17 Case 18 Case 19 Case 20 Case 21 Case 22
Creditworthiness of the tenant
6 6 6 6 6 5 6 6 4 No rating
Financial indicators
7 6 6 6 6 4 6 6 5 No rating
Future cash flows
3 6 6 6 7 4 3 4 4 No rating
Length of contracts with
insurance companies
2 6 6 6 5 5 3 6 4 No rating
number of contracts with
insurance companies
2 3 2 6 2 5 5 4 4 No rating
Added: (Bank) guarantees with
regard to the rent: 5
3 4 4 2 4 5 6 4 No rating
Added: relation and policy of stakeholders such as banks
and WFZ: 6
3 4 5 2 4 6 4 4 No rating

Risk in Healthcare Real Estate Investment: Appendices 26
Evolution of the Risk Factors Quality of the Management of the Tenant and the Vision of the Tenant
Literature List Case 1 Case 2 Case 3 Case 4 Case 5 Case 6 Case 7 Case 8 Case 9 Case 10 Case 11 Case 12
Management and vision of the
tenant
Changed: quality of the
management of the tenant: 5
5 6 6 6 No rating 5 6 No rating 6 2 5
Added:
Customer satisfaction: 6
7 6 No rating 5 5 No rating 5 2 6
Added: quality of the control
information: 5 4 4 5 6 No rating 5 5 No rating 6 2 7
Added:
absenteeism staff: 4
No rating 5 5 No rating 4 4 No rating 6 2 7
Added: Under inspection in the
past 3 years: 3 3 5 4 7 No rating 5 5 No rating 5 2 4
Added: Composition and term of office of the management
team: 3
5 No rating 5 5 No rating 4 2 5
Added: adaptability of the tenant: no
rating
4 5 No rating 7 2 6
Added: the ratio between income
of the tenant and real estate costs of tenant:
no rating
3 5 No rating 7 2 7
Changed: Vision of the tenant: 5
6 5 No rating 5 No rating 5 5 No rating 6 3 3
Added: plans on investment by
tenant: 2 6 5 3 5 No rating 4 4 No rating 5 3 4
Added: Ratio of renting vs. owning by tenant: 5
5 5 Merged: flexibility in real
estate: 4 5
Changed: strategy of the
tenant with regard to real
estate: No rating
4 5 No rating 5 3 5
Added: flexibility in real estate: 7
No rating
Added: portfolio of care: 6
No rating 6 6 No rating 4 2 No rating 5 3 7
Added: vision of tenant on
healthcare: 6 4 No rating 5 6 No rating 6 3 4
Continuation on next page
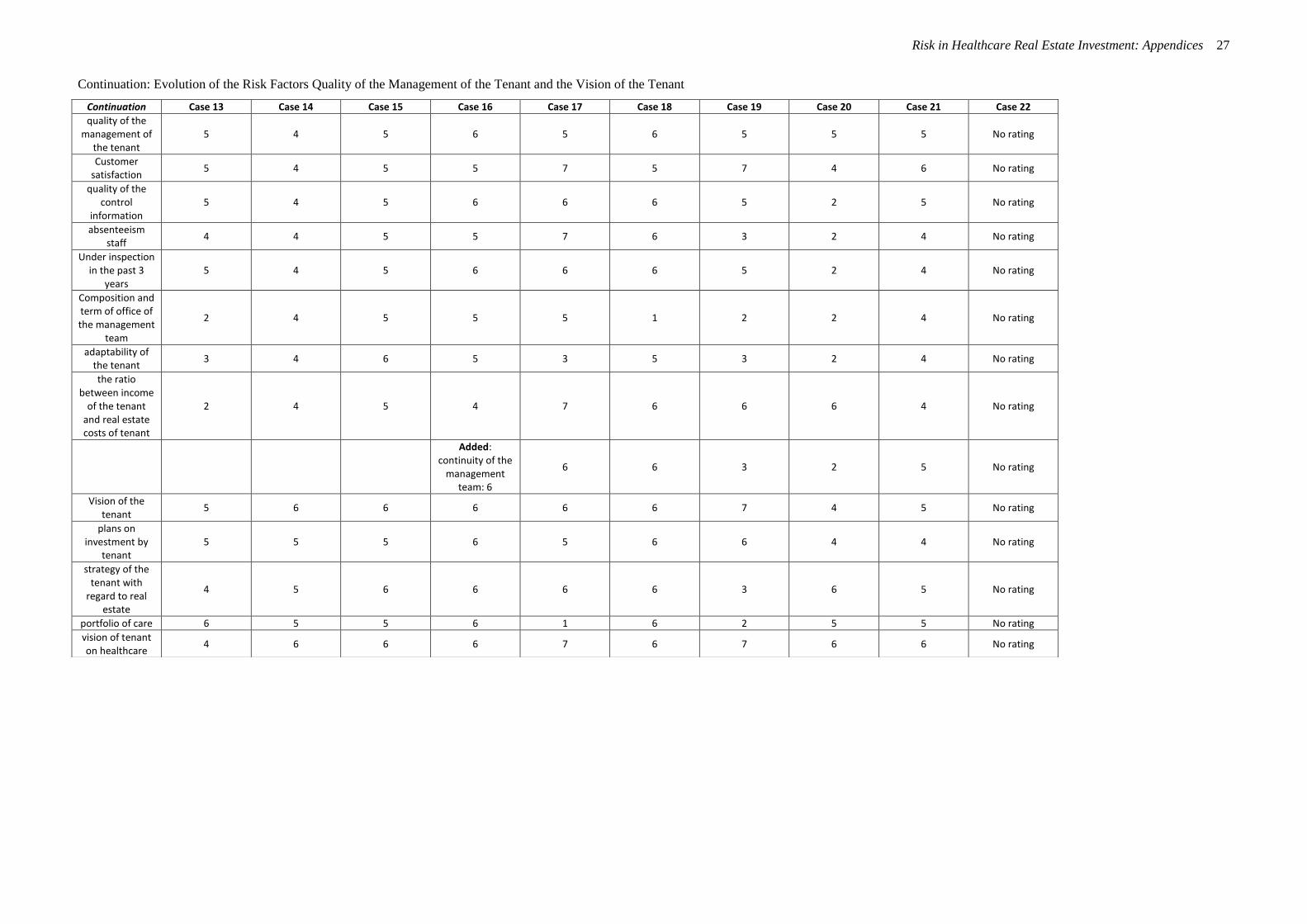
Risk in Healthcare Real Estate Investment: Appendices 27
Continuation: Evolution of the Risk Factors Quality of the Management of the Tenant and the Vision of the Tenant
Continuation Case 13 Case 14 Case 15 Case 16 Case 17 Case 18 Case 19 Case 20 Case 21 Case 22
quality of the management of
the tenant 5 4 5 6 5 6 5 5 5 No rating
Customer satisfaction
5 4 5 5 7 5 7 4 6 No rating
quality of the control
information 5 4 5 6 6 6 5 2 5 No rating
absenteeism staff
4 4 5 5 7 6 3 2 4 No rating
Under inspection in the past 3
years 5 4 5 6 6 6 5 2 4 No rating
Composition and term of office of the management
team
2 4 5 5 5 1 2 2 4 No rating
adaptability of the tenant
3 4 6 5 3 5 3 2 4 No rating
the ratio between income
of the tenant and real estate costs of tenant
2 4 5 4 7 6 6 6 4 No rating
Added: continuity of the
management team: 6
6 6 3 2 5 No rating
Vision of the tenant
5 6 6 6 6 6 7 4 5 No rating
plans on investment by
tenant 5 5 5 6 5 6 6 4 4 No rating
strategy of the tenant with
regard to real estate
4 5 6 6 6 6 3 6 5 No rating
portfolio of care 6 5 5 6 1 6 2 5 5 No rating
vision of tenant on healthcare
4 6 6 6 7 6 7 6 6 No rating
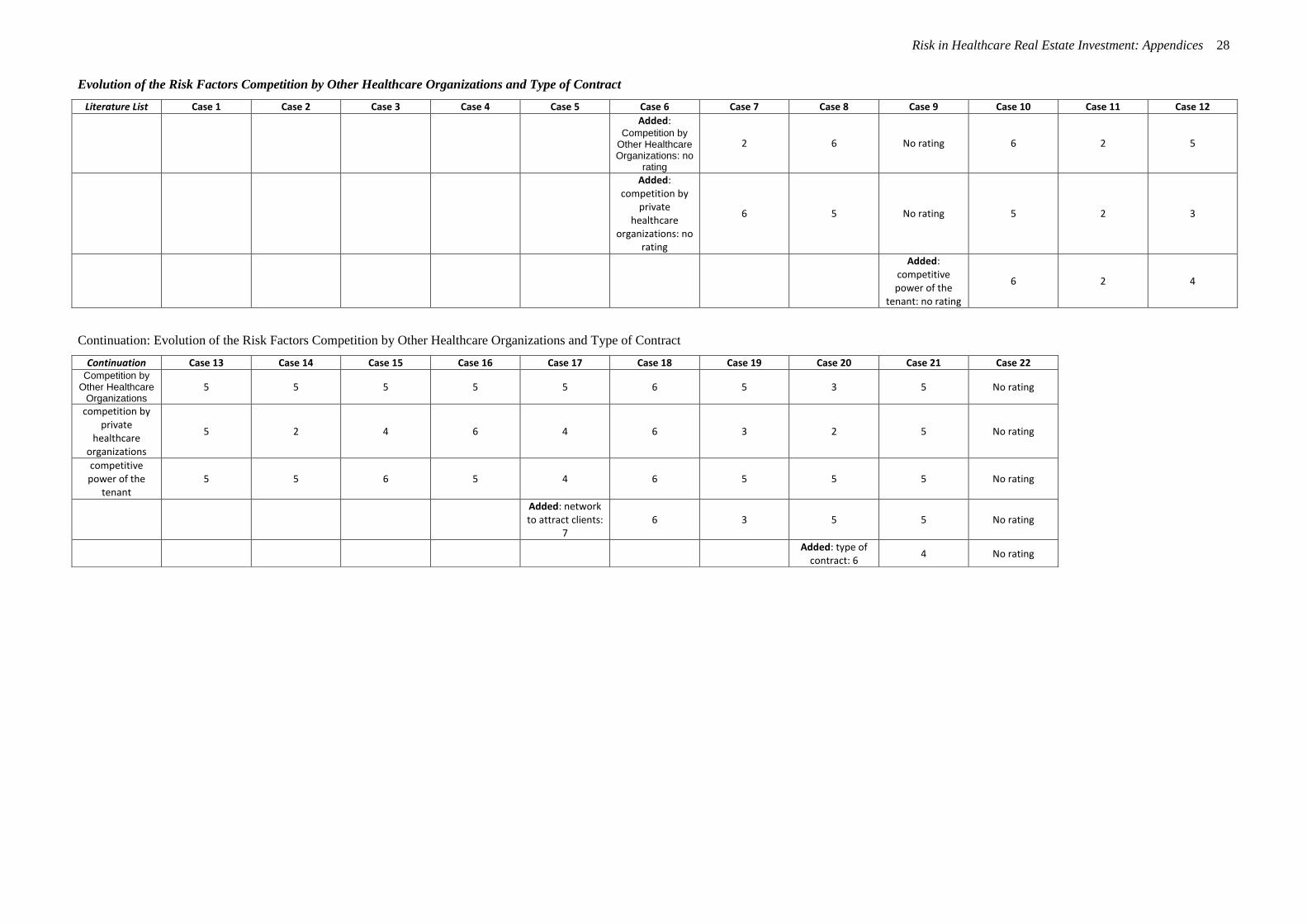
Risk in Healthcare Real Estate Investment: Appendices 28
Evolution of the Risk Factors Competition by Other Healthcare Organizations and Type of Contract
Literature List Case 1 Case 2 Case 3 Case 4 Case 5 Case 6 Case 7 Case 8 Case 9 Case 10 Case 11 Case 12
Added: Competition by
Other Healthcare Organizations: no
rating
2 6 No rating 6 2 5
Added: competition by
private healthcare
organizations: no rating
6 5 No rating 5 2 3
Added: competitive power of the
tenant: no rating
6 2 4
Continuation: Evolution of the Risk Factors Competition by Other Healthcare Organizations and Type of Contract
Continuation Case 13 Case 14 Case 15 Case 16 Case 17 Case 18 Case 19 Case 20 Case 21 Case 22 Competition by
Other Healthcare Organizations
5 5 5 5 5 6 5 3 5 No rating
competition by private
healthcare organizations
5 2 4 6 4 6 3 2 5 No rating
competitive power of the
tenant 5 5 6 5 4 6 5 5 5 No rating
Added: network to attract clients:
7 6 3 5 5 No rating
Added: type of
contract: 6 4 No rating
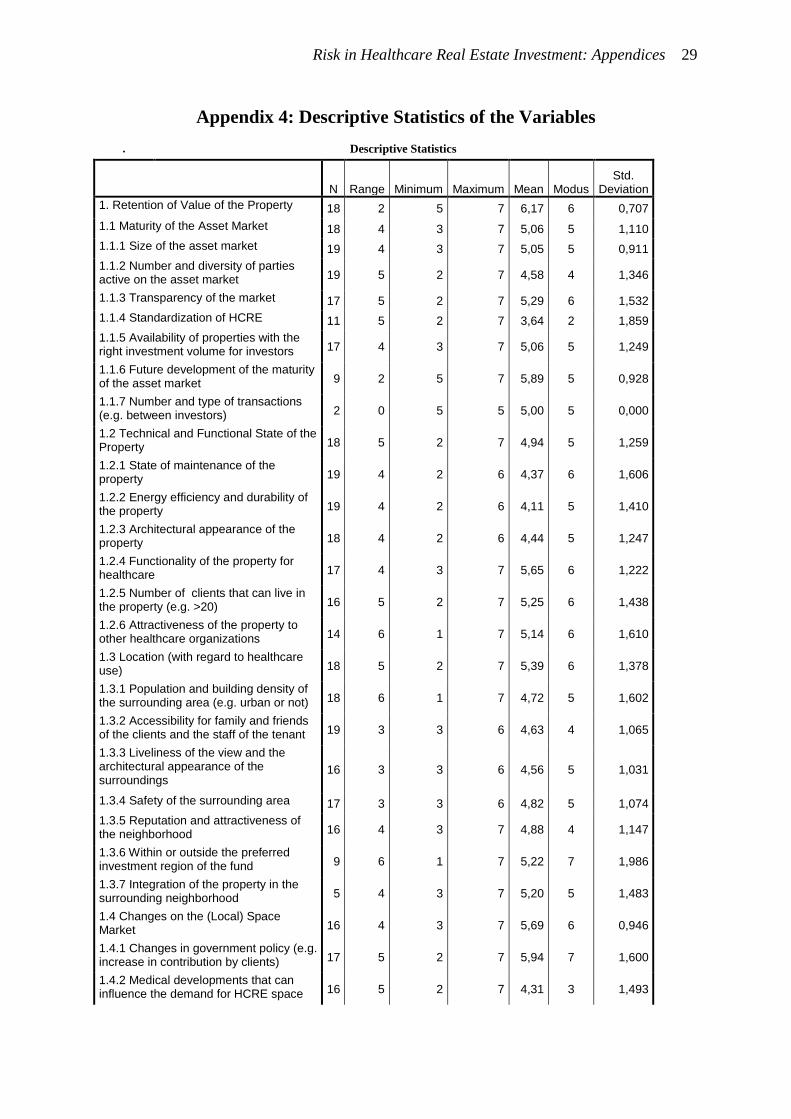
Risk in Healthcare Real Estate Investment: Appendices 29
Appendix 4: Descriptive Statistics of the Variables
. Descriptive Statistics
N Range Minimum Maximum Mean Modus Std.
Deviation
1. Retention of Value of the Property 18 2 5 7 6,17 6 0,707
1.1 Maturity of the Asset Market 18 4 3 7 5,06 5 1,110
1.1.1 Size of the asset market 19 4 3 7 5,05 5 0,911
1.1.2 Number and diversity of parties active on the asset market 19 5 2 7 4,58 4 1,346
1.1.3 Transparency of the market 17 5 2 7 5,29 6 1,532
1.1.4 Standardization of HCRE 11 5 2 7 3,64 2 1,859
1.1.5 Availability of properties with the right investment volume for investors 17 4 3 7 5,06 5 1,249
1.1.6 Future development of the maturity of the asset market 9 2 5 7 5,89 5 0,928
1.1.7 Number and type of transactions (e.g. between investors) 2 0 5 5 5,00 5 0,000
1.2 Technical and Functional State of the Property 18 5 2 7 4,94 5 1,259
1.2.1 State of maintenance of the property 19 4 2 6 4,37 6 1,606
1.2.2 Energy efficiency and durability of the property 19 4 2 6 4,11 5 1,410
1.2.3 Architectural appearance of the property 18 4 2 6 4,44 5 1,247
1.2.4 Functionality of the property for healthcare 17 4 3 7 5,65 6 1,222
1.2.5 Number of clients that can live in the property (e.g. >20) 16 5 2 7 5,25 6 1,438
1.2.6 Attractiveness of the property to other healthcare organizations 14 6 1 7 5,14 6 1,610
1.3 Location (with regard to healthcare use) 18 5 2 7 5,39 6 1,378
1.3.1 Population and building density of the surrounding area (e.g. urban or not) 18 6 1 7 4,72 5 1,602
1.3.2 Accessibility for family and friends of the clients and the staff of the tenant 19 3 3 6 4,63 4 1,065
1.3.3 Liveliness of the view and the architectural appearance of the surroundings
16 3 3 6 4,56 5 1,031
1.3.4 Safety of the surrounding area 17 3 3 6 4,82 5 1,074
1.3.5 Reputation and attractiveness of the neighborhood 16 4 3 7 4,88 4 1,147
1.3.6 Within or outside the preferred investment region of the fund 9 6 1 7 5,22 7 1,986
1.3.7 Integration of the property in the surrounding neighborhood 5 4 3 7 5,20 5 1,483
1.4 Changes on the (Local) Space Market 16 4 3 7 5,69 6 0,946
1.4.1 Changes in government policy (e.g. increase in contribution by clients) 17 5 2 7 5,94 7 1,600
1.4.2 Medical developments that can influence the demand for HCRE space 16 5 2 7 4,31 3 1,493
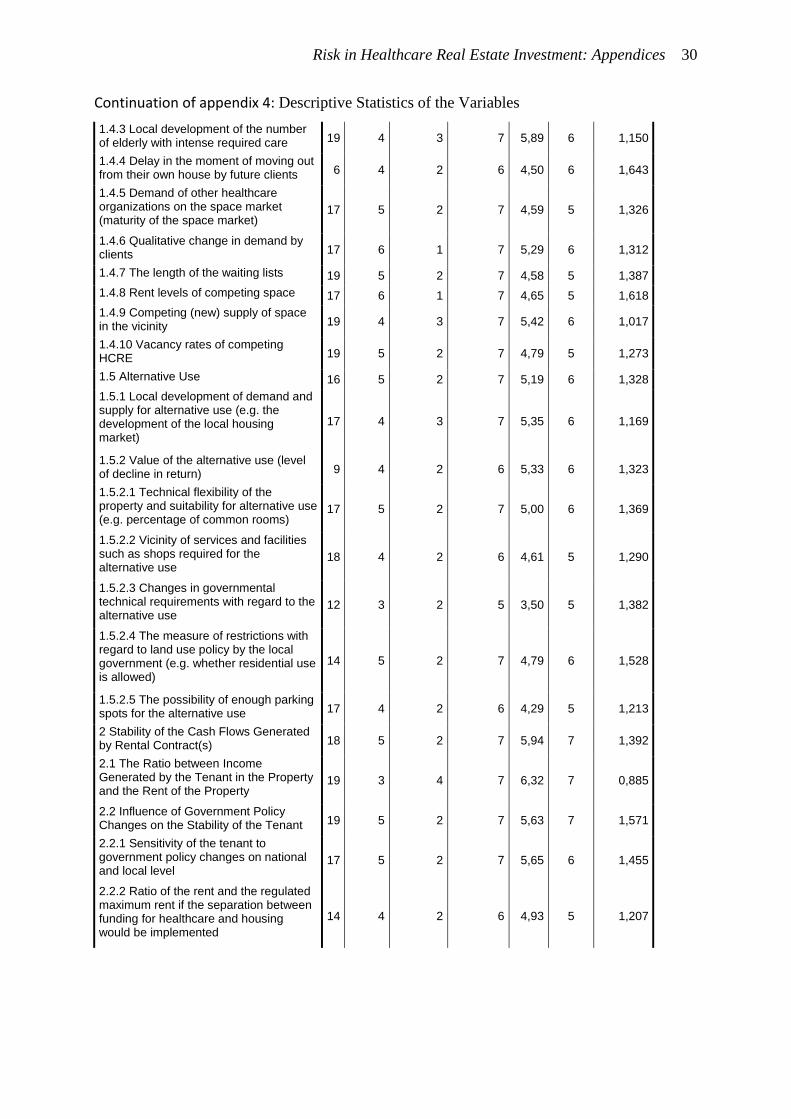
Risk in Healthcare Real Estate Investment: Appendices 30
Continuation of appendix 4: Descriptive Statistics of the Variables
1.4.3 Local development of the number of elderly with intense required care 19 4 3 7 5,89 6 1,150
1.4.4 Delay in the moment of moving out from their own house by future clients 6 4 2 6 4,50 6 1,643
1.4.5 Demand of other healthcare organizations on the space market (maturity of the space market)
17 5 2 7 4,59 5 1,326
1.4.6 Qualitative change in demand by clients 17 6 1 7 5,29 6 1,312
1.4.7 The length of the waiting lists 19 5 2 7 4,58 5 1,387
1.4.8 Rent levels of competing space 17 6 1 7 4,65 5 1,618
1.4.9 Competing (new) supply of space in the vicinity 19 4 3 7 5,42 6 1,017
1.4.10 Vacancy rates of competing HCRE 19 5 2 7 4,79 5 1,273
1.5 Alternative Use 16 5 2 7 5,19 6 1,328
1.5.1 Local development of demand and supply for alternative use (e.g. the development of the local housing market)
17 4 3 7 5,35 6 1,169
1.5.2 Value of the alternative use (level of decline in return) 9 4 2 6 5,33 6 1,323
1.5.2.1 Technical flexibility of the property and suitability for alternative use (e.g. percentage of common rooms)
17 5 2 7 5,00 6 1,369
1.5.2.2 Vicinity of services and facilities such as shops required for the alternative use
18 4 2 6 4,61 5 1,290
1.5.2.3 Changes in governmental technical requirements with regard to the alternative use
12 3 2 5 3,50 5 1,382
1.5.2.4 The measure of restrictions with regard to land use policy by the local government (e.g. whether residential use is allowed)
14 5 2 7 4,79 6 1,528
1.5.2.5 The possibility of enough parking spots for the alternative use 17 4 2 6 4,29 5 1,213
2 Stability of the Cash Flows Generated by Rental Contract(s) 18 5 2 7 5,94 7 1,392
2.1 The Ratio between Income Generated by the Tenant in the Property and the Rent of the Property
19 3 4 7 6,32 7 0,885
2.2 Influence of Government Policy Changes on the Stability of the Tenant 19 5 2 7 5,63 7 1,571
2.2.1 Sensitivity of the tenant to government policy changes on national and local level
17 5 2 7 5,65 6 1,455
2.2.2 Ratio of the rent and the regulated maximum rent if the separation between funding for healthcare and housing would be implemented
14 4 2 6 4,93 5 1,207
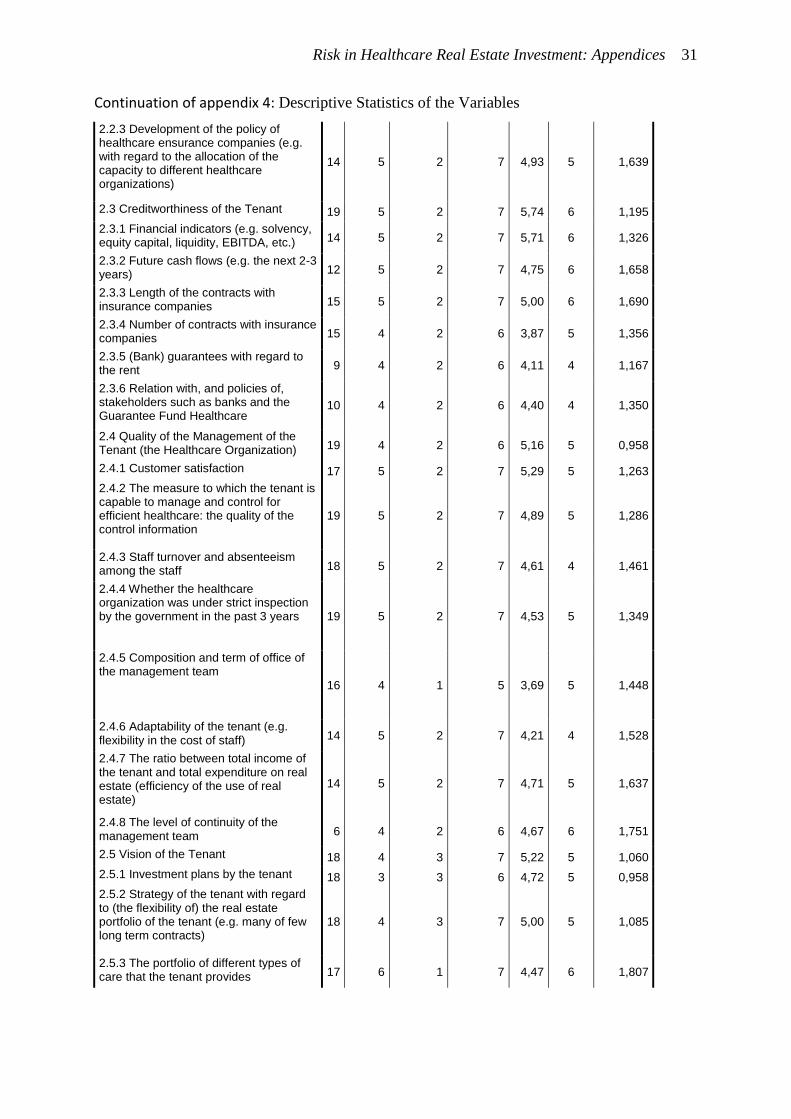
Risk in Healthcare Real Estate Investment: Appendices 31
Continuation of appendix 4: Descriptive Statistics of the Variables
2.2.3 Development of the policy of healthcare ensurance companies (e.g. with regard to the allocation of the capacity to different healthcare organizations)
14 5 2 7 4,93 5 1,639
2.3 Creditworthiness of the Tenant 19 5 2 7 5,74 6 1,195
2.3.1 Financial indicators (e.g. solvency, equity capital, liquidity, EBITDA, etc.) 14 5 2 7 5,71 6 1,326
2.3.2 Future cash flows (e.g. the next 2-3 years) 12 5 2 7 4,75 6 1,658
2.3.3 Length of the contracts with insurance companies 15 5 2 7 5,00 6 1,690
2.3.4 Number of contracts with insurance companies 15 4 2 6 3,87 5 1,356
2.3.5 (Bank) guarantees with regard to the rent 9 4 2 6 4,11 4 1,167
2.3.6 Relation with, and policies of, stakeholders such as banks and the Guarantee Fund Healthcare
10 4 2 6 4,40 4 1,350
2.4 Quality of the Management of the Tenant (the Healthcare Organization) 19 4 2 6 5,16 5 0,958
2.4.1 Customer satisfaction 17 5 2 7 5,29 5 1,263
2.4.2 The measure to which the tenant is capable to manage and control for efficient healthcare: the quality of the control information
19 5 2 7 4,89 5 1,286
2.4.3 Staff turnover and absenteeism among the staff 18 5 2 7 4,61 4 1,461
2.4.4 Whether the healthcare organization was under strict inspection by the government in the past 3 years 19 5 2 7 4,53 5 1,349
2.4.5 Composition and term of office of the management team
16 4 1 5 3,69 5 1,448
2.4.6 Adaptability of the tenant (e.g. flexibility in the cost of staff) 14 5 2 7 4,21 4 1,528
2.4.7 The ratio between total income of the tenant and total expenditure on real estate (efficiency of the use of real estate)
14 5 2 7 4,71 5 1,637
2.4.8 The level of continuity of the management team 6 4 2 6 4,67 6 1,751
2.5 Vision of the Tenant 18 4 3 7 5,22 5 1,060
2.5.1 Investment plans by the tenant 18 3 3 6 4,72 5 0,958
2.5.2 Strategy of the tenant with regard to (the flexibility of) the real estate portfolio of the tenant (e.g. many of few long term contracts)
18 4 3 7 5,00 5 1,085
2.5.3 The portfolio of different types of care that the tenant provides 17 6 1 7 4,47 6 1,807
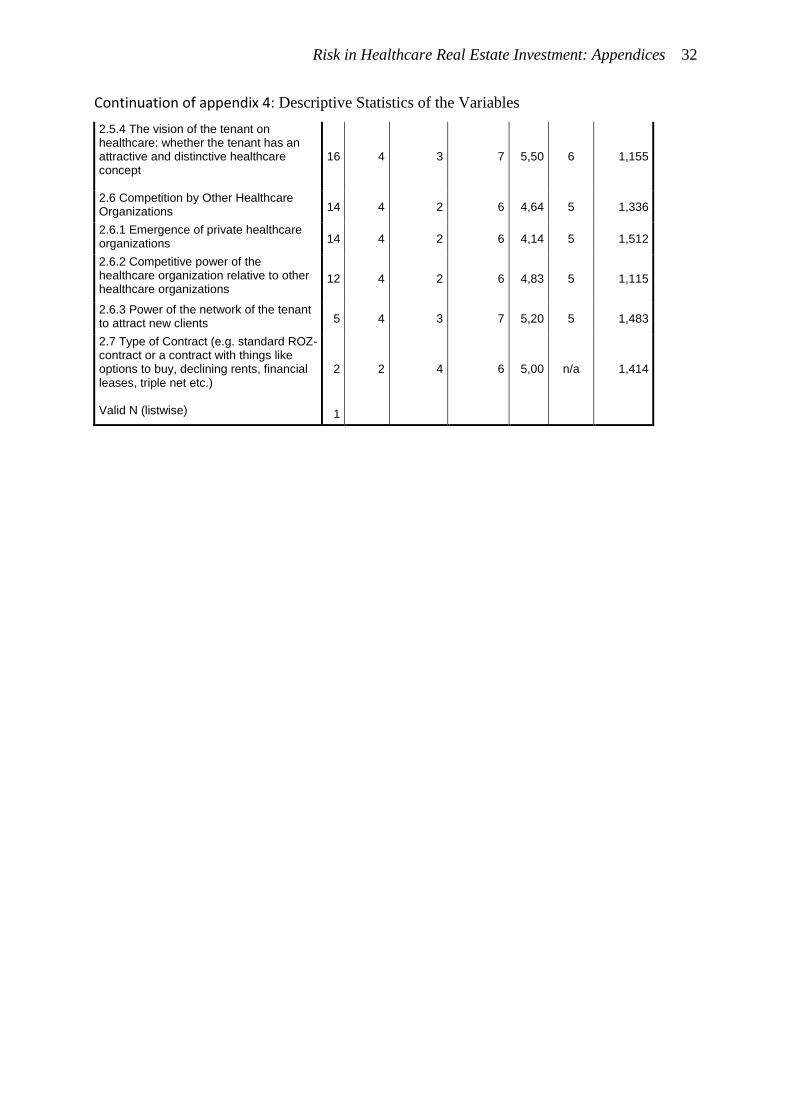
Risk in Healthcare Real Estate Investment: Appendices 32
Continuation of appendix 4: Descriptive Statistics of the Variables
2.5.4 The vision of the tenant on healthcare: whether the tenant has an attractive and distinctive healthcare concept
16 4 3 7 5,50 6 1,155
2.6 Competition by Other Healthcare Organizations 14 4 2 6 4,64 5 1,336
2.6.1 Emergence of private healthcare organizations 14 4 2 6 4,14 5 1,512
2.6.2 Competitive power of the healthcare organization relative to other healthcare organizations
12 4 2 6 4,83 5 1,115
2.6.3 Power of the network of the tenant to attract new clients 5 4 3 7 5,20 5 1,483
2.7 Type of Contract (e.g. standard ROZ-contract or a contract with things like options to buy, declining rents, financial leases, triple net etc.)
2 2 4 6 5,00 n/a 1,414
Valid N (listwise) 1
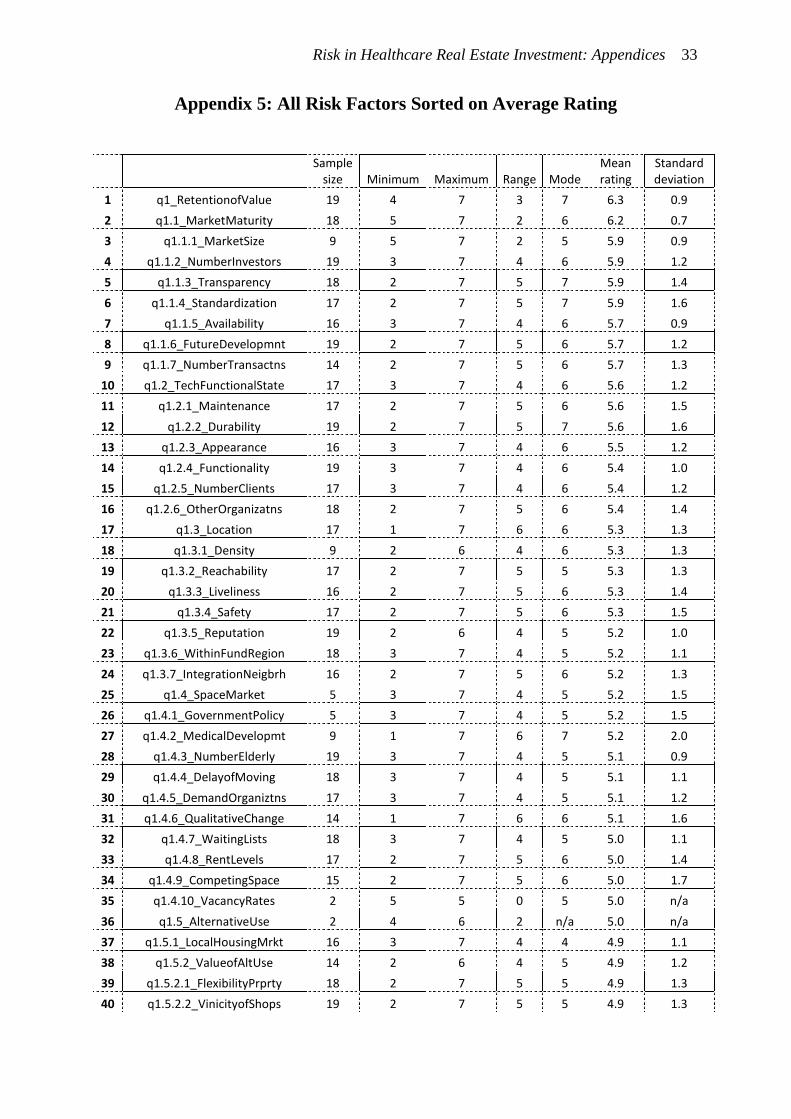
Risk in Healthcare Real Estate Investment: Appendices 33
Appendix 5: All Risk Factors Sorted on Average Rating
Sample size Minimum Maximum Range Mode
Mean rating
Standard deviation
1 q1_RetentionofValue 19 4 7 3 7 6.3 0.9
2 q1.1_MarketMaturity 18 5 7 2 6 6.2 0.7
3 q1.1.1_MarketSize 9 5 7 2 5 5.9 0.9
4 q1.1.2_NumberInvestors 19 3 7 4 6 5.9 1.2
5 q1.1.3_Transparency 18 2 7 5 7 5.9 1.4
6 q1.1.4_Standardization 17 2 7 5 7 5.9 1.6
7 q1.1.5_Availability 16 3 7 4 6 5.7 0.9
8 q1.1.6_FutureDevelopmnt 19 2 7 5 6 5.7 1.2
9 q1.1.7_NumberTransactns 14 2 7 5 6 5.7 1.3
10 q1.2_TechFunctionalState 17 3 7 4 6 5.6 1.2
11 q1.2.1_Maintenance 17 2 7 5 6 5.6 1.5
12 q1.2.2_Durability 19 2 7 5 7 5.6 1.6
13 q1.2.3_Appearance 16 3 7 4 6 5.5 1.2
14 q1.2.4_Functionality 19 3 7 4 6 5.4 1.0
15 q1.2.5_NumberClients 17 3 7 4 6 5.4 1.2
16 q1.2.6_OtherOrganizatns 18 2 7 5 6 5.4 1.4
17 q1.3_Location 17 1 7 6 6 5.3 1.3
18 q1.3.1_Density 9 2 6 4 6 5.3 1.3
19 q1.3.2_Reachability 17 2 7 5 5 5.3 1.3
20 q1.3.3_Liveliness 16 2 7 5 6 5.3 1.4
21 q1.3.4_Safety 17 2 7 5 6 5.3 1.5
22 q1.3.5_Reputation 19 2 6 4 5 5.2 1.0
23 q1.3.6_WithinFundRegion 18 3 7 4 5 5.2 1.1
24 q1.3.7_IntegrationNeigbrh 16 2 7 5 6 5.2 1.3
25 q1.4_SpaceMarket 5 3 7 4 5 5.2 1.5
26 q1.4.1_GovernmentPolicy 5 3 7 4 5 5.2 1.5
27 q1.4.2_MedicalDevelopmt 9 1 7 6 7 5.2 2.0
28 q1.4.3_NumberElderly 19 3 7 4 5 5.1 0.9
29 q1.4.4_DelayofMoving 18 3 7 4 5 5.1 1.1
30 q1.4.5_DemandOrganiztns 17 3 7 4 5 5.1 1.2
31 q1.4.6_QualitativeChange 14 1 7 6 6 5.1 1.6
32 q1.4.7_WaitingLists 18 3 7 4 5 5.0 1.1
33 q1.4.8_RentLevels 17 2 7 5 6 5.0 1.4
34 q1.4.9_CompetingSpace 15 2 7 5 6 5.0 1.7
35 q1.4.10_VacancyRates 2 5 5 0 5 5.0 n/a
36 q1.5_AlternativeUse 2 4 6 2 n/a 5.0 n/a
37 q1.5.1_LocalHousingMrkt 16 3 7 4 4 4.9 1.1
38 q1.5.2_ValueofAltUse 14 2 6 4 5 4.9 1.2
39 q1.5.2.1_FlexibilityPrprty 18 2 7 5 5 4.9 1.3
40 q1.5.2.2_VinicityofShops 19 2 7 5 5 4.9 1.3
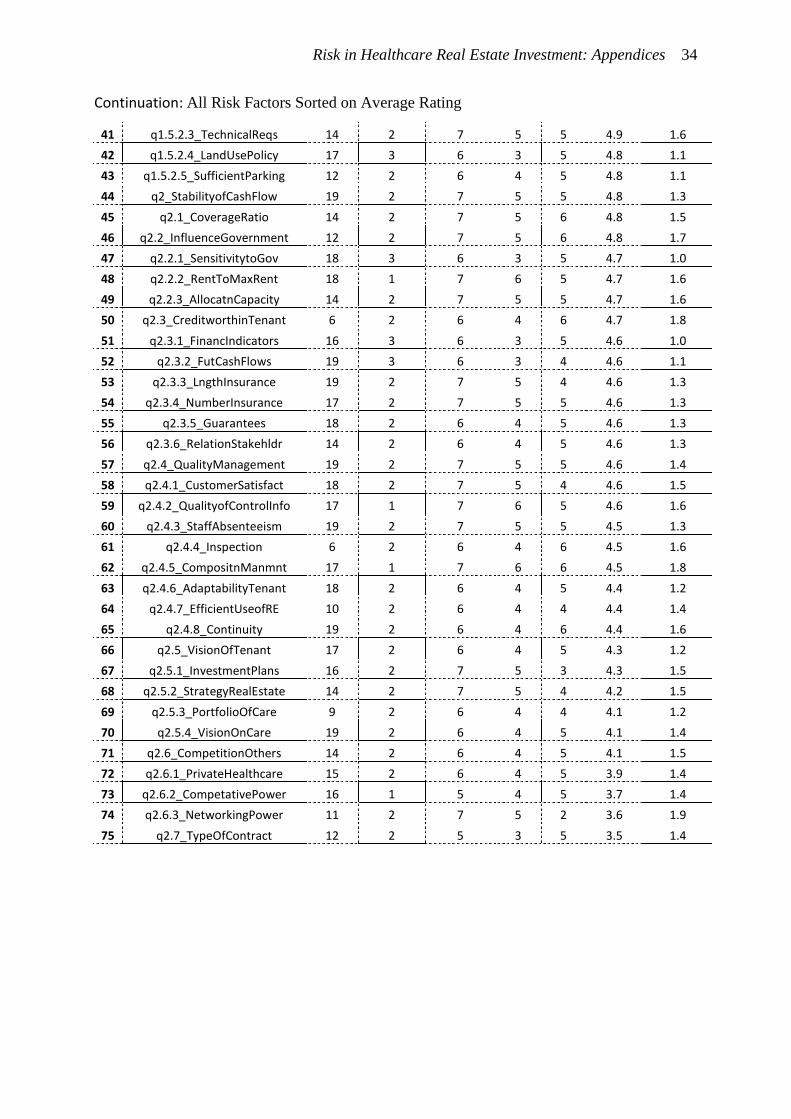
Risk in Healthcare Real Estate Investment: Appendices 34
Continuation: All Risk Factors Sorted on Average Rating
41 q1.5.2.3_TechnicalReqs 14 2 7 5 5 4.9 1.6
42 q1.5.2.4_LandUsePolicy 17 3 6 3 5 4.8 1.1
43 q1.5.2.5_SufficientParking 12 2 6 4 5 4.8 1.1
44 q2_StabilityofCashFlow 19 2 7 5 5 4.8 1.3
45 q2.1_CoverageRatio 14 2 7 5 6 4.8 1.5
46 q2.2_InfluenceGovernment 12 2 7 5 6 4.8 1.7
47 q2.2.1_SensitivitytoGov 18 3 6 3 5 4.7 1.0
48 q2.2.2_RentToMaxRent 18 1 7 6 5 4.7 1.6
49 q2.2.3_AllocatnCapacity 14 2 7 5 5 4.7 1.6
50 q2.3_CreditworthinTenant 6 2 6 4 6 4.7 1.8
51 q2.3.1_FinancIndicators 16 3 6 3 5 4.6 1.0
52 q2.3.2_FutCashFlows 19 3 6 3 4 4.6 1.1
53 q2.3.3_LngthInsurance 19 2 7 5 4 4.6 1.3
54 q2.3.4_NumberInsurance 17 2 7 5 5 4.6 1.3
55 q2.3.5_Guarantees 18 2 6 4 5 4.6 1.3
56 q2.3.6_RelationStakehldr 14 2 6 4 5 4.6 1.3
57 q2.4_QualityManagement 19 2 7 5 5 4.6 1.4
58 q2.4.1_CustomerSatisfact 18 2 7 5 4 4.6 1.5
59 q2.4.2_QualityofControlInfo 17 1 7 6 5 4.6 1.6
60 q2.4.3_StaffAbsenteeism 19 2 7 5 5 4.5 1.3
61 q2.4.4_Inspection 6 2 6 4 6 4.5 1.6
62 q2.4.5_CompositnManmnt 17 1 7 6 6 4.5 1.8
63 q2.4.6_AdaptabilityTenant 18 2 6 4 5 4.4 1.2
64 q2.4.7_EfficientUseofRE 10 2 6 4 4 4.4 1.4
65 q2.4.8_Continuity 19 2 6 4 6 4.4 1.6
66 q2.5_VisionOfTenant 17 2 6 4 5 4.3 1.2
67 q2.5.1_InvestmentPlans 16 2 7 5 3 4.3 1.5
68 q2.5.2_StrategyRealEstate 14 2 7 5 4 4.2 1.5
69 q2.5.3_PortfolioOfCare 9 2 6 4 4 4.1 1.2
70 q2.5.4_VisionOnCare 19 2 6 4 5 4.1 1.4
71 q2.6_CompetitionOthers 14 2 6 4 5 4.1 1.5
72 q2.6.1_PrivateHealthcare 15 2 6 4 5 3.9 1.4
73 q2.6.2_CompetativePower 16 1 5 4 5 3.7 1.4
74 q2.6.3_NetworkingPower 11 2 7 5 2 3.6 1.9
75 q2.7_TypeOfContract 12 2 5 3 5 3.5 1.4
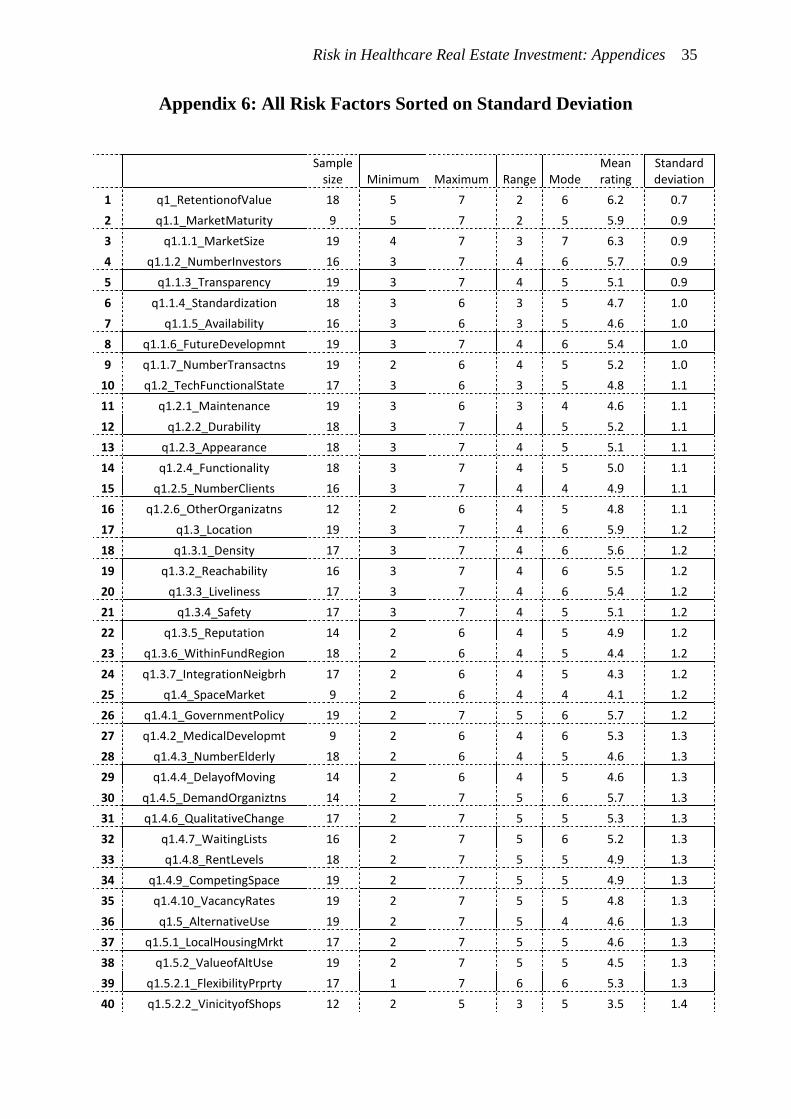
Risk in Healthcare Real Estate Investment: Appendices 35
Appendix 6: All Risk Factors Sorted on Standard Deviation
Sample size Minimum Maximum Range Mode
Mean rating
Standard deviation
1 q1_RetentionofValue 18 5 7 2 6 6.2 0.7
2 q1.1_MarketMaturity 9 5 7 2 5 5.9 0.9
3 q1.1.1_MarketSize 19 4 7 3 7 6.3 0.9
4 q1.1.2_NumberInvestors 16 3 7 4 6 5.7 0.9
5 q1.1.3_Transparency 19 3 7 4 5 5.1 0.9
6 q1.1.4_Standardization 18 3 6 3 5 4.7 1.0
7 q1.1.5_Availability 16 3 6 3 5 4.6 1.0
8 q1.1.6_FutureDevelopmnt 19 3 7 4 6 5.4 1.0
9 q1.1.7_NumberTransactns 19 2 6 4 5 5.2 1.0
10 q1.2_TechFunctionalState 17 3 6 3 5 4.8 1.1
11 q1.2.1_Maintenance 19 3 6 3 4 4.6 1.1
12 q1.2.2_Durability 18 3 7 4 5 5.2 1.1
13 q1.2.3_Appearance 18 3 7 4 5 5.1 1.1
14 q1.2.4_Functionality 18 3 7 4 5 5.0 1.1
15 q1.2.5_NumberClients 16 3 7 4 4 4.9 1.1
16 q1.2.6_OtherOrganizatns 12 2 6 4 5 4.8 1.1
17 q1.3_Location 19 3 7 4 6 5.9 1.2
18 q1.3.1_Density 17 3 7 4 6 5.6 1.2
19 q1.3.2_Reachability 16 3 7 4 6 5.5 1.2
20 q1.3.3_Liveliness 17 3 7 4 6 5.4 1.2
21 q1.3.4_Safety 17 3 7 4 5 5.1 1.2
22 q1.3.5_Reputation 14 2 6 4 5 4.9 1.2
23 q1.3.6_WithinFundRegion 18 2 6 4 5 4.4 1.2
24 q1.3.7_IntegrationNeigbrh 17 2 6 4 5 4.3 1.2
25 q1.4_SpaceMarket 9 2 6 4 4 4.1 1.2
26 q1.4.1_GovernmentPolicy 19 2 7 5 6 5.7 1.2
27 q1.4.2_MedicalDevelopmt 9 2 6 4 6 5.3 1.3
28 q1.4.3_NumberElderly 18 2 6 4 5 4.6 1.3
29 q1.4.4_DelayofMoving 14 2 6 4 5 4.6 1.3
30 q1.4.5_DemandOrganiztns 14 2 7 5 6 5.7 1.3
31 q1.4.6_QualitativeChange 17 2 7 5 5 5.3 1.3
32 q1.4.7_WaitingLists 16 2 7 5 6 5.2 1.3
33 q1.4.8_RentLevels 18 2 7 5 5 4.9 1.3
34 q1.4.9_CompetingSpace 19 2 7 5 5 4.9 1.3
35 q1.4.10_VacancyRates 19 2 7 5 5 4.8 1.3
36 q1.5_AlternativeUse 19 2 7 5 4 4.6 1.3
37 q1.5.1_LocalHousingMrkt 17 2 7 5 5 4.6 1.3
38 q1.5.2_ValueofAltUse 19 2 7 5 5 4.5 1.3
39 q1.5.2.1_FlexibilityPrprty 17 1 7 6 6 5.3 1.3
40 q1.5.2.2_VinicityofShops 12 2 5 3 5 3.5 1.4
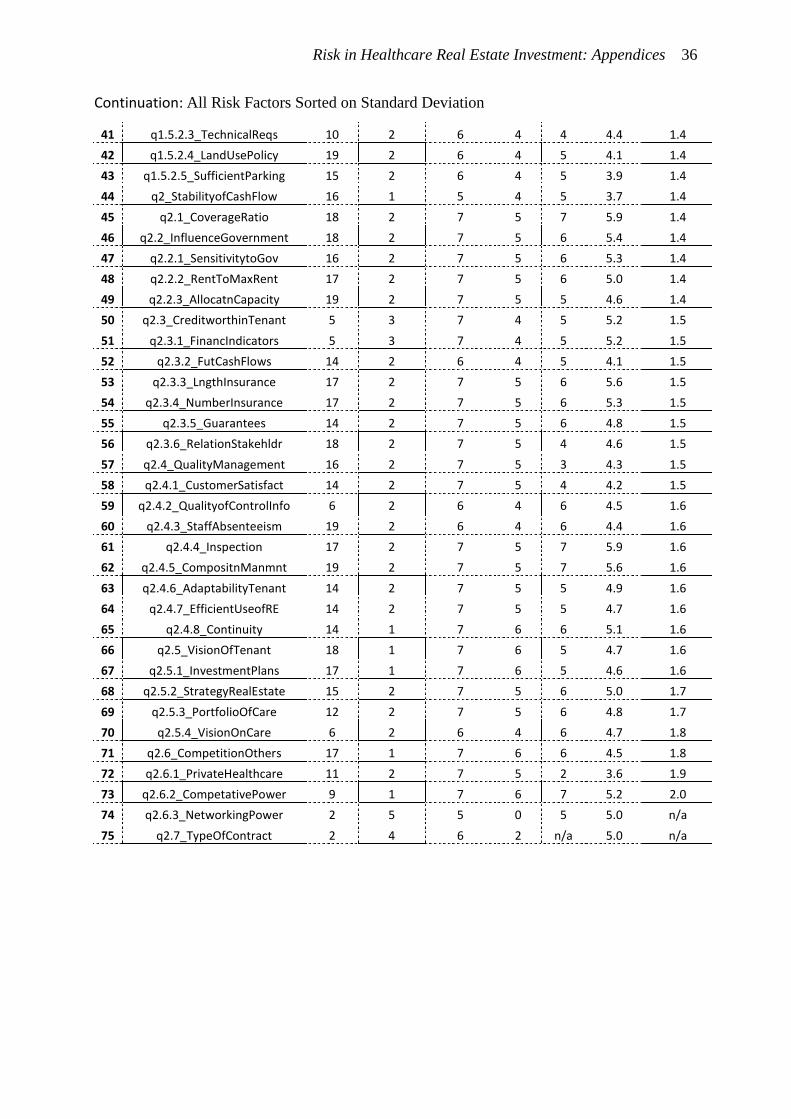
Risk in Healthcare Real Estate Investment: Appendices 36
Continuation: All Risk Factors Sorted on Standard Deviation
41 q1.5.2.3_TechnicalReqs 10 2 6 4 4 4.4 1.4
42 q1.5.2.4_LandUsePolicy 19 2 6 4 5 4.1 1.4
43 q1.5.2.5_SufficientParking 15 2 6 4 5 3.9 1.4
44 q2_StabilityofCashFlow 16 1 5 4 5 3.7 1.4
45 q2.1_CoverageRatio 18 2 7 5 7 5.9 1.4
46 q2.2_InfluenceGovernment 18 2 7 5 6 5.4 1.4
47 q2.2.1_SensitivitytoGov 16 2 7 5 6 5.3 1.4
48 q2.2.2_RentToMaxRent 17 2 7 5 6 5.0 1.4
49 q2.2.3_AllocatnCapacity 19 2 7 5 5 4.6 1.4
50 q2.3_CreditworthinTenant 5 3 7 4 5 5.2 1.5
51 q2.3.1_FinancIndicators 5 3 7 4 5 5.2 1.5
52 q2.3.2_FutCashFlows 14 2 6 4 5 4.1 1.5
53 q2.3.3_LngthInsurance 17 2 7 5 6 5.6 1.5
54 q2.3.4_NumberInsurance 17 2 7 5 6 5.3 1.5
55 q2.3.5_Guarantees 14 2 7 5 6 4.8 1.5
56 q2.3.6_RelationStakehldr 18 2 7 5 4 4.6 1.5
57 q2.4_QualityManagement 16 2 7 5 3 4.3 1.5
58 q2.4.1_CustomerSatisfact 14 2 7 5 4 4.2 1.5
59 q2.4.2_QualityofControlInfo 6 2 6 4 6 4.5 1.6
60 q2.4.3_StaffAbsenteeism 19 2 6 4 6 4.4 1.6
61 q2.4.4_Inspection 17 2 7 5 7 5.9 1.6
62 q2.4.5_CompositnManmnt 19 2 7 5 7 5.6 1.6
63 q2.4.6_AdaptabilityTenant 14 2 7 5 5 4.9 1.6
64 q2.4.7_EfficientUseofRE 14 2 7 5 5 4.7 1.6
65 q2.4.8_Continuity 14 1 7 6 6 5.1 1.6
66 q2.5_VisionOfTenant 18 1 7 6 5 4.7 1.6
67 q2.5.1_InvestmentPlans 17 1 7 6 5 4.6 1.6
68 q2.5.2_StrategyRealEstate 15 2 7 5 6 5.0 1.7
69 q2.5.3_PortfolioOfCare 12 2 7 5 6 4.8 1.7
70 q2.5.4_VisionOnCare 6 2 6 4 6 4.7 1.8
71 q2.6_CompetitionOthers 17 1 7 6 6 4.5 1.8
72 q2.6.1_PrivateHealthcare 11 2 7 5 2 3.6 1.9
73 q2.6.2_CompetativePower 9 1 7 6 7 5.2 2.0
74 q2.6.3_NetworkingPower 2 5 5 0 5 5.0 n/a
75 q2.7_TypeOfContract 2 4 6 2 n/a 5.0 n/a





























