Embed Size (px)
Citation preview
ORIGINAL ARTICLES
Effects of secular trends in obesity on coronary risk factors in children: The Bogalusa Heart Study
Samuel Sl Gidding, MD, Weihang Bao, PhD, Sathanur R, Srinivasan, PhD, and Gerald S, Berenson, MD
From the Departments of Pediatrics and Preventive Medicine, Northwestern University Medical School, Chicago, Illinois, and the Department of Applied Health Sciences, Tulane Center for Cardiovascular Health, Tulane University Medical Center, New Orleans, Louisiana
Objective: To determine whether a secular trend toward increased weight gain was present in children examined 11 years apart in the Bogaiusa Heart Study and, if present, the association of this trend with the cardiovascular risk status of the children. Study design: Two biracial cohorts (approximately 65% white, 35% black) were identified. One cohort was examined first in 1973 at 7 to 9 years of age and was reexamined in 1981 (n = 417). The second was examined first in 1984 at the same age and reexamined in 1992 (n = 235). Measurements made at each assessment included age, gender, race, height, weight, blood pressure, and lipoproteins. The two cohorts were then compared. Results: The two cohorts were comparable at their first assessment. However, at follow-up 8 years later the more recent cohort was 5 to 7 kg heavier without any difference in linear growth; this increased ponderosity was associated with adverse changes in lipids and lipoproteins: the high-density lipoprotein-choles- terol concentration was 0.15 to 0.35 mmol/L (6 to 13 mg/dl) lower, triglyceride values were 0.09 to 0.40 mmol/L (8 to 36 mg/dl) higher, and there were small in- creases in total cholesterol and low-density lipoprotein-cholesterol concentra- tions in white girls. Multivariate analyses showed that in the more recent cohort these changes were related more to a change in ponderosity than to ponderos- ity. Although blood pressure was generally lower in the recent cohort, increasing ponderosity was associated with higher blood pressure. Conclusions: There is a secular trend toward increased ponderosity in children examined in the Bogalusa Heart Study. This trend is associated with worsening cardiovascular risk, particularly with regard to lipoproteins. (J PEDIATR 1995;127: 868-74)
The development of obesity in childhood is a major deter-
minant of the acquisition of cardiovascular risk later in
Supported by grants from the National Heart, Lung, and Blood In- stitute of the U.S. Public Health Service (HL-38844). Submitted for publication March 1, 1995; accepted July 24, 1995.
Reprint requests: Gerald S. Berenson, MD, Tulane Center for Car- diovascular Health, Tulane School of Public Health and Tropical Medicine, 1501 Canal St., 14th Floor, New Orleans, LA 70112- 2824. Copyright © 1995 Mosby-Year Book, Inc. 0022-3476/95/55.00 + 0 9120168050
life. 1-6 Children who become more obese are more likely to
have elevated blood pressure, elevated concentrations of
low-density lipoprotein--cholesterol and triglycerides, and
I HDL-C High-density lipoprotein-cholesterol ] LDL-C Low-density lipoprotein--cholesterol [
decreased concentrations of high-density lipoprotein-cho-
lesterol as adolescents and young adults. Being overweight as a child is highly predictive of being overweight as an adult. 5
8 6 8
The Journal of Pediatrics Gidding et al. 8 6 9 Volume 127, Number 6
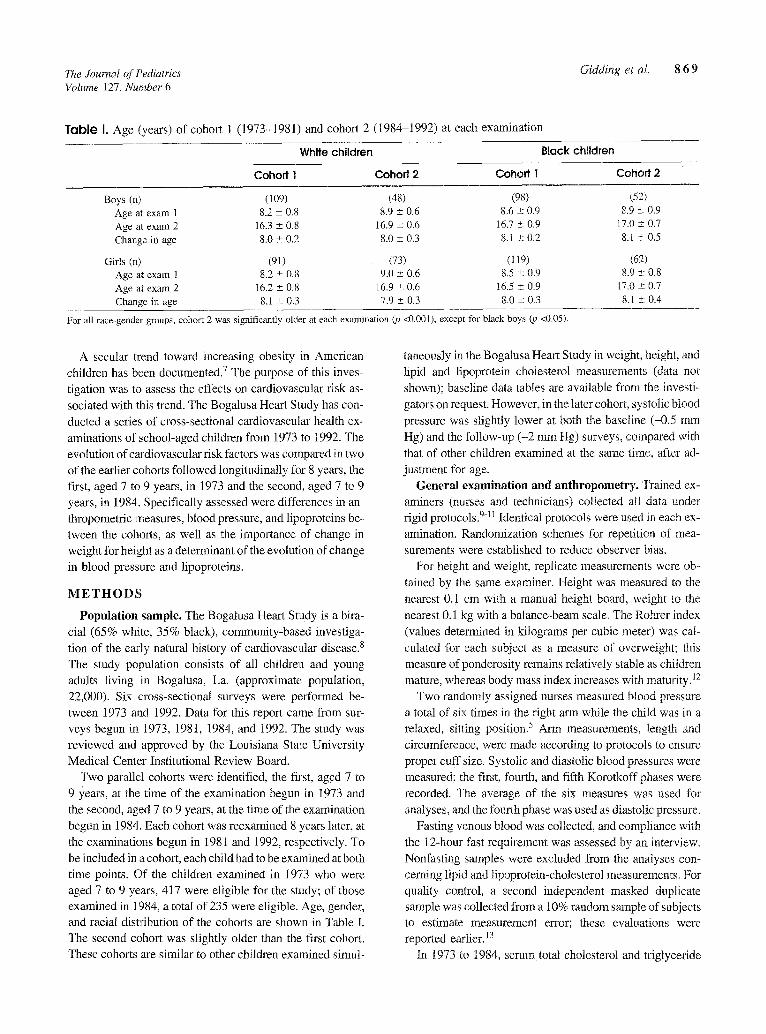
Table I. Age (years) of cohort 1 (1973-1981) and cohort 2 (1984-1992) at each examination
White children Black children
Cohort 1 Cohort 2 Cohort 1 Cohor t 2
Boys (n) (109) (48) (98) (52) Age at exam 1 8.2 _+ 0.8 8.9 ± 0.6 8.6 ± 0.9 8.9 ± 0.9 Age at exam 2 16.3 ± 0.8 16.9 ± 0.6 16.7 ± 0.9 17.0 ± 0.7 Change in age 8.0 -+ 0.2 8.0 ± 0.3 8.I ± 0.2 8.1 ± 0.5
Girls (n) (91) (73) (119) (62) Age at exam 1 8.2 ± 0.8 9.0 ± 0.6 8.5 ± 0.9 8.9 +-- 0.8 Age at exam 2 16.2 ± 0.8 16.9 ± 0.6 16.5 ± 0.9 17.0 ± 0.7 Change in age 8.1 _+ 0.3 7.9 + 0.3 8.0 ± 0.3 8.l ± 0.4
For all race-gender groups, cohort 2 was significantly older at each examination (p
A secular trend toward increasing obesity in American children has been documented] The purpose of this inves-
tigation was to assess the effects on cardiovascular risk as-
sociated with this trend. The Bogalusa Heart Study has con-
ducted a series of cross-sectional cardiovascular health ex-
aminations of school-aged children from 1973 to 1992. The
evolution of cardiovascular risk factors was compared in two
of the earlier cohorts followed longitudinally for 8 years, the first, aged 7 to 9 years, in 1973 and the second, aged 7 to 9 years, in 1984. Specifically assessed were differences in an-
thropometric measures, blood pressure, and lipoproteins be- tween the cohorts, as well as the importance of change in
weight for height as a determinant of the evolution of change
in blood pressure and lipoproteins.
M E T H O D S
Population sample. The Bogalusa Heart Study is a bira- cial (65% white, 35% black), community-based investiga-
tion of the early natural history of cardiovascular disease, s
The study population consists of all children and young adults living in Bogalusa, La. (approximate population,
22,000). Six cross-sectional surveys were performed be-
tween 1973 and 1992. Data for this report came from sur- veys begun in 1973, 1981, 1984, and 1992. The study was reviewed and approved by the Louisiana Starve University
Medical Center Institutional Review Board. Two parallel cohorts were identified, the first, aged 7 to
9 years, at the time of the examination begun in 1973 and
the second, aged 7 to 9 years, at the time of the examination
begun in 1984. Each cohort was reexamined 8 years later, at
the examinations begun in 1981 and 1992, respectively. To
be included in a cohort, each child had to be exmnined at both time points. Of the children examined in 1973 who were
aged 7 to 9 years, 417 were eligible for the study; of those examined in 1984, a total of 235 were eligible. Age, gender, and racial distribution of the cohorts are shown in Table I. The second cohort was slightly older than the first cohort.
These cohorts are similar to other children examined simul-
<0.001), except for black boys (p <0.05).
taneously in the Bogahisa Heart Study in weight, height, and lipid and lipoprotein cholesterol measurements (data not
shown); baseline data tables are available from the investi-
gators on request. However, in the later cohort, systolic blood
pressure was slightly lower at both the baseline (-0.5 rnm
Hg) and the follow-up (-2 mm Hg) surveys, compared with
that of other children examined at the same time, after ad-
justment for age. General examination and anthropometry. Trained ex-
aminers (nurses and technicians) collected al~ data under rigid protocols. 9-[1 Identical protocols were used in each ex-
amination. Randomization schemes for repetition of mea-
surements were established to reduce observer bias.
For height and weight, replicate measurements were ob-
tained by the same examiner. Height was measured to the
nearest 0.1 cm with a manual height board, weight m the
nearest 0.1 kg with a balance-beam scale. The Rohrer index
(values determined in kilograms per cubic meter) was cal-
culated for each subject as a measure of overweight; this measure of ponderosity remains relatively stable as children
mature, whereas body mass index increases with maturity.~2
Two randomly assigned nurses measured blood pressure a total of six times in the right arm while the child was in a relaxed, sitting position. 5 Arm measurements, length and
circumference, were made according to protocols to ensure proper cuff size. Systolic and diastolic blood pressures were
measured; the first, fourth, and fifth Korotkoff phases were
recorded. The average of the six measures was used for
analyses, and the fourth phase was used as diastolic pressure.
Fasting venous blood was collected, and compliance with
the 12-hour fast requirement was assessed by an interview.
Nonfasting samples were excluded from the analyses con-
cerning lipid and lipoprotein-cholesterol measurements. For quality control, a second independent masked duplicate sample was collected from a 10% random sample of subjects to estimate measurement error; these evaluations were reported earlier. 13
In 1973 to 1984, serum total cholesterol and triglyceride
8 7 0 Gidding et al. The Journal of Pediatrics December 1995
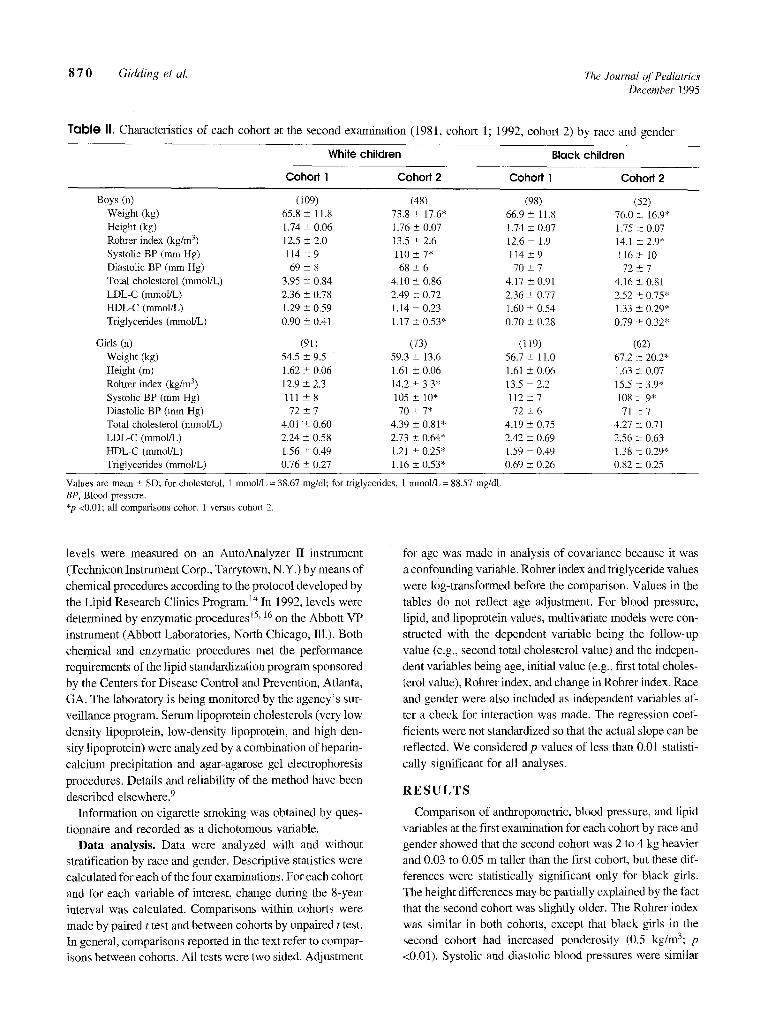
T a b l e II. Characteristics of each cohort at the second examination (1981, cohort 1; 1992, cohort 2) by race and gender
White children Black children
Coho~l Cohofl2 Cohofll Cohod 2
Boys (n) (109) (48) (98) Weight (kg) 65.8 ÷ 11.8 73.8 ± 17.6" 66.9 ± 11.8 Height (kg) 1.74 _+ 0.06 1.76 ± 0.07 1.74 ± 0.07 Rohrer index (kg/m 3) 12.5 ± 2.0 13.5 ± 2.6 12.6 ± 1.9 Systolic BP (mm Hg) 114 ± 9 110 ± 7* 114 ± 9 Diastolic BP (ram Hg) 69 ± 8 68 ± 6 70 ± 7 Total cholesterol (mmol/L) 3.95 ± 0.84 4.10 _+ 0.86 4.17 ± 0.91 LDL-C (mmol/L) 2.36 ± 0.78 2.49 ± 0.72 2.36 -+ 0.77 HDL-C (retool/L) 1.29 ± 0.59 1.14 ± 0.23 1.60 ± 0.54 Tfiglycerides (mmol/L) 0.90 -+ 0.41 1.17 + 0.53* 0.70 ± 0.28
Girls (n) (9l) (73) (119) Weight (kg) 54.5 ± 9.5 59.3 -+ 13.6 56.7 ± 11.0 Height (m) 1.62 ± 0.06 1.61 _+ 0.06 1.61 ± 0.06 Rohrer index (kg/m 3) 12.9 +- 2.3 14.2 ± 3.3* 13.5 ± 2.2 Systolic BP (ram Hg) I l l ± 8 105 ± 10" 112 _+ 7 Diastolic BP (ram Hg) 72 + 7 70 ± 7* 72 ± 6 Total cholesterol (retool/L) 4.01 ± 0.60 4.39 ± 0.81" 4.19 ± 0.75 LDL-C (mmol/L) 2.24 ÷ 0.58 2.73 ± 0.64* 2.42 ± 0.69 HDL-C (mmol/L) 1.56 ± 0.49 1.21 _+ 0.25* 1.59 ± 0.49 Triglycerides (mmol/L) 0.76 ± 0.27 1.16 _+ 0.53* 0.69 ± 0.26
(52) 76.0 ± 16.9" 1.75 ± 0.07 14.1 ± 2.9* 116 ± 10 7 2 ± 7
4.16 ± 0.81 2.52 ± 0.75* 1.33 ± 0.29* 0.79 ± 0.32*
(62) 67.2 ± 20.2* 1.63 ± 0.07 i5.5 +_ 3.9* 108 ± 9* 71 ±7
4.27 ± 0.71 2.56 ~- 0.63 1.38 --- 0.29* 0.82 ± 0.25
Values are mean _+ SD; for cholesterol, 1 mmol/L = 38.67 mg/dl; for triglycerides, 1 mmol/L = 88.57 mg/dl. BP, Blood pressure. *p <0.01; all comparisons cohort 1 versus cohort 2.
levels were measured on an AutoAnalyzer 1I instrument
(Technicon Instrument Corp., Tarrytown, N.Y.) by means of
chemical procedures according to the protocol developed by
the Lipid Research Clinics Program. 14 In 1992, levels were
determined by enzymatic procedures 15' 16 on the Abbott VP
instrument (Abbott Laboratories, North Chicago, Ill.). Both
chemical and enzymatic procedures met the performance
requirements of the lipid standardization program sponsored
by the Centers for Disease Control and Prevention, Atlanta,
GA. The laboratory is being monitored by the agency's sur-
veillance program. Serum lipoprotein cholesterols (very low
density lipoprotein, low-density lipoprotein, and high-den-
sity lipoprotein) were analyzed by a combination of heparin-
calcium precipitation and agar-agarose gel electrophoresis
procedures. Details and reliability of the method have been
described elsewhere. 9
Information on cigarette smoking was obtained by ques-
tionnaire and recorded as a dichotomous variable.
Data analysis. Data were analyzed with and without
stratification by race and gender. Descriptive statistics were
calculated for each of the four examinations. For each cohort
and for each variable of interest, change during the 8-year
interval was calculated. Comparisons within cohorts were
made by paired t test and between cohorts by unpaired t test.
In general, comparisons reported in the text refer to compar-
isons between cohorts. All tests were two sided. Adjustment
for age was made in analysis of covariance because it was
a confounding variable. Rohrer index and triglyceride values
were log-transformed before the comparison. Values in the
tables do not reflect age adjustment. For blood pressure,
lipid, and lipoprotein values, multivariate models were con-
structed with the dependent variable being the follow-up
value (e.g., second total cholesterol value) and the indepen-
dent variables being age, initial value (e.g., first total choles-
terol value), Rohrer index, and change in Rohrer index. Race
and gender were also included as independent variables af-
ter a check for interaction was made. The regression coef-
ficients were not standardized so that the actual slope can be
reflected. We considered p values of less than 0.01 statisti-
cally significant for all analyses.
R E S U L T S
Comparison of anthropometric, blood pressure, and lipid
variables at the first examination for each cohort by race and
gender showed that the second cohort was 2 to 4 kg heavier
and 0.03 to 0.05 m taller than the first cohort, but these dif-
ferences were statistically significant only for black girls.
The height differences may be partially explained by the fact
that the second cohort was slightly older. The Rohrer index
was similar in both cohorts, except that black girls in the
second cohort had increased ponderosity (0.5 kg/m3; p
<0.01). Systolic and diastolic blood pressures were similar
The Journal of Pediatrics Gidding et al. 8 7 1 Volume 127, Number 6
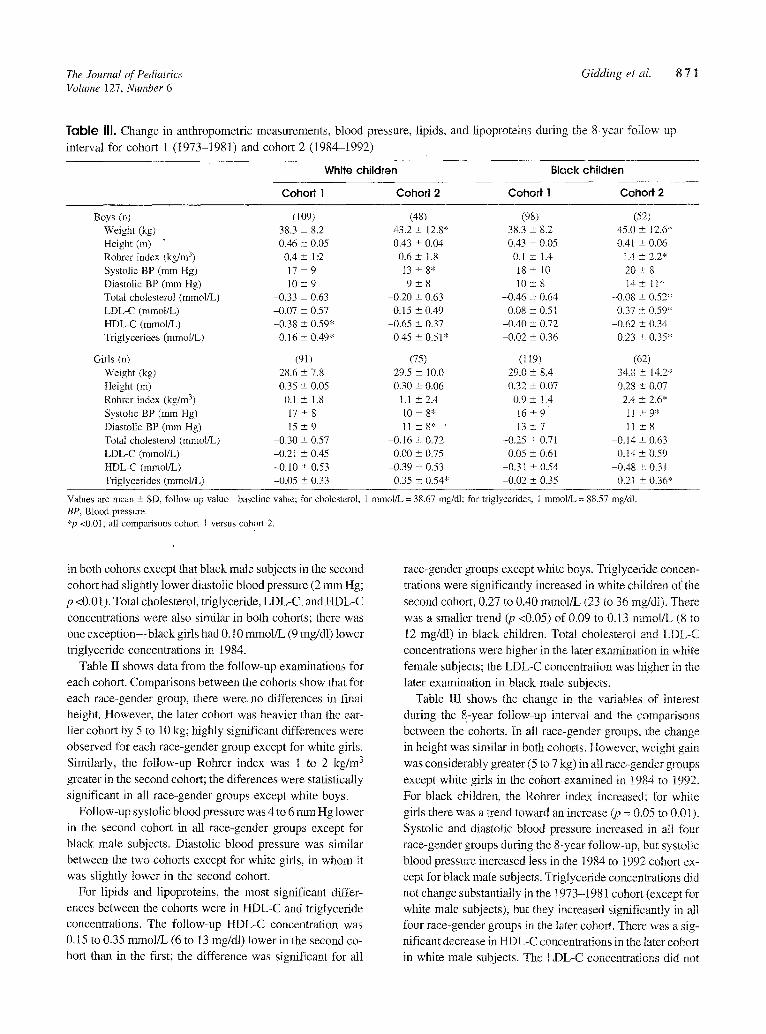
Tab le Ill. Change in anthropometric measurements, blood pressure, lipids, and lipoproteins during the 8-year follow-up
interval for cohort 1 (1973-1981) and cohort 2 (1984-1992)
White children Black children
Cohort 1 Cohoff 2 Cohort I Cohoff 2
Boys (n) (I 09) (48) (98) Weight (kg) 38.3 +. 8.2 43.2 + 12.8" 38.3 _+ 8.2 Height (m) 0.46 +- 0.05 0.43 + 0.04 0.43 _+ 0.05 Rohrer index (kg/m 3) 0.4 -+ 1:2 0.6 +- 1.8 0.1 _+ 1.4 Systolic BP (ram Hg) 17 +- 9 I3 -+ 8* 18 _+ 10 Diastolic BP (ram Hg) 10 +- 9 9 _+ 8 10 -+ 8 Total cholesterol (mmol/L) -0.33 +- 0.63 -0.20 +- 0.63 -0.46 -+ 0.64 LDL-C (mmol/L) -0.07 -+ 0.57 0.15 -+ 0.49 -0.08 _+ 0.51 HDL-C (mmol/L) -0.38 _+ 0.59* -0.65 +- 0.37 -0.40 _+ 0.72 Triglycerides (mmol/L) 0.16 _+ 0.49* 0.45 _+ 0.51" -0.02 -+ 0.36
Girls (n) (91) (75) (119) Weight (kg) 28.6 -+ 7.8 29.5 + 10.0 29.0 _+ 8.4 Height On) 0.35 _+ 0.05 0.30 - 0.06 0.32 _+ 0.07 Rohrer index (kghn 3) 0.1 +- 1.8 1.1 -+ 2.4 0.9 +- 1.4 Systolic BP (mm Hg) 17 -+ 8 10 _+ 8* 16 _+ 9 Diastolic BP (ram Hg) 15 -+ 9 11 +- 8* • 13 -+ 7 Total cholesterol (mmol/L) -0.30 -+ 0.57 -0.16 -+ 0.72 -0.25 + 0.71 LDL-C (mmol/L) -0.21 -+ 0.45 0.00 ± 0.75 0.05 _+ 0.61 HDL-C (retool/L) -0.10 + 0.53 -0.39 +- 0.53 -0.31 +- 0.54 Triglycerides (mmol/L) -0.05 + 0.33 0.35 +- 0.54* -0.02 _+ 0.35
(52) 45.0 -+ 12.6" 0.41 +_ 0.06
t.4 -+ 2.2* 20+- 8 14_ + 11"
-0.08 + 0.52* 0.37 -+ 059*
-0.62 _+ 0.34 0.23 + 0.35*
(62) 34,8 -+ 14.2" 0.28 _+ 0.07
2.4 _+ 2.6* it +-9* 11+,8
-0.14 -+ 0.63 0.14 -+ 0.59
-0.48 + 0.31 0.21 -+ 0.36*
Values are mean _+ SD, follow-up value--baseline value; for cholesterol, 1 mmol/L = 38.67 rag/d1; for triglycerides, 1 mmol/L = 88.57 mg/dl. BP, Blood pressure. *p <0.01; all comparisons coho~ I versus cohort 2.
in both cohorts except that black mate subjects in the second
cohort had slightly lower diastolic blood pressure (2 mm Hg;
p <0.01). Total cholesterol, triglyceride, LDL-C, and HDL-C
concentrations were also similar in both cohows; there was
one except ion--black girls had 0.10 mmol/L (9 mg/dl) lower
triglyceride concentrations in 1984.
Table II shows data from the follow-up examinations for
each cohort. Comparisons between the cohorts show that for
each race-gender group, there were. no differences in final
height. However, the later cohort was heavier than the ear-
lier cohort by 5 to 10 kg; highly significant differences were
observed for each race-gender group except for white girls.
Similarly, the follow-up Rohrer index was 1 to 2 kg/m 3
greater in the second cohort; the diferences were statistically
significant in all race-gender groups except white boys.
Follow-up systolic blood pressure was 4 to 6 e lm Hg lower
in the second cohort in all race-gender groups except for
black male subjects. Diastolic blood pressure was similar
between the two cohorts except for white girls, in whom it
was slightly lower in the second cohort.
For lipids and lipoproteins, the most significant differ-
ences between the cohorts were in HDL-C and triglyceride
concentrations. The follow-up HDL-C concentration was
0.15 to 0.35 mmol/L (6 to 13 mg/dl) lower in the second co-
hort than in the first; the difference was significant for all
race-gender groups except white boys. Triglyceride concen-
trations were significantly increased in white children of the
second cohort, 0.27 to 0.40 mmol/L (23 to 36 mg/d]). There
was a smaller trend (p <0.05) of 0.09 to 0.13 wcmol/L (8 to
12 mg/dl) in black children. Total cholesterol and LDL-C
concentrations were higher in the later examination in white
female subjects; the LDL-C concentration was higher in the
later examination in black male subjects.
Table III shows the change in the variables of interest
during the 8-year follow-up interval and the comparisons
between the cohorts. In all race-gender groups, the change
in height was similar in both cohorts. However, weight gain
was considerably greater (5 to 7 kg) in all race-gender groups
except white gifts in the cohort examined in 1984 to 1992.
For black children, the Rohrer index increased; for white
girls there was a trend toward an increase (p = 0,05 to 0.01).
Systolic and diastolic blood pressure increased in a!l four
race-gender groups during the 8-year follow-up, but systolic
blood pressure increased less in the 1984 to 1992 cohort ex-
cept for black male subjects. Triglyceride concentrations did
not change substantially in the ~ 973-1981 cohort (except ~br
white male subjects), but they increased significantly in all
four race-gender groups in the later cohort. There was a sig-
nificant decrease in HDL-C concentrations in the later cohort
in white male subjects. The LDL-C concentrations did not
8 7 2 Gidding et al. The Journal of Pediatrics December 1995
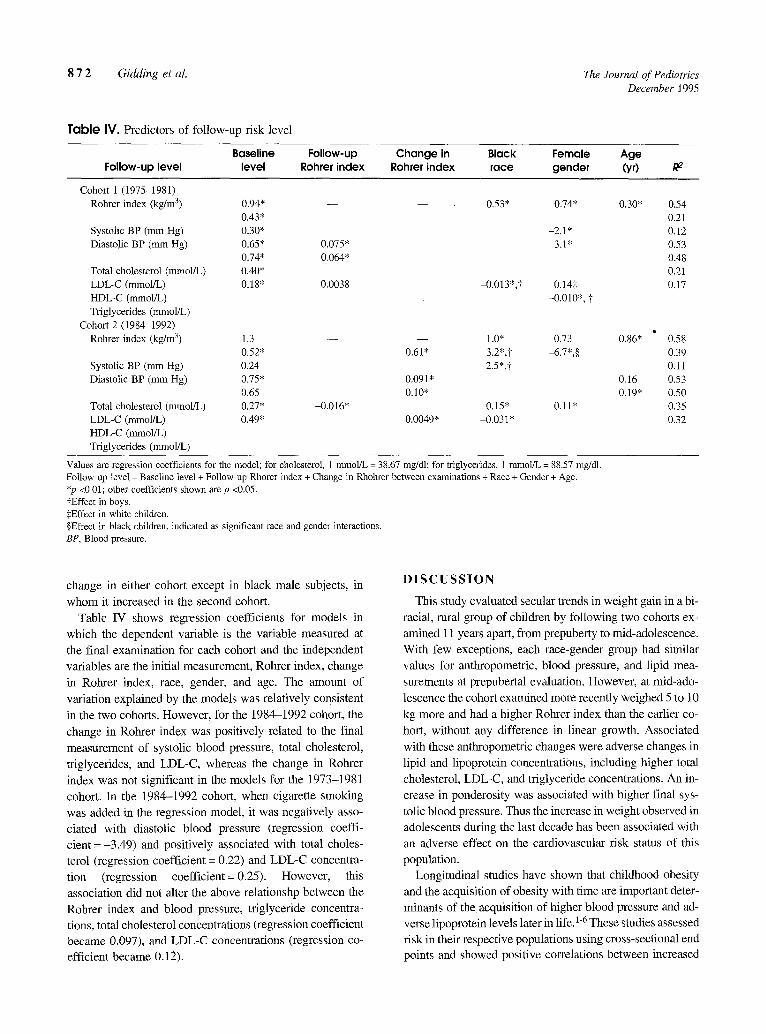
Table IV. Predictors of follow-up risk level
Baseline Follow-up Change in Black Female Age Follow-up level level Rohrer index Rohrer index race gender (yr) R 2
Cohort 1 (1975-1981) Rohrer index (kg/m 3) 0.94* - - - - 0.53* 0.74* 0.30* 0.54
0.43* 0.21 Systolic BP (ram Hg) 0.30* -2.1" 0.12 Diastolic BP (mm Hg) 0.65* 0.075* 3.1" 0.53
0.74* 0.064* 0.48 Total cholesterol (retool/L) 0.40* 0.21 LDL-C (retool/L) 0.18" 0.0038 -0.013",? 0.145 0.17 HDL-C (mmol/L) -0.010", t Triglycerides (retool/L)
Cohort 2 (1984-1992) • Rohrer index (kg/m 3) 1.3 - - - - 1.0" 0.73 0.86* 0.58
0.52* 0.61" 3.2*,? -6.7*,§ 0.39 0.24 2.5",t 0.11 0.75* 0.091" 0.16 0.53 0.65 0.10" 0.19" 0.50 0.27* -0.016" 0.15" 0.11" 0.35 0.49* 0.0049* -0.031 * 0.32
Systolic BP (mm Hg) Diastolic BP (mm Hg)
Total cholesterol (mmol/L) LDL-C (mmol/L) HDL-C (mmol/L) Triglycerides (mmol/L)
Values are regression coefficients for the model; for cholesterol, 1 mmol/L = 38.67 mg/dl; for triglycerides, 1 mmol/L = 88.57 mg/dl. Follow-up level = Baseline level + Follow-up Rhorer index + Change in Rhohrer between examinations + Race + Gender + Age. *p <0.01; other coefficients shown are p <0.05. tEffect in boys. :~Effect in white children. §Effect in black children, indicated as significant race and gender interactions. BP, Blood pressure.
change in either cohort except in black male subjects, in whom it increased in the second cohort.
Table IV shows regression coefficients for models in which the dependent variable is the variable measured at the final examination for each cohort and the independent variables are the initial measurement, Rohrer index, change in Rohrer index, race, gender, and age. The amount of variation explained by the models was relatively consistent in the two cohorts. However, for the 1984-1992 cohort, the change in Rohrer index was positively related to the final measurement of systolic blood pressure, total cholesterol, triglycerides, and LDL-C, whereas the change in Rohrer index was not significant in the models for the 1973-1981 cohort. In the 1984-1992 cohort, when cigarette smoking was added in the regression model, it was negatively asso- ciated with diastolic blood pressure (regression coeffi- cient =-3.49) and positively associated with total choles- terol (regression coefficient = 0.22) and LDL-C concentra- tion (regression coefficient = 0.25). However, this association did not alter the above relationshp between the Rohrer index and blood pressure, triglyceride concentra- tions, total cholesterol concentrations (regression coefficient became 0.097), and LDL-C concentrations (regression co- efficient became 0.12).
D I S C U S S I O N
This study evaluated secular trends in weight gain in a bi- racial, rural group of children by following two cohorts ex- amined 11 years apart, from prepuberty to mid-adolescence. With few exceptions, each race-gender group had similar values for anthropometric, blood pressure, and lipid mea- surements at prepubertal evaluation. However, at mid-ado- lescence the cohort examined more recently weighed 5 to 10 kg more and had a higher Rohrer index than the earlier co- hort, without any difference in linear growth. Associated with these anthropometric changes were adverse changes in lipid and lipoprotein concentrations, including higher total cholesterol, LDL-C, and triglyceride concentrations. An in- crease in ponderosity was associated with higher final sys- tolic blood pressure. Thus the increase in weight observed in adolescents during the last decade has been associated with an adverse effect on the cardiovascular risk status of this population.
Longitudinal studies have shown that childhood obesity and the acquisition of obesity with time are important deter- minants of the acquisition of higher blood pressure and ad- verse lipoprotein levels later in life.l-6 These studies assessed risk in their respective populations using cross-sectional end points and showed positive correlations between increased

The Journal of Pediatrics Gidding et al. 8 7 3 Volume 127, Number 6
weight gain (or increases in measures of ponderosity) and
risk status. This study confirmed a hypothesis suggested by these findings, that the secular trend in the population toward increasing ponderosity would lead to an overall worsening of cardiovascular risk for adolescents with regard to lipids
and lipoproteins. The increasing ponderosity is thought to be related to in-
creased sedentary activity. 17, 18 Increased hours spent watch-
ing television and in other, similar pursuits have been asso- ciated with increased future weight gain.17 Other population-
based trends that may be associated with sedentary activity
include less time spent in physical education in schools, and an increased reluctance of parents to allow children to play
in unsupervised settings because of crime or inadequate rec- reational facilities. 19 Another potential contributing factor,
which has not been documented, is the increasing availabil- ity of food through improved mass transportation, develop-
ment of large grocery stores, and increasing school nutrition programs for children of lower socioeconomic status. Our
previous studies, however, noted secular trends toward reli- ance on school lunch, school breakfast, and fast food as a
source of regular meals but did not show an increase in ca- loric intake in 10-year-old children. 2° Unfommately, the
Bogalusa Heart Study does not have data on fitness or phys- ical activity in the cohort.
An unexpected finding of this study was the decrease in blood pressure in the more recent cohort compared with the
first. Although increase in weight was positively related to an increase in systolic blood pressure, the overal~ increase in
weight in the cohort did not lead to an increase in blood pressure in children during the 11-year interval. The reason
may be that, in children, height is a more important deter- minant of blood pressure than weight. 2I
Other factors besides increased weight gain may be
responsible for the lipid changes seen in this study. However,
secular trends in diet, including lower total and saturated fat
intake as a percentage of total calories, would be expected to lower LDL-C values. 2°, 22 Unfortunately, the Bogalusa
Heart Study does not have dietary data for these cohorts to
assess this interaction. Laboratory drift Could affect lipid re-
sults despite strict attention to blood drawing, analytic methods, and standardization procedures. 23 Nevertheless,
the association between weight gain and concentrations of lipids and lipoprotein cholesterols presented in the multi-
variate analysis was independent of secular trend or labora-
tory drift in lipid values. We believe that excess ponderosity
is an important explanation because of the consistency of the findings with known correlates of excess weight gain in both small cohort and epidemiologic studiesY
In summary, this study showed a secular trend toward in- creased ponderosity in children associated with a worsening of cardiovascular risk status. This trend may develop into a
significant public health problem because it may increase the
risk of diabetes and coronary artery disease, counterbalanc-
ing efforts to reduce the prevalence of cigarette smoking and to improve diet and physical activity in childrenY
We thank the Bogalusa staff and the children and young adults who participated in the study, without whom this program would not be possible.
R E F E R E N C E S
1. Wattigney WA, Harsha DW, Srinivasan SR, Webber LS, Berenson GS. Increasing impact of obesity on serum lipids and Iipoproteins in young adults. Arch Intern Med 1991 ; 151:2017- 22.
2. Burns TL, Moll PP, Lauer RMI The relation between pon- derosity and coronary risk factors in children and their relatives: the Muscatine Ponderosity Family Study. Am J Epidemiol 1989; 129:973-87.
3. Lauer RM, Lee J, Clarke WR. Factors affecting the relationship between childhood and adult cholesterol levels: the Muscatine Study. Pediatrics 1988;82:309-18.
4. Laner RM, Clarke WR, Beaglehole R. Level, trend, and vari- ability of blood pressure during childhood: the Muscatine Study. Circulation 1984;69:242-9.
5. Webber LS, Cresanta JL, Croft JB, Srinivasan SR, Berenson GS. Transition of cardiovascular risk factors from adolescence to young adulthood: the Bogalusa Heart Study. II. Alteration in anthropometric, blood pressure and serum lipoprotein vari- ables. J Chronic Dis 1986;39:91-103.
6. Freedman DS, Burke GL, Harsha DW, et al. Relationship of changes in obesity to serum lipid and lipoprotein changes in obesity to serum lipid and lipoprotein changes in childhood and adolescence. JAMA 1985;254:515-20.
7. Gortmaker SL, Dietz WH Jr, Sobol Am, Wehler CA. Increas- ing pediatric obesity in the United States. Arch Pediatr Adolesc Med [Am J Dis Child] 1987;141:535-40.
8. Berenson GS, McMahan CA, Voors AW, et al. Cardiovascular risk factors in children: the early natural history of atheroscle- rosis and essential hypertension. New York: Oxford University Press, 1980.
9. Srinivasan SR, Frerichs RR, Webber LS, Berenson GS. Serum lipoprotein profile in children from a biracial community: the Bogalusa Heart Study. Circulation 1976;54:309-18.
10. Voors AW, Foster TA, Frerichs RR, Webber LS, Berenson GS. Studies of blood pressure in children, ages 5-14 years, in a to- tal biracial community: the Bogalusa Heart Study. Circulation 1976;54:319-27.
11. Foster TA, Voors AW, Webber LS, Frerichs RR, Berenson GS. Anthropometric and maturation measurements of children ages 5-14 years, in a biracial community: the Bogalusa Heart Study. Am J Clin Nutr 1977;30:582-91.
12. Voors AW, Webber LS, Frefichs RR, Berenson GS. Body height and body mass as determinants of basal blood pressure in children: the Bogalusa Heart Study. Am J Epidemiol 1977; 106:101-8.
13. Foster TA, Webber LS, Srinivasan SR, Voors AW, Berenson GS. Measurement error of risk factor variables in an epidemi- ologic study of children: the Bogalusa Heart Study. J Chronic Dis 1980;33:661-72.
14. Lipid Research Clinics Program. Manual of laboratory opera- tions; vol 1. Lipid and lipoprotein analysis. (DHEW Publica-
8 7 4 Gidding et al. The Journal qf Pediatrics December 1995
tion No. [NIH] 75-628.) Washington, D.C.: National Institutes of Health, 1974.
15. Allaln CC, Poon LS, Chan CSG, Richmond W, Fu PC. Enzy- matic determination of total serum cholesterol. Clin Chem 1974;20:470-5.
16. Bircolo G, David H. Quantitative determination of serum trig- lycerides by the use of enzymes. Clin Chem 1973;19:476-82.
17. Dietz WH, Gortmaker SL. Do we fatten our children at the television set? Obesity and television viewing in children and adolescents. Pediatrics 1985;75:807-12.
18. Ravussin E, Lillioja S, Knowler WC, et al. Reduced rate of en- ergy expenditure as a risk factor for body-weight gain. N Engl J Med 1988;318:467-72.
19. Strong WB. Physical activity and children. Circulation 1990; 81:1697-701.
20. Nicklas TA, Webber LS, Srinivasan SR, Berenson GS. Secu- lar trends in dietary intakes and cardiovascular risk factors of 10-year-old children (1973-1988). Am J Clin Nutr 1993; 57:930-7.
21. Voors AW, Webber LS, Berenson GS. Relationship of blood pressure levels to height and weight in children. J Cmdiovasc Med 1978;3:911-8.
22. Stephen AM, Wald NJ. Trends in individual consumption of dietary fat in the United States, 1920-1984. Am J Clin Nutr 1990;52:457-69.
23. Sklov MC, Srinivasan SR, Webber LS, Berenson GS. Vari- ability of total cholesterol concentrations in serum by repeated measurements in a large pediatric population: limitations of quality controls for laboratory analyses. Clin Chem 1981; 27:1988-92,
24. Van Itallie TB. Health implications of overweight and obesity in the United States. Ann Intern Med 1985;103:983-8.
25. Strong WB, Deckelbaum R J, Gidding SS, et al. Integrated car- diovascular health promotion in childhood: a statement for health professionals for the Subcommittee on Atherosclerosis and Hypertension in Childhood of the Council on Cardiovas- cular Disease in the Young--American Heart Association. Circulation 1992;84:1638-50.
FELLOWSHIPS
Fellowships available in pediatric subspecialties and those for general academic pediatric training
are listed once a year, in J anua ry , in THE JOURNAL OF PEDIATRICS. Each June , forms for listing
fellowships available for the academic year beginning 18 months after publication are sent to the
Chairman of the Department of Pediatrics at major hospitals in the United States and Canada. In
addition, a copy of the application form appears in the July, August , and September issues of
THE JOURNAL (please use the current form). Should you desire to list fellowships, a separate ap-
plication must be made each year for each position. All applications must be returned to
Mosby-Year Book, Inc., by Oetober 15 preceding the listing year to ensure publication. Additional
forms will be supplied on request from the Journal Editing Department, Mosby-Year Book, Inc.,
11830 Westline Industrial Drive, St. Louis, MO 63146-3318/800-325-4177, ext. 4317, or 314-453-
4317.