Embed Size (px)
Citation preview

Effective Use of Medicaid to Support EHDI Programs
Peggy McManusMaternal and Child Health Policy Research Center
Karl WhiteNational Center for Hearing Assessment and Management
Janet FarrellMassachusetts State EDHI Program

Faculty Disclosure Information
In the past 12 months, we have not had a significant financial interest or other relationship with the manufacturers of products or providers of the services that will be discussed in our presentation
This presentation will not include discussion of pharmaceuticals or devices that have not been approved by the FDA nor will the presentation discuss unapproved or "off-label" uses of pharmaceuticals or devices.

Medicaid is the largest single insurer of children in the United States (30% of all children are enrolled in Medicaid and 40% of all births are paid by Medicaid)
Medicaid reimbursement polices and practices significantly affect policies and practices of private health insurers
EPSDT (Early and Periodic Screening, Diagnosis, and Treatment) is a required part of Medicaid that provides preventive health care (and where needed) treatment services to children

Assessing Current Practices
15 state email survey, conducted by MCH Policy Research Center, January – March 2005
Examined Fee for Service (FFS) policies for a comprehensive set of hearing services
Obtained 2005 fees and compared them to 2000 fees collected by MCHPRC in previous study

Research Questions
1. Do states have reimbursable codes for a comprehensive set of hearing services?
2. What are average payment amounts, range of payments, & fee distribution in 2005?
3. What changes in reimbursement have states made since 2000?
4. How do state Medicaid fees compare to Medicare fees?

Strategic Directions Meeting
July 12 & 13, 2005 in Salt Lake Cite 10 states participated (State EDHI coordinator and
State EPSDT Director)
Each state developed a written action plan focused on using EPSDT to improve EHDI services for children

Overview
Strategic Directions for Medicaid and EPSDT►Hearing Standards and Policies►Information and Education►Quality and Financial Incentives►Collaboration with EHDI Programs
Lengthy interviews conducted with 10 state EPSDT directors ---CO, IL, IA, MA, NC, NH, UT
Based on interview form developed with assistance from NCHAM and State EDHI directors

Standards and Policies
Examined state EPSDT policies for hearing screening and follow-up
Stated EPSDT hearing standards mostly based on AAP preventative care guidelines
EPSDT standards focus almost exclusively on screening, not referral and follow-up
JCIH guidelines seldom referenced

Standards and Policies
States have organized mechanism for regularly updating EPSDT with input from other state agencies and key stakeholder groups
Effective ways of implementing new standards – work closely with state AAP chapters
Hospital involvement also critical State universal newborn hearing screening
laws- key in facilitating adoption of standards More attention needed to address a follow-up
of failed screens

Information and Education
Examined state EPSDT strategies for using effective educational strategies in working with PCP’s, families, hospitals, HCO’s, and local health departments
PCP’s ►No magic bullets or single approaches ►Very little done so far on follow-up ►Important to have good, actionable data
about how PCP’s perform ►Evidence-based data also important ►Newsletters that profile promising practices useful

Information and Education
PCP’s (continued): ►Ongoing training of residents helps
►CME necessary, but not sufficient
►More needed to target PCP’s in rural
areas, with small numbers of children
in practice

Information and Education
Families:►Work with existing family networks
►More education needed on follow-up, especially with families whose children have complex health care needs
►Follow-up telephone calls & face-to-face meetings work best

Information and Education
Hospitals►State EHDI efforts, especially involving on-site work,
critical in implementing universal newborn hearing screening
►Funding hearing aid loaner programs important
►Need to target small, rural hospitals and move beyond screening
►Perinatal conferences important
►Also, having short educational videos about hearing screening for use by hospitals important

Information and Education
Use of popular media helpfulCritical to have a “why” piece –
explaining why both screening & follow-up are necessary
Informing families about standard of care is important and can positively influence parent demand for services

Information and Education
Local Health Departments►EPSDT outreach workers have critical
role to play, but few have focused on hearing
►Important to link with home visiting, case management, disease
management, & other initiatives involving LHDs
►Regular training opportunities for LHDs, with CME important

Information and Education
Hard-to-reach groups►EPSDT outreach workers have critical
role to play►Home visiting & case management
programs reach high-risk groups, though hearing follow-up seldom addressed
►More attention to cultural competence to reduce families’ delays in seeking follow-up
►Translation & transportation support

Information and Education
Overarching Comments►Comprehensive strategy needed, promoted through
various channels (e.g. immunization)
►Have a simple, consistent message – 1/3/6
►Involve key groups at outset
►Address shortage of audiologists, including
causes—education & training, reimbursement, other
►Streamline & integrate hearing follow-up services
with CM, EI, WIC, 1-800#, EPSDT outreach

Quality and Financial Incentives
Examined opportunities for incorporating quality incentives from Healthy People 2010
Examined Medicaid reimbursement levels

Quality Incentives
Few EPSDT programs use or are aware of Health People 2010 hearing objectives
Most Medicaid quality standards from NCQA (HEDIS), AAP
Use of quality indicators (e.g., 1/3/6) could be an effective strategy
Important to have actionable data for use by providers
Comparative state data also helpful

Quality Incentives
NICHQ’s model of collaborating with practices, conducting chart reviews, identifying improvement strategies, and providing feedback (e.g. lead, immunization)
Need to make sure hearing screening and follow-up is incorporated into EPSDT evaluations. Records could be tagged for follow-up

Quality Incentives
Consider a GPRA project (e.g. immunization) CMS could set a standard (e.g. dental care) Maintain close link with public health Issue certificates of excellence to providers
scoring 95% or higher Acknowledge the good work of providers
“They’re not doing this work for the financial rewards, but for the benefits of the children.”

Reimbursement Incentives
“Ha, ha, ha. Stand in line.”State Medicaid and public health funding
is already stretched to its limitsImportant to piggyback with existing
EPSDT administrative outreach effortsThrough Medicaid’s administrative
match, possibly some potential for funding follow-up activities

Reimbursement Incentives
To claim administrative match requires financial support from other state agencies- good luck!
To justify payment changes, evidence of cost savings needed
Professional organizations & provider groups need to advocate for rate increases showing costs not being met and access adversely affected

Reimbursement Incentives
Also, comparative state fee data useful – no one wants to be lowest
See examples from dental care. Also, incentives used successfully with EPSDT visit rates, immunizations, and lead screening
Examine hospital payment mechanisms to assess where to place incentive
Consider outside foundation and community funds

Collaboration
Examined new and existing opportunities to promote collaboration
Consider roles and responsibilities for state EHDI programs to play with Medicaid and participating MCOs and other providers
Already a great deal of collaboration between Medicaid and EHDI programs, mostly around newborn screening
Meetings at least quarterly help, involving Medicaid and other key stakeholders
Written interagency agreements useful in promoting accountability

Collaboration
Examples: MD- a portion of EHDI coordinator’s time/salary is dedicated to working with Medicaid
IL: “Think Tank Day” on newborn hearing projects for coming year; developed education, referral, and follow-up document; grand rounds training with AAP; newborn screening advisory group; now working on parent website

MA Statistics
80,000 births annually >99% hearing screening rate
universal at all birthing facilities follow-up occurs on all referrals at the state level
Did not pass, missed, home births, and resident births born out of state)
<1.5% refer rate
200 children diagnosed with hearing loss after referral from newborn hearing screening
(estimated data from the Childhood Hearing Data System)

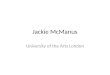
Massachusetts PrenatalCare Payment Source
28.9% publicly insured (MassHealth, CommonHealth, Medicaid Managed Care, Healthy
Start, Medicare and Free Care)
Medicaid covered 1 out of every 4 women 70% privately insured 0.7% self-paid for prenatal care 0.4% other
Massachusetts Department of Public Health, Massachusetts Births 2003

EPSDT and EHDI
Attended national meeting Developed a workplan
who is responsible, what needs to happen, start and end dates, obstacles and resources
Began a schedule of regular meetings with both programs
Collaborated with internal and external partners

Workplan Activities
Updated EPSDT Policy Manual expanded section on hearing assessment information on risk indicators for hearing loss
Updated periodicity schedule for MA Health Quality Partners (MHPQ) intended for quality practice recommendations endorsed by many of the major insurers in the state

Outreach to Medicaid Managed Care Organizations (MCOs)
Developed newborn hearing screening training for MCOs
Presented at the MCH/MCO Workgroup Meeting provided resources
Included the DPH, School Health Vision Screening Initiative and Women, Infants and Children (WIC) Program in training
Addressed opportunities for future collaboration

Training for Audiological Diagnostic Centers
EPSDT Reimbursement: hearing aids and hearing
related services Provided contact information: MassHealth
prior approval, MCOs customer assistance Developed list of questions about prior
approval issues Follow-up meeting planned with prior approval
staff from MassHealth

Head Start Training
Met with EPSDT and Head Start to discuss hearing and vision screening issues
Developed module for “best practices” training for early childhood vision and hearing screening and EPSDT
audience: Head Start Health Services Managers and Child Care Consultants, School Health Nurses
exceeded capacity of 100 for the training

Next Steps
Explore opportunities to work with cochlear implant programs in MA
MCO newsletters Explore feasibility of utilizing MassHealth data to
improve follow-up Analyze Family Satisfaction Survey results to
assess differences in responses for publicly insured families
Develop strategies to recognize MassHealth providers that dispense hearing aids to children