Embed Size (px)
DESCRIPTION
ED training Respiratory/ patient with dyspnea. Dr Jaycen Cruickshank Emergency Medicine Training Hub Ballarat & Grampians Region 2012. Respiratory - dyspnea Learning objectives. - PowerPoint PPT Presentation
Citation preview

ED trainingRespiratory/
patient with dyspnea
Dr Jaycen Cruickshank
Emergency Medicine Training Hub
Ballarat & Grampians Region
2012

Respiratory - dyspneaLearning objectivesThe respiratory session will examine contrasting clinical cases of dyspnoea that will illustrate the
principles of diagnostic reasoning. lmportant physical findings that help discriminate different causes of dyspnoea will be discussed along with appropriate initial investigations.
Learning objectives Be able to describe the differences and similarities in the medical history, physical examination
and investigations of common or life threatening causes of dyspnoea. To manage asthma and pneumonia using best practice guidelines To be able to use the Wells score & PERC rule in diagnosis of PE
Pre reading Hughes T & Cruickshank J. Adult Emergency Medicine at a Glance. Chichester, West Sussex,
UK : John Wiley & Sons, 2011. Chapter 36 Shortness of breath. Chapter 7 Blood gas analysis.
Other learning resources Relevant clinical clinical guidelines at Ballarat Health Services:
Refer to ED lecture series and self directed workbooks

Other learning resources
Other learning resources http://www.mdcalc.com/wells-criteria-for-pulmonary-embolism-pe/ Wells et al. Excluding pulmonary embolism at the bedside without diagnostic imaging:
management of patients with suspected pulmonary embolism presenting to the emergency department by using a simple clinical model and d-dimer. Ann Intern Med. 2001 Jul 17;135(2):98-107. http://www.ncbi.nlm.nih.gov/pubmed/11453709
Written asthma action plans. http://www.nationalasthma.org.au/managing-asthma/controlling-your-asthma/written-asthma-action-plans
Pneumonia severity scoring systems for community-acquired pneumonia in adults (Appendix 2.4) http://jasper.tg.com.au/complete/tgc/abg/8052.htm
http://lifeinthefastlane.com/2009/11/a-classic-respiratory-case/

Preparation slidesThese may be pre reading +/- presented by teacher
The first part of this presentation is designed to be pre reading.
Learners are encouraged to do some reading before the tutorial
The slides may be presented briefly at the start of a session to recap
Your hospital should have some clinical guidelines which will provide relevant local information

Emergency Department HMO education series 2012
How do we make a diagnosis in a patient with dyspnea?
History Cardinal features Associated features Risk factors (for diseases), past history (known
diseases), respiratory reserve “what can do usually?”
Examination findings Suitable/targeted investigations
CXR, ECG, ABG’s, basic bloods Lung function, CT, VQ, exercise test, echo

Emergency Department HMO education series 2012
A focussed history determines both diagnosis and severity. SOB + associated symptoms
suggests a cause or differential diagnosis
SOB + Pleuritic pain= Pneumonia, pneumothorax
SOB + wheeze = Asthma, COPD
SOB + stridor = Inspiratory obstruction e.g croup
SOB + fever/cough/sputum = Pneumonia, other infection
SOB + haemoptysis Upper airway cause, Pneumonia, PE,
cancer, vasculitis
The severity of symptoms E.g is the person breathless at
rest, on exertion Certain features aid diagnosis Acute onset Pneumothorax, PE, AF, APO, asthma Gradual onset or with exertion Cardiac cause, chronic anaemia Worse at night, or lying down Cardiac failure

Background history Would you prefer to know risk factors for disease or known diseases?
Exacerbations of known diseases are common and the diagnostic challenge is likely to focus on precipitant, and the severity of the consequences of the exacerbation
Ask about Medications, including doses, compliance, recent changes Who normally looks after the patient and where Is there access to a good summary of recent treatment – think the GP, specialist clinic
letters, recent admissions As you build up a differential diagnosis, ask questions that are relevant to each
differential e,g I am thinking PE, so I will ask about recent travel, perhaps use the Well’s criteria I am thinking pneumonia, I might ask about hospital vs community acquired,
immunosuppresion, contacts, birds, known recent outbreaks e.g Legionella I am thinking what should I not miss, e.g cardiac causes This type of approach to differential diagnoses is often helpful when working through
a list of possible diseases.

Emergency Department HMO education series 2012
Paediatrics A quick reminder that for
paediatric assessment, there are resources available to assist with normal values
Hypoxia needs immediate correction, remember cyanosis a pre terminal sign in children
Most of the examination can be completed without O2 sats or a stethoscope using observation

Emergency Department HMO education series 2012
You need to be familiar with this for winter. Standardised way to assess, present, refer kids.
The Royal Children’s clinical guidelines are an excellent resource to look up while working in the Emergency Department.
http://www.uhs.nhs.uk/Media/suhtideal/TopNavigationArticles/SkillsForPractice/ClinicalSkills/paediatricassessment.pdf
Recognition of the seriously ill child http://paeds.org/apls/aplsrecog.html the structured approach to the seriously ill child
http://www.paeds.org/apls/aplsapp.html

Clinical cases to demonstrate
We have a very thorough powerpoint presentation that contains more detail, a very methodical approach.
Highly recommended. The rest of this presentation will contain
some cases. A further series of cases will be presented at
the actual teaching session.

Emergency Department HMO education series 2012
Case A
A young man presents to the Emergency Department via ambulance
He complains of sudden onset of SOB. Present for a few hours and now quite
severe.

Emergency Department HMO education series 2012
Further history
Previously well, smokes 10 cigarettes/day Left sided chest pain
Moderate Pleuritic Started with the SOB
Is there anything else you would like to ask? What is your ddx?

Emergency Department HMO education series 2012
Differential diagnosis
Pneumothorax Arrhythmia
Pulmonary Embolism
Asthma (less likely)
Much less likely Pneumonia
Not to be mentioned before all organic causes considered anxiety Imagine that being your
diagnosis and you missed the pneumothorax…

Emergency Department HMO education series 2012
Examination findings Looks unwell, quite
distressed with WOB RR 26, HR 125 SR, BP
80/60, afebrile Saturation 93% RA (room
air) Trachea midline chest expansion on the
left Hyperesonant percussion
note on the left air entry left lung
What is going on? Is this serious? What is your immediate
management?

Emergency Department HMO education series 2012
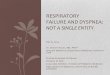
Describe this CXR… ideally this intervention before this CXR…

Emergency Department HMO education series 2012
Diagnosis and management?
Initial therapy? Who will help you?
Where you are working, will you call a MET, ask for senior help?
Urgent chest tube (this may have even been done without a CXR if the patient was unwell enough)

Emergency Department HMO education series 2012
Describe this CXR
See notes for report

Emergency Department HMO education series 2012
Describe this CXR

Emergency Department HMO education series 2012
Case B
Young man Brought to the ED by
his partner Progressive SOB over
48 hours. Now present at rest
How is your differential diagnosis altered by the gradual onset? Asthma Pneumonia Other?

Emergency Department HMO education series 2012
Further history & examination
Wheeze Dry cough Recent URTI Childhood asthma (age
3-12), hay fever No cardiac history No risk factors for PE
RR 24, HR 110 SR, BP 110/70
Sat 97% RA Widespread wheeze
(what causes this sound?)

Emergency Department HMO education series 2012
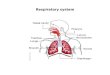
Investigations If the CXR is normal… Peak Flow 300/min (how does this
help us?) ABG ph 7.5/CO2 30/O2 70/HCO3
23 What do the blood gases show? How severe is the problem
What if the CXR not normal, as seen on right
Does it exclude asthma?

Emergency Department HMO education series 2012
Diagnosis is asthma:
The treatment plan is easy, but can you document it well? Bronchodilators, corticosteroids, oxygen
Describe the stickers used to standardise prescribing in the ED at Ballarat Health Services
Describe a safe asthma discharge plan What are asthma action plans? http://www.nationalasthma.org.au/health-professionals/tools-for-primary-care/asthma-action-plans/asthma-action-
plan-library

Emergency Department HMO education series 2012
What scoring tools for pneumonia?
CURB-65, SMARTCOP? How do scoring tools help predict:
Need for admission, and appropriate ward Antibiotics and route Mortality
Is it acceptable to write clinical notes on a patient with a diagnosis of pneumonia and not document severity using one of these tools? No
Various website and apps can assist you in remembering them. www.mdcalc.com

Further cases…
To be presented at the teaching session. See part 2 & 3