Embed Size (px)
Citation preview

Region VIII EMS Systems
July 2016

Introduction
• SME video of the month
• Review of Respiratory SOPs
• Three scenarios

Announcements
• Region-None
• System- New SOP’s In Effect July 1st

Dyspnea
• Common type of emergency call in EMS
• Has various causes
• Is both a sign and a symptom
• Sensation of breathlessness or inadequate breathing
• Can be acute or chronic


Differential Diagnosis of Dyspnea
• In disease states the cause is usually a result of cardiac,
pulmonary pathology or trauma
• Severe dyspnea is a medical emergency if not treated
appropriately respiratory failure and death can occur
• When eliciting a history it is helpful to determine if the
dyspnea is acute or chronic utilizing
– Sample
– OPQRST

Dyspnea
• Acute– Asthma
– Carbon monoxide poisoning
– Cardiac tamponade
– Heart failure
– Myocardial infarction
– Hypotension
– Pulmonary embolism
– Pneumothorax
– Pneumonia
– Upper airway obstruction
• Chronic– Asthma
– COPD
– Deconditioning
– Heart dysfunction
– Interstitial lung disease
– Obesity


Differential Diagnosis Dyspnea
• Common Respiratory Causes
– Foreign body Aspiration (upper /
middle airway)
– Anaphylaxis (upper airway)
– Pulmonary Embolism (lower
airway)
– Pneumothorax (lower airway)
– Tension pneumothorax (lower
airway)
– Croup (upper airway)
– Acute epiglottitis (upper airway)
– Asthma (lower airway)
– COPD (lower airway)
– Pneumonia (lower airway)

Differential Diagnosis of Dyspnea
• Right and left heart failure
• Myocardial infarction
• Cardiomyopathy
• Valvar dysfunction
• Pericarditis
• Arrhythmias
• Hypovolemia
H’s & T’s
• Hypoxia,
• Hydrogen ion (acidosis), Hyper-
/hypokalemia
• Hypothermia
• Hypoglycemia
• Toxins/Tamponade
• Tension pneumothorax
• Thrombosis
• Trauma
Cardiac causes of dyspnea include



Dyspnea Scales

Location and lung soundsLocation Sound Phase Disease Process
Upper Airway Stridor Inspiration Viral Croup
Epiglottitis
Foreign Body Aspiration
Lower Airway Rhonchi Primarily Expiration Frank Aspiration
Bronchitis
Cystic Fibrosis
Wheeze Primarily Expiration Reactive airway disease
Asthma
Congestive heart failure
Emphysema
Endobronchial obstruction
Crackles End Inspiration Pneumonia
Exacerbation of congestive heart failure
Pulmonary edema
Diminished breath sounds Either or both Emphysema
Atelectasis
Pneumothorax (simple or tension)
Flail chest
Neuromuscular disease
Pleural effusion
Chest Wall Pleural rub Either Pleuritis
Pleurisy
Pleural effusion

Upper Airway
• Main symptoms of upper airway problem are
– Dyspnea
– Noisy breathing
• More prominent during exercise
• May be aggravated by change in body position
• Breathing is labored and increases if lying supine

Upper Airway
• Signs occur mostly during inspiration
– Change in voice: Hoarseness, barking cough
– Inspiratory stridor
– Cyanosis, drooling
– Nasal flaring
– Tachypnea
– Retractions
– Poor air entry on auscultation
– Prolonged inspiratory phase

Upper Airway
• Noisy breathing:
– Snoring: Indicates partial obstruction of the upper airway that
causes a vibration of air as it passes thru the nasopharynx and
oropharynx (tongue)
– Stridor: A harsh, continuous crowing sound. Mostly occur
during inspiration

Upper Airway
• Conditions include
– Foreign body obstruction
– Pharyngeal edema
– Croup
– Epiglottitis
– Anaphylaxis

Angioedema
• Rapid swelling of the dermis, subcutaneous tissue
mucosa and submucosal tissues
• Skin is swollen, tender and warm
• May last days or resolve spontaneously

Angioedema• Substances known to trigger allergic angioedema
– Certain types of food particularly nuts, shellfish, milk, eggs
– Certain medication- penicillin, aspirin, NSAIDS
– Insect bites and stings
– Latex
• Cases without an identifiable cause are known as idiopathic
angioedema. May be a problem with the immune system
causing it to misfire. Triggers include:
– Anxiety - Hot or cold temps
– Stress - Exercise
– Minor infections

Angioedema
• Hereditary angioedema is caused by a genetic mutation in
the C1 esterase inhibitor
• The body does not produce enough of this C1 protein
• C1 plays an important role in regulating the immune
system
• Triggers include : Trauma- including surgery and
infection, oral contraceptives, and pregnancy

Angioedema
• Acute episodes often involve the lip, eyes, and face.
• May also affect other parts of the body including
respiratory and gastrointestinal mucosa.
• Laryngeal swelling can be life threatening
• Often associated with local burning sensation and pain
• Pronounced itchiness and local erythema

Angioedema
• Severe attacks can indicate the onset of systemic
anaphylaxis
• Characterized initially by dyspnea
• Medications used in treating urticaria and anaphylaxis are
also used in treating angioedema
• In severe cases of laryngeal edema a surgical airway may
be needed

Angioedema

Upper Airway Condition
Anaphylaxis
• Serious life threatening allergic reaction
– Most common causes
• Food
• Latex
• Medications
• Insect stings
• Envenomation

Upper Airway Condition
Anaphylaxis• Signs and symptoms
– A swollen tongue or throat, which can cause wheezing
(wheezing is a lower condition) and dyspnea
– A weak and rapid pulse
– Nausea, vomiting or diarrhea
– Dizziness or fainting
– Abdominal pain

Upper Airway Condition
Anaphylaxis • Signs and symptoms
(continued)Skin reactions, including
hives itching, and flushed
or pale skin
– A feeling of warmth
– The sensation of a lump in the
throat
– Constriction of the airway
– Chest pain
– Headache
– Rhinitis

ADULT ALLERGIC REACTION / ANAPHYLAXIS
BLS/ALS 1. Adult Initial Medical Care SOP, p. 4-5 2. Apply ice/cold pack to site 3. BLS: at the direction of Medical Control, administer one dose EPINEPHRINE auto-
injector (EpiPen®)
ALS Allergic reaction with systemic signs, i.e. wheezing, diffuse hives, or prior history of systemic reaction, without signs of hypoperfusion 4. Administer BENADRYL (diphenhydramine) 50 mg IM or slow IV/IO. Max dose 50
mg. 5. Administer EPINEPHRINE 1:1000 0.3 mg IM. May repeat x 1 after 15 minutes if
minimal response
If age > 50 years old and/or cardiac disease history, contact Medical Control prior to administration of EPINEPHRINE
6. If wheezing, consider ALBUTEROL 2.5 mg (3 mL) via nebulizer
ALS Anaphylaxis: multisystem reaction with signs of hypoperfusion; altered mental status or severe respiratory distress/wheezing/hypoxia 1. If signs of hypoperfusion, IV/IO FLUID BOLUS in 200 mL increments
Administer EPINEPHRINE 1:10,000 0.5 mg slow IV/IO or EPINEPHRINE 1:1000 0.5 mg IM. May repeat EPINEPHRINE q 3 minutes
2. Administer BENADRYL (diphenhydramine) 50 mg slow IV/IO
If no IV, give BENADRYL (diphenhydramine) 50 mg IM
No repeat dose 3. If wheezing, consider ALBUTEROL 2.5 mg (3 mL) via nebulizer 4. Consider DOPAMINE per CARDIOGENIC SHOCK SOP, p. 23, for refractory
hypotension
Note
EPINEPHRINE may be given IM if IV/IO access delayed.

EpiPen

Auvi-Q
• Epinephrine auto injector
• Same dosing as the EpiPens
– 0.3mg IM
– 0.15mg IM
• Talks to the patient
– Walks them through the steps for injection

Change in epinephrine ratios

Epinephrine
• Confusion has been associated with numerous
medication errors over the years
• The new epinephrine labeling will only be displayed on
mass concentrations
• 1:1000 will be labeled 1mg/ml
• 1:10,000 will be labeled 0.1mg/ml
• Effective May 1, 2016

Epinephrine

Capnography
• Measures:– Ventilation: for patient with a pulse
– Perfusion: When patient is pulseless
– Partial pressure (mmHg) or volume (% vol) of CO2 in the
airway at the end of exhalation
– Breath-to-breath measurement provides information within
seconds
– Not affected by motion, artifact, poor perfusion or dysrhythmias

Capnography
• Reflects how effective our interventions are
• Can be utilized to more objectively determine a patient’s
respiratory distress
• Provides earliest, most accurate indication of respiratory
distress
• Changes in capnography waveform provide earliest
indication of apnea, upper airway obstruction and
laryngospasm or worsening of patient’s condition

Capnography
• Utilization in upper airway conditions
• Apnea:
– No waveform, no chest wall movement, no breath sounds
• Upper airway changes or obstruction:
– chest wall moving
– decrease or no breath sounds
– May be responsive to airway maneuvers with a return of
waveform or improvement in waveform

Capnography

Lower airway
• Lung/Lower airway Causes
– Pneumonia
– Pneumothorax
– Pulmonary embolism
– Interstitial lung disease
– Adult Respiratory Distress Syndrome
– COPD
– Asthma


Lower Airway
• Signs and Symptoms
– Tachypnea
– Wheezing (expiratory most common)
– Increased respiratory effort
– Retractions
– Prolonged expiration

Lower Airway Condition
Pulmonary Embolism • A sudden blockage in the lung usually caused by a clot
that formed in the smaller vessels such as arms, legs,
pelvis

Lower Airway Condition
Pulmonary Embolism• Signs and symptoms
– Sudden onset chest pain
• Sharp, knife like or deep ache that worsens with inspiration
– Dyspnea
– Anxiety
– Cough
– Diaphoresis
– Syncope
– Tachycardia
– Tachypnea
– Decrease ETCO2 (<20 mmHg) despite normal respiratory rate and
perfusing rhythm

Lower Airway Condition
Pulmonary Embolism • A popular prehospital assessment tool for patient with
respiratory complaints is end tidal CO2 (EtCO2)
• In patients with pulmonary embolism, expect to see
normal (35-45mmHg) to slightly low EtCO2 resulting from
tachypnea and a normal waveform
• Deliver oxygen to maintain SPO2 above 94%

12 lead changes with PE

12 Lead

Pulmonary Embolism

BLS Scenario
• Medic is dispatched for a 20 y/o female complaining of
shortness of breath
• You arrive on the scene and observe the patient sitting in
a chair in the tripod position
• States watching TV when developed sudden onset of pain
between shoulder blades
• Pt is agitated, short of breath, and has faint cyanotic color
to her face

BLS Scenario
• VS BP 98/62, HR 118, RR 32 and shallow
• SPO2 89% with decreased breath sounds on right and
clear on left
• What are your priorities
• What information do you need
• What is your immediate treatment

Lower Airway Condition
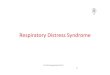
Pneumothorax A pneumothorax occurs when
the potential space between the
parietal and visceral pleura of
the lung fills with air and
collapses the lung. It can occur
spontaneously or following
trauma or pathology

Lower Airway Condition
Primary Spontaneous Pneumothorax
• Risk factors Spontaneous Pneumothorax
– Age 15-30 years old
– Male have higher incidence than women
– Tall thin stature

Lower Airway Condition
Secondary Pneumothorax• Secondary pneumothorax occurs in the presence of existing lung
pathology
• Pneumonia is a possible cause of pneumothorax. Consider
Pneumocystis jiroveci pneumonia (PCP) , toxoplasmosis, and
Kaposi sarcoma in patients with human immunodeficiency virus
infection (HIV). A patient with HIV can have spontaneous
pneumothorax as the presenting symptom of their illness. HIV
carries a lifetime risk of 6% for pneumothorax, and about 85% of
that number is related to PCP pneumonia.

Lower Airway Condition
Secondary Pneumothorax
– Risk Factors
• History of Asthma, COPD, Cystic Fibrosis, TB, Whooping
cough
• Previous history of pneumothorax
• Smoking
• Lung Cancer
• HIV

Lower Airway Condition
Primary and Secondary Pneumothorax• Signs and symptoms vary greatly depending on how
much air enters the pleural space
– Sudden onset chest pain may describe as sudden, sharp, or
stabbing increases when taking deep breath
– Dyspnea
– Tachycardia
– Tachypnea
– Pulses paradoxes
– Hypoxia and altered mental status
– Absent or diminished lung sounds on affected side

Pneumothorax

Lower Airway Condition
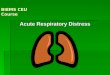
Asthma• Obstructive lower airway
diseases are characterized
by diffuse obstruction to
airflow within the lungs.
• The most common
obstructive airway diseases
are emphysema, chronic
bronchitis and asthma.

Lower Airway Condition
Asthma
• Asthma prevalence is higher in children than adults
• Children who have wheezing that begins prior to 5 years
old and persists into adulthood have increased risk of
developing asthma
• Children who have a lower incidence of pulmonary
disease even after age 5 have a lower incidence of
pulmonary disease even if the wheezing persists into
adulthood

Lower Airway Condition
Asthma
Signs and symptoms
– Wheezing
– Dyspnea
– Chest tightness
– Cough
• Signs of recent upper respiratory
infection
– Rhinorrhea, congestion,
headache , pharyngitis, and
myalgia
• Signs of exposure to allergens
– Rhinorrhea
– Pharyngitis
– Hoarseness
– Cough
– Chest tightness, discomfort, or
pain



Capnography

Lower Airway Condition
COPD• COPD is an airflow obstruction caused by chronic
bronchitis or loss of alveolar surface area associated with
emphysema
• Characterized by some degree of wheezing and airway
edema even though the mechanism is slightly different
from asthma

Lower Airway Condition
COPD• Factors indicating severe exacerbation of COPD
– Oxygen saturation <90%
– Tachypnea
– Peripheral or central cyanosis
– Mental status changes caused by hypercapnia
– ETCO2 waveform
– ETCO2 readings

Lower Airway Condition
COPD• Signs and symptoms
– Dyspnea
– Exertion intolerance
– Wheezing
– Productive cough
– Chest pain or discomfort
– Diaphoresis
– Orthopnea
– Increased respiratory rate
– Decreased oxygen saturation

Capnography

Treatment COPD
• Emergency management
– Oxygen to maintain saturation of 92%*
• An oxygen saturation that falls into the 80’s and pale or cyanotic
extremities requires aggressive airway and ventilation management
• CPAP has been shown to decrease work of breathing, increase
oxygenation and decreasing the need for intubation
• NEVER WITHOLD OXYGEN FROM A HYPOXIC PATIENT

CPAP
• Improves respiratory function in asthma/COPD
• Improvement seen due to:
– Decrease work of breathing/ reduction in fatigue
– Improved oxygenation
– Splinting of larger airways and bronchioles to reduce airway
collapse and mucous plugging

ADULT ACUTE ASTHMA COPD WITH WHEEZING
REACTIVE (LOWER) AIRWAY DISEASE
BLS 1. Adult Initial Medical Care SOP, p. 4-5
2. If patient has prescribed inhaler, obtain time of last usage. If appropriate, assist
patient with prescribed inhaler.
3. Reassess patient's respiratory status and begin transport
4. At discretion of Medical Control, additional doses of inhaler may be given
5. ALBUTEROL 2.5 mg (3 mL) via nebulizer per System-specific procedure
6. Consider possibility of congestive heart failure (CHF) / pulmonary edema in
wheezing patient, if patient has a history of CHF, and/or pulmonary edema. If so,
treat per PULMONARY EDEMA SOP, p. 22.
ALS 1. Adult Initial Medical Care SOP, p. 4-5 2. ALBUTEROL 2.5 mg (3 mL) via nebulizer 3. Partial response: repeat ALBUTEROL immediately 4. If no response to ALBUTEROL or patient in severe respiratory distress:
consider NIPPV / CPAP per System-specific procedure
If age ≤ 50 and patient has no history of cardiac disease, consider EPINEPHRINE 1:1000 0.3 mg IM
If age > 50 and/or cardiac disease history, contact Medical Control
5. If imminent respiratory arrest, INTUBATE and use in-line ALBUTEROL 2.5 mg (3 mL)

Hyperventilation syndrome
• Respiratory disorder, psychologically or physiologically
based, involving breathing to deeply or too rapidly
• Causes are unknown
• Sudden and everyday are two forms
• Causes carbon dioxide levels to decrease

Hyperventilation syndrome
• Lower levels of carbon dioxide reduce blood flow to the
brain resulting in nervous system and emotional
symptoms– Weakness
– Fainting
– Dizziness
– Confusion
– Agitation
– Feeling as if you can’t breathe

Hyperventilation
• Over breathing can also cause Calcium levels to drop in your blood which
results in these CNS symptoms
– Numbness and tingling (in arms and around mouth)
– Spasms or cramps in hands and feet
– Muscle twitching
• May also cause cardiac symptoms– Chest pain or tenderness
– Shortness of breath
– Wheezing

Hyperventilation Syndrome
• Symptoms usually last longer (hours as apposed to
minutes)
• Usually happens in younger people
• Improves with exercise
• Pain does not improve with medication

Hyperventilation Syndrome
• Medical conditions can cause hyperventilation
• In children a medical cause is more likely than stress
• Administer oxygen
• Paper bag treatment is no longer considered appropriate
• Tetany, paresthesia and carpopedal spasm may occur

Hyperventilation syndrome

Hyperventilation Syndrome

ALS Scenario
• Medic is dispatched for the 60 year old female with
shortness of breath
• Pt is in tripod position with increased work of breathing
and accessory muscle use, breathing at a rate of 40 and
unable to speak more than one word/sentence
• She tells to you I…..can……’t……….breathe

ALS Scenario
• HPI= per patient’s husband, patient awoke this morning
with shortness of breath and has experienced increased
work of breathing with exertion
• Patient has recent history of a cold, but husband
concerned she may now have pneumonia
• PMHX- diabetes, heart failure, hypertension
• Medications: Lasix 80 mg bid, digoxin 0.125mg daily,
Regular insulin 30u twice daily , Levaquin and an
albuterol inhaler

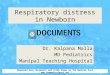
ALS Scenario
• VS 170/104 HR 118 RR 28 SPO2 87% RA
• ECG
• What are your treatment priorities

Case Scenario
• You are dispatched for the patient complaining of
shortness of breath at the local rehab facility You find a
40 year old, obese female, lying supine on her bed with
very labored respirations audible from outside the room
• The patient is staring at the ceiling and does not respond
to your presence Patient is pale with cyanosis around the
lips. Staff disappears when you get there

Scenario
• Assessment reveals
– Airway- Patent, no vomitus or obstruction
– Breathing- Shallow, very labored and rapid at 36 bpm with lung sounds
diminished and audible rales in all fields Perioral and peripheral cyanosis
present
– Circulation- Skin is pale, cool, diaphoretic No trauma or bleeding Pulse
difficult to palpate
– GCS = 3
– History CHF, COPD, recent hip replacement surgery

Case Scenario• Initial Capnography waveform
• Placed on Hi flow oxygen at 15
L/m via BVM

Scenario
• Potential causes
• Treatment
• Rapid transport

Questions?