Embed Size (px)
Citation preview
Evaluation of Dyspnea
Variable Definitions Of Dyspnea
• Unpleasant or uncomfortable respiratory sensations • Difficult, labored, uncomfortable breathing• Awareness of respiratory distress• The sensation of feeling breathless or air hunger• An uncomfortable sensation of breathing
• ATS guidelines: subjective experience of breathing discomfort that consists of qualitatively distinct sensations that vary in intensity
ATS. AJRCCM, 1999.

Variation In Symptoms of Dyspnea by Condition
Manning. NEJM, 1995.

Respiratory Control Systems
• Designed to maintain gas exchange equilibrium and acid base status
• Abnormalities in this system -> dyspnea-> severe patient distress

Mechanisms Of Dyspnea: Respiratory Center Output
• Chemoreceptors– Peripheral: carotid
bodies, aortic arch • Sense changes in PO2,
acidosis, hypercapnea– Central: medulla
• pH and PCO2 changes• Hypercapnea
– Potent stimulus of dyspnea
• Hypoxia– Less potent stimulus
than hypercapnea
Manning. NEJM, 1995.
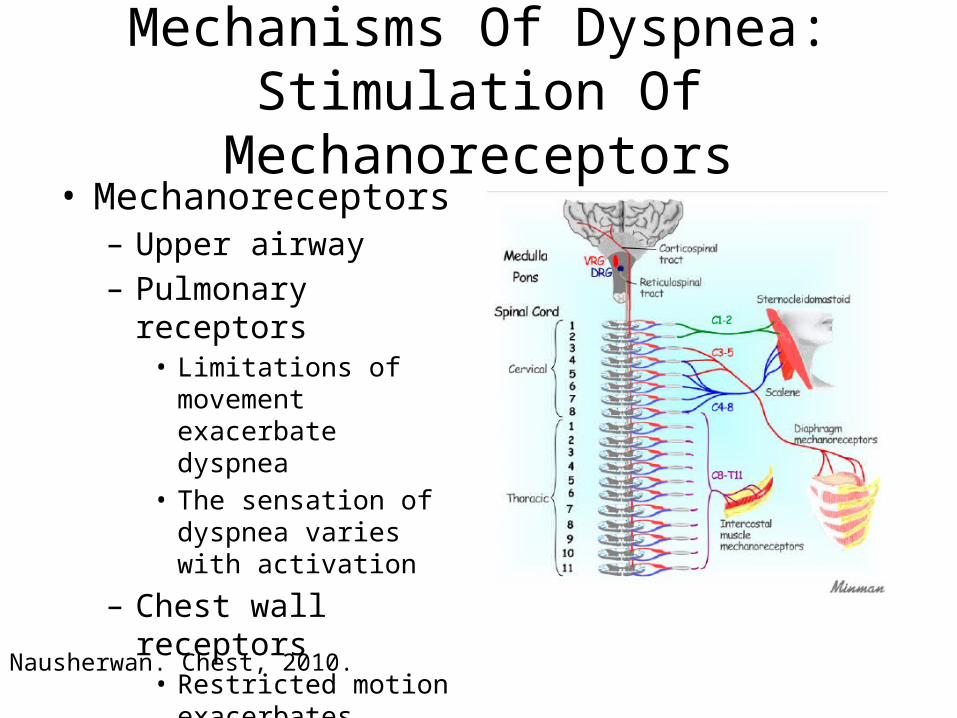
Mechanisms Of Dyspnea: Stimulation Of Mechanoreceptors
• Mechanoreceptors– Upper airway– Pulmonary receptors
• Limitations of movement exacerbate dyspnea
• The sensation of dyspnea varies with activation
– Chest wall receptors• Restricted motion
exacerbates dyspnea• Redundant to pulmonary
receptors
Nausherwan. Chest, 2010.
Other Mechanisms Of Dyspnea
• Mechanical loading– Changes in airway resistance, pulmonary or chest wall
compliance• Neuromechanical dissociation
– Air flow not equal to expected results of brain output• Impaired oxygen utilization or delivery
– Anemia• Increased CO -> EDP-> pulmonary edema• Localized acidosis or resp muscle fatigue
– Deconditioning• Poor cardiac and peripheral efficiency, early anaerobic metabolism
and acidosis
Structural Approach
• Respiratory– Controller: depth and rate of breathing– Ventillatory pump: movement of gas in and out of
the alveolous– Gas exchanger: pulmonary vasculature, alveoli
• Cardiac– Anemia– Deconditioning– Heart failure

Most Common Causes of Dyspnea
• Asthma• COPD• ILD• Cardiac disease
Differential Diagnosis of Dyspnea
• Cardiac– Heart failure– Coronary artery disease– Arrhythmia– Pericardial disease– Valvular heart disease– Pulmonary hypertension

Diagnosis of Dyspnea
• Pulmonary– Chronis obstructive pulmonary disease– Asthma– Interstitial lung disease– Pleural effusion– Malignancy– Bronchiectasis

Diagnosis of Dyspnea• Non-cardiac/Non-pulmonary
– Thromboembolic disease– Psychogenic– Deconditioning – Obesity– Anemia– GERD– Metabolic conditions– Cirrhosis– Thyroid disease– Neuromuscular – Chest wall– Upper airway

Approach To The Patient
• History and physical• EKG• Echocardiogram• CXR/CT scan• Spirometry• Cardiopulmonary exercise testing
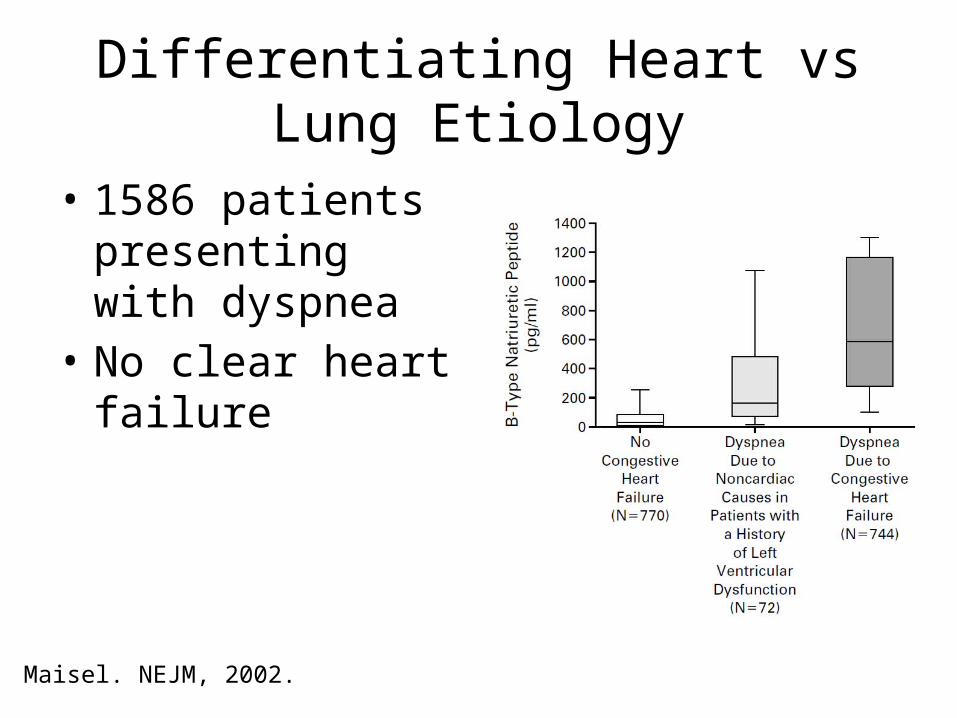
Differentiating Heart vs Lung Etiology
• 1586 patients presenting with dyspnea
• No clear heart failure
Maisel. NEJM, 2002.
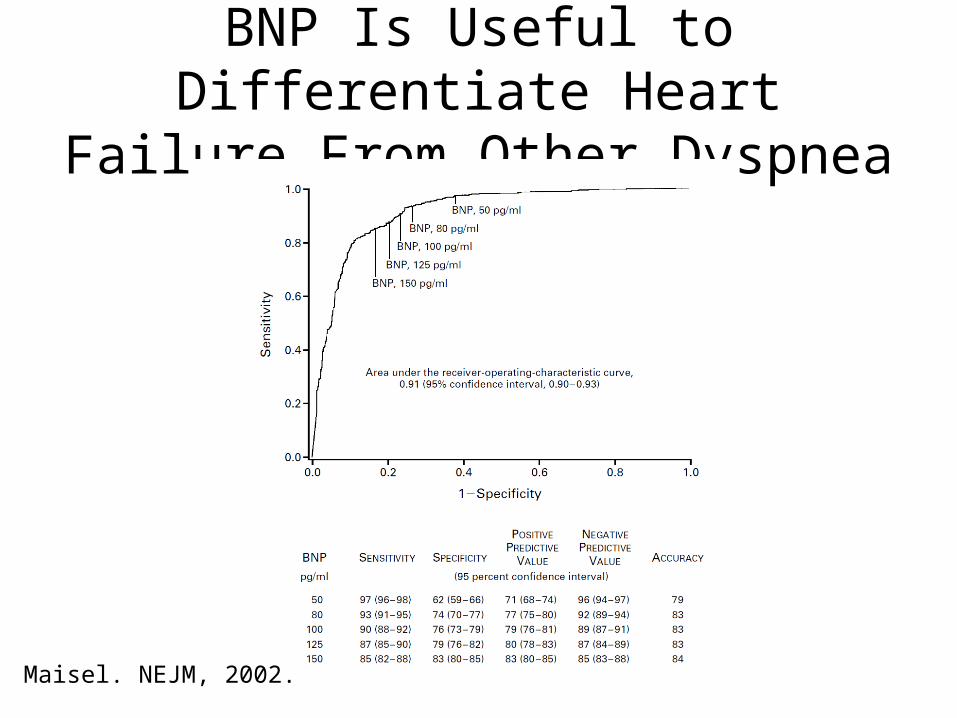
BNP Is Useful to Differentiate Heart Failure From Other Dyspnea
Maisel. NEJM, 2002.
Case 1
• A 30 year old woman presents with progressive exercise tolerance for the last 3 months. She ran a marathon at age 26, but now has shortness of breath walking up 1 flight of stairs. She denies chest pain, orthopnea or PND but has intermittent mild ankle edema.

Case1
• Her blood pressure is normal and her exam is unremarkable. Her EKG and CXR are shown. What test should be ordered next?– A treadmill stress test– Pulmonary function testing– A blood test for BNP– A CT scan of the chest– An echocardiogram

Electrocardiogram

Chest XR

Case 1
• What test should be ordered next?– A treadmill stress test– Pulmonary function testing– A blood test for BNP– A CT scan of the chest– An echocardiogram

Case 1
• An echocardiogram is performed.

Echocardiogram

Case 1
• The next best step is to:– Start sildenafil 20 mg TID– Send the patient for a right heart catheterization– Send tests for rheumatologic disease– Start an ACE Inhibitor

Hemodynamics
RA (mmHg) 9
PA (mmHg) 92/44 (65)
PCWP (mmHg) 7
CO (L/min) 3
PVR (Wood Units)
19

Right Sided Heart Failure
• Most commonly associated with left sided heart failure
• Pulmonary hypertension is another common cause
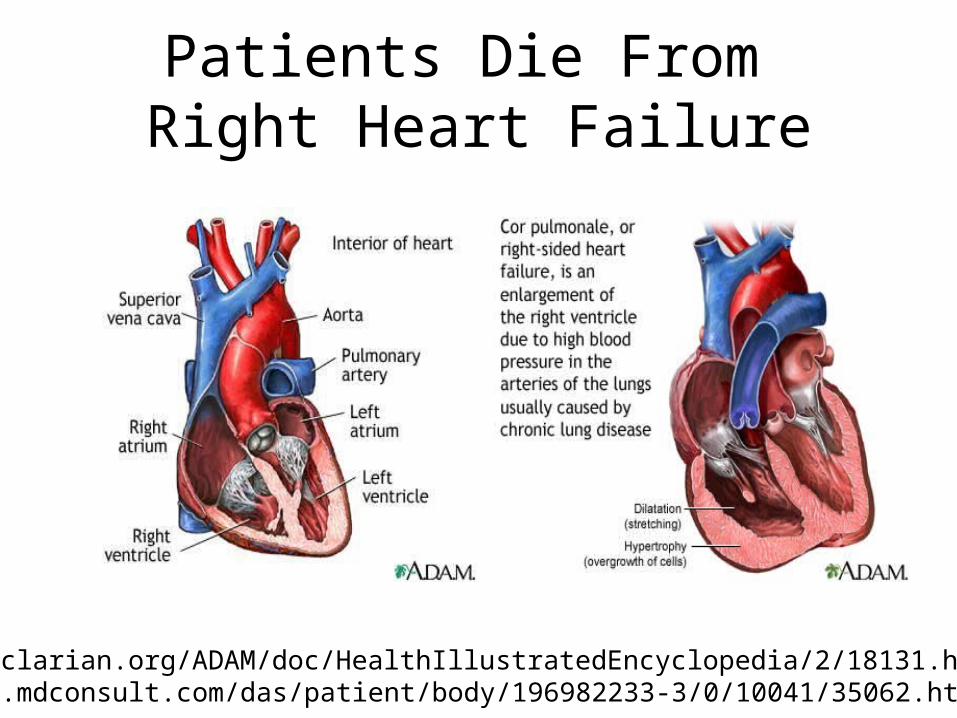
Patients Die From Right Heart Failure
www.clarian.org/ADAM/doc/HealthIllustratedEncyclopedia/2/18131.htmwww.mdconsult.com/das/patient/body/196982233-3/0/10041/35062.html

WHO Classification of PH
I. Pulmonary arterial hypertension
1. Idiopathic2. Heritable3. Drug/toxin induced4. Associated (HIV, CTD,
CHD, schistosomiasis)I . ′ PVOD, PCHII. PH from left heart
disease1. Systolic dysfunction2. Diastolic dysfunction 3. Valvular disease
III. PH from lung disease or hypoxemia
1. ILD2. COPD3. OSA4. Altitude
IV. CTEPHV. Multifactorial
1. Hematologic2. Systemic (sarcoid,
vasculitis)3. Metabolic (glycogen
storage)4. Other (tumor)
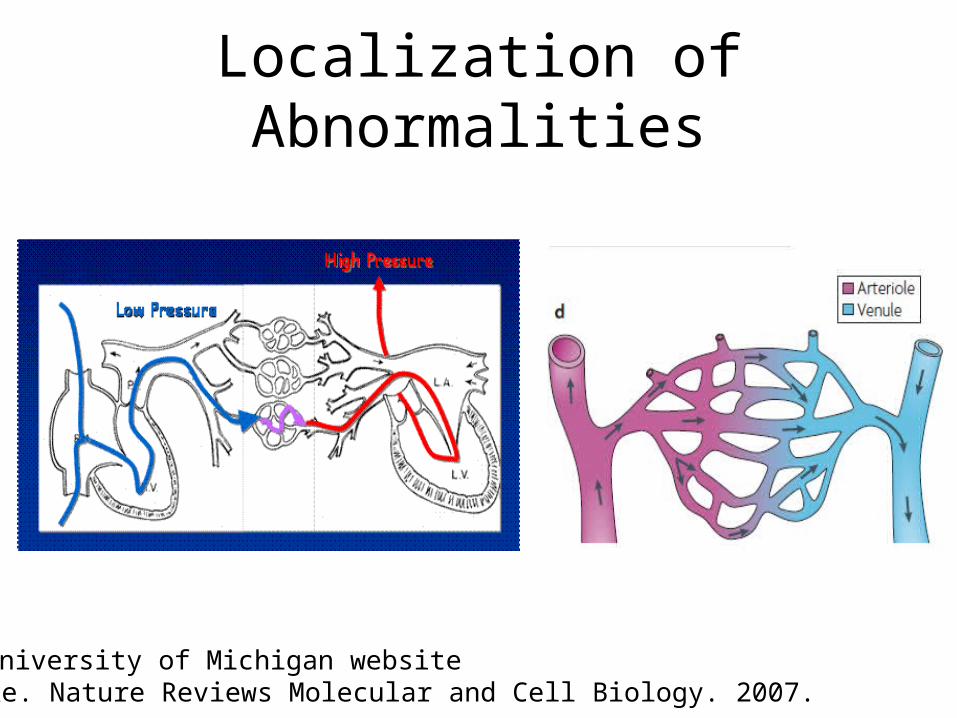
Localization of Abnormalities
Dijke. Nature Reviews Molecular and Cell Biology. 2007.University of Michigan website
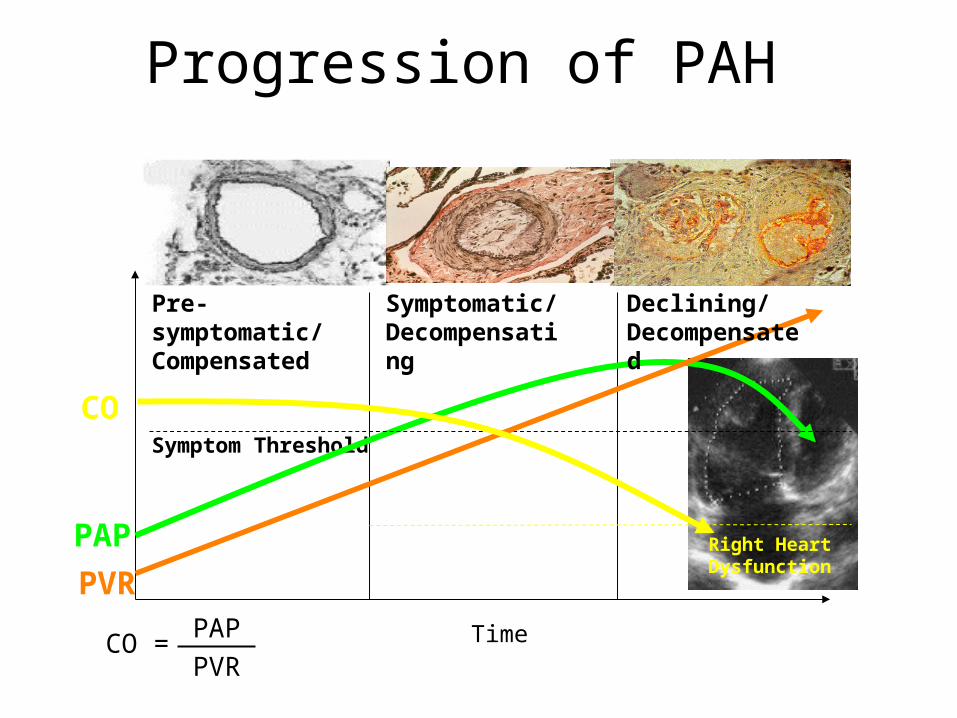
Progression of PAH
PAP
PVR
CO
Time
Pre-symptomatic/ Compensated
Symptomatic/ Decompensating
Symptom Threshold
Right Heart Dysfunction
Declining/ Decompensated
CO =PAP
PVR

Humbert. NEJM, 2004.
Targets for Therapies in Pulmonary Arterial Hypertension

Acute Pulmonary Embolism

Case 2
• A 68 year old HTN, diabetic female presents with progressive shortness of breath over the last 5 years. She can walk about 2 blocks before needing to rest.

Case 2
• The examination shows tachycardia and a normal blood pressure. There are bibasilar crackles and an S3 on exam.

EKG


Case 2
• There was trace LE edema. The EKG shows LVH. An echocardiogram shows LVH and severe diastolic dysfunction.

Case 2
• The next best step is:– A nuclear stress test– Aggressive blood pressure management– A coronary angiogram– Aggressive management of diabetes

Diastolic Heart Failure
• Nearly ½ of all patients with heart failure
• 65% 5 year mortality
Shah. JAMA, 2008.
Typical Features Of Patients With Diastolic Heart Failure
• Female: 62-66%• Elderly: mean age 72-74• Comorbidities
– CAD 36-53%– HTN 55-77%– AF 32-41%– DM 32-45%– CKD 23-26%– Obesity– Anemia

Mortality In Diastolic Heart Failure Is High
Owan. NEJM, 2006.
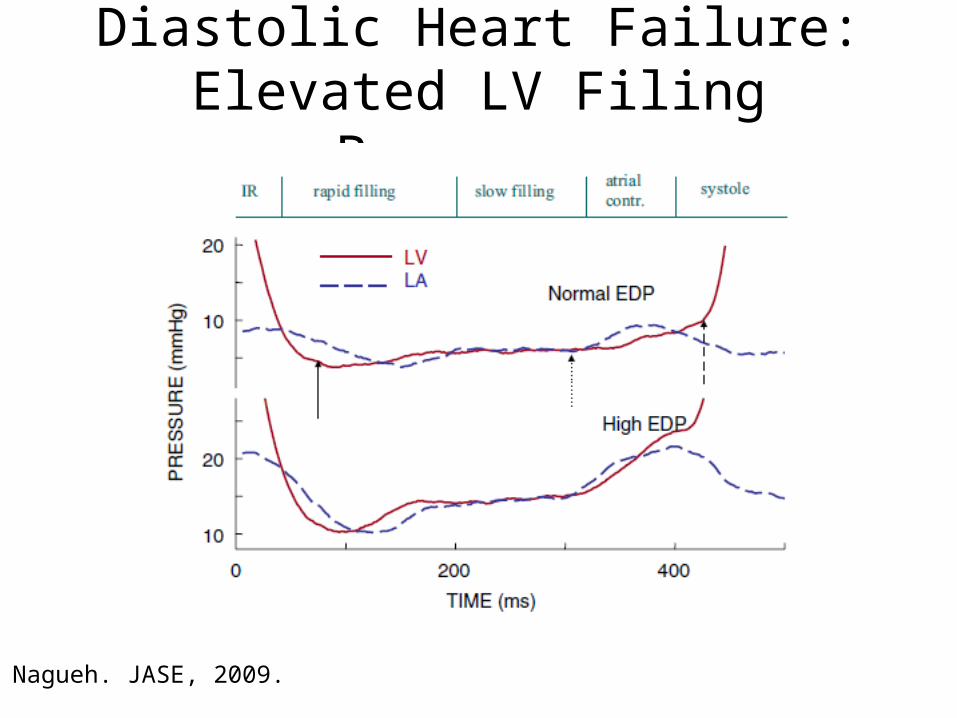
Diastolic Heart Failure: Elevated LV Filing Pressures
Nagueh. JASE, 2009.

What Does DHF Look Like On Echo?
Nagueh. JASE, 2009.

Treatment
• Treatment of comorbidities