Embed Size (px)
Citation preview

ED Stream WorkshopAcute MOC
August 2013
ED Stream Workshop
John Hunter Hospital
Emergency Department
1

List All MOC used in your Facility
NSW Health Models of Care
1. Triage and Registration
2. Clinical Initiatives Nurse
3. Resuscitation & trauma
4. Acute care
5. Early Emergency Department Senior Assessment and Streaming
6. Fast Track
7. Sub-acute
8. 2:1:1
9. Emergency department Short Stay Units
2

JHH ED FT Key Principles
1. Patient selection
2. Business rules, guidelines & expectations to patient management
3. Optimising use of beds
4. Medical and Nursing senior clinical decision makers
5. Minimizing wastage
6. Improving equipment
7. Improving utilisation of current resources
3

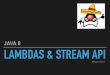
John Hunter ED Fast Track Model
1. Patient selection: new criteria July 2013
4
YES NO Pre-empt (in the WR)
Limb injuries Joint Sprains
Limb injury
finger/toe injury
Minor contusion/abrasions
Follow up post #
No neurovascular compromise Not severely deformed/dislocated Not elderly who cannot mobilize or unable to cope at home No acute medical cause for fall Not a septic joint
Organise X-Rays & analgesia (as per NIX and NIA guidelines)
Skin Simple laceration to face, trunk, limb
Scalp laceration
Suture removal
No neurovascular compromise Not septic/ unwell Not immune-compromised Not requiring procedural sedation
Cellulitis No significant co-morbidities Not septic/ unwell Not immune-compromised Not peri-orbital, orbital
Skin or subcutaneous abscess
No significant co-morbidities Not septic, unwell Not immune-compromised
NBM for sedation
Skin burn; <5% TBA superficial/partial thickness
Not face, groin, fingers, toes, or overlying joints
Analgesia Wet dressings
Dressings change Bites/stings Needle stick injury
Pulmonary Cough
Not tachypnoeic Not hypoxic; saturations > 95% Not septic, unwell looking No significant co-morbidities Not immune-compromised
If the patient is febrile or has crepitations on auscultation then ask FT Doctor for a CXR request form
Throat pain No stridor or airway compromise No significant co-morbidities Not unable to swallow
Isolated rib injury Must be < 50yo Not requiring narcotic analgesia Not tachypnoeic Not hypoxic; O2 sats < 95% No significant co-morbidities
Ask the FT Doctor for a CXR request form to exclude a pnuemothorax Analgesia(as per NIA guidelines)
Gastro-intestinal Vomiting and diarrhoea Must be < 50 yo No significant co-morbidities Abnormal vital signs
Anti-emetics Trial of fluids
Gastro-intestinal Vomiting and diarrhoea
Must be < 50 yo No significant co-morbidities Abnormal vital signs Abdominal pain Not septic, unwell looking
Anti-emetics Trial of fluids
Abdominal pain Not requiring narcotic analgesia No exacerbation of pain on movement, walking or coughing Normal vitals including fever Non complicated abdominal or surgical history No recent abdominal surgery
Bloods (as per C-Path matrix) Urine bHCG
Haemorrhoids 1° or 2°
Genito-urinary UTI Not septic Normal vital signs Non complicated urological Hx, No significant co-morbidities No flank pain
Urine
Flank pain + haematuria Must be < 50yo No history of AAA
Urine Analgesia
head Minor head injury Must be < 65yo normal GCS or mentation No meningism No focal neuro abnormalities, No vomiting, LOC > 5mins No amnesia > 30mins Not anti-coagulated No underlying acute medical problem causing the fall
Dental Toothache Not septic Analgesia
Ophthalmology Conjunctivitis
Corneal FB
Corneal abrasions
Hyphema
Peri-orbital cellulitis
Chemical splash
No Major facial trauma
ENT Nasal, ear FB
Isolated nasal #
Rash Urticarial rash Non blanching rash
YES NO Pre-empt (in the WR)
Limb injuries Joint Sprains
Limb injury
finger/toe injury
Minor contusion/abrasions
Follow up post #
No neurovascular compromise Not severely deformed/dislocated Not elderly who cannot mobilize or unable to cope at home No acute medical cause for fall Not a septic joint
Organise X-Rays & analgesia (as per NIX and NIA guidelines)
Skin Simple laceration to face, trunk, limb
Scalp laceration
Suture removal
No neurovascular compromise Not septic/ unwell Not immune-compromised Not requiring procedural sedation
Cellulitis No significant co-morbidities Not septic/ unwell Not immune-compromised Not peri-orbital, orbital
Skin or subcutaneous abscess
No significant co-morbidities Not septic, unwell Not immune-compromised
NBM for sedation
Skin burn; <5% TBA superficial/partial thickness
Not face, groin, fingers, toes, or overlying joints
Analgesia Wet dressings
Dressings change Bites/stings Needle stick injury
Pulmonary Cough
Not tachypnoeic Not hypoxic; saturations > 95% Not septic, unwell looking No significant co-morbidities Not immune-compromised
If the patient is febrile or has crepitations on auscultation then ask FT Doctor for a CXR request form
Throat pain No stridor or airway compromise No significant co-morbidities Not unable to swallow
Isolated rib injury Must be < 50yo Not requiring narcotic analgesia Not tachypnoeic Not hypoxic; O2 sats < 95% No significant co-morbidities
Ask the FT Doctor for a CXR request form to exclude a pnuemothorax Analgesia(as per NIA guidelines)
Gastro-intestinal Vomiting and diarrhoea Must be < 50 yo No significant co-morbidities Abnormal vital signs
Anti-emetics Trial of fluids

John Hunter ED Fast Track Model
• Business Rules and Expectations• Fast Track Trial 2012, staff survey 2013• New Business rules JHH ED July 2013• 30-60 minutes in assessment cubicles• Staff roles• Process mapping of top 10 DRGs• Improving patient flow in FT utilising waiting room, patient recliners, ESSU• Minimizing wastage• Improving equipment &utilisation of current resources
5
John Hunter Hospital Emergency Department
Fast Track
Fast track (FT) is a dedicated area in the Emergency Department for the treatment of Ambulant, non-complex, single problem patients who can be discharged within <2 hours.
Senior Staffing, revised processes and pathways, room equipment and layout are designed for rapid turnaround of patients. The Key Performance Indicators (KPI’s) for the Fast Track area is for 90% of patients to be discharged within 4 hours.
Triage allocates patients into the FT area using a pre-determined inclusion/exclusion criterion (see below). FT provides an alternative option to treat non-complex patients in a timely manner, reducing long waiting times for minor problems. The Fast Track Model of Care has been aligned to the NSW Emergency Department Model of Care Guidelines.
Key Principles of Fast TrackExpedite the patient journey for less-urgent/non-complex patientsUsing dedicated staff (seconded to FT for 3 month blocks) Working within team based careClearly defined roles with expected performance measuresOperating hours which reflect high demand periods (0800-2400hrs)Uses quarantined space where patients are treated in a dedicated area by dedicated staffCommence treatment earlyStrict inclusion and exclusion criteria supported by business rulesUse of clinical protocols that promote initiation of nursing careRapid access to appropriate imaging and pathologyPatients with a single system problem that can be discharged <2 hoursEasy access to specialty outpatient, GP and community care referral services
Information managementiPM will be used to enter all patient informationUse of standardised communication for medical and nursing staff- ISBARCAP- system to be used for reviewing pathology and imaging results, as well as formulating discharge paperwork

John Hunter ED Fast Track Model
• Optimising use of limited bed space– Competing need for beds
orthopaedics/subspecialist vs. ED– Minimising time wasted waiting in a bed
• 4 ED assessment beds• 1 specialty assessment/treatment bed• 7 recliner beds• 8 waiting room beds
– New operational rules for patient flow, bed use• Senior Nurse as flow coordinator and protector of bed space
6

John Hunter ED Fast Track Model
• Senior Decision Makers– 2012 JHH ED Fast Track Trial
• Senior staff work over twice as fast as junior staff• “dedicated senior medical and nursing staff working to optimise the
performance of Fast Track systems as they have the ability to make timely treatment and disposition decisions with minimal consultation” Considine et al 2010
– 2 teams consisting of 1 senior Doctor and 1 senior Nurse each promoting team work
– Feasibility study in utilising Nurse Practitioners?
7

John Hunter ED Fast Track Model
• Minimising wastage– Senior staff order less pathology and imaging tests– Reduce time wastage
• Protecting assessment & treatment beds for patients receiving active management
• Improved collaboration between doctors and nurses; eliminating time wasted by the nurse waiting for the doctor to finish their assessment before nursing duties are completed
8

John Hunter ED Fast Track Model
• Equipment to improve efficiency– Desk, computer, phone, Otoscope/Opthalmoscope in
each ED assessment room– 1 dressing-suture trolley each team– Assessment-treatment bed for orthopaedics– IT screen displaying time stamps of FT patients– Fact sheets/handouts incorporated in D/C summaries– Portable Tonopen– DECT phone to improve communication between
triage/ED coordinator/ESSU/SAS
9

John Hunter ED Fast Track Model
Improved utilisation of current resources– Enhanced Physiotherapy role
• uses existing resources to
manage minor limb injuries• New Guidelines July 2013• Significant improvements in
patient care and flow will lead
to a submission for weekend cover
10

Benefits of the Model
2012 Fast Track trial• Improved patient flow• Improved waiting times• Improved 4 hour National Emergency Access
Targets• Optimising use of FT bed space
11

Challenges
• Implementation and training of staff in new business rules and guidelines• Sustainability when Doctors constantly rotate through FT• Large number of subspecialty reviews and transfers to JHH ED FT
– Orthopaedics: 8.7 patients a day, ⅓ transfers, ⅓ GP referrals, 39% meet NEAT
– Uncontrolled variables: delayed registrar reviews, admissions and transfers to ward
– ED has no control over patient flow of the patients requiring subspecialty review
– Solution is to open ‘rapid access clinics’
• Limited space• Does not operate during the night 2400-0800
12

Clinician run model
13

Differences between your Model and the definition in the “Emergency Department Models of Care July 2012”
Consistencies•Staffing
– Dedicated senior medical & nursing staff– Physiotherapy
•Designated and segregated treatment area•Pathways and process mapping; need to develop standing order protocols for early nursing care•Strict inclusion/exclusion criteria
14

Identify the Resource Required for your Fast Track Model
•Staffing: model of 2 doctors and 2 nurses implemented July
•Training & implementation of new business rules and guidelines
•Development of new guidelines and standing orders for nurses
•Physical space and procedure room
•Clinical operation plans
15

Monitoring and Evaluation
Daily statistics•Number of patients through FT•Number discharged within 2hrs & 4hrs•Waiting time•Admissions•Did not waits•Patient incidences and complaints•Weekly staff feedback•Number of Orthopaedic patients, admission rate, NEAT•Number of Opthalmology, admission rate, NEAT
16

Evidence of Success
Review in October
17