Embed Size (px)
Citation preview
Ÿ Ebstein’s Anomaly by virtue of its rarity, remains an ignored disease with vague management guidelines.
Ÿ Inspite of it being acknowleged as a cardiomyopathy, criteria for doing a Bidirectional Glenn are not defined.
● Gender : 5(27.8%) females and 13 (72.2%) males
● Age : Median age - 14 (range 5 to 27) years
Ÿ To describe a for Ebstein’s ‘Comprehensive Repair Protocol’anomaly and report our early results.
Ÿ To emphasize that ‘Z’ value of ‘True Tricuspid Annulus’ (TTA)can be used as an objective parameter to decide the need for a Bidirectional Glenn shunt [one and half ventricle repair].
Ÿ Prospective cohort studyŸ 18 consecutive patients undergoing surgery for Ebstein’s
anomaly.Ÿ Echocardiography done to define the type and severity of the
disease, TTA dimension and its ‘Z’ score. Postoperatively atŸ Electrophysiological studies were performed, if indicated.
Patients were operated in a comprehensive manner to create a one and a half ventricle heart : i. Delaminationii. Longitudinal plication of the atrialized right ventricleiii. to create a reduced neo annulusSuture annuloplastyiv. Complete tricuspid repairtrileafletv. to finally reinforce the repairRing annuloplastyvi. Bidirectional Glenn vii. Right atrial reduction plasty viii. Arrhythmia correction procedures (if indicated).
AIM :
Patients and Methods :
Operative Technique :
Patient Profile
Background
Ebstein’s Anomaly - “The One and a Half Ventricle Heart”A. Malhotra, V. Agrawal, K. Patel, M. Shah, M. Hinduja, V. Wadhawa, J. Khandeparkar, N. Oswal
U. N. Mehta Institute of Cardiology and Research Center, Ahmedabad, India
TTA Z SCORE
CARPENTIER CLASS
NO OF PATIENTS
> +4
> +4
+2 to +4
+2 to +4
D
C
C
B
1 [5.5%]
7 [38.9%]
6 [33.3%]
4 [22.2%]
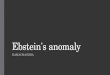
SVC
RIGHTATRIUN
FRV
STL
ARVIVC
STLSTL
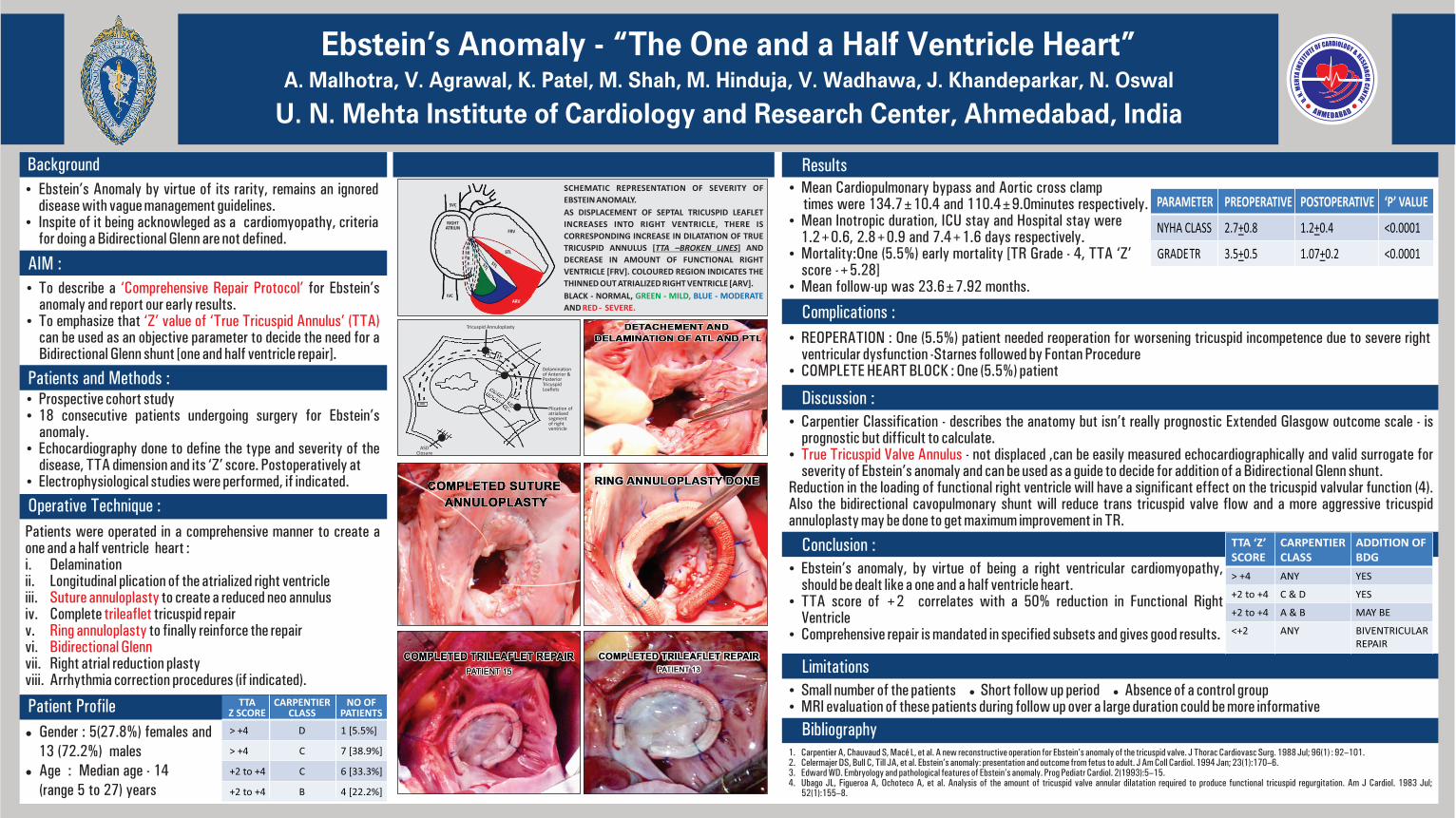
SCHEMATIC REPRESENTATION OF SEVERITY OF
EBSTEIN ANOMALY.
AS DISPLACEMENT OF SEPTAL TRICUSPID LEAFLET
INCREASES INTO RIGHT VENTRICLE, THERE IS
CORRESPONDING INCREASE IN DILATATION OF TRUE
TRICUSPID ANNULUS [TTA –BROKEN LINES] AND
DECREASE IN AMOUNT OF FUNCTIONAL RIGHT
VENTRICLE [FRV]. COLOURED REGION INDICATES THE
THINNED OUT ATRIALIZED RIGHT VENTRICLE [ARV].
BLACK - NORMAL, GREEN - MILD, BLUE - MODERATE
AND RED - SEVERE.
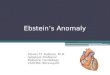
Tricuspid Annuloplasty
Delaminationof Anterior & Posterior TricuspidLeaflets
Plication of atrialised segment of right ventricle
ASDClosure
Ÿ Small number of the patients ● Short follow up period ● Absence of a control groupŸ MRI evaluation of these patients during follow up over a large duration could be more informative
1. Carpentier A, Chauvaud S, Macé L, et al. A new reconstructive operation for Ebstein’s anomaly of the tricuspid valve. J Thorac Cardiovasc Surg. 1988 Jul; 96(1) : 92–101. 2. Celermajer DS, Bull C, Till JA, et al. Ebstein’s anomaly: presentation and outcome from fetus to adult. J Am Coll Cardiol. 1994 Jan; 23(1):170–6. 3. Edward WD. Embryology and pathological features of Ebstein’s anomaly. Prog Pediatr Cardiol. 2(1993):5–15. 4. Ubago JL, Figueroa A, Ochoteco A, et al. Analysis of the amount of tricuspid valve annular dilatation required to produce functional tricuspid regurgitation. Am J Cardiol. 1983 Jul;
52(1):155–8.
Limitations
Bibliography
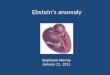
Ÿ REOPERATION : One (5.5%) patient needed reoperation for worsening tricuspid incompetence due to severe right ventricular dysfunction -Starnes followed by Fontan Procedure
Ÿ COMPLETE HEART BLOCK : One (5.5%) patient
Ÿ Carpentier Classification - describes the anatomy but isn’t really prognostic Extended Glasgow outcome scale - is prognostic but difficult to calculate.
Ÿ - not displaced ,can be easily measured echocardiographically and valid surrogate for True Tricuspid Valve Annulus severity of Ebstein’s anomaly and can be used as a guide to decide for addition of a Bidirectional Glenn shunt.
Reduction in the loading of functional right ventricle will have a significant effect on the tricuspid valvular function (4). Also the bidirectional cavopulmonary shunt will reduce trans tricuspid valve flow and a more aggressive tricuspid annuloplasty may be done to get maximum improvement in TR.
Ÿ Ebstein’s anomaly, by virtue of being a right ventricular cardiomyopathy, should be dealt like a one and a half ventricle heart.
Ÿ TTA score of +2 correlates with a 50% reduction in Functional Right Ventricle
Ÿ Comprehensive repair is mandated in specified subsets and gives good results.
Results
Complications :
Discussion :
Conclusion : TTA ‘Z’SCORE
CARPENTIER CLASS
ADDITION OF BDG
> +4 ANY YES
+2 to +4 C & D YES
+2 to +4 A & B MAY BE
<+2 ANY BIVENTRICULAR REPAIR
Ÿ Mean Cardiopulmonary bypass and Aortic cross clamp times were 134.7±10.4 and 110.4±9.0minutes respectively.Ÿ Mean Inotropic duration, ICU stay and Hospital stay were 1.2+0.6, 2.8+0.9 and 7.4+1.6 days respectively.Ÿ Mortality:One (5.5%) early mortality [TR Grade - 4, TTA ‘Z’
score -+5.28] Ÿ Mean follow-up was 23.6±7.92 months.
PARAMETER PREOPERATIVE POSTOPERATIVE ‘P’ VALUE
NYHA CLASS 2.7+0.8 1.2+0.4 <0.0001
TRGRADE 3.5+0.5 1.07+0.2 <0.0001