Embed Size (px)
Citation preview

266
Early Reduction for Congenital Dislocation of the Knee withinTwenty-four Hours of Birth
Chun-Chien Cheng, MD; Jih-Yang Ko1, MD
Background: Congenital dislocation of the knee (CDK) is a very rare condition that com-prises a spectrum of deformities from subluxation to complete dislocation.The incidence of CDK is estimated at 1 per 100,000 live births, which is 1%of the incidence of developmental dysplasia of the hip (DDH). Moreover,40–100% of patients with CDK have additional musculoskeletal anomalies,the most common being DDH and clubfoot. In general, the diagnosis isestablished immediately after birth according to the position of the kneerecurvatum. Treatment with conservative methods at an early stage is mostlikely to yield successful results. We report here successful treatment of aseries of CDK patients with early reduction.
Methods: From July 1990 to June 2007, 19 patients with CDK (affecting 25 knees)were treated with early reduction. Of these, 6 knees had dislocation, and 19had subluxation. Since 1990, treatment has been guided by a protocol thatconsiders patient age and the severity of the condition. In patients examinedwithin 24 hours of birth, early, direct reduction under gentle, persistent man-ual traction was attempted. Birth history and perinatal course were obtainedfrom medical records. Associated musculoskeletal anomalies were observedand treated after reduction of the knee joint. A Pavlik harness was used for atleast 4 months in the concomitant treatment of DDH and CDK. Knee func-tion was graded as excellent, good, fair, or poor. Radiographs were used toassess DDH during follow-up.
Results: After an average follow-up duration of 4.3 years, 18 patients showed anexcellent or good outcome. One patient, whose knee could not be reduced,had severe multiple anomalies and died 16 days after birth. Fifteen of thenineteen patients had associated musculoskeletal anomalies, including DDHand foot deformity. Two cases of residual hip dysplasia after Pavlik harnessapplication required an acetabular osteotomy.
Conclusions:For CDK patients, early and direct closed reduction within 24 hours of birthaffords outcomes graded as either excellent or good.(Chang Gung Med J 2010;33:266-73)
Key words: congenital dislocation of the knee (CDK); developmental hip dysplasia (DDH)
From the Department of Orthopedic Surgery, Antai Medical Care Cooperation, Antai Tian-Sheng Memorial Hospital; 1Departmentof Orthopedic Surgery, Chang Gung Memorial Hospital – Kaohsiung Medical Center, Chang Gung University College of Medicine,Kaohsiung, Taiwan.Received: Mar. 28, 2009; Accepted: Jul. 6, 2009Correspondence to: Dr. Jih-Yang Ko, Department of Orthopedic Surgery, Chang Gung Memorial Hospital – Kaohsiung MedicalCenter. 123, Dapi Rd., Niaosong Township, Kaohsiung County 833, Taiwan (R.O.C.) Tel.: 886-7-7317123 ext. 8003; Fax: 886-7-7354309; E-mail: [email protected]
Original Article

Chang Gung Med J Vol. 33 No. 3May-June 2010
Chun-Chien Cheng, et alCongenital dislocation of the knee
267
Congenital dislocation of the knee (CDK) wasfirst described by Chatelaine in 1822. It is a rare
condition that comprises a spectrum of deformitiesfrom subluxation to complete dislocation.(1-10) Theincidence of CDK is estimated at 1 per 100,000 livebirths, which is 1% of the incidence of developmen-tal dysplasia of the hip (DDH).(2,11) Moreover,40–100% of patients with CDK have additional mus-culoskeletal anomalies,(2-4) the most common beingDDH and clubfoot.
Although there are some reports of occurrenceswithin families, most cases of CDK are sporadic.(3-6)
The deformity may be unilateral or bilateral, and pre-dominantly affects girls. In general, the characteristicpresentation of genu recurvatum facilitates the recog-nition of CDK (Fig. 1A).(7-11) A dimple or deep creasemay be present over the anterior aspect of the knee.Many modalities can be utilized for conservativetreatment, including serial casting, a Pavlik harness,skin traction, and skeletal traction.(1,3,6,7,11-14) Haga et al.advised waiting 1 month for spontaneous reductionof CDK in cases not associated with clubfoot orLarsen’s syndrome.(12) However, Laurence claimed
that the prognosis of CDK is adversely affected by adelay in treatment,(7) and by the presence of certainassociated deformities or generalized joint laxity.This difference of opinion can make the treatment ofCDK confusing. We report here on our experience intreating a series of CDK patients with early reduc-tion, and their outcomes.
METHODS
We retrospectively reviewed 19 infants withCDK (affecting 25 knees) who had been treated withearly reduction at our institution between July 1990and June 2007. There were 5 boys and 14 girls. Thebirth history and perinatal course were obtained frommedical records.
The severity of knee deformity was classified aseither subluxation or dislocation according to thetibiofemoral articular relationship.(1,3,7) The diagnosiswas dislocation if the tibia was displaced anterior tothe long axis of the femur (Fig. 2A), and subluxationif longitudinal contact was at least partially main-tained (Fig. 1B). There were 6 knees with disloca-
A B C
D E F
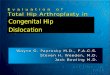
Fig. 1 Case 19 (A) The characteristic appearance of bilateral CDK at birth. (B) Radiograph before reduction demonstrating anteri-or subluxation in the bilateral knees. (C) The closed reduction starts with gentle, persistent manual traction. (D) During traction, ananteriorly directed force is applied to the distal femur, and a posteriorly directed force to the proximal tibia. (E) Reduction of thedislocated knee is achieved with flexion > 90°, and the extremity is immobilized with a splint. (F) Follow-up radiograph showingnormal alignment of both knees at 9 months of age.

Chang Gung Med J Vol. 33 No. 3May-June 2010
Chun-Chien Cheng, et alCongenital dislocation of the knee
268
tion, and 19 knees with subluxation. Of 6 patientswith bilateral knee problems, bilateral knee subluxa-tion was noted in 5, and bilateral knee dislocation in1. Associated musculoskeletal anomalies were notedin 15 patients.
A general treatment protocol that considerspatient age and condition severity was established byour senior author (J.Y. Ko).(1) For patients examinedwithin 24 hours of birth, early and direct reductionunder gentle, persistent manual traction was attempt-ed (Fig. 1C). During this approach, an anteriorlydirected force was applied to the distal femur, and aposteriorly directed force to the proximal tibia, in aneffort to effect reduction of the dislocation or sublux-ation (Fig. 1D). Reduction of the dislocated knee wasachieved with flexion > 90°. The extremity was thenimmobilized in a dorsal long leg splint or cast, withknee flexion > 90° (Fig. 1E). The reduction of CDKwas confirmed following radiographic examination.Toe circulation was checked to avoid compartmentsyndrome. The casting or splinting was changedevery 2 weeks over a 6 to 8-week period if therewere no associated musculoskeletal anomalies. Allpatients were monitored for any unexpected sequelaeor complications. If there were no associated anom-alies, the patient was examined every 2 months untilof walking age, and then examined annually.Radiographs of the knee were taken before and afterreduction of the knee joint, every 4 months duringthe first year of follow-up, and then annually. Nospecific rehabilitation was administered unless therewas an associated musculoskeletal anomaly that
influenced motion or stability of the knee; this wasthe case for 1 patient with arthrogryposis multiplexcongenita. Fourteen patients received concomitanttreatment using a Pavlik harness for associatedDDH; the treatment was initiated from the age of 6weeks and was maintained for at least 4 months.The follow-up period ranged from 9 months to 14years (average, 4.3 years).
Knee function was graded as (A) excellent, afull range of stable, pain-free movement; (B) good,flexion to ≥ 90°, slight instability or pain; (C) fair,flexion 45–90°, mild instability or pain; or (D) poor,flexion < 45°, gross instability, or severe pain.(1) Kneefunction, radiographs, and the outcomes for anyassociated anomalies were all assessed in the finalfollow-up session.
RESULTS
Pertinent data for each patient are noted in theTable 1. All 19 infants (25 knees) with CDK weretreated with this method. There was a predominanceof girls (14/19, 74%). Six patients had bilateralinvolvement, with bilateral knee subluxation in 5patients and bilateral knee dislocation in 1. Breechpresentation was noted in the perinatal history of 3patients (patients 3, 6, and 8). One infant (patient 12)had the combined problems of premature birth,breech presentation, and premature rupture of themembranes.
Fifteen patients (79%) had associated muscu-loskeletal anomalies, including DDH, arthrogryposis,
Fig. 2 Case 11 (A) Radiograph demonstrating anterior dislocation of the left knee. (B) Follow-up radiograph showing normalalignment of the left knee at 3 years of age.
A B

Chang Gung Med J Vol. 33 No. 3May-June 2010
Chun-Chien Cheng, et alCongenital dislocation of the knee
269Table 1.
Clin
ical
Dat
a fo
r C
onge
nita
l Dis
loca
tion
of th
e K
nee
RO
M (
°)
Cas
eG
ende
rA
ge a
tSi
deC
lass
ific
atio
nA
ssoc
iate
dB
efor
eA
fter
Pain
Inst
abilt
ityY
ears
of
Res
ult
Tre
atm
ent
Ano
mal
ies
(hyp
erex
t./fl
ex.)
follo
w-u
p
1Fe
mal
e6
hL
Dis
loca
tion
–80
/00/
130
––
11E
xcel
lent
2M
ale
6 h
LSu
blux
atio
n–
45/5
0/12
5–
–4
Exc
elle
nt
3Fe
mal
e8
hL
Subl
uxat
ion
R D
DH
60/0
0/13
0–
–14
Exc
elle
nt
4Fe
mal
e20
hR
Subl
uxat
ion
Bil
DD
H50
/510
/140
––
7E
xcel
lent
LSu
blux
atio
n50
/00/
140
–sl
ight
Goo
d
5Fe
mal
e10
min
RD
islo
catio
nB
il D
DH
90/-
105/
140
––
3E
xcel
lent
LD
islo
catio
n90
/-10
5/14
0–
–E
xcel
lent
6M
ale
2 h
RSu
blux
atio
nA
MC
, Bil.
clu
bfee
t60
/00/
135
––
8E
xcel
lent
LSu
blux
atio
nB
il D
DH
*60
/00/
135
––
Exc
elle
nt
7Fe
mal
e5
hR
Subl
uxat
ion
Bil
DD
H70
/-5
0/14
0–
–8
Exc
elle
nt
8Fe
mal
e1
hR
Dis
loca
tion
Bil
DD
H, b
il cl
ubfe
et,
80/-
10Fa
ilure
Exp
ired
hy
dron
ephr
osis
, ASD
, 16
day
s la
ter
corp
us c
allo
sus
agen
esis
9Fe
mal
e8
hR
Subl
uxat
ion
L D
DH
60/2
00/
135
––
2E
xcel
lent
10Fe
mal
e4
hR
Dis
loca
tion
Bil
DD
H75
/-5
0/12
0–
–2
Exc
elle
nt
11M
ale
16 h
LD
islo
catio
nB
il D
DH
, bil
hind
foot
val
gus
80/-
50/
130
––
3E
xcel
lent
12M
ale
24 h
RSu
blux
atio
nB
il D
DH
60/1
05/
125
––
4E
xcel
lent
LSu
blux
atio
n70
/10
10/1
20–
–E
xcel
lent
13Fe
mal
e2
hL
Subl
uxat
ion
R c
alca
neal
val
gus
50/5
0/14
0–
–4
Exc
elle
nt
14Fe
mal
e24
hR
Subl
uxat
ion
L D
DH
*70
/55/
135
––
3E
xcel
lent
LSu
blux
atio
n80
/010
/120
––
Exc
elle
nt
15Fe
mal
e24
hL
Subl
uxat
ion
–60
/10
0/14
0–
–1.
5E
xcel
lent
16Fe
mal
e24
hL
Subl
uxat
ion
L D
DH
90/1
0-1
0/13
0–
–2
Exc
elle
nt
17Fe
mal
e24
hL
Subl
uxat
ion
L D
DH
70/1
00/
140
––
3E
xcel
lent
18Fe
mal
e24
hR
Subl
uxat
ion
R D
DH
50/5
0/14
0–
–1.
5E
xcel
lent
19M
ale
21 h
RSu
blux
atio
n–
80/1
00/
130
––
9 m
onth
sE
xcel
lent
LSu
blux
atio
n60
/10
0/14
0–
–E
xcel
lent
Abbreviations:
R: r
ight
; L: l
eft;
Bil:
bila
tera
l; D
DH
: dev
elop
men
tal d
islo
catio
n of
the
hip;
AM
C: a
rthr
ogry
posi
s m
ultip
lex
cong
enita
; hyp
erex
t./fl
ex.:
hype
rext
ensi
on/f
lex-
ion;
RO
M: r
ange
of
mot
ion;
*: P
atie
nts
6 an
d 14
und
erw
ent l
eft a
ceta
bula
r os
teot
omy
at a
ge 3
and
2 y
ears
res
pect
ivel
y.

Chang Gung Med J Vol. 33 No. 3May-June 2010
Chun-Chien Cheng, et alCongenital dislocation of the knee
270
and foot deformity. Twelve patients (16 knees) had acombination of ipsilateral CDK and DDH, and 2patients had contralateral hip dysplasia. Threepatients (patients 6, 8, and 11; 4 knees) had a combi-nation of CDK, DDH, and foot deformities. Of the 6patients with bilateral CDK, bilateral DDH wasnoted in 2 with knee subluxation, and in 1 with kneedislocation. One patient had unilateral DDH, andanother with arthrogryposis multiplex congenita alsohad bilateral DDH and bilateral clubfeet.
The difficulty in achieving early reduction ofCDK was found to be related to the duration betweenbirth and treatment. Dislocated knees could bereduced in 5 minutes or less within 8 hours of birth(10 knees), while more than 20 minutes was neededfor reduction in patients treated 20 hours after birth(7 knees). There was only one failure due to severeknee contracture in 1 patient (patient 8) who hadsevere multiple anomalies (hydronephrosis, atrialseptal defect, and corpus callosus agenesis); thispatient died 16 days after birth. The other 24 kneestreated all had an excellent (22 knees) or good out-come (1 knee) as of the latest follow-up (average fol-low-up duration = 4.3 years). Knee function outcomewas not influenced by the severity of deformity (sub-luxation or dislocation), laterality (unilateral or bilat-eral), or concomitant DDH. Gait and growing prob-lems were not influenced by knee reduction in thesepatients. However, hindfoot valgus and residual tal-ipes equinovarus were noted in 1 patient each. APavlik harness was used for at least 4 months in theconcomitant treatment of DDH and CDK. Two of the14 patients with associated DDH (2 hips, patients 6
and 14) had residual hip dysplasia (Fig. 3A), andunderwent acetabular osteotomy at 3 and 2 years old,respectively. Good coverage and stability of all hipswere obtained in the final follow-up session (Fig.3B).
DISCUSSION
The incidence of CDK is estimated to be 1 per100,000 live births, an occurrence 100 times lesscommon than congenital dislocation of the hip.(11)
There are numerous hypotheses concerning the etiol-ogy of CDK, and both intrinsic and extrinsic causeshave been suggested. The intrinsic causes are geneticabnormalities, whereas the extrinsic causes aremechanical factors. In a review of 200 cases byProvenzano,(5) 7 families had a history of CDK. MacFarland(4) reported a case of a family in which amother and her three children from three differentfathers all had CDK. Curtis and Fisher havedescribed “heritable congenital tibio-femoral sublux-ation,”(3) a genetically transmitted syndrome whereCDK is combined with some abnormalities of theface and spine. The familial occurrence suggests apossible genetic basis for CDK, whereas a non-genetic dysplasia etiology is supported by the spo-radic occurrence of most cases. The latter etiology ismore in keeping with the present series of patients,who all lacked a positive family history.
The extrinsic causes of CDK are considered toinclude a lack of amniotic fluid, lack of intrauterinespace, malposition of the fetus, fibrotic contractureof the quadriceps, and traumatic dislocation during
Fig. 3 Case 6 (A) Radiograph demonstrating residual dysplasia of the left hip. (B) Follow-up radiograph showing good coverage at8 years of age.
A B

Chang Gung Med J Vol. 33 No. 3May-June 2010
Chun-Chien Cheng, et alCongenital dislocation of the knee
271
birth.(3,6,8,10) Abnormal intrauterine positioning isimplicated by observations of hyperextended kneesbeing associated with a breech presentation. Fetalmolding due to oligohydramnios or extended breechposition was suggested as a cause by Shattuck, andsupported by Niebauer and King.(8) The incidence ofbreech positioning at delivery was 21% in ourpatients. Other factors proposed as contributing toCDK include quadriceps contracture and hypoplasiaof the anterior cruciate ligament.(6,10) Although manyfactors contribute to the development of CDK, a dis-location that cannot be treated by closed reductionwithin 24 hours of birth by our method may be con-sidered teratogenic, and other congenital anomaliesshould be investigated in these cases.
There are a large number of associated muscu-loskeletal conditions in CDK, the most common ofwhich are DDH, club foot, arthrogryposis, andLarsen’s syndrome. In our series, 15 patients (78.9%)had associated musculoskeletal anomalies. Becausethe incidence of CDK is far less common than DDH,it is difficult to consider DDH as a causative factorof CDK. Rather, we propose that CDK contributes,at least in part, to the development of DDH, with thecontractive quadriceps femoris muscle and dorsallydisplaced hamstrings potentially rendering the hipjoint unstable. This is in agreement with the majorityof studies that suggest that CDK should be treatedfirst.(2,3,7)
The mainstay of treatment for CDK is earlynon-operative reduction. Many modalities have beenutilized, including serial casting, Pavlik harness, skintraction, and skeletal traction. Haga et al. suggestedwaiting 1 month for spontaneous reduction of CDKnot associated with clubfoot or Larsen’s syndrome.(12)
Mayer reviewed 68 patients, and found that treat-ment was successful in 81% of patients if performedbefore the age of 3 months, but only 33% if per-formed between the ages of 3 and 6 months.(13)
Similar results were reported in a review of 10 kneesby Stern.(9) Laurence suggested that treatment shouldbe serial splinting for 2 weeks, followed by 2 monthsof traction if this fails.(7) We found that patients whoresponded to early closed treatment generally hadnormal knee function, without any complications, atfollow-up. These results compare favorably to previ-ous reports of knees reduced 2 days after birth.(1) Inour previous report, traction followed by casting oruse of a spica cast with or without general anesthesia
was needed in all patients treated 2 days after birth.Serial casting was needed in patients treated from 24to 48 hours after birth. Serial casting increased thecomplexity of reduction. The present report appearsto be the first to recommend early, gentle reductionof CDK within 24 hours of birth. The difficulty inreducing CDK increases with the increase in thenumber of hours after birth. Indeed, reduction isespecially easy in patients treated less than 8 hoursafter birth. In addition, delayed reduction mayrequire traction or anesthesia, which increases hospi-talization costs and surgical risks. When there arerisk factors for CDK such as oligohydramnios andbreach presentation and CDK is impressed on prena-tal l ultrasonographic examination,(15,16) a paediatricorthopaedic surgeon should be consulted so thatCDK can be reduced as soon as possible.
It has been reported that the Pavlik harness cansimultaneously reduce both CDK and DDH.(14) If nottreated early, the associated DDH may be resistant toclosed reduction, and surgical reduction with orwithout acetabular osteotomy may be indicated forthese patients. Two of our patients had residual hipdysplasia after concomitant treatment with a Pavlikharness for 4 months; this is consistent with otherreports where treatment of DDH was not startedearly.
In conclusion, early reduction of CDK within 24hours of birth affords excellent or good outcomes forall CDK patients not presenting with severe associat-ed congenital anomalies (teratogenic CDK).
REFERENCES
1. Ko JY, Shih CH, Wenger DR. Congenital dislocation ofthe knee. J Pediatr Orthop 1999;19:252-9.
2. Johnson E, Audell R, Opppenheim WL. Congenital dislo-cation of the knee. J Pediatr Orthop 1987;7:194-200.
3. Curtis BH, Fisher RL. Heritable congenital tibiofemoralsubluxation. Clinical features and surgical treatment. JBone Joint Surg Am 1970;52:1104-14.
4. Mac Farland B. Congenital dislocation of the knee. JBone Joint Surg 1929;11:281-5.
5. Provenzano RW. Congenital dislocation of the knee.Report of a case. N Engl J Med 1947;236:360-2.
6. Katz MP, Grogono BJS, Soper KC. The etiology andtreatment of congenital dislocation of the knee. J BoneJoint Surg Br 1967;49:112-20.
7. Laurence, M. Genu recurvatum congenitum. J Bone JointSurg Br 1967;49:121-34.

Chang Gung Med J Vol. 33 No. 3May-June 2010
Chun-Chien Cheng, et alCongenital dislocation of the knee
272
8. Niebauer JJ, King DE. Congenital dislocation of the knee.J Bone Joint Surg Am 1960;42:207-25.
9. Stern MB. Congenital dislocation of the knee. ClinOrthop Relat Res 1968;61:261-8.
10. Middleton DS. The pathology of genu recurvatum. Br JSurg 1935;22:696-702.
11. Jacobsen K, Vopalecky F. Congenital dislocation of theknee. Acta Orthop Scand 1985;56:1-7.
12. Haga N, Nakamura S, Sakaguchi R, Yanagisako Y,Taniguchi K, Iwaya T. Congenital dislocation of the kneereduced spontaneously or with minimal treatment. JPediatr Orthop 1997;17:59-62.
13. Meyer L. Congenital anterior subluxation of the knee:
Description of a new specimen, summary of the patholo-gy of the deformity and discussion of its treatment. Am JOrthop Surg 1913;10:411-37.
14. Iwaya T, Sakaguchi R, Tsuyama N. The treatment of con-genital dislocation of the knee with Pavlic harness. IntOrthop 1983;7:25-30.
15. Elchalal U, Ben Itzhak I, Ben-Meir G, Zalel Y. Antenataldiagnosis of congenital dislocation of the knee: a casereport. Am J Perinatol 1993;10:194-5.
16. Lage Jde A, Guamiero R, de Barros Filho TE, deCamargo OP. Intrauterine diagnosis of congenital disloca-tion of the knee. J Pediatr Orthop 1986;6:110-1.

273
1
1990 7 2007 6 ( )
4.3 ( )
( 2010;33:266-73)
1
98 3 28 98 7 6833 123
Tel.: (07)7317123 8003; Fax: (07)7354309; E-mail: [email protected]










![Case Report Down-Turner Syndrome: A Case with Double ...downloads.hindawi.com/journals/cripe/2016/8760504.pdf · Associations with hemangioma [] or congenital knee dislocation[ ]havebeendescribed.Down-Turnersyndrome](https://img.pdfslide.us/doc/110x75/5e527c536b7c111ffc58b6a3/case-report-down-turner-syndrome-a-case-with-double-associations-with-hemangioma.jpg)