Embed Size (px)
Citation preview

Early Post-LASIK Flap Amputation in the Treatment of Aggressive Fungal Keratitis
in Association With Construction of the
Refractive Suite
John Au MD - no financial disclosures
William Dupps Jr MD, PhD – Avedro Consultant
Karolinne Rocha MD, PhD - No financial disclosures
Ronald Krueger MD, MSE - Alcon, Clarity Medical
Systems and LensAR Consultant

Post Laser Vision Correction Infectious Keratitis
• Infectious keratitis following laser vision correction
as reported by the 2008 American Society of
Cataract and Refractive Surgery (ASCRS) survey was
19 of 20,941 eyes or 0.09%.
• The most commonly cultured organism in this series
was methicillin-resistant Staphylococcus aureus
(MRSA).
• One case definitively resulted from a fungal infectionSolomon R, Donnenfeld E, Holland E, Yoo S, Daya S, Guel J, Mah F, Scoper S, Kim T. Microbial keratitis trends following refractive surgery: Results of the ASCRS Infectious keratitis survey and comparisons with prior ASCRS surveys of infectious keratitis following keratorefractive procedures. J Cataract Refract Surg 2011;37:1343-1350

Case Presentation• 24-year old female -1.25D sphere in both eyes
• Her exam, pachymetry and corneal tomography were normal
• Her history included prior right V1 dermatome herpes zoster
without ophthalmic involvement
• Treated with wavefront-optimized femtosecond-LASIK on the
WaveLight FS-200 and Allegretto Eye-Q laser platform (Alcon, Fort
Worth, TX, USA)
• She had an uneventful procedure and was started on ciprofloxacin
0.3% (Ciloxan®) and dexamethasone 0.1% drops four times daily
each.
• On post-op day one, UDVA was 20/15 in each eye. Her exam was
unremarkable

Case Presentation
• During the week prior to this case, a new wall was
built within the refractive suite waiting area, which
was not directly continuous with the laser suite
• However, the day prior to the case, construction
workers had removed some ceiling tiles in the
laser suite in preparation for the upcoming
construction and removal of an internal wall

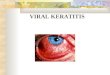
Postoperative Day 2• Patient presents with pain and
decreased vision• UDVA OD 20/50

Clinical Plan• Clinical suspicion for fungal keratitis was high
• The flap was lifted and a gelatinous branching infiltrate was seen,
extending superficially into the flap and posteriorly into the stromal bed
• Cultures were obtained and the interface was irrigated extensively
• Because the infiltrate penetrated into the flap stroma, and due to the
rapid progression (< 24 hours) of a presumed of fungal keratitis, a
decision was made to amputate the flap
• Hourly topical fortified tobramycin (13.5mg/ml), vancomycin (25mg/ml)
and voriconazole 1% were begun immediately
• Although the infiltrate was clearly in the flap interface and not involving
the overlying epithelium, a 10 day course of of oral valacyclovir 1 gram
TID was given due to the patient’s history of right V1 herpes zoster
• Prednisolone was discontinued

Postoperative Course
• Post-flap amputation Day 4
• UDVA 20/100-
• Infiltrate was improving and the epithelium was
approximately 85% healed over the stromal bed

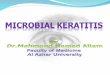
Postoperative Course• Fungal cultures grew Aspergillus flavus, all other cultures
were negative
• Pathology of the flap showed fungal elements (black arrows)
PAS stain

Postoperative Course• Post-flap amputation day 11 UDVA 20/40; MRx -0.50 SPH with BCVA 20/20-
• Post-flap amputation month 5 UDVA 20/15, but having double image
• Epithelial thickness is variable (40-59 um) due to irregular stromal surface
Post-flap amputation day 11

Post-flap amputation month 8planned PTK/PRK ENH
• VisX S4 PTK OD• 6.5 mm OZ, 0.2 TZ• 71 um depth• H-PRK OD, +1.0 D
Pre PTK
1 Month Post PTKUCVA 20/40MR -1.00 (20/25+)…still healing!

Factors That Allowed For Good Visual Outcome Post Flap
Amputation 1. Penetration of the antibiotics and antifungal medication
to the infiltrate were optimized
2. The patient had a low myopic correction with robust
residual stromal bed thickness for possible future
refractive treatment
3. The flap was created with a femtosecond laser, and,
therefore, had a uniform planar shape, allowing for
minimal refractive change when compared to a
meniscus shaped microkeratome flap, when amputated

ConclusionAlthough we cannot not definitively
link this infection to the preceding
construction work, it is reasonable to
conclude one should avoid performing
Laser Vision Correction following
recent construction work in the
refractive suite