Embed Size (px)
Citation preview


Outline
Motivation Summary of impact evaluations Conditions Administration

Motivation
Conditional cash transfer (CCT) programs have become very popular: first in Latin America and now across the world

4
Defining Characteristics of CCTs
CCTs- transfer cash*- to poor households- on condition that their children
go to school and use preventive health care
Twin goals:- Immediate poverty relief
through transfers- Long run poverty reduction
through improvements in poor children’s human capital
*food may work too, though with much higher administrative costs
Pot
entia
l cov
erag
eof
poo
r
Improvement in service use
Unconditional cash transfers
Classic CCT in MIC
Secondary scholarship in LIC
CCT for HIV/TB
We focus here today
Demand-side tools to increase service use

A family of program approaches Conditions Education and Health Education Only
Bolsa Familia (Brazil) Oportunidades (Mexico)
Bono de Desarrollo Humano (Ecuador) Bolsa Escola (Brazil) Familias en Acción (Colombia)
Nationwide
Program of Advancement through Health and Education (Jamaica)
Jaring Pengamanan Sosial (Indonesia)
Female Secondary School Assistance Program (Bangladesh)
Chile Solidario Japan Fund for Poverty Reduction Girls Scholarship
Program (Cambodia) Education Sector Support Project (Cambodia)
Niche (regional or
narrow target population) Social Risk Management Project (Turkey)
Basic Education Development Project (Yemen) Programa de Asignación Familiar (Honduras)
Cash Transfer for Orphans and Vulnerable Children (Kenya)
Subsidio Condicionado a la Asistencia Escolar - Bogota (Colombia)
Atención a Crisis (Nicaragua)
Pro
gra
m s
ize/
targ
et
Small scale/pilot
Red de Protección Social (Nicaragua) Punjab Education Sector Reform Program
(Pakistan)

Reasons for growing interest: CCTs have often replaced a myriad of badly
targeted, regressive, ineffective subsidies and piece-meal programs
CCTs as a new “contract” between the state and CCT beneficiaries. Emphasis on “co-responsibilities” rather than “conditions”
CCTs have shown positive results through credible impact evaluation studies
Large-scale CCTs have survived political transitions

2. Evidence of CCT performance:

CCT benefits are decidedly progressive…
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
1 2 3 4 5 6 7 8 9 10
Deciles of per capita consumption minus transfer
Prop
ortio
n of
tota
l ben
efits
rece
ived
Bolsa FamiliaChile SolidarioChile SUFEcuador BDHHonduras PRAFMexico OportunidadesJamaica PATHCambodia: JFPRBangladesh FSSP
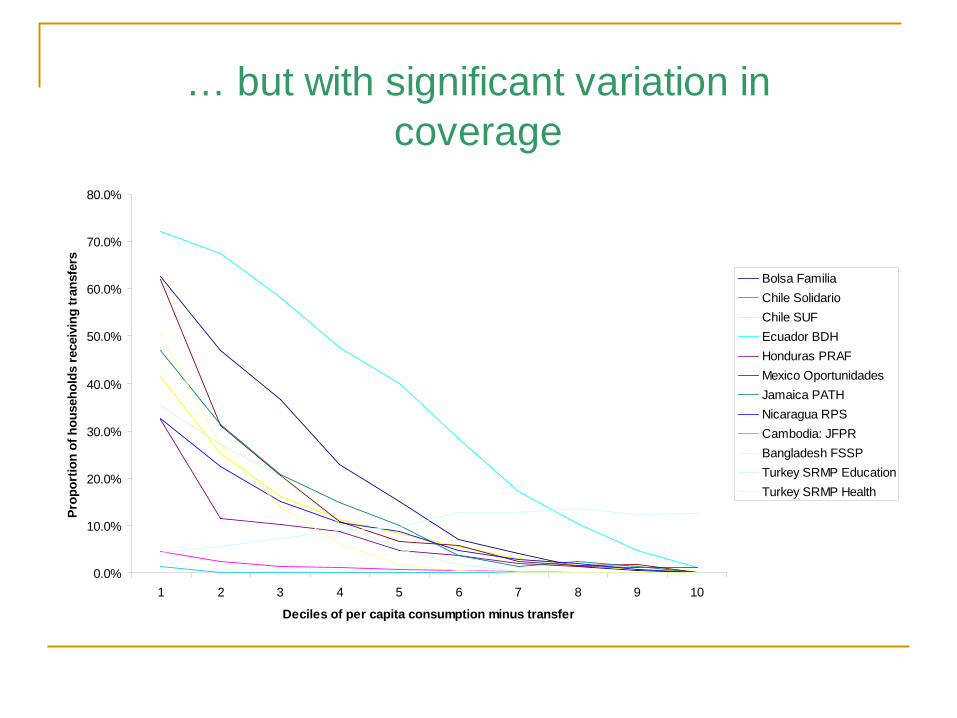
… but with significant variation in coverage
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
1 2 3 4 5 6 7 8 9 10
Deciles of per capita consumption minus transfer
Prop
ortio
n of
hou
seho
lds
rece
ivin
g tr
ansf
ers
Bolsa FamiliaChile SolidarioChile SUFEcuador BDHHonduras PRAFMexico OportunidadesJamaica PATHNicaragua RPSCambodia: JFPRBangladesh FSSPTurkey SRMP EducationTurkey SRMP Health

Reductions in poverty among beneficiaries
CCT impacts on consumption and povertyMexico(1999)
Nicaragua(2002)
Colombia(2006)
Cambodia(2007)
Median per capita consumption (US $)
0.66 0.52 1.19 0.75
Average transfer (% of per capita consumption)
20% 30% 13% 3%
Impact on per capita consumption (%)
8% 21% 10% --
Impact: headcount index (% points)
1.3** 5.3** 2.9** --
Impact: sqd. poverty gap (% points)
3.4** 8.6** 2.2** --

Families spend a higher share of resources on food and obtain a more varied diet

Disincentive effects have not been a problem Substantial reductions in child work:
Mexico: child labor among teenagers fell by 2% points for girls, and 5% points for boys
Cambodia: reduction of 10% points in work for pay; average of 14 fewer hours worked for pay
Modest reductions in adult labor market participation (Mexico, Ecuador, Cambodia),
Households invest part of the transfer (evidence for Mexico and Brazil –but not in Nicaragua)

CCT impacts on education outcomesCCT impacts on enrollment
Age range
Baseline enrollment
Impact (% points)
Size of transfer
Colombia 8-1314-17
91.7%63.2%
2.1**5.6***
17%
Chile 6-15 60.7% 7.5*** 3-7%
Ecuador 6-17 75.2% 10.3*** 10%
Mexico Grade 0-5Grade 6
Grade 7-9
94.0%45.0%42.5%
1.98.7***
0.620%
Nicaragua 7-13 72.0% 12.8*** 30%
Cambodia Grade 7-9 65.0% 31.3*** 2%
Pakistan 10-14 29.0% 11.1*** 3%

CCT impacts on health outcomes
CCT impacts on health center visitsAge
rangeBaseline
levelImpact (%
points)Size of transfer
Colombia <24 months24-48
months
n.a.n.a.
22.8**33.2***
17%
Chile 0-6 years 17.6% 2.4 7%
Ecuador 3-7 years n.a. 2.7 10%
Honduras 0-3 years 44.0% 20.2*** 9%
Mexico 0-3 years 69.8% 8.4 20%
Nicaragua 0-3 55.4% 13.1* 27%

Impacts on education and health outcomes concentrate among the poor
Example: Nicaragua

Improvements in final outcomes in some but not all cases…
CCT impacts on child nutrition (height-for-age z-scores)Age
rangeBaseline
levelImpact (%
points)Size of transfer
Colombia <24 months24-48
months
n.a. 0.16**0.01
17%
Ecuador <24 months24-48
months
-1.07-1.12
-0.03-0.06
10%
Mexico 12-36 months
n.a. 0.96 cm** 20%
Nicaragua <60 months -1.79 0.17** 27%
Honduras <72 months -2.05 -0.02 9%

Mixed effects in education
Mexico and Colombia: Chilren learning apace with non-participant
peers,
Cambodia: Beneficiaries have more schooling than
children in the control group but didn’t perform better on mathematics or vocabulary test

Encouraging effects on early childhood development…
CCT impacts on child development (children age 3-6)Nicaragua Ecuador
(poorest 40%)Ecuador
(poorest 10%)
Receptive language 0.223***(0.078)
0.011(0.108)
0.177(0.148)
Memory 0.092(0.072)
0.192*(0.105)
0.228**(0.109)
Socio-emotional 0.067(0.065)
0.150(0.103)
0.389**(0.159)
Fine motor 0.150(0.110)
0.160**(0.076)
0.288**(0.117)
Note: all program impacts are in standard deviations.

Limitations on Evaluations
So far almost all evaluations are “black box” designs that do not permit us to distinguish separate effects of: Transfers Conditions Information Change in intra-hh
distribution of resources
19

3. Conditions

Why conditions?
Households sometimes invest inefficiently little in child human capital
Persistently underestimate returns to human capital Externalities to education and health investments “Incomplete altruism” between parents and children
Political economy justifications Conditions increase political support to transfer programs Emphasis on “co-responsibilities” rather than “conditions”

There is a lot of variability in the practice:
In the definitions of co-responsabilities –grades, exact services in health and frequency of use, information component, who, etc.
In penalties: “hard” – amount of transfer reduced in next payment cycle, and
by full amount corresponding to action eg. Mexico, Jamaica, Colombia, Turkey
‘softer”: Brazil – first warnings, then social worker assistance Kenya – similar at community leve, then small reduction
In the rigor of monitoring Almost 100% (Mexico, Jamaica); almost 0% (until
recently Ecuador, Dominican Rep, Phillippines)22
Are conditions necessary?Mexico:
Children in households w/o monitoring 5.4% points less likely to enroll in school
Ecuador: Program effects are only significant for
households that believed transfer are ‘conditonal’
Cambodia: Program has no effect on enrollment for siblings
at other levels
Malawi: Experimental program early results show UCT
and CCT effects similar

There are tensions between social assistance and human capital goals
Mexico: Impact on enrollment most significant at transition grades. But targeting transition reduces ability to redistribute income.
40
50
60
70
80
90
100
P2 P3 P4 P5 P6 S1 S2 S3 S4
Continuation rate (%)
Primary school
Lower secondary school
Secondary64%
Entering grade
PROGRESA INTERVENTION Upper secondary
school43%
Progresa villages
Control villages
76%
50%

The size of these tradeoffs vary by context
Mexico (2002)
Cambodia (2004)
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
1 2 3 4 5 6 7 8 9
Grade
Surv
ival
Rat
ePo
ores
t 20%

Complementary interventions
CCTs are not the only policy needed
Improvements in access or quality of health and education services – and most countries with CCT programs also have initiatives in these directions
CCTs may be complemented by other social assistance and social insurance programs

4. Administration

Systems for monitoring compliance
Require real time collection and use of data flowing between multiple agencies
Are demanding, but mature programs do not have excessive adminstrative costs
I sometimes think the data flow expertise is secret weapon of CCT programs

The institutional legacy of CCTs
Led the way in the design of well-run administrative structures for beneficiary selection, payments, transparency
Groundbreaking importance paid to impact evaluation with credible counterfactuals
The record of the early programs in these regards was not inherent to CCTs, but should be safeguarded and emulated