Embed Size (px)
Citation preview

Articlemorits
Percutaneous coronary intervention for cardiacallograft vasculopathy in Asian patients
Hung-Yu Chang, M.D. 1,2, Chin-Kun Tseng, M.D. 1,3, Jeng Wei, M.D. 4 and Wei-Hsian Yin, M.D.,Ph.D. 1,2,∗
1 Division of Cardiology, Heart Center, Cheng Hsin General Hospital, Taipei, Taiwan2 Faculty of Medicine, School of Medicine, National Yang-Ming University, Taipei, Taiwan3 Department of Internal Medicine, Song-Shan Armed Forces General Hospital, Taipei, Taiwan4 Division of Cardiovascular Surgery, Heart Center, Cheng Hsin General Hospital, Taipei, Taiwan* Correspondence: [email protected] ; Tel.: +886-2-2826-4400 ext. 2509† Both authors (Hung-Yu Chang, Chin-Kun Tseng) have equal contribution to this study
Accepted 25 July 2019; Volume: 1; Issue: 2; Pages: 1-9; DOI: 10.6907/SCJ.201904_1(2).0001
Abstract:Background:The optimal treatment of cardiac allograft vasculopathy (CAV) remains controversial. Percutaneouscoronary intervention (PCI) is one of the treatment options. There was paucity of data on Asianpatients with CAV undergoing PCI. The purpose of our study was to investigate the clinical outcomesof PCI in Asian patients with CAV.
Methods and Results:The study involved 21 heart transplant recipients who underwent PCI for 40 de novo coronarylesions since 2004. The treatment included 20 lesions with stenting and 20 lesions with balloonangioplasty.All PCIs were successful and there were no in-hospital complications. The follow-upangiography was performed after a mean period of 37±17 months. Comparing with the balloonangioplasty group, the stenting group showed significantly higher binary restenosis rate (80% vs. 3%,p=0.001), higher percentage diameter restenosis (71±29 vs. 46±21%, p=0.004), and higher late lumenloss (2.1±1 vs. 0.9±0.4mm, p<0.001). Kaplan-Meier survival curves showed that the target lesionrevascularization rates were significantly higher in the stenting group than the balloon angioplastygroup (70 vs. 25%, p=0.021).
Conclusions:PCI can be performed safely in cardiac transplant recipients. The need for repeat interventionwas common. Target lesion revascularization rates were significantly higher in the stenting groupcompared to the balloon angioplasty group. Further trials are required to evaluate the optimal PCIstrategy in Asian patients with CAV.
Keywords: Heart transplantation; Cardiac allograft vasculopathy; Percutaneous coronaryintervention
1. IntroductionHeart transplantation (HTX) is a well-established surgical option for patients with end-stage
heart failure.1 However, coronary allograft vasculopathy (CAV) remains the most significant cause
Strait Circulation Journal 2019, 2, 1.

Strait Circulation Journal 2019, 2, 1 2
of late cardiac death after HTX.[1,2] Fifty percent of patients develop angiographic evidence of CAVat 5 years after HTX.[3] CAV is an immunologic phenomenon. The underlying mechanisms of CAVinclude endothelial dysfunction, luminal narrowing and intimal hyperplasia which usually result indiffuse narrowing of the transplant coronary arteries, and are significantly different from the morefocal presentation in native coronary artery atherosclerotic disease.[4]
Despite various medical therapies[1,5–7] employing calcium-channel blocker,angiotensin-converting enzyme inhibitors and statins, CAV can still progress and results insignificant morbidity and mortality. Because of the diffuse nature of the CAV and its associatedcomplex characteristics, coronary artery bypass surgery on CAV are often technically difficult andhence not commonly considered as the initial treatment strategy.[8,9] Currently, re-transplantation isthe only definitive treatment for CAV. However, major ethical issues have to be faced before the use ofthe scarce donor organs for such patients needing re-transplantation as poorer allograft survival isexpected compare to that after the first cardiac transplant.[1,2,10]
Percutaneous coronary intervention (PCI) is an acceptable palliative treatment strategy for CAVpatients. Nevertheless, the restenosis rates, procedural complications and long-term mortality weresignificantly higher compared to PCI to native coronary arteries.[3,11–15] In a recent report fromUniversity of California, outcomes among patients who underwent PCI for CAV were very poor,composite endpoint of freedom from death, myocardial infarction, target vessel revascularization andre-transplantation was only 17%.[16]
The data on PCI in Asian patients with CAV was very limited. The coronary arterial size, coronarylesion characteristics, the difference in protocols of immunosuppressant therapies and the difference inracial groups could affect treatment results. Previous study has shown that non-white race was anindependent risk factor for the development of restenosis after PCI with drug-eluting stent in CAV.[17]We designed the study to investigate clinical and angiographic outcomes of PCI in Asian patients withCAV.
2. Methods
2.1. Study Cohort
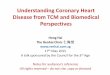
The study began after obtaining ethical approval from our hospital’s Institutional Review Board. Atotal of 345 patients who underwent HTX at our center were screened. All transplant procedures wereperformed by the biatrial anastomotic technique, as described by Lower (Figure 1).[18] All patientsreceived triple immunosuppressive drugs including cyclosporine or tacrolimus, mycophenolatemofetil, and prednisolone. Of these, 21 heart transplant recipients who received PCI for 40 de novocoronary lesions between 2004 and 2012 were included in the study. The demographic data, clinicaldata, and cardiac catheterization images for each patient were reviewed retrospectively.
2.2. PCI
Diagnostic coronary angiography was performed and the decision of PCI was made after reviewmeeting involving both cardiologist and cardiovascular surgeon. Coronary angiography and the PCIwere performed via either radial or femoral artery approach. Aspirin, unfractionated heparin, andclopidogrel were given routinely before the PCI procedure. The form of CAV intervention (balloonangioplasty or stenting) selected was dependent on the operator’s preference as well as financialconsideration of the patient.
The definition of the CAV was based on the international society of heart and lung transplantation(ISHLT) nomenclature (Table 1).[19] The minimal luminal diameter and percentage diameter stenosiswere measured by quantitative coronary angiography using the outer diameter of the catheter as thecalibration reference standard. Reference vessel diameter was measured as the mean of the proximaland distal shoulders of the lesion.

Strait Circulation Journal 2019, 2, 1 3
Figure 1. Illustration of orthotopic heart transplantation using biatrial anastomosis in current study.
Nomenclature NoteISHLT CAV0 No detectable angiographic lesion(Not significant)ISHLT CAV1 Angiographic LM <50%, or primary vessel with maximum lesion of <70%, or any(Mild) branch stenosis <70% (including diffuse narrowing) without allograft dysfunctionISHLT CAV2 Angiographic LM ≥50%; a single primary vessel ≥70%, or isolated branch(Moderate) stenosis ≥70% in branches of 2 systems, without allograft dysfunctionISHLT CAV3 Angiographic LM ≥50%, or two or more primary vessels ≥70% stenosis, or(Severe) isolated branch stenosis ≥70% in all 3 systems; or ISHLT CAV1 or CAV2 with
allograft dysfunction (Left ventricular ejection fraction ≤45%)
CAV = Cardiac allograft vasculopathy; ISHLT = International Society for Heart and LungTransplantation; LM = left main.
Table 1. Recommended nomenclature of the International Society for Heart and Lung Transplantationfor cardiac allograft vasculopathy[19]
Follow-up coronary angiography was performed routinely at 9-12 months post PCI and earlierwhen restenosis was suspected with clinical presentation of angina. Late luminal loss was definedas the difference in the minimal luminal diameter between post PCI and follow-up angiographymeasurements. Binary restenosis was defined as more than or equal to 50% narrowing of the targetlesion by quantitative coronary angiography at follow-up.
2.3. Statistical Analysis
The statistical analyses were performed using SPSS Statistics 17.0 software (Chicago, Ill).Quantitative data are expressed as the mean value ± SD. The student’s t-test was used for thecomparisons between continuous data. The Chi-square test with a Pearson or Fisher’s exact test wasused for the comparisons between the categorical data. A Kaplan-Meier survival analysis with thelog-rank test was used to compare the different treatments for the target lesion revascularization.A multivariate analysis was performed with a Cox stepwise forward regression to determine the

Strait Circulation Journal 2019, 2, 1 4
independent predictors of the target lesion revascularization. Variables selected for the multivariateanalysis were those with a p-value <0.1 after the initial univariate analysis. A p-value of <0.05 wasconsidered as statistically significant.
3. Results
3.1. Baseline Patients Characteristics
The study consisted of 21 cardiac recipients (mean recipient age 40±14 years, donor age 37±10years) who underwent PCI for 40 de novo coronary lesions (2±2 lesions per patient). Mean durationof PCI post transplantation was 111±54 months. Baseline characteristics of the patients are shownin Table 2. Fifteen (71%) were men, 7 (33%) had hypertension, 8 (38%) had diabetes and 6 (29%) hadhyperlipidemia. Ten patients (48%) were treated with statin and 19 patients (90%) were treated withantiplatelet agents before PCI.
Variables n=21Male 15 (71%)Recipient age (y/o) 40±14Donor age (y/p) 37±10Donor heart ischemic time (minutes) 180±57Hypertension 7 (33%)Diabetes 8 (38%)Hyperlipidemia 6 (28%)Serum Creatinine (mg/dL) 1.4±0.7Current/Ex-smoker 5 (24%)Left ventricular ejection fraction (%) 60±11Right ventricular systolic pressure (mmHg) 31±8Cyclosporine 18 (86%)Tacrolimus 3 (14%)Mycophenolate mofetil 15 (71%)Prednisolone 16 (76%)Statin 10 (48%)Antiplatelet agents 19 (90%)Beta-blocker 15 (71%)Renin-angiotension system blockade 19 (90%)International society of heart and lung transplantation nomenclature for CAVCAV1 0 (0%)CAV2 10 (48%)CAV3 11 (52%)Time interval from transplant to percutaneous intervention (months) 111±54
CAV = Cardiac allograft vasvulopathy
Table 2. Baseline patient characteristics
3.2. Baseline Angiographic and PCI Procedure
The treatment involved 20 procedures of stent deployment (group 1) and 20 procedures of balloonangioplasty (group 2). Baseline angiographic characteristics are shown in Table 3. The reference vesselsize diameter (3.2±0.5mm vs. 2.8±0.7mm, p=0.044) was larger, but the percentage diameter stenosis(86±10% vs. 78±9%, p=0.016) was higher in the group 1 than group 2 patients. The minimal luminaldiameter, lesion length, anatomic distribution and lesion complexity were comparable between bothgroups.

Strait Circulation Journal 2019, 2, 1 5
Group 1 (Stent) Group 2 (Balloon) p-valuen=20 n=20
Left main coronary artery 0 (0%) 0 (0%) NSLeft anterior descending artery 9 (45%) 9 (45%) NSLeft circumflex artery 7 (35%) 4 (20%) NSRight coronary artery 4 (20%) 7 (35%) NSTotal occlusion 3 (15%) 1 (5%) NSMinimal luminal diameter (mm) 0.5±0.3 0.6±0.3 NSReference vessel size(mm) 3.2±0.5 2.8±0.7 0.044Lesion length (mm) 18±5 18±3 NSPercent diameter stenosis (%) 86±10 78±9 0.016Procedural success 20 (100%) 20 (100%) NSPost-procedural minimal luminal diameter (mm) 3.1±0.5 2.5±0.7 0.009Acute gain (mm) 2.6±0.6 1.9±0.5 <0.001
Table 3. Baseline characteristics of treated lesions
All PCIs were performed successfully with no procedure-related complications. In the group1, 11 lesions were treated with bare metal stents and 9 lesions were treated with drug-eluting stents.Post-procedural minimal luminal diameter (3.1±0.5mm vs. 2.5±0.7 mm, p=0.009) and acute gain(2.6±0.6mm vs. 1.9±0.5 mm, p<0.001) were larger in the group 1 than group 2.
3.3. Angiographic Follow-up
Follow-up angiography was performed in 19 of 20 lesions (95%) in the group 1 and 19 of 20lesions (95%) in the group 2 at follow-up of 37±17 months. Two patients did not have angiographicfollow-up because of death. Angiographic follow-up results are shown in Table 4.
Group 1 (Stent) Group 2 (Balloon) p-valuen=19 n=19
Angiographic follow-up interval (months) 25±16 22±11 NSClinical follow-up interval (months) 42±19 35±15 NSFollow-up minimal luminal diameter (mm) 0.9±1 1.6±0.8 0.035Follow-up percent diameter stenosis (%) 71±29 46±21 0.004Total occlusion 4 (21%) 1 (5%) NSLate lumen loss (mm) 2.1±1 0.9±0.4 <0.001Binary restenosis 16 (84%) 6 (32%) 0.001Target lesion revascularization 14 (74%) 5 (26%) 0.004
Table 4. Angiographic follow-up of previously treated lesions
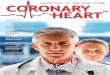
Binary restenosis was found in 24 lesions (63%) during follow-up. The percentage diameterrestenosis was 58±28% and late lumen loss was 1.5±1mm. The group 1 patients had higher binaryrestenosis rate (80 vs. 30%, p=0.001), higher percent diameter restenosis (71±29% vs. 46±21%, p=0.004),and more significant late lumen loss (2.1±1mm vs. 0.9±0.4mm, p<0.001) compared to the group 2patients. Four stented (21%) lesions and single balloon angioplasty lesion (5%) were found occludedduring follow-up angiography. The target lesion revascularization rate was 50%. The Kaplan-Meiersurvival curves showed that the target lesion revascularization rates were significantly higher in thegroup 1 than group 2 (70% vs. 25%, p=0.021, Figure 2). Among lesions in group 1 treated with baremetal stents and drug eluting stents, follow-up angiographic outcomes showed comparable results(binary restenosis rates 90.0% vs. 77.8%, p=0.582; total occlusion rates 20.0% vs. 22.2%, p=0.906; percentdiameter stenosis 77±23mm vs. 63±37mm, p=0.338; target lesion revascularization 80.0% vs. 66.7%,p=0.628, respectively).

Strait Circulation Journal 2019, 2, 1 6
Figure 2. Kaplan-Meier survival curves showing the significant difference in the target lesionrevascularization rates between the patients receiving balloon angioplasty and receiving stentimplantation.
3.4. Clinical Outcomes and Predictors
Revascularizations were performed in 8 (38%) patients for 16 restenosis lesions and coronaryartery bypass surgery was performed in 3 (14%) patients for 4 restenosis lesions. Four (19%) patientsdied during the follow-up. The major adverse cardiac events that include death, myocardial infarction,redo-transplantation and target lesion revascularization occurred in 12 (57%) patients during thefollow-up.
Multivariate analysis showed that the independent predictors of the target lesion revascularizationwere total occlusive lesion (p<0.001, odds ratio [OR] 15.8, 95% confidence interval [CI] 4.0-63.3) andstent deployment instead of balloon angioplasty (p=0.017, OR 3.7, 95% CI 1.2-10.8).
4. Discussion
4.1. Major Findings
One of the main findings of our study was that PCI could be performed safely in transplantrecipients with CAV. However, the restenosis rates and the target lesion revascularization rates werehigh in these patients. Target lesion revascularization rates were significantly higher in patientsreceiving stent than balloon angioplasty.
4.2. PCI for CAV
CAV occurs in 18% of cardiac transplant recipients at 1-year and 50% of patients at 5 years aftertransplantation.[1–3] The CAV is a known complex disease and the optimal strategy to delay thedisease progression has yet to be identified.

Strait Circulation Journal 2019, 2, 1 7
PCI can be performed in selected CAV patients as a palliative option to reduce ischemia-relatedmorbidity and mortality. In the previous reports, PCI was associated with procedural success rates of92% to 93% and the restenosis rates ranged from 20% to 55% at 6 to 15 months after procedure.[8,12,20]In our cohort involving only Asian patients, the procedural success rate was 100%. After a follow-upperiod of 37±17 months, the binary restenosis rate was 63%. These results were similar to thepreviously published reports.
4.3. Balloon Angioplasty and Stent Deployment for CAV
Although stents are widely utilized in native coronary artery disease, their use in CAV has notbeen studied extensively. In native coronary artery disease, acute recoil could be overcome by coronaryartery stenting, which increases acute luminal gain compare to balloon angioplasty alone. Our studyinvolving the CAV lesions showed similar results. The acute gain and the post-procedural minimalluminal diameter were significantly larger in the stenting group than the balloon angioplasty group.CAV lesions treated with stents had a significantly larger reference vessel diameter than that treatedwith balloon angioplasty (3.2±0.5 vs. 2.8±0.7 mm, p=0.044).
In native coronary artery PCI, negative arterial remodeling may occur 4-6 months after balloonangioplasty and lead to subsequent restenosis. Coronary artery stenting can prevent negative arterialremodeling and reduce the rate of restenosis. In addition, neointimal hyperplasia is widely regarded asa main cause of in-stent restenosis after native coronary artery PCI. Anti-proliferative drugs are usedfocally in the form of drug-eluting stents in order to attenuate cell proliferation and reduce in-stentrestenosis.[21,22] However, the underlying mechanism and histologic findings of native coronaryartery disease and CAV are entirely different.[23] In transplanted cardiac recipients, the use of systemicimmunosuppressant agents could inhibit cell proliferation and decrease local inflammatory reserve.[24]Hence, the response to balloon angioplasty and coronary stenting in CAV would be different from thatin native coronary artery disease. Stent deployment may not be feasible in all lesions, especially inthe small-vessel disease. Moreover, meta-analysis from Western countries showed that there were nodifferences in outcomes among patients who underwent PCI with drug-eluting stent as compared tobare metal stent.[9]
Two independent predictors of the target lesion revascularization were identified in current study.Firstly, similar to the previously published report, chronic total occlusion is a main risk predictor forrestenosis.[12] Secondly, stent deployment was another independent predictor of future target lesionrevascularization. In our cohort, CAV lesions treated by stenting had a higher binary restenosis rate(80% vs. 30%, p=0.001), higher percentage diameter restenosis (71±29% vs. 46±21%, p=0.004), andhigher late lumen loss (2.1±1 vs. 0.9±0.4mm, p<0.001) comparing to lesions treated with balloonangioplasty. Our study results were hence in contrary to the previously published studies whichshowed less short and mid-term restenosis after stent deployment.[14] During long-term follow-up,the restenosis rates were similar between the stent and balloon angioplasty groups, and both treatmentstrategy had no positive impact on graft survival.[21] Stent deployment may provoke more severeinflammatory reaction in CAV and hence result in a higher restenosis rate in our study populations.Lastly, as our study represented purely Chinese patients, whether the influence of race played a part inthe outcome in CAV treatment would warrant further investigation.
4.4. Study limitations
There are several limitations which should be acknowledged in the present study. First, the designwas an observational, single-center, retrospective survey. Despite covariate adjustment, several factorssuch as lifestyle modification, drug compliance, body weight and lipid profiles, were not measured incurrent study but might also affect restenosis rates and target lesion revascularization. Second, despitewe extensively screened a total of 345 heart transplant recipients and identified 51 patients with CAV,only 20 patients received PCI were included in current study.

Strait Circulation Journal 2019, 2, 1 8
5. ConclusionOur results indicated that PCI could be performed safely in patients with CAV. The restenosis
rates and target lesion revascularization rates were significantly higher in the stenting group compareto the balloon angioplasty group during follow up. Differences in coronary lesion characteristics andresponse to stent deployment of Asian versus Western cardiac transplant recipients warrant furtherinvestigation.
Conflicts of Interest:The authors declare no conflict of interest.
References
1. Taylor, D.O.; Edwards, L.B.; Boucek, M.M.; Trulock, E.P.; Waltz, D.A.; Keck, B.M.; Hertz, M.I. Registry of theInternational Society for Heart and Lung Transplantation: twenty-third official adult heart transplantationreport—2006. The Journal of heart and lung transplantation 2006, 25, 869–879.
2. Avery, R.K. Cardiac-allograft vasculopathy. New England Journal of Medicine 2003, 349, 829–830.3. Redonnet, M.; Tron, C.; Koning, R.; Bouchart, F.; Cribier, A.; Soyer, R.; Bessou, J. Coronary angioplasty and
stenting in cardiac allograft vasculopathy following heart transplantation. Transplantation proceedings.Elsevier, 2000, Vol. 32, pp. 463–465.
4. Billingham, M. Histopathology of graft coronary disease. The Journal of heart and lung transplantation: theofficial publication of the International Society for Heart Transplantation 1992, 11, S38–44.
5. Lee, M.S.; Tadwalkar, R.V.; Fearon, W.F.; Kirtane, A.J.; Patel, A.J.; Patel, C.B.; Ali, Z.; Rao, S.V. Cardiacallograft vasculopathy: A review. Catheterization and Cardiovascular Interventions 2018, 92, E527–E536.
6. Wenke, K.; Meiser, B.; Thiery, J.; Nagel, D.; von Scheidt, W.; Steinbeck, G.; Seidel, D.; Reichart, B. Simvastatinreduces graft vessel disease and mortality after heart transplantation: a four-year randomized trial.Circulation 1997, 96, 1398–1402.
7. Paul, L.C. Calcium channel blockers and angiotensin-converting enzyme inhibitors in the prevention ofgraft vasculopathy. The Journal of Heart and Lung Transplantation 2000, 19, 409–413.
8. Halle, A.A.; DiSciascio, G.; Massin, E.K.; Wilson, R.F.; Johnson, M.R.; Sullivan, H.J.; Bourge, R.C.; Kleiman,N.S.; Miller, L.W.; Aversano, T.R.; others. Coronary angioplasty, atherectomy and bypass surgery in cardiactransplant recipients. Journal of the American College of Cardiology 1995, 26, 120–128.
9. Luc, J.G.; Choi, J.H.; Rizvi, S.S.A.; Phan, K.; Escrivà, E.M.; Patel, S.; Reeves, G.R.; Boyle, A.J.; Entwistle, J.W.;Morris, R.J.; others. Percutaneous coronary intervention versus coronary artery bypass grafting in hearttransplant recipients with coronary allograft vasculopathy: a systematic review and meta-analysis of 1,520patients. Annals of cardiothoracic surgery 2018, 7, 19.
10. Parameshwar, J.; Wallwork, J.; Schofield, P.; Large, S. The management of post-cardiac transplantationcoronary artery disease. Eur J Cardio-thorac Surg 1996, 10, 528–533.
11. Tanaka, K.; Li, H.; Curran, P.J.; Takano, Y.; Arbit, B.; Currier, J.W.; Yeatman, L.A.; Kobashigawa, J.A.; Tobis,J.M. Usefulness and safety of percutaneous coronary interventions for cardiac transplant vasculopathy.The American journal of cardiology 2006, 97, 1192–1197.
12. Benza, R.L.; Zoghbi, G.J.; Tallaj, J.; Brown, R.; Kirklin, J.K.; Hubbard, M.; Rayburn, B.; Foley, B.; McGiffin,D.C.; Pinderski, L.J.; others. Palliation of allograft vasculopathy with transluminal angioplasty: a decadeof experience. Journal of the American College of Cardiology 2004, 43, 1973–1981.
13. Doshi, A.A.; Rogers, J.; Kern, M.J.; Hauptman, P.J. Effectiveness of percutaneous coronary intervention incardiac allograft vasculopathy. The American journal of cardiology 2004, 93, 90–92.
14. Simpson, L.; Lee, E.K.; Hott, B.J.; Vega, D.J.; Book, W.M. Long-term results of angioplasty vs stenting incardiac transplant recipients with allograft vasculopathy. The Journal of heart and lung transplantation 2005,24, 1211–1217.
15. Bader, F.M.; Kfoury, A.G.; Gilbert, E.M.; Barry, W.H.; Humayun, N.; Hagan, M.E.; Thomas, H.; Renlund, D.Percutaneous coronary interventions with stents in cardiac transplant recipients. The Journal of heart andlung transplantation 2006, 25, 298–301.

Strait Circulation Journal 2019, 2, 1 9
16. Lee, M.S.; Lluri, G.; Finch, W.; Park, K.W. Role of percutaneous coronary intervention in the treatment ofcardiac allograft vasculopathy. The American journal of cardiology 2018, 121, 1051–1055.
17. Aqel, R.A.; Wells, B.J.; Hage, F.G.; Tallaj, J.; Benza, R.; Pamboukian, S.; Rayburn, B.; McGiffin, D.; Kirklin, J.;Bourge, R. Re-stenosis after drug-eluting stents in cardiac allograft vasculopathy. The Journal of Heart andLung Transplantation 2008, 27, 610–615.
18. Yacoub, M.; Mankad, P.; Ledingham, S. Donor procurement and surgical techniques for cardiactransplantation. Semin Thorac Cardiovasc Surg 1990, 2, 153–61.
19. Mehra, M.R.; Crespo-Leiro, M.G.; Dipchand, A.; Ensminger, S.M.; Hiemann, N.E.; Kobashigawa,J.A.; Madsen, J.; Parameshwar, J.; Starling, R.C.; Uber, P.A. International Society for Heart andLung Transplantation working formulation of a standardized nomenclature for cardiac allograftvasculopathy—2010, 2010.
20. Christensen, B.V.; Meyer, S.M.; Iacarella, C.L.; Kubo, S.H.; Wilson, R.F. Coronary angioplasty in hearttransplant recipients: a quantitative angiographic long-term follow-up study. The Journal of heart and lungtransplantation: the official publication of the International Society for Heart Transplantation 1994, 13, 212–220.
21. Wellnhofer, E.; Hiemann, N.E.; Hug, J.; Dreysse, S.; Knosalla, C.; Graf, K.; Meyer, R.; Lehmkuhl, H.B.;Hetzer, R.; Fleck, E. A decade of percutaneous coronary interventions in cardiac transplant recipients: amonocentric study in 160 patients. The Journal of Heart and Lung Transplantation 2008, 27, 17–25.
22. Roiron, C.; Sanchez, P.; Bouzamondo, A.; Lechat, P.; Montalescot, G. Drug eluting stents: an updatedmeta-analysis of randomised controlled trials. Heart 2006, 92, 641–649.
23. Ruygrok, P.N.; Farb, A.; Coverdale, H.A.; Gibbs, H.C.; Virmani, R. Histology of in-stent restenosis in atransplanted heart. The Journal of heart and lung transplantation 2004, 23, 143–146.
24. Reddy, P.R.; Gulati, A.; Steen, L.; Sinacore, J.; Leya, F.; Heroux, A. Outcomes of bare metal versusdrug-eluting stents in allograft vasculopathy. The Journal of Heart and Lung Transplantation 2008,27, 1222–1228.