Embed Size (px)
DESCRIPTION
.
Citation preview

Coronary Heart DiseaseGuidance for implementing the preventive aspects
of the National Service Framework

The Health Development Agency
The Health Development Agency (HDA) is a special health authority with a remitto improve the health of people in England and in particular, to reduce
inequalities in health. It achieves this by:
• Working with key statutory and non-statutory organisations at national,regional and local level
• Finding out what works and maintaining this evidence base
• Turning the evidence into action by building up the skills and capacity ofthose working to improve the public’s health
• Advising on the setting of standards for public health planning andpractice.

Contents
iiiINTRODUCTION
Methods used to develop the guidance 1Focusing on coronary risk factors 3
PREVENTION OF CHD THROUGHPROMOTING HEALTHIER LIFESTYLES 5
Chapter 1: REDUCING SMOKING PREVALENCE 7
1.1 Introduction 71.1.1 The National Service Framework
for coronary heart disease 71.1.2 Benefits of smoking cessation for CHD 81.1.3 Trends in smoking 8
1.2 Objectives of interventions to reduce smoking 91.3 Features of effective interventions 91.4 Components of a local strategy 10
1.4.1 Develop smoking cessation services 101.4.2 Reduce smoking in public places
including workplaces 121.4.3 Support national media campaigns 131.4.4 Use media advocacy 131.4.5 Monitor the voluntary advertising ban 141.4.6 Reduce sales of cigarettes to children
under 16 years old 141.4.7 Encourage the introduction of smoking
policies in schools 141.5 Reducing inequity 15
1.5.1 Black and minority ethnic groups 151.6 Tables of suggested activities to support
local actionIntervention, Evidence, Outcome, Who could be involved?,Skills and resources, Points to consider, Further information 17
1.7 References 21
Contents

Coronary heart disease: guidance for implementing the preventive aspects of the NSF
iv
Chapter 2: IMPROVING DIET AND NUTRITION 25
2.1 Introduction 252.2 Objectives of nutritional interventions 25
2.2.1 Professional knowledge and expertise 262.3 Features of effective interventions 272.4 Components of a local strategy 27
2.4.1 Schools 272.4.2 Local/community projects 282.4.3 Workplace 282.4.4. Healthcare 29
2.5 Reducing inequity 292.5.1 Black and minority ethnic groups 302.5.2 Children 30
2.6 Tables of suggested activities to support local actionIntervention, Evidence, Outcome, Who could be involved?, Skills and resources, Points to consider, Further information 31
2.7 References 40
Chapter 3: INCREASING PHYSICAL ACTIVITY 43
3.1 Introduction 433.2 Objectives of physical activity interventions 433.3 Features of effective interventions 443.4 Components of a local strategy 44
3.4.1 Healthcare interventions 443.4.2 Exercise referral schemes 443.4.3 Workplaces 443.4.4 Mass media 453.4.5 Schools 453.4.6 Older people 453.4.7. Physically active transport 46
3.5 Reducing inequity 463.6 Useful sources of information about community
based programmes 473.7 Tables of suggested activities to support local action
Intervention, Evidence, Outcome, Who could be involved?, Skills and resources, Points to consider, Further information 48
3.8 References 54

Contents
v
Chapter 4: REDUCING OVERWEIGHT AND OBESITY 57
4.1 Introduction 574.2 Objectives of weight management 58
4.2.1 Definitions of ‘lifestyle’ weight managementinterventions 58
4.3 Features of effective interventions 594.3.1 Skills 60
4.4 Reducing inequity 604.5 Further information 614.6 Tables of suggested activities to support
local actionIntervention, Evidence, Outcome, Who could be involved?, Skills and resources,Points to consider, Further information 63
4.7 References 68
STRATEGY DEVELOPMENT 71
Chapter 5: DEVELOPING A LOCAL STRATEGY 73
5.1 Establishing a local CHD implementation team 735.1.1 Milestones and goals 73
5.2 Developing local delivery plans 735.3 Building effective partnerships 74
5.3.1 New freedoms to promote and supportjoint working 74
5.3.2 Making the partnership effective 755.4 Involving local communities 75
5.4.1 Consulting local communities 765.4.2 Developing capacity 775.4.3 Engaging ‘excluded’ groups 77
5.5 Health needs assessment 775.6 Community profiling 775.7 Equity profiling 78
5.7.1 Audit of current provision 785.7.2 Personal and professional development audit 78
5.8 Monitoring progress 795.8.1 Developing local targets 805.8.2 Monitoring frameworks 82
5.9 Illustrative monitoring frameworks5.10 Further sources of information 875.11 References 90
Appendix 91Contributors 91
Glossary 93

Coronary heart disease is the biggest killer of men and women in this country. More than 111,000 people die fromthis condition, and about 300,000 have heart attacks every year. The national service framework for coronary heartdisease (NSF CHD), which the government published in March 2000, is our blueprint for tackling this chronic disease.This document is a key component of that blueprint.
The framework and The NHS plan describe a range of strategies to diagnose, treat and care for people who sufferfrom heart disease, and also how to prevent it occurring in the first place. The health service must give people whowant to make changes to their lifestyles, the support and advice that they need. Effective interventions at an earlystage will not only reduce the immediate risks, but also slow down the progression of the disease, identify the earlysymptoms and limit the incidence of death and long term incapacity.
This document explains how this is possible at local level. It provides evidence-based examples of effective interventionsfor dealing with all the primary risk factors for heart disease – smoking, poor nutrition, physical inactivity, overweightand obesity. It is, in effect, an early warning system for tackling heart disease.
I am confident that the document will help to transform prevention services throughout the NHS.
Alan MilburnSecretary of State for Health
Foreword by the Secretary of State for Health
i

The prevention of coronary heart disease (CHD) is agovernment priority. The white paper Saving lives: ourhealthier nation [Department of Health (DH) 1999] set atarget of reducing the death rate from heart disease,stroke and related conditions by 40% in those agedunder 75 years by the year 2010. CHD is common,frequently fatal and largely preventable. The burden ofheart disease is higher, and has fallen less in the UK than many other countries. It is the leading cause of death,killing over 110,000 people in England in 1998, including more than 41,000 under the age of 75 years (DH 2000a).
The recently published NHS plan reinforces CHD as a clinical priority and focuses on preventive aspects of the disease. The Plan emphasises theimportance of the NHS role of working in partnership with others to address health inequalities (DH 2000b). The plan highlights theimportance of the NSF CHD which, for the first time, sets out national quality standards for preventive and clinical services.
The HDA, at the request of the DH, has developed thisguidance. It is intended to assist local implementationteams [health authorities (HAs), primary care groups(PCGs) and primary care trusts (PCTs), local authorities(LAs) and other local stakeholders] in developing theirapproaches to addressing the preventive aspects of theNSF CHD. It therefore relates to Standards 1, 2, 3, 4 and 12 (see Box on the next page). The guidance should be read in conjunction with the NSF CHD main report (DH 2000c), Chapter 1 of the NSF (DH2000a) and relevant sections of Chapter 2 (DH 2000d) and Chapter 12 (DH 2000e). The HDA’sHealth update: coronary heart disease and strokeprovides useful information on trends and risk factors (HDA 2000).
The guidance covers strategy development andinterventions to promote CHD-related healthier lifestyles (smoking, nutrition, physical activity and weight management). In the strategy section, approaches that should underpin all health improvement work are covered briefly and furtherinformation is signposted where available. In the sections on risk factors, key objectives are presented that will contribute to CHD prevention together with an overview of effective approaches that will promotehealthier lifestyles. In addition to CHD, the risk factorsand the strategies listed in this resource will also have a significant impact on other initiatives in publichealth, such as The cancer plan, the forthcoming NSF for older people and the NSF on diabetes. A range of interventions to be developed locally issuggested, involving a range of players in a variety of settings, which could link with other local initiatives.
This work is evolving and represents the first stage ofsupport for those working on preventive aspects of the NSF CHD at a local level (see box on next page). The HDA welcomes comment on this document and suggestions on how to improve the guidance. Please contact Karen Ford ([email protected])or Hilary Whent ([email protected]) at the HDA.
Methods used to develop the guidance
A range of research and expert opinion has been drawnupon in preparing this report. Systematic reviews andliterature reviews have been scanned, and literaturesearches and consultation with expert informants havebeen carried out. Some 65 critical readers were sent afirst draft of this document and amendments were madein the light of their comments.
Introduction
Introduction
1

The HDA takes a broad approach to evidence, valuing arange of research methods, which contribute to themultidisciplinary nature of health improvement work.Implications from the research evidence have been drawnout and recommendations for local action are made.Gaps in the evidence base have been highlighted.
A broad front approach: upstream anddownstream
The government recognises the socio-economicinfluences on population health. In its strategy to improve
public health, it identifies the complex interaction of causes of poor health, and recommends action right across government to reduce social inequalities in health (DH 1999). Thegovernment’s strategy is informed by the evidence from the Independent Inquiry into Inequalities in Health, chaired by Sir Donald Acheson (Acheson 1998). This recommended that a broad front approach be taken to tackle the underlying, root causes of inequalities in health. The inquiry reported that policies to improve health are needed both ‘upstream’ and ‘downstream’.
Coronary heart disease: guidance for implementing the preventive aspects of the NSF
2
Preventive aspects of the National Service Framework
Reducing heart disease in the population
Standard 1
The NHS and partner agencies should develop, implement and monitor policies that reduce the prevalence ofcoronary risk factors in the population, and reduce inequalities in risks of developing heart disease.
Standard 2 The NHS and partner agencies should contribute to a reduction in the prevalence of smoking in the general population.
Milestones: pages 20–21 of NSF CHD (DH 2000c)
Prevention of coronary heart disease in high risk patients in primary care
Standard 3GPs and primary care teams should identify all people with established cardiovascular disease and offer themcomprehensive advice and appropriate treatment to reduce their risks.
Standard 4GPs and primary care teams should identify all people at significant risk of cardiovascular disease but who have notyet developed symptoms and offer them appropriate advice and treatment to reduce their risks.
Milestones: pages 25–26 of NSF CHD (DH 2000c)
Cardiac rehabilitation
Standard 12NHS trusts should put in place agreed protocols/systems of care so that, prior to leaving hospital, people admitted tohospital suffering from coronary heart disease have been invited to participate in a multidisciplinary programme ofsecondary prevention and cardiac rehabilitation. The aim of the programme will be to reduce their risk ofsubsequent cardiac problems and to promote their return to a full and normal life.
Milestones: pages 54–55 of NSF CHD (DH 2000c)

3
‘For instance, a policy which reduces inequalities inincome and improves the income of the less well off, and one which provides pre-school education for all four year olds are examples of “upstream” policies which are likely to have a wide range ofconsequences, including benefits to health. Policiessuch as providing nicotine replacement therapy onprescription, or making better facilities for takingphysical exercise, are “downstream” interventionswhich have a narrower range of benefits’ (Acheson1998).
This guidance document fully endorses this approach to improving health.
Where evidence is available on the impact of upstream policies, it is reported. However, for the most part, there is greater evidence of the impact ofdownstream policies. There are more reported studies of interventions aimed at individuals (lifestyle and health related behaviours) than there are of policies that seek to influence the broader determinants of CHD.
This preponderance of research aimed at assessing the effectiveness of downstream policies should not beseen as evidence that downstream policies are moreeffective than upstream policies. It simply reflects the fact that downstream policies tend to be more amenableto research efforts that seek to assess the effectiveness of interventions.
Focusing on coronary risk factors
‘... by April 2001 all NHS bodies, working closely with local authorities will have agreed and becontributing to the delivery of local programmes of effective policies on:a) reducing smoking b) promoting healthy eatingc) increasing physical activityd) reducing overweight and obesity’(DH 2000c, page 57; DH 2000a, page 18)
The NSF CHD focuses on three main lifestyle behaviours that are associated with risk of CHD: smoking, physical activity and diet. It also focuses on obesity, which is associated with both these last two factors, and is also independently associated with some
increase in CHD risk. In addition, there is now strongevidence that a moderate intake of alcohol reduces the risk of CHD, but an excessive alcohol intake increases the risk.
Quantifying the impact of risk factors on CHD
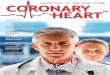
It is hard to give figures for the proportion of CHD thatcould be prevented if lack of physical activity, poor diet(high fat, low fruit and vegetables) and smoking weresuccessfully eliminated. This is because many people withheart disease have multiple risk factors, and it is hard todisentangle the separate effects. The American PublicHealth Association did make an attempt at such anestimate (Smith and Pratt 1993) and the results areshown in the box below. A similar modelling exercise inthe UK would be expected to produce slightly differentfindings because more of the UK population are smokers,while fewer are obese. However, the information is usefulin giving some indication of the relative importance ofthese risk factors in terms of the potential for making animpact on CHD rates.
In the following sections, information is presented abouteffective interventions, which aim to bring about changein these risk factors. Implications are drawn from theevidence and suggestions are made for local action at anumber of levels, involving a range of players and linkingto other local initiatives. Further information sources arealso signposted.
The gaps have been identified in the evidence base. There is an urgent need for more and better designedevaluations of interventions aiming to improve health andwell being and the dissemination of results. Evaluation is
Introduction
Proportion of CHD attributable to variousmodifiable risk factors in the USA
Risk factor Best estimate Range% %
Cholesterol >200 mg/dl 43 39–47Physical inactivity 35 23–46Cigarette smoking 22 17–25Obesity 17 7–32
Source: Smith and Pratt (1993)

a planned set of activities, which helps people to see how work is progressing and whether or not it iseffective. It should be seen as an integral part of projectsand programmes. Evaluation requires relevant skills and it is worth considering making links with local researchers(within the NHS, LAs and academic institutions). There are many approaches to evaluation and sources of supportare listed on p89.
References
Acheson, D., 1998. Independent inquiry into inequalities in health.
London: The Stationery Office.
DH, 1999. Saving lives: our healthier nation. London: The Stationery Office.
DH, 2000a. National service framework for coronary heart disease:
Chapter 1. Reducing heart disease in the population. London: DH.
DH, 2000b. The NHS plan. A plan for investment. A plan for reform.
London: The Stationery Office.
DH, 2000c. National service framework for coronary heart disease: main
report. London: DH.
DH, 2000d. National service framework for coronary heart disease,
Chapter 2. Preventing coronary heart disease in high risk patients.
London: DH.
DH, 2000e. National service framework for coronary heart disease:
Chapter 12. Cardiac rehabilitation. London: DH.
HDA, 2000. Health update: coronary heart disease and stroke.
London: HDA.
Smith, C. and Pratt, M., 1993. Cardiovascular disease. In: R. Brownson,
P. Remington and J. Davis, eds. Chronic disease epidemiology and
control. Washington: American Public Health Association.
Coronary heart disease: guidance for implementing the preventive aspects of the NSF
4

1.1 Introduction
Smoking is the cause of one out of every seven deathsfrom heart disease (nearly one in four deaths among menand one in 10 among women). Nine in 10 deaths fromlung cancer among men and nearly three in four amongwomen are estimated to have been caused by smoking –84% of all lung cancer deaths. Among those aged under65 years, two in five deaths from stroke were caused bysmoking. Smoking is also linked to many other seriousconditions, including asthma and other respiratory illnesses, cataracts, peripheral vascular disease,periodontal disease and brittle bone disease (Callum1998). Treating the illnesses and diseases caused bysmoking is estimated to cost the NHS up to £1.7 billionevery year (Raw et al. 1998).
Passive smoking – breathing in other people’s tobaccosmoke – is also a major cause of mortality and morbidity.It contributes to death from heart disease and a range ofother health problems (Royal College of Physicians 1992).
In December 1998, the Government’s first-ever whitepaper on tobacco, Smoking kills, set three targets, foradults smoking, smoking during pregnancy and childrensmoking (DH 1998a).
• To reduce adult smoking in all social classes so that the overall rate falls from 28% to 24% or less by2010, with a fall to 26% by the year 2005. In terms oftoday’s population, this would mean 1.5 million fewersmokers in England.
• To reduce the percentage of women who smokeduring pregnancy from 23% to 15% by the year 2010,with a fall to 18% by the year 2005. This will meanapproximately 55,000 fewer women in England whosmoke during pregnancy.
• To reduce smoking among children from 13% to 9% or less by the year 2010, with a fall to 11% by the year 2005. This will mean approximately110,000 fewer children smoking in England by the year 2010.
The cancer plan published in September 2000 introduces new national and local targets to address inequalities in smoking rates between socio-economic groups. At a national level the target is:
• To reduce smoking rates among manual groups from32% in 1998 to 26% by 2010 (DH 2000a).
1.1.1 The National Service Frameworkfor coronary heart disease
The NSF CHD (DH 2000b) states that ‘by October 2000 HAs, LAs, PCGs/PCTs and NHS trusts will have set up, or have firm plans in place [for a range of NHSsmoking cessation services which will enable national and regional targets for the numbers of smokers quitting to be met]. By April 2001, HAs, LAs, PCGs/PCTsand NHS trusts will have agreed and be contributing tothe delivery of the local programme of effective policieson reducing smoking; as an employer, have implementeda policy on smoking and be able to refer clients/serviceusers to specialist smoking cessation services, includingclinics …’
The immediate priorities for implementing the smokingcessation area of the NSF CHD are:
• By April 2001, health authorities will introducespecialist smoking cessation clinics, helping 150,000people
Chapter 1Reducing smoking prevalence
Reducing smoking prevalence
7

• Delivering the early milestones set out in Chapter 1 ofNSF CHD: Reducing heart disease in the population(DH 2000b).
The requirements of smoking cessation are detailed in Appendix A, Chapter 1 of NSF CHD: Reducingheart disease in the population (DH 2000b).
1.1.2 Benefits of smoking cessation for CHD
The costs and benefits of smoking cessation are wellestablished (Raw et al. 1998).
• Reductions in smoking prevalence are guaranteed to bring population health gains (Raw et al. 1998; US Department of Health and Human Services 1990).
• Smoking cessation reduces the risk of dying fromsmoking related diseases.
Smokers have about twice the risk of dying fromCHD compared with lifetime non-smokers. Thisexcess risk is reduced by about half among ex-smokers after only one year of abstinence anddeclines gradually thereafter. After 15 years ofabstinence, the risk of CHD is similar to that ofpeople who have never smoked (Tang et al. 1992).
Smoking cessation is particularly important in thesecondary prevention of CHD. In smokers with existing CHD, the risk of premature CHD mortalitycan be reduced by 50% or more on giving up (USDepartment of Health and Human Services 1990).
• Reductions in smoking prevalence will produce sizeablereductions in common hospitalised events and costs(Naidoo et al. 1999).
• The cost savings that can be made through moderatesuccess in smoking cessation programmes aresignificant and cumulative (Naidoo et al. 1999).
1.1.3 Trends in smoking
AdultsThe prevalence of smoking in the UK over the past 20years or so has fallen. In 1998, 27% of adults aged 16 years and over smoked cigarettes compared with 40%
in 1978. However, most of this decline occurred in the1970s and 1980s. In the 1990s, the decline in smokingprevalence among adults levelled off (DH 2000c).
The prevalence of smoking is higher among people inmanual than non-manual social classes (32% comparedwith 21% in 1998). The widening of this gap over thepast 20 years reflects a steeper decline in smokingprevalence among non-manual classes compared withmanual classes (DH 2000c).
The social class differentials in smoking are reflected inthe social gradients of deaths caused by smoking. Thepercentage of deaths from ischaemic heart diseasecaused by smoking ranges from 39% for men aged35–64 years in social classes I–II to 49% of those inclasses IV–V. For women aged 35–64 years the figuresrange between 35% for classes I–II to 46% for classes IV–V (Callum 1998).
Pregnant womenThe proportion of women who smoke during pregnancyhas fluctuated over the past eight years (Owen et al. 1998;Owen and Penn 1999). In 1999 nearly a third of women(30%) smoked during pregnancy compared with 27% in1992. Among young pregnant women (aged 16–24 years)from social groups C2DE (similar to manual and unemployedclasses), the percentage is even higher, with 51% smokingduring pregnancy in 1999 (Owen and Penn 1999).
TeenagersIn 1999, an estimated 9% of children aged 11–15 yearssmoked cigarettes (DH 2000c). This figure has variedconsiderably over time, showing a low of 8% in 1988and a high of 13% in 1996 (DH 2000b). As the majorityof smokers take up the habit in their teens, any increasesin the rates of young smokers will eventually feedthrough into adult smoking rates.
Black and minority ethnic groupsCigarette smoking among minority ethnic groups isgenerally less than among the UK population as a whole(28%1). However, a more detailed examination revealsimportant differences between and within groups. Thesmoking rate among Bangladeshi men is very high (49%).
Coronary heart disease: guidance for implementing the preventive aspects of the NSF
8
1Differences between the HEA (1999a) and DH (2000c) surveys in
timing and methodology most likely account for the 1% difference in
the estimates of the percentage of adults who smoke.

This same group of men also has high rates of chewingtobacco products. Smoking rates are even higher amongmiddle-aged and older Bangladeshi men (54% and 70%for men aged between 30–49 and 50–74 years,respectively). Smoking rates among African-Caribbeanmen and women resemble, and sometimes exceed, therates for the UK population as a whole. Smoking ratesamong African-Caribbean women are higher for youngerwomen [Health Education Authority (HEA) 1999a].
Poverty and smokingTraditional measures of social class tend to underplay theextent to which smoking has become concentrated in thepoorest sections of society. Recent studies have shownthat smoking levels have remained virtually unchangedamong those in the poorest groups, and among lonemothers smoking levels have risen (Marsh and McKay1994; Dorsett and Marsh 1998; Jarvis 1998). In a detailedstudy, lone parents living in rented accommodation andrelying on social security benefits were found to havesmoking levels in excess of 75% (Dorsett and Marsh 1998).
1.2 Objectives of interventions to reduce smoking
The importance of a comprehensive approach has longbeen recognised (WHO 1979). As well as approachesaimed at the individual, there has been a recognition ofthe need for policy and legislative measures and socialand environmental initiatives as essential components ofany strategy to reduce tobacco use (WHO 1998). Ideally,each component of such a comprehensive strategy wouldencompass the following objectives:
• Promote quitting (not cutting down) among adults andyoung people
• Reduce exposure to environmental tobacco smoke
• Create a social environment that is supportive of non-smoking and cessation.
In the context of reducing smoking among adults, asecondary objective could include strategies to preventthe uptake of smoking among young people. However, it is important to note that there is little evidence thatteenage strategies, especially in the absence of adultstrategies, have any impact on the uptake of smokingamong children (Reid 1996; Hill 1999).
Local strategies to reduce smoking prevalence shouldreflect the policies and population groups set out in thewhite paper on tobacco Smoking kills (DH 1998a), TheNHS plan (DH 2000d, Chapter 13), NSF CHD (DH 2000b)and The cancer plan (DH 2000a).
Local strategies should also include an alliance of NHS,local government, education and commercial interests, as well as voluntary agencies, to help reduce smokingand to provide information on smoking by using localmedia, creating local activities and promoting debate togenerate interest. Some areas of the country already have smoking alliances. These cover about 60% of thepopulation of England and are supported by the DH.
1.3 Features of effective interventions
A comprehensive approach – combining community wideapproaches with economic and regulatory measures –was identified by the US Surgeon General as the strategy most likely to have the greatest long-term,population impact (US Department of Health and Human Services 2000). Educational and clinicalapproaches were considered to be of greater importance in helping individuals resist or abandon the use of tobacco.
Community wide approaches typically involve a range of agencies including health services, voluntary agencies, the media (paid and unpaid), as well as government andlocal authorities (see 5.3, Building effective partnerships,p74). Together, they undertake a range of activities suchas direct smoking cessation, helplines, training andresources for health professionals, development ofpolicies to reduce smoking in public places, mediacampaigns and advocacy, reducing sales to minors andwork in schools. Overall, community interventions seek toinfluence both individual behaviour and the environmental,social and cultural conditions that affect tobacco use(Lantz et al. 2000).
The impact of a comprehensive approach is difficult toevaluate, especially given the potential for individualcomponents to work synergistically to produce combined effects (Chapman 1993; US Department ofHealth and Human Services 2000). For example, theeffectiveness of school based programmes appears to be enhanced when they are included in broad basedcommunity interventions (Lantz et al. 2000). Nevertheless,
Reducing smoking prevalence
9

studies that have sought to measure the effects of acomprehensive approach have yielded encouragingresults (US Department of Health and Human Services2000; Lantz et al. 2000; Sowden and Arblaster, 2000a,b;Wakefield and Chaloupka 2000).
It is accepted that population-wide approaches should aimto reduce both adult and teenage smoking. But where shouldthe emphasis lie? Experts agree that teenage smoking ratesare unlikely to decline in the absence of a fall in adult rates.The view that smoking among adults should therefore betackled ahead of teenagers was discussed by Hill (1999)in a recent article. His argument is fivefold:
• First, reducing smoking among adults will lead to aquicker and bigger reduction of tobacco related harm, because there is a higher level of smokingrelated mortality and morbidity among adults thanteenagers
• Second, reducing smoking among adults will provideprotection to the unborn and recently born againstexposure to direct and indirect tobacco smoke
• Third, quitting by adults (especially by parents) reducesthe likelihood of children taking up smoking
• Fourth, while there are clear ethical reasons foreducating children about what is the largestpreventable cause of death, beyond this, the methodsof delivering interventions are fraught with practicalproblems and the evidence of effectiveness ofinterventions aimed at young people is poor
• Finally, the fact that the tobacco industry itselfsupports antismoking campaigns targeted at teenagersshould be taken as a warning signal: ‘Even PhillipMorris was confident that [antismoking] youthcampaigns could do them little damage’ (Hill 1999).
1.4 Components of a local strategy
1.4.1 Develop smoking cessation services
• The health improvement programme (HImP) shouldemphasise the importance of an integrated serviceincluding primary care advice, specialist smoking cessationclinics, one-to-one cessation advice [Health Service Circular(HSC) 1998, 1999; Action on Smoking and Health
(ASH) 2000a,b]. The requirements for smoking cessationare detailed in Appendix A, Chapter 1 of NSF CHD:Reducing heart disease in the population (DH 2000b).
• Build upon and develop these guidelines for localcessation services.
• Provide special services for pregnant women.
The NHS plan (DH 2000d) states that ’the specialistsmoking cessation services will focus on heavilydependent smokers needing intensive support, and onpregnant smokers as part of antenatal care. Primary caregroups will take the lead in commissioning – and whereappropriate providing – these services’. In support of thesmoking cessation treatments bupropion is now availableon prescription and The NHS plan recommends thatnicotine replacement therapy (NRT) should also be madeavailable on prescription. These services followedevidence based guidelines for smoking cessationpublished in December 1998 (Raw et al. 1998). Theseguidelines have been updated and will be available inDecember 2000. The Committee on Safety of Medicineswill consider whether NRT can be made available forgeneral sale. An evaluation of the first year of thedevelopment of the national cessation services hasrecently been published (Adams et al. 2000).
At a meeting of smoking cessation experts held in July2000, it was agreed that the smoking cessation servicesshould offer support to all people who request it. Thefocus on particular groups could be achieved throughrecruitment to the services – for example by engagingmidwives or promoting the services at antenatal classes(ASH 2000a,b; http://www.ash.org.uk/?cessation). Themeeting, with representation from the DH, identified amodel approach to smoking cessation services in primarycare, which also sought to provide clarification on the roleof intermediate cessation services. Discrepancies in theguidelines concerning intermediate services had causedconfusion in some health action zones (HAZs) (Adams etal. 2000). Both intermediate services and specialist clinicshave been subsumed in the model by the term ‘qualifyingspecialist services’ for which a minimum standard ofservice to the smoker has been set and for which thecentrally provided smoking cessation budget may be used.
The model of the service is set out in Figure 1 on facingpage. For full details and further guidance see: http://www.ash.org.uk/?cessation
Coronary heart disease: guidance for implementing the preventive aspects of the NSF
10

Model of the service to the smokerEach smoker contacting the NHS should be offered apackage of both pharmaceutical aids and behaviouralsupport that meets their particular needs and circumstances.Given restrictions on who can prescribe drugs, andlimitations on the extent to which those who mayprescribe are able to offer support, it will not always bepossible to provide a ‘one-stop shop’. The aim must be tomake access to drugs and support as straightforward aspossible. The elements of the support package include:
• Influences on smokers’ motivations to quit, includingadvice from primary care professionals, nationalcampaigns, No Smoking Day and manufacturers’advertising
• Brief opportunistic interventions by the GP and otherprimary care professionals
• Prescribing pharmacotherapies: NRT and bupropion(Zyban)
• Behavioural support. This will need to be tailored tomatch the circumstances of the smoker, but the rangeof options includes:
Referral to a ‘qualifying’ specialist service – thesewould qualify for funding from the smokingcessation budgets if they offered a certain minimum service standard
Discussion of other support options (eg telephone,self-help) that the smoker could consider, if he/shechose not to attend a qualifying specialist service.
Reducing smoking during pregnancyFor pregnant women, pregnancy specific materials aremore cost effective than less specific, cheaper, standardinformation because of their greater effectiveness (Buckand Godfrey 1994). The intensity of the intervention alsoaffects outcome. While there is some evidence of theeffectiveness of advice when literature is coupled withfollow up, more intensive interventions (eg a structured
Reducing smoking prevalence
11
Figure 1. Configuration of smoking cessation support services.

cessation course based on self-help booklets) providestronger evidence (Raw et al. 1998). Public educationcampaigns may be effective in shifting pregnant women’sattitudes and behaviour (Campion et al. 1994). Thedifficulties of advising outright cessation in pregnancy hasled some health professionals to suggest cutting down asan alternative. However, there is little evidence to showthat cutting down is of any health benefit (Raw et al.1998). Thus quitting as opposed to cutting down needsto be emphasised.
Many women who do stop smoking in pregnancy goback to smoking after the birth of the baby. In oneAmerican study over half (56%) of women who stoppedduring pregnancy were smoking within one month of thebirth (Secker-Walker et al. 1995). Relapse preventioninterventions with pregnant women and women whohave recently given birth are needed.
• All those responsible for providing antenatal careshould ensure that relapse prevention is included as a component in the smoking cessation service.
The lower rate of cessation associated with mothers from lower socio-economic groups, led the ScientificAdvisory Group on Inequalities to conclude that‘interventions that target the individual behaviour alone may not be sufficient ... broader policies to combat inequality are also required’ (Acheson 1998).
Further information on smoking and pregnancy can beobtained in the following reports:
• Smoking and pregnancy: a survey of knowledge,attitudes and behaviour 1992–1999 (Owen and Penn1999)
• Smoking and pregnancy: guidance for purchasers andproviders (HEA 1994a)
• Helping pregnant smokers quit: training for healthprofessionals (HEA 1994b)
• Smoking and pregnancy: developing a communications strategy for cessation (Owen and Bolling 1996)
• Smoking and pregnancy: a growing problem (HEA1996a).
Mechanisms for delivering cessation services for youngpeople are outlined in the document Smoking cessationin young people: should we do more to help youngpeople quit? (HDA 2000a).
1.4.2 Reduce smoking in public places including workplaces
Restricting smoking is important not only for limiting thepublic’s exposure to toxins in sidestream smoke, but alsofor broader policy reasons. First, it puts smoking in abroader context than one of personal choice and personalrisk and legitimises it as a social problem; second, it maybe the source of litigation against employers or businesses;and third, the spread of smoking restrictions reduces theopportunities to smoke and thus reduces consumption(Borland et al. 1991; Brenner and Mielck 1992; Marcus etal. 1992; Wakefield et al. 1992; Jeffery et al. 1994;Glasgow et al. 1997; Brauer and Mannetje 1998).
The Health and Safety Executive (HSE) has beenexamining current practice on restricting smoking at workwith a view to issuing an Approved Code of Practice (ACoP).There are potential legal liabilities for employers who donot address passive smoking in the workplace. Employeeshave recourse to civil law, contract and employment lawand the general provisions of the Health and Safety atWork Act (1974). The ACoP will clarify the legal positionfor both employers and employees, and enable LAenvironmental health officers (EHOs) to intervene.
Local plans should include objectives to:
• Ensure that all local hospitals have smoking policies(DH 1998a; HEA 1999b), and that these are fullyimplemented
• Implement policies to restrict smoking in public places[Scientific Committee on Tobacco and Health (SCOTH)1998]
• Encourage restaurants, bars and other leisure facilitiesto provide smoke free areas.
Many employers now find an advantage in smokingrestrictions through savings on sickness absences,increased productivity, lower insurance and cleaningcosts. The checklist in Box 1.1 will help managers ofworkplaces to develop an effective strategy on smoking.
Coronary heart disease: guidance for implementing the preventive aspects of the NSF
12

Further informationFor examples of case studies of effective practice withinthe NHS see Tobacco control policies within the NHS:case studies of effective practice (HDA 2000b). For furtherinformation on developing, reviewing and amendingtobacco control policies, see Been there, done that: revisitingtobacco control policies in the NHS (HEA 1999b). Samplepolicies and consultation questionnaires can be found inSmoking policy for the workplace: an update (HEA 1999c)and Towards tobacco-free environments: guidelines forlocal authorities (HEA 1999d). Also see the ASH website:http://www.ash.org.uk
1.4.3 Support national media campaigns
Mass media campaigns can influence smoking behaviour(DH 1998a; Lantz et al. 2000; Sowden and Arblaster2000a,b) and may be especially appropriate for reachingthose who are less educated (Mackaskill et al. 1992) andthose in poor communities (Jenkins et al. 1997). Messagecontent and the intensity and duration over which themessages are delivered appear to be important factors indetermining the impact of mass media campaigns (Greyet al. 2000; Lantz et al. 2000).
Media campaigns should focus predominantly on adults,since the majority of cigarettes (>95%) are consumed byadults and adult smokers are a major factor influencingthe uptake of smoking by minors.
Local media may be used to raise the profile of nationalcampaigns (No Smoking Day). For ideas in planning localmedia campaigns see: http://www.no-smoking-day.org.uk/campaign.htmTel: 020 7916 8070.
• Local plans should include links to the network of localsmoking control alliances in England.
1.4.4 Use media advocacy
There is some evidence that the use of media advocacy(see Box 1.2) may affect tobacco consumption (Buck andGodfrey 1994), but its major role is in social marketing.This involves shaping the media agenda, prompting policychanges and influencing the social norms aroundsmoking (Reid et al. 1992). Media advocacy techniques
Reducing smoking prevalence
Box 1.1 Management checklist for a smoking policy
• Review current situation.• Assess need, capacity to change.• Make sure you consult with everyone.• Seek feedback, not permission.• Decide on the policy details.• Decide on a total or partial ban.• Decide what restrictions to impose if a total ban
is not possible.• Communicate final decisions clearly to all staff.• Label smoking and smoke-free areas.• Monitor and review the policy.
Source: HEA (1999c)
Box 1.2 Checklist for setting up local media advocacy work
First think about the following points:• What you hope to achieve• Who your campaign is aimed at• How much you think it will cost• How it will be supported by local activity and
action• How you plan to evaluate it (have you achieved
what you hoped?).
Create a media plan:• What stories or angles will attract the media?• What information is needed for a newsworthy
press release?• Draw up a media list – names and contact
numbers of relevant journalists• Find out the deadlines for media you are
targeting• Find out how media contacts want you to
communicate with them (press release, directcontact)
• Decide who will act as spokespersons• Coordinate media schedules with partners who
may also be using the media• If the campaign is a long one, create a media
calendar to ensure a constant supply of newsitems.
13

may be especially effective with poor communities(Jernigan and Wright 1993) since low income groups,including smokers, are high consumers of TV.
For further guidance on media advocacy and factors thatinfluence its effectiveness, see An investigation into thepotential of media advocacy as a health promotionstrategy (HDA in press).
1.4.5 Monitor the voluntary advertising ban
Indirect marketing of cigarette brands is the growing andpreferred marketing strategy of the tobacco industry,perhaps in response to threats of advertising restrictions.Until legislation is introduced, the existing ‘voluntaryagreements’ on tobacco promotion should continue to be monitored locally, not so much because theserestrictions have been found to be effective in preventinguptake of smoking, but because infringement of the rules offers opportunities for media advocacy. Thoseprovisions include, for example, banning advertising onbillboards near schools and promotions in magazines foryoung people.
People working locally should be vigilant in monitoring anynew marketing strategies, for example, using events atdiscos, student functions and the Internet to promote brands.
1.4.6 Reduce sales of cigarettes to children under 16 years old
Combining regular test purchasing with a high profilemedia approach has been found to be successful inreducing the incidents of reported sales of cigarettes topeople under 16 years of age. Overall, the evidence ofeffectiveness of sales restrictions suggests that vigorouslocal enforcement of the law forbidding sale of tobaccoto under-16s can reduce sales (Stead and Lancaster2000). This strategy has also been shown to have a small delaying effect on the uptake of smoking amongchildren. There is little evidence, however, to suggest thatit has any effect on the uptake of smoking amongchildren. Considerable resources are required, both interms of trading standards officers’ and court time.
The existing law is not being applied effectively (DH1998a). The Local Government Association and LocalAuthorities Co-ordinating Body on Food and Trading are
developing a new enforcement protocol to address this.Features of the protocol are listed in Box 1.3.
Proof-of-age card schemes have been developed, but thegovernment recommends that a single system be agreed. Thevending machine trade association, the National Associationof Cigarette Machine Operators, has produced a new,stricter code for its members to clarify siting arrangementsand monitoring for vending machines (DH 1998a).
1.4.7 Encourage the introduction of smoking policies in schools
A formal, well publicised school policy on smokingreinforces non-smoking as the norm in society, supportshealth messages in the curriculum and may have positive effects on smoking levels among pupils, staff and all adult users of the premises (see Box 1.4).Additional potential benefits include reducedabsenteeism, reduced costs and elimination of theharmful effects of passive smoking.
• Provide support to schools to introduce no smokingpolicies.
The National Curriculum Science Order recommends thatteaching the harmful effects of tobacco, alcohol andother drugs should begin at Key Stage 2 (age 7–11years). The Office of Fair Standards and Training inEducation (OFSTED) 1999 report Drug education inschools and the Department for Education andEmployment (DfEE 1998) report Protecting young people:good practice in drug education in schools and the youth
Coronary heart disease: guidance for implementing the preventive aspects of the NSF
Box 1.3 Enforcement protocol
• Local authorities should publish a clear statementon underage tobacco sales.
• Ensure that all shops and vending machinesdisplay notices stating the law.
• Use test purchases to assess local compliance byretailers. Gather information about premiseslikely to be breaching the law.
• Use media advocacy to raise the profile locally.• Educate to increase compliance.• Detail enforcement action taken, prosecutions
and fines, to act as a deterrent.
14

service recommend teaching young people from the ageof five years upwards about the risks and consequencesof tobacco, alcohol and drug use, together with teachingthe life skills needed to resist the pressure to misuse thesesubstances. Teaching should clearly cover issues relevantto the child’s age and experience. This frequently entailstackling smoking and alcohol-related issues first, as theseare the substances that young people will generally beexposed to first.
1.5 Reducing inequity
With little or no decline in the lowest income groups,smoking has become concentrated in Britain’s pooresthouseholds. For example, among lone parents on benefitsand living in council housing, more than three-quarterssmoke (Dorsett and Marsh 1998). Moreover, recentresearch suggests that nicotine dependence is higher inpeople experiencing disadvantage (Jarvis and Wardle1999). In keeping with these findings, the Independent
Inquiry into Inequalities in Health recommended a short-term strategy to reduce nicotine dependence, which islikely to be stronger in disadvantaged smokers, throughthe provision of free NRT. A complementary, longer-termstrategy aims at removing the cultural and environmentalbarriers that disadvantaged people face. Communitybased interventions, brief advice from a GP andspecialised smoking clinics are also recommended aseffective settings in which to provide NRT (Acheson 1998).
Attempts to set up community based projects to promotesmoking cessation have met with mixed success. In areport of initiatives set up in low income communities inScotland, the authors concluded that:
‘small grant funding for time limited projects canpromote work on smoking amongst women livingor working in low income communities. Althoughreducing smoking was a long term goal for themajority of the initiatives most did not perceivethemselves as a cessation group. As a result they did not measure success by the numbers quitting.Changes in individual smoking behaviours werenoted and these ranged from extending the period of smoke free time, to restricting smoking to a specific room or location and trying nicotinereplacement therapy’ (ASH Scotland and HEBS 1999).
Examples of other community based projects fundedthrough small grants schemes can be found inEmpowering smokers to quit: success principles forcommunity stop-smoking projects (HEA 1996b).
The use of mass media, especially TV, may be particularly appropriate for reaching less educated and/ordisadvantaged smokers. This reflects the tendency for theless educated to receive information from TV more oftenthan those who are more educated (Buck and Godfrey1994). Indeed, research has shown that mass mediaantismoking campaigns can have a significant impact onlow income and low educational groups (Macaskill et al.1992; Jenkins et al. 1997).
1.5.1 Black and minority ethnic groups
Little has been published on the impact of smokingcessation interventions in reducing tobacco use amongblack and minority ethnic groups in England. However,studies from the USA suggest that they can be effective
Reducing smoking prevalence
15
Box 1.4 Checklist for a school’s smoking policy
• Put the development of a smoking policy on theagenda.
• Review the current situation.• Identify staff with sufficient skill and seniority to
take responsibility for developing a new policy ifnecessary.
• Form a working party involving key people fromthe school and community, if appropriate.
• Establish a rationale for the policy.• Identify educational, health and economic
reasons for introducing a policy or improvingexisting conditions.
• Draft the policy.• Evaluate the draft policy by consulting with all
relevant parties, identify potential constraints andproblems.
• Inform everyone about the policy before it isimplemented.
• Allow sufficient time for implementation of thenew policy – three to six months is considered areasonable time between initiating andimplementing the policy.
• Monitor the operation of the new policy.

(Botvin et al. 1992; Elder et al. 1993; Lillington et al.1995; Elder et al. 1996). In the absence of UK studies,patterns of tobacco use (HEA 1999a) and research intothe role of tobacco within and between black andminority ethnic groups (Maltby et al. 2000) can providesome pointers for the way forward. Examples of these arehighlighted below (HEA 1999a; Maltby et al. 2000).
• The high rates of tobacco chewing, especially among Bangladeshis, suggests that this practice should be included in interventions aimed at reducingtobacco use.
• Sensitivity to gender issues is vital.
• Literature should be multi-lingual and in a style that isculturally familiar (eg use of vignettes to highlighthealth risks associated with tobacco use).
• Information campaigns should be developed to redressmisperceptions about tobacco use (eg belief thattobacco use can relieve indigestion; belief that healthypractice in other areas such as diet and exercise willoffset the detrimental effects of smoking).
• Ethnic differences in attitudes and beliefs aboutcigarette smoking should be incorporated into smokingcessation interventions.
Thus, to be successful, a tobacco cessation campaignmust take account of the culture, tradition and religion of the particular target group. In so doing it
will need to involve community groups, religious groups,smoking cessation coordinators, local tobacco alliances,primary health care (PHC) teams, culturally relevant localand national media as well as key individuals withindifferent ethnic groups.
In response to ethnic health inequalities, the governmenthas announced that £1,000,000 will be made available to help reduce the high rates of smoking among certainethnic groups.
Further information on black and minorityethnic groupsDH, 1996. Directory of ethnic minority initiatives, G60/008 3934 1P 5K
May 96 (23). London: DH.
Gervais, M. and Jovchelovitch, S., 1998. The health beliefs of the
Chinese community in England: a qualitative research study.
London: HEA.
HEA, 1999. Black and minority ethnic groups and tobacco use in
England: a practical resource for health professionals. London: HEA.
HEA, 2000. Black and minority ethnic groups in England: the second
health and lifestyles survey. London: HEA.
McKeigue, P. and Sevak, L. 1994. Coronary heart disease in South
Asian communities. London: HEA.
Sproston, K., Pitson, L., Whitfield, G. and Walker E., 1999. Health
and Lifestyles of the Chinese population in England. London: HEA.
Coronary heart disease: guidance for implementing the preventive aspects of the NSF
16

Reducing smoking prevalence
17
Dep
ends
on
the
part
icul
arin
terv
entio
n un
der
cons
ider
atio
n (s
ee b
elow
).
Can
dou
ble
the
effe
ctiv
enes
sof
an
inte
rven
tion,
be
it br
ief
advi
ce f
rom
a G
P or
inte
nsiv
esu
ppor
t th
roug
h a
spec
ialis
tcl
inic
or
will
-pow
er a
lone
.
Inte
rven
tion
Smok
ing
cess
atio
n
Nic
otin
ere
plac
emen
tth
erap
y
Bupr
opio
n (Z
yban
)
Evid
ence
Effe
ctiv
enes
s an
d co
st e
ffec
tiven
ess
are
wel
l est
ablis
hed
(Fio
re e
t al
.19
96; R
aw e
t al
. 199
8). U
pdat
edgu
idel
ines
(Dec
200
0).
Dou
bles
cha
nce
of s
ucce
ss o
fsm
oker
s w
ishin
g to
sto
p (F
iore
et
al.
1996
; Raw
et
al. 1
998)
.
Just
laun
ched
in t
he U
K. A
nef
fect
ive
phar
mac
othe
rapy
(Hur
t et
al. 1
997;
Jor
enby
et
al. 1
999)
, it
will
be a
vaila
ble
on p
resc
riptio
n.
Wh
o c
ou
ld b
ein
volv
ed?
Hea
lth p
rofe
ssio
nals,
LAs,
spe
cial
istsm
okin
g ce
ssat
ion
coor
dina
tors
,vo
lunt
ary
sect
or,
HA
Zs, l
ocal
sm
okin
gal
lianc
e.
PHC
, pha
rmac
ists,
heal
th p
rom
otio
nsp
ecia
lists
.
GPs
and
tho
seap
prov
ed f
orpr
escr
ibin
g th
roug
hth
e Pa
tient
Gro
upD
irect
ive,
PHC
, pha
rmac
ists,
heal
th p
rom
otio
nsp
ecia
lists
.
Skill
s an
d r
eso
urc
es
Smok
ing
cess
atio
n sk
ills,
carb
on m
onox
ide
mon
itor,
leaf
lets
. Alth
ough
tra
inin
gsc
hem
es a
re a
vaila
ble
natio
nally
, acc
redi
ted
cour
ses
shou
ld b
e es
tabl
ished
.D
emon
stra
te c
ultu
ral
sens
itivi
ty.
Smok
ing
cess
atio
n sk
ills,
acce
ss t
o N
RT p
rodu
cts.
Smok
ing
cess
atio
n sk
ills.
Poin
ts t
o c
on
sid
er
Maj
or c
ompo
nent
of
gove
rnm
ent
stra
tegy
to
redu
ce s
mok
ing
in E
ngla
nd.
HSC
(199
9) h
as s
et o
utgu
idel
ines
on
mon
itorin
g fo
rth
e ne
w s
ervi
ces.
The
avai
labi
lity
and
acce
ssib
ility
of
serv
ices
sho
uld
take
acc
ount
of
cultu
ral
diff
eren
ces.
Cur
rent
ly, s
ome
are
avai
labl
eon
pre
scrip
tion
as w
ell a
sbe
ing
avai
labl
e ov
er t
heco
unte
r (O
TC).
Nas
al s
pray
isO
TC a
nd 2
mg
gum
is a
lsoav
aila
ble
on t
he g
ener
al s
ales
list
(GSL
).
Pres
crip
tion
only
.
Furt
her
info
rmat
ion
HSC
(199
8, 1
999)
, DH
(199
8a),
Ach
eson
(199
8).
Coc
hran
e Li
brar
y w
ebsit
e:ht
tp://
ww
w.u
pdat
e-so
ftw
are.
com
/clib
hom
e/cl
ib.h
tmEv
alua
tion
of y
ear
one
ofna
tiona
l ces
satio
n st
rate
gy(A
dam
s et
al.
2000
). A
SH(2
000a
).
See
abov
e.
Ou
tco
me
Tabl
e 1.
6 Su
gges
ted
acti
viti
es t
o su
ppor
t lo
cal a
ctio
n

Coronary heart disease: guidance for implementing the preventive aspects of the NSF
18
Brie
f ad
vice
in N
HS
and
prim
ary
care
Ve
ry b
rief
advi
ce (t
hree
min
utes
) can
res
ult
in a
2%
incr
ease
in n
umbe
r of
smok
ers
abst
inen
t fo
r six
mon
ths
or lo
nger
com
pare
dw
ith n
o ad
vice
. Brie
f ad
vice
(10
min
utes
) can
res
ult
in a
3% in
crea
se. A
ddin
g N
RT t
obr
ief
advi
ce c
an r
esul
t in
a6%
incr
ease
.
Com
pare
d w
ith n
oin
terv
entio
n in
tens
ive
supp
ort
can
resu
lt in
an
8% in
crea
sein
the
num
ber
of s
mok
ers
abst
inen
t fo
r six
mon
ths
orlo
nger
.
Resu
lt in
a 5
% in
crea
se in
the
num
ber
of s
mok
ers
abst
inen
tfo
r six
mon
ths
or lo
nger
.
Resu
lt in
a 7
% in
crea
se in
the
num
ber
of s
mok
ers
abst
inen
tfo
r six
mon
ths
or lo
nger
.
Qui
t ra
te o
f 15
.6%
(adj
uste
d)re
port
ed in
Eng
land
with
mas
s m
edia
cam
paig
n (O
wen
2000
).
Inte
nsiv
e su
ppor
t(e
g sm
oker
s’ c
linic
s)
Cess
atio
n ad
vice
and
supp
ort
for
hosp
ital
pat
ient
s
Cess
atio
n ad
vice
and
supp
ort
for
preg
nant
sm
oker
s
Tele
phon
ehe
lplin
es
Fior
e et
al.
1996
; Raw
et
al. 1
998;
upda
ted
guid
elin
es (D
ec 2
000)
.
Fior
e et
al.
1996
; Raw
et
al. 1
998;
upda
ted
guid
elin
es (D
ec 2
000)
.
Raw
et
al. 1
998;
Fio
re e
t al
. 199
6;up
date
d gu
idel
ines
(Dec
200
0).
Evid
ence
bas
e fo
r ef
fect
iven
ess
isgr
owin
g an
d Th
orax
gui
delin
esin
dica
te t
hat
they
may
pro
vide
an
effe
ctiv
e se
rvic
e (R
aw e
t al
. 199
8).
A m
eta-
anal
ysis
repo
rts
a sig
nific
ant
effe
ct (F
iore
et
al. 1
996)
.
See
abov
e.
Prov
ider
s of
(nat
iona
lan
d lo
cal)
help
lines
,w
orkp
lace
, pub
licpl
aces
, NH
S,co
mm
unity
gro
ups,
cess
atio
n se
rvic
es.
Inte
rven
tion
Evid
ence
Fior
e et
al.
1996
; Raw
et
al. 1
998;
upda
ted
guid
elin
es (D
ecem
ber
2000
).
Wh
o c
ou
ld b
ein
volv
ed?
PHC
tea
m, l
ink
with
othe
r su
ppor
tse
rvic
es if
appr
opria
te
[eg
heal
thy
livin
gce
ntre
s (H
LCs)
,ho
spita
l sta
ff,
doct
ors,
nur
ses,
mid
wiv
es].
Skill
s an
d r
eso
urc
es
Smok
ing
cess
atio
n sk
ills.
Smok
ing
cess
atio
n sk
ills.
Smok
ing
cess
atio
n sk
ills.
Smok
ing
cess
atio
n sk
ills.
Smok
ing
cess
atio
n sk
ills,
trai
ned
staf
f re
quire
d.
Poin
ts t
o c
on
sid
er
Reac
h lo
wer
tha
n th
at f
orbr
ief
advi
ce, b
ut a
ssoc
iate
dw
ith a
hig
her
succ
ess
rate
;re
sour
ce in
tens
ive;
eas
e of
acce
ss (e
g co
nven
ienc
e, s
afe
loca
tion,
tim
ing)
and
cos
t (if
any
) are
impo
rtan
tco
nsid
erat
ions
.
Mas
s re
ach,
eas
y an
dco
nven
ient
for
sm
oker
.G
uide
lines
are
ava
ilabl
e fo
rth
ose
wan
ting
to s
et u
p lo
cal
help
lines
. Alte
rnat
ivel
y,ac
tiviti
es a
nd li
tera
ture
cou
ldbe
und
erta
ken
to r
aise
pub
licaw
aren
ess
of a
nd u
se o
fex
istin
g he
lplin
es. C
an b
eus
ed t
o pr
omot
e ot
her
cess
atio
n su
ppor
t se
rvic
es in
loca
lity.
Furt
her
info
rmat
ion
As
abov
e.
As
abov
e. T
he M
auds
ley
smok
ers’
clin
ic is
an
exam
ple
of g
ood
prac
tice
high
light
edin
the
tob
acco
whi
te p
aper
(DH
199
8a).
Lich
tens
tein
et
al. (
1996
),N
HS
Dire
ct H
elpl
ine
0800
169
016
9,Q
uit
(Cha
rity)
02
0 73
88 5
775,
Qui
tline
080
0 00
2200
.
Ou
tco
me

Reducing smoking prevalence
19
Like
ly im
pact
unc
erta
in.
A U
S st
udy
of e
mpl
oyee
sre
port
ed a
red
uctio
n of
5%
in s
mok
ing
prev
alen
ce a
nd10
% in
con
sum
ptio
n af
ter
the
intr
oduc
tion
of w
orkp
lace
bans
. Oth
er b
enef
its in
clud
ere
cogn
ition
of
non-
smok
ing
as n
orm
, pro
tect
ion
of n
on-
smok
ers,
incr
ease
d pu
blic
awar
enes
s an
d ac
cept
ance
of
heal
th r
isks.
May
enc
oura
gead
oles
cent
s no
t to
sta
rt.
Qui
t ra
nge
0–5%
for
adu
ltin
terv
entio
ns (R
eid
1996
),di
rect
influ
ence
on
clim
ate
ofpu
blic
opi
nion
.
Redu
ce s
mok
ing
inpu
blic
and
wor
kpl
aces
Mas
s m
edia
cam
paig
ns
Ass
ocia
ted
with
red
uced
cons
umpt
ion,
pos
sible
red
uctio
ns in
prev
alen
ce in
the
long
er t
erm
(Bre
nner
and
Mie
lck
1992
; Buc
kan
d G
odfr
ey 1
994;
Rei
d 19
96).
Can
enh
ance
nat
ural
qui
t ra
te a
ndm
ay r
educ
e re
laps
e (R
eid
1996
;M
cVey
and
Sta
plet
on in
pre
ss);
may
also
red
uce
upta
ke o
f sm
okin
g in
youn
g pe
ople
(Sow
den
and
Arb
last
er 2
000a
).
Briti
sh H
ospi
talit
yA
ssoc
iatio
n, T
heRe
stau
rant
Ass
ocia
tion,
Brit
ishIn
stitu
te o
fIn
nkee
ping
, Bre
wer
san
d Li
cens
edRe
taile
rs A
ssoc
iatio
n,A
ssoc
iatio
n of
Lice
nsed
Mul
tiple
Reta
ilers
, em
ploy
ers
and
empl
oyee
s, N
HS.
Nat
iona
l and
loca
lm
edia
, com
mun
ityse
ttin
gs a
ndac
tiviti
es, w
orkp
lace
san
d pu
blic
pla
ces.
Inte
rven
tion
Oth
er t
reat
men
ts
Evid
ence
Insu
ffic
ient
evi
denc
e of
eff
ectiv
enes
sfo
r hy
pnot
hera
py a
nd a
cupu
nctu
re,
etc.
(Abb
ot e
t al
. 200
0; W
hite
et
al.
2000
).
Wh
o c
ou
ld b
ein
volv
ed?
Priv
ate
sect
or, l
inks
with
oth
er s
mok
ing
cess
atio
n pr
ovid
ers.
In v
iew
of
lack
of
evid
ence
bas
e,co
nsid
er c
onta
ctin
gre
cogn
ised
prof
essio
nal
asso
ciat
ions
for
trai
ned
indi
vidu
als.
Skill
s an
d r
eso
urc
es
Cos
tly; r
equi
res
min
imal
leve
lof
exp
osur
e an
d de
velo
pmen
tof
new
mes
sage
s to
avo
idco
nsum
er b
urn-
out.
Poin
ts t
o c
on
sid
er
Smok
ers
shou
ld b
e gi
ven
info
rmat
ion
abou
t ot
her
trea
tmen
ts t
o en
able
the
m t
om
ake
an in
form
ed c
hoic
ew
ithou
t di
scou
ragi
ngat
tem
pts
to s
top.
Lev
el o
ftr
aini
ng li
kely
to
vary
fro
mno
ne t
o su
ffic
ient
to
just
ifym
embe
rshi
p of
a p
rofe
ssio
nal
body
(Raw
et
al. 1
998)
.
Cha
rter
agr
eed
betw
een
gove
rnm
ent
and
licen
sed
hosp
italit
y tr
ade.
The
HSE
ispr
oduc
ing
a ne
w A
CoP
on
smok
ing
in t
he w
orkp
lace
,w
hich
will
pro
vide
pra
ctic
alad
vice
on
how
to
com
ply
with
the
law
.
Hig
h re
ach;
wor
ks w
ell w
ithot
her
inte
rven
tions
suc
h as
tax
incr
ease
s; c
an s
uppo
rtlo
cal c
essa
tion
serv
ices
; foc
ussh
ould
be
on a
dults
.
Furt
her
info
rmat
ion
Briti
sh H
ypno
ther
apy
Ass
ocia
tion
(BH
A),
1W
ythb
urn
Plac
e, L
ondo
nW
1H 5
WL
Tel:
0207
723
4443
, em
ail:
fireb
ird@
agon
et.c
o.uk
Briti
sh S
ocie
ty o
fH
ypno
ther
apist
s (B
SH),
37O
rbai
n Ro
ad, L
ondo
n SW
67J
Z Te
l: 02
0 73
85 1
166
Ass
ocia
tion
of G
ener
alPr
actit
ione
rs o
f N
atur
alM
edic
ine
(AG
PNM
), 38
Nig
elH
ouse
, Por
tpoo
l Lan
e,Lo
ndon
EC
1N 7
UR
Te
l: 02
0 74
05 2
781.
Inst
itute
of
Com
plem
enta
ryM
edic
ine
(ICM
), PO
Box
194
,Lo
ndon
SE1
6 1Q
Z Te
l: 02
0 72
37 5
165.
DH
(199
8a),
HEA
(199
9c,d
).Th
e N
atio
nal H
SE (N
HSE
) is
deve
lopi
ng a
too
lkit
to h
elp
with
the
impl
emen
tatio
n of
its p
olic
ies.
DH
sm
okin
g po
licy
team
,D
H c
omm
unic
atio
ns t
eam
,re
view
of
use
of m
ass
med
iaca
mpa
igns
in E
ngla
ndav
aila
ble
from
HD
A (G
rey
etal
. 200
0). C
ochr
ane
Libr
ary
web
site
htt
p://w
ww
.upd
ate-
soft
war
e.co
m/c
libho
me/
clib
Ou
tco
me

Coronary heart disease: guidance for implementing the preventive aspects of the NSF
20
One
yea
r ne
t qu
it ra
tes
estim
ated
0.3
–0.5
% (R
eid
etal
., 19
92; B
uck
and
God
frey
1994
); in
fluen
ce o
n pu
blic
opin
ion;
pro
vide
s ba
sis f
orot
her
initi
ativ
es; m
ayco
ntrib
ute
to im
pact
of
mas
sm
edia
cam
paig
n;
exte
nds
deba
te a
bout
smok
ing.
Impa
ct o
f m
onito
ring
loca
lin
frin
gem
ent
of v
olun
tary
agre
emen
t no
t kn
own,
but
does
off
er o
ppor
tuni
ties
for
med
ia a
dvoc
acy.
Loca
l act
ivity
can
red
uce
sale
s; u
sefu
l for
med
iaad
voca
cy; m
ay h
ave
a sm
all
dela
ying
eff
ect
on c
hild
ren’
sup
take
.
Impl
emen
tatio
n va
ries
so t
hat
outc
ome
is un
clea
r; re
info
rces
non-
smok
ing
as t
he n
orm
;ot
her
pote
ntia
l ben
efits
incl
ude
redu
ced
abse
ntee
ism,
redu
ced
cost
s an
d el
imin
atio
nof
pas
sive
smok
ing.
Adv
erti
sing
ban
Redu
ce il
lega
l sal
es
Smok
ing
polic
ies
insc
hool
s
Poss
ible
eff
ect
on a
dult
cons
umpt
ion
and
teen
age
prev
alen
ce (R
eid
et a
l. 19
92;
Sow
den
and
Arb
last
er, 2
000a
).
Loca
l act
ivity
can
red
uce
sale
s. T
his
may
hav
e a
smal
l del
ayin
g ef
fect
on
child
ren’
s up
take
of
smok
ing.
Impa
ct o
n up
take
of
smok
ing
unce
rtai
n.
Gov
ernm
ent,
heal
thpr
omot
ion
spec
ialis
ts,
toba
cco
advo
cate
san
d ot
hers
can
mon
itor
exist
ing
volu
ntar
yag
reem
ents
.
Mag
istra
tes,
ret
aile
rs,
loca
l tra
ding
stan
dard
s of
ficer
s,sc
hool
s, p
aren
ts,
loca
l gov
ernm
ent
asso
ciat
ion,
LA
s,N
atio
nal A
ssoc
iatio
nof
Cig
aret
te M
achi
neO
pera
tors
.
Scho
ol t
each
ers,
gove
rnor
s, h
eads
,pa
rent
s, p
upils
, loc
alco
mm
unity
(for
polic
ies
that
invo
lve
non-
smok
ing
insc
hool
pre
mise
s fo
rco
mm
unity
act
iviti
es).
Inte
rven
tion
Med
ia a
dvoc
acy
and
No
Smok
ing
Day
Evid
ence
Effe
ctiv
enes
s lo
wer
tha
n m
ore
inte
nsiv
e in
terv
entio
ns b
ut h
ighl
yco
st-e
ffec
tive
beca
use
the
reac
h is
muc
h gr
eate
r (R
eid
et a
l., 1
992;
Buck
and
God
frey
199
4).
Wh
o c
ou
ld b
ein
volv
ed?
NH
S, lo
cal
gove
rnm
ent,
com
mer
cial
inte
rest
s,vo
lunt
ary
agen
cies
.
Skill
s an
d r
eso
urc
es
Che
aper
tha
n pa
idad
vert
ising
but
sub
stan
tial
reso
urce
s re
quire
d fo
rge
nera
ting
stor
ies;
good
con
tact
s w
ith lo
cal
med
ia a
nd t
he le
isure
and
hosp
italit
y tr
ade.
Tra
inin
g in
med
ia a
dvoc
acy
need
ed.
Requ
ires
subs
tant
ial
reso
urce
s.
Poin
ts t
o c
on
sid
er
Relie
s on
goo
d lin
ks w
ithot
her
agen
cies
(eg
volu
ntar
yse
ctor
, loc
al g
over
nmen
t,ho
spita
lity
trad
e) t
o cr
eate
loca
l act
iviti
es.
Loca
l act
ivity
cou
ld in
clud
em
onito
ring
infr
inge
men
ts t
ovo
lunt
ary
agre
emen
ts (e
gad
vert
ising
on
billb
oard
s ne
arsc
hool
s, p
rom
otio
ns in
mag
azin
es a
imed
at
youn
gpe
ople
).
Exist
ing
law
sta
tes
that
it is
illeg
al t
o se
ll to
bacc
opr
oduc
ts t
o un
der
16s,
but
enfo
rcem
ent
is pr
oble
mat
ic.
Poss
ibly
add
s to
per
cept
ion
that
sm
okin
g is
a fo
rbid
den
frui
t (K
ay S
cott
Ass
ocia
tes
2000
).
Supp
orts
hea
lth m
essa
ges
inth
e na
tiona
l cur
ricul
um.
Furt
her
info
rmat
ion
http
://w
ww
.no-
smok
ing-
day.
org.
uk/c
ampa
ign.
htm
Ex
ampl
e of
goo
d pr
actic
e:Ro
y C
astle
Goo
d A
ir A
war
ds
DH
(199
2). I
ssue
d w
ith D
Hci
rcul
ar E
L (9
2) 7
1.
Nat
iona
l Ass
ocia
tion
ofC
igar
ette
Mac
hine
Ope
rato
rsha
s pr
oduc
ed a
cod
e fo
rm
embe
rs. L
ocal
Gov
ernm
ent
Ass
ocia
tion
(LG
A) a
nd L
ocal
Aut
horit
ies
Coo
rdin
atin
gBo
dy o
n Fo
od a
nd T
radi
ngha
ve p
rodu
ced
an L
Aen
forc
emen
t pr
otoc
ol.
HEA
(199
3, 1
999e
).
Ou
tco
me

1.7 References
Abbot, N.C., Stead, L.F., White, A.R., Barnes, J. and Ernst, E., 2000.
Hypnotherapy for smoking cessation, Cochrane Review. In: Cochrane
Library, Issue 3. Oxford: Update Software.
Acheson, D., 1998. Independent inquiry into inequalities in health
report. London: The Stationery Office.
Adams, C., Bauld, L. and Judge, K., 2000. Baccy to front. Health Service
Journal, 110 (5713), 28–31.
ASH, 2000a. Smoking cessation in primary care: how to spend NHS money
much more effectively. London: ASH. (http://www.ash.org.uk/?cessation)
ASH, 2000b. Smoking cessation services: Implementing the NHS
National Plan. London: ASH.
ASH Scotland and HEBS, 1999. Women, low income and smoking:
breaking down the barriers. Edinburgh: Action on Smoking and Health
Scotland and Health Education Board for Scotland.
Borland, R., Owen, N., Hill, D. and Schofield, P., et al., 1991. Predicting
attempts and sustained cessation of smoking after the introduction of
workplace smoking bans. Health Psychology, 10 (5), 336–342.
Botvin, G.J., Dusenbury, L., Baker, E., Ortiz, S., Botvin, E.M. and Kerner, J.,
1992. Smoking prevention among urban minority youth: assessing effects
on outcome and mediating variables. Health Psychology, 11 (5), 290–299.
Brauer, M. and Mannetje, A., 1998. Restaurant smoking restrictions and
environmental tobacco smoke exposure. American Journal of Public
Health, 88 (12), 1834–1836.
Brenner, H. and Mielck, A., 1992. Restrictions to smoking at the
workplace and smoking habits: a literature review. Soz Praventivmed,
37 (4), 162–167.
Buck, D. and Godfrey, C., 1994. Helping smokers give up: guidance for
purchasers on cost effectiveness. London: HEA.
Callum, C., 1998. The UK smoking epidemic: deaths in 1995. London:
HEA.
Campion, P., Owen, L., McNeill, A. and McGuire, C., 1994. Evaluation
of a mass media campaign on smoking and pregnancy. Addiction, 89
(10), 1245–1254.
Chapman, S., 1993. Unravelling gossamer with boxing gloves: problems
in explaining the decline in smoking. British Medical Journal, 307, 429–432.
DFEE, 1998. Protecting young people: good practice in drug education
in schools and the youth service. Sudbury, Suffolk: DfEE Publications.
DH, 1992. Effect of tobacco advertising on tobacco consumption: a
discussion document reviewing the evidence (C. Smee, Chair,
Department of Health Economics and Operational Research Division).
London: DH [issued with DH EL(92)71].
DH, 1998a. Smoking kills, white paper on tobacco. London: The
Stationery Office.
DH, 1998b. Directory of African Caribbean initiatives. Birmingham: N Films Ltd.
DH, 2000a. The cancer plan. London: The Stationery Office.
DH, 2000b. National service framework for coronary heart disease.
London: DH.
DH, 2000c. Statistics on smoking: England, 1978 onwards. London: DH
Statistical Bulletin.
DH, 2000d. The NHS plan. A plan for investment. A plan for reform.
London: The Stationery Office. http://www.nhs.uk/nhsplan
Dorsett, R. and Marsh, A., 1998. The health trap: poverty, smoking and
lone parenthood. London: Policy Studies Institute.
Elder, J P., Wildey, M., de Moor, C., Sallis, J.F., Jr., Eckhardt, L.,
Edwards, C., Erickson, A., Golbeck, A., Hovell, M., Johnston, D.,
Levitz, M.D., Molgard, C., Young, R., Vito, D. and Woodruff, S.I., 1993.
The long-term prevention of tobacco use among junior high school
students: classroom and telephone interventions. American Journal of
Public Health, 83 (9), 1239–1244.
Elder, J.P., Edwards, C.C., Conway, T.L., Kenney, E., Johnson, C.A. and
Bennett, E.D., 1996. Independent evaluation of the California Tobacco
Education Program. Public Health Report, 111 (4), 353–358.
Fiore, M.C., Bailey, W.C., Cohen, S.J., Dorfman, S.F., Goldstein, M.G., Gritz,
E.R., Heyman, R.B., Holbrook, J., Jaen, C.R., Kottke, T.E., Lando, H.A.,
Mecklenburg, R., Mullen, P.D., Nett, L.M., Robinson, L., Stitzer, M.L.,
Tommasello, A.C., Villejo, L. and Wewers, M.E., 1996. Smoking cessation,
Clinical Practice Guideline No. 18. Rockville: Agency for Health Care
Policy and Research, US Department of Health and Human Services,
Publication No. 96-0692.
Glasgow, R.E., Cummings, K.M. and Hyland, A., 1997. Relationship of
worksite smoking policy to changes in employee tobacco use: findings
from COMMIT. Community Intervention Trial for Smoking Cessation.
Tobacco Control, 6 (suppl 2), S44–S48.
Reducing smoking prevalence
21

Grey, A., Owen, L. and Bolling, K., 2000. A breath of fresh air: tackling
smoking through the media. London: HDA.
HDA, 2000a. Smoking cessation in young people: should we do more
to help young people quit? London: HDA.
HDA, 2000b. Tobacco control policies within the NHS: case studies of
effective practice. London: HDA.
HDA, in press. An investigation into the potential of media advocacy as
a health promotion strategy. London: HDA.
HEA, 1993. Smoking policies in schools: guidelines for policy
development. London: HEA.
HEA, 1994a. Smoking and pregnancy: guidance for purchasers and
providers. London: HEA.
HEA, 1994b. Helping pregnant smokers quit: training for health
professionals. London: HEA.
HEA, 1996a. Smoking and pregnancy: a growing problem.
London: HEA.
HEA, 1996b. Empowering smokers to quit: success principles for
community stop-smoking projects. London: HEA.
HEA, 1999a. Black and minority ethnic groups in England: health and
lifestyles. London: HEA.
HEA, 1999b. Been there, done that: revisiting tobacco control policies in
the NHS. London: HEA.
HEA, 1999c. Smoking policy for the workplace: an update. London:
HEA.
HEA, 1999d. Towards tobacco-free environments: guidelines for local
authorities. London: HEA.
HEA, 1999e. Smoke-free schools: seven steps to success.
London: HEA.
HSC, 1998. Tobacco white paper, HSC 1998/234. London: NHS
Executive.
HSC, 1999. New NHS smoking cessation services, HSC 1999/087.
London: NHS Executive.
Hill, D., 1999. Why we should tackle adult smoking first. Tobacco
Control, 8, 333–335.
Hurt, R.D, Sachs, D.P.L., Glover, E.D., Offord, M.S., Johnston, J.A.,
Lowell, P.D., Khayrallah, M.A., Schroeder, D.R., Glover, P.N.,
Sullivan, C.R., Croghan, I.T. and Sullivan, P.M., 1997. A comparison of
sustained-release Buproprion and placebo for smoking cessation. New
England Journal of Medicine, 337, 1195–1002.
Jarvis, M., 1998. Extra analyses of the General Household Survey
commissioned by the Health Education Authority. London: HEA.
Jarvis, M. and Wardle, J., 1999. Social patterning of health behaviours:
the case of cigarette smoking. In: M. Marmott and R. Wilkinson, eds.
Social determinants of health. Oxford: Oxford University Press, 1999,
240–255.
Jeffery, R.W., Kelder, S.H., Forster, J.L., French, S.A., Lando, H.A.,
Baxter J.E., 1994. Restrictive smoking policies in the workplace: effects
on smoking prevalence and cigarette consumption. Preventive Medicine,
23 (1), 78–82.
Jenkins, C.N., McPhee S.J., Le, A., Pham, G.Q., Ha, N.T., Steward, S.,
1997. The effectiveness of a media-led intervention to reduce smoking
among Vietnamese-American men. American Journal of Public Health,
87 (6), 1031–1034.
Jernigan, D. and Wright, P., eds., 1993. Making news: changing policy.
Case studies of media advocacy on alcohol and tobacco use. Bethesda,
MD: Center for Substance Abuse Prevention.
Jorenby, D.E., Leischow, S.J., Nides, M.A., Rennard, S.I., Johnston, J.A.,
Hughes, A.R., Smith, S.S., Muramoto, M.L., Daughton, D.M., Doan, K.,
Fiore, M.C. and Baker, T.B., 1999. A controlled trial of sustained-release
buproprion, a nicotine patch, or both for smoking cessation. New
England Journal of Medicine, 340, 685–691.
Kay Scott Associates, 2000. Need a fag, need a fag. Smoking and
young people, Report on six qualitative discussion groups. London: ASH.
Lantz, P.M., Jacobson, P.D., Warner, K.E., Wasserman, J., Pollack, H.A.
and Ahlstrom, A., 2000. Investing in youth tobacco control: a review
of smoking prevention and control strategies. Tobacco Control, 9,
47–63.
Lichtenstein, E., Glasgow, R.E., Lando, H.A., Ossip-Klein, D.J. and Boles,
S.M., 1996. Telephone counselling for smoking cessation: rationales and
meta-analytic review of evidence. Health Education Research, 11,
243–257.
Lillington, L., Royce, J., Novak, D., Ruvalcaba, M. and Chlebowski, R.,
1995. Evaluation of a smoking cessation program for pregnant minority
women. Cancer Practice, 3 (3), 157–163.
Coronary heart disease: guidance for implementing the preventive aspects of the NSF
22

Macaskill, P., Pierce, J.P., Simpson, J.M. and Lyle, D.M., 1992.
Mass media-led antismoking campaign can remove the education
gap in quitting behaviour. American Journal of Public Health, 82 (1),
96–98.
Maltby, S., Simmons, R., Choudry, S., Warrant, M. and Haggett, C.,
2000. Research on tobacco use among black and minority ethnic
groups. London: HDA.
Marcus, B.H., Emmons, K.M. and Abrams D.B., 1992. Restrictive
workplace smoking policies: impact on non-smokers’ tobacco exposure.
Journal of Public Health Policy, 13 (1), 42–51.
Marsh, A. and McKay, S., 1994. Poor smokers. London: Policy Studies
Institute.
Naidoo, B., Stevens, W. and McPherson, K., 1999. A report for the
Health Education Authority on modelling the short-term consequences
of smoking cessation in England on the hospitalisation rates for acute
myocardial infarction and stroke. London: London School of Hygiene
and Tropical Medicine.
OFSTED, 1997. Drug education in schools. London: The Stationery
Office.
Owen, L., 2000. Impact of a telephone helpline for smokers who called
during a mass media campaign. Tobacco Control, 9, 148–154.
Owen, L. and Penn, G., 1999. Smoking and pregnancy: a survey of
knowledge, attitudes and behaviour 1992–1999. London: HEA.
Owen, L., McNeill, A. and Callum, C., 1998. Trends in smoking during
pregnancy in England, 1992–7: quota sampling surveys. British Medical
Journal, 317, 728.
Owen, L. and Bolling, K., 1996. Smoking and pregnancy: developing a
communications strategy for cessation. London: HEA.
Raw, M., McNeill, A., and West, R., 1998. Smoking cessation guidelines
for health professionals. Thorax, 53 (suppl 5).
Reid, D., 1996. Tobacco control: overview. British Medical Bulletin, 52
(1), 108–120.
Reid, D., Killoran, A., McNeill, A. and Chambers, J., 1992. Choosing the
most effective health promotion options for reducing a nation’s
smoking prevalence. Tobacco Control, 1, 185–197.
Royal College of Physicians, 1992. Smoking and the young. London:
Royal College of Physicians.
SCOTH, 1998. Report of the Scientific Committee on Tobacco and Health.
London: The Stationery Office.
Secker-Walker, R.H., Solomon, L.J., Flynn, B.S., Skelly, J.M., 1995.
Smoking relapse prevention counselling during prenatal and early
postnatal care. American Journal of Preventive Medicine, 11, 86–93.
Sowden, A.J. and Arblaster, L., 2000a. Mass media interventions for
preventing smoking in young people, Cochrane Review. In: Cochrane
Library, Issue 2. Oxford: Update Software.
Sowden, A. and Arblaster, L., 2000b. Community interventions for
preventing smoking in young people, Cochrane Review. In: Cochrane
Library, Issue 2. Oxford: Update Software.
Stead, L. and Lancaster, T., 2000. A systematic review of interventions
for preventing tobacco sales to minors. Tobacco Control, 9, 169–176.
Tang, J.L., Cook, D.G. and Shaper, A.G., 1992. Giving up smoking: how
rapidly does the excess risk of ischaemic heart disease disappear?
Journal of Smoking-Related Diseases, 3, 203–215.
US Department of Health and Human Services, 1990. The health
benefits of smoking cessation, a report of the Surgeon General, DHHS
Publication No. CDC 90-8416. Rockville, MD: National Centers for
Disease Control and Prevention, Office on Smoking and Health.
US Department of Health and Human Services, 2000. Reducing tobacco
use, a report of the Surgeon General, DHHS Publication No. CDC20402,
S/N017-001-00544-4. Rockville, MD: National Centers for Disease
Control and Prevention, Office on Smoking and Health.
Wakefield, M. and Chaloupka, F., 2000. Effectiveness of comprehensive
tobacco control programmes in reducing teenage smoking in the USA.
Tobacco Control, 9, 177–186.
Wakefield, M.A., Wilson, D., Owen, N., Esterman, A. and Roberts, L.,
1992. Workplace smoking restrictions, occupational status, and reduced
cigarette consumption. Journal of Occupational Medicine, 34 (7),
693–697.
White, A.R., Rampes, H. and Ernst E., 2000. Acupuncture for smoking
cessation, Cochrane Review. In: Cochrane Library, Issue 3. Oxford:
Update Software.
WHO, 1979. Controlling the smoking epidemic, WHO Technical Report
Series No. 636. Geneva: WHO.
WHO, 1998. Guidelines for controlling and monitoring the tobacco
epidemic. Geneva: WHO.
Reducing smoking prevalence
23

Box 2.1 Identification of barriers to healthy eating and interventions to address them: an example
Chapter 2Improving diet and nutrition
Improving diet and nutrition
252.1 Introduction
Diet plays a fundamental role in the development ofCHD. The type and amount of fat and its relationship toblood cholesterol levels have been recognised for sometime as being particularly influential. Salt intake has beenimplicated in relation to blood pressure and, more recently,an increased intake of fruit and vegetables has beenidentified as an important factor in reducing the rates of both heart disease and some cancers (DH 1994,1998). The promotion of healthy eating is important inreducing the risk not only of CHD but also of otherchronic conditions, such as obesity and diet related cancers.
Effective strategies to promote healthy eating are generallythose that work at several levels. It is important to identifythe barriers to dietary change in the local population andthen select interventions to address them (see Box 2.1).
2.2 Objectives of nutritional interventions
Diet is one of the key modifiable risk factors in theprevention of CHD. The government’s Committee on the Medical Aspects of Food and Nutrition Policy(COMA; DH 1994) recommended a reduction in fat(particularly saturated fat), a reduction in salt and anincrease in complex carbohydrates. In addition, fruit and vegetable consumption should be increased by atleast 50% (to at least five portions per day). Therecommendations are summarised in nutrition briefing papers produced by the HEA (1992, 1996). Also, it has been estimated that around one-third of all cancers might be influenced by diet. In 1998,COMA reviewed the evidence on diet and cancer in theUK (DH 1998). The working group recommendationswere consistent with other dietary recommendationsmade for the prevention of obesity, diabetes andcardiovascular disease.
Barrier
• Belief that the family is already eating enough fruitand vegetables
• Dislike of taste of vegetables and lack of confidencein cooking and preparing them; fear of waste andof rejection by the family
• Difficulty in finding affordable, good quality fruitand vegetables locally
Intervention
• Information about five portions a day and portionsizes
• Set up cooking skills clubs and tasting sessions, ordevelop cooking sessions as part of the activities ofexisting groups (eg women’s groups, youth groups)
• Set up community owned retailing and food cooperatives to introduce affordable supplies

26
In promoting a healthy balanced diet to reduce the risk ofcardiovascular disease and diet related cancers in thepopulation, interventions should focus on the following:
• Reducing the amount of fat, and in particular, theamount of saturated fatIt has been estimated that a 10% reduction insaturated fat intake within the UK population wouldbe associated with a reduction in CHD mortality ofbetween 20% and 30% (Marmot 1994). Therefore, tohelp achieve a healthy diet, people should beencouraged to use reduced fat spreads and dairyproducts in place of full fat versions, to replace oils andfats high in saturates with those high inmonounsaturates, to reduce the amount of fat used incooking, to trim fat from meat and to reduce theamount of products such as biscuits, pastries, cakes,and crisps in the diet.
• Increasing the amount of fruit and vegetableseaten to at least five portions each dayApart from being rich sources of carbohydrate, dietaryfibre, antioxidants and other bioactive factors, fruit andvegetables are also rich sources of potassium, which isassociated with lower blood pressure and a lower riskof stroke (Joshipura et al. 1999). For many people, thiswill mean almost doubling their intake. It will meanhaving fruit and vegetables at most meals, and assnacks between meals. Access to affordable, goodquality supplies of fruit and vegetables must beensured and skills and confidence to prepare and cookfruit and vegetables should be developed [NationalHeart Forum (NHF) 1997].
• Increasing the intake of fibre rich, starchy foods,such as bread, potatoes, pasta and rice, by half asmuch againMake these foods the main part of most meals, andreplace fattier snacks.
• Reducing the average salt intake by around athirdThere is now a consensus that dietary sodium is afactor in the development of high blood pressure (DH 1994). People should be encouraged to graduallyreduce the salt they add to food, both in cooking andat the table. Also, people should be more aware oflow-salt alternatives to processed foods if available andshould recognise the salt content of processed foodsby reading food labels.
• Increasing the amount of fish eaten to at leasttwo portions each week, one of which should bean oily fish Encourage people to eat fish more often: this maymean working with communities to develop theircooking skills and confidence to cook fish.
A useful tool to support health promoters in promoting abalanced diet is The balance of good health [HEA, DH andMinistry of Agriculture, Fisheries and Foods (MAFF) 1994].It shows what proportion of the diet should come fromthe different food groups and could provide a consistentand easily understood message about a balanced diet1.
The balance of good health has also been modified foruse with black and minority ethnic groups. The BritishDietetic Association and Sainsburys have developed anAfrican-Caribbean version and the British NutritionFoundation has produced a model suitable for use withthe Chinese community. Dietitians at WandsworthCommunity Health Trust, with support from SpillersMilling, formed a healthy alliance and produced a versionsuitable for use with South Asian groups.
2.2.1 Professional knowledge and expertise
Identifying the barriers and developing an integratedprogramme of complementary activities will require theinput of staff with a range of skills. While most areashave access to a community dietitian, it is quite commonfor clinical duties to interfere with the dietitian’s ability tospend time in the community. In planning the resourcesneeded to implement the strategy, it may be worthconsidering ring fencing a block of dietitian time todevote to community work. Public health nutritionists canprovide the expertise to develop and implement a publichealth nutrition strategy and to work on other nutritionissues at a population level. In recent years, the NutritionSociety has introduced a registration system for publichealth nutritionists (RPH Nutr). In addition, the NutritionSociety has recently developed an associate registration
Coronary heart disease: guidance for implementing the preventive aspects of the NSF
1The balance of good health does not apply to children under two years
of age, who need a diet that is higher in fat and lower in fibre rich,
starchy foods, to children aged between two and five years (a gradual
transition towards a diet consistent with The balance of good health is
needed here) or to people with special dietary requirements or those
under medical supervision.

• Clear goals were set, based on theories of behaviouralchange, rather than relying on the provision ofinformation alone
• There was personal contact with individuals or smallgroups sustained over time
• Participants received personalised feedback on anychanges in their behaviour and risk factors
• Changes in the local environment were promoted, forexample in shops and catering outlets to help peoplechoose a healthy diet.
Providing information alone is not a solution. Improvingpeople’s knowledge about diet does not necessarily lead to behaviour change. Improvements in knowledge should be accompanied by the development of skills and provide the opportunity to put the knowledge intopractice. For example, there is little point in encouraging people to eat more fish, in particular oilyfish, if access to these foods is not available, and ifpeople lack the skills and confidence to prepare and cook fish. Integrated programmes of activity could bemore effective if they first identify the barriers to dietary change, and then provide the information, skillsand opportunities to put the suggestion into practice(NHF 1999).
2.4 Components of a local strategy
2.4.1 Schools
A meta-analysis of 12 intervention studies to promoteheart-healthy eating behaviour in schools concluded thatthey can have a significant effect (McArthur 1998).
Two reviews have identified the following features of aneffective school intervention (Contento 1995; Roe et al.1997):
• Nutrition education interventions are more likely to beeffective when they employ educational strategies thatare directly relevant to a particular behaviour (eg dietor physical activity) and are derived from appropriatetheory and research
• Interventions need adequate time and intensity to be effective
Improving diet and nutrition
27
scheme for newly qualified public health nutritionprofessionals who have not yet accumulated the three years’ experience required for full registration as a public health nutritionist. The Register of Public Health Nutritionists can be found onhttp://www.nutsoc.org.uk/RPHNutr.html or contact JackieLandman at the Nutrition Society (020 7602 0228) forfurther information on the associate scheme.
Local people are an important addition to this skill base.Research suggests that the efficiency and effectiveness ofcommunity based interventions can be improved by usinglocal people to complement the work of healthprofessionals. McGlone et al. (1999) suggested that ‘iflocal food projects are to work, then they must genuinelyinvolve local people’. Services provided by local peopleare often considered more appropriate and moreaccessible for the health needs of the community. Suchservices foster self-reliance, community participation andcan help overcome barriers. They also allow access togroups that are typically hard to reach and can beparticularly beneficial for black and minority ethnicgroups. These benefits are two way, as local people havethe opportunity to develop their own skills. Exploratorywork with this peer education approach (Hodgson et al.1995; Kennedy et al. 1999) showed that it was possibleto achieve both significant increases in nutritionknowledge and potentially beneficial changes in thedietary practices of low income families. The bestapproach appears to be one in which guided ‘hands on’food preparation/cooking sessions allow the participantsto acquire knowledge and skills. However, it was notedthat this approach was resource intensive, particularly inprofessional staff time, and there is little evidence ofeffectiveness in terms of dietary change. This approachmay result in potential health, social and economicbenefits and therefore warrants further study.
2.3 Features of effective interventions
A meta-analysis of randomised controlled trials shows that dietary interventions can be effective in reducingCHD risk factors (Brunner et al. 1997). A systematic reviewof the effectiveness of interventions to promote healthyeating found that characteristics of a successfulintervention had the following features (Roe et al. 1997):
• It focused on diet alone, or diet plus physical activityrather than tackled a range of risk factors

• Family involvement enhances the effectiveness of programmes for younger children
• Incorporation of a self-evaluation or self-assessmentand feedback is effective in interventions for older children
• Effective nutrition education includes consideration ofthe whole school environment and community
• Interventions in the larger community can enhanceschool nutrition education
• The most effective interventions focus on diet alone ordiet and physical activity.
2.4.2 Local/community projects
This section includes a range of interventions from small-scale local projects to well funded communityinterventions. Little rigorous evaluation of theeffectiveness of the small scale projects has been carried out.
Roe et al. (1997) concluded that intensive, smaller scaleprojects generally resulted in positive changes in diet andblood cholesterol, at least in the short term. However,many large community-wide studies failed to show asimilar effect because they were conducted in the 1980s,a time when awareness of CHD risk factors had increasedin the population. Therefore, in one study, the reductionin blood cholesterol observed in the interventioncommunities was also found in the comparisoncommunity. In addition, there was a diversity of otherinformational and educational interventions; therefore,the investigators were unable to attribute any change totheir specific intervention.
Effective community interventions appear to:
• Focus on diet or diet plus physical activity
• Use a theoretical model
• Use diverse multiple interventions at individual, group,community and environmental level
• Include small-group interventions (Contento 1995; Roeet al. 1997).
McGlone et al. (1999) identified the characteristics ofprojects that appear to have been ‘successful’ using arange of criteria:
• Flexibility needed by agencies to respond to the needsof particular communities
• Access to secure, and ongoing, funds
• Professionals work in partnership with a community
• Projects need to involve local people, and ensure equalrespect
• Evaluation should not be confined to narrow clinical andbehavioural measures. Include food purchasing patterns,structural changes and social outcomes, for example
• Strike a balance between partnerships and localownership
• Local and national networks should enable sharing ofexperiences
• Training for professionals and members of thecommunity to acquire skills for a new way of working
• Government policies that do not deter volunteers (egsocial welfare benefits)
• Provide incentives for local projects and smallbusinesses, such as tax relief
• Allow time for community projects to develop, on thebasis that there is no ‘quick fix’ and that local policyshould support realistic time frames for communityfood projects.
However, to date, there has been no systematicevaluation of the effectiveness of local projects.
2.4.3 Workplace
Three out of four good-quality interventions showedpositive effects of nutrition workplace interventions, withdecreases in blood cholesterol of between 2.5% and10% (Roe et al. 1997). An HEA review of theeffectiveness of health promotion interventions in theworkplace (Peersman et al. 1998) identified four studies
Coronary heart disease: guidance for implementing the preventive aspects of the NSF
28

Another systematic review (Roe et al. 1997) includedinterventions in the primary healthcare setting. Four‘good quality’ studies were identified in the past 10 years. Modest and sustained effects on both blood cholesterol and dietary fat intake were achieved fordietary interventions only, or for multifactorialinterventions.
Characteristics of an effective healthcare interventioninclude:
• Small group or one to one counselling sessions
• Targeting higher risk groups, which is also more cost-effective (Van der Weidjen 1998; Wood et al. 1998)
• Family counselling and education for those at increasedrisk
• Tailoring to the personal characteristics of individuals
• Educational and behavioural frameworks which areclient centred
• Staff training and development (topic basedknowledge and counselling skills)
• Low intensity interventions, such as mailed, computergenerated, personalised, nutrition education materialfor well-motivated groups (Roe et al. 1997).
2.5 Reducing inequity
There are inequalities in diet between those on higher and lower incomes (Acheson 1998). The most striking difference is that people in lower socio-economic groups tend to eat less fruit andvegetables. The 1997 National Food Survey (MAFF 1998) found that consumption of fruit andvegetables by those in the upper socio-economic groups was a third higher than that of those in lowergroups. This social class difference has also been reported in children (Gregory et al. 2000). Studies have shown that people on a low income can describe a healthy diet as well as those on higher incomes (Lobstein 1997). Food poverty, affordability and access to a healthy and varied diet have beenidentified as possible barriers (Lobstein 1997; DH 1996).
Improving diet and nutrition
29
on healthy eating with adequate methodologies. Threeshowed positive effects on fat, fruit and vegetable intake,intention to change the diet and self-efficacy.
Characteristics of an effective workplace interventioninclude:
• Visible and enthusiastic support and involvement frommanagement
• Involvement by employees at all levels in the planningand implementation phases
• A focus on definable and modifiable risk factors ratherthan multiple risk factor interventions
• Screening and/or individual counselling
• Changes to the composition of best selling foodsprovided in canteens and vending machines
• Tailoring to the characteristics and needs of theemployees
• Use of local resources in organisation andimplementation of the intervention
• Combine population based policy initiatives withintensive individual and group oriented interventions
• Built-in sustainability.
2.4.4 Healthcare
In a meta-analysis by Brunner et al. (1997), the studyparticipants were well motivated. Most studies wereconducted in either a healthcare or an institutionalsetting. Interventions included dietary advice to reduce fat or sodium and to increase fibre. The authorsestimated that, if changes in dietary behaviour weresustained, they could lead to a reduction in the incidenceof CHD by 14% and the incidence of stroke by 9%.
A meta-analysis by Yu-Poth (1999) reported a 10%reduction in plasma total cholesterol with a low intensityintervention, and a 13% reduction with the high intensityintervention. Tang et al. (1998) reported reductions in bloodcholesterol following individual dietary advice to modify fatintake: 8.5% at three months and 5.5% at 12 months.

raised by the recent National Diet and Nutrition Surveys,of children aged 11⁄2 to 41⁄2 years (Gregory et al. 1995)and 4 to 18 years (Gregory et al. 2000). Acheson (1998)concluded that ‘pre-school education or day care may beespecially effective in improving the achievement andhealth of the most disadvantaged children’. A recentreview by Tedstone et al. (1998) of the effectiveness ofinterventions to promote healthy eating in pre-schoolchildren aged 1–5 years found that pre-school and daycare centres were likely to be appropriate settings forinterventions, and that parental involvement mayenhance the effectiveness of interventions and should be facilitated. In more detail, the review reported that:
• Traditional, video or computer-based teaching methods were successful at increasing nutritionknowledge and the effectiveness was enhanced by theinclusion of parents
• Behavioural modification techniques using repeatedexposure to initially novel foods were successful inincreasing willingness to consume the foods only iftasting was facilitated as part of the exposure
• The use of reward to encourage consumption of foodswas not successful once the reward had been removed
• One to one diet counselling that was ‘needs focused’was successful at bringing about improvements in UKmothers.
Acknowledgement
Information in Table 2.6 concerning some of the local community interventions was drawn in part fromMaking Links – a toolkit for local food projects (Sustain2000).
30
The Acheson report (Acheson 1998) recommendedfurther development of policies that will ensure adequateretail provision of food to those who are disadvantaged.A report by Policy Action Team (PAT) 13 (1999)confirmed that accessing affordable, good quality fruitand vegetables within some local areas might be difficult.However, access should not be seen purely in terms ofphysical proximity, and other kinds of access need to beconsidered, for example, financial access, knowledge andinformation (HEA 1998a). In areas where a large proportionof the population is unemployed, on low income or inreceipt of benefits, interventions to improve people’saccess to a healthier diet are likely to be a key priority.
2.5.1 Black and minority ethnic groups
Improving the health of minority ethnic groups is also apriority in the government’s drive to reduce socialexclusion and inequalities in health. Further impetus wasprovided by Acheson (1998), who recommended that theneeds of black and minority ethnic groups be consideredspecifically. The HEA (2000) found that among black andminority ethnic groups, understanding of healthy eatingmessages varied widely across groups and knowledge offoods high in complex carbohydrates, fibre, fat andsaturated fat was often poor across all ethnic groups.There is, therefore, a need to raise awareness of the linksbetween diet and CHD among these groups and topromote culturally relevant messages.
2.5.2 Children
Early childhood experiences strongly influence dietarypreference and good eating habits. While they may nothave an immediate effect on the rates of CHD, strategiesto promote healthy eating among children will benefit inthe longer term. They will help to address the concerns
Coronary heart disease: guidance for implementing the preventive aspects of the NSF

Improving diet and nutrition
31
Ou
tco
me
Com
plia
nce
with
lega
lre
quire
men
t; gi
ves
a so
und
basis
to
a w
hole
sch
ool
appr
oach
; will
con
trib
ute
toac
hiev
ing
the
Nat
iona
lH
ealth
y Sc
hool
s St
anda
rd(N
HSS
); cl
ear
guid
ance
and
fram
ewor
k fo
r m
onito
ring
will
be
prov
ided
; will
ens
ure
good
nut
ritio
nal s
tand
ards
for
free
mea
ls.
Inte
rven
tion
Nut
riti
onal
stan
dard
s fo
rsc
hool
lunc
hes
From
Apr
il 20
01,
new
legi
slatio
n w
illre
quire
sch
ool
lunc
hes
to m
eet
min
imum
nut
ritio
nal
stan
dard
s.
Evid
ence
Roe
et a
l. (1
997)
iden
tifie
d tw
ogo
od q
ualit
y st
udie
s re
leva
nt t
osc
hool
mea
ls. E
lliso
n et
al.
(198
9,19
90) s
how
ed t
hat
pass
ive
man
ipul
atio
n of
fat
con
tent
red
uced
satu
rate
d fa
t in
take
by
2% w
ith a
simila
r in
crea
se in
pol
yuns
atur
ated
fat
inta
ke. W
hita
ker
et a
l. (1
994)
show
ed a
3%
incr
ease
in lo
w f
atch
oice
s w
hen
prom
oted
.
Wh
o c
ou
ld b
ein
volv
ed?
Loca
l edu
catio
nau
thor
ity (L
EA),
dire
ctse
rvic
e or
gani
satio
n;co
ntra
ct c
ater
ers
and
in-h
ouse
die
titia
ns;
Loca
l Aut
horit
yC
ater
ers’
Ass
ocia
tion
(LA
CA
): ht
tp://
ww
w.
laca
.co.
uk
Scho
ols
Nut
ritio
nA
ctio
n G
roup
(SN
AG
)in
itiat
ive
can
help
scho
ols
in d
evel
opin
ga
scho
ol f
ood
polic
y.
Loca
l hea
lthy
scho
ols
prog
ram
me.
Chi
ld P
over
ty A
ctio
nG
roup
:ht
tp://
ww
w.c
pag.
org.
uk
Skill
s an
d r
eso
urc
es
Supp
ort
for
cate
rers
fro
mco
mm
unity
die
titia
n or
pub
liche
alth
nut
ritio
nist
in t
rain
ing
in h
ealth
ier
cate
ring
prac
tices
and
in m
onito
ring
com
plia
nce
with
the
sta
ndar
ds.
Poin
ts t
o c
on
sid
er
Pric
ing
of h
ealth
ier
choi
ces
–an
d ca
tere
rs’ p
erce
ptio
ns o
fth
e hi
gher
pro
duct
ion
cost
s;in
trod
ucin
g a
scho
ol f
ood
polic
y to
sup
port
ado
ptio
n of
the
stan
dard
s; o
ppor
tuni
ty t
ore
view
sna
ck p
rovi
sions
at
sam
e tim
e, a
s w
ell a
sbr
eakf
ast
club
s an
d ve
ndin
gm
achi
nes.
Mee
ting
and
mon
itorin
gst
anda
rds
will
be
a le
gal
requ
irem
ent.
Furt
her
info
rmat
ion
Dep
artm
ent
for
Educ
atio
nan
d th
e En
viro
nmen
t (D
fEE)
http
://w
ww
.nut
ritio
nal.s
tand
ards
@df
ee.g
ov.u
k
Nat
iona
l Sta
ndar
ds f
orSc
hool
Lun
ches
, Eng
land
.Re
gula
tions
200
0. S
tatu
tory
Inst
rum
ent
num
ber
1777
.Th
e St
atio
nery
Off
ice.
£1.
50.
Eatin
g w
ell a
t sc
hool
: die
tary
guid
ance
for
sch
ool m
eal
prov
ider
s(1
997)
. DfE
EPu
blic
atio
ns, P
O B
ox 5
050,
Ann
esle
y, N
ottin
gham
,N
G15
0D
J. Te
l: 08
4560
2260
. Fre
e of
cha
rge.
Scho
ol M
eals
Ass
essm
ent
Pack
(SM
AP;
com
pute
rpa
ckag
e as
sess
ing
the
nutr
ition
al q
ualit
y of
seco
ndar
y sc
hool
mea
ls)pr
oduc
ed b
y th
e N
HF.
SMA
P, P
O B
ox 7
, Lon
don
W5
2GQ
. £45
.00,
che
ques
paya
ble
to B
SS.
Scho
ol f
ood
polic
y gu
ide
prod
uced
by
SNA
G.
Con
tact
Joe
Har
vey,
Hea
lthEd
ucat
ion
Trus
t (te
l/fax
:01
789
7739
15).
Nut
ritio
n gu
idel
ines
for
scho
ol m
eals
(199
2) a
vaila
ble
from
The
Car
olin
e W
alke
rTr
ust,
22 K
inde
rsle
y W
ay,
Abb
ots
Lang
ley,
Her
ts, W
D5
0DQ
. Cos
t £1
0 in
clud
ing
post
age
and
pack
ing
(p&
p).
Wha
t ar
e to
day’
s ch
ildre
nea
ting?
The
Gar
dner
Mer
chan
tSc
hool
Mea
ls Su
rvey
200
0.G
ardn
er M
erch
ant
(tel:
0179
3 51
2112
).
Tabl
e 2.
6 Su
gges
ted
acti
viti
es t
o su
ppor
t lo
cal a
ctio
n

Coronary heart disease: guidance for implementing the preventive aspects of the NSF
32
Add
ress
es a
ran
ge o
f ris
kfa
ctor
s fo
r C
HD
as
part
of
who
le s
choo
l app
roac
h. H
asa
form
alise
d su
ppor
tne
twor
k. C
ould
be
used
to
form
alise
and
sec
ure
fund
ing
for
any
scho
ol b
ased
initi
ativ
es. A
llow
s a
flexi
ble
appr
oach
to
mee
ting
stan
dard
crit
eria
. N
HSS
sup
port
mat
eria
ls w
illfa
cilit
ate
stra
tegi
cco
nnec
tions
and
hel
p id
entif
ylo
cal p
artn
ers
as w
ell a
spr
ovid
e ca
se s
tudy
exa
mpl
esof
goo
d pr
actic
e.
Eval
uatio
n of
pilo
t sit
es (R
iver
s et
al.
2000
) fou
nd c
onfli
ct b
etw
een
heal
thy
eatin
g cr
iteria
and
sch
ool
mea
ls co
ntra
cts.
New
lega
lm
inim
um s
tand
ards
for
sch
ool
lunc
hes
shou
ld o
verc
ome
this.
Not
yet
eva
luat
ed n
atio
nally
.
Loca
l hea
lthy
scho
ols
prog
ram
me
coor
dina
tors
bas
ed in
LEA
s or
HA
s.
Ou
tco
me
Inte
rven
tion
Evid
ence
Wh
o c
ou
ld b
ein
volv
ed?
Skill
s an
d r
eso
urc
es
Loca
l pro
gram
me
coor
dina
tors
will
wel
com
eth
e in
volv
emen
t of
com
mun
ity d
ietit
ians
, pub
liche
alth
nut
ritio
nist
s, h
ealth
prom
otio
n sp
ecia
lists
, in
mee
ting
the
stan
dard
.
Poin
ts t
o c
on
sid
er
Scho
ols
agre
e pr
iorit
ies
with
coor
dina
tors
of
loca
l hea
lthy
scho
ol p
rogr
amm
es. H
ealth
yea
ting
may
not
be
the
first
prio
rity.
This
is an
opp
ortu
nity
to
beco
me
invo
lved
in t
hest
rate
gic
plan
ning
to
mee
tth
e he
alth
y ea
ting
stan
dard
.
Lega
l req
uire
men
ts f
or s
choo
llu
nche
s w
ill in
crea
se t
hepr
iorit
y fo
r he
alth
y ea
ting.
All
LEA
s ha
ve n
ow s
igne
d up
to a
chie
ve t
he N
HSS
.
Furt
her
info
rmat
ion
Futu
re o
f fo
od in
sch
ools
repo
rt(1
998)
. Ava
ilabl
e fr
eeof
cha
rge
from
Pen
ny R
olfe
,C
hart
wel
ls, Ic
knie
ld H
ouse
,40
Wes
t St
reet
, Dun
stab
le,
Beds
LU
6 1T
A.
McM
ahon
, W. a
nd M
arsh
,T.
, 199
9. F
illin
g th
e ga
p.C
hild
Pov
erty
Act
ion
Gro
up.
Cos
t £5
.00,
http
://w
ww
.cpa
g.or
g.uk
or94
Whi
te L
ion
Stre
et,
Lond
on W
1 9P
F. T
el: 0
2078
37 7
979.
The
ir w
ebsit
eal
so c
onta
ins
brie
fing
pape
rson
sch
ool m
eals
and
heal
thy
eatin
g an
d sc
hool
mea
ls in
Scot
land
.
Nat
iona
l Hea
lthy
Scho
olSt
anda
rd g
uida
nce.
DfE
E (1
999)
. Ava
ilabl
e fr
eefr
om D
fEE
Publ
icat
ions
, PO
Box
5050
, Ann
esle
y,N
ottin
gham
NG
15 0
DJ.
The
‘You
r he
alth
y sc
hool
’se
ctio
n of
http
://w
ww
.wire
dfor
heal
th.
gov.
uk
Food
– a
fac
t of
life
: ran
geof
tea
chin
g re
sour
cem
ater
ial f
or p
rimar
y an
dse
cond
ary
scho
ols
(Brit
ishN
utrit
ion
Foun
datio
n).
Con
tact
020
740
4 65
04 o
rht
tp://
ww
w.n
utrit
ion.
org.
uk
Nat
iona
l hea
lthy
scho
ol s
tand
ard
(NH
SS)
Crit
eria
for
hea
lthy
eatin
g, t
o in
form
impl
emen
tatio
n of
who
le s
choo
lap
proa
ch.

Improving diet and nutrition
33
Ou
tco
me
Off
er b
road
er b
enef
its
(eg
pre-
and
aft
er-s
choo
lca
re).
Opp
ortu
nity
to
enco
urag
e th
ein
take
of
frui
t on
cer
eal,
asju
ice
or a
fter
sch
ool a
ssn
acks
. May
also
hel
p to
addr
ess
low
inta
kes
of ir
onan
d ot
her
mic
ronu
trie
nts
(Gre
gory
et
al. 2
000)
.
HEA
You
ng P
eopl
e an
dH
ealth
Sur
vey
(199
9) r
evea
led
that
alm
ost
one
in f
ive
(18%
)yo
ung
peop
le a
ged
11–1
6ye
ars
neve
r (o
r ha
rdly
eve
r)ha
d br
eakf
ast
befo
re s
choo
l(m
ales
13%
, fem
ales
23%
).
Inte
rven
tion
Evid
ence
34 b
reak
fast
clu
bs; b
reak
fast
clu
bev
alua
tions
cur
rent
ly u
nder
way
.
Wh
o c
ou
ld b
ein
volv
ed?
LEA
Dire
ct S
ervi
ceO
rgan
isatio
ns; s
choo
lca
tere
rs; h
ead
teac
hers
, sch
ool
gove
rnor
s an
d PT
As;
regi
onal
and
loca
lco
ordi
nato
rs o
f th
ehe
alth
y sc
hool
spr
ogra
mm
es; s
choo
lsnu
triti
on a
ctio
ngr
oups
(SN
AG
s);
Kello
gg’s
http
://w
ww
.bre
akfa
st-c
lubs
.co.
uk/
Loca
l hea
lthy
scho
ols
prog
ram
me.
Skill
s an
d r
eso
urc
es
Paid
sta
ff t
o pr
epar
e fo
odan
d su
perv
ise c
hild
ren;
venu
e, f
acili
ties
and
equi
pmen
t fo
r th
e sa
fe a
ndhy
gien
ic p
repa
ratio
n an
dst
orag
e of
foo
d; a
ctiv
ities
/re
sour
ces
to o
ccup
y th
ech
ildre
n; r
esea
rch
supp
ort
toev
alua
te s
ucce
ss o
fpr
ogra
mm
e.
Poin
ts t
o c
on
sid
er
Cou
ld f
orm
par
t of
a w
hole
scho
ol a
ppro
ach
to im
prov
ing
diet
.
Brea
kfas
ts a
nd s
nack
s of
fere
dne
ed t
o re
flect
The
bala
nce
of g
ood
heal
th(H
EA, D
H a
ndM
AFF
199
4) (e
g w
hole
grai
nce
real
s w
ith s
emisk
imm
edm
ilk a
nd f
ruit)
.
Free
EU
inte
rven
tion
stoc
ks o
ffr
uit
coul
d be
use
ful.
Frui
t is
avai
labl
e to
sch
ools
but
this
mus
t be
in a
dditi
on t
o no
rmal
supp
lies
and
not
used
as
part
of s
choo
l can
teen
mea
ls.
Cur
rent
ly, g
over
nmen
t is
fund
ing
brea
kfas
t cl
ubs
inar
eas
of d
epriv
atio
n,in
clud
ing
HA
Zs, e
duca
tion
actio
n zo
nes
(EA
Zs) a
nd S
ure
Star
t ar
eas,
to
help
tac
kle
heal
th in
equa
litie
s.
Furt
her
info
rmat
ion
Brea
kfas
t C
lubs
. A h
owto
…gu
ide.
Kel
logg
’s N
ewPo
licy
Inst
itute
and
Kello
gg’s
. Ava
ilabl
e fr
omht
tp://
ww
w.b
reak
fast
-cl
ub.c
o.uk
Stre
et, C
. and
Ken
way
, P.,
1998
. Fit
for
scho
ol –
how
brea
kfas
t cl
ubs
mee
t he
alth
educ
atio
n an
d ch
ildca
rene
eds.
New
Pol
icy
Inst
itute
.C
ost
£12.
50.
Don
ovan
, N. a
nd S
tree
t, C
.,19
99. F
ood
for
thou
ght
–br
eakf
ast
club
s an
d th
eir
chal
leng
es.N
ew P
olic
yIn
stitu
te. C
ost
£7.5
0.
Repo
rts
avai
labl
e fr
om:
New
Pol
icy
Inst
itute
, 109
Coo
perg
ate
Hou
se, 1
6Br
une
Stre
et, L
ondo
n E1
7N
J(te
l: 02
0 77
21 8
421)
.
Scot
tish
Com
mun
ity D
iet
Proj
ect,
c/o
Scot
tish
Con
sum
er C
ounc
il, R
oyal
Exch
ange
Hou
se, 1
00 Q
ueen
Stre
et, G
lasg
ow G
1 3D
N(te
l 014
1 22
6 52
61).
Emai
lsc
dp@
scot
cons
umer
.org
.uk
Web
site:
http
://w
ww
.die
tpro
ject
.co.
uk
Info
rmat
ion
on E
Uin
terv
entio
n st
ocks
of
frui
tfr
om t
he In
terv
entio
nBo
ard’
s fr
uit
and
vege
tabl
ew
ithdr
awal
sec
tion
(tel:
0118
953
169
4). A
nin
form
atio
n sh
eet f
or s
choo
lsis
avai
labl
e (fo
rm H
OR
18).
Scho
ol f
ood
polic
y gu
ide
prod
uced
by
SNA
G.
Con
tact
Joe
Har
vey,
Hea
lthEd
ucat
ion
Trus
t (te
l/fax
:01
789
7739
15).
Brea
kfas
t an
d af
ter
scho
ol c
lubs
Gov
ernm
ent
has
rece
ntly
fun
ded
230
scho
ol b
reak
fast
club
s as
par
t of
its
driv
e to
tac
kle
ineq
ualit
ies
in h
ealth
.

Coronary heart disease: guidance for implementing the preventive aspects of the NSF
34
Clu
bs c
an s
timul
ate
inte
rest
and
conf
iden
ce t
o de
velo
pco
okin
g sk
ills
out
of t
hesc
hool
set
ting;
Coo
king
for
Kids
rep
orts
opp
ortu
nitie
s to
rein
forc
e nu
triti
on a
nd f
ood
hygi
ene
less
on t
augh
t in
clas
s, a
hea
d st
art
in Y
ear
7fo
od t
echn
olog
y; g
ettin
g to
know
new
sch
ool/t
each
er in
adva
nce;
opp
ortu
nity
to
build
inte
rest
and
ent
husia
sm f
orco
okin
g sk
ills.
Part
of
a ‘w
hole
sch
ool’
appr
oach
to
heal
thy
eatin
g;re
info
rces
the
tau
ght
curr
icul
um o
n he
alth
y ea
ting
and
oral
hea
lth; c
ompl
emen
tsth
e ne
w n
utrit
iona
l sta
ndar
dsfo
r sc
hool
lunc
hes;
pro
vide
sid
eal o
ppor
tuni
ty t
o in
crea
sefr
uit
and
vege
tabl
e in
take
san
d pr
omot
e sn
acks
saf
e fo
rte
eth.
Hea
lthy
tuc
k sh
ops,
brea
k ti
mes
and
vend
ing
Food
and
drin
ksav
aila
ble
at b
reak
times
are
an
impo
rtan
t pa
rt o
f a
who
le s
choo
lap
proa
ch t
o he
alth
yea
ting
and
are
anid
eal o
ppor
tuni
ty t
oin
crea
se c
hild
ren’
sfr
uit
and
vege
tabl
ein
take
s.
Food
Sta
ndar
ds A
genc
y ha
s fu
nded
thre
e st
udie
s pr
omot
ing
frui
t an
dve
geta
bles
in s
choo
ls (A
nder
son
et a
l., U
nive
rsity
of
Dun
dee;
Bar
ker
et a
l., U
nive
rsity
of
Shef
field
; Moo
re e
t al
., U
nive
rsity
of
Brist
ol).
Loca
l gro
wer
s,m
arke
ts,
gree
ngro
cers
, foo
dco
oper
ativ
es a
ndsu
perm
arke
ts; L
EAs;
scho
ol c
ater
ers,
loca
lan
d re
gion
al N
HSS
prog
ram
me
coor
dina
tors
; hea
dte
ache
rs a
nd s
choo
lgo
vern
ors;
SN
AG
s;co
mm
unity
deve
lopm
ent
wor
kers
.
Ou
tco
me
Inte
rven
tion
Cook
ing
skill
scl
ubs
Coo
king
and
foo
dpr
epar
atio
n sk
ills
com
pulso
ry w
ithin
Nat
iona
l Cur
ricul
umFo
od T
echn
olog
y(K
ey S
tage
1 a
nd 2
,op
tiona
l at
Key
Stag
e3
and
4).
Nat
iona
l Ini
tiativ
es o
nco
okin
g sk
ills
incl
ude
Coo
king
for
Kid
s(D
fEE)
for
Yea
rs 6
and
7 an
d Fo
cus
onFo
od c
ooki
ng s
kills
bus,
Ret
ail S
ervi
ces
Ass
ocia
tion
(RSA
)an
d W
aitr
ose.
Evid
ence
Lang
et
al. 1
999
show
ed a
gen
eral
dear
th o
f co
okin
g sk
ills
in t
hepo
pula
tion
and
that
sch
ools
are
ake
y se
ttin
g fo
r le
arni
ng s
uch
skill
s.
Focu
s on
Foo
d is
bein
g ev
alua
ted
byth
e U
nive
rsity
of
Read
ing,
res
ults
due
2001
.
Cook
ing
for
Kids
repo
rted
a r
ange
of b
enef
its a
t en
d of
firs
t ye
ar,
soci
al a
s w
ell a
s ed
ucat
iona
l(W
aldo
n 19
99, u
npub
lishe
d re
port
).
Wh
o c
ou
ld b
ein
volv
ed?
DfE
E’s
Coo
king
for
Kids
; RSA
and
Wai
tros
e Fo
cus
onFo
od; L
EAs;
hea
dte
ache
rs, p
aren
ts a
ndsc
hool
gov
erno
rs,
scho
ol c
ater
ers,
teac
hers
of
food
tech
nolo
gy; l
ocal
chef
s re
stau
rate
urs
and
shop
s w
ho m
aybe
will
ing
tohe
lp/d
onat
ein
gred
ient
s.
Loca
l hea
lthy
scho
ols
prog
ram
me.
Skill
s an
d r
eso
urc
es
Acc
ess
to s
choo
l kitc
hens
or
com
mun
ity k
itche
nseq
uipp
ed f
or t
he s
afe
and
hygi
enic
pre
para
tion
and
stor
age
of f
ood;
tea
chin
gst
aff/s
choo
l mea
ls st
aff
will
ing
to p
artic
ipat
e ou
t of
hour
s; p
aren
ts o
r vo
lunt
eers
to a
ssist
with
sup
ervi
sion;
ingr
edie
nts
and
equi
pmen
t;fu
ndin
g so
urce
s (e
gEd
ucat
ion
Extr
a; T
heFo
unda
tion
for
Aft
er S
choo
lC
lubs
).
A d
edic
ated
per
son
tom
anag
e or
derin
g an
dpr
epar
atio
n of
frui
t/veg
etab
les;
fac
ilitie
s fo
rth
e sa
fe a
nd h
ygie
nic
stor
age,
was
hing
and
prep
arat
ion
of f
ruit
and
vege
tabl
es; f
or t
uck
shop
s/ve
ndin
g m
achi
nes,
som
eone
to
man
age
the
mon
ey; a
pric
ing
polic
yw
here
fru
it is
purc
hase
d;st
ock
rota
tion
and
tem
pera
ture
in v
endi
ngm
achi
nes.
Poin
ts t
o c
on
sid
er
Clu
bs t
ake
plac
e ou
t of
scho
ol h
ours
or
in h
olid
ays
and
for
mos
t ch
ildre
n th
is is
aon
e da
y ex
perie
nce.
Not
a r
epla
cem
ent
for
regu
lar
teac
hing
of
cook
ing
skill
s;ca
n be
a u
sefu
l par
t of
aw
hole
sch
ool a
ppro
ach;
for
som
e ch
ildre
n th
is m
ay b
eon
e of
ver
y fe
w o
ppor
tuni
ties
to c
ook.
New
Nat
iona
l Pla
n fo
r th
eN
HS
has
anno
unce
d a
Nat
iona
l Sch
ool F
ruit
Sche
me
whe
re e
very
chi
ld in
nur
sery
and
aged
fou
r to
six
yea
rs in
infa
nt s
choo
ls w
ill b
e en
title
dto
a f
ree
piec
e of
fru
it ev
ery
scho
ol d
ay (s
ee B
reak
fast
and
afte
r sc
hool
clu
bs).
Nat
iona
l Die
t an
d N
utrit
ion
Surv
ey o
f yo
ung
peop
le(G
rego
ry e
t al
.200
0) s
how
edlo
w in
take
s of
fru
it an
dve
geta
bles
and
hig
h in
take
sof
con
fect
ione
ry a
nd s
oft
drin
ks.
Frui
t an
d ve
geta
ble
inta
kes
are
low
est
in h
ouse
hold
s on
low
inco
me
and
rece
ivin
gbe
nefit
s.
Furt
her
info
rmat
ion
http
://w
ww
.wire
dfor
heal
th.
gov.
uk
Cook
ing
for
Kids
pro
ject
man
ual.
Ava
ilabl
e fr
ee f
rom
Joe
Mon
ks a
t th
eD
epar
tmen
t of
Hea
lth t
el02
0 79
72 2
000.
Focu
s on
Foo
ds c
ampa
ign:
http
://w
ww
.wai
tros
e.co
m/
focu
sonf
ood/
Tel:
0142
2 38
3191
.
Briti
sh D
iete
tic A
ssoc
iatio
nG
ive
Me
5 Pa
ckht
tp://
ww
w.b
da.u
k.co
m/
Tel:
0121
633
955
5.
Info
rmat
ion
on E
Uin
terv
entio
n st
ocks
of
frui
t(s
ee B
reak
fast
and
aft
ersc
hool
clu
bs).
Scho
ol f
ood
polic
y gu
ide
prod
uced
by
SNA
G.
Con
tact
Joe
Har
vey,
Hea
lthEd
ucat
ion
Trus
t(te
l/fax
: 017
89 7
7391
5).

Improving diet and nutrition
35
Cook
and
eat
Sess
ions
Mai
nly
loca
lin
itiat
ives
, som
eba
sed
orig
inal
ly o
nth
e fo
rmer
Get
cook
ing!
prog
ram
me.
Can
hel
p pe
ople
acc
ess
affo
rdab
le m
eals;
may
red
uce
soci
al is
olat
ion;
empo
wer
men
t of
pro
ject
wor
kers
and
dev
elop
men
t of
thei
r sk
ills
base
; may
pro
vide
poin
t of
acc
ess
to o
ther
heal
th a
nd s
ocia
l ser
vice
s.
Com
mun
ity
cafe
s
Run
on a
loca
l and
‘not
for
pro
fit’ b
asis,
ofte
n pa
rt o
f a
wid
erco
mm
unity
cen
tre
offe
ring
othe
rse
rvic
es; a
im t
opr
ovid
e af
ford
able
(not
nec
essa
rily
heal
thy)
mea
ls in
aso
ciab
le a
tmos
pher
e,to
red
uce
soci
aliso
latio
n.
Not
wel
l doc
umen
ted;
an
eval
uatio
nof
a c
omm
unity
caf
é in
sou
thea
stEn
glan
d (K
adus
kar
et a
l.19
99)
coul
d no
t de
term
ine
whe
ther
the
cafe
was
suc
cess
ful i
n its
aim
of
prov
idin
g ch
eap,
goo
d qu
ality
foo
d.
Ou
tco
me
Sust
ain
(200
0) r
epor
ted
that
such
pro
ject
s co
uld
incr
ease
nutr
ition
al k
now
ledg
e an
dim
prov
e sk
ills
as lo
ng a
s th
eap
proa
ch w
as r
elev
ant
topa
rtic
ipan
ts’ c
ultu
ral a
ndso
cio-
econ
omic
circ
umst
ance
s.
Eval
uatio
ns a
lso r
epor
t w
ider
heal
th b
enef
its s
uch
asre
duci
ng s
ocia
l iso
latio
n, a
ndbu
ildin
g se
lf co
nfid
ence
.
May
pro
vide
a f
orum
inw
hich
to
disc
uss
othe
r he
alth
issue
s.
Inte
rven
tion
Evid
ence
Car
aher
et
al.(
1999
) sug
gest
ed t
hat
rede
signe
d co
okin
g an
d fo
odcl
asse
s ch
ange
d di
ets
of y
oung
peop
le a
nd t
heir
fam
ilies
.
A g
ener
al la
ck o
f co
okin
g sk
ills
inth
e po
pula
tion
was
fou
nd a
ndco
nfid
ence
to
cook
var
ied
with
age
and
gend
er (L
ang
et a
l.19
99).
Incr
ease
d se
lf co
nfid
ence
and
este
em f
ound
in G
et C
ooki
ng in
Wal
es(C
arah
er a
nd L
ang
1995
).
Saff
ron
Food
and
Hea
lth P
roje
ct(D
obso
n et
al.
2000
) sug
gest
s th
atth
e ai
m o
f co
mm
unity
foo
d pr
ojec
tsm
ust
be t
o ge
t pe
ople
inte
rest
edan
d im
prov
e co
nfid
ence
and
bas
icco
okin
g sk
ills.
Wh
o c
ou
ld b
ein
volv
ed?
Sess
ions
cou
ld b
e ru
nin
gro
ups
such
as
wom
en’s
gro
ups,
yout
h cl
ubs;
chu
rch,
tem
ples
or
relig
ious
sett
ings
; loc
alca
terin
g co
llege
s,an
d ho
me
econ
omic
ste
ache
rs; L
AC
A; l
ocal
reta
ilers
or
gard
enin
gan
d al
lotm
ent
sche
mes
for
pro
duce
and
ingr
edie
nts;
heal
th v
isito
rs.
Skill
s an
d r
eso
urc
es
Venu
e, f
acili
ties
and
equi
pmen
t fo
r th
e sa
fe a
ndhy
gien
ic p
repa
ratio
n an
dst
orag
e of
foo
d; f
undi
ng;
ingr
edie
nts;
a p
roje
ct le
ader
with
pra
ctic
al f
ood
prep
arat
ion
skill
s, f
ood
hygi
ene
and
nutr
ition
alkn
owle
dge;
link
wor
kers
/pe
er e
duca
tors
, par
ticul
arly
for
wor
k w
ith m
inor
ity e
thni
cgr
oups
or
youn
g pe
ople
;bu
dget
man
agem
ent
skill
s.
Venu
e, f
acili
ties
and
equi
pmen
t fo
r th
e sa
fe a
ndhy
gien
ic p
repa
ratio
n of
food
s; a
pro
ject
lead
er w
ithfo
od p
repa
ratio
n an
d bo
okke
epin
g sk
ills;
tra
inin
g in
food
pre
para
tion
and
food
hygi
ene
for
volu
ntee
rs a
ndpa
id s
taff
.
Poin
ts t
o c
on
sid
er
Cou
ld b
e us
ed t
o en
cour
age
inta
kes
of f
ruit
and
vege
tabl
es b
y pr
ovid
ing
oppo
rtun
ity t
o ta
ste
new
varie
ties.
May
pro
vide
a w
ayin
to
wor
king
with
cer
tain
audi
ence
s (e
g So
uth
Asia
nw
omen
) as
a so
cial
lyac
cept
able
act
ivity
.
Caf
es r
elia
nt o
n ex
tern
alfu
ndin
g, a
nd s
o su
stai
nabi
lity
may
be
an is
sue;
invo
lvin
gth
e co
mm
unity
inde
velo
pmen
t se
ems
to le
adto
gre
ater
sus
tain
abili
ty;
shou
ld b
e ru
n as
a p
rope
rbu
sines
s, c
ompl
ying
with
envi
ronm
enta
l hea
lth (E
H)
and
trad
ing
stan
dard
s; lo
cal
circ
umst
ance
s im
port
ant:
part
icul
arly
goo
d fo
r pe
ople
who
are
hom
eles
s, la
ckco
okin
g fa
cilit
ies
or a
reel
derly
/sin
gle
on lo
w in
com
e.
Furt
her
info
rmat
ion
Food
and
low
inco
me
(FLI
)da
taba
se(h
ttp:
//ww
w.h
ea.o
rg.u
k),
our
heal
thie
r na
tion
inpr
actic
e (O
HN
iP),
HA
Znet
.
Sout
h A
sian
cook
ing
club
inLu
ton
HA
Z is
a Be
acon
Site
and
can
be v
isite
d at
: htt
p://
ww
w.n
hsbe
acon
s.or
g.uk
/
Saff
ron
Food
and
Hea
lthPr
ojec
t:ht
tp://
ww
w.c
rsp.
ac.u
k
Get
coo
king
and
get
shop
ping
pack
fro
m S
usta
in,
£14
(tel:
020
7837
122
8).
OK!
Let
’s c
ook,
Hea
lthy
Nor
folk
200
0, £
2 (te
l: 01
603
487
990)
.
No
dosh
goo
d no
shfr
omN
ight
safe
, Bla
ckbu
rn, £
1(te
l: 01
25 4
5876
87).
FLI d
atab
ase;
OH
NiP
;H
AZn
et.
Just
for
sta
rter
sfr
om t
heH
ealth
Edu
catio
n Bo
ard
for
Scot
land
(tel
: 013
1 53
655
00) ‘
star
ting
up’ a
dvic
ean
d re
cipe
s.
Com
mun
ity C
ater
ing
Initi
ativ
es c
onfe
renc
e re
port
and
‘how
to’
info
rmat
ion,
from
Com
mun
ity H
ealth
UK,
£7.5
0 +
£1.7
5 (p
&p)
(te
l: 01
225
462
680)
.
Hea
rtbe
at A
war
d ca
tere
rs’
guid
e (s
ee ‘C
ater
ing
awar
ds’).
LA, E
HO
and
trad
ing
stan
dard
s; fu
ndin
gco
uld
be a
vaila
ble
from
rege
nera
tion
rela
ted
initi
ativ
es
(eg
New
Dea
l for
Com
mun
ities
and
Sing
le R
egen
erat
ion
Budg
et);
links
with
loca
l sup
erm
arke
ts,
reta
ilers
, com
mun
ityow
ned
reta
iling
(foo
dco
oper
ativ
es) a
ndgr
owin
g sc
hem
es;
loca
l cat
erin
g co
llege
s,LA
CA
(inv
estig
ate
peer
educ
atio
n of
loca
lvo
lunt
eers
); jo
bce
ntre
s fo
r cat
erer
sse
ekin
g w
ork.

Coronary heart disease: guidance for implementing the preventive aspects of the NSF
36
Com
mun
ity
grow
ing
sche
mes
May
var
y fr
om c
ityfa
rms
to a
llotm
ents
or s
chem
es s
et u
p on
was
tela
nd; c
anin
crea
se s
uppl
ies
ofaf
ford
able
veg
etab
les
and
frui
t lo
cally
; can
be li
nked
to
food
coop
erat
ives
;so
met
imes
set
up
with
an
envi
ronm
enta
l rat
her
than
hea
lth a
gend
a.
Brad
ford
‘Gar
deni
ng f
or H
ealth
’pr
ojec
t, ru
n w
ith B
angl
ades
hiw
omen
. Par
ticip
ants
rep
orte
dea
ting
mor
e fr
uit
and
vege
tabl
es,
bein
g m
ore
activ
e, lo
sing
wei
ght
and
feel
ing
mor
e co
nfid
ent
to g
oou
t al
one
(Hus
sain
and
Rob
inso
n20
00).
Ou
tco
me
Like
ly t
o be
bro
ader
tha
nin
crea
sing
the
avai
labi
lity
offr
uit
and
vege
tabl
es a
lone
(e
g pr
ovid
ing
a so
cial
mee
ting
plac
e in
the
loca
lco
mm
unity
); em
pow
erm
ent
of lo
cal c
omm
unity
and
ski
llsde
velo
pmen
t in
tho
seru
nnin
g it;
Bol
ton
Food
coop
erat
ive
deve
lope
d sp
in-
offs
, sup
plyi
ng f
ruit
tuck
shop
s in
sch
ools
and
deliv
ery
to t
he e
lder
ly. T
heTo
wer
Ham
lets
coo
pera
tive
has
subs
eque
ntly
dev
elop
ed a
loca
l far
mer
s’ m
arke
t.
Inte
rven
tion
Com
mun
ity
owne
dre
taili
ng (
food
coop
erat
ives
)
Loca
lly o
rgan
ised
initi
ativ
es t
hat
can
impr
ove
acce
ssib
ility
to f
oods
suc
h as
fru
itan
d ve
geta
bles
inar
eas
that
lack
loca
laf
ford
able
sup
plie
s.
In s
ome
area
s it
isdi
ffic
ult
to a
cces
saf
ford
able
goo
dqu
ality
fru
it an
dve
geta
bles
(PA
T 13
1999
).
Evid
ence
Eval
uatio
ns in
Bol
ton
and
in T
ower
Ham
lets
and
Ste
pney
(Pric
e an
dSe
phto
n 19
95; O
stas
iew
icz
1997
)sh
owed
incr
ease
d av
aila
bilit
y of
fru
itan
d ve
geta
bles
. It
allo
wed
peo
ple
totr
y ne
w f
oods
at
affo
rdab
le p
rices
;in
crea
sed
the
conf
iden
ce, s
elf
este
em a
nd d
evel
oped
new
ski
lls in
thos
e ru
nnin
g th
e co
oper
ativ
e.
Wh
o c
ou
ld b
ein
volv
ed?
LA E
HO
and
tra
ding
stan
dard
s; f
undi
ngco
uld
be a
vaila
ble
from
reg
ener
atio
n-re
late
d in
itiat
ives
(e
g N
ew D
eal f
orC
omm
uniti
es a
ndSi
ngle
Reg
ener
atio
nBu
dget
); s
uppl
iers
such
as
loca
lw
hole
sale
rs, f
arm
ers’
mar
kets
or
com
mun
ity a
llotm
ent
and
grow
ing
sche
mes
.
Incr
ease
buy
ing
pow
er b
y lin
king
with
oth
er lo
cal f
ood
coop
erat
ives
.
May
incr
ease
phy
sical
act
ivity
,re
duce
soc
ial i
sola
tion,
and
build
con
fiden
ce.
Part
icip
ants
in t
he B
radf
ord
Proj
ect
initi
ally
gre
w f
amili
arA
sian
vege
tabl
es b
ut t
hen
grew
and
sta
rted
to
eat
Briti
sh v
eget
able
var
ietie
sw
hich
are
che
aper
; also
deve
lope
d m
arke
tabl
ega
rden
ing
skill
s.
Skill
s an
d r
eso
urc
es
Venu
e, in
clud
ing
hygi
enic
stor
age
spac
e an
d t
rans
port
;eq
uipm
ent
such
as
till,
scal
es,
float
; sta
rt u
p co
sts
and
fuel
cost
s; s
taff
, inc
ludi
ng d
river
san
d a
book
keep
er.
Star
t up
cos
ts; l
and,
equi
pmen
t, st
orag
e, w
ater
supp
ly, s
eeds
; pro
ject
lead
ers
with
exp
erie
nce
in g
arde
ning
/ho
rtic
ultu
re w
ho w
ill n
eed
tobe
pai
d; a
boo
kkee
per;
ifw
orki
ng w
ith b
lack
and
min
ority
eth
nic
grou
ps m
ayne
ed a
link
wor
ker.
Poin
ts t
o c
on
sid
er
Food
coo
pera
tives
are
lega
len
titie
s an
d ha
ve t
o ru
n on
am
embe
rshi
p ba
sis. F
ees
for
mem
bers
hip
can
help
with
star
t up
cos
ts.
Com
mitm
ent
of t
he s
taff
ises
sent
ial t
o en
sure
sur
viva
l.Pa
ymen
t fo
r th
eir
time
may
help
.
Ther
e is
a ne
ed t
o co
mpl
yw
ith t
radi
ng s
tand
ards
and
EH r
egul
atio
ns, a
nd t
o su
pply
cultu
rally
app
ropr
iate
foo
ds.
Food
coo
pera
tives
are
not
view
ed a
s a
long
-ter
mso
lutio
n bu
t ca
n be
use
dal
ongs
ide
othe
r re
gene
ratio
nin
itiat
ives
to
impr
ove
acce
ss.
The
NH
S Pl
anst
ates
tha
t th
ego
vern
men
t w
ill w
ork
with
indu
stry
to
incr
ease
pro
visio
nof
fru
it an
d ve
geta
bles
and
whe
re n
eces
sary
to
esta
blish
loca
l foo
d co
oper
ativ
es.
Get
ting
acce
ss t
o la
nd a
ndse
ttin
g up
an
agre
emen
t fo
rits
use
ove
r a
suita
ble
perio
dof
tim
e; p
ossib
leco
ntam
inat
ion
of la
nd in
som
e ar
eas;
sha
ring
out
prod
uce
betw
een
part
icip
ants
and/
or
selli
ng it
on
to f
ood
coop
erat
ives
, far
mer
s’m
arke
ts, c
omm
unity
caf
es;
may
be
usef
ul in
are
as o
fre
gene
ratio
n w
here
acc
ess
toaf
ford
able
fru
it an
dve
geta
bles
are
poo
r.
May
hel
p m
eet
prio
ritie
s of
LA 2
1.
Furt
her
info
rmat
ion
Star
t yo
ur o
wn
food
co-
opvi
deo
Bolto
n co
-op,
£15
(tel
:01
204
3600
94/3
6009
5).
Food
for
tho
ught
repo
rt a
ndvi
deo.
Wol
verh
ampt
on F
ood
Co-
ops
Um
brel
la G
roup
Ltd
,£1
(tel
: 019
02 3
04 8
51).
The
co-o
p st
art
up p
ack
CW
S. A
vaila
ble
free
(tel
:01
61 8
27 5
349)
.
CW
S sm
all g
rant
sC
omm
unity
Div
iden
dSc
hem
e (te
l: 01
61 8
27 5
950)
.
FLI d
atab
ase,
OH
NiP
,H
AZn
et.
Sand
wel
l Bea
con
site
http
://w
ww
.nhs
beac
ons.
org.
uk/
FLI d
atab
ase.
Sust
ain
publ
icat
ions
:G
row
ing
food
in c
ities
(£10
); Ci
ty h
arve
st (£
30 f
ull r
epor
t,su
mm
ary
£5);
tel:
020
7837
122
8.
Fede
ratio
n of
City
Far
ms
and
Com
mun
ity G
arde
ns, S
tart
erpa
ck(te
l 011
7 92
3 18
00).
Loca
l Age
nda
21
(LA
21)
coo
rdin
ator
s;LA
leisu
re o
ren
viro
nmen
tal
serv
ices
; loc
alho
rtic
ultu
ral c
olle
ges.
Fund
ing
coul
d be
avai
labl
e fr
omre
gene
ratio
n re
late
din
itiat
ives
(eg
New
Dea
l for
Com
mun
ities
and
Sing
leRe
gene
ratio
n Bu
dget
).
Nat
iona
l Soc
iety
of
Allo
tmen
t and
Lei
sure
Gar
dene
rs L
td
(tel:
0153
6 26
6576
).

Improving diet and nutrition
37
Com
mun
ity
shop
san
d si
mila
r sc
hem
es
Set
up in
res
pons
e to
clos
ure
of lo
cal s
hops
on h
ousin
g es
tate
s or
in r
ural
are
as; m
ay b
eru
n on
a ‘n
ot f
orpr
ofit’
bas
is, u
sual
lyby
vol
unte
ers.
Com
mun
ity s
hops
are
a r
ecen
tin
nova
tion,
whi
ch h
ave
not
yet
been
eva
luat
ed.
Ou
tco
me
Impr
oved
acc
ess
to a
ffor
dabl
efr
uit
and
vege
tabl
es; r
etai
lou
tlet
for
com
mun
itygr
owin
g sc
hem
es;
envi
ronm
enta
l ben
efits
inth
at p
rodu
ce is
not
tran
spor
ted
grea
t di
stan
ces;
incr
ease
d so
cial
cap
ital.
Inte
rven
tion
Farm
ers’
mar
kets
Mar
kets
tha
t al
low
farm
ers
and
grow
ers
to s
ell d
irect
ly t
oco
nsum
ers,
the
reby
redu
cing
the
pric
e.
They
are
oft
en s
et u
pas
env
ironm
enta
lin
itiat
ives
and
req
uire
prod
uce
to b
e gr
own
with
in a
cer
tain
radi
us o
f th
e m
arke
t.So
me
focu
s on
orga
nic
prod
uce.
Evid
ence
Farm
ers’
mar
kets
off
er g
ood
valu
efo
r m
oney
; pro
vide
an
oppo
rtun
ityto
buy
fre
sh, l
ocal
pro
duce
; giv
elo
cal p
eopl
e a
sens
e of
wel
l bei
ngan
d be
long
ing;
pro
vide
a s
ocia
lm
eetin
g pl
ace;
and
also
pla
y a
role
in r
evita
lisin
g th
e lo
cal r
ural
econ
omy
(Bur
et
al. 1
999;
Bul
lock
2000
).
Wh
o c
ou
ld b
ein
volv
ed?
LA a
nd t
radi
ngst
anda
rds;
any
loca
lgr
ower
s’as
soci
atio
ns;
LA 2
1 co
ordi
nato
r;N
atio
nal A
ssoc
iatio
nof
Far
mer
s’ M
arke
ts(te
l: 01
225
7879
14);
Soil
Ass
ocia
tion
loca
lfo
od li
nks
depa
rtm
ent
(tel:
0117
914
242
6).
Impr
oved
acc
ess
to f
oods
such
as
frui
t an
d ve
geta
bles
;us
eful
in r
ural
are
as w
here
publ
ic t
rans
port
is p
oor;
shop
staf
f ca
n de
velo
p m
arke
tabl
esk
ills
and
gain
wor
kex
perie
nce;
can
be
part
of
neig
hbou
rhoo
d re
new
alin
itiat
ives
.
Skill
s an
d r
eso
urc
es
Staf
f (p
aid
or v
olun
tary
) to
liaise
with
loca
l cou
ncil,
grow
ers
and
cons
umer
s;su
itabl
e ve
nue
in p
roxi
mity
to
area
of
need
; acc
ess
togr
ower
s w
illin
g to
par
ticip
ate
with
in t
he lo
calit
y.
Proj
ect
lead
ers
with
ret
ail
expe
rienc
e an
d/or
boo
kke
epin
g sk
ills;
driv
er a
ndtr
ansp
ort
to t
rave
l to
who
lesa
lers
; fun
ding
fro
mgr
ants
or
subs
idie
s; s
uita
ble
prem
ises
with
sto
rage
faci
litie
s an
d eq
uipm
ent
inth
e lo
calit
y, w
hich
com
plie
sw
ith E
H a
nd h
ealth
and
safe
ty r
egul
atio
ns.
Poin
ts t
o c
on
sid
er
Nee
ds h
elp
and
supp
ort
from
LA; n
eed
to e
ncou
rage
grow
ers
to p
artic
ipat
e; n
eeds
publ
icity
; an
acce
ssib
le v
enue
not
requ
iring
cos
tly p
ublic
tran
spor
t; en
sure
bon
a fid
egr
ower
s on
ly p
artic
ipat
e; m
ayim
prov
e ac
cess
to
reta
ilse
rvic
es a
nd in
crea
se s
uppl
yof
aff
orda
ble
frui
t an
dve
geta
bles
; may
aff
ect
trad
ein
loca
l sm
all s
hops
.
Mee
ts p
riorit
ies
of L
A 2
1.
‘Not
for
pro
fit’,
ther
efor
ede
pend
ent
on g
rant
s or
subs
idie
s; m
embe
rshi
p fe
esca
n he
lp s
tart
up
cost
s: m
ust
com
ply
with
tra
ding
stan
dard
s, E
H r
egul
atio
ns; i
nso
me
area
s m
ore
appr
opria
teto
tak
e pe
ople
to
shop
sra
ther
tha
n sh
ops
to p
eopl
e(P
AT
13 1
999)
; cou
ld h
elp
impr
ove
acce
ss t
o fr
uit
and
vege
tabl
es; m
ay c
ontr
ibut
e to
neig
hbou
rhoo
d re
new
alst
rate
gies
.
Furt
her
info
rmat
ion
The
Nat
iona
l Ass
ocia
tion
ofFa
rmer
s’ M
arke
ts h
as a
list
of f
arm
ers’
mar
kets
(te
l: 01
225
7879
14)
http
://w
ww
.farm
ersm
arke
ts.
net
‘Eco
-logi
c’ p
ublic
atio
ns o
nfa
rmer
s’ m
arke
ts
(tel:
0122
5 48
4472
).
The
Soil
Ass
ocia
tion
prov
ides
trai
ning
on
sett
ing
up a
ndru
nnin
g a
farm
ers’
mar
ket:
(tel:
0117
914
242
6).
How
to
mak
e yo
urco
mm
unity
sho
p su
ccee
d.C
omm
unity
Ent
erpr
ise L
td(te
l: 01
31 4
75 2
345)
.
Villa
ge s
hops
and
pos
tof
fices
: a g
uide
to
depl
oym
ent
of v
illag
ein
vest
men
t to
res
cue,
sus
tain
and
revi
ve.V
IRSA
, £15
(tel
:01
305
259
383)
.
If th
e vi
llage
sho
p cl
oses
…a
hand
book
on
com
mun
itysh
ops.
Oxf
ord
Rura
lC
omm
unity
Cou
ncil,
£3.
50(te
l: 01
865
8834
88).
LA, E
H d
epar
tmen
tan
d tr
adin
gst
anda
rds;
Vill
age
Reta
il Se
rvic
esA
ssoc
iatio
n (V
IRSA
;te
l: 01
305
259
383)
;fu
ndin
g co
uld
beav
aila
ble
from
rege
nera
tion-
rela
ted
initi
ativ
es (e
g N
ewD
eal f
orC
omm
uniti
es a
ndSi
ngle
Reg
ener
atio
nBu
dget
).
Com
mun
ity O
wne
dRe
taili
ng: t
rain
ing
and
supp
ort
inse
ttin
g up
neig
hbou
rhoo
dsh
ops
(tel:
0143
5 88
3005
)ht
tp://
ww
w.c
omm
uni
t.ret
ailin
g.co
.uk

Coronary heart disease: guidance for implementing the preventive aspects of the NSF
38
Supe
rmar
ket
tour
s
Usu
ally
led
by a
diet
itian
or
nutr
ition
ist w
ith s
mal
lgr
oups
of
cons
umer
s.M
ay f
ocus
on
inte
rpre
ting
food
labe
ls an
d he
alth
clai
ms
and
onse
lect
ing
food
s an
ddi
scus
sing
heal
thie
rpr
epar
atio
n m
etho
ds.
Som
etim
es u
sed
with
grou
ps w
ith a
part
icul
ar a
rea
ofin
tere
st (e
g di
abet
es).
Cate
ring
aw
ards
For
exam
ple,
Hea
rtbe
at A
war
d is
ana
tiona
lly r
ecog
nise
dbu
t lo
cally
run
aw
ard
mad
e to
cat
erer
sw
ho a
dopt
hea
lthie
rpr
actic
es, h
ave
good
stan
dard
s of
foo
dhy
gien
e an
d of
fer
nons
mok
ing
seat
ing.
Usu
ally
run
by
LAEH
Os
in p
artn
ersh
ipw
ith d
ietit
ians
and
heal
th p
rom
otio
nsp
ecia
lists
.
Incr
ease
in s
elf
repo
rted
‘hea
lthy’
purc
hase
s an
d be
havi
our
com
pare
dw
ith c
ontr
ols,
one
mon
th a
fter
tw
o-ho
ur t
our,
but
stud
y w
as o
fpo
or q
ualit
y (S
ilzer
et
al.1
994)
.
One
of
six s
chem
es e
valu
ated
by
HEA
in 1
998
show
ed s
igni
fican
tlygr
eate
r us
e of
hea
lthie
r ca
terin
gpr
actic
es in
aw
ard
hold
ing
prem
ises
(Pat
erso
n et
al.,
in p
repa
ratio
n).
A q
uart
er o
f H
eart
beat
Aw
ard
prem
ises
repo
rted
incr
ease
s in
sal
esof
som
e he
alth
ier
item
s bu
t sa
les
ofle
ss h
ealth
y ch
oice
s te
nded
to
rem
ain
the
sam
e (H
olds
wor
th e
t al
.19
99).
Gre
ater
pro
visio
n of
som
e he
alth
ier
food
s, h
ealth
ier
optio
ns a
nd g
reat
erco
mm
itmen
t to
hea
lthy
eatin
g(W
arm
et
al. 1
997)
.
Ou
tco
me
Acc
ess
to m
ains
trea
m s
hops
and
serv
ices
(PA
T 13
199
9).
Ove
rcom
e di
ffic
ultie
sex
perie
nced
by
peop
le in
carr
ying
hea
vy f
ruit
and
vege
tabl
es f
rom
sho
ps.
Inte
rven
tion
Tran
spor
t to
sho
pssc
hem
es
Can
be
run
on a
loca
lba
sis o
r by
link
ing
with
sup
erm
arke
tch
ains
or
loca
lre
taile
rs.
Evid
ence
Case
stu
dy
Hac
kney
Com
mun
ity t
rans
port
deve
lope
d to
incr
ease
acc
ess
tolo
cal a
ctiv
ities
for
disa
bled
and
elde
rly p
eopl
e. ‘P
lusb
uses
’ now
run
ever
y 30
min
utes
on
a fix
ed r
oute
whi
ch li
nks
up t
he lo
cal h
ospi
tal,
day
cent
res,
sch
ools,
sho
ps a
ndot
her
tran
spor
t in
terc
hang
es.
Wh
o c
ou
ld b
ein
volv
ed?
Loca
l sup
erm
arke
tsan
d lo
cal c
ham
ber
ofco
mm
erce
or
trad
e.
May
be
usef
ul a
s pa
rt o
f a
wid
er p
rogr
amm
e of
hea
lthy
eatin
g su
perm
arke
t in
itiat
ives
,bu
t m
ost
need
to
be
coor
dina
ted
natio
nally
rat
her
than
loca
lly.
Roe
et a
l. (1
997)
fou
nd f
our
good
qua
lity
supe
rmar
ket
stud
ies:
thr
ee p
oint
of
purc
hase
labe
lling
, one
vid
eofe
edba
ck w
hich
sho
wed
incr
ease
s in
sal
es o
fpr
omot
ed p
rodu
cts
whi
le t
hest
udy
was
run
ning
.
Bett
er r
elat
ions
hips
bet
wee
nca
tere
rs a
nd E
H d
epar
tmen
t;go
od p
ublic
rel
atio
ns (P
R) f
orca
tere
rs, a
com
mitm
ent
tocu
stom
er c
are
and
to f
ood
hygi
ene
trai
ning
; diff
icul
t to
dem
onst
rate
the
eff
ect
of t
hesc
hem
e on
the
ove
rall
diet
of
cons
umer
s.
Skill
s an
d r
eso
urc
es
Driv
ers,
veh
icle
s an
d fu
ndin
gto
sup
port
run
ning
cos
ts;
insu
ranc
e an
d co
mpl
ianc
ew
ith s
afet
y re
gula
tions
.
Die
titia
n/pu
blic
hea
lthnu
triti
onist
; goo
d re
latio
nshi
pw
ith lo
cal s
uper
mar
ket
and
abili
ty t
o id
entif
y an
d us
e PR
oppo
rtun
ities
.
EH, d
iete
tics
and
heal
thpr
omot
ion
expe
rtise
on
smok
ing
polic
ies;
par
tner
ship
wor
king
ski
lls; e
valu
atio
nsk
ills;
tim
e fo
r pr
oces
sing
annu
al r
enew
als
in a
dditi
onto
new
app
licat
ions
; fun
ding
to s
uppo
rt s
chem
e; P
Rsu
ppor
t.
Poin
ts t
o c
on
sid
er
Are
as t
hat
need
to
be li
nked
,fr
eque
ncy
of s
ervi
ces;
link
ing
with
loca
l ret
aile
rs b
ussc
hem
es.
Sche
mes
may
be
very
use
ful
in in
crea
sing
acce
ss t
oaf
ford
able
sup
plie
s of
fru
itan
d ve
geta
bles
.
Use
ful w
ith g
roup
s w
ith a
part
icul
ar f
ocus
(eg
diab
etic
s);
usef
ul t
o ba
se t
he t
our
onTh
eba
lanc
e of
goo
d he
alth
(HEA
, DH
and
MA
FF 1
994)
;op
port
unity
to
mak
e lin
ksw
ith lo
cal r
etai
lers
.
To m
axim
ise im
pact
may
be
best
con
cent
rate
d in
ven
ues
whe
re th
e sa
me
peop
le e
atev
ery
day
(eg
wor
kpla
ces,
priso
ns);
need
s to
hav
e bo
thdi
etet
ic a
nd E
HO
inpu
t,re
quire
s a
good
wor
king
rela
tions
hip
betw
een
the
two
depa
rtm
ents
; cou
ld h
elp
tosu
ppor
t HIm
Ps a
s re
quire
s jo
int
wor
king
bet
wee
n LA
and
HA
trus
ts. E
valu
atio
n is
vita
l, as
fund
ers
may
see
k ev
iden
ce o
fbe
nefit
s be
fore
com
mitt
ing
reso
urce
s to
con
tinue
the
sche
me.
Thi
s w
ill a
lso h
elp
tobu
ild e
vide
nce
base
nat
iona
lly.
Furt
her
info
rmat
ion
Com
mun
ity T
rans
port
Ass
ocia
tion
(tel:
0161
367
8780
).
Ferg
uslie
Par
k A
cces
s to
Shop
ping
pro
ject
rep
ort
(tel:
0141
887
965
0).
Reta
ilers
’ ow
n m
ater
ials
base
d on
The
bala
nce
ofgo
od h
ealth
(HEA
, DH
and
MA
FF 1
994)
cou
ld b
e us
edas
a r
esou
rce.
Hea
rtbe
at A
war
d St
arte
r pac
k;A
cat
erer
’s g
uide
to th
eH
eart
beat
Aw
ard
(pac
ks 5
);H
eart
beat
Aw
ard
flyer
s(p
acks
50).
Hea
rtbe
at a
war
d ce
rtifi
cate
san
d w
indo
w s
ticke
rs (p
acks
10 e
ach)
.
A g
uide
to e
valu
atin
g th
eH
eart
beat
Aw
ard.
(HEA
1998
).
The
Hea
rtbe
at A
war
d: M
akin
gth
e m
ost o
f the
med
ia(H
EA19
96).
All
HEA
pub
licat
ions
ava
ilabl
efr
om M
arst
on B
ook
Serv
ices
(tel:
0123
5 46
5565
).
Supe
rmar
kets
,nu
triti
onist
s ba
sed
inhe
ad o
ffic
e; lo
cal
pres
s; g
roup
s w
ithpa
rtic
ular
inte
rest
(e
g di
abet
ics,
mot
hers
of
youn
gch
ildre
n).
Cat
erer
s, c
ater
ing
trai
ners
, em
ploy
ers,
occu
patio
nal h
ealth
nurs
es; h
ealth
prom
otio
n sp
ecia
lists
with
an
inte
rest
inev
alua
tion.

Improving diet and nutrition
39
Prom
otin
g he
alth
yea
ting
in p
re-
scho
ols,
suc
h as
fam
ily c
entr
es r
unby
soc
ial s
ervi
ces
orpr
ivat
e da
ynu
rser
ies
Pre-
scho
ol a
nd d
ay c
are
cent
res
wer
e lik
ely
to b
e ap
prop
riate
sett
ings
for
inte
rven
tions
(Ted
ston
eet
al.
1998
b).
Ou
tco
me
Aro
und
an e
ight
h of
ene
rgy,
fat,
and
satu
rate
d fa
t in
the
diet
is f
rom
the
foo
d ea
ten
away
fro
m h
ome.
Wor
kpla
ce c
ater
ers
may
prep
are
a sig
nific
ant
prop
ortio
n of
mea
ls fo
rre
gula
r cu
stom
ers
and
soha
ve a
n im
port
ant
influ
ence
on t
he o
vera
ll di
et.
Inte
rven
tion
Ado
ptio
n of
heal
thie
r ca
teri
ngpr
acti
ces
inw
orkp
lace
cat
erin
gan
d hi
ghlig
htin
g‘h
ealt
hier
‘ cho
ices
Evid
ence
Posit
ive
effe
ct o
n fo
od c
hoic
es f
orth
e du
ratio
n of
inte
rven
tions
mod
ifyin
g re
cipe
s or
hig
hlig
hted
heal
thie
r ch
oice
s in
var
iety
of
sett
ings
; no
good
qua
lity
stud
ies
ina
wor
kpla
ce s
ettin
g (R
oe e
t al
.19
97);
incr
ease
in s
ales
of
low
fat
mea
ls in
the
wor
kpla
ce w
hen
high
light
ed w
ith s
ymbo
ls on
men
usan
d po
ster
s (L
evin
199
6).
Mak
ing
smal
l cha
nges
to
best
selli
ng d
ishes
can
be
effe
ctiv
e in
prom
otin
g he
alth
ier
choi
ces,
and
pres
enta
tion
is im
port
ant.
Prom
otin
g m
enu
item
s is
succ
essf
ulw
here
par
alle
l cho
ices
are
on
offe
r(H
EA 1
998b
).
Wh
o c
ou
ld b
ein
volv
ed?
Cat
erer
s, s
ervi
cest
aff,
cate
ring
man
ager
s, c
hef
trai
ners
; wor
kpla
cem
anag
emen
t, hu
man
reso
urce
s,oc
cupa
tiona
l hea
lth;
cont
ract
cat
erer
sdi
etiti
ans/
in h
ouse
chef
tra
iner
s;co
mm
unity
die
titia
ns,
Publ
ic H
ealth
Nut
ritio
nist
s,w
orkp
lace
hea
lthpr
omot
ion
spec
ialis
ts.
Incr
ease
chi
ld c
arer
s, c
hild
ren
and
pare
nts’
nut
ritio
nal
know
ledg
e; im
prov
e m
ain
mea
l pro
visio
n an
d be
twee
nm
eal s
nack
s an
d dr
inks
.
Skill
s an
d r
eso
urc
es
Som
e tr
aini
ng o
f ca
tere
rs a
ndse
rvic
e st
aff;
basic
res
earc
hsk
ills
to c
arry
out
nee
dsas
sess
men
t am
ong
cust
omer
s.
Com
mun
ity d
enta
l sta
ff a
ndco
mm
unity
die
titia
ns c
anpr
ovid
e sp
ecia
list
know
ledg
ean
d lo
cal d
ata
(eg
on o
ral
heal
th o
f un
der
fives
).
Poin
ts t
o c
on
sid
er
Wor
kpla
ce o
ffer
s a
maj
orop
port
unity
to
gain
acc
ess
to,
and
com
mun
icat
e w
ith, a
larg
e pr
opor
tion
of t
he a
dult
popu
latio
n; a
ckno
wle
dged
by
gove
rnm
ent
as a
use
ful
sett
ing
for
gene
ral h
ealth
prom
otio
n.
Cov
ert
chan
ges
to t
he m
enu
over
all h
ave
pote
ntia
l to
bene
fit a
ll cu
stom
ers,
prom
otin
g he
alth
ier
optio
nson
ly b
enef
its c
usto
mer
s th
atch
oose
the
m.
Shou
ld e
xten
d to
ven
ding
and
snac
k pr
ovisi
on a
nd t
oho
spita
lity
cate
ring.
May
hel
p ca
tere
r qu
alify
for
an H
BA.
A c
ompr
ehen
sive
heal
thy
eatin
g po
licy
shou
ld in
clud
eal
l mea
ls, s
houl
d co
nsid
erch
ildre
n w
ith s
peci
alre
quire
men
ts a
nd s
houl
dfo
ster
goo
d ea
ting
skill
s an
dta
ble
man
ners
.
A m
ore
limite
d po
licy
may
not
cove
r be
twee
n m
eal
snac
ks.
Furt
her
info
rmat
ion
Tipp
ing
the
bala
nce
vide
oan
d w
orks
hop
note
s, H
EA;
A c
ater
er’s
gui
de t
o th
eH
eart
beat
Aw
ard,
HEA
; Din
eou
t ea
t w
ell,
leaf
let,
DH
; Th
e na
tiona
l cat
erin
gin
itiat
ive:
pro
mot
ing
heal
thie
r ch
oice
s,H
EA;
Fram
ewor
k fo
r ac
tion.
Hea
lth a
t w
ork
in t
he N
HS,
HEA
.
Thes
e pu
blic
atio
ns a
reav
aila
ble
free
fro
m M
arst
onBo
ok S
ervi
ces
(tel:
0123
5 46
5565
).
Web
site:
http
://w
ww
.sur
esta
rt.g
ov.u
k/ho
me.
cfm
on S
ure
Star
tin
clud
es a
com
preh
ensiv
eco
ntac
t lis
t fo
r un
der
5sag
enci
es a
nd w
eb li
nks.
Car
olin
e W
alke
r Tr
ust
(199
8). E
atin
g w
ell f
orun
der-
5s in
chi
ld c
are.
Prac
tical
and
nut
ritio
nal
guid
elin
es.2
2 Ki
nder
sley
Way
, Abb
ots
Lang
ley,
Her
tfor
dshi
re, W
D5
0DQ
.C
ost
£12.
95 (i
nclu
ding
p&
p).
Wat
t, R.
, ed.
, 199
9. O
ral
heal
th p
rom
otio
n: a
gui
de t
oef
fect
ive
wor
king
in p
re-
scho
ol s
ettin
gs.L
ondo
n:H
EA. A
vaila
ble
free
fro
mM
arst
on B
ook
Serv
ices
(te
l: 01
235
4655
65).
Hea
lth p
rom
otio
nsp
ecia
lists
; LA
ear
lyye
ars
advi
ser;
volu
ntar
y se
ctor
(e
g Pr
e-Sc
hool
Lear
ning
Alli
ance
,N
atio
nal
Chi
ldm
indi
ngA
ssoc
iatio
n); l
ocal
Sure
Sta
rtpr
ogra
mm
es w
orki
ngin
par
tner
ship
with
pare
nts.

Gregory, J.R., Collins, D.L., Davies, P.S.W., Hughes, J.M. and Clarke,
P.C., 1995. National diet and nutrition survey: children aged 11⁄2 to 41⁄2
years. Vol. 1, Report of the diet and nutrition survey. London: The
Stationery Office..
Gregory, J., Lowe, S., Bates, C. J., Prentice, A., Jackson, L. V., Smithers,
G., Wenlock, R. and Farron, M., 2000. National diet and nutrition
survey: young people aged 4 to 18 years. Vol. 1, Report of the diet
and nutrition survey. London: The Stationery Office.
HEA, 1992. Scientific basis of nutrition education: a synopsis of
dietary reference values. London: HEA.
HEA, 1996. Nutritional aspects of cardiovascular disease. London: HEA.
HEA, 1998a. Deprived neighbourhoods and access to retail services:
a report on work undertaken by the Health Education Authority on
behalf of the Department of Health and the Social Exclusion Unit
(unpublished). London: HEA.
HEA, 1998b. The national catering initiative: promoting healthier
choices. London: HEA.
HEA, 1999. Young people and health: health behaviour in school-aged
children. A report of the 1997 findings. London: HEA.
HEA, 2000. Black and minority ethnic groups in England: the second
health and lifestyles survey. London: HEA.
HEA, DH and MAFF, 1994. The balance of good health.
London: HEA.
Hodgson, P., Wyles, D., Kennedy-Haynes, L. and Hunt, C., 1995. Friends
with food: the development of a nutrition education programme for
low income groups, 1990–1994. Huddersfield: Huddersfield Health
Promotion Unit.
Holdsworth, M., Haslam, C. and Raymond, N.T., 1999. An assessment
of compliance with nutrition criteria and food purchasing trends in
Heartbeat Award premises. Journal of Human Nutrition and Dietetics,
12, 327–335.
Hussain, H. and Robinson, J., 2000. Gardening for health:
evaluation. Bradford: Heartsmart and Bradford Community
Environment Project.
Joshipura, K.J., Ascherio, A., Manson, J.E. and Stampfer, M.J., 1999.
Fruit and vegetable intake in relation to risk of ischemic stroke.
Journal of the American Medical Association, 282,
1233–1239.
2.7 References
Acheson, D., 1998. Independent inquiry into inequalities in health
report. London: The Stationery Office.
Brunner, E., White, I., Thorogood, M., Bristow, A., Curle, D. and
Marmot, M., 1997. Can dietary interventions change diet and
cardiovascular risk factors? A meta-analysis of randomised control
trials. American Journal of Public Health, 87 (9), 1415–1422.
Bullock, S., 2000. The economic benefits of farmers’ markets. London:
Friends of the Earth.
Bur, A.M., Jewell, T. and Rayner, K., 1999. Sussex Farmers’ Market: an
evaluation of three pilot markets in Lewes. Lewes: Common Cause.
Caraher, M. and Lang, T., 1995. Evaluating cooking skills classes: a
report to Health Promotion Wales. Cardiff: Health Promotion Wales.
Caraher, M. and Lang, T., 1999. Can’t cook, won’t cook: a review of
cooking skills and their relevance to health promotion. International
Journal of Health Promotion and Education, 37 (3), 89–100.
Contento, I., 1995. The effectiveness of nutrition education and
implications for nutrition education policy. Journal of Nutrition
Education, 27, 279–418.
DH, 1994. Nutritional aspects of cardiovascular disease: report of the
cardiovascular review group of the Committee on Medical Aspects of
Food Policy. London: The Stationery Office.
DH, 1996. Low income, food, nutrition and health: report from the
Nutrition Task Force. London: DH.
DH, 1998. Nutritional aspects of the development of cancer: report of
the working group on diet and cancer of the Committee on Medical
Aspects of Food and Nutrition Policy. London: The Stationery Office.
Dobson, B., Kellard, K. and Talbot, D., 2000. A recipe for success? An
evaluation of a community food project. Loughborough: Centre for
Research in Social Policy, Loughborough University.
Ellison, R.C., Capper, A.L., Goldberg, R.J., Witschi, J.C. and Stare, F.J., 1989.
The environment component changing school food service to promote
cardiovascular health. Health Education Quarterly, 16, 285–297.
Ellison, R.C., Goldberg, R.J., Witschi, J.C., Capper, A.L., Puleo, E.M. and
Stare, F.J., 1990. Use of fat modified food products to change dietary
fat intake of young people. American Journal of Public Health, 80,
1374–1376.
Coronary heart disease: guidance for implementing the preventive aspects of the NSF
40

Improving diet and nutrition
41
Kaduskar, S., Boaz, A., Dowler, E., Meyrick, J. and Rayner, M., 1999.
Evaluating the work of a community café in a town in the South
East of England: reflections on methods, process and results. Health
Education Journal, 58, 341–354.
Kennedy, L. A., Ubido, J., Elhassan, S., Price, A. and Sephton, J., 1999.
Dietetic helpers in the community: the Bolton Community Nutrition
Assistants Project. Journal of Human Nutrition and Dietetics, 12,
501–512.
Lang, T., Caraher, M., Dixon, P. and Carr-Hill, R., 1999. Cooking skills
and health. London: HEA.
Levin, S., 1996. Pilot study of a cafeteria program relying primarily
on symbols to promote healthy choices. Journal of Nutrition
Education, 28 (5), 282–285.
Lobstein, T., 1997. If they don’t eat a healthy diet, it’s their own
fault! Myths about food and low income. London: National Food
Alliance.
Lowe, F., 2000. The psychological determinants of children’s food
preferences. Bangor: University of Wales (in press).
Marmot, M., 1994. The cholesterol papers. British Medical Journal,
308, 351–352.
McArthur, D., 1998. Heart-healthy eating behaviors of children
following a school based intervention: a meta-analysis. Issues in
Comprehensive Pediatric Nursing, 21, 35–48.
McGlone, P., Dobson, B., Dowler, E. and Nelson, M., 1999. Food
projects and how they work. London: Joseph Rowntree Foundation.
MAFF, 1998. National food survey 1997, annual report on food
expenditure, consumption and nutrient intakes. London:
The Stationery Office.
NHF, 1997. At least five a day – strategies to increase fruit and
vegetable consumption. London: The Stationery Office/NHF.
NHF, 1999. Looking to the future: making CHD an epidemic
of the past. London: The Stationery Office.
Ostasiewicz, L., 1997. Evaluation of Tower Hamlets food co-ops.
London: Tower Hamlets Food Co-op.
Paterson, K., Poulter, J., Swann, C. and Peploe, K., 2000. The
effecitveness of the Heartbeat Award in England: a review. London
(in preparation).
PAT 13, 1999. Improving shopping access for people living in deprived
neighbourhoods. London: Social Exclusion Unit.
Peersman, G., Harden, A. and Oliver, S., 1998. Effectiveness of health
promotion interventions in the workplace: a review. London: HEA.
Price, S. and Sephton, J., 1995. Evaluation of Bolton’s food co-ops.
Bolton: Community Healthcare.
Rivers, K., Aggleton, P., Chase, E., Downie, A., Mulvihill, C., Sinkler, P.,
Tyrer, P. and Warwick, I., 2000. Setting the standard: research linked to
the development of the national healthy school standard (NHSS).
London: DH and DfEE.
Roe, L., Hunt, P., Bradshaw, H. and Rayner, M., 1997. Health promotion
interventions to promote healthy eating in the general population: a
review. London: HEA.
Silzer, J.S., Sheeska, J., Tomasik, H.H. and Woolcot, D.M., 1994. An
evaluation of ‘Supermarket Safari’ nutrition education tours. Journal of
the Canadian Dietetic Association, 55, 179–183.
Sustain, 2000. Making links – a toolkit for local food projects. 2nd ed.
London: Sustain: the alliance for better food and farming.
Tang, J.L., Armitage, J.M., Lancaster, T., Silagy, C.A., Fowler, G.H. and
Neil, H.A.W., 1998. Systematic review of dietary intervention trials to
lower blood total cholesterol in free-living subjects. British Medical
Journal, 316, 1213–1220.
Tedstone, A.E., Aviles, M. Shetty, P. and Daniels, L.A., 1998.
Effectiveness of interventions to promote healthy eating in pre-school
children aged 1–5 years: a review. London: HEA.
Van der Weijden, T., 1998. Economic evaluation of cholesterol related
interventions in dietary practice: an appraisal of the evidence. Journal of
Epidemiology and Community Health, 52, 586–594.
Warm, D.L, Rushmere, A.E, Margetts, B.M, Kerridge, L. and
Speller, V.M., 1997. The Heartbeat Award Scheme: an evaluation
of catering practices. Journal of Human Nutrition and Dietetics, 10,
171–179.
Whitaker, R.C., Wright, J.A., Koepsell, T.D., Finch, A.J. and Psaty, B.M.,
1994. Randomized intervention to increase children’s selection of
low-fat foods in school lunches. Journal of Paediatrics, 125,
535–540.
Wood, D., Durrington, P., Poulter, N., McInnes, G., Rees, A. and Wray,
R., on behalf of the British Cardiac Society, British Hyperlipidaemia

Yu-Poth, S, 1999. Effects of the National Cholesterol Education
Programs’ Step I and Step II dietary intervention programs on
cardiovascular risk factors: a meta-analysis. American Journal of Clinical
Nutrition, 69, 632–646.
Association, British Hypertension Society and British
Diabetic Association, 1998. Joint British recommendations
on prevention of coronary heart disease in clinical practice.
Heart, 80 (suppl 2).
Coronary heart disease: guidance for implementing the preventive aspects of the NSF
42

3.1 Introduction
There is international consensus that a physically active lifestyle is important for health and has greatpotential health gain (WHO/Federation of Sports Medicine 1995; US Department of Health and HumanServices 1996).
Physical activity has been shown to have the followingbenefits:
• Regular physical activity or cardiorespiratory fitnessdecreases the risk of cardiovascular disease mortality ingeneral and of CHD mortality in particular
• The level of decreased risk of CHD attributable toregular physical activity is similar to that of otherlifestyle factors, such as not smoking
• Regular physical activity prevents or delays thedevelopment of high blood pressure, and exercisereduces blood pressure in people with hypertension
• Physical activity is also important in controllingdiabetes, regulating weight and reducing the risks ofosteoporosis and colon cancer.
Since there is a high rate of inactivity in the population,the majority of the population could benefit fromincreasing their activity. The attributable risk frominactivity for CHD is considerable. It has been estimatedthat in the US, 35% of CHD deaths could be attributedto inactivity (Powell and Blair 1994). Physical activity is animportant element in controlling overweight and obesity(discussed in more detail in Chapter 4).
3.2 Objectives of physical activity interventions
The current guideline is to achieve 30 minutes of moderateintensity activity (such as brisk walking, heavy gardeningand heavy housework) on at least five days of the week(DH 1996). Walking and cycling are frequently cited asexamples of how to achieve this recommendation(WHO/Federation of Sports Medicine 1995; USDepartment of Health and Human Services 1996).
The overall prevalence of physical activity is low (see Box3.1). Data from the 1998 Health Survey for England (JointSurveys Unit 1999) showed that 37% of men and 25%of women met the current guidelines for activity (30minutes of activity per day on at least five days of the
Chapter 3Increasing physical activity
Increasing physical activity
Box 3.1 Proportion of men and women in England meeting physical activity guidelines by age, 1998
Age (years) 16–24 25–34 35–44 45–54 55–64 65–74 75+ All ages
Men 58 48 43 36 32 17 7 37Women 32 31 32 30 21 12 4 25
Source: Joint Surveys Unit (1999)
43

week). These levels drop with age. Participation is loweramong many black and minority ethnic groups.
An important step in the effective promotion of physical activity is developing strategies that encourage partnerships between a variety of professionals and community groups. Reviews of effective policy development emphasise the importance of a strong evidence base, ownership by arange of stakeholders, community involvement, needsanalysis and evaluation (HEA 1995; NHF 1995; Foster2000). For more data on the effectiveness of physicalactivity strategies, see Table 4.7 in Chapter 4: Reducingoverweight and obesity.
3.3 Features of effective interventions
A review of randomised controlled trials of physicalactivity promotion found some evidence that physicalactivity can be increased and maintained for up to twoyears. Interventions that encourage walking and do notrequire attendance at a facility appear most likely to leadto sustainable increases in physical activity (Hillsdon et al.1999). Others have found that promoting lifestylephysical activity (eg walking) leads to similar changes inbehaviour and CHD risk factors as does promotingstructured, facility-based, interventions (Dunn et al. 1999).
Hillsdon et al. (1999) also reported that brisk walking hasthe greatest potential for meeting current physical activityrecommendations. Regular brisk walking can lead to themajority of health benefits associated with physicalactivity (Morris and Hardman 1997).
Interventions aimed at modifying the environment, suchas signs posted to increase stair climbing (Brownell et al.1980; Blamey et al. 1995), have proved effective alsoover the short term.
3.4 Components of a local strategy
3.4.1 Healthcare interventions
Interventions in healthcare settings can increase physicalactivity for both primary and secondary prevention(Simons-Morton et al. 1998). Long-term effects are morelikely with continuing intervention and multipleintervention components such as supervised exercise,
provision of equipment and behavioural approaches(Simons-Morton et al. 1998).
Mixed results have been obtained on the effectiveness ofprimary care based interventions, but these have beenshown to be moderately effective. A recent study did notfind evidence of longer-term maintenance of increasedlevels of physical activity (Harland et al. 1999). A benefitof primary care based intervention is that it can reach awide range of the population (Harland et al. 1999).
3.4.2 Exercise referral schemes
These involve primary care staff (usually practice nurses orGPs) referring patients to leisure centres for advice andassistance in increasing physical activity. Although there isa lack of rigorous evaluation of these programmes, thereis some evidence of short-term increases in the level ofactivity. However, there is no evidence of a sustainedlong-term behaviour change. Data from case studies suggestan impact on a range of parameters in a variety of people.The effectiveness of the schemes may be improved when:
• Staff are trained in behaviour change strategies
• Quality supervision is achieved by adequatepractitioner–patient ratios
• Liaison between health and leisure service personnel isestablished and maintained
• Community based networks offer support beyond thereferral period, incorporating sustained, active living(Riddoch et al. 1998).
Some practitioners have expressed concerns about theamount of time and resources required to set up and runhigh quality referral schemes that address the needs ofonly a small section of the population. Targeting ofappropriate referrals will be an important task whereschemes are adopted.
3.4.3 Workplaces
Workplaces provide an organisational structure for coordination of health programmes. However, existingresearch, although not conclusive, shows that it can leadto increases in physical activity (Shephard 1990; Bovell
Coronary heart disease: guidance for implementing the preventive aspects of the NSF
44

1992; Dishman et al. 1998). A booklet is available with ideas for introducing workplace physical activity,giving examples of three case studies (Elder 1996). Some interventions to promote active commuting usingwritten materials have shown increases in physical activity levels (Mutrie et al. 1999; see also section 3.4.7:Physically active transport).
3.4.4 Mass media
In mass media interventions, the number of contacts and tailored interventions was important for increasing effectiveness but there was little impact on long-term physical activity behaviour (Marcus et al.1998).
3.4.5 Schools
Physical activity programmes in schools have beenassociated with a number of positive changes. Mostinterventions are developed as a result of collaborationbetween schools and external advisory and supportservices, in the context of local healthy schoolsprogrammes (HEA 1998a). Reviews of activity promotion in schools (Shephard et al. 1980; Simons-Morton et al. 1988; Pieron et al. 1996; Harris1997; Sallis et al. 1990, 1993) have concluded that:
• Appropriately designed, delivered and supported physical activity curriculum can enhance current levels ofphysical activity and can improve physical skilldevelopment
• Young people benefit from access to suitable and accessible facilities and opportunities for physicalactivity
• Interventions are likely to be more effective when young people are involved in planningprogrammes.
A qualitative exploration of the views of young people(aged 11–15 years) shows clear gender differences, withyoung women less likely to engage in active pursuits. Aflexible and differentiated approach to physical activitypromotion may be required to meet the needs andpreferences of this group (Mulvihill et al. 2000).
Features of well-designed schemes [Department ofEnvironment, Transport and the Regions (DETR) 1999]include:
• Quality of teacher skills, knowledge and experienceenhanced through professional education and trainingprogrammes
• Differentiation in the design of interventions accordingto young people’s developmental and other needs
• A range of enjoyable, health enhancing physicalactivities
• A whole school approach to the promotion of physicalactivity, including
– a physical and health education curriculum– extracurricular activities– links with the local community– safe transport routes to schools
• The involvement and support of the local community
• Provision of appropriate activities to meet the religiousand cultural needs of people from minority ethnic groups
• A mechanism to demonstrate how a school willmeasure increases in the levels of participation inregular physical activity.
3.4.6 Older people
Physical activity promotion for older people (HEA 1995;Walters et al. 1999) should:
• Provide opportunities for affordable, accessible physical activity (particularly for those least likely totake part)
• Address psycho-social needs and combine fun andsocialising with physical activity
• Involve older people in the planning, implementationand evaluation of programmes
• Address the specific needs of different groups
• Address the political, social and economic barriers thatdiscourage older people from participating
Increasing physical activity
45

• Ensure that the outdoor environment is safe andpleasant for taking exercise.
Addressing the environmental and planning aspects thatpromote or deter physical activity is important in meetingthe needs of older people. This includes factors that makeolder people feel unsafe, either from other people orhostile environments (Walters et al. 1999).
A WHO (1996) consensus statement is available on levelsof physical activity to improve health in older adults.
3.4.7 Physically active transport
Transport offers potential for health enhancing physicalactivity. Cycling and walking can be of suitable intensity,and trips such as commuting or travel to school areregular, frequent and often of a suitable length (71% ofjourneys are less than five miles, and 45% less than two)(DETR 1996). Mutrie et al. (1999) found significantincreases in walking to work when written interactivepromotional material was used, but no increases in cyclecommuting. Evidence suggests that promoting workplacebased cycling requires attention to environmental factors,both in the workplace (eg cycle parking and showers) andto the road environment (eg safety). Walking and cyclingto work have been shown to lead to improved healthoutcomes (Vuori and Oja 1999).
3.5 Reducing inequity
Deprived groups are twice as likely to be sedentary as themost affluent groups (Gordon et al. 1999). A higherproportion of men in lower social classes participate inmoderate or vigorous activity, but this is mainly due tooccupational physical activity. The trend does not apply towomen. However, a higher proportion of men and
women in non-manual occupations participate in sportsand leisure activities compared with those in manualoccupations.
The characteristics of good practice in work on physicalactivity and inequalities (HEA 1999a) include:
• Proactive outreach work
• A multidisciplinary approach
• Involving the targeted communities
• Developing new partnerships with professionals whohave good access to ‘hard to reach’ groups.
Barriers to participation in physical activity among blackand minority ethnic groups tend to be similar to many ofthose in other groups, including lack of time and concernsabout body shape. Additional barriers include racism,cultural inappropriateness (eg lack of single sex provision),the importance of family responsibilities and languageissues (HEA 1997a). More single sex exercise facilities mayencourage uptake among Asian women (HEA 2000).
Participation in physical activity tends to be low amongpeople with disabilities. A key issue is for people withdisabilities to participate in activities that they enjoy,perceive as supportive in maintaining activities of dailyliving and are activities which can be incorporated easilyinto routine life. Activities must be:
• Appropriate from a social, environmental andphysiological perspective
• Planned in close cooperation with the target group
• Involve specialist advice where appropriate (HEA 1997b).
Coronary heart disease: guidance for implementing the preventive aspects of the NSF
46

Increasing physical activity
47
3.6 Useful sources of information about community based programmes
The European Heart Network has produced a report Physical activity andcardiovascular disease prevention in the European Union. It summarises theevidence on the relationship between physical activity and cardiovascularhealth and provides recommendations to encourage a more activeenvironment.
http://www.ehnheart.org/pdf/activity.pdf
Europe on the move! is an information network of the Europeanprogramme for the Promotion of Health-Enhancing Physical Activity (HEPA).There are many links on their website to European local initiatives withcontact details. A guide for promoting walking in the community has beenproduced by the Finnish Rheumatism Association and links are available viathis site.
http://www.europe-on-the-move.nl/europe/start.html
Promotion of transport, walking and cycling in Europe: strategy directions isa web accessible document that includes useful and practical informationon promoting transport walking and cycling. It suggests strategies, definestargets, and provides advice on funding, advocacy and lobbying, monitoringand evaluation. It can be accessed at the Europe on the Move site.
http://www.europe-on-the-move.nl/europe/start.html
Looking to the future: making CHD an epidemic of the past (NHF 1999)reviews successes and failures of health policy in reducing high rates ofCHD.
Moving on: international perspectives on promoting physical activity is areport from a symposium in 1994 designed to support the Physical ActivityTask Force in its role of developing a national strategy for promotingphysical activity in England (Killoran et al. 1995).
A community approach to behavioural change in the promotion of physical activity,published by the Center for Disease Control and Prevention (CDC), is aimedat all those interested in a community-wide strategy (central and localgovernment, transport, health and community planners, exercise specialistsand health professionals, community groups, businesses, schools, colleges anduniversities).
http://www.cdc.gov/nccdphp/dnpa/pahand.htm
The CDC in the USA has a report entitled Physical activity and health whichcovers the promotion of physical activity in our daily lives.
http://www.cdc.gov/nccdphp/sgr/summary.htm
The CDC has also published a set of guidelines on the promotion of physicalactivity in children and adolescents, with guidance on the benefits andconsequences of physical activity.
http://www.cdc.gov/nccdphp/dash/physact.htm
For helpful advice on active school travel projects the School Travel AdvisoryGroup (STAG) report gives extensive recommendations for the developmentof active travel patterns in the school setting. These have been endorsed byDH, DETR and the DfEE.
www.local-transport.detr.gov.uk/schooltravel

Coronary heart disease: guidance for implementing the preventive aspects of the NSF
48
Tabl
e 3.
7 Su
gges
ted
acti
viti
es t
o su
ppor
t lo
cal a
ctio
n
Prim
ary
care
Inte
rven
tion
Evid
ence
Ou
tco
me
Skill
s an
d r
eso
urc
esPo
ints
to
co
nsi
der
Furt
her
info
rmat
ion
Indi
vidu
al p
atie
ntri
sk a
sses
smen
t an
dad
vice
Som
e ev
iden
ce f
or s
hort
-ter
mef
fect
iven
ess
but
no e
vide
nce
ofsu
stai
nabi
lity
(Bul
l and
Jam
rozi
k19
98; M
arcu
s et
al.
1998
; Eak
in e
tal
. 200
0).
Iden
tific
atio
n of
leve
ls of
activ
ity, i
nter
vent
ions
bas
edon
pre
dict
ed r
isk.
Ass
essm
ent
prot
ocol
s,ta
ilore
d ad
vice
, res
pons
ive
tocl
ient
’s n
eeds
, kno
wle
dge
ofhe
alth
impa
ct o
f ph
ysic
alac
tivity
on
heal
th.
NSF
CH
D r
equi
rem
ent
to‘id
entif
y al
l peo
ple
atsig
nific
ant
risk
ofca
rdio
vasc
ular
dise
ase
…an
dof
fer
them
app
ropr
iate
adv
ice
and
trea
tmen
t to
red
uce
thei
rris
ks’ (
Stan
dard
4);
know
ledg
e of
loca
l fac
ilitie
sus
eful
; kno
wle
dge
ofm
essa
ges
abou
t ph
ysic
alac
tivity
may
be
low
am
ong
PHC
sta
ff; f
ocus
on
activ
eliv
ing
likel
y to
be
appr
opria
tefo
r m
any
peop
le.
Coa
ts e
t al
. (19
95).
Coun
selli
ng f
orbe
havi
our
chan
geFr
eque
nt p
rofe
ssio
nal c
onta
ct is
asso
ciat
ed w
ith a
dher
ence
(Hill
sdon
et a
l. 19
99).
Long
-ter
m e
ffec
ts a
rem
ore
likel
y w
ith c
ontin
uing
inte
rven
tions
and
beh
avio
ural
appr
oach
es (S
imon
s-M
orto
n et
al.
1998
).
Sust
aine
d be
havi
our
chan
gein
tar
get
grou
p, p
ossib
lere
duct
ion
in r
isk f
acto
rs
(eg
hype
rten
sion)
in t
arge
tgr
oup.
Mot
ivat
iona
l int
ervi
ewin
g,go
od k
now
ledg
e ab
out
phys
ical
act
ivity
and
loca
lfa
cilit
ies.
Ava
ilabi
lity
and
time
of P
HC
staf
f; m
ost
effe
ctiv
e in
tho
seac
tivel
y co
ntem
plat
ing
incr
easin
g le
vels
of p
hysic
alac
tivity
.
Har
land
et
al. (
1999
);H
illsd
on e
t al
. (19
99).
Phys
ical
act
ivit
yre
ferr
alSm
all b
ut p
ossib
ly m
eani
ngfu
lim
prov
emen
ts a
chie
ved
(Rid
doch
et
al. 1
998)
; no
evid
ence
of
long
-ter
mim
pact
.
Effe
ctiv
e pa
rtne
rshi
p be
twee
nhe
alth
and
leisu
re s
ervi
ces,
iden
tific
atio
n an
d re
ferr
al o
fap
prop
riate
pat
ient
s,su
stai
ned
beha
viou
r ch
ange
s.
Col
labo
ratio
n w
ith le
isure
serv
ices
tra
ined
sta
ff,
com
mun
ity n
etw
orks
to
supp
ort
post
-ref
erra
l; co
stly
,re
sour
ce in
tens
ive.
Effe
ctiv
enes
s im
prov
ed w
hen:
staf
f ar
e tr
aine
d in
beh
avio
urch
ange
str
ateg
ies,
and
qua
lity
supe
rvisi
on is
ach
ieve
d by
adeq
uate
pat
ient
/pra
ctiti
oner
ratio
s; o
ppor
tuni
ties
for
targ
etin
g gr
oups
with
clin
ical
cond
ition
s pu
ttin
g th
em a
tris
k.
Ridd
och
et a
l. (1
998)
.
Wh
o c
ou
ld b
ein
volv
ed?
PHC
sta
ff.
PHC
sta
ff,
phys
ioth
erap
ists,
leisu
re p
rofe
ssio
nals.
GP,
PH
C s
taff
, lei
sure
serv
ice
pers
onne
l,H
LC s
taff
.

Increasing physical activity
49
Inte
rven
tion
Prom
otio
n of
act
ive
tran
spor
t
This
incl
udes
wal
king
to s
choo
l (e
g W
alki
ng b
uses
)an
d w
alki
ng/c
yclin
gto
wor
k.
Evid
ence
Wal
king
is a
key
inte
rven
tion
topr
omot
e ac
tive
lifes
tyle
s (M
orris
and
Har
dman
199
7). E
nviro
nmen
tal
chan
ges
are
impo
rtan
t to
fac
ilita
teits
upt
ake.
Are
as t
hat
prom
ote
the
need
s of
cyc
lists
and
ped
estr
ians
have
abo
ve a
vera
ge u
se o
f th
ese
mod
es (e
g Yo
rk t
rans
port
pol
icy:
Hou
se o
f C
omm
ons
1996
).
Ou
tco
me
Redu
ced
dang
er t
ope
dest
rians
/cyc
lists
by
enco
urag
ing
grea
ter
activ
etr
ansp
ort;
mod
al s
hift
tow
ards
the
se t
rans
port
choi
ces.
Skill
s an
d r
eso
urc
es
Cro
ss s
ectio
nal f
inan
cing
thro
ugh
HIm
Ps p
ossib
le; s
kills
– jo
int
wor
king
, tar
get
sett
ing
and
plan
ning
.
Poin
ts t
o c
on
sid
er
Prod
uctio
n of
a lo
cal
tran
spor
t pl
an (L
TP) i
s a
requ
irem
ent
for
LAs;
prom
otio
n of
cyc
ling
and
wal
king
is e
ncou
rage
d, a
s is
join
t w
orki
ng w
ith H
As,
HIm
Pco
ordi
nato
rs a
nd o
ther
s.
Sche
mes
add
ress
ing
dang
erfr
om v
ehic
les
(eg
20 m
phzo
nes)
hav
e sh
own
dram
atic
acci
dent
red
uctio
n ou
tcom
es(6
1% d
rop
in p
edes
tria
nca
sual
ties
and
a 67
% d
rop
inch
ild p
edes
tria
n an
d cy
clist
sca
sual
ties;
Web
ster
and
Mac
kie
1996
).
Furt
her
info
rmat
ion
HEA
(199
8c, 1
999b
,c);
DET
R (1
999,
200
0). F
ree
copi
es o
f th
e la
tter
(Sch
ool
trav
el s
trat
egie
s an
d pl
ans.
Abe
st p
ract
ice
guid
e fo
r lo
cal
auth
oriti
es) a
re a
vaila
ble,
tel
:08
70 1
2262
36 (q
uotin
g:99
ASC
S 02
40A
).
WH
O (1
998)
; web
site:
ww
w.w
ho.d
k/en
viro
nmen
t/pa
mph
lets
Wh
o c
ou
ld b
ein
volv
ed?
Tran
spor
t
LAs,
edu
catio
nse
rvic
es; b
usin
ess;
nong
over
nmen
tal
orga
nisa
tions
(NG
Os)
;lo
cal r
oad
safe
tyof
ficer
s; p
olic
e;
LA 2
1.

Coronary heart disease: guidance for implementing the preventive aspects of the NSF
50
Inte
rven
tion
NH
SS, ‘
who
lesc
hool
’ app
roac
h
Scho
ol t
rave
l pla
ns[in
clud
ing
Safe
rRo
utes
to
Scho
ol(S
RTS)
]
Evid
ence
Posit
ive
outc
omes
hav
e be
enre
port
ed f
ollo
win
g im
plem
enta
tion
of p
hysic
al a
ctiv
ity p
rogr
amm
es in
scho
ols.
Cas
e st
udie
s ha
ve s
how
n in
crea
ses
in c
yclin
g, w
alki
ng a
nd b
us u
se
(eg
Wal
king
bus
es) (
DET
R 20
00a)
.
Ou
tco
me
Sugg
ests
all
pupi
ls ex
perie
nce
two
hour
s of
phy
sical
act
ivity
a w
eek;
enc
oura
ges
staf
f,pu
pils,
par
ents
/car
ers
and
othe
r ad
ults
to
beco
me
invo
lved
in p
rom
otin
gph
ysic
al a
ctiv
ity.
Skill
s an
d r
eso
urc
es
In-s
ervi
ce t
rain
ing
of t
each
ers.
May
invo
lve
phys
ical
cha
nges
to r
oad
layo
ut o
r sc
hool
envi
ronm
ent;
prov
ision
of
safe
cyc
le p
arks
.
Poin
ts t
o c
on
sid
er
Phys
ical
act
ivity
par
ticip
atio
nm
ay e
nhan
ce a
cade
mic
perf
orm
ance
and
enc
oura
gelif
elon
g ph
ysic
al a
ctiv
ity;
prov
ides
pos
itive
envi
ronm
enta
l im
pact
(eg
redu
ced
car
trav
el);
help
sfu
lfil N
atio
nal C
urric
ulum
requ
irem
ents
for
sci
ence
and
phys
ical
edu
catio
n as
wel
l as
cont
ribut
es t
o th
e na
tiona
lfr
amew
ork
for
pers
onal
,so
cial
and
hea
lth e
duca
tion
(PSH
E).
Scho
ol t
rave
l pla
ns a
resu
ppor
ted
by In
tegr
ated
Tran
spor
t W
hite
Pap
er (D
ETR
1998
); ca
n be
inco
rpor
ated
into
a lo
cal t
rans
port
pla
n;lin
ks t
o lo
cal e
nviro
nmen
tal
conc
erns
(Com
mun
itySt
rate
gy, L
A21
).
Furt
her
info
rmat
ion
The
NH
SS id
entif
ies
crite
riaon
phy
sical
act
ivity
to
info
rmgo
od p
ract
ice
and
the
impl
emen
tatio
n of
a ‘w
hole
scho
ol’ a
ppro
ach
(NH
SS20
00).
NH
SS s
uppo
rt m
ater
ial o
nph
ysic
al a
ctiv
ity f
or p
rimar
yan
d se
cond
ary
scho
ols;
NH
SS p
hysic
al a
ctiv
ity,D
Han
d D
fEE
(200
0). L
ondo
n:H
DA
.
Briti
sh H
eart
Fou
ndat
ion
(BH
F) (2
000)
.
http
://w
ww
.wire
dfor
heal
th.
gov.
uk/
The
STA
G r
epor
t is
avai
labl
eat
: htt
p://w
ww
.loca
l-tr
ansp
ort.d
etr.g
ov.u
k/sc
hool
trav
el/in
dex.
htm
#199
8-19
99re
port
DET
R Sc
hool
Tra
vel P
lan
Best
Prac
tice
Gui
de:
http
://w
ww
.loca
l-tr
ansp
ort.d
etr.g
ov.u
k/sc
hool
tra
vel/b
pgla
/inde
x.ht
m
Scho
ol T
rave
l Str
ateg
ies
and
Plan
s C
ase
Stud
ies
Repo
rtca
n be
acc
esse
d at
:ht
tp://
ww
w.lo
cal-
tran
spor
t.det
r.gov
.uk/
scho
oltr
avel
/bpg
la/c
ases
tudi
es/in
dex
.htm
In t
his
guid
e, d
etai
ls ar
epr
ovid
ed f
or u
rban
and
rur
alsc
hool
s.
Sust
rans
SRT
S ca
n be
acce
ssed
at:
http
://w
ww
.sus
tran
s.or
g.uk
/f_
srs.
htm
Wh
o c
ou
ld b
ein
volv
ed?
Staf
f, pu
pils,
loca
led
ucat
ion
auth
ority
(LEA
), he
alth
y sc
hool
sne
twor
k, le
isure
serv
ices
, tra
nspo
rtde
part
men
t, N
GO
s(e
g Su
stra
ns).
Scho
ols
Impr
oved
env
ironm
ent
for
cycl
ing
and
wal
king
; cha
nges
in u
se o
f m
otor
ised
trav
el t
osc
hool
; red
uced
roa
d da
nger
.
Staf
f, pu
pils,
par
ents
,lo
cal t
rans
port
plan
ners
, NG
Os
(Sus
tran
s), s
choo
lgo
vern
ors.

Increasing physical activity
51
Inte
rven
tion
’Gre
en‘ t
rans
port
plan
s (G
TPs)
Stai
r us
e pr
omot
ion
Evid
ence
Sche
mes
to
prom
ote
wal
king
to
wor
k ca
n be
eff
ectiv
e (W
alk
in t
ow
ork
out,
Mut
rie e
t al
. 199
9);
chan
ges
in t
rave
l mod
es w
hen
GTP
sha
ve b
een
impl
emen
ted.
Prom
otio
n of
sta
ir us
e w
as e
ffec
tive
in G
lasg
ow, u
sing
post
ers
(Bla
mey
et a
l. 19
95).
Ou
tco
me
Perc
enta
ge o
f em
ploy
ers
with
deve
lope
d tr
ansp
ort
plan
s;ch
ange
s in
wor
kpla
ce t
rave
l.
Skill
s an
d r
eso
urc
es
Prov
ide
safe
par
king
for
bicy
cles
and
sho
wer
s.
Poin
ts t
o c
on
sid
er
NSF
CH
D m
ilest
one:
‘By
Apr
il20
02 e
very
loca
l hea
lthco
mm
unity
will
… h
ave
deve
lope
d “g
reen
” tr
ansp
ort
plan
s’ (m
ilest
one
3).
Prom
otio
n of
GTP
s ne
ed n
otbe
con
fined
to
heal
th s
ervi
cesit
es. W
orkp
lace
cyc
ling
prom
otio
n in
par
ticul
arre
quire
s en
viro
nmen
tal
chan
ges
(in t
he w
orkp
lace
and
on t
he r
oad)
.
Che
ap in
terv
entio
n;ob
ject
ives
alli
ed w
ithen
viro
nmen
tal c
once
rns
(redu
ctio
n in
use
of
elec
tric
ity).
Furt
her
info
rmat
ion
Tran
spor
t 20
00 (1
998)
.
DET
R ad
vice
for
gov
ernm
ent
depa
rtm
ents
: ‘gr
een
tran
spor
t gu
ide’
http
://w
ww
.env
ironm
ent.
detr
.gov
.uk/
gree
ning
/flee
t/gc
ont.h
tm
DET
R (1
999,
200
0b).
Free
copi
es o
f th
e la
tter
(Sch
ool
trav
el s
trat
egie
s an
d pl
ans.
Abe
st p
ract
ice
guid
e fo
r lo
cal
auth
oriti
es) a
re a
vaila
ble,
tel
:08
70 1
2262
36 (q
uotin
g:99
ASC
S 02
40A
).
WH
O (1
998)
; web
site:
ww
w.w
ho.d
k/en
viro
nmen
t/pa
mph
lets
Wh
o c
ou
ld b
ein
volv
ed?
Staf
f, un
ions
, loc
altr
ansp
ort
plan
ners
,lo
cal p
ublic
tra
nspo
rtpr
ovid
ers.
Wor
kpla
ce in
terv
enti
ons
Stai
r us
e to
bec
ome
the
norm
; inc
reas
ed p
rom
inen
ceof
sta
irs in
bui
ldin
g de
sign
com
pare
d to
lift
s/es
cala
tors
;in
crea
sed
use
of s
tairs
.
Staf
f, un
ions
,em
ploy
ers,
arc
hite
cts.

Coronary heart disease: guidance for implementing the preventive aspects of the NSF
52
Inte
rven
tion
Prom
otin
g us
e of
faci
litie
s
Thes
e in
clud
e le
isure
and
spor
ts c
entr
es,
com
mun
ity c
entr
es,
and
loca
l com
mun
ityin
terv
entio
ns f
orm
inor
ity g
roup
s.
Evid
ence
Acc
ess
and
cost
are
impo
rtan
tde
term
inan
ts f
or m
any
grou
ps.
Invo
lvin
g ‘h
ard
to r
each
’ gro
ups
islik
ely
to in
crea
se u
ptak
e an
dap
prop
riate
ness
of
proj
ects
.
Ou
tco
me
Skill
s an
d r
eso
urc
es
Aud
it an
d ev
alua
tion
skill
s,tr
ansla
tion,
kno
wle
dge
oflo
cal f
acili
ties;
com
mun
ityde
velo
pmen
t sk
ills;
sep
arat
ech
angi
ng a
reas
; pro
visio
n of
appr
opria
te f
acili
ties.
Poin
ts t
o c
on
sid
er
Cul
tura
l and
lang
uage
issu
esm
ay b
e im
port
ant.
‘Spo
rty’
conn
otat
ions
of
leisu
re a
ndex
erci
se c
entr
es c
an b
e of
fpu
ttin
g. H
LC f
undi
ng is
avai
labl
e. P
roje
cts
need
to
bead
ditio
nal t
o st
atut
ory
prov
ision
and
invo
lve
com
mun
ities
in d
evel
opm
ent
and
man
agem
ent.
Furt
her
info
rmat
ion
HEA
(199
7a,b
, 199
8b,
1999
a).
The
Con
fede
ratio
n of
Indi
anO
rgan
isatio
ns r
uns
anex
erci
se p
roje
ct t
o in
crea
sele
vels
of w
alki
ng in
the
Asia
n co
mm
unity
inLe
ices
ter
(con
tact
San
deep
Rohi
t, te
l: 01
16 2
25 9
299,
for
deta
ils).
Wh
o c
ou
ld b
ein
volv
ed?
Leis
ure
acti
viti
es
Iden
tific
atio
n of
gro
ups
not
part
icip
atin
g in
loca
lpr
ovisi
on; i
ncre
ased
part
icip
atio
n by
‘har
d to
reac
h’ g
roup
s; in
volv
emen
t in
desig
n an
d ru
nnin
g of
proj
ects
by
repr
esen
tativ
esfr
om s
peci
fic lo
cal g
roup
s,su
ch a
s ol
der
peop
le, b
lack
and
min
ority
eth
nic
grou
ps,
youn
g pe
ople
, peo
ple
with
disa
bilit
ies.
Leisu
re s
ervi
ces,
prof
essio
nals/
com
mun
ity le
ader
sin
volv
ed w
ith ’h
ard
to r
each
‘ gro
ups,
PHC
, com
mun
itygr
oups
, HLC
s.

Increasing physical activity
53
Inte
rven
tion
Hea
lth
wal
ks a
ndot
her
non-
faci
lity
base
d ph
ysic
alac
tivi
ty
Inte
grat
ion
of lo
cal
plan
s
Evid
ence
Unc
erta
inty
abo
ut w
ho p
artic
ipat
esan
d im
pact
s on
oth
er p
hysic
ally
activ
e be
havi
ours
; 11%
of
the
Sonn
ing
Com
mon
pop
ulat
ion;
thr
eetim
es m
ore
wom
en t
han
men
(Bar
tlett
199
8); s
ome
evid
ence
of
ash
ift f
rom
car
jour
neys
to
wal
king
/cyc
ling.
Envi
ronm
ent
impo
rtan
t fo
r in
form
alph
ysic
al a
ctiv
ity (e
g w
alki
ng, a
ctiv
epl
ay) b
ut f
requ
ently
not
for
mal
lyev
alua
ted.
Ou
tco
me
Loca
l hea
lth w
alks
,pa
rtne
rshi
ps w
ithtr
ansp
ort/e
nviro
nmen
tse
rvic
es; r
aise
d pr
ofile
of
phys
ical
act
ivity
; add
ress
esso
me
safe
ty is
sues
.
Skill
s an
d r
eso
urc
es
Map
s an
d/or
mar
ked
rout
es,
trai
ned
lead
ers.
Skill
s in
dev
elop
ing
part
ners
hips
acr
oss
sect
ors.
Poin
ts t
o c
on
sid
er
Part
icip
ants
ten
d to
be
olde
ran
d fr
om h
ighe
r so
cio-
econ
omic
gro
ups.
Con
sider
com
mun
ity g
arde
ning
sche
mes
or
gard
enin
g on
pres
crip
tion.
LAs
will
hav
e re
quire
men
t to
prod
uce
com
mun
ityst
rate
gies
and
man
y ha
veLA
21 p
lans
. Nei
ghbo
urho
odre
new
al c
onsu
ltatio
n w
aspu
blish
ed r
ecen
tly. S
uppo
rts
seve
ral s
usta
inab
lede
velo
pmen
t ai
ms.
Per
sona
lsa
fety
is f
requ
ently
an
impo
rtan
t co
ncer
n re
stric
ting
use
of o
pen
spac
e an
d ne
eds
to b
e ad
dres
sed.
Lot
tery
fund
ing
(£12
5m) i
s av
aila
ble
for
‘Gre
en a
nd s
usta
inab
leco
mm
uniti
es’.
Furt
her
info
rmat
ion
Bart
lett
, H.,
1998
. Wal
king
the
way
to
heal
th. B
HF/
Con
sum
ers
Ass
ocia
tion
(CA
).
Sonn
ing
Com
mon
Hea
lthW
alk
prog
ram
me
anex
ampl
e (B
artle
tt 1
998)
.
New
Opp
ortu
nitie
s Fu
nd(N
OF)
web
site:
http
://w
ww
.nof
.org
.uk/
env/
tem
p.cf
m?c
onte
nt=e
nvi_
1
Com
mun
ity s
trat
egy
cons
ulta
tion
web
site:
http
://w
ww
.loca
l-re
gion
s.de
tr.g
ov.u
k/co
nsul
t/lg
bill9
9/pc
sdra
ft/in
dex.
htm
DET
R (1
999,
200
0b).
Free
copi
es o
f th
e la
tter
(Sch
ool
trav
el s
trat
egie
s an
d pl
ans.
Abe
st p
ract
ice
guid
e fo
r lo
cal
auth
oriti
es) a
re a
vaila
ble,
tel
:08
70 1
2262
36 (q
uotin
g:99
ASC
S 02
40A
).
WH
O (1
998)
; web
site:
http
://w
ww
.who
.dk/
envi
ron
men
t/pam
phle
ts
Wh
o c
ou
ld b
ein
volv
ed?
PHC
sta
ff,
envi
ronm
ent,
plan
ning
and
tran
spor
tpr
ofes
siona
ls, le
isure
serv
ices
, LA
21.
Com
mun
ity
stra
tegi
es/L
A 2
1/ne
ighb
ourh
ood
rene
wal
Dev
elop
men
t of
eff
ectiv
ein
ters
ecto
ral p
artn
ersh
ips;
prov
ision
of
safe
,ap
prop
riate
ly b
uilt
desig
n fo
rac
tive,
hig
h qu
ality
life
styl
es.
Com
mun
ities
, loc
alpl
anne
rs, a
rchi
tect
s,de
velo
pers
, bus
ines
s,Re
gion
alD
evel
opm
ent
Age
ncie
s (R
DA
s),
gove
rnm
ent
offic
es,
polic
e.

3.8 References
Bartlett, H., Ashley, A. and Howells, K., 1998. Evaluation of the
Sonning Common health walks scheme. Oxford: Brookes University.
BHF, 2000. Active school resource pack. London: BHF.
Blamey, A., Mutrie, N. and Aitchison, T., 1995. Health promotion
by encouraging use of stairs. British Medical Journal, 311, 289–290.
Bovell, V., 1992. The economic benefits of health promotion in the
workplace. London: HEA.
Brownell, K.D., Stunkard, A.J. and Albaum, J.M., 1980. Evaluation and
modification of exercise patterns in the natural environment. American
Journal of Psychiatry, 137, 1540–1545.
Bull, F.C. and Jamrozik, K., 1998. Advice on exercise from a family
physician can help sedentary patients to become active. American
Journal of Preventive Medicine, 152, 85–94.
Coats, A., McGee, H. and Stokes. H., eds., 1995. British Association of
Cardiac Rehabilitation guidelines for cardiac rehabilitation.
Oxford: Blackwell Science.
DETR, 1996. Vulnerable road users, Transport Committee, third report.
London: The Stationery Office.
DETR, 1998. A new deal for transport: better for everyone. London:
DETR.
DETR, 1999. School travel: strategies and plans: a best practice guide
for local authorities. London: DETR.
DETR, 2000a. School travel strategies and plans: case study reports.
London: DETR.
DETR, 2000b. Encouraging walking: advice to local authorities.
London: DETR.
DH, 1996. Strategy statement on physical activity. London: DH.
Dishman, R.K., Oldenburg, B., O’Neal, H. and Shephard R.J., 1998.
Worksite physical activity interventions. American Journal of Preventive
Medicine, 15, 344–361.
Dunn, A., Marcus, B., Kampert, J., Garcia, M., Kohl, H. and Blair, S.
1999. Comparison of lifestyle and structured interventions to promote
physical activity and cardiorespiratory fitness: a randomised trial. Journal
of the American Medical Association, 281, 327–34.
Eakin, E.G., Glasgow, R.E. and Riley, K.M., 2000. Review of primary
care-based physical activity intervention effectiveness and implications
for practice and future research. Journal of Family Practice, 49 (2), 158–168.
Elder, P., 1996. Promoting physical activity in NHS workplaces. London:
NHS Executive and HEA.
Foster, C., 2000. Guidelines for health-enhancing physical activity
promotion programmes. Oxford: BHF Health Promotion Research Group.
Gordon, D., Shaw, M., Dorling, D. and Smith, G.D., eds., 1999.
Inequalities in health: the evidence presented to the independent inquiry
into inequalities in health, chaired by Sir Donald Acheson. Bristol: The
Policy Press.
Harland, J., White, M., Drinkwater, C., Chin, D., Farr, L. and Howel, D.,
1999. The Newcastle exercise project: a randomised controlled trial of
methods to promote physical activity in primary care. British Medical
Journal, 319, 828–832.
Harris, J., 1997. Physical education: a picture of health? The
implementation of health related exercise in the national curriculum in
secondary schools in England and Wales, doctoral dissertation.
Loughborough: Loughborough University.
HEA, 1995. Promoting physical activity: guidance for commissioners,
purchasers and providers. London: HEA.
HEA, 1997a. Physical activity ‘from our point of view’: qualitative
research among South Asian and black communities.
London: HEA.
HEA, 1997b. Guidelines: promoting physical activity with people
with disabilities. London: HEA
HEA, 1998a. Young and active? Young people and health enhancing
physical activity: evidence and implications. London: HEA.
HEA, 1998b. Guidelines: promoting physical activity with older people.
London: HEA.
HEA, 1998c. Transport and health: a briefing for health professionals
and local authorities. London: HEA
HEA, 1999a. Physical activity and inequality: a briefing paper.
London: HEA.
HEA, 1999b. Making THE links: integrating sustainable transport, health
and environment policies: a guide for local authorities and health
authorities. London: HEA.
Coronary heart disease: guidance for implementing the preventive aspects of the NSF
54

HEA, 1999c. Active transport: a guide to the development of local
initiatives to promote cycling and walking. London: HEA.
HEA, 2000. Health and lifestyle survey. London: HEA.
Hillsdon, M., Thorogood, M. and Foster, C., 1999. A systematic review
of strategies to promote physical activity. In: D. MacAuley, ed. Benefits
and hazards of exercise, Vol. 1. London: British Medical Journal
Publications, 25–46.
House of Commons, 1996. Risk reduction for vulnerable road users,
Transport Committee, third report. London: The Stationery Office.
Joint Surveys Unit, 1999. Health survey for England, 1998.
London: The Stationery Office.
Killoran, A., Fentem, P. and Caspersen, C., eds., 1995. Moving on:
international perspectives on promoting physical activity. London: HEA.
Marcus, B.H., Owen, N., Forsyth, L.H., Cavill, N.A. and Fridinger, F.,
1998. Interventions to promote physical activity using mass media,
print media and information technology. American Journal of
Preventive Medicine, 15, 362–378.
Morris, J. N. and Hardman, A. E., 1997. Walking to health. Sports
Medicine, 23, 306–332.
Mulvihill, C., Rivers, K. and Aggleton, P., 2000. Views of young
people towards physical activity: determinants and barriers to
involvement. Health Education, 100, 190–199.
Mutrie, N., Blamey, A. and Whitelaw, A., 1999. A randomised
controlled trial of a cognitive behavioural intervention aimed at
increasing active commuting in a workplace setting. Edinburgh:
Chief Scientist’s Office of the Scottish Executive.
NHF, 1995. Physical activity: an agenda for action. London: NHF.
NHF, 1999. Looking to the future: making CHD an epidemic of the past.
London: The Stationery Office.
NHSS, 2000. National Healthy Schools Standard: physical activity. London: HDA.
Pieron, M., Cloes, M., Delfosse, C. and Ledent, M., 1996. An
investigation of the effects of daily physical education in kindergarten
and elementary schools. European Physical Education Review, 2, 116–132.
Powell, K.E. and Blair, S.N., 1994. The public health burdens of
sedentary living habits: theoretical but realistic estimates. Medicine and
Science in Sports and Exercise, 26, 851–856.
Riddoch, C., Puig-Ribera, A. and Cooper, A., 1998. Effectiveness of
physical activity promotion schemes in primary care: a review.
London: HEA.
Sallis, J.F., Hovell, M.F., Hofstetter, C.R., Elder, J.P., Hackley, M.,
Casperson, C.J. and Powell, K.E., 1990. Distance between homes and
exercise facilities related to frequency of exercise among San Diego
residents. Public Health Reports, 105, 179–185
Sallis, J.F., Nader, P.R., Broyules, S.L., Berry, C.C., Elder, J.P., McKenzie,
T.L. and Nelson, J.A., 1993. Correlates of physical activity at home in
Mexican-American and Anglo-American pre-school children. Health
Psychology, 12, 390–398.
Shephard, R.J., Jequier, J.-C., Lavallee, H., La Barre, R. and Rajic, M.,
1980. Habitual physical activity: effects of sex, milieu, season and
required activity. Journal of Sports Medicine, 20, 55–66.
Shephard, R.J., 1990. Costs and benefits of an exercising versus a
non-exercising society. In: C. Bouchard, R.J. Shephard, T. Stephens,
J.R. Sutton and B.D. McPherson, eds. Exercise, fitness and health.
Champaign, IL: Human Kinetics, 1990, 49–60.
Simons-Morton, D.G., Calfas, K.J., Oldenburg, B. and Burton, N., 1998.
Effects of interventions in health care settings on physical activity or
cardiorespiratory fitness. American Journal of Preventive Medicine,
15, 413–430.
Transport 2000, 1998. Healthy transport toolkit. London: Transport 2000.
US Department of Health and Human Services, 1996. Physical activity
and health: a report of the Surgeon General. Atlanta: US Department of
Health and Human Services, Centers for Disease Control and Prevention.
Vuori, P. and Oja, P., 1999. The health potential of physical
activity through transport by walking and cycling: a scientific review
prepared for the charter on transport, environment and health.
Copenhagen: WHO.
Walters, R., Cattan, C., Speller, V. and Stuckelberger, A., 1999. Proven
strategies to improve older people’s health: a Eurolink Age report for
the European Commission. Brussels: Eurolink Age.
Webster, D.C. and Mackie, A.M., 1996. TRL report 215: review of traffic
calming schemes in 20mph zones. Wokingham: Transport and Road
Research Laboratory.
WHO/Federation of Sports Medicine, 1995. Exercise for health:
WHO/FIMS committee on physical activity for health. Bulletin of the
World Health Organization, 73 (2), 135–136.
Increasing physical activity
55

WHO, 1996. Guideline series for healthy ageing: No. 1. The Heidelberg
Guidelines for promoting physical activity among older persons.
Geneva: WHO.
WHO, 1998. Walking and cycling in the city, LAs, health and
environment briefing pamphlet series no. 35. Copenhagen: WHO
Regional Office for Europe.
Coronary heart disease: guidance for implementing the preventive aspects of the NSF
56

4.1 Introduction
The prevalence of overweight and obesity has increasedin the United Kingdom in recent decades (see Box 4.1).The incidence of CHD is highest in obese men andwomen, especially in those under 50 years old. There is agraded, increased risk of cardiovascular and totalmortality in people with a body mass index (BMI) over 25kg/m2 (Nutrition and Physical Activity Task Forces 1995).Approximately 75% of non-insulin dependent diabeticpatients are overweight (Jung 1997). In women, a weightgain of about 10 kg can lead to a threefold increased riskof developing diabetes (Jung 1997). Women with a BMIover 35kg/m2 (compared with a BMI of 22 kg/m2) have a93 times higher risk of diabetes and men have a 42-foldincreased risk (Jung,1997).
Obesity in childhood is on the increase and predictsadolescent obesity and adult obesity (Parsons et al. 1999).Adolescent obesity is associated with an increased risk ofadult mortality and morbidity (Epstein 1995). Children aremore likely to be obese if they have an obese parent.
There are critical periods in the life course where weightgain is more likely. In women these are between the agesof 15 and 19 years, after marriage, pregnancy, themenopause and retirement. In men the categories arebetween ages 35 and 40 years, after marriage and afterretirement.
Although the causes of obesity are varied, energy intakeexceeds energy expenditure for weight gain to occur. Major weight gain tends not to occur over the short-term,and an energy imbalance of only 1–2% per day can leadto the trend towards overweight and obesity seen in theUK over the years. Daily energy consumption hasdecreased by approximately 20% since 1970, but obesity has increased over this period of time (Prenticeand Jebb 1995). The number of hours spent watching TV has increased since the 1960s and a more automated lifestyle (domestic appliances, use of a motor car) eliminates the amount of physical activityincorporated into daily life. The population is moresedentary with the result that the amount of energyexpended has reduced. The prevalence of obesity is
Chapter 4Reducing overweight and obesity
Reducing overweight and obesity
Box 4.1 Prevalence of overweight and obesity
Men % Women %
Overweight (BMI 25–29.9 kg/m2) 45% 33%Obese (BMI >30kg/m2) 17% 20%Overweight or obese aged 16–24 years 27% 28%Overweight or obese aged 55–64 years 74% 69%Over last 10 years, increase in obesity Increase by 50% Increase by 42%
25% of women in unskilled occupation are obese compared with 14% of women in professional jobs.
Source: Petersen et al. (1999)
57

increasing, despite decreasing energy intake (Barlow andDietz 1998).
Losing weight is in itself beneficial to reducing CHD riskbut increased cardiorespiratory fitness should also beencouraged. Normal weight men with low cardiorespiratoryfitness have a greater risk of cardiovascular diseasemortality than overweight or obese men who do nothave low cardiorespiratory fitness (Wei et al. 1999). Seebox 4.2.
4.2 Objectives of weight management
Prevention, identification and treatment of obesity, andsustainability of weight loss after the intervention are allimportant in a weight management strategy.
Specifically:
• To prevent an increase in prevalence of obesity inchildren and adults
• To promote a reduction of obesity in children andadults
• To support weight maintenance in young children andweight loss in children and adults
• To encourage weight maintenance and preventincreases of weight in individuals who havesuccessfully reduced their body weight.
The US National Heart, Lung and Blood Institute (1998) guidelines have suggested that weight loss programmes should aim initially to reduce body weightby 10% from baseline, at a rate of one or two pounds(approximately 0.5–1 kg) a week, for six months. TheScottish Intercollegiate Guidelines Network (SIGN 1996)recommend a period of 12 weeks of weight loss followedby 12 weeks of weight stabilisation in order for energyexpenditure to readjust.
US guidelines for the evaluation and treatment of obesity in children (Barlow and Dietz 1998) recommendthat children with a BMI greater than or equal to the85th percentile with complications of obesity or with aBMI greater than or equal to the 95th percentile, with orwithout complications, should undergo evaluation andpossible treatment.
Determinants of weight and weight gain aremultifactorial (Sherwood et al. 2000). The Pound ofPrevention study concluded that exercise, fat intake and total energy intake all contribute to successful long-term control of body weight (Sherwood et al. 2000).Energy consumption must be reduced. High calorie/lowvolume foods should be avoided and replaced with anincrease in complex carbohydrates (such as whole grainfoods) and an increase in fruit and vegetables. A reduced fat intake is also an important element of abalanced healthy diet. See the sections on promotinghealthy eating (Chapter 2), and increasing physical activity (Chapter 3) in this document for further details on the effectiveness of interventions for those risk factors.
4.2.1 Definitions of ‘lifestyle’ weightmanagement interventions
Behavioural therapyCognitive behaviour modification and behavioural skills training to modify eating and physical activity habits to prevent weight regain are often used with dietary therapy.
Coronary heart disease: guidance for implementing the preventive aspects of the NSF
58 Box 4.2 Health benefits of weight reduction
A 10 kg reduction in body weight can lead to thefollowing health benefits:
Mortality >20% fall in total mortality>30% fall in diabetes related deaths>40% fall in obesity-related cancer deaths
Hypertension Approximately 10 mmHg systolic and diastolic blood pressure
Lipids 10% total cholesterol reduction15% low density lipoprotein cholesterol reduction30% triglycerides reduction7% increase in high density lipoprotein cholesterol
Diabetes Fall of 50% in fasting glucose
Source: Jung (1997)

Family therapyBehavioural therapy sessions involve all members of thefamily rather than individual counselling of the affectedmember (to be used in the prevention of obesity inchildren specifically).
Dietary therapyTwo main types of dietary therapy are a low calorie diet(800–1500 kcal daily), and a very low calorie diet (lessthan 800 kcal of energy daily), which usually consists of aprotein-enriched liquid.
Exercise therapyThe primary goal is to move sedentary people into anactive category (even if it is moderate levels of intensity)and to move moderate level individuals into morevigorous levels. Accumulation of daily physical activityshould be the key if 30 minutes at least five times a weekseems unobtainable. (See Chapter 3 on Increasingphysical activity for further information.)
4.3 Features of effective interventions
A number of themes are emerging on what strategies arethe most effective in preventing obesity. These are: toreduce sedentary behaviour in obese children; to use diet,physical activity and behavioural strategies for adults, incombination where possible; and to use maintenancestrategies such as continued therapist contact. A gradual,incremental stepwise approach seems to have the mostbeneficial long-term effect. Evidence for the effectivenessof obesity prevention and treatment is inconclusive(Harvey et al. 2000).
Where possible, the intended target group or geographicarea should be consulted to establish what strategies aremost appropriate and it is important to monitor the impact.Accurate recording of baseline data at the local level andthe establishment of clear objectives can aid this. It isimpossible to measure the impact of an intervention wherethe aims and objectives are too vague and multi-faceted.
The overwhelming evidence is that overweight and obesepeople should be encouraged to integrate changes totheir lifestyle over a longer period of time to maintain thebenefit of initial weight loss (Tremblay et al. 1999). Acombination of decreased food intake and increasedphysical activity is more likely to lead to sustained weightloss (Sherwood et al. 2000).
• A combination of diet and physical activity (inconjunction with behavioural counselling) is probablymore effective in sustaining weight loss than diet orexercise alone in adults. The type of activity does notseem important.
• Family therapy is more effective than conventional diet and exercise in preventing weight gain in children (but not necessarily in treatment of obesity).Family therapy is essential in treatment with youngerchildren.
• Small, sustainable modifications in diet, exercise andcommunication are more effective than restrictivestrategies. With small steps, the family/individual canaccommodate the required lifestyle modifications.
• Maintenance of weight loss interventions (self-helppeer groups, relapse prevention strategies andcontinued therapist contact by phone and mail) mayrequire longer-term contact to promote sustainabilityof weight loss.
Further information is available from Glenny et al. (1997),NHS Centre for Reviews and Dissemination (1997) andEdmunds and Waters (2000). More detail can be found inTable 4.7 at the end of this chapter.
Modest, regular bouts of physical activity can lead tobenefits. The type of exercise is not important and shortbouts of walking can cumulatively be of much benefit.Walking a mile a day for a year is equivalent in energy tothat stored in 3 kg of adipose tissue (DH 1994). Habitualphysical activity can also help keep weight off afterweight loss has been achieved, and can reduce the threat of the post-weight-loss seesaw effect (DH 1994).Generally, it is agreed that the cumulative effect ofphysical activity can benefit weight loss (DH 1994)although this view has been questioned by some(Sherwood et al. 2000).
Very low calorie diets are not advisable in children(Epstein 1995) and they are not effective. In terms ofincreasing children’s physical activity, a more active daily lifestyle should be encouraged rather thanstructured aerobic exercise schedules (Epstein 1995). It appears to be more effective to promote less sedentary lifestyles (with less opportunity to eatexcessively while watching TV, for example) than simply attempt to increase activity.
Reducing overweight and obesity
59

Potential barriers to effective obesity management mayinclude lack of access to appropriate support services,lack of motivation by professionals due to negativeperceptions of overweight and obese people or theefficacy of treatments (Harvey et al. 2000). There is stillvery little information about how clinical practice in aprimary care setting or the organisation of care in thisarea might be improved (Harvey et al. 2000). A workbook has been published by the former HEA to guide health professionals in their weight management strategies (Cowburn and Foster 1998). It provides self-learning advice in counselling approaches.
4.3.1 Skills
A local assessment of the provision of weightmanagement services will be necessary. The PCGs will be carrying out a mapping/profiling exercise. Ifobesity management services are not considered, anequity profile (see p78) should be part of the localassessment. Groups at greater risk of obesity and related CHD illness should be identified and targeted. A local mapping exercise can help achieve this goal(population structure by age, ethnicity, employment and housing status as well as identification of foodsuppliers, access to parks/leisure facilities and specialist centres).
There will be a need for training of the professionals who will be delivering the services (primary care, specialist exercise and nutrition staff). This will involve providing information about what options andservices are available as well as equipping them with the skills to identify, treat and manage ‘at risk’overweight or obese people.
4.4 Reducing inequity
There are socioeconomic and ethnic differences in theprevalence of obesity. There is a higher level of obesity inthe more deprived groups (Gordon et al. 1999). Thisshould be considered when planning obesity preventionand treatment interventions. Studies have shown thatweight loss and prevention of weight regain are lesseffective in lower income groups (Jeffery and French1997; Hardeman et al. 2000).
Epidemiological evidence suggests that there are anumber of groups who are most at risk of gainingweight, and subsequently of suffering from co-morbidityassociated with obesity. These groups are:
• South Asians
• African-Caribbeans
• Those living in socially deprived areas
• Smokers planning to stop (need to liaise with smoking cessation planners)
• People with disabilities.
Identification of individuals or groups who are at risk of associated obesity co-morbidities must be anessential element of a strategy to reduce the increasedprevalence of overweight or obesity. Consideration mustbe given to disabled people who may suffer a range ofadditional barriers to managing their weight andparticipating in weight loss programmes. There is noevidence to suggest effective interventions in this area, but training in identifying and prescribing appropriatestrategies must be considered.
Coronary heart disease: guidance for implementing the preventive aspects of the NSF
60

Reducing overweight and obesity
61
4.5 Further information
There is an obesity toolkit available from the Faculty of Public HealthMedicine, Tackling obesity: a toolbox for local partnership action. A numberof interventions are listed by setting (community, home, school andworkplace). It is divided into prevention, and weight management in thetreatment of obesity (Davis et al. 2000). A copy was sent out to all directorsof public health and all health promotion units.
Tel: 020 7935 0243;email: [email protected]
A comprehensive overview of obesity will shortly be available on the web aspart of the Health Care Needs Assessment Series. It covers the epidemiologicaldata, services available and the effectiveness of interventions of theprevention and treatment of obesity in adults and children.
http://hcna.radcliffe-online.com
A directory of projects of weight management compiled by the DH is availablein each regional office. Three main themes emerged: that weight loss israrely maintained, that multicomponent programmes are more successfuland that regular follow up is important (Hughes and Martin 1999) .
The US National Institute of Health’s Clinical guidelines on the identification,evaluation, and treatment of overweight and obesity in adults (NationalHeart, Lung, and Blood Institute 1998) is available on the web. Usefulinformation for healthcare professionals working in obesity treatment andprevention can be located on their website.
http://www.nhlbi.nih.gov/guidelines/obesity/ob_gdlns.htm http://www.nhlbi.nih.gov/guidelines/obesity/ob_home.htm
The appendices in the Clinical guidelines on the identification, evaluation,and treatment of overweight and obesity in adults list a number of usefulstrategies to help treat obesity. Examples of weight goal records, foodsubstitution ideas and food preparation leaflets, guide to behaviouralchange strategies and exercise programmes for gradual build up ofactivity/fitness are included. Consideration should be given to making thisavailable to health professionals.
http://www.nhlbi.nih.gov/guidelines/obesity/practgde.htm
An initiative Shape up America, designed for doctors, nurses, dietitians andother health professionals, has produced guidance on treating obesity. Itincludes ideas for weight gain prevention and weight loss. The appendicesmay be a useful practical toolkit for suggested approaches and includesuggestions for walking (including safety considerations and food diaries).
http://www.shapeup.org/professional/index.html
The US CDC has a report entitled Physical activity and health, which coversthe promotion of physical activity in our daily lives (US Department of Healthand Human Services 1996).
http://www.cdc.gov/nccdphp/sgr/summary.htm
CDC has published a set of guidelines on the promotion of physical activityin children and adolescents, with guidance on the benefits andconsequences of physical activity. There is a separate set of guidelines forthe promotion of healthy eating in schools.
Physical activity:http://www.cdc.gov/nccdphp/dash/physact.htmNutrition:http://www.cdc.gov/nccdphp/dash/nutraag.htm

Coronary heart disease: guidance for implementing the preventive aspects of the NSF
62
Further information (continued)
WHO report Obesity: preventing and managing the global epidemic (1999). The executive summary can beviewed in the publicationssection at http://www.iotf.org/
There are two Cochrane reviews in progress on the prevention andtreatment of obesity in childhood.
Campbell et al. (2000a,b).
A community approach to behavioural change in the promotion of physicalactivity, published by the CDC, is aimed at all those interested in a community-wide strategy (central and local government, transport, health and communityplanners, exercise specialists and health professionals, community groups,businesses, schools, colleges and universities).
Community physical activityapproach:http://www.cdc.gov/nccdphp/dnpa/pahand.htm
The International Obesity Task Force (IOTF) has a web site with many linksto obesity related sites.
http://www.iotf.org/

Reducing overweight and obesity
63
Tabl
e 4.
6Su
gges
ted
acti
viti
es t
o su
ppor
t lo
cal a
ctio
n
Com
mun
ity
Inte
rven
tion
Evid
ence
Ou
tco
me
Skill
s an
d r
eso
urc
esPo
ints
to
co
nsi
der
Furt
her
info
rmat
ion
Indi
vidu
al w
eigh
tm
anag
emen
tin
tegr
ated
wit
hpo
pula
tion
inte
rven
tion
s
Indi
vidu
al s
trat
egie
s m
ay b
e m
ost
effe
ctiv
e al
ongs
ide
wid
eren
viro
nmen
tal i
nter
vent
ions
(Jef
fery
1995
; Nes
tle a
nd J
acob
son
2000
).
Incr
ease
in a
cces
sible
and
safe
set
tings
for
the
prom
otio
n of
phy
sical
act
ivity
;gr
eate
r ac
cess
to
affo
rdab
lean
d he
alth
y fo
od o
ptio
ns.
Aw
aren
ess
of t
heco
mpl
exiti
es in
the
aet
iolo
gyof
obe
sity
and
anun
ders
tand
ing
of t
he
mul
tifac
toria
l app
roac
h to
redu
cing
obe
sity.
Mas
s m
edia
has
lim
ited
shor
t-te
rm im
pact
on
phys
ical
activ
ity p
artic
ipat
ion
but
may
have
an
impa
ct in
enco
urag
ing
a cl
imat
e of
chan
ge (C
avill
1998
).
Smal
l but
ste
ady
chan
ge in
die
t an
dac
tivi
ty
Wei
ght
loss
abo
ut 1
–2 lb
/wee
k fo
ra
perio
d of
six
mon
ths.
In t
helo
nger
ter
m, w
eigh
t lo
ss c
an b
em
aint
aine
d. W
omen
who
did
som
efo
rm o
f m
oder
ate
exer
cise
on
are
gula
r ba
sis g
aine
d w
eigh
t m
ore
slow
ly t
han
thos
e w
ho w
ere
less
activ
e (S
herw
ood
et a
l. 20
00).
Wei
ght
redu
ctio
n by
abo
ut10
% o
f ba
selin
e w
eigh
t;pr
even
tion
of r
elap
se t
opr
evio
us w
eigh
t le
vel.
Skill
in e
ncou
ragi
ng p
atie
nts
who
may
bec
ome
disil
lusio
ned
with
slo
w lo
ss.
Ther
e is
cum
ulat
ive
bene
fit in
freq
uent
, but
sho
rt s
pells
of
phys
ical
act
ivity
.
Com
bine
die
t,ph
ysic
al a
ctiv
ity
and
beha
viou
ral
ther
apy
A c
ombi
natio
n of
inte
rven
tions
ism
ost
effe
ctiv
e (C
linic
al E
vide
nce
2000
). Ev
iden
ce s
ugge
sts
that
effe
cts
are
shor
t te
rm.
Impr
oved
link
s be
twee
nle
isure
fac
ilitie
s, c
ater
ers,
LA
san
d H
As.
Regu
lar
mee
tings
bet
wee
ndi
ffer
ent
sect
ors
will
be
requ
ired.
Iden
tify
lead
per
son
or o
rgan
isatio
n.
Freq
uent
ong
oing
con
tact
issu
gges
ted
to h
elp
mai
ntai
nth
e be
nefit
s.
Wh
o c
ou
ld b
ein
volv
ed?
HA
s, e
duca
tion
sect
or, l
ocal
envi
ronm
ent
plan
ners
.
Prim
ary
care
tea
m,
diet
itian
s,be
havi
oura
lth
erap
ists.
Nut
ritio
n an
dph
ysic
al a
ctiv
ityex
pert
s.

Coronary heart disease: guidance for implementing the preventive aspects of the NSF
64
Inte
rven
tion
Seco
ndar
ypr
even
tion
insc
hool
s
Use
‘who
le s
choo
l’ap
proa
ch (G
oran
et
al. 1
999;
Sto
ry19
99).
Prim
ary
prev
enti
onin
sch
ools
Use
‘who
le s
choo
l’ap
proa
ch.
Supp
orti
ve a
ndre
spec
tful
app
roac
h
Evid
ence
Abo
ut a
10%
mea
n re
duct
ion
inov
erw
eigh
t w
as r
epor
ted
(Sto
ry19
99).
Youn
ger
(pre
-ado
lesc
ent)
inte
rven
tions
wer
e m
ore
succ
essf
ul.
This
resu
lt w
as b
ased
on
a sh
ort-
term
fol
low
up
(mos
tly le
ss t
han
sixm
onth
s).
App
roac
h sh
own
to b
e ef
fect
ive
(Sto
ry 1
999)
.
Qua
litat
ive
inte
rvie
ws
of U
S ch
ildre
n(S
tory
199
9); i
ncre
ased
adh
eren
ce if
appr
oach
ed in
a s
ensit
ive
man
ner.
Prev
ent
incr
ease
s in
wei
ght
inal
read
y ov
erw
eigh
t ch
ildre
n.
Prev
ent
beco
min
g ov
erw
eigh
tor
obe
se.
Build
sel
f-co
nfid
ence
and
sel
fes
teem
.
Skill
s an
d r
eso
urc
es
Acc
ess
to g
yms
and
play
ing
field
s. C
hild
ren
can
eat
up t
otw
o m
eals
per
day
in s
choo
ls;fa
mili
es a
re n
ot t
o in
cur
the
cost
(Gor
an e
t al
. 199
9).
Will
req
uire
tra
ined
you
thco
unse
llors
/die
titia
ns.
Poin
ts t
o c
on
sid
er
Nee
d lo
nger
-ter
m d
ata
to s
eew
heth
er w
eigh
t lo
ss c
an b
esu
stai
ned.
Pot
entia
l har
mfu
lef
fect
s (s
tigm
atisa
tion,
eat
ing
diso
rder
s, la
belli
ng) m
ayre
sult.
Pot
entia
l fra
mew
ork
for
PSH
E.
Prov
ide
a cu
ltura
llyap
prop
riate
inte
rven
tion;
incl
ude
clas
sroo
m h
ealth
educ
atio
n cl
asse
s; p
oten
tial
fram
ewor
k fo
r PS
HE.
Be a
war
e of
adv
erse
psyc
holo
gica
l im
pact
.
Furt
her
info
rmat
ion
Mor
e in
form
atio
n on
you
ngpe
ople
’s a
ttitu
des
to d
iet,
heal
th a
nd e
xerc
ise c
an b
efo
und
at:
http
://w
ww
.ex.
ac.u
k/~d
regi
s/Pu
bs/y
p98.
htm
l
A s
umm
ary
of t
he s
ide
effe
cts
of t
reat
men
t in
child
ren
can
be f
ound
in(E
pste
in e
t al
. 199
8).
A s
yste
mat
ic r
evie
w o
nhe
alth
pro
mot
ion
in s
choo
lsis
avai
labl
e (L
ister
-Sha
rpet
al. 1
999)
. It
can
also
be
acce
ssed
on
the
Web
:ht
tp://
hta.
nhsw
eb.n
hs.u
k
Ou
tco
me
Wh
o c
ou
ld b
ein
volv
ed?
Scho
ol n
urse
s,te
ache
rs, c
ouns
ello
rs,
loca
l hea
lthy
scho
ols
prog
ram
me.
Scho
ols
LAs,
foo
d se
ctor
,le
isure
fac
ilitie
sm
anag
ers,
tea
cher
s,sc
hool
bas
edco
unse
llors
, you
thw
orke
rs/y
outh
clu
bs,
pare
nts,
loca
l hea
lthy
scho
ols
prog
ram
me.
Teac
hers
, sch
ool
base
d co
unse
llors
,pa
rent
s, lo
cal h
ealth
ysc
hool
s pr
ogra
mm
e.

Reducing overweight and obesity
65
Inte
rven
tion
The
‘Sto
plig
ht D
iet’
for
trea
tmen
t of
pre-
adol
esce
ntch
ildre
n
It ha
s ‘re
d’ f
oods
for
best
avo
ided
, ‘am
ber’
for
food
s th
at c
an b
eea
ten
in m
oder
atio
nan
d ‘g
reen
’ for
ple
ntifu
l.
Regu
lar
daily
acti
vity
in c
hild
ren;
com
bine
die
t an
dex
erci
se
Enco
urag
e le
ssse
dent
ary
leis
ure
tim
e
Fam
ily g
roup
sess
ions
wit
hdi
etar
y ad
vice
, and
regu
lar
visi
ts t
o G
P
Evid
ence
Youn
ger
child
ren
achi
eved
bet
ter
wei
ght
loss
, and
mai
nten
ance
of
loss
(Eps
tein
et
al. 1
998)
.
Inte
grat
ing
regu
lar
activ
ity in
to d
aily
life
is m
ore
effe
ctiv
e th
an s
truc
ture
dae
robi
c ex
erci
se. T
he e
ffec
t w
asm
aint
aine
d at
a t
wo
year
fol
low
up
(Eps
tein
et
al. 1
998)
.
Tria
l of
redu
cing
TV
wat
chin
gre
sulte
d in
dec
reas
ed a
dipo
sity
(Rob
inso
n 19
99).
Tria
l of
a re
war
dsy
stem
for
dec
reas
ing
sede
ntar
ybe
havi
our
show
ed a
red
uctio
n in
perc
enta
ge o
verw
eigh
t (E
pste
in e
tal
. 199
5).
Prev
ente
d pr
ogre
ssio
n to
sev
ere
obes
ity in
ado
lesc
ence
in 1
0- a
nd11
-yea
r-ol
ds (F
lodm
ark
et a
l. 19
93),
but
no d
iffer
ence
at
one-
year
fol
low
up.
A t
rial w
ith a
10-
year
fol
low
up
show
ed t
hat
invo
lvem
ent
of p
aren
tan
d ch
ild w
as m
ost
effe
ctiv
e(E
pste
in e
t al
. 199
8). I
nclu
sion
ofm
aste
ry e
lem
ent
(taki
ng c
ontr
ol o
fow
n be
havi
ours
) and
use
of
rew
ards
wer
e fo
und
to b
e m
ore
effe
ctiv
e in
red
ucin
g w
eigh
t in
child
ren.
Wei
ght
loss
; mod
ifica
tion
ofea
ting
and
exer
cise
beha
viou
rs.
Regu
lar
phys
ical
act
ivity
inda
ily li
fe b
ecom
es t
he n
orm
.
Incr
ease
d ac
tivity
and
less
‘sna
ckin
g’ t
ime.
Enco
urag
e ch
ange
s in
habi
tual
life
styl
e by
all
fam
ilym
embe
rs.
Skill
s an
d r
eso
urc
es
Leaf
lets
on
diet
s.
Educ
atio
n fo
r pa
rent
s an
dch
ildre
n w
ill b
e re
quire
d.
Teac
hers
to
expl
ain
how
to
be s
elec
tive
in c
hoic
e of
TV
wat
chin
g; le
afle
ts t
o pa
rent
sab
out
reco
rdin
g ch
ild’s
activ
ities
; TV
mon
itorin
gbo
xes
coul
d be
con
sider
ed.
Poin
ts t
o c
on
sid
er
Ensu
re t
he c
hild
has
adeq
uate
nut
ritio
n fo
rgr
owth
. Mon
itor
psyc
holo
gica
l im
pact
on
child
ren.
Safe
ty is
sues
with
loca
l urb
anpl
anne
rs a
nd r
ecre
atio
nal
divi
sion
to e
nsur
e sa
fe p
lay
area
s.
Long
-ter
m o
utco
me
not
yet
know
n.
One
stu
dy s
how
s th
at if
the
child
and
par
ent
are
coun
selle
d se
para
tely
, bet
ter
wei
ght
loss
is a
chie
ved.
Bot
har
e in
volv
ed in
the
pro
cess
,bu
t ar
e se
en a
part
.
Self-
mon
itorin
g an
d go
alse
ttin
g pr
aise
are
sug
gest
ed.
Gra
dual
beh
avio
ural
the
rapy
over
a lo
nger
per
iod
of t
ime
had
a be
tter
long
-ter
m e
ffec
tth
an in
tens
e se
ssio
ns (E
pste
inet
al.
1998
).
Furt
her
info
rmat
ion
Epst
ein,
L.H
. and
Squ
ires,
S.S.
, 199
8. T
he S
topl
ight
Die
t fo
r ch
ildre
n. B
osto
n,M
A: L
ittle
, Bro
wn
and
Co.
BHF
leaf
lets
for
par
ents
: Get
kids
on
the
go:
http
s://w
ww
.bhf
.org
.uk/
publ
icat
ions
/upl
oade
d_pd
fs/a
ctiv
echi
ldre
n.pd
f
Ou
tco
me
Wh
o c
ou
ld b
ein
volv
ed?
Scho
ol b
ased
hea
lthca
rers
(die
titia
ns a
ndsc
hool
nur
ses)
, PE
teac
hers
, fam
ily.
Child
ren
Scho
ol, p
hysic
aled
ucat
ion
(PE)
teac
hers
, exe
rcise
spec
ialis
ts, f
amily
,lo
cal p
arks
and
recr
eatio
n ar
eas;
loca
l hea
lthy
scho
ols
prog
ram
me.
Pare
nts,
tea
cher
s,yo
uth
wor
kers
, loc
alhe
alth
y sc
hool
spr
ogra
mm
e.
Cou
nsel
ling
serv
ices
,di
etiti
ans,
PC
Gs,
scho
ol n
urse
s.

Coronary heart disease: guidance for implementing the preventive aspects of the NSF
66
Inte
rven
tion
Indi
vidu
alis
edad
vice
and
ris
kas
sess
men
t
Prov
ide
regu
lar
follo
w u
p co
ntac
t.
Exer
cise
as
inte
gral
part
of
inte
rven
tion
Enco
urag
e fr
iend
san
d fa
mily
to
acco
mpa
nypa
rtic
ipan
t (m
aybe
abu
ddy
sche
me
whe
repa
rtic
ipan
ts c
an li
nkup
with
ano
ther
mem
ber
of t
hegr
oup)
.
Ener
gy-r
estr
icte
ddi
et (
1,00
0–2,
000
kcal
/day
) ra
ther
than
fat
res
tric
ted
diet
(22
–26
g/da
y)
Spec
ialis
t w
eigh
tlo
ss c
linic
wit
hin
aG
P pr
acti
ce
Evid
ence
Gro
up s
essio
ns a
ppea
red
mor
eef
fect
ive
(Hug
hes
and
Mar
tin 1
999)
.Su
stai
ned
wei
ght
loss
in p
rimar
yca
re s
ettin
gs is
unc
omm
on (H
ughe
san
d M
artin
199
9).
Mod
erat
e (s
hort
-ter
m) e
ffec
ts o
fpr
imar
y ca
re b
ased
cou
nsel
ling
and
inte
rven
tions
tai
lore
d to
par
ticul
arne
eds
with
writ
ten
mat
eria
ls ha
d a
stro
nger
eff
ect
(Eak
in e
t al
. 200
0).
Rand
omise
d co
ntro
lled
tria
l (RC
T)sh
owed
gre
ater
wei
ght
loss
in t
heen
ergy
res
tric
ted
diet
, at
18 m
onth
follo
w u
p (C
linic
al E
vide
nce
2000
).
A w
eekl
y cl
inic
(with
a h
ealth
visit
or) a
chie
ved
wei
ght
loss
eve
n at
a on
e-ye
ar f
ollo
w u
p; 3
3%ac
hiev
ed a
10%
wei
ght
redu
ctio
nan
d 6%
mai
ntai
ned
this
loss
at
one
year
(Sle
ath
1999
).
App
ropr
iate
ly t
ailo
red
inte
rven
tions
for
par
ticul
argr
oups
lead
to
bett
erco
mpl
ianc
e an
d ef
fect
ive
outc
omes
; can
be
used
for
high
er r
isk g
roup
s su
ch a
set
hnic
min
ority
or
disa
bled
grou
ps.
Incr
ease
d ac
tivity
as
part
of
ever
yday
livi
ng; b
ette
rba
lanc
e of
ene
rgy
inta
ke a
ndex
pend
iture
.
Mai
nten
ance
of
wei
ght
loss
thro
ugh
regu
lar
follo
w u
p.
Skill
s an
d r
eso
urc
es
Link
with
loca
l com
mun
itygr
oups
wor
king
with
eth
nic
min
oriti
es; l
angu
age
skill
s,re
cogn
ition
of
cultu
ral a
ndre
ligio
us r
equi
rem
ents
; see
Impr
ovin
g di
et a
nd n
utrit
ion
(Cha
pter
2) f
or in
terv
entio
ns.
Trai
ning
for
prim
ary
care
team
s ab
out
the
role
of
phys
ical
act
ivity
; see
Incr
easin
g ph
ysic
al a
ctiv
ity(C
hapt
er 3
).
Trai
ning
for
hea
lthpr
ofes
siona
ls (s
ee Im
prov
ing
diet
and
nut
ritio
n,
Cha
pter
2).
Room
in t
he p
ract
ice;
tra
inin
gfo
r a
heal
th v
isito
r (w
hich
coul
d be
sha
red
betw
een
prac
tices
in t
he a
rea)
.
Poin
ts t
o c
on
sid
er
Ass
essin
g re
adin
ess
toch
ange
is im
port
ant
whe
nre
com
men
ding
a w
eigh
tre
duct
ion
prog
ram
me
(Die
tz19
99).
Iden
tify
barr
iers
(acc
ess
to a
ffor
dabl
e,nu
triti
ous
food
, chi
ld c
are
arra
ngem
ents
, ope
ning
hou
rsof
fac
ilitie
s).
A m
otiv
ated
coo
rdin
ator
and
supp
ortiv
e te
am m
ay im
prov
eou
tcom
es.
Patie
nts
shou
ld b
e gi
ven
choi
ce o
f ac
tivity
(inc
ludi
ngho
me
base
d) (H
illsd
on 1
998)
.Ex
erci
se r
efer
ral s
chem
es c
anid
entif
y su
itabl
e ca
ndid
ates
and
esta
blish
the
resp
onsib
ilitie
s w
ithin
apr
ogra
mm
e be
twee
n th
epa
rtie
s (H
ughe
s an
d M
artin
1999
), bu
t re
crui
tmen
t an
dad
here
nce
may
be
fairl
y lo
wan
d no
t re
ach
thos
e w
ithm
ost
to g
ain
(Hill
sdon
199
8)
Furt
her
info
rmat
ion
A f
ram
ewor
k ha
s be
ende
velo
ped
that
run
s th
roug
hth
e st
ages
of
prom
otin
gex
erci
se f
or w
eigh
tm
anag
emen
t fr
om a
sses
sing
read
ines
s to
cha
nge
to t
hepr
oces
s of
cha
nge
and
inte
rven
tions
(Bid
dle
and
Fox
1998
).
See
Impr
ovin
g di
et a
ndnu
triti
on (C
hapt
er 2
).
Ou
tco
me
Wh
o c
ou
ld b
ein
volv
ed?
Prim
ary
care
tea
ms,
GPs
, com
mun
itydi
etiti
ans,
com
mun
ity(e
thni
c gr
oup)
link
wor
kers
, hea
lthvi
sitor
s.
Prim
ary
care
leve
l
PCG
s, p
ract
ice
nurs
es, l
eisu
re f
acili
type
rson
nel;
som
ehe
alth
visi
tors
hav
eth
is ro
le.
Die
titia
ns, p
ract
ice
nurs
es.
PCG
, hea
lth v
isito
r,co
mm
unity
die
titia
n.

Reducing overweight and obesity
67
Inte
rven
tion
Freq
uent
con
tact
over
long
ter
m
Prov
isio
n of
hom
eex
erci
se e
quip
men
t
Also
sup
ervi
sed
exer
cise
ses
sions
with
simpl
e be
havi
oura
lth
erap
y (S
BT) a
t on
eye
ar c
ompa
red
with
SBT
and
simpl
eex
erci
se (C
linic
alEv
iden
ce 2
000)
.
Com
mer
cial
wei
ght
loss
pro
gram
mes
Evid
ence
Syst
emat
ic r
evie
w s
how
ed t
hat
any
type
of
freq
uent
con
tact
led
to le
ssw
eigh
t ga
in (C
linic
al E
vide
nce
2000
). In
terv
entio
ns s
houl
d la
st f
orle
ast
six m
onth
s an
d in
corp
orat
eco
ntin
uing
con
tact
to
prev
ent
wei
ght
rega
in (N
atio
nal H
eart
, Lun
gan
d Bl
ood
Inst
itute
199
8). F
ace
tofa
ce c
onta
ct (h
ouse
visi
ts) w
ere
show
n to
be
effe
ctiv
e in
red
ucin
gw
eigh
t re
gain
in o
ne R
CT
(mor
e so
than
pho
ne o
r le
tter
con
tact
)(C
linic
al E
vide
nce
2000
).
Impr
oved
wei
ght
loss
ach
ieve
d w
ithpr
ovisi
on o
f ex
erci
se e
quip
men
t fo
rth
e ho
me
com
bine
d w
ith a
dvic
e on
cont
inuo
us e
xerc
ise (v
ersu
sin
term
itten
t) (C
linic
al E
vide
nce
2000
). Su
perv
ised
exer
cise
ses
sions
(thre
e tim
es a
wee
k fo
r 12
wee
ks)
plus
SBT
was
mor
e ef
fect
ive
inw
eigh
t lo
ss a
t on
e ye
ar, b
ut a
noth
erfo
und
that
sup
ervi
sed
wal
ks o
r a
pers
onal
tra
iner
res
ulte
d in
less
wei
ght
loss
tha
n SB
T al
one
(Clin
ical
Evid
ence
200
0).
Evid
ence
tha
t be
tter
wei
ght
loss
isac
hiev
ed in
gro
up s
ettin
gs (D
avis
etal
. 200
0).
Redu
ce w
eigh
t ga
in.
Cum
ulat
ive
daily
act
ivity
can
be o
f be
nefit
in a
wei
ght
cont
rol p
rogr
amm
e an
d ca
nim
prov
e ad
here
nce
(Jaci
cic
etal
. 199
5).
Impr
ove
psyc
holo
gica
l wel
l-be
ing.
Mak
e th
e pr
oces
s of
losin
g w
eigh
t m
ore
enjo
yabl
e.
Skill
s an
d r
eso
urc
es
Reso
urce
s to
fol
low
up
over
long
er t
ime
perio
d re
quire
d(s
taff
/pho
ne c
alls/
lett
er);
freq
uent
or
long
-ter
m f
ollo
wup
may
req
uire
ext
ra p
ract
ice
reso
urce
s.
Supe
rvise
d se
ssio
ns r
equi
reex
tra
reso
urce
s. L
iaiso
n w
ithle
isure
fac
ilitie
s or
loca
lsu
pplie
rs m
ay m
ake
it ea
sier
to p
rovi
de h
ome
base
deq
uipm
ent
(con
sider
are
ntin
g sc
hem
e?).
Mot
ivat
ed c
lass
lead
er m
aybe
impo
rtan
t.
Poin
ts t
o c
on
sid
er
Self-
help
pee
r gr
oups
, sel
f-m
anag
emen
t te
chni
ques
and
fam
ily o
r sp
ousa
l inv
olve
men
tm
ay a
ll be
of
som
e he
lp(C
linic
al E
vide
nce
2000
).
App
roac
h ca
n en
cour
age
sede
ntar
y pe
ople
to
beco
me
mor
e ac
tive.
Sm
alle
r bo
uts
ofac
tivity
may
app
ear
mor
eat
tain
able
. Aim
to
accu
mul
ate
abou
t 30
min
utes
of a
ctiv
ity p
er d
ay (N
atio
nal
Hea
rt, L
ung
and
Bloo
dIn
stitu
te 1
998)
.
Eval
uatio
n to
ols
for
com
mer
cial
wei
ght
loss
prog
ram
mes
are
nee
ded
(Con
ley
1998
).
Furt
her
info
rmat
ion
Ou
tco
me
Wh
o c
ou
ld b
ein
volv
ed?
GP,
pra
ctic
e nu
rse
orw
eigh
t sp
ecia
list.
Mai
nten
ance
of
wei
ght
loss
Phys
ical
act
ivity
advi
sor,
coun
selli
ngse
rvic
es.

4.7 References
Barlow, S.E. and Dietz, W.H., 1998. Obesity evaluation and treatment:
expert committee recommendations. Pediatrics, 102, E29.
Biddle, S.J.H. and Fox, K.R., 1998. Motivation for physical activity
and weight management. International Journal of Obesity and
Related Metabolic Disorders, 22 (suppl 2), S39–S47.
Campbell, K., Waters E., O'Meara, S. and Summerbell, C., 2000a.
Interventions for preventing obesity in children, protocol for a Cochrane
Review. In: Cochrane Library, Issue 3. Oxford: Update Software.
Campbell, K., Summerbell, C., O'Meara, S. and Waters, E., 2000b.
Interventions for treating obesity in children, protocol for a Cochrane
Review. In: Cochrane Library, Issue 3. Oxford: Update Software.
Cavill, N., 1998. National campaigns to promote physical
activity: Can they make a difference? International Journal of
Obesity and Related Metabolic Disorders, 22 (suppl 2), S48–S51.
Clinical Evidence, 2000. Clinical evidence: a compendium of
the best available evidence for effective health care. London:
BMJ Books.
Conley, R., 1998. The commercial sector: marketing and fitness
responsibly. International Journal of Obesity and Related
Metabolic Disorders, 22 (suppl 2), S55–S58.
Cowburn, G. and Foster, C., 1998. Managing weight: a workbook
for health and other professionals. London: HEA.
Davis, A., Giles, A. and Rona, R., 2000. Tackling obesity: a toolbox for
local partnership action. London: Faculty of Public Health Medicine.
DH, 1994. Nutritional aspects of cardiovascular disease: report of the
cardiovascular review group of the Committee on Medical Aspects of
Food Policy. London: The Stationery Office.
Dietz, W., 1999. How to tackle the problem early? The role of
education in the prevention of obesity. International Journal of Obesity
and Metabolic Disorders, 23 (suppl 4), S7–S9.
Eakin, E.G., Glasgow, R.E. and Riley, K.M., 2000. Review of primary
care-based physical activity intervention studies. The Journal of Family
Practice, 49, 158–168.
Edmunds, L. and Waters, E., 2000. Childhood obesity. In: V.A. Moyer, E.J.
Elliot, R.L. Davis, R. Gilbert, T. Klassen, S. Logan, C. Mellis and K. Williams,
eds. Evidence based pediatrics and child health. London: BMJ Books, 141–153.
Epstein, L.H., 1995. Management of obesity in children. In:
K.D. Brownell and Fairburn, C.G., eds. Eating disorders and obesity.
New York: The Guilford Press, 516–519.
Epstein, L.H., Valoski, A.M., Vara, L.S., McCurley, J., Wisniewski, L.,
Kalarchian, M.A., Klein, K.R. and Shrager, L.R., 1995. Effects of
decreasing sedentary behavior and increasing activity on weight change
in obese children. Health Psychology, 14, 109–115.
Epstein, L.H., Myers, M.D., Raynor, H.A. and Saelens, B.E., 1998. Treatment
of pediatric obesity. International Journal of Obesity and Related
Metabolic Disorders, 101, 554–570.
Flodmark, C.E., Ohlsson, T., Ryden, O. and Sveger, T., 1993. Prevention
of progression to severe obesity in a group of obese schoolchildren
treated with family therapy. Pediatrics, 91, 880–884.
Glenny, A.M., O’Meara, S., Sheldon, T. A. and Wilson, C., 1997.
The treatment and prevention of obesity: a systematic review of the
literature. International Journal of Obesity and Related Metabolic
Disorders, 21, 715–737.
Goran, M.I., Reynolds, K.D. and Lindquist, C.H., 1999. Role of
physical activity in the prevention of obesity in children. International
Journal of Obesity and Related Metabolic Disorders, 23 (suppl 3),
S18–S33.
Gordon, D., Shaw, M., Dorling, D. and Davey Smith, G., eds., 1999.
Inequalities in health: the evidence presented to the independent
inquiry into inequalities in health, chaired by Sir Donald Acheson.
Bristol: The Policy Press.
Hardeman, W., Griffin, S., Johnston, M., Kinmonth, A.L. and
Wareham, N.J., 2000. Interventions to prevent weight gain:
a systematic review of psychological models and behavioural change
methods. International Journal of Obesity and Related Metabolic
Disorders, 24, 131–143.
Harvey, E. L., Glenny, A., Kirk, S.F.L. and Summerbell, C.D., eds.,
2000. Improving health professionals’ management and the
organisation of care for overweight and obese people. Oxford:
Update Software.
Hillsdon, M., 1998. Promoting physical activity: issues in primary health
care. International Journal of Obesity and Related Metabolic Disorders,
22 (suppl 2), S52–S54.
Hughes, J. and Martin, S., 1999. The Department of Health’s
project to evaluate weight management services. Journal of
Human Nutrition and Dietetics, 12, 1–8.
Coronary heart disease: guidance for implementing the preventive aspects of the NSF
68

Jacicic, J.M., Wing, R.R., Butler, B.A. and Robertson, R.J., 1995.
Prescribing exercise in multiple short bouts versus one continuous bout:
effects on adherence, cardiorespiratory fitness, and weight loss in
overweight women. International Journal of Obesity and Related
Metabolic Disorders, 19, 893–901.
Jeffery, R.W., 1995. Public health approaches to the management of
obesity. In: K.D. Brownell and C.G. Fairburn, eds. Eating disorders and
obesity. New York: The Guilford Press, 558–563
Jeffery, R.W. and French, S.A., 1997. Preventing weight gain in adults:
design, methods and one year results from the Pound of Prevention
study. International Journal of Obesity and Related Metabolic Disorders,
21, 457–464.
Jung, R.T., 1997. Obesity as a disease. British Medical Bulletin, 53,
307–321.
Lister-Sharp, D., Chapman, S., Stewart-Brown, S. and Sowden, A.,
1999. Health promoting schools and health promotion in schools: two
systematic reviews. Health Technology Assessment, 3, 1–207.
National Heart, Lung, and Blood Institute, 1998. Clinical guidelines on
the identification, evaluation, and treatment of overweight and obesity
in adults. Bethesda, MD: The Evidence Report, National Institutes
of Health.
Nestle, M. and Jacobson, M.F., 2000. Halting the obesity epidemic:
a public health policy approach. Public Health Reports, 115, 12–24.
NHS Centre for Reviews and Dissemination, 1997. The prevention and
treatment of obesity. Effective Health Care, 3, 1–12.
Nutrition and Physical Activity Task Forces, 1995. Obesity: reversing the
increasing problem of obesity in England. London: DH.
Parsons, T.J., Power, C., Logan, S. and Summerbell, C.D., 1999.
Childhood predictors of adult obesity: a systematic review. International
Journal of Obesity and Related Metabolic Disorders, 23 (suppl 8),
S1–S107.
Petersen, S., Mockford, C. and Rayner, M., 1999. Coronary heart
disease statistics. London: BHF.
Prentice, A.M. and Jebb, S.A., 1995. Obesity in Britain: gluttony or
sloth? British Medical Journal, 311, 437–439.
Robinson, T.N., 1999. Reducing children’s television viewing to prevent
obesity. Journal of the American Medical Association, 282, 1561–1567.
Sherwood, N.E., Jeffery, R.W., French, S.A., Hannan, P.J. and Murray,
D.M., 2000. Predictors of weight gain in the Pound of Prevention study.
International Journal of Obesity, 24, 395–403.
SIGN, 1996. Obesity in Scotland: integrating prevention with weight
management, SIGN Publication No. 8. Edinburgh: SIGN.
Sleath, C., 1999. Can clinically significant weight loss be achieved and
sustained? An evaluation of a general practice based weight control
clinic. Journal of Human Nutrition and Dietetics, 12, 28–31.
Story, M., 1999. School based approaches for preventing and treating
obesity. International Journal of Obesity and Related Metabolic
Disorders, 23 (suppl 7), S43–S51.
Tremblay, A., Doucet, E. and Imbeault, P., 1999. Physical activity and
weight maintenance. International Journal of Obesity and Related
Metabolic Disorders, 23 (suppl 3), S50–S54.
US Department of Health and Human Services, 1996. Physical activity
and health, a report of the Surgeon-General. Atlanta: US Department of
Health and Human Services, Centers for Disease Control and Prevention.
Wei, M., Kampert, J.B., Barlow, C.E., Nichaman, M.Z., Gibbons, L.W.,
Paffenbarger, R.S. and Blair, S.N., 1999. Relationship between low
cardiorespiratory fitness and mortality in normal-weight, overweight,
and obese men. Journal of the American Medical Association, 282,
1547–1553.
WHO, 1999. Obesity: preventing and managing the global epidemic,
Technical Report Series. Geneva: WHO.
Reducing overweight and obesity
69

5.1 Establishing a local CHD implementation team
As outlined in the NSF CHD, every HA should make contact with all local NHS organisations, LAs and other partner agencies to establish animplementation team. This will work on behalf of thelocal health community with members representingrelevant stakeholders, including users and carers (DH2000a, Chapter 3.7, p63). Partnership working, both for strategy development and implementation will be crucial to success.
5.1.1 Milestones and goals
Organisational and health promotion milestones and goals are set out on pp57–60 of the NSF CHD mainreport (DH 2000a). These include responsibilities for NHS organisations and LAs as employers (smokingpolicy, ‘green transport’ policies, and employee-friendlypolicies) and responsibilities for implementing thepreventive aspects of the NSF. In particular, by April 2001 all NHS bodies, working closely with LAs, will have agreed and be contributing to the delivery of local programmes of effective policies (DH 2000a, p57;DH 2000b, p18) on:
• Reducing smoking • Promoting healthy eating• Increasing physical activity• Reducing overweight and obesity.
5.2 Developing local delivery plans
The local implementation team is responsible forproducing a local delivery plan for implementing the NSFCHD. Local delivery plans should be in place and agreedby all the relevant players by October 2000 (DH 2000a,Chapter 3.38, p70).
The key elements of NSF CHD delivery are:
• Identifying service developments – what needs to be done differently?
• Identifying organisational and systems developments – how will the service developments be delivered?
• Professional and personal development – what skillsare needed and who needs them? (DH 2000a, pp64–65).
The NSF CHD should be delivered within the context of the overall HImP and the National PrioritiesGuidance. The plan should be consistent with thedevelopment plan for clinical governance and be reflected within the service and financial frameworks. The plans should also link and be consistent with primarycare investment plans (DH 2000c), and the emerging LAcommunity strategies. Teams should identify other localstrategies and plans to which the delivery plan should belinked and map the contribution that they currently maketo CHD prevention.
Chapter 5Developing a local strategy
Developing a local strategy
73

74
It will be important to consider local plans in the contextof regional health strategies. Box 5.1 identifies localinitiatives which are relevant to CHD prevention.
In order to develop their local implementation plans,teams need to develop partnerships, involve their localcommunities and assess local needs. The planning processfollows a number of key stages as outlined in Figure 1.
5.3 Building effective partnerships
Local implementation of the NSF CHD is intended to be partnership based. There are three broad objectives for local partnerships to prevent CHD:
• improving the coordination and integration of policies (eg integration of the CHD prevention strategy with relevant health and other policies such as health at work and healthy schools policies; environmental, regeneration and leisure policies)
• developing innovative and high quality services by bringing together the contributions and expertise of all partners
• increasing and maximising the financial and other resources available for local services bydeveloping joint ventures between statutoryorganisations, the voluntary sector and the private sector (such as healthy living centre approaches, health at work initiatives).
The development of effective policies and interventions to prevent CHD requires the involvement of the NHS, LAs, voluntary organisations, businesses and the local community in the strategic reshaping of service provision. In many areas this will mean building on alliances and partnerships, which already exist. Existing localpartnerships should be reviewed. They may be able to take on this responsibility, or new partnerships may need to be formed to deliver the NSF locally.
5.3.1 New freedoms to promote and support joint working
New powers to enable HAs and LAs to work together more effectively came into force on 1 April 2000 (DH 2000d). Pooled budgets, integrated provision and lead commissioning are operational flexibilities, which enable services to be developed according to need, irrespective of the boundaries between organisations.
Coronary heart disease: guidance for implementing the preventive aspects of the NSF
Figure 1. Suggested framework for local plans.
Box 5.1 Local plans and initiatives linking to CHD prevention
All areas should include:• HlmP• Primary care investment plans• Community strategy• LA 21/sustainable development/environment
strategy• LTP.
Those areas covered by the following (eg):• HAZ• Healthy cities/health for all• HLCs• School health plans• Sports and leisure strategies• Anti-poverty strategies• Existing health topic strategies• Secondary prevention strategies (including
coronary rehabilitation services, open accesschest pain clinics)
• Regeneration initiatives and plans (eg New Dealfor Communities).

5.3.2 Making the partnership effective
Effective partnership working should include (Geddes1998; Plamping et al. 2000; Watson et al. 2000):
• Leadership and vision – the management anddevelopment of a shared realistic vision for thepartnership’s work through the creation of commongoals
• Involvement and commitment – the commitment oflocal players and particularly the involvement ofcommunities as equal partners. Senior levelcommitment and involvement from NHS, LAs andother partner organisations
• Resources – the contribution and shared utilisation ofinformation, financial, human and technical resources.LAs and HAs should report the proportion of theirbudgets to be given to health promotion, includingheart health promotion (DH 2000b, p15).
Box 5.2 provides examples of a range of people andorganisations who could be involved in different aspectsof CHD prevention.
5.4 Involving local communities
A community development approach enablescommunities to make their own decisions about how toachieve better health for themselves, their families andthe wider community. Professionals are required to act asfacilitators, rather than imposing an agenda on thecommunity. Community development projects do notusually have a focus on disease prevention; however,many address at least one of the lifestyle risk factors forCHD and/or its broader social determinants.
The NSF requires that there is at least one communitydevelopment project with a focus on CHD in one of themost deprived communities in every LA area. Healthvisitors will be a vital resource in securing successfulcommunity development (DH 2000a, p19). HLCs, whichare funded through the NOF, can provide a focus forcommunity development initiatives(http://www.nof.org.uk).
Consulting and involving communities is a key part ofgovernment policy which service providers are required
Developing a local strategy
75
Box 5.2 Who could be involved in the CHD prevention partnership?
From the NHS:• Community Health NHS Trusts• Community nurses, health visitors and midwives• Hospitals and staff• GPs (Local Medical Committee and/or GP Forum)• HAs• Health promotion• Nutrition and dietetic services• Occupational health• Physiotherapy• PCGs/PCTs• Public health• Smoking cessation services• Ambulance trusts• NHS Direct• Community pharmacistsFrom LAs:• Community development• Education• Environmental health• Highways• Housing• Leisure• LA 21• Regeneration and planning• Social care services• Schools• Transport, roads and highways• Youth and community servicesFrom the voluntary sector:• Local voluntary organisations with a remit for CHD
prevention or which address relevant CHD risk factors• Local voluntary organisations who have links with
local target groups (eg groups who work witholder people, black and minority ethnic groups)
From the local community:• Schools and colleges• Groups which work with relevant local target groupsFrom private sector:• Food retailers and local businesses• Medium to large size local employers (for health
at work policies)• Private sector leisure providers• Restaurateurs, caterers and other local food outlets• Private transport companies

to implement and is a key part of many local initiatives (eg NHSE 1998, 1999; DETR 2000). Involving localcommunities in developing strategies and action plansimproves the quality and effectiveness of programmes(Nichols 1999).
Local communities should be actively involved in CHDpartnerships at every stage to include strategy development,action planning, delivery and review and evaluation.
Local people are able to provide insights into the natureof health and social issues and the appropriateness andacceptability of policies and strategies (Rogers et al.1997). Actively involving local communities in needsassessment research processes, ensuring theirrepresentation within planning and managementarrangements and providing training and resources forvolunteers and local networks are key factors for successin initiatives to improve health and well being (Gillies 1998).
5.4.1 Consulting local communities
The Audit Commission (1999) has identified principles ofgood practice in this area. Consultation should:
• Be related to a decision that the organisations intendto take
• Have clear objectives• Be competently carried out• Be inclusive• Be used in practice.
Effective consultation is not easy to achieve. It needs tobe carefully planned, effectively carried out andthoughtfully used. Communities contain many different
interests and interest groups and it is important to try toestablish whom a representative is representing, and towhom in the community the representative is accountable.Findings from community consultations have to bebalanced with other factors such as other stakeholderpriorities, available resources and statutory requirements.There are many different consultation methods, eachwith their own advantages and disadvantages. Theseinclude: meetings, surveys, focus groups, user groups,citizens’ juries, citizens’ panels, neighbourhood fora,youth councils, community visioning/mapping exercises,and participatory appraisal and participatory actionresearch. A broad spectrum of approaches should beused and selection of those which are relevant to thepurpose of the consultation, and suitable for those whoare being consulted, is recommended.
Public participation and consultation occurs at differentlevels, and the degree of control local people experiencerelates to the level of involvement (see Box 5.3).
When planning community consultation it is important to:
• Identify information from consultation that has alreadytaken place through existing initiatives such as LA 21
• Work with other partners to agree a joint approach to consultation and to agree the most appropriatemethods (this will avoid consultation overload, andmake the best use of available resources)
• Present the exercise realistically to avoid raisingunrealistic expectations
• Plan feedback to the participants.
Coronary heart disease: guidance for implementing the preventive aspects of the NSF
76
Box 5.3 Level of involvement
Less involvement High involvement
Source: Audit Commission (1999)
One off polls(eg referendum, publicopinion survey)
Regular surveys of views(eg panel survey)
One off deliberativeexercises(eg citizens’ jury,community visioningevents)
Ongoing consultationgroups(eg neighbourhoodforum)

Once the consultation is completed consider who elsewould find the results useful in planning and deliveringtheir services, and disseminate the findings accordingly.
5.4.2 Developing capacity
To support effective community development andinvolvement, consideration needs to be given to capacitybuilding on three levels (Russell and Killoran 1999):
• Individual development
• Capacity building within local groups (eg throughtraining, support workers, skills development,administrative resources)
• Developing the local community infrastructure.
Capacity building enables individuals in communities to develop knowledge, skills and self-efficacy that mayhelp them to continue to be involved with preventioninitiatives and to sustain programmes and activities within the community.
5.4.3 Engaging ‘excluded’ groups
As a first step it is vital that the implementation team has a clear picture of those who take part. A participation profile may include:
• Demographic analysis (age, ethnicity, gender, disability)
• Geographical breakdown (town, ward, enumerationdistrict)
• Economic background (employment status, occupation).
Comparing this with the profile of the whole populationwill enable the identification of those who are not yetinvolved, and allow efforts to be targeted to includethem. A first step is to ascertain whether there are anyspecific reasons preventing participation, and to addressthem. Reasons may include:
• Language barriers• Time• Lack of awareness of the consultation or project• A feeling that ‘it isn’t for us’.
Implementation teams need to know the composition of their communities and have targets and strategies toensure they are included in the process. Capacity building will be particularly important with groups who are less likely to be involved. A traditionally‘excluded’ group may be an appropriate focus for a community development project.
5.5 Health needs assessment
Assessing local need, and profiling the local community is the first step towards developing a local delivery plan. Different areas will be at differentstages. As part of the HImP and Director of PublicHealth’s Annual Report, many places will have welldeveloped local needs assessment for CHD andcommunity profiles will already have been undertaken. In other places more work will need to be done. LocalPublic Health and Health Promotion experts provide an important resource for local implementation groups.
This guidance concentrates on prevention activities only, but consideration should be given to needsassessment as part of planning the delivery of other parts of the NSF CHD. Needs assessment isintended to inform local plans: to look at unmet need for services and to provide information that will allow services to be tailored to local populations.Successful local strategies to address CHD risk will take a broad approach to needs assessment, involving a wide range of partners and ensuringcommunity involvement.
5.6 Community profiling
A community profile describes the local area in terms of local populations (eg ethnicity, age, gender) and characteristics of the local environment (eg employers and employment; parks and open spaces; housing and estates) of importance in planning local CHD preventionstrategies.
Assessing health needs of the local population involves:
• Defining the different ’segments‘ or target groupswithin their local population
Developing a local strategy
77

• Describing these different groups according to theirneeds and preferences using a variety of data.
Target groups can be distinguished in two ways:
• Geographical groups bound together by locality
• Social groups bound together by some other attribute,such as age, gender, ethnic origin, health status orsocio-economic status (and combinations of these).
Consultation with local communities will identify factors that local people consider are important, which should be included in the profile.
A well developed community profile would include local data (qualitative and quantitative) on the burden of CHD disease, and on risk factors (smoking prevalence, physical activity, diet, and weight);perceptions of health, service and facility provision and use, socio-economic information. Examples of data items to include are presented on p82 on local indicators. Where local data do not exist, riskprofiles may be derived from national data sets (byapplying risk profiles based on the total population to alocality). Consideration should be given to collectingmissing local data, relevant to the local action plan.Sources of local data can be found in Box 5.4. As part ofthe development plan, identify gaps in current data whichneed to be filled to enable better targeting andmonitoring of local implementation.
5.7 Equity profiling
The incidence of CHD is not uniformly distributed among the population. CHD risk is stratified by sex, age, social class, ethnic origin, and region of residence.The NSF highlights the importance of developing a local equity profile, with equity targets. Directors of public health are charged with producing the profile. The equity profile is intended to identify inequalities in heart health and in access to preventive and treatmentservices. It will concentrate on the needs of individualsand groups, especially those for whom specialconsideration is warranted (poorer people, children,pregnant women, women of childbearing age, minority ethnic groups, other vulnerable groups). Theequity profile should identify the inequalities which exist locally in terms of CHD mortality and morbidity. The equity targets are local targets to reduce theseinequalities. As part of the prevention strategy equityprofiling should cover smoking, nutrition, physical activity and weight management, with associated targets.
5.7.1 Audit of current provision
Local needs assessment requires a comprehensive audit of activity relevant to the four areas for prevention (smoking, physical activity, nutrition andoverweight and obesity). An example for physical activity is presented in Box 5.5. This type of audit willallow the identification of gaps and in conjunction with the equity profile, will identify unmet need forinterventions.
5.7.2 Personal and professional development audit
A local skills audit is an important aspect of needsassessment. There will be a need for appropriate personal and professional development for a wide range of people. This will include not just healthprofessionals, but other professional groups involved in planning and delivering services (eg LA officers, teachers, social workers, youth leaders, voluntary sector staff) and members of the public involved in needs assessment and in delivering community-based programmes.
Coronary heart disease: guidance for implementing the preventive aspects of the NSF
78
Box 5.4 Local sources of data
• The annual reports of the Director of PublicHealth
• HlmPs and other local plans and profiles (eg poverty profile)
• LA data sets• Socio-economic data derived from the census• Neighbourhood statistics• Regional data sets (eg health and lifestyle
surveys)• Public health observatories• Local surveys (eg by LAs, HAs and local colleges
or universities)

5.8 Monitoring progress
Monitoring is a review of progress towards goals. To do this it is important to set targets and relatedindicators. Targets are an expression of the goals of theprogramme and indicators track movement towards oraway from them. The NSF CHD identifies priorities and uses milestones, which set out the time by which the recommendations should be implemented. Thesemilestones should be used to set local targets and bereflected in HImPs and other local plans.
The broad performance indicators for CHD fit within theareas of the national Performance Assessment Framework
(PAF) and are designed to track progress. The PAF issummarised in the main NSF document (DH 2000a, p74).There will be additional performance indicators for CHD and these are also set out in the main NSF CHD (DH 2000a, pp81–82). Chapter 1 of the NSF CHDincludes a framework for the preventive aspects of theprogramme, and highlights data items that should becollected locally (DH 2000b, p16). A technical supplement to follow the white paper Saving lives: ourhealthier nation (DH 1999) is currently being drafted andwill set out the scientific basis for target setting and the indicators available for the assessment of progress atboth national and local level. See further sources ofinformation on p88.
Developing a local strategy
79
Box 5.5 Audit of local provision of services and facilities for physical activity
Group/locality
How many? Where? How accessible to group?
FacilitiesSwimming poolsSports facilitiesHealth clubsSchool facilitiesCommunity facilities
Conducive environmentsCycle routes/tracksWalksParks/playing fieldsOther open spaces
Active local groupsSports clubsSports promotion unitsPrimary careHealth promotionLocal resources
Workplace facilities
NHSLALocal business
Source: HEA (1995)

80
5.8.1 Developing local targets
A target is usually expressed numerically (quantitative).Targets should be feasible in the timeframe and berevised according to changes in the policy environment.They should be measurable – that is, it must be possibleto measure them and to collect the required data items.There is a national target for reducing the death ratefrom CHD: stroke and related diseases in people under75 years should be reduced by at least two-fifths by 2010 (DH 1999). The NSF CHD emphasises the need forintervention with other sections of the population such as children and pregnant women that will have an impact on CHD long after the 2010 deadline.
Local targets can be based on national targets for CHDrisk factors, modified to take into account the populationprofile. They can be set in terms of long-term disease risk,risk factors or be focused on areas or groups at particularrisk. Local targets need to take into account past trendsand performance. Baseline measures for the target in questionneed to be collected (although initially, national data canbe adapted while local data are collected). An example,focusing on physical activity, is presented in Box 5.6.
Equity targetsThe government intends to set national targets forreducing inequalities in health (DH 2000c). However, asdiscussed above, local plans should include an equity
Coronary heart disease: guidance for implementing the preventive aspects of the NSF
Box 5.6 Example of local targets for physical activity
*The recommendation is that adults build into their daily routine half an hour of moderate intensity physical activity.
Note: For each target baseline values should be established. If data exist the trend over time should be looked at to
help set achievable targets. Sources of data for measuring progress should be identified, and plans made to collect missing
data items.
Local targets for physicalactivity
Description Example
Long-term disease or healthstatus
Mortality and morbidity A reduction in CHD mortality rates by 32%by 2010
Risk factor Relating to physical activity An increase in the proportion of thepopulation taking the recommendedamount of physical activity* to 45% by 2003(from 37% of men and 25% of women)
Process/Intermediate Policy An increase in the number of employerswith more than 100 employees with aworkplace physical activity policy by 20%by 2003
Groups or areas at particularrisk
A decrease in the proportion ofBangladeshi people who are sedentary(from 52% men and 56% of women to30% by 2005)
Access and delivery An increase in young women from Xlocality accessing leisure services from 10%to 20% by 2004

profile and equity targets. Equity targets should addressthe wider determinants of health and specify the need forlevelling up (Kendall 1998). Those setting equity targetsshould be aware that differential targets may be requiredto take account of differential causes and effects indifferent population groups. Improving the potential forhealth amongst the most vulnerable could mean areduction in services for other sections of the population.
ObjectivesObjectives are the methods used to achieve the targetsand are usually expressed in the form of desired changes.For example, if the aim were to increase access to leisureprovision, objectives could include: to set up a special busservice to take people to facilities; to make facilitiesavailable more cheaply to certain groups; and to increaseopening hours.
IndicatorsIndicators measure the movement towards or away fromobjectives. They are used to assess progress againstbaselines and for comparative purposes. A small numberof indicators will be collated nationally as part of the NSFCHD, but local implementation teams will need to assessperformance using a wider range of appropriate localindicators.
Indicators can be based on the input, process, output andoutcome (Ziglio 1996).
Input measures of resources and action
Process also known as formative or intermediateindicators. These relate to the implementationof the actions defined in the delivery plan.
Output also known as impact indicators. Thesemeasure the immediate impact of the work onits target group.
Outcome also known as summative indicators. Thesefocus on the end product and look at theextent to which the objectives have beenachieved. It is a measure of the long-term goal, such as the improvement in health status.
The NSF CHD notes that most local indicators will relateto inputs and processes where it will be important toassess the level of progress, and where data can beanalysed at a local level. Output indicators can also be
defined and assessed locally. Outcome measures, on thewhole, can be assessed only regionally and nationally,where the numbers will be large enough to show trendsover time (DH 2000a, p77).
All performance indicators should relate to evidence-based changes towards the achievement of the desired outcomes. Not all will be quantifiable. Indicators can be quantitative or qualitative or acombination of the two.
• Quantitative indicators can use standardised measuring instruments to collect data systematicallyover time. The size of the effect can be measured andcompared over time with baselines (Hawe et al. 1990).A list of local sources of data is presented on p78. A CD-ROM resource, Health and lifestyles guide tosources (HEA 1997) is available, which provides anoverview of quantitative health and lifestyle surveys ofsound methodological design available at a nationallevel. It presents details of these surveys, indicatinginformation that could be usefully collected at a locallevel and used to support policy development andplanning.
• Qualitative indicators assess non-quantifiable aspects of the intervention that contributed to its impact.These indicators are generally assessed throughquestionnaires, observational studies, interview studies,focus groups and other forms of communityconsultation. Qualitative indicators can be a series ofcriteria that need to be fulfilled in order for theintervention or programme to be deemed a success or failure.
See boxes 5.7 and 5.8 on p82.
Challenges in setting indicators in public health• Limited data and resources (can lead to availability
driving the indicator rather than the other way around)
• Setting robust indicators for non-quantifiable outputs
• Need to define short-, medium- and long-term goals(health promotion is usually evaluated in the shortterm but the objectives are often long-term)
• Attributing cause and effect – interventions are oftenmulti-agency and multi-intervention
Developing a local strategy
81

• Changes over time may occur for reasons independentof the intervention or there may be a long chain ofevents between intervention and effect.
5.8.2 Monitoring frameworks
A series of monitoring frameworks could be developed asa management tool for project planning. The frameworksshould:
• Enable the identification of the local targets in relationto the national NSF CHD goal
• Specify objectives set as a contribution to the target
• Outline the interventions planned to achieve it
• Derive indicators to monitor change.
Illustrative monitoring frameworks are provided in Table5.9 (pp83–86).
Coronary heart disease: guidance for implementing the preventive aspects of the NSF
82
Box 5.7 Checklist for setting local indicators
• Define target/problem/standard or criteria• Establish aim – defined by clients or institution
concerned with needs/rights• Define who is responsible for the achievement of
the move towards the target• Define whose interventions are you measuring• Set a timeframe – devise framework in which the
indicator is to be targeted• Assess availability and quality of data • Formulate a monitoring system to collect data• Decide on form (eg a rate of change expressed
as a proportion or the setting of a standard as away of assessing the quality of a service orinteraction)
• Set baseline or reference data to standardiseindicator
• Test indicator, if possible, or set date for review
Box 5.8 Examples of indicators used in public health
• Shifts in policies or practices such as policystatements
• Awareness among the public, NHS and LA employees• Access to services, equity• Participation or drop out rate• Levels of client satisfaction • Changes in individual knowledge, awareness and
self efficacy• Changes in behaviour • Health status, quality of life (QOL) and quality
adjusted life years (QALYs) • Community changes (eg decrease in fear of local
crime, reduced levels of racial or sectarian violence)• Environmental changes (eg increase in the
number of cycling routes) • Partnership working (eg evidence of partnerships
with the community and evidence of increasedinvolvement over time, equitable involvement ofdifferent community groups)
• Advocacy (eg unpaid media coverage, policysetting and implementation)
• Quality of services eg interaction between healthprofessional and client
• Quality of life and sustainability indicators (LA 21indicators)

Developing a local strategy
83
NSF
CH
D G
OA
L an
d O
HN
TA
RGET
Con
trib
ute
to t
he t
arge
t re
duct
ion
of d
eath
s fr
om c
ircul
ator
y di
seas
e of
up
to 2
00,0
00 li
ves
in t
otal
by
2010
LOCA
L TA
RGET
bas
ed o
n CO
MA
(19
91, 1
994)
To in
crea
se t
heav
aila
bilit
y of
heal
thie
r fo
odpr
oduc
ts t
o th
elo
cal p
opul
atio
n
OBJ
ECTI
VE
Com
preh
ensiv
e an
d re
gula
rsu
pply
of
frui
t an
d ve
geta
bles
to
all s
ectio
ns o
f th
e po
pula
tion
with
loca
lly o
rgan
ised
initi
ativ
esan
d co
mm
unity
ow
ned
reta
iling
(food
co-
ops)
.
INTE
RVEN
TIO
N
To r
educ
e th
e av
erag
e pe
rcen
tage
of
tota
l foo
d en
ergy
der
ived
by
the
popu
latio
n fr
om s
atur
ated
fat
ty a
cids
to n
o m
ore
than
10%
and
tot
al f
at t
o no
mor
e th
an 3
5% b
y 20
05. T
o in
crea
se t
he c
onsu
mpt
ion
of f
ruit
and
vege
tabl
es t
o fiv
e po
rtio
ns a
day
by
2005
.
Loca
l sur
vey
2000
Obs
erva
tion/
loca
lsu
rvey
Focu
s gr
oups
SOU
RCE
2000
: 54%
2001
: 58%
2002
: 62%
RESU
LT
Perc
enta
ge o
f pe
ople
who
agr
ee t
hat
they
can
fin
d fr
uit
and
vege
tabl
es a
t an
aff
orda
ble
pric
e lo
cally
.
Incr
ease
in a
war
enes
s an
d ac
cess
to
loca
lly g
row
npr
oduc
e fr
om c
omm
unity
allo
tmen
t an
d gr
owin
gsc
hem
es b
y 10
%.
Incr
ease
in p
ropo
rtio
n of
com
mun
ity o
wne
d re
taili
ngsc
hem
es e
stab
lishe
d (e
g, b
asel
ine
2000
: one
in f
ive
loca
litie
s; 2
002:
one
per
loca
lity)
.
Evid
ence
tha
t pe
ople
on
low
inco
mes
fin
d fa
rmer
s’m
arke
ts u
sefu
l.
IND
ICA
TOR
Tabl
e 5.
9Ill
ustr
ativ
e m
onit
orin
g fr
amew
orks
To e
ncou
rage
the
cons
umpt
ion
ofta
sty,
hea
lthy
food
s, in
clud
ing
frui
t an
dve
geta
bles
,am
ong
low
inco
me
grou
ps
Bett
er p
rovi
sion
of a
dequ
ate
nutr
ition
mes
sage
s.Pe
rcen
tage
of
the
loca
l pop
ulat
ion
who
are
abl
e to
sta
teco
rrec
tly a
t le
ast
thre
e of
the
fol
low
ing
way
s of
achi
evin
g a
heal
thie
r di
et: (
1) e
at lo
ts o
f fr
uit,
vege
tabl
esor
sal
ad, (
2) c
ut d
own
on f
atty
or
frie
d fo
ods,
eat
gril
led
food
, (3)
eat
lots
of
fibre
, cer
eals,
who
lem
eal f
ood
and
(4) e
at lo
ts o
f st
arch
y fo
ods
such
as
brea
d, p
otat
oes,
past
a or
ric
e.
Incr
ease
in c
onsu
mpt
ion
of f
ruit
and
vege
tabl
es a
ndst
arch
y fo
ods,
dec
reas
ed c
onsu
mpt
ion
of f
ats
amon
gso
cial
cla
sses
IV a
nd V
.
Prev
ious
nat
iona
lex
ampl
es:
HEM
S (1
996,
199
8)
Nat
iona
l Foo
d Su
rvey
1996
:M
ales
14%
Fem
ales
17%
1998
:M
ales
15%
Fem
ales
17%
Base
:16
–74
year
s ol
d

Coronary heart disease: guidance for implementing the preventive aspects of the NSF
84
NSF
CH
D G
OA
L an
d O
HN
TA
RGET
Con
trib
ute
to t
he t
arge
t re
duct
ion
of d
eath
s fr
om c
ircul
ator
y di
seas
e of
up
to 2
00,0
00 li
ves
in t
otal
by
2010
LOCA
L TA
RGET
To d
evel
op a
‘who
le s
choo
l’ap
proa
ch t
ohe
alth
y ea
ting
OBJ
ECTI
VE
The
scho
ol in
clud
es e
duca
tion
on h
ealth
ier
eatin
g, p
ract
ical
cook
ing
skill
s an
d ba
sic f
ood
safe
ty p
ract
ices
in t
he t
augh
tcu
rric
ulum
.
Polic
y gu
idel
ines
for
eat
ing
heal
thy
snac
ks in
sch
ools.
Prov
ision
of
brea
kfas
t cl
ubs
inse
lect
ed s
choo
ls.
INTE
RVEN
TIO
N
To r
educ
e th
e av
erag
e pe
rcen
tage
of
tota
l foo
d en
ergy
der
ived
by
the
popu
latio
n fr
om s
atur
ated
fat
ty a
cids
to n
o m
ore
than
10%
and
tot
al f
at t
o no
mor
e th
an 3
5% b
y 20
05. T
o in
crea
se t
he c
onsu
mpt
ion
of f
ruit
and
vege
tabl
es t
o fiv
e po
rtio
ns a
day
by
2005
.
Liai
son
with
loca
lhe
alth
y sc
hool
spr
ogra
mm
e co
ordi
nato
r
Aud
it
Feed
back
and
dat
afr
om t
each
ing
staf
f,pu
pils,
cat
erin
g st
aff
and
pare
nts
Obs
erva
tion
Dat
a fr
om L
EAs
and
scho
ols
Obs
erva
tion/
audi
t
SOU
RCE
RESU
LT
An
incr
ease
in t
he n
umbe
r of
sch
ools
with
a p
olic
y on
heal
thy
eatin
g (in
clud
ing
snac
ks) a
t sc
hool
.
Evid
ence
of
revi
ew a
nd e
ffic
ient
use
of
reso
urce
s.
Incr
ease
in n
umbe
r of
sch
ools
selli
ng f
ruit
in t
uck
shop
sto
6–1
1 ye
ar o
lds
and
11–1
6 ye
ar o
lds;
sal
es d
ata:
fru
itas
a p
ropo
rtio
n of
all
snac
k ite
ms
sold
in s
choo
ls.
Evid
ence
tha
t in
itiat
ives
are
sus
tain
able
.
An
incr
ease
in t
he n
umbe
r of
sel
ecte
d sc
hool
s w
hopr
ovid
e br
eakf
ast
club
s; a
n in
crea
se in
the
num
ber
ofsc
hool
child
ren
in s
elec
ted
scho
ols
who
eat
bre
akfa
st;
perc
enta
ge o
f sc
hool
s ad
dres
sing
heal
thy
eatin
g th
roug
ha
‘who
le s
choo
l’ ap
proa
ch.
Qua
lity
of p
rovi
sion
IND
ICA
TOR

Developing a local strategy
85
NSF
CH
D G
OA
L an
d O
HN
TA
RGET
Con
trib
ute
to t
he t
arge
t re
duct
ion
of d
eath
s fr
om c
ircul
ator
y di
seas
e of
up
to 2
00,0
00 li
ves
in t
otal
by
2010
LOCA
L TA
RGET
To r
educ
e th
eim
pact
of
hear
tdi
seas
e an
dst
roke
To in
crea
seaw
aren
ess
of t
heim
port
ance
of
phys
ical
act
ivit
yfo
r ol
der
peop
le
To p
rom
ote
men
tal a
s w
ell
as p
hysi
cal
wel
l bei
ng a
ndre
duce
isol
atio
n
OBJ
ECTI
VE
Impr
ove
com
mun
ity in
volv
emen
tan
d re
latio
ns b
y Su
ppor
t Yo
urN
eigh
bour
hood
sch
eme.
Hom
e ba
sed
prog
ram
me
with
heal
th v
isito
r w
ith t
elep
hone
prom
ptin
g to
enc
oura
ge w
alki
ng(c
heck
eff
ectiv
enes
s)
INTE
RVEN
TIO
N
To im
prov
e th
e he
alth
of
peop
le a
ged
65–7
5 ye
ars
by in
crea
sing
the
leng
th o
f th
eir
lives
and
the
num
ber
ofye
ars
free
fro
m il
lnes
s by
201
0.
Hea
lth S
urve
y fo
rEn
glan
d (a
nnua
l);lo
cal s
urve
y/qu
alita
tive
data
fro
mne
ighb
ourh
ood
fora
.
Cas
e st
udie
s
Hea
lth S
urve
y fo
rEn
glan
d (a
nnua
l)
Loca
l sur
vey
adap
tatio
n of
ques
tions
; H
EMS
(199
8).
SOU
RCE
RESU
LT
Invo
lvem
ent
of o
lder
peo
ple
in p
lann
ing;
pro
port
ion
ofol
der
peop
le w
ho h
elp
out
with
:•
Mea
ls on
whe
els
•D
ay c
entr
es f
or t
he e
lder
ly r
un b
y co
unci
l or
volu
ntar
yor
gani
satio
ns•
Volu
ntar
y or
gani
satio
ns•
Hel
p at
ano
ther
ser
vice
.
Qua
lity
of li
fe m
easu
rem
ent.
Evid
ence
tha
t ol
der
peop
le f
eel a
sen
se o
f co
ntro
l and
invo
lvem
ent
with
initi
ativ
es.
Perc
enta
ge o
f ol
der
peop
le w
ho s
tate
tha
t th
ey a
re a
ble
to e
njoy
day
to
day
activ
ities
.
Perc
enta
ge o
f ol
der
peop
le w
ho f
ind
it di
ffic
ult
to g
etar
ound
the
hou
se o
n th
eir
own.
Perc
enta
ge o
f ol
der
peop
le w
ho h
ave
wal
ks t
hat
last
for
at le
ast
15 m
inut
es b
ut le
ss t
han
30 m
inut
es.
IND
ICA
TOR

Coronary heart disease: guidance for implementing the preventive aspects of the NSF
86
NSF
CH
D G
OA
L an
d O
HN
TA
RGET
Con
trib
ute
to t
he t
arge
t re
duct
ion
of d
eath
s fr
om c
ircul
ator
y di
seas
e of
up
to 2
00,0
00 li
ves
in t
otal
by
2010
LOCA
L TA
RGET
To in
crea
se
the
leve
l of
awar
enes
s am
ong
heal
thpr
ofes
sion
als
onth
e am
ount
and
type
of
phys
ical
acti
vity
nee
ded
for
a be
neft
to
heal
th
Sou
rce:
Ad
apte
d f
rom
Mo
rgan
, A. a
nd
Fo
rd, K
., 19
98.
A s
erie
s o
f h
ealt
h p
rom
oti
on
mo
nit
ori
ng
fra
mew
ork
s fo
r u
se in
dem
on
stra
tin
g c
on
trib
uti
on
to
nat
ion
al t
arg
ets:
a d
iscu
ssio
n
do
cum
ent.
Un
pu
blis
hed
.
To in
crea
se le
vels
of p
hysi
cal
acti
vity
OBJ
ECTI
VE
Prov
ision
of
info
rmat
ion
and
guid
ance
to
prof
essio
nals.
Wal
k in
to
wor
k ou
tin
itiat
ive
(Mut
rie e
t al
.199
9).
Revi
ew o
f lo
cal p
olic
ies/
faci
litie
sth
at e
ncou
rage
phy
sical
act
ivity
;re
com
men
datio
ns f
or a
ctio
n.
INTE
RVEN
TIO
N
Incr
ease
the
pro
port
ion
of t
he lo
cal p
opul
atio
n w
ho a
re p
hysic
ally
act
ive
at a
mod
erat
e in
tens
ity le
vel f
or a
tle
ast
30 m
inut
es o
n fiv
e or
mor
e da
ys o
f th
e w
eek
(from
a lo
cal b
asel
ine)
by
20%
.
Prev
ious
exa
mpl
e:H
EA E
valu
atio
n of
Hea
lth a
nd L
eisu
rePr
ofes
siona
ls 19
95,
1996
, 199
7.
Loca
l sur
vey
data
Loca
l sur
vey
data
LA 2
1 in
dica
tor
info
rmat
ion
Loca
l sur
vey
data
SOU
RCE
%19
9519
9619
97
GP
30
4Pr
actic
enu
rse
23
7Le
isure
wor
kers
3340
42H
ealth
prom
otio
n3
45
RESU
LT
Perc
enta
ge o
f he
alth
pro
fess
iona
ls an
d le
isure
ser
vice
wor
kers
who
cor
rect
ly id
entif
y th
e re
com
men
ded
phys
ical
act
ivity
mes
sage
IND
ICA
TOR
Perc
enta
ge o
f th
ose
invo
lved
in t
he p
rogr
amm
e w
hoco
ntin
ued
to w
alk
to w
ork
afte
r six
mon
ths.
Dec
reas
e in
the
pro
port
ion
of t
he s
eden
tary
loca
lpo
pula
tion
by 5
% f
rom
bas
elin
e of
27%
(men
) and
28%
(wom
en).
An
incr
ease
in t
he p
olic
ies
such
as
pede
stria
n pr
ecin
cts,
allo
win
g bi
cycl
es t
o be
tak
en o
n tr
ains
.
The
num
ber
and
qual
ity o
f ph
ysic
al f
acili
ties
avai
labl
e fo
rph
ysic
al a
ctiv
ity s
uch
as b
ike
trac
ks, w
alki
ng p
aths
,pu
blic
sw
imm
ing
pool
s; in
crea
se in
the
per
cent
age
ofjo
urne
ys m
ade
by w
alki
ng.

5.10 Further sources of information
Partnerships
Advice and information is available from the Health and Social Care
Joint Unit in the Department of Health and information is available at
http://www.doh.gov.uk/jointunit/partnership.htm
Audit Commission, 1998. A fruitful partnership: effective partnership
working. London: Audit Commission (may be ordered on tel: 0800 50
20 30).
Geddes, M., 1998. Achieving best value through partnership. London:
DETR.
NHSE, 1998. Health improvement programmes: planning for better
health and better health care. HSC 1998/167 LAC 98(23). London: NHS.
NHSE, 1999. Planning for health and health care: incorporating
guidance on health improvement programmes, service and financial
frameworks, joint investment plans and primary care investment plans.
HSC 1999/244 LAC 99(39). London: NHS.
Plamping, D., Pratt, J. and Gordon, P., 2000. Practical partnerships for
health and local authorities. British Medical Journal, 320, 1723–1725.
http://www.bmj.com/
Pratt, J., Plamping, D. and Gordon, P., 1998. Partnerships: fit for
purpose?. London: King’s Fund.
Russell, H. and Killoran, A., 1999. Public health and regeneration:
making the links. London: HEA.
Watson, J., Speller, V., Markwell, S. and Platt, S., 2000. The Verona
benchmark: applying evidence to improve the quality of partnership
working. International Journal of Health Promotion and Education, 7,
17–23.
Best value
The Audit Commission publishes a number of reports on best value.
Some of these can be directly accessed through their website:
http://www.audit-commission.gov.uk
Local Government Improvement and Development Agency (IDeA)
has placed many resources relating to best value on line:
http://www.idea.gov.uk
Community and public involvement
Audit Commission, 1999. Listen up! Effective community consultation.
London: Audit Commission (may be ordered on tel: 0800 50 20 30).
Summary and management paper available from:
http://www.audit-commission.gov.uk/ac2ss.first.htm
Useful wallchart included in the main publication but can be obtained
by tel: 020 7828 1212.
Cohen, J. and Emanuel, J., 2000. Positive participation: consulting and
involving young people in health-related work. A planning and training
resource. London: HEA.
DH, 1999. Patient and public involvement in the new NHS.
London: DH. http://www.doh.gov.uk/involve.htm
DETR, 2000. Preparing community strategies: draft guidance to local
authorities from the Department of Environment, Transport and the
Regions. London: DETR.
Local Government Improvement and Development Agency (IDeA) has
placed many resources relating to best value on line. This includes a
document dealing with consultation:
http://www.idea.gov.uk/bestvalue/consult/main.htm
National Consumer Council, Consumer Congress and Service First Unit,
1999. Involving users: improving the delivery of healthcare. London:
Cabinet Office.
National Consumer Council, Consumer Congress and Service First Unit,
1999. Involving users: improving the delivery of local public services.
London: Cabinet Office.
Northern and Yorkshire Region NHS Executive, 1999. NHS primary care
group’s public engagement toolkit. Durham: Northern and Yorkshire
Region NHS Executive.
http://www.doh.gov.uk/pub/docs/doh/toolkit1.pdf
Rifkin, S., Lewando-Hundt, G. and Draper, A., 2000. Participatory
approaches in health promotion and health planning.
London: HDA.
Service First Unit, 1999. An introductory guide: how to consult your
users. London: Cabinet Office.
Service first publications can be found through the Cabinet Office
website: http://www.cabinet-
office.gov.uk/servicefirst/index/publications.htm#policy
Developing a local strategy
87

Health needs assessment
HEA, 1999. Indicators of good practice: an organisational self-
assessment tool. London: HEA.
Sustain, 2000. Reaching the parts. Community mapping: working
together to tackle social exclusion and food poverty. London:
Sustain, in association with Oxfam’s UK Poverty Programme.
Indicators and monitoring
Bowling, A., 1991. Measuring health: a review of quality of life
measurement. Milton Keynes: Open University Press.
Buck, D., Godfrey, C. and Morgan, A., 1997. The contribution of
health promotion to meeting health targets: questions of measurement,
attribution and responsibility. Health Promotion International, 12 (3),
239–250.
Cheadle, A., Sterling, T., Schmid, T. and Fawcett, S., 1995.
Evaluating community based nutrition programmes: comparing
grocery store and individual level survey measures of program
impact. Preventive Medicine, 24 (1), 71–79. The indicators are shown on
http://www.faculty.washington.edu/cheadle/cli/
Funnell, R., Oldfield, K. and Speller, V., 1995. Towards healthier
alliances: a tool for planning, evaluating and developing healthy
alliances. London: HEA.
Hawe, P., Degeling, D. and Hall, J., 1990. Evaluating health
promotion. Sydney: Maclennan and Petty.
Kendall, L., 1998. Local inequalities targets. London: Kings Fund.
Macleod Clark, J., Latter, S., Maben, J. and Franks, H., 1997.
Promoting health through primary health care nursing. London: HEA.
Morgan, A., Buck, D. and Godfrey, C., 1996. Performance indicators
and health promotion targets. York: Centre for Health Economics,
University of York.
Mutrie, N., Blamey, A. and Whitelaw, A., 1999. A randomised
controlled trial of a cognitive behavioural intervention aimed at
increasing active commuting in a workplace setting. Edinburgh: Chief
Scientist’s Office of the Scottish Executive.
Ziglio, E., 1996. Indicators of health promotion policy: directions for research.
In: B. Bandura and I. Kickbush, eds. Health promotion research: towards
a new social epidemiology. Copenhagen: WHO Regional Office for Europe.
The HDA has commissioned the Office for National Statistics to develop
and validate a module of questions to measure a range of components
of social capital. These questions will be used to measure social capital
at a national level in the General Household Survey 2000/2001. The
questions will investigate areas such as the strength of voluntary
organisations, norms of neighbourliness, reciprocity and trust and
infrastructure resources, community networks and attitudes to
community involvement. Some HAZs are using this questionnaire in
their local surveys to enable them to make comparisons between
their local area and the national average. Further information on this
project can be obtained from Antony Morgan (antony.morgan@hda-
online.org.uk) or Caroline Mulvihill (caroline.mulvihill@hda-
online.org.uk) at the HDA.
The National Centre for Health Outcomes Development
(http://nww.nchod.nhs.uk/) provides relevant data and information on
measurement tools for public health. It is a key source of information on
assessment of health and outcomes of health interventions at individual,
HA, Hospital and Community Trust, PCG/PCT and LA levels for the
English NHS and the government. The website contains information on
a range of indicators relevant to CHD, for example fat consumption,
mean adult BMI and smoking statistics.
HEA, 1997. Health and lifestyles: guide to sources. London: HEA.
A technical supplement to follow the white paper, Saving lives: our
healthier nation (DH, 1999), is currently being drafted. It will suggest
some measures of progress to monitor the strategy, draw together
information on data sources, and signpost relevant initiatives and
references which may be helpful to those involved in monitoring
progress at national or at local level. A short draft version is currently
available on the OHN web site, situated at http://www.ohn.gov.uk (look
under ‘OHN’, then ‘Technical’), which will be regularly updated and
supplemented with additional material as appropriate.
StatBase ® http://www.statistics.gov.uk/statbase/mainmenu.asp
StatBase ® is an on-line database which holds a large selection of
Government statistics. It also provides descriptions of all the UK
Government Statistical Service’s data sources, derived analyses, all its
statistical products and services and all the relevant contact points.
Social Exclusion Unit, 2000. Measuring deprivation: a review of indices
in common use.
http://www.cabinet-office.gov.uk/seu/2000/pat18/Depindices.htm
This Working Paper was produced to inform, and support the work of
the Social Exclusion Unit’s Policy Action Team (PAT) 18 on Better
information. It reviews the most commonly used deprivation measures
and highlights some of the issues surrounding their use.
Social Exclusion Unit, 2000. Report of PAT 18: Better information.
London: The Stationery Office.
Coronary heart disease: guidance for implementing the preventive aspects of the NSF
88

OHN indicators
Data to measure progress towards OHN indicators are collected by
local directors of public health. Many of these are also applicable
to the NSF CHD indicators. The OHNiP database:
(http://www.ohn.gov.uk/database/database.htm) holds information on a
wide range of projects and initiatives that in different ways contribute
to the aims of the OHN health strategy. The database can be searched
by health keyword, target audience, government initiative or zone and
setting.
The Health Survey for England has covered cardiovascular disease (1998)
and ethnic minority groups (1999), published by The Stationery Office.
The full text of the CHD survey is available at http://www.official-
document.co.uk/document/doh/survey98/hse-00.htm and information
on the ethnic minority survey is at
http://www.doh.gov.uk/public/hs99ethnic.htm
In 2000 the survey will focus on older people.
Health Education Monitoring Survey (HEMS)
The 1998 HEMS includes a measurement of social capital. The survey
contains six questions whereby a neighbourhood social capital score can
be calculated (Rainford L., Mason V., Hickman M. and Morgan, A.,
2000. Health in England: investigating the links between social
inequalities and health. London: The Stationery Office).
HAZnet: http://www.haznet.org.uk
Evidence is a key feature in the work of HAZs and HAZnet works
towards creating and disseminating an evidence base for new ways
of working. HAZnet has a database of area-based initiatives, local
evaluation projects and other research specific to HAZs, which may
also be of relevance as case studies for the NSF CHD.
LA 21. Local indicators of sustainable development.
http://www.environment.detr.gov.uk/sustainable/localind/nutshell/index.htm
The DETR has recently launched a handbook, Local quality of life counts,
which offers ideas for measuring sustainable development and quality of
life in local communities. The handbook gives a menu of 29 indicators
from which local authorities may wish to consider using a selection for
reporting in their LA 21 and community strategies. A number of these
indicators are also applicable to the NSF CHD. These include 15 headline
indicators that are intended to make up a ‘quality of life barometer’,
which will be used to measure overall progress, including success in
tackling poverty and social exclusion and expected years of healthy life.
The handbook also provides advice on indicator development for:
• Access to key services (i.e. medical services and shops)
• Mode and average distance of travel to work
• Percentage of school children travelling to and from school by
different modes
• Recorded crime per 1,000 population, fear of crime, social
participation, community well being and social and community
enterprises (social capital).
Neighbourhood statistics
Following the recommendations of the Social Exclusion Unit’s Policy
action team 18: better information, a set of standard neighbourhood
statistics covering the social exclusion characteristics of a neighbourhood
will be collated annually. This work will be led by the Office for National
Statistics and will be coordinated across Government departments and
with local government and other public, private and voluntary sector
organisations who collect relevant information so as to avoid duplication
and minimise costs. It is envisaged that this information will be available
down to ward level. Information will be collected within nine suggested
domains which include access to services, community well being/social
environment, crime, economic deprivation, education, skills and
training, health, housing, physical environment and work deprivation.
Evaluation
The HDA has produced a practical toolkit on evaluation. It outlines the
purpose and principles and describes the variety of approaches to
evaluation. In addition it provides guidance on quantitative and
qualitative research methods, developing recommendations and
dissemination of findings. This toolkit will be available on Evidence Base
2000 on the HDA website (http://www.hda-online.org.uk/evidence) in
autumn 2000.
Funnell, R., Oldfield, K. and Speller, V., 1995. Towards healthier
alliances: a tool for planning, evaluating and developing healthy
alliances. London: HEA.
Meyrick, J. and Sinkler, P., 1999. An evaluation resource for healthy
living centres. London: HEA.
Thorogood, M and Coombes, Y., 2000. Evaluating health
promotion: practice and methods. Oxford: Oxford University Press.
5.11 References
Audit Commission, 1999. Listen up! Effective community consultation.
London: Audit Commission.
DETR, 2000. Preparing community strategies: draft guidance to local
authorities from the Department of the Environment, Transport and
Regions. London: DETR.
Developing a local strategy
89

DH, 1999. Saving lives: our healthier nation. London:
The Stationery Office.
DH, 2000a. National service framework for coronary heart disease:
main report. London: DH.
DH, 2000b. National service framework for coronary heart disease:
Chapter 1. Reducing heart disease in the population. London: DH.
DH, 2000c. The NHS plan. A plan for investment. A plan for reform.
London: The Stationery Office.
DH, 2000d. Implementation of Health Act partnership arrangements.
HSC2000/10 LAC2000/09. London: DH.
Geddes, M., 1998. Achieving best value through partnership.
London: DETR.
Gillies, P., 1998. Effectiveness of alliances and partnerships for health
promotion. Health Promotion International, 13 (2), 99–121.
Hawe, P., Degeling, D. and Hall, J., 1990. Evaluating health promotion.
Sydney: Maclennan and Petty.
HEA, 1995. Promoting physical activity: guidance for commissioners,
purchasers and providers. London: HEA.
HEA, 1997. Health and lifestyles: guide to sources. CD ROM.
London: HEA.
Kendall, L., 1998. Local inequalities targets. London: King’s Fund.
NHSE, 1998. Health improvement programmes: planning for
better health and better health care. HSC 1998/167 LAC 98(23).
London: NHS.
NHSE, 1999. Planning for health and health care: incorporating
guidance on health improvement programmes, service and
financial frameworks, joint investment plans and primary care
investment plans. HSC 1999/244 LAC 99(39). London: NHS.
Nichols, V., 1999. The role of community involvement in health
needs assessment in London. London: HEA.
Plamping, D., Pratt, J. and Gordon, P., 2000. Practical partnerships for
health and local authorities. British Medical Journal, 320, 1723–1725.
Rogers, A., Popay, J., Williams, G. and Latham, M., 1997.
Inequalities in health and health promotion: insights from the
qualitative research literature. London: HEA.
Russell, H. and Killoran, A., 1999. Public health and regeneration:
making the links. London: HEA.
Watson, J., Speller, V., Markwell, S. and Platt, S., 2000. The
Verona Benchmark: applying evidence to improve the quality of
partnership working. International Journal of Health Promotion
and Education, 7, 17–23.
Ziglio, E., 1996. Indicators of health promotion policy: directions for
research. In: B. Bandura and I. Kickbush, eds. Health promotion
research: towards a new social epidemiology. Copenhagen: WHO
Regional Office for Europe.
Coronary heart disease: guidance for implementing the preventive aspects of the NSF
90

This guidance has been developed in consultation with a range of professionals through a workshop and criticalreview. The HDA would like to thank them for their cooperation.
Researched and written by
Health Development Agency
Hugo Crombie Public health adviser, physical activity Karen Ford Head of public health advice and learning Caroline Mulvihill Research and development specialist Lesley Owen Public health adviser, smoking Karen Peploe Public health adviser, food and nutritionHilary Whent Head of public health advice and learning Patti White Public health adviser, smoking Tricia Younger Head of action zone development
London School of Hygiene and Tropical Medicine
Dalya Marks Research fellowMargaret Thorogood Reader in public health and preventative medicine
Freelance consultants
Isobel Bowler Health policy consultantLynn Stockley Nutrition consultant
AppendixContributors
Appendix
91

Reviewers
Waqar Ahmad Professor of primary care research, Nuffield Institute, University of LeedsDanila Armstrong Health development manager, NHS Executive, LondonAmanda Avery Community dietitian, Community Nutrition Group, British Dietetic AssociationJanet Baker Deputy regional director of public health, NHS Executive, West MidlandsClive Bates Director, Action on Smoking and HealthYve Buckland Chair, Health Development AgencyJennie Carpenter Head of public health strategy and function in and through the NHS, DHGill Cowburn Senior researcher, Health Promotion Research Group, BHFAdam Crosier Research and development specialist, HDAAliya Darr Research fellow, Nuffield Institute, University of LeedsMike De Silva Policy officer, DHNick Dean Acting head, Health Strategy Branch, DHElizabeth Dowler Public health nutritionist, University of WarwickLaurel Edmunds Senior researcher, Health Promotion Research Group, BHFClaudette Edwards Public health adviser, black and minority ethnic groups, HDACarl Evans CHD/smoke prevention team, DHCharlie Foster Senior researcher, Health Promotion Research Group, BHFMollie Foxall HAZ CHD lead, Manchester Health AuthorityJeff French Director of planning, partnerships and communication, HDAAlison Giles Policy development officer, NHFMadeline Garraway Public health adviser, older people, HDALucy Hamer Development adviser, HImPs, HDALesley Hammond Health promotion officer, Environmental Services Division, Wycombe District CouncilDominic Harrison Regional health development specialist, HDA (northwest region)Nick Hicks Strategy unit team member, DHMelvyn Hillsdon Lecturer in health promotion, London School of Hygiene and Tropical MedicineJane Huntley Head of workplace health, HDAPaul Lincoln Director, NHFRichard Longbottom Senior planning manager, Bradford Health AuthorityJeanette Longfield Coordinator, SustainSusan Martin Deputy branch head PH2, DHAnn McNeill Freelance consultantDawn Milner Senior medical officer, DHAntony Morgan Head of health information, HDAMike Rayner Director, Health Promotion Research Group, BHFSheela Reddy Nutrition division, Food Standards AgencyImogen Sharp Branch head, CHD/stroke prevention, DHDave Shields Health development manager, Southampton City CouncilViv Speller Director of health improvement, HDACathy Stillman-Lowe Public health adviser, oral health, HDACarolyn Summerbell Reader in human nutrition, School of Health, University of TeesideCatherine Swann Research and development specialist, HDAMarilyn Toft Head of schools and young people, HDANikki Wade Health development specialist, Cambridgeshire Health AuthoritySheila Webb Consultant in public health, Bradford Health AuthorityJean Woodhouse Health promotion officer, Northumberland Health AuthorityLynn Young Community health adviser, Royal College of Nursing
Coronary heart disease: guidance for implementing the preventive aspects of the NSF
92

ACoP Approved Code of PracticeAGPNM Association of General Practitioners of
Natural MedicineASH Action on Smoking and Health
BHA British Hypnotherapy AssociationBHF British Heart FoundationBMEG Black and minority ethnic groupsBMI Body mass indexBSH British Society of Hypnotherapists
CA Consumers’ AssociationCDC Center for Disease Control and PreventionCHD Coronary heart diseaseCOMA Committee on the Medical Aspects of Food
and Nutrition Policy
DETR Department of Environment, Transport andthe Regions
DfEE Department for Education and EmploymentDH Department of Health
EAZ Education action zoneEH Environmental healthEHO Environmental health officerEU European Union
FLI Food and low income (database)
GP General practitionerGSL General sales listGTP ‘Green’ transport plan
HA Health authorityHAZ Health action zoneHDA Health Development AgencyHDL High density lipoproteinHEA Health Education Authority
HEMS Health education monitoring surveyHEPA Health-enhancing physical activityHLC Health living centreHlmP Health improvement programmeHSC Health Services CircularHSE Health and Safety Executive
ICM Institute of Complementary MedicineIDeA Improvement and Development AgencyIOTF International Obesity Task Force
LA Local authorityLACA Local Authority Caterers’ AssociationLA 21 Local Agenda 21LDL Low density lipoproteinLEA Local education authorityLGA Local Government AssociationLTP Local transport plan
MAFF Ministry of Agriculture, Fisheries and Food
NGO Nongovernmental organisationNHF National Heart ForumNHS National Health ServiceNHSE National Health Service ExecutiveNHSS National Healthy Schools StandardNOF New Opportunities FundNRT Nicotine replacement therapyNSF National Service FrameworkNSF CHD National Service Framework for Coronary
Heart Disease
OFSTED Office of Fair Standards and Training in Education
OHN Our Healthier NationOHNiP Our healthier nation in practice (database)OTC Over the counter
Glossary
Glossary
93

PAF Performance Assessment Frameworkp&p Postage and packingPAT Policy action teamPCG Primary care groupPCT Primary care trustPE Physical educationPHC Primary health carePR Public relationsPSHE Personal, social and health educationPTA Parent–teacher association
QALY Quality adjusted life yearQOL Quality of life
RCT Randomised controlled trialRDA Regional Development AgencyRPHNutr Registered Public Health Nutritionist
RSA Retail Services Association
SACN Scientific Advisory Committee on NutritionSBT Simple behavioural therapySCOTH Scientific Committee on Tobacco and HealthSIGN Scottish Intercollegiate Guidelines NetworkSMAP School Meals Assessment PackSNAG Schools Nutrition Action GroupSRTS Safer routes to schoolSTAG School travel advisory group
UK United KingdomUSA United States of America
VIRSA Village Retail Services Association
WHO World Health Organization
Coronary heart disease: guidance for implementing the preventive aspects of the NSF
94