Embed Size (px)
Citation preview

Drugs and Alcohol in
Primary Care Steve Brinksman
Clinical Lead SMMGP Medical Director Cranstoun Group
GP

Trends and Issues
• “Traditional” drugs
• Alcohol
• Addiction to Medicines
• Novel Psychoactives
• Prevalence
• Age
• Co-morbidities
• Recovery v Harm Reduction

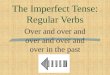
Drugs ordered by their overall harm scores, showing the separate contributions to the overall scores of harms to users and harm to others. The weights after normalisation (0–100) are shown in the key (cumulative in the sense of the sum of all the normalised weights for all the criteria to users, 46; and for all the criteria to others, 54). CW=cumulative weight. GHB=γ hydroxybutyric acid. LSD=lysergic acid diethylamide.
Drug harms in the UK: a multicriteria decision analysis
The Lancet, Volume 376, Issue 9752, Pages 1558 - 1565, 6 November 2010
doi:10.1016/S0140-6736(10)61462-6

Estimates suggest over 300,000 problematic heroin & crack users in the UK
Over 6 billion £s a year spent on illicit drugs in the UK
70% of acquisitive crime drug related
Over a 20 year injecting career, 75% will become infected with hepatitis C
Mortality rates between 6-16x higher than general population

Ageing Populations


Age Effects?

Drug Related Deaths
• There were 3,744 drug poisoning deaths involving both legal and illegal drugs registered in England and Wales in 2016, the highest since comparable records began in 1993.
• Of these, 2,539 (or 69%) were drug misuse deaths involving illegal drugs only.
• The mortality rate from drug misuse was the highest ever recorded, at 65.8 deaths per million population.

Graph showing deaths, comparing untreated patients with those in Methadone maintenance treatment in the Swedish study (2).
(Reproduced from Gronbladh et al)

Role of Primary Care
• Chronic relapsing nature of condition –
patient stays registered whether still using,
on OST or abstinent
• Advantages of primary care treatment,
including continuity and the treatment of
associated health problems
• Familiarity in dealing with complex problems needing behavioural change

“Habit is habit, and not to be flung out of the window by
any man, but coaxed down-stairs one step at a time.”
Samuel Langhorne Clemens

Co-morbiditity
• COPD
• Ischaemic Heart Disease
• Hypertension and CKD
• Liver Disease including Cirrhosis
• Diabetes
• Mental Health
• Poly Drug Use

Engaging users with treatment programmes has been shown to vastly reduce the cost of drug addiction to society in a number of ways: for every £1 spent on drug treatment, there is a saving of £9.50 to society as a whole (Department of Health, 2008).

Reduce barriers to entry
High quality medical and psychosocial services
Treatment retention
Orientation towards social rehabilitation
Sufficient duration of treatment
Detoxification only of willing, well stabilised patients with established abstinence

Recovery as a journey
engagement Reintegration Reducing Harm
Supported Stability
Abstinence
Recovery

Alcohol in the mix
Public Health advises just one glass of wine a day

Alcohol related deaths

The numbers – PHE data
FACTS FIGURES
LAs 152
Inc + High % 22
Dep % 3.8
Practices 8,261
GPs 33,364
ENGLAND LAs PRACTICE GP
Total Population
53,588,218
352,554
6,487
1,606
Adult Population
43,580,873
286,716
5,275
1,306
Dependent
drinkers
1,568,911 10,322
190
47
Increasing and
Higher Risk
9,849,277 64,798
1,192
295
18 Alcohol interventions in Primary Care
13 Alcohol interventions in
Primary Care


Chronic Liver Disease
Key drivers for growth in burden and
mortality, First 3 all preventable:
•Alcohol
•Chronic viral hepatitis B/C
•Obesity
• Non-alcoholic fatty liver disease (NAFLD) leading to
non-alcoholic steatohepatitis (NASH)
•Others – including autoimmune or inherited
• eg Primary Biliary Cirrhosis (PBC), haemochromatosis

Prevalence of HCV Infection
Overall, it is estimated that around 214,000 people (0.4%) in the UK are chronically infected with hepatitis C. Despite being a curable infection only 3% of those infected receive treatment each year.
Hepatitis C in the UK 2013. PHE publications gateway number: 2014058 July 2014

Why Treat Hepatitis C?
Van de Meer et al JAMA 2012

Primary Care has a key role to play
• Prevent transmission
• Increase detection
• Diagnose infection in people who have the disease
• Arrange treatment in those with chronic infection with the aim of eradicating the virus, or at least minimising its effects
• HBV is preventable with an effective vaccine
• With modern therapy, depending on the genotype of HCV up to 95% of patients with chronic HCV can be cured
• Treatment for HCV has been recommended by NICE

Addiction to Medicines

Opioid Analgesics

Opioid deaths mirror prescribing*
•ONS ‘Deaths Related to Drug Poisoning in England and Wales, 2013’ and •‘Prescription opioid abuse in the UK’, Giraudon I et al., British Journal of Clinical Pharmacology 2013
Addiction to medicines policy November 2014 * Not including illicit opioids
“may signal an emerging problem in the UK similar to the issue that is now well established in the USA.”
0
50
100
150
200
250
1993
1995
1997
1999
2001
20
03
2005
2007
2009
2011
2013
Other opiate
Tramadol
Dihydrocodeinenot fromcompound
Codeine notfrom compound

Newer Drugs
Novel Psychoactive Substances, Club Drugs, Legal Highs

Relevance in Primary Care
• Secure environments and homeless -SCRAs [Synthetic Cannabinoid Receptor Agonists]
• LUTS symptoms in young people-Ketamine
• Chemsex-GHB,metamfetamine,ketamine

Public Health v Primary Care
Oh, East is East, and West is West, and never the twain shall meet
Rudyard Kipling

Commissioning
• Role of health and Well Being Board
• Other partners –Third Sector, Police & Crime Commissioners, Social Services, Housing etc.
• Links to Secondary Care Services
• Pathways

Funding Issues
• CCG / Public Health split in some areas
• Competing Priorities
• Drug and Alcohol treatment not part core service for GPs
• However required to work with patients
• Huge impact on hospital admissions

Key Points
• Long term drug use leads to multiple physical and mental health problems and premature ageing
• Patterns of drug use change but remain worryingly high
• Poly drug use is the usual pattern
• Primary Care with support from Secondary Care and the Third Sector can provide effective care and aftercare