Embed Size (px)
Citation preview

Self-Harm and CAMHS
Dr Tauseef Mehdi
Consultant Child and Adolescent Psychiatrist


Case Example
• Tina was a 15-year-old girl whose boyfriend recently broke up with her. On the way home from school, she saw him kissing another girl. When she arrived home, she immediately went upstairs to her bedroom, locked the door, and cut herself on the wrist several times with a razor blade. Although she wore long sleeves to dinner that evening, her mother spotted the wounds and brought her daughter to the emergency room, saying her daughter had tried to kill herself. Tina, however, stated emphatically that she did not want to die. “I cut myself because it made me feel better,” she said.
• A consulting psychiatrist interviewed Tina in the emergency room. A nurse had warned the psychiatrist that Tina was “borderline” and “gamey,” stating, “She just cut herself for attention. Don’t let her manipulate you.” However, after an extensive interview with Tina, there were insufficient criteria to merit a diagnosis of borderline personality disorder. In fact, despite her obvious problems coping with distress, Tina did not meet the criteria for any major mental disorder in the Diagnostic and Statistical Manual of Mental Disorders.

Another Case..
• NW - 15 year old British girl Sri Lankan family. On Friday, opened up to head teacher at school about problems (low self-esteem, recurrent mild sporadic self-cutting, and other stuff). Head teacher contacted social services who advised immediate admission in paediatric ward and for an “assessment on Monday”.

Self-Harm: Contents
• How big is the problem?
• Risk factors
• Causal Model
• Co-occurring difficulties
• Management
• Discussion

Self-harm
• Any self-poisoning or self-injury regardless of intent
• Suicide – coroner needs to be satisfied that the act was self-inflicted and death was the intended outcome.

Epidemiology – Prevalence studies
CASE Study 2008 Evans et al 2005 Hawton et al 2002
Type 7 country school
based comparative
community study
Systematic review of
128 studies
School based study
in England
Age group 15 +16 12-20 15-16
Number 30,000 n = 513,188 6020
Method Anonymous
questionnaire
Self-reported
suicidal
phenomenon
Self-reported
anonymous
questionnaire
Annual Prevalence M:2.6%, F:8.9% 7%
Lifetime Prevalence M:4.3%, F:13.5% 13.2 13.2%

CASE study 2008

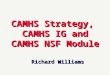
CASE 2008 - Method of SH

CASE Study – other findings
• Most acts took place at home (83%)
• Alcohol (19.9%) and drugs (12.8) were not usually involved
• Premeditation – 48% decided to harm within the last hour
• Reasons – “to get relief from a terrible state of mind” followed by “to die”
• Attempted suicide – lifetime 9.8%, annual 6.3%

Motives
Variety of intentions of SH
1.Finding one’s thought or situation unbearable
2.Needing to communicate distress to others
3.Escape from a terrible state of mind
4.Self-punishment
5.To die
6.Reduce anger, tension or dissociative numbness (habitual self-cutters)

Epidemiology • Presentation to hospital occurs only in 1 in 8
adolescents
• SH more common in females than males (F:M is as high as 6:1 in the 12-15s)
• Self-cutting most common method (CASE) However, it is self-poisoning that presents to hospital.
• Self-harm is the strongest predictors of death by suicide in adolescence

Outcomes – Repetition of SH
• Repetition of self-harm occurred in 27.3% of individuals (N = 3920) who presented between 2000 and 2005 and were followed up until 2007 (Hawton et al 2012).
• Bridge et al (2006) reported 5-15% annual risk of repetition
• Gibb (2005) - 10 year follow up post attempted suicide reported 28% , highest risk in 1st two years

Suicide
• Suicide < attempted suicide < SH < suicidal ideation



Suicide – Prevalence in Adolescence
• UK – 1999, 15-24 year old rates; (per 100,000) WHO
Male – 12.2
Female – 2.3

Suicide
• Suicides by 10- to 29-year-olds increased throughout the mid 1980s up until the late 1990s before showing a steady decline until 2005. Since then, the rate has remained relatively stable. This age group has consistently had the lowest suicide rate since 2001.

Self—Harm outcomes
• Outcome – suicide
- Spirito et al 1989 – 11% adolescents
- Hawton et al 2006 – 11000 15 year olds followed up over 11 years following self –harm; suicide rate = 2.6% (10.2% death by any cause)
- Hawton and Harris 2008 – 710 <15 year olds, FU x 11 years after SH; suicide rate = 1.1%

Interventions that reduce suicide following SH?
• Meta-analysis of 18 studies – no evidence that intervention after self-harm actually reduced later suicide. Crawford et al 2007

Suicide
• Rare outcome, but a tragic one nonetheless, MOST ARE PREVENTABLE (WHO 2004).
• 2nd biggest killer of young people after RTAs.
• Self-harm is one of the strongest predictors of death by suicide.
• Self-cutters carry greater risk of eventual suicide than self-poisoning (d/c > in self-cutters)
• Suicide rates are underestimated.
• All self-harm patients presenting to hospital should receive and assessment of risk and needs (National collaborating centre for mental health 2004, NICE- Self-Harm)

Proximal Risk Factors
• Recent changes in mental or physical state
• Substance Misuse
• Recent stressful life events
• Current or past abuse
• Subjective meanings to events

Distal Risk Factors
• Socio-demographic: Females>Males, onset is early adolescent period with increase in late adolescence, past history of abuse, forensic history, peer self-harm, LAC, single parent family, asylum seekers, SE deprivation and family history of SH, communication
• Psychiatric/Psychological: previous history of self harm, any psychiatric disorder/s, certain personality traits

Aetiological Factors
• Self-Harm is not a mental illness – affect dysregulation
• Research as pointed towards a build up of distressing emotional states that reach a threshold that SH is necessary to find relief/escape.
• Reinforcing effect - repetition

Endogenous Opioid System

Our first case
• Tina explained to the psychiatrist that she cut herself because it was “calming.” She said that a year ago she first started pinching herself as a way to hurt herself. One day she saw her father’s razor blades and started cutting herself on her arms. “It helps me chill,” she said. “My mind slows down, I stop crying, and I just feel better.” She said the razor slicing into her skin did not hurt badly—just enough for her to “feel alive.” She felt so much better after cutting herself that afternoon that she was able to concentrate on her homework and not think any more of her ex-boyfriend and the girl he was kissing.

Motives
Variety of intentions of SH
1.Finding one’s thought or situation unbearable
2.Needing to communicate distress to others
3.Escape from a terrible state of mind
4.Self-punishment
5.To die
6.Reduce anger, tension or dissociative numbness (habitual self-cutters)

Functions of Self Harm
• Affect regulation and distress management
• Increasing affective experience
• Interpersonal functions – attention, manage expectations/pressure from others, communication


Psychiatric disorders associated with SH and suicide
• Systematic review of 7 psychological autopsy studies (PAS) (Cavanagh 2003) suggested that 47-74% of suicides examined were attributable to mental disorder
• Several PAS indicate an interaction between mental illness, substance misuse and interpersonal problems.
• Multiple mental disorders ups the risk of SH/suicide.
• Stressful life events - suicide
• Mood disorders, substance misuse and anxiety disorders were the highest co-occurring psychiatric condition in a self-harming adolescent sample
• 5-10% have NO MENTAL DISORDER.

Immediate Management
• Priority is to ensure the safety of the youth (themselves and others)
• NICE suggests all under 16s presenting with self-harm get admitted to a paediatric unit and be assessed by a specialist in CAMHS.
• Recommended, no evidence – from clinical experience, change of emotional state of the young person, change of psychosocial context, SH marker of distress.

CAMHS assessment
• Assessment of risk
• Assessment and treatment of psychiatric disorder – mood disorders and substance misuse disorders being most common
• Safeguarding and social assessment
• Ensuring immediate safety plan (explain) and crisis management – then further CAMHS input
• Ensuring effective follow up arrangements if discharged - “therapeutic assessment” enhances follow up engagement.

SH - Follow up management
• Dialectic Behaviour Therapy, CBT and MBT – favourable
• Psychosocial interventions – Disappointing results - several trials testing family problem solving therapy, emergency cards, motivational interviewing, brief psychological therapy vs. TAU showed no differences in repetition of self-harm.
• Group therapy (Wood 2001) – one with promising result, but two further trials failed to confirm benefits (NICE recommendation)
• Multi-systemic family based therapy (Huey 2004) – encouraging

SH - Follow up management
Medication usage – controversial, increased suicidality!
Very limited evidence for pharmacotherapy for Self-Harm – although the opioid system is being looked into.
Fluoxetine + CBT have conferred advantages in those affected by depression with reduction of suicidal ideation and acts (TADS 2004)

Hospitalisation
• No evidence this prevents further SH attempts or dying by suicide (Gould 2003, Kings 2006)
• No rigorous RCTs show psychiatric inpatient admissions reduce self-harm
• In fact, some adolescents may increase their self-harm behaviour once placed in an inpatient unit (Huey 2004)!

Information for young people/ carers
• Young Minds ‘Feeling suicidal’ ‘Worried about Self Harm’ leaflets –easy to read, reassuring, contains references to other useful sources of help www.youngminds.org.uk
• Young Minds also run parent helpline
• National self harm network www.nshn.co.uk ‘Supports individuals who self harm to decrease emotional distress and to
increase quality of life, empowering and enabling them to seek further support and alternatives to self harm.’
• www.youthaccess.org.uk database of local organisations that offer
counselling • www.selfharm.co.uk

Information for young people/ carers
• Young Minds ‘Feeling suicidal’ ‘Worried about Self Harm’ leaflets –easy to read, reassuring, contains references to other useful sources of help www.youngminds.org.uk
• Young Minds also run parent helpline
• National self harm network www.nshn.co.uk ‘Supports individuals who self harm to decrease emotional distress and to
increase quality of life, empowering and enabling them to seek further support and alternatives to self harm.’
• www.youthaccess.org.uk database of local organisations that offer
counselling • www.selfharm.co.uk