Embed Size (px)
Citation preview

DRG Systeme in Europa
Management im GesundheitswesenKrankenversicherung und Leistungsanbieter
20. Dezember 2012 Krankenversicherung und Leistungsanbieter 1
Reinhard Busse, Prof. Dr. med. MPH FFPHFG Management im Gesundheitswesen, Technische Universität Berlin
(WHO Collaborating Centre for Health Systems Research and Management)&
European Observatory on Health Systems and Policies

Activity
Expenditure
Control
Technical
EfficiencyQuality
Admini-
strative
simplicity
Trans-
parency
Number of
services per
case
Number
of cases
Fee-for-
Hospital payment systemsWhy DRGs? Advantages and disadvantages of
different forms of hospital payment
2
Fee-for-
service+ + - 0 0 - 0
Global
budget - - + 0 0 + -
Krankenversicherung und Leistungsanbieter20. Dezember 2012

Activity
Expenditure
Control
Technical
EfficiencyQuality
Admini-
strative
simplicity
Trans-
parency
Number of
services per
case
Number
of cases
Fee-for-
Hospital payment systems
USA 1980s
Why DRGs? Advantages and disadvantages of
different forms of hospital payment
� “dumping“ (avoidance), “creaming“
(selection) and “skimping“ (undertreatment)
� up/wrong-coding, gaming
3
Fee-for-
service+ + - 0 0 - 0
DRG-
based
payment
- + 0 + 0 - +
Global
budget - - + 0 0 + -
European
countries 1990s/2000s
USA 1980s
Krankenversicherung und Leistungsanbieter20. Dezember 2012
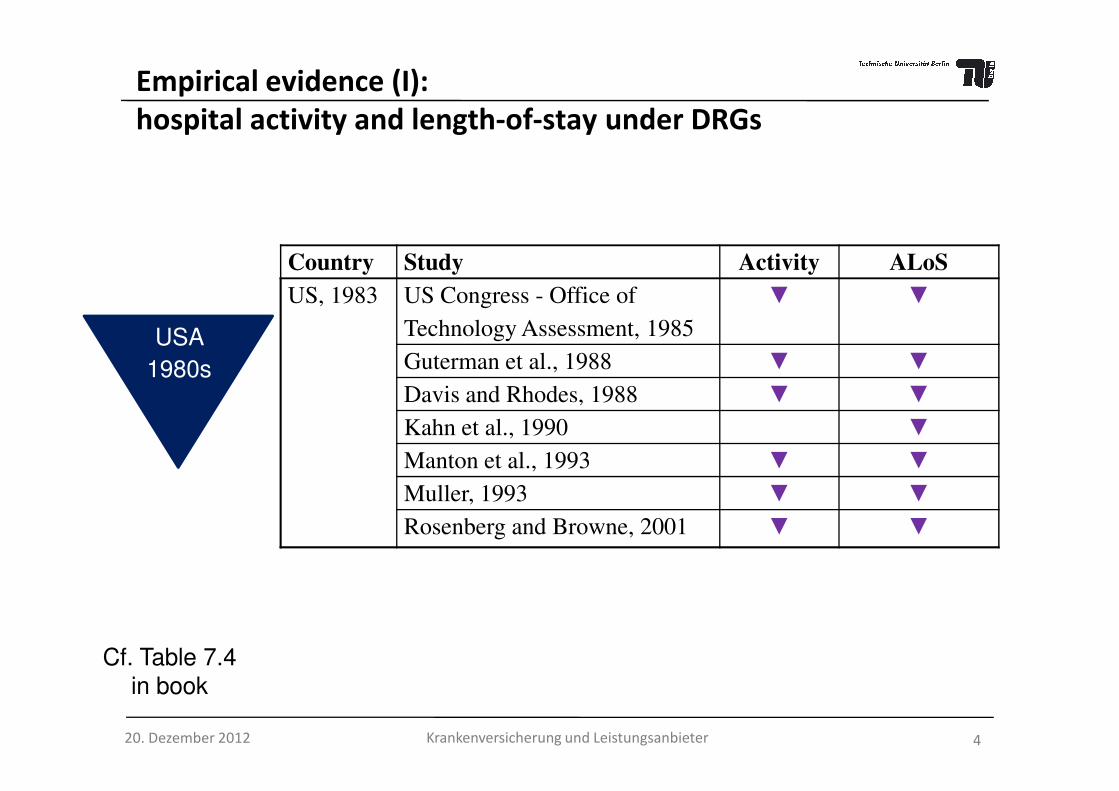
Country Study Activity ALoS
US, 1983 US Congress - Office of
Technology Assessment, 1985
▼ ▼
Guterman et al., 1988 ▼ ▼
Davis and Rhodes, 1988 ▼ ▼
Empirical evidence (I):
hospital activity and length-of-stay under DRGs
USA
1980sDavis and Rhodes, 1988 ▼ ▼
Kahn et al., 1990 ▼
Manton et al., 1993 ▼ ▼
Muller, 1993 ▼ ▼
Rosenberg and Browne, 2001 ▼ ▼
4Krankenversicherung und Leistungsanbieter
Cf. Table 7.4
in book
20. Dezember 2012

Empirical evidence (II)
Country Study Activity ALoS
Sweden,
early 1990s
Anell, 2005 ▲ ▼
Kastberg and Siverbo, 2007 ▲ ▼
Italy, 1995 Louis et al., 1999 ▼ ▼
Ettelt et al., 2006 ▲
Spain, 1996 Ellis/ Vidal-Fernández, 2007 ▲
Norway,
1997
Biørn et al., 2003 ▲
Kjerstad, 2003 ▲
Hagen et al., 2006 ▲
European
countries
1990/ 2000s
Cf. Table 7.4
in book
20. Dezember 2012
Hagen et al., 2006 ▲
Magnussen et al., 2007 ▲
Austria, 1997 Theurl and Winner, 2007 ▼
Denmark, 2002 Street et al., 2007 ▲
Germany, 2003 Böcking et al., 2005 ▲ ▼
Schreyögg et al., 2005 ▼
Hensen et al., 2008 ▲ ▼
England,
2003/4
Farrar et al., 2007 ▲ ▼
Audit Commission, 2008 ▲ ▼
Farrar et al., 2009 ▲ ▼
France, 2004/5 Or, 2009 ▲ 5

So then, why DRGs?
To get a common “currency” of hospital activity for
• transparency � efficiency benchmarking &
performance measurement (protect/ improve quality),
• budget allocation (or division among providers),
• planning of capacities,• planning of capacities,
• payment (� efficiency)
Exact reasons, expectations and DRG usage differ
among countries – due to (de)centralisation, one
vs. multiple payers, public vs. mixed ownership.
6Krankenversicherung und Leistungsanbieter20. Dezember 2012

Country 19
85
19
90
19
95
20
00
20
05
20
10
Original purpose Principal purpose in 2010
Austria LKF (self-developed) Budgetary allocation Budgetary al location, Planning
England HRG (self-developed) Measuring hospital activity Payment
Estonia NordDRG (HCFA-DRG) Payment Payment
Finland NordDRG (HCFA-DRG)Measuring hospital activity,
benchmarking
Planning, benchmarking,
hospital bi ll ing
France GHM (HCFA-DRG) Measuring hospital activity Payment
Germany G-DRG (AR-DRG) Payment Payment
Ireland HCFA-DRG AR-DRG Budgetary allocation Budgetary al location
Netherlands DBC (self-developed) Payment Payment
Poland JGP (HRG) Payment Payment
Portugal HCFA-DRG AP-DRG Measuring hospital activity Budgetary al location
Spain AP-DRG
(Catalonia) HCFA/CMS-DRG
Sweden NordDRG (HCFA-DRG) PaymentPayment, measuring hospital
activity, benchmarking
19
85
19
90
19
95
20
00
20
05
20
10
Introduction of DRGs
DRG-based hospital payment
Notes: the name of the DRG system used in countries is shown in bold, in brackets is the (origin of of a national DRG system); LKF=
leistungsorientierte Krankenanstaltenfinanzierung; HRG= Healthcare Resource Groups; NordDRG= common DRG system of the nordic countries;
HCFA= Health Care Financing Administration; GHM= Groupes Homogènes de Malade; G-DRG= German-DRG; AR-DRG= Austral ian Refined-DRG;
DBC= Diagnose Behandeling Combinaties; JGP= Jednorodne Grupy Pacjentów; AP-DRG= All Patient-DRG
Budgetary allocationBudgetary al location,
benchmarking
Krankenversicherung und Leistungsanbieter 720. Dezember 2012

Excluded costs
(e.g. for infrastructure; in U.S. also physician services)
Payments for non-patient care activities
(e.g. teaching, research, emergency availability)
Payments for patients not classified into DRG system
(e.g. outpatients, day cases, psychiatry, rehabilitation)
For what types of activities? Scope of DRGs (I)
DRG-based case payments,
DRG-based budget allocation(possibly adjusted for outliers, quality etc.)
(e.g. outpatients, day cases, psychiatry, rehabilitation)
Other types of payments for DRG-classified patients
(e.g. global budgets, fee-for-service)
Additional payments for specific activities for DRG-
classified patients (e.g. expensive drugs, innovations),possibly listed in DRG catalogues
Krankenversicherung und Leistungsanbieter 820. Dezember 2012

Original
DRG
DRG system
(included in or
DRG system
(included in or
DRG system
(identical or
DRG system
(included in or
For what types of activities? Scope of DRGs (II)
Psychiatry Day casesAcute
inpatient careOutpatient care Rehabilitation
DRG
systems
(included in or
separate from
original DRGs)
(included in or
separate from
originalDRGs)
(identical or
different to
original DRGs)
(included in or
separate from
original DRGs)
Krankenversicherung und Leistungsanbieter 920. Dezember 2012

Scope in the Netherlands:
DBCs (diagnosis-treatment combinations); examples
Inpatient acute care incl. ICU
Ambulatory
specialist
DBC 1Ambulatory specialist
care
care
Hospitalisation
Discharge
DBC 2
DBC 3
DBC 6
DBC 5
DBC 4
10Krankenversicherung und Leistungsanbieter20. Dezember 2012

Data collection
Price setting
Actual
reimbursement
• Demographic data
• Clinical data
• Cost data
• Sample size, regularity
Essential building blocks of DRG systems
2
34
Patient
classification
system
• Diagnoses
• Procedures
• Severity
• Frequency of revisions
• Cost weights
• Base rate(s)
• Prices/ tariffs
• Average vs. “best”
• Volume limits
• Outliers
• High cost cases
• Quality
• Innovations
• Negotiations
Import 1
11Krankenversicherung und Leistungsanbieter20. Dezember 2012
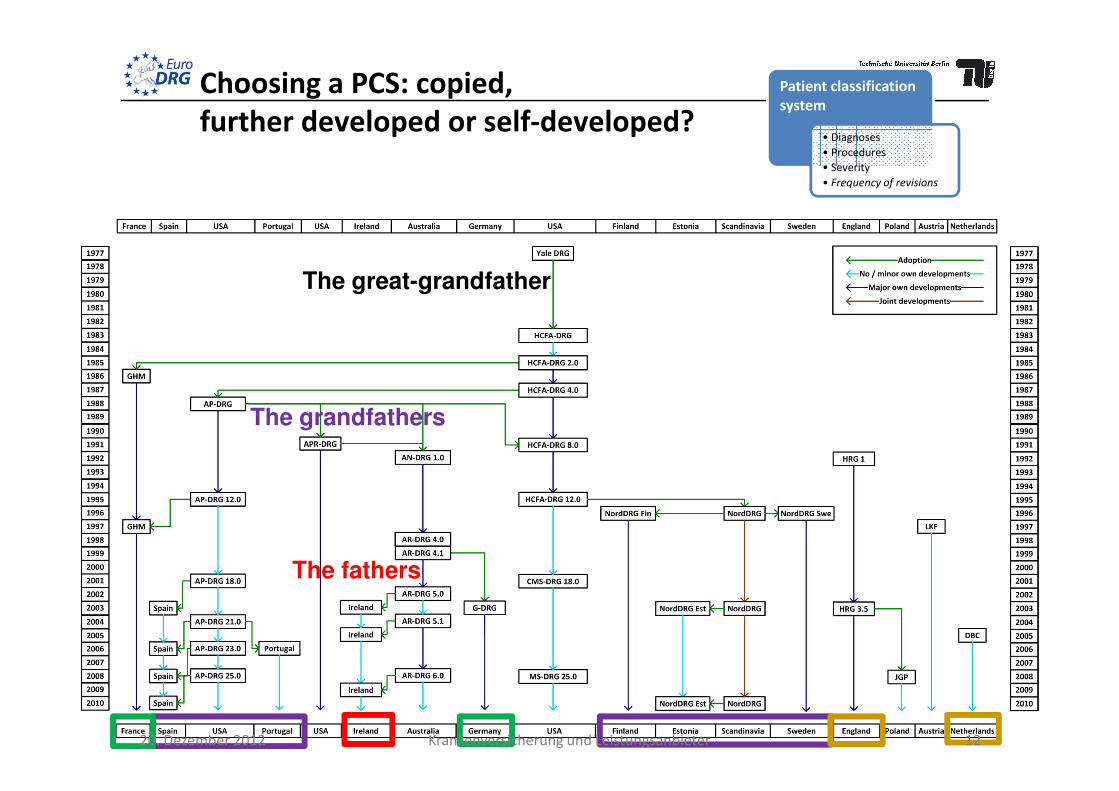
Choosing a PCS: copied,
further developed or self-developed?
Patient classification
system
• Diagnoses
• Procedures
• Severity
• Frequency of revisions
The great-grandfather
The grandfathers
The fathers
20. Dezember 2012 12Krankenversicherung und Leistungsanbieter

Classification variables and severity
levels in European DRG-like PCS
AP-DRG AR-DRG G-DRG GHM NordDRG HRG JGP LKF DBC
Classification Variables
Patient characteristics
Age x x x x x x x x -
Gender - - - - x - - - -
Diagnoses x x x x x x x x x
Neoplasms / Malignancy x x x - - - - - -
Body Weight (Newborn) x x x x - - - - -
Mental Health Legal Status - x x - - - - - -
Patient classification
system
• Diagnoses
• Procedures
• Severity
• Frequency of revisions
Mental Health Legal Status - x x - - - - - -
Medical and management decision variables
Admission Type - - - - - x x - -
Procedures x x x x x x x x x
Mechanical Ventilation - - x x - - - - -
Discharge Type x x x x x x x - -
LOS / Same Day Status - x x x x x x - -
Structural characteristics
Setting (inpatient, outpatient, ICU etc.) - - - x - - - - x
Stay at Specialist Departments - - - - - - - x -
Medical Specialty - - - - - - - - x
Demands for Care - - - - - - - - x
Severity / Complexity Levels 3* 4 unlimited 5** 2 3 3 unlimited -
Aggregate case complexity measure - PCCL PCCL x - - - - -
PCCL = Patient Clinical Complexity level
* not explicitly mentioned (Major CCs at MDC level plus 2 levels of severity at DRG level)
** 4 levels of severity plus one GHM for short stays or outpatient care 1320. Dezember 2012 Krankenversicherung und Leistungsanbieter
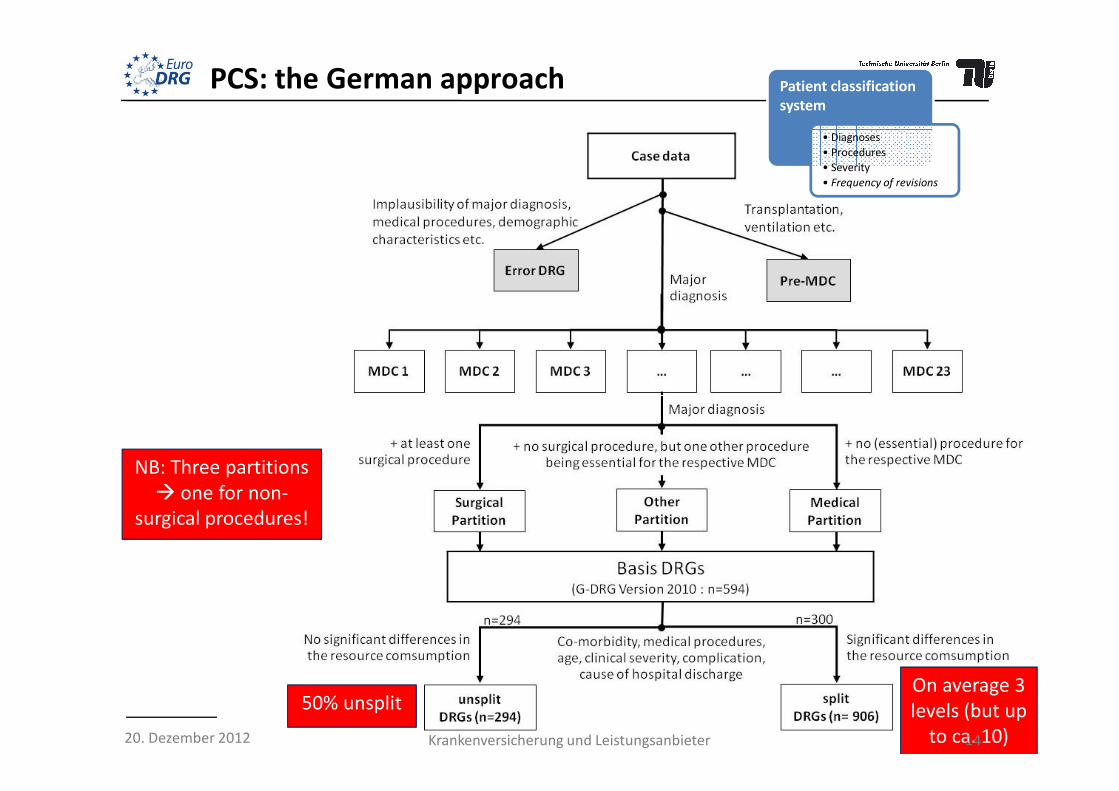
PCS: the German approach Patient classification
system
• Diagnoses
• Procedures
• Severity
• Frequency of revisions
NB: Three partitions
� one for non-
surgical procedures!
50% unsplitOn average 3
levels (but up
to ca. 10)20. Dezember 2012 14Krankenversicherung und Leistungsanbieter

Actual classification differs: appendectomy
15Krankenversicherung und Leistungsanbieter20. Dezember 2012

Basic characteristics of DRG-like PCS in Europe
Patient classification
system
• Diagnoses
• Procedures
• Severity
• Frequency of revisions
AP-DRG AR-DRG G-DRG GHM NordDRG HRG JGP LKF DBC
DRGs / DRG-like groups 679 665 1,200 2,297 794 1,389 518 979 ≈30,000
MDCs / Chapters 25 24 26 28 28 23 16 - -
Partitions 2 3 3 4 2 2* 2* 2* -
16Krankenversicherung und Leistungsanbieter20. Dezember 2012

MDC
differences
across DRG
systemssystems
Patient classification
system
• Diagnoses
• Procedures
• Severity
• Frequency of revisions
20. Dezember 2012 17Krankenversicherung und Leistungsanbieter

Main questions relating to data collection
Clinical data� classification system for diagnoses and
� classification system for procedures
Cost data� imported (not good but easy) or
� collected within country (better but needs
Data collection
• Demographic data � collected within country (better but needs standardised cost accounting)
Sample size� entire patient population or
� a smaller sample
Many countries: clinical data = all patients;
cost data = hospital sample with standardised cost accounting system
• Clinical data
• Cost data
• Sample size, regularity
18Krankenversicherung und Leistungsanbieter20. Dezember 2012

Diagnosis and procedure coding across Europe
Country Diagnosis Coding Procedure Coding
Austria ICD-10-AT Leistungskatalog
England ICD-10 OPCS - Office of Population Censuses and Surveys
Estonia ICD-10 NCSP - Nomesco Classification of Surgical Procedures
Finland ICD-10 NCSP - Nomesco Classification of Surgical Procedures
France ICD-10 CCAM - Classification Commune des Actes Médicaux
Data collection
• Demographic data
• Clinical data
• Cost data
• Sample size,
regularity
France ICD-10 CCAM - Classification Commune des Actes Médicaux
Germany ICD-10-GM OPS - Operationen- und Prozedurenschlüssel
Ireland ICD-10-AM ACHI - Australian Classification of Health Interventions
The Netherlands ICD-10 Elektronische DBC Typeringslijst
Poland ICD-10 ICD-9-CM
Portugal ICD-9-CM ICD-9-CM
Spain ICD-9-CM ICD-9-CM
Sweden ICD-10 NCSP - Nomesco Classification of Surgical Procedures
(almost)
standardisedno uniform standard available
19Krankenversicherung und Leistungsanbieter20. Dezember 2012
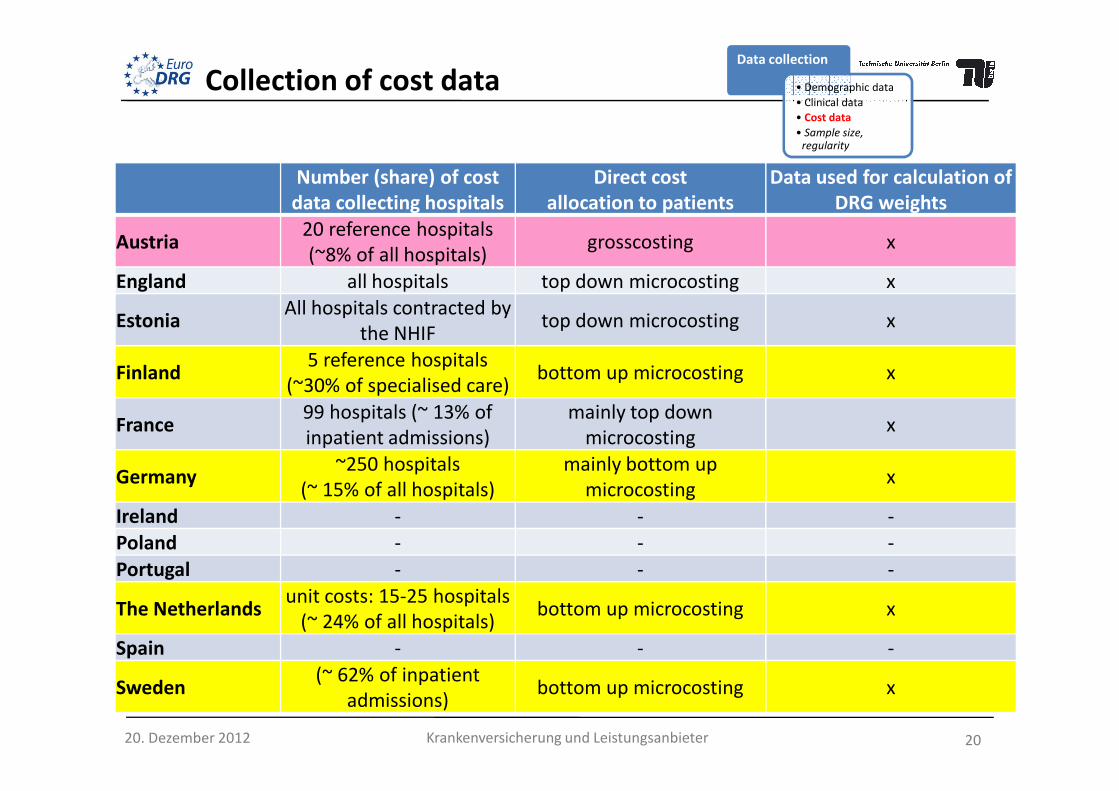
Number (share) of cost
data collecting hospitals
Direct cost
allocation to patients
Data used for calculation of
DRG weights
Austria20 reference hospitals
(~8% of all hospitals)grosscosting x
England all hospitals top down microcosting x
EstoniaAll hospitals contracted by
the NHIFtop down microcosting x
Finland5 reference hospitals
(~30% of specialised care)bottom up microcosting x
Data collection
• Demographic data
• Clinical data
• Cost data
• Sample size,
regularity
Collection of cost data
(~30% of specialised care)
France99 hospitals (~ 13% of
inpatient admissions)
mainly top down
microcostingx
Germany~250 hospitals
(~ 15% of all hospitals)
mainly bottom up
microcostingx
Ireland - - -
Poland - - -
Portugal - - -
The Netherlandsunit costs: 15-25 hospitals
(~ 24% of all hospitals)bottom up microcosting x
Spain - - -
Sweden(~ 62% of inpatient
admissions)bottom up microcosting x
20Krankenversicherung und Leistungsanbieter20. Dezember 2012

Number (share) of cost
data collecting hospitals
Direct cost
allocation to patients
Data used for calculation of
DRG weights
Austria20 reference hospitals
(~8% of all hospitals)grosscosting x
England all hospitals top down microcosting x
EstoniaAll hospitals contracted by
the NHIFtop down microcosting x
Finland5 reference hospitals
(~30% of specialised care)bottom up microcosting x
Collection of cost dataData collection
• Demographic data
• Clinical data
• Cost data
• Sample size,
regularity
(~30% of specialised care)
France99 hospitals (~ 13% of
inpatient admissions)
mainly top down
microcostingx
Germany~250 hospitals
(~ 15% of all hospitals)
mainly bottom up
microcostingx
Ireland
Imported DRG systems and weights (or with only minor modifications)Poland
Portugal
The Netherlandsunit costs: 15-25 hospitals
(~ 24% of all hospitals)bottom up microcosting x
Spain Imported DRG systems and weights
Sweden(~ 62% of inpatient
admissions)bottom up microcosting x
21Krankenversicherung und Leistungsanbieter20. Dezember 2012

Cost accounting in hospitals: how Germany does itData collection
• Demographic data
• Clinical data
• Cost data
• Sample size,
regularity
22Krankenversicherung und Leistungsanbieter
99 cost categories!
20. Dezember 2012

“cost weight“
(varies by DRG)
“base rate“ or adjustment
Price setting
• Cost weights
• Base rate(s)
• Prices/ tariffs
• Average vs. “best”
How to calculate costs and set prices fairly (I)
• Based on good quality data
(not possible if cost weights imported)
• “Cost weights x base rate”
vs. “Tariff + adjustment” vs. Scores (see below)
• Average costs vs. “best practice” (for few HRGs in England)
(varies by DRG)
Relative weight
(e.g. Germany)1.0
€ 3000 (+/-)
(varies slightly by state)
Raw tariff
(e.g. France)€ 3000
1.0 (+/-)
(varies by region and hospital)
Raw tariff
(e.g. England)£ 3000
1.0 – 1.32
(varies by hospital)
Score (e.g. Austria) 130 points € 30
X
X
X
23Krankenversicherung und Leistungsanbieter20. Dezember 2012
X

Country Monetary conversion/
adjustment factors
Applicability of conversion
rate / adjustment factors
Austria (Implicit) Point value Depending on state
England Market forces factor Hospital-specific
Estonia Base rate Nationwide
Finland Base rate Hospital-specific
France (1) Regional adjustment
(2) Transition coefficient (until
2012)
(1) Region-specific
(2) Hospital-specific
How to calculate costs and set prices fairly (II)
Price setting
• Cost weights
• Base rate(s)
• Prices/ tariffs
• Average vs. “best”
24
2012)
Germany Base rate State-wide
Ireland Base rates (1) Specific to one of four hospital
peer groups
(2) Hospital-specific
Netherlands Direct (no conversion) Not applicable
Poland Point value Nationwide
Portugal Base rate Hospital peer group
Spain (Catalonia) (1) Direct (no conversion)
(2) Base rate
(1) Not applicable
(2) Region-wide (CMS-DRGs)
Sweden Base rate County-specific
Krankenversicherung und Leistungsanbieter20. Dezember 2012

Costs/
revenues
Total costs of treating one patient
2) Increase revenue
1
1p̂R =
2p̂
Incentives of DRG-based hospital payment 1Being aware of incentives and hospital strategies
in times of DRGs
LOS1a) Reduce LOS
1b) Reduce intensity of services1p̂R =
25
Options to avoid deficits under activity based payments
Krankenversicherung und Leistungsanbieter20. Dezember 2012

Incentives of DRG-based
hospital payment
Strategies of hospitals
1. Reduce costs per
patient
a) Reduce length of stay
• optimize internal care pathways
• inappropriate early discharge (‘bloody discharge’)
b) Reduce intensity of provided services
• avoid delivering unnecessary services
• withhold necessary services (‘skimping/undertreatment’)
c) Select patients
• specialize in treating patients for which the hospital has a competitive
advantage
• select low-cost patients within DRGs (‘cream-skimming’)
Incentives and hospital strategies
20. Dezember 2012 Krankenversicherung und Leistungsanbieter 26
• select low-cost patients within DRGs (‘cream-skimming’)
2. Increase revenue per
patient
a) Change coding practice
• improve coding of diagnoses and procedures
• fraudulent reclassification of patients, e.g. by adding inexistent
secondary diagnoses (‘up-coding’)
b) Change practice patterns
• provide services that lead to reclassification of patients into higher
paying DRGs (‘gaming/overtreatment’)
3. Increase number of
patients
a) Change admission rules
• reduce waiting list
• admit patients for unnecessary services (‘supplier-induced demand’)
b) Improve reputation of hospital
• improve quality of services
• focus efforts exclusively on measurable areas

How European DRG systems reduce unintended
behaviour: 1. long- and short-stay adjustments
Revenues
Short-stay
outliers
Long-stay
outliers
InliersActual
reimbursement
LOSDeductions
(per day)
Surcharges
(per day)
Lower LOS
threshold
Upper LOS
threshold
• Volume limits
• Outliers
• High cost cases
• Quality
• Innovations
• Negotiations
27Krankenversicherung und Leistungsanbieter20. Dezember 2012

How European DRG systems reduce unintended
behaviour: 2. Fee-for-service-type additional payments
Actual
reimbursement
England France Germany Nether-
lands
Payments per
hospital stay
One One One Several
possible
Payments for
specific high-
Unbundled
HRGs for e.g.:
• Chemotherapy
Séances GHM for
e.g.:
• Chemotherapy
Supplementary
payments for e.g.:
• Chemotherapy
No
• Volume limits
• Outliers
• High cost cases
• Quality
• Innovations
• Negotiations
specific high-
cost services • Chemotherapy
•Radiotherapy
•Renal dialysis
•Diagnostic
imaging
•High-cost drugs
• Chemotherapy
•Radiotherapy
•Renal dialysis
Additional
payments:
• ICU
• Emergency care
• High-cost drugs
• Chemotherapy
•Radiotherapy
•Renal dialysis
•Diagnostic imaging
•High-cost drugs
Innovation-
related add’l
payments
Yes Yes Yes Yes (for
drugs)
28Krankenversicherung und Leistungsanbieter20. Dezember 2012

How European DRG systems reduce unintended
behaviour: 3. adjustments for quality
Actual
reimbursement
• England & Germany: no extra payment if
patient readmitted within 30 days
• Germany: deduction for not submitting quality• Volume limits
• Outliers
• High cost cases
• Quality
• Innovations
• Negotiations
• Germany: deduction for not submitting quality
data
• England: up 1.5% reduction if quality
standards are not met
• France: extra payments for quality
improvement (e.g. regarding MRSA)
29Krankenversicherung und Leistungsanbieter20. Dezember 2012

Actual
reimbursement
How DRG systems try to counter-act such behaviour:
quality
• Volume limits
• Outliers
• High cost cases
• Quality
• Innovations
• Negotiations
30Krankenversicherung und Leistungsanbieter20. Dezember 2012

4. Frequent revisions of PCS and payment rates
Country PCS Payment rate
Frequency of updates Time-lag to data Frequency of updates Time-lag to data
Austria Annual 2–4 years 4–5 years 2–4 years
England Annual Minor revisions annually; irregular
overhauls about every 5–6 years
Annual 3 years (but adjusted for
inflation)
Estonia Irregular (first update
after 7 years)
1–2 years Annual 1–2 years
Finland Annual 1 year Annual 0–1 year
France Annual 1 year Annual 2 years
Germany Annual 2 years Annual 2 years
Ireland Every 4 years Not applicable (imported
AR-DRGs)
Annual (linked to
Australian updates)
1–2 years
Netherlands Irregular Not standardized Annual or when
considered necessary
2 years, or based on
negotiations
Poland Irregular – planned
twice per year
1 year Annual update only of
base rate
1 year
Portugal Irregular Not applicable (imported
AP-DRGs)
Irregular 2–3 years
Spain (Catalonia) Biennial Not applicable (imported
3-year-old CMS-DRGs)
Annual 2–3 years
Sweden Annual 1–2 years Annual 2 years
31Krankenversicherung und Leistungsanbieter20. Dezember 2012

How do DRG systems deal with innovations?
Actual
reimbursement
32Krankenversicherung und Leistungsanbieter20. Dezember 2012
• Volume limits
• Outliers
• High cost cases
• Quality
• Innovations
• Negotiations

How do DRG systems deal with innovations?
Actual
reimbursement
33Krankenversicherung und Leistungsanbieter20. Dezember 2012
• Volume limits
• Outliers
• High cost cases
• Quality
• Innovations
• Negotiations

List B–DBCs as basis for price
negotiations in the Netherlands Actual
reimbursement
• Volume limits
• Outliers
• High cost cases
• Quality
• Innovations
• Negotiations
34Krankenversicherung und Leistungsanbieter20. Dezember 2012

Conclusions
• DRG-based hospital payment is the main method of provider payment in Europe, but systems vary across countries
– Different patient classification systems
– DRG-based budget allocation vs. case-payment
– Regional/local adjustment of cost weights/conversion rates
• To address potential unintended consequences, countries
– implemented DRG systems in a step-wise manner – implemented DRG systems in a step-wise manner
– operate DRG-based payment together with other payment mechanisms
– refine patient classification systems continously (increase number of groups)
– place a comparatively high weight on procedures
– base payment rates on actual average (or best-practice) costs
– reimburse outliers and and high cost services separately
– update both patient classification and payment rates regularly
• If done right (which is complex), DRGs can contribute to increased transparency and efficiency – and possibly quality
35Krankenversicherung und Leistungsanbieter20. Dezember 2012

20. Dezember 2012 36Krankenversicherung und Leistungsanbieter





























