Embed Size (px)
Citation preview

“the best way to protect children is to prevent child abuse and neglect from occurring in the first place” (Inverting the Pyramid, The Allen Consulting Group,2008: x)
•In rich nations, approximately 10% of children are abused.

“Successful family support aims to inculcate in parents the experience of themselves as worthy, and to foster self-esteem, self-confidence and enhanced competence as a parent” (Hearn 1995).
These self-attributes stem from the emergence of trust through the experience of successful relationships (Rutter et al 1990).
Family support reflects a set of values and a deep respect for the complex tasks involved in parenting (Whittaker 1993).
BUT: where are the children? how to handle tensions in conflicts of interest between parents and children

From ORGANISATIONAL
LEVEL Service based Child protection focus
PRACTITIONER LEVEL Systemic Solution focused Expert, rule based/
USER LEVEL Isolationist Cognitive development Authoritarian/non-
shared
To
Outcomes based Child & family welfare
Relational Relationship based Reflective
Transactional-Ecological Social and emotional
development. Participatory/shared
COMPLEXITY

Carer’s own relationship and attachment history,
Carer’s state of mind, and level of reflective
function
Caregiving environment generated by carer
Social stress, relationships,environmental
stressors
Child’s attachment behaviour, adaptive strategies, and
developmental states and behaviours,
ECOLOGICAL TRANSACTIONAL APPROACH

Early intervention - national studies of systems set up to help children and families with early stage problems or ‘additional needs’ (Common Assessment Framework in England 2006 and Wales 2009)
Family support - smaller scale studies of services for children/ families with problems of greater intensity/duration (Family Centre study 2006 and Intensive Family Preservation study 2006)
Serious maltreatment -national studies (England and Wales) of children who have died or been seriously harmed through maltreatment (1999-2010)

Levels of Prevention/Thresholds of Intervention (adapted from Every Child Matters 2003:21,DfES 2006:7)
Where do the studies fit?Threshold wrangles
Which professionals involved ?

England Professional anxiety – about process, about increased
workload, about lack of skill Lack of professional trust, conflicts of interest (inter-
agency working), threshold and boundary struggles ‘Willingness’ and ‘vision’ not matched by results until
the process was clarified (much later) and owned by all sectors
Wales Decision that each agency had to provide the help
required was a disincentive to identifying need No clear process meant that no-one knew what to do The electronic database dominated the early set up.

Child protection work following family support principles. Care and compassion mixed with rigorous, tough minded assessment
“A high level of closeness and trust appeared to develop quickly between the worker and the family members,”
“it was wonderful, just to have somebody that I knew I could ring up when things started going wrong and she would be there for me – it was absolutely brilliant – I can’t tell you what a feeling that gave me”
Children valued having a say, having some choices, and being listened to.

Evidence from both studies that parents and children had a better sense of self-worth - being newly perceived as a good parent and good person made a difference
In parents this coincided with better care for their children, and an improved ability to tolerate their children’s difficult behaviour,
Being better accepted by others, eg being more likeable and less overwhelming for social workers:
“we used to dread working with this family but they’re much easier to work with now” - the capacity to make better use of services as a good outcome.

Good support to families was matched by good staff supervision and support to staff – ‘containment’ of families and staff was key
compassion and kindness was directed towards staff, families, and anyone who crossed the centre threshold. A member of staff said:
“you feel cherished and cared for and protected. People do things to make you feel safe, which helps you to cope with losses like bereavement”

“….in the drive to avoid further risk for the child my impression was that, at times, children’s services had a punitive, even suspicious attitude towards the mother”
(student social worker’s dissertation 2010)
Does this approach increase safety for the child? (maybe)
Does it improve relationships of trust between worker and mother and child and mother? (probably not)
NB Most maltreated children live at home even when abuse is substantiated.

Are each of these cases unique or part of a pattern? (Both).
Over 600 cases studied between 2003-2010 some patterns are evident
Known to social services?: Just under half of children NOT known at time of incident (BUT ¾ known to in past)
High Child Protection Risks?: Less than 1:5 children with a current CP plan (BUT in 1:3 cases, child or sib had plan in the past)
Age of child? : Nearly half under 1, nearly quarter 1-5, nearly quarter 11-17, (less than 10% aged 6-10)
More cases of death than serious injury, but serious injury cases rising

“[mother] had a series of violent
partners…, suffered with mental health problems, anxiety and depression and was misusing alcohol. The family changed address frequently….all three children witnessed serious domestic abuse… [mother] failed to attend a number of medical appointments with the children.”
How different from any case on a social worker’s or health visitor’s case load where children don’t die??

Levels of intervention Spread of serious child abuse cases across all levels (nb “child
protection does not come labelled as such”, Laming 2003 ) – implications for awareness of child protection risks in early intervention and better links with common assessment and lead practitioner working at lower levels
Need for all agencies to understand the importance of inter-acting risk factors (ecological transactional perspectives).
Family Cooperation: many factors influence this eg behaviour of professionals
towards families, family’s suspicion of some agencies (cf DfES Policy Review 2007 )
Need to understand patterns of poor cooperation – hostility, disguised compliance, ambivalence, avoidance of contact etc as part of inter-acting risk factors.

Parental hostility/worker paralysis “workers can become paralysed by their own
fears/anxieties, which can lead to the assessment process remaining incomplete”
This hampers workers’ abilities to reflect, make judgements and act clearly
To work effectively with hostility and notice potentially damaging patterns of cooperation, like disguised compliance, practitioners need to be self-aware, flexible and sensitive to the factors underlying their own and the family’s behaviour and emotions.
Besieged, overwhelmed workers may feel they have nothing left to give

Fixed views about family,Fixed assessment views
(eg neglect)
Efforts not to be judgemental, whole picture missed, silo practice.
Invisible children
Overwhelmed chaotic families, negative family support, drugs, violence,mental ill health, criminality
Too much to achieve, low expectations, ‘success’ is getting through the door, muddle about confidentiality

Confident professional Judgement, sustained challenge.
Support and
trust within teams.
Good working relationships with children and their families
Child seen. kept in mind, understood
Clear communication with other agencies.
Good, reflective, challenging supervision

The dominant culture of audit, target setting and performance indicators encourages speedy processing and external accountability. It does not confer trust in workers’ professional judgement and leaves little time for reflection and relationship building with needy children and families or with colleagues.
Practitioners who establish trusting relationships with children and families are found in settings where strong relationships are goals to be achieved
Trust and kindness, which are at the heart of relationships, are harder to find in many areas of practice with children who are severely maltreated.
Practitioners and managers must be well supported in order to be curious and sceptical; to think critically and systematically but to act compassionately. It is not helpful to be sceptical in the absence of compassion

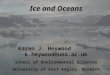
23 3
9 12
Level of intervention and degree of cooperation with agencies at time of incident n=47
Levels 3 and 4Child protection/ regulatory/ restoratory services
Levels 1 and 2(Universal services and early needs)
Lack of cooperation Co-operation

Level of services (Levels 1-4)and Degree of parental/child cooperation →

ReferencesFamily Support/ Early Intervention StudiesBrandon, M., and Connolly, J., (2006) ‘Are Intensive Family Preservation
Services Useful? : A study in the United Kingdom’, Family Preservation Journal, Vol. 9, 56-69.
Brandon, M., (2006) ‘Confident workers, confident families: Exploring sensitive outcomes in family centre work in England’, International Journal of Child and Family Welfare, Vol. 9,1-2: 63-78.
Brandon, M., Howe, A., Dagley, V., Salter, and C., Warren, C., (2006) ‘What appears to be helping or hindering practitioners in implementing the Common Assessment Framework and Lead Professional Working’, Child Abuse Review, 15, (6) 396-413.
Serious abuse study Brandon, M., and Thoburn, J., (2008) ‘Safeguarding children in the UK: a
longitudinal study of services to children suffering or likely to suffer significant harm’ Child and Family Social Work, 13(4) 365-377.
• • • •

References



![Mackiewicz, M. arXiv:1706.05208v4 [cs.CV] 23 Sep 2018 · French, G. g.french@uea.ac.uk Mackiewicz, M. m.mackiewicz@uea.ac.uk Fisher, M. mark.fisher@uea.ac.uk September 25, 2018 Abstract](https://img.pdfslide.us/doc/110x75/5fd4e3c82abb3256c83d0f9c/mackiewicz-m-arxiv170605208v4-cscv-23-sep-2018-french-g-gfrenchueaacuk.jpg)