-
8/19/2019 Done-Cranial Nerve Disorder-Mom Heny-Jumat,20 Nov
2013
1/10
Askep Cranial Nerve Disorder
Heny Suseani Pangastuti, SKp.,M.Kes
Jumat, 20 November 2015
-
8/19/2019 Done-Cranial Nerve Disorder-Mom Heny-Jumat,20 Nov
2013
2/10
A. TRIGEMINAL NEURALGIA (TIC DOULOUREUX)
• Adanya gangguan pada saraf
kranial ke V yang ditandaiadanya nyeri paroxymal pada
daerah yang diinervasi oleh 3cabang saraf, tetapi paling
-
8/19/2019 Done-Cranial Nerve Disorder-Mom Heny-Jumat,20 Nov
2013
3/10
sering terjadi pada cabang ke2 dan ke 3
(Maloni, 2! cit" #runer $suddart
• penyakit kronik pada saraftrigeminal yang menyebabkannyeri
%ajah berat denganpenyebab yang tidak diketahui
Karakerisik n!eri
• &yeri muncul dan hilang tiba'
tiba, digambarkan sebagaisensasi nyeri tusuk atausengatan
listrikditembak yangunilateral pada satu sisirahang atau pipi"
• )ada beberapa penderita,mata, telinga atau
langit'langitmulut dapat pula terserang"
• )ada kebanyakan penderita,nyeri berkurang saat malamhari, atau
pada saat penderitaberbaring
•
*apat muncul kontraksi ototfasialis involuntary yangmenyebabkan
menutupnyamata atau t%itch of themouth
• intense skin surface pain +
timesday or a fe% times ayear
• tarts peripherally andadvances centrally
• ome trigger -ones initiate
pain
• = tic ou!oureu" (painful
t%itch!"
• .arly attacks, appearing mostoften in the /fth decade of
life,usually mild and brief"
• )ain'free intervals may be
measured in terms of minutes,hours, days, or longer"
• 0ith advancing years, the
painful episodes tend tobecome more fre1uent andagoni-ing"
•
he patient lives in constantfear of attacks"
pen!e"a"
• idak pasti
• Mungkn krn kompresi atau
iritasi dari saraf trigeminalatau perubahan degeneratifpada
ganglion gasserian
•
)enyebab lain tekanan padapembuluh darah karenaabnormalitas
(!oop o# anartery !, gangguan pada saraftrigeminal, gasserian
gang!ion,or root entry $one
• )aroxysms can occur %ith anystimulation of the terminals ofthe
a4ected nerve branches
such as %ashing the
face, shaving,
brushing the teeth,
eating, and drinking"
A draft of cold air and
direct pressure againstthe nerve trunk
• 5ertain areas are called trigger
points because the slightesttouch immediately starts a
paroxysm or episode"
• o avoid stimulating theseareas, patients %ith
trigeminalneuralgia try not to touch or%ash their faces, shave,
che%,or do anything else that mightcause an attack"
• hese behaviors are a clue todiagnosis"
#$ARMACOLOGIC T$ERA#%
-
8/19/2019 Done-Cranial Nerve Disorder-Mom Heny-Jumat,20 Nov
2013
4/10
• Antisei-ure agents
– such as carbama-epine
(egretol!
•
relieve pain byreducing thetransmission ofimpulses
atcertain nerveterminals"
• 5arbama-epine istaken %ith meals"
• erum levels
must be
monitored toavoid toxicity inpatients %hore1uire highdoses to
controlthe pain"
• ide e4ects
include nausea,di--iness,dro%siness, andaplastic anemia"
• he patient ismonitored forbone marro%depression
duringlongterm therapy"
– 6abapentin (&eurontin!and baclofen (7ioresal!are also used
for paincontrol"
– 8f pain control is still not
achieved, phenytoin(*ilantin! may be usedas adjunctive
therapy(9o%land, 2!"
– Alcohol or phenol
injection of thegasserian ganglion andperipheral branches ofthe
trigeminal nerve
relieves pain for severalmonths" :o%ever, the
pain returns %ith nerveregeneration"
&URGICAL MANAGEMENT
• Microvascular *ecompression
of the rigeminal &erve"
• )aercutaneous 9adiofre1uency rigeminal 6angliolysis"
Eviden'e....Revie o *+ s,dies-
- microvascular decompression(MV*!
- he e;cacy of MV* andpercutaneous balloonmicrocompression
()#5!%ere similar (!, andtheir e4ects %eresuperior to those of
theother modalities () @"+!"
- radiofre1uencythermorhi-otomy (9'
9!
- Although 9'9provided a high initialpain relief, its
average
pain free rate %as>"BC for a meanfollo%'up of > years"
- he recurrence rate %ashigh after 9'9 (BDC!,%hile the
lo%estrecurrence rate (+E"3C!%as after MV* () @"+!"
-
8/19/2019 Done-Cranial Nerve Disorder-Mom Heny-Jumat,20 Nov
2013
5/10
- 0ithin the long'termfollo%'up periodrecurrence of
paina4ects at least +FC ofpatients %ho undergoany surgical
treatmentfor &"
CONCLU&ION&-
- he study suggests thateach surgical techni1uefor
treatment oftrigeminal neuralgia has
merits and limitations"
- MV* provides thehighest rate of long'term patientGsatisfaction
%ith thelo%est rate of painrecurrence"
atli M, atici
-
8/19/2019 Done-Cranial Nerve Disorder-Mom Heny-Jumat,20 Nov
2013
6/10
• Anjurkan klien untuk
tidak mengunyah padasisi yang terkena hinggarasa kebal
hilang
•
-
8/19/2019 Done-Cranial Nerve Disorder-Mom Heny-Jumat,20 Nov
2013
7/10
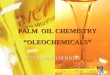
• one sided paralysis of facial muscles and upper eyelid,
• loss of taste on a4ected side,
• increased tearing of eye on a4ected side
3ell4s pals! is 'onsidered "! so/e o represen a !pe o
press,re
paral!sis.
Manae/en
• he objectives to maintain the muscle tone of the face
and to prevent or
minimi-e denervation"
• reassured that no stroke has occurred and that spontaneous
recovery
occurs %ithin 3 to > %eeks in most patients"
• :eat may be applied to the involved side of the face to
promote comfort
and blood o% through the muscles"
-
8/19/2019 Done-Cranial Nerve Disorder-Mom Heny-Jumat,20 Nov
2013
8/10
• .lectrical stimulation may be applied to the face to prevent
muscle
atrophy"
• Although most patients recover %ith conservative treatment,
surgical
exploration of the facial nerve may be indicated in patients %ho
are
suspected of having a tumor or for surgical decompression of the
facial
nerve and for surgical treatment of a paraly-ed face"
TREATMENT
• 5orticosteroid therapy (prednisone!
– to reduce inammation and edema
– this reduces vascular compression and permits
restoration of blood
circulation to the nerve"
– .arly administration of corticosteroid therapy appears to
diminish
the severity of the disease, relieve the pain, and prevent
or
minimi-e denervation"
• antiviral medications
• acial pain is controlled %ithanalgesic agents"
D1. Keperaaan
• 9isk for injury
• Acut pain
• disturbed body image
• 8mbalance nutrition less than
body re1uirements
NOC-
- Hno%ledge personal safety
- 9isk control Visual impairment
- issue integrity skin $ mucousmembran
NIC-
- :ealth education
Keepin 5e ineri! o 5e'ornea -
- )lace an eye patch on thea4ected eye during sleep tokeep it
shut"
- .ncourage patient to reportimmediately any painexperienced
around the eye,
reporting the level of pain andits location"
- Assess the condition of theeye including redness and
anydischarges"
- each the patient toadminister arti/cial tears
orophthalmic ointment asordered"
Alleviain 5e pain
• 8nstruct the patient to placemoist heat on the face"
• )erform routine massage onthe face to relieve musclepain"
• each the patient toadminister corticosteroids tominimi-e
the inammationand non'narcotic analgesics todecrease the pain
-
8/19/2019 Done-Cranial Nerve Disorder-Mom Heny-Jumat,20 Nov
2013
9/10
#ROMOTING $OME ANDCOMMUNIT%63A&ED CARE -Tea'5in #aiens
&el6Care.
• 0hile the paralysis lasts, the
involved eye must beprotected"
• re1uently, the eye does not
close completely and the blinkreex is diminished, so the "
• 5orneal irritation andulceration may occur if theeye is
unprotected"
• *istortion of the lo%er lid
alters the proper drainage oftears"
• o prevent injury, the eye
should be covered %ith aprotective shield at night"
• he eye patch may abrade thecornea, ho%ever, becausethere
is some
• di;culty in keeping the
partially paraly-ed eyelidsclosed"
• he application of eye
ointment at bedtime causesthe eyelids to adhere to oneanother
and remain closedduring sleep"
• he patient can be taught toclose the paraly-ed
eyelidmanually before going tosleep"
• 0rap'around sunglasses orgoggles may be %orn todecrease normal
evaporationfrom the eye"
Co/pli'aions
• Jlceration of the cornea
• 8mpairment of vision
• N,rsin Aler7
Heratitis, or the inammationof the cornea, is one of themost
dangerous complicationsfor a patient %ith #ellLs palsy"As a
precautionary measure,the nurse must ensure that thecornea is still
protected even if the eyelids %onLt close"
8UI9 TIME -
+" Apakah perbedaan antara#ellLs )alsy dan troke O
Kelaskan P
2" #erikut merupakan diagnosakepera%atn yang dapatditegakkan
pada pasien #ellL s
)alsy, kecuali """"a" 9isk for injuryb" Acut painc" disturbed
body imaged" gangguan maenelan
8"vascular ischemia,88" viral disease (herpes simplex,
herpes -oster!,888" autoimmune disease,8V" paparan A5
3" yang merupakan kemungkinanpenyebab dari #ellLs )alsyadalah
"""
B" #erikut yang merupakan terapipembedahan untuk pasien
%&'()M'N*+ N)&*+('* adalah """a" Micro analitic
nerve
trigeminal &euralgiab" Microvascular
*ecompressionc" 9adiotherapy pada cranial
d" Masage pada daerah facial>" Kelaskan beberapa
Hriteria
nyeri pada pasien rigelmia&euralgia P
Kunci Ja-aban
1. Paa pasien stro/e,/e!umpuanpara!ysis tia/anya terai paa
aerauni!atera! -aa namun uga
paa anggota gera/ yaitu
tangan an /a/i paasebagian sisi atau
-
8/19/2019 Done-Cranial Nerve Disorder-Mom Heny-Jumat,20 Nov
2013
10/10
/ese!uruan, seang/an paa pasien 3e!!4s Pa!sy para!ysisanya
terai i aera -aa.
2. .
6. *.
7. 3.
5. 8+iat NS9 seniri /a-an :