-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
1/34
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
2/34
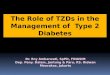
Body fluid compartments
Total body fluid = 60% body weight
Two-thirds is in the intracellular K+ rich
(120 mmol/L)
One-third is in the extracellular space
Na+ rich (140 mmol/L)
One-quarter of extracellular fluid is in
the intravascular space
In a 70-kg man Total body fluid = 42 L
Intracellular fluid = 28 L
Extracellular fluid = 14 L
Intravascular fluid = 3.5 L
There is movement of water
between these compartments
Plasma sodium concentration is
an index of total body fluid
osmolality
Body fluid compartments and osmolality(Robert U, NEPHROLOGY
Medical Progress December 2003)
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
3/34
Plasma sondium (Na+) concentration :
the ratio between sodium and water in the plasma
Normal : 135 145 mmol/L
Hyponatremia : < 135 mmol/L
Is, Na+ loss or water gain
HYPONATREMIA
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
4/34
Types and Causes of Hyponatremia
Pseudohyponatremia
A rare measurement artefact caused by reduced plasma water, as
a
result of excess lipids (triglycerides) or abnormal proteins
(e.g. IgM)
Hyperosmolar (iso-osmolar and other) hyponatremia
Hyperglycaemia (and other impairment solutes, but not urea)
Surgical (e.g. transurethral prostatectomy) irrigation fluids
(mannitol,
sorbitol, glycine)
Subarachnoid haemorrhage
True (hypo-osmolar) hyponatremia
q ECF (q TBNa+) reduced effective arterial volume (Na+ loss)
o ECF (o TBNa+) reduced effective arterial volume (oedema)
q ECF ( TBNa+) normal effective arterial volume (no oedema),
SIADH, drugs, stress, q cortisol, q thyroxine)
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
5/34
The formula of osmolality
Posm = 2[Na+] + [glucose]/18 + [BUN]/2.8
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
6/34
Hiponatremia
Translocational
hyperglycemia
irrigation fluids
(mannitol, sorbitol)
surgical
(transurethral prostatectomy)
Normal or high osmotic Low osmotic
(true hyponatremia)
Psudohyponatremia
protein
lipid
Urinary osmolality *)
> 100 mosm/kgUrinary osmolality
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
7/34
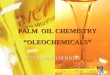
A Clinical Approach to Hyponatremia
Hypo-osmotic hyponatremia
Urinary sodium
concentration
Urinary
osmolality
Treatment Normal saline Water restriction Treat + restrict
water
Hypovolaemia Euvolaemia Hypervolaemia
Renal loss
Diuretic
Na+ loss
Extra Renal loss
Gastrointestinal
tract Skin
Heart failure
Liver failure
Nephrotic syndrome
Syndrome of
inappropriate
antidiuretic
PsychogenicHypothyroid
Drugs
(Robert U, NEPHROLOGY Medical Progress December 2003)
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
8/34
SALT LOSING NEPHRITIS
Nephritis with an excessive urinary loss of Na
hypovolemic hyponatremia
urinary Na+ >20 mmil/L
mostly without hypertension
medullary cystic disease
chronic interstitial nephritis
polycystic kidney disease analgetic nephropathy
partial urinary tract obstruction
chronic glomerulonephritis (rarely)
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
9/34
Diagnosis criteria for SIADH
(Syndrome of inappropriate ADH secretion
Essential
ECF effective osmolality below 270 mosmol/kg water
Inappropriate urinary concentration (> 100 mosmol/kg)
Clinical euvolemia
Increased urinary [Na+
] while on a normal salt and water intake Absence of adrenal,
thyroid, pituitary or renal insufficiency or
diuretic use
Supplemental
Abnormal water load test (inability to excrete at least 90% of
20
mL/kg water load in 4 h and/or failure to dilute urinary
osmolality tobelow 100 mosmol/kg)
Plasma ADH level inappropriately raised relative to plasma
osmolality
No significant correction of plasma [Na+] with volume expansion
but
improvement after fluid restriction THE LANCET, Vol 352, July
18, 1998)
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
10/34
CLINICAL MANIFESTATION:
Symtoms of hyponatremia due to the
consequences of plasma hypoosmolality
HypoosmolalityMove of water from extra
to intracellular
intracellular
edema
Particularly in CNS
Symptoms:
- Lethargy
- confusion
- nausea-vometing
- muscle cramps
- seizures- coma
Note:
Permanent neurologic damage may be occur in premenopausal
women
- the cause is not well understood
- so: hyponatremic women must be watched carefully
Lauriat, SM. J. Am Soc Nephrol. 8 : 1997
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
11/34
postoperative menstrual women
elderly women in thiazide diuretics
children
psychiatric polydipsic patients
hypoxemic patients
PATIENTS AT RISK FOR PERMANENTNEUROLOGIC COMPLICATION
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
12/34
Important questions must be answered :
1. Is the patients symptomatic ? Symptomatic patients have
to
treat aggressively but promptly
2. is the hyponatremia
- acute (before 48 hrs) ?
- chronic (after 48 hrs) ?
Acute hyponatremic, carries a
greater risk of permanent
neurologic sequelae if the
correction is not expeditiously
3. Whats the Na+ level ? Severe hypoNa+ is Na level
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
13/34
SEVERE
HYPONATREMIA
(Na+
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
14/34
HypoN+ present for
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
15/34
HypoNa+ present for >48 hrs or the duration is unknown
increase the serum Na+ by 10% with hypertonic saline
infusion at rate 1,5 -2 ml/kg/hr (or in 4-6 hrs)
after the initial correction, do not exceed a correction
rate of 1-1,5 ml/kg/hr
coadministration of loop diuretic
until the symptoms resolved or Na+ level 130 mmol/L
do not increase the serum Na+ by more than 15 mmol/L
24 hrs serum Na+ should be carefully monitored (every 4-6
hrs)
SEVERE CHRONIC SYMPTOMATIC HYPONa+
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
16/34
TreatmentTreatment MechanismMechanism
Fluid restrictionFluid restriction Decreases free waterDecreases
free water
Pharmacological inhibition of ADHPharmacological inhibition of
ADH
LithiumLithium Inhibits renal response to ADHInhibits renal
response to ADH
DemeclocyclineDemeclocycline Inhibits renal response to
ADHInhibits renal response to ADH
VV22 receptor antagonistreceptor antagonist Antagonises
vasopressinAntagonises vasopressin
Increased solute intakeIncreased solute intake
FurosemideFurosemide Increases free water clearanceIncreases
free water clearance
UreaUrea Osmotic diuresisOsmotic diuresis
THE LANCET, Vol 352, July 18, 1998)
CHRONIC ASYMPTOMATIC HYPONa+
No immediate therapy is required and underlying diseasecan be
sought
No urgency to coorect the serum Na+
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
17/34
HYPOKALEMIA
Serum K level < 3.5 mmol/L (normal: 3.5 5.5 mmol/L)
True hypokalemia : decreased of serum K level
False (spurious) hypokalemia :
false in laboratory result
in extreme leucocytosis (in vitro), wbc uptake kalium
in the test tube
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
18/34
DIAGNOSTIC APPROACH OF HYPOKALEMIA
Hypokalemia
Kalium depletionTranscelular shift
insulin therapy
beta2 agonists
alkalosis
Urine K 20 meq/L renal losses
Viarable PH
post obstructive
ATN recovery
aminoglycoside
Metabolic acidosis
RTA
Diabetic ketoacidosis
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
19/34
CLINICAL MANIFESTATIONS
Cardiac
ventricular irritability
abnormal ECG
predisposition of digitalis intoxication
coronary artery spasm Neuromuscular
muscle spasm, tetany, paralysis
gastrointestinal (constipation, ileus)
Renal polyuria
increased amoniogenesis
Endocrene
carbohydrate intolerance
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
20/34
MANAGEMENT
Emergency or not emergenny ? clinical manifestation
ECG
degree of hypo K
Estimated degree of decreases in total body kalium decreased in
average of 0,3 mmol/L for each 100 mmol of
kalium depletion
Serum K level Deficit
Mild 3.00 3.4 meq/L 150 200 meq/L
Moderate 2.00 3.0 meq/L 200 400 meq/L
Severe < 2 meq/L 500 1000 meq/L
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
21/34
Treat the underlying causes
In mild hypo K : oral K preparation 600 -1200 meq/day
- small risk of hyper K
MANAGEMENT
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
22/34
Mild and severe hypo K : intravenous administration
do not give direct i.v injection : CRIME
intravenous drips peripheral or central venous line
10 20 meq/hr : into peripheral vein
> 40 meq/hr : into central vein
with ECG monitor
Monitoring K level carefully (every 4-6 hrs)
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
23/34
TAKE- HOME MESSAGE :
In diagnostic and treatment of water and electrolyte
dysbalance :
knowledge of basic renal physiology is useful for
understanding.
a promptly management and monitoring is needed
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
24/34
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
25/34
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
26/34
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
27/34
A Clinical Approach to Hyponatremia
Pseudohyponatremia
High protein
High Lipid
Hypo-osmotic
hyponatremia
Assess extracellular fluid
(volume) status
Jugular venous pressure
Postural blood pressure
Presence of edema
Hyperosmotic
hyponatremia
HyperglycaemiaMannitol
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
28/34
Acute Hyponatremia
Iatrogenic often post-op
Large volumes hypotonic fluids
Pain, hypotension, nausea,
drugs - may increase ADH
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
29/34
Acute Symptomatic Hyponatremia
Risk of cerebral oedema greater than the risk
treatment complications
Treat with furesemide and hypertonic saline (3%)
untilconvulsions subside usually means increasing [Na]
by 10%
3% NaCl @ 1-2 ml/kg/hr (for ~ 4 hrs) or 1.0-1.5
mEq/1/hr
Do not exceed correction of 1.5 meq/1/hr
Do not increase [Na] more than 12-15 meq/l/day
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
30/34
Chronic Hyponatremia
Often asymptomatic
No hurry
Water restriction
Treat th eunderlying cause if possible eg. Heart
failure, SIADH, thiazides
Increase In [Na] may be associated with subtle
improvements eg less falls
Tolvaptan trials-improved Mental Component of
SF-36 despite normal baseline
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
31/34
Severe hyponatremia
(
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
32/34
1. Because cerebral water is increased only byapproximately 10%
in severe chronic
hyponatremia, promptly increase the serum
sodium level by 10%, or by approximately
10 mmol/L
2. After the initial correction, do not exceed a
correction rate of 1 to 1.5 mmol/L hr
3. Do not increase the serum sodium by more
than 12 mmol/L in 24 hours
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
33/34
Hyponatremia and Hypernatremia
Sodium concentration is simply the ratio od
sodium to water; thus, hyponatremia (plasma
sodium (PNa] < 130 mmol/L) is Na+ loss or water
gain
In clinical practice, hyponatremia usually results
from gain of water or failure to excrete it, and cells
may or may not be swollen
-
8/8/2019 mia (kULIAH Khusus, Jumat 6 Juni 2008)
34/34
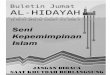
(Robert U, NEPHROLOGY Medical Progress December 2003)
K+ Secretion Along the Collecting Duct
AldosteroneAldosterone Distal NDistal N++
deliverydelivery
KK++
secretionsecretion
ooECFECF qq oo mm
qqECFECF oo qq mm
Conns syndrome (Conns syndrome (ooECF)ECF) oo oo oo
Diuretics (Diuretics (qqECF)ECF) oo oo oo
Addisons disease (Addisons disease (qqECF)ECF) qq qq qq
Acute glomerulonephritis (Acute glomerulonephritis (ooECF)ECF)
qq qq qq
Hyperkalemia vs. normokalemia occurs in oliguric vs.
non-oliguric acute renal failure
ECF = extracellular fluid