Embed Size (px)
Citation preview

QALYs: The Holy Grail?
Dominique Dubois MD FFPM FBCPMPhysician Specialist in Pharmaceutical Medicine
Vice-Chairman Pharmed post-graduate programme in Pharmaceutical Medicine and Medicines Development Sciences, Brussels, Belgium

Agenda
• Measuring utilities: strengths and weaknesses
• Where is the light(house)?
11/17/2016 Quality Adjusted Life Years 2

QALYs = Quality Adjusted Life Years
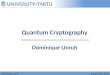
Quality Adjusted Life Years11/17/2016 3

One QALY is equal to 1 year of life in perfect health
TIME
(Years)
1
0
4
0.5
INDEX (“utility level”)
2
0.6+0.4
5
+0.5
Lieven Annemans
Health economics for non-economists
Gent, Academia Press, 2008 (www.academiapress.be)
Quality Adjusted Life Years
1
11/17/2016 4

The State of the Debate on QALYs
“Different methods for valuing health yield different results and this needs to be better understood”
Quality Adjusted Life Years
Toward a Consensus on the QALYMichael Drummond, Diana Brixner, Marthe Gold, Paul Kind, Alistair McGuire,
Erik Nord, (Consensus Development Group)
V A L U E I N H E A L T H Volume 12 • Supplement 1 • 2009 S31–S35
11/17/2016 5

Quality Adjusted Life Years
Nuijten MJC and Dubois DJ (2011) Cost-utility analysis: current methodological issues and
future perspectives. Front. Pharmacol. 2:29. doi: 10.3389/fphar.2011.00029
“Cost–effectiveness of a new pharmaceutical may depend heavily on underlying methodological choices for measurement of QALYs.”
11/17/2016 6

Quality Adjusted Life Years
QALY Assessment for Healthcare Decision Making
Should Be Abandoned”
http://www.echoutcome.eu/index.php
http://www.echoutcome.eu/images/Echoutcome__Leaflet_Guidelines___final.pdf
Final conference of the ECHOUTCOME project held in Brussels on January 25th, 2013
11/17/2016 7
“Given the overwhelming methodological limitations,

Relative importance of decision criteria according to Belgian citizens
Added value of new interventions:
The general public gives the highest weight to
the impact on quality of life.
Quality Adjusted Life Years
Cleemput I, Devriese S, Kohn L, Devos C, van Til J, Groothuis-Oudshoorn K, Vandekerckhove P, Van de Voorde C. Incorporating
societal preferences in reimbursement decisions – Relative importance of decision criteria according to Belgian citizens. Health
Services Research (HSR) Brussels: Belgian Health Care Knowledge Centre (KCE). 2014. KCE Reports 234. D/2014/10.273/91.
11/17/2016 8

INCORPORATING SOCIETAL PREFERENCES INREIMBURSEMENT DECISIONS
RELATIVE IMPORTANCE OF DECISION CRITERIA ACCORDING TO BELGIAN CITIZENS
• In the appraisal of therapeutic need, the general public as well as the policy makers gave the highest weight to the current quality of life. For the general public, the inconvenience of current treatment is more important than the impact of the disease on life expectancy, despite current treatment. This is the other way around for the decision makers.
• In the appraisal of the added value of new interventions, the general public gives the highest weight to the intervention’ impact on quality of life, followed by its impact on the prevalence of the disease and on life expectancy. Decision makers have the same preference order, but their weight for the impact on life expectancy is relatively larger than in the general public.
11/17/2016 Quality Adjusted Life Years 9
Cleemput I, Devriese S, Kohn L, Devos C, van Til J, Groothuis-Oudshoorn K, Vandekerckhove P, Van de Voorde C. Incorporating
societal preferences in reimbursement decisions – Relative importance of decision criteria according to Belgian citizens. Health
Services Research (HSR) Brussels: Belgian Health Care Knowledge Centre (KCE). 2014. KCE Reports 234.
D/2014/10.273/91.

How to Measure?

Types of HRQL measures
1. Generic profile measures: SF-36
2. Condition/Disease-specific measures
3. Direct preference measures
4. Indirect preference measures
Quality Adjusted Life Years11/17/2016 11

Medical Outcomes Study Short Form-36 (SF-36)
• Physical functioning (10 items)
• Role limitations/physical (4 items)
• Bodily Pain (2 items)
• General health perceptions (5 items)
• Vitality (4 items)
• Social functioning (2 items)
• Role limitations/emotional (3 items)
• Mental Health (5 items)
• Reported Health Transition
(How health is now compared to 1 year ago) (1 item)
Quality Adjusted Life Years11/17/2016 12

SF-36® Health Survey
Quality Adjusted Life Years11/17/2016 13

Types of HRQL measures
1. Generic profile measures: SF-36
2. Condition/Disease-specific measures
3. Direct preference measures
4. Indirect preference measures
Quality Adjusted Life Years11/17/2016 14

Direct Utility- or Preference based measures
- Standard gamble
- Time trade-off
- Visual analogue scales
Quality Adjusted Life Years11/17/2016 15

Quality Adjusted Life Years
Visual Analogue Scale
How good or bad is your health state today?
0
Worst imaginable
Health state
100
Best imaginable
Health state
11/17/2016 16

Time Trade-off
17
Alternative 1
Alternative 2HEALTHY 1.0
TIME
STATE i hi
DEAD 0x t
VALUE
Alternative 1: State i for time t (life expectancy followed by death)Alternative 2: Healthy for time x < t followed by deathPreference score for state i: hi = x/t
Quality Adjusted Life Years11/17/2016

Standard Gamble
18
Health State 1
Full Health
Immediate Death
Probability P (x%)
Probability 1-P
Certainty
Gamble
11/17/2016 Quality Adjusted Life Years

Indirect Utility- or Preference Based Measures
– SF-6D
– EQ-5D (EuroQol)
– Health Utility Index (HUI)
– Quality of Well-Being (QWB)
Quality Adjusted Life Years11/17/2016 19

SF-6D
Physical functioning
Role limitations
Social functioning
Pain
Mental health
Vitality
Quality Adjusted Life Years11/17/2016 20

EQ-5D
Quality Adjusted Life Years
Mobility
Self-care
Usual activities
Pain/
discomfort
Anxiety/
depression
11/17/2016 21

National Institute for Health and Care Excellence
Quality Adjusted Life Years11/17/2016 22

EQ-5D Descriptive system and EQ 5D VAS
Quality Adjusted Life Years11/17/2016 23

EQ-5D descriptive system
• Mobility
• Self-care
• Usual activities (eg work, study, housework, family or leasure activities)
• Pain/discomfort
• Anxiety/Depression
• Each (single item) dimension has 3 levels:
– No problems
– Some problems
– Severe problems
17-nov-16 24

EQ-5D Descriptive System1. Mobility
I have no problems in walking about
I have some problems in walking about
I am confined to bed
2. Self-care
I have no problems with self-care
I have some problems washing or dressing myself
I am unable to wash or dress myself
3.Usual Activities
I have no problems with performing my usual activities
(e.g. work, study, housework, family or leisure activities)
I have some problems with performing my usual activities
I am unable to perform my usual activities
4.Pain/Discomfort
I have no pain or discomfort
I have moderate pain or discomfort
I have extreme pain or discomfort
5.Anxiety/Depression
I am not anxious or depressed
I am moderately anxious or depressed
I am extremely anxious or depressed
Quality Adjusted Life Years
Please tick one
11/17/2016 25

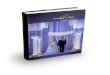
EQ-5D Scoring Algorithm
Full health 1.00 Constant term (for any dysfunctional state): -0.081 Mobility:
Level 2 -0.069 Level 3 -0.314
Self-care: Level 2 -0.104 Level 3 -0.214
Usual activities: Level 2 -0.036 Level 3 -0.094
Pain or discomfort: Level 2 -0.123 Level 3 -0.386
Anxiety or depression Level 2 -0.071 Level 3 -0.236
N3 (level 3 occurs within at least one dimension) -0.269
Quality Adjusted Life Years
Dolan P, Medical Care 35 (11): 1095-1108, (1997)
11/17/2016 26

EQ-5D Estimated value for state 12123
Full health 1.00
Constant term (for any dysfunctional state): -0.081
Mobility: Level 1 -0
Self-care: Level 2 -0.104
Usual activities: Level 1 -0
Pain or discomfort: Level 2 -0.123
Anxiety or depression: Level 3 -0.236
N3 (level 3 occurs within at least one dimension) -0.269
Estimated Value for state 12123: 0,187
Quality Adjusted Life Years
Dolan P, Medical Care 35 (11): 1095-1108, (1997
11/17/2016 27

Patient Reported Outcome Measures (PROMs)
Quality Adjusted Life Years
http://www.hscic.gov.uk/catalogue/PUB17201
Provisional Monthly Patient Reported Outcome Measures (PROMs) in England – April 2014 to November 2014
Publication date: April 09, 2015
11/17/2016 28

5 Things You Should Do with EQ5D Data
https://www.ohe.org/news/5thingsyoushoulddoeq5ddata
Friday, 29 January 2016Written by Professor Nancy Devlin, Director of Research at
OHE and member of the EuroQol Group

5 Things You Should Do with EQ5D Data
1. What not to do – don’t skip straight to ‘utilities’ or use of scores of any kind to summarise patients’ data
2. Look at patients’ responses to the question items (dimensions). Good, old fashioned descriptive statistics …
11/17/2016 Quality Adjusted Life Years 30

5 Things You Should Do with EQ5D Data
3. Summarising change without using value sets
– Their health state is better
– Their health state is worse
– Their health state is exactly the same
– The changes in health are ‘mixed’: better on one dimension, but worse on another.
11/17/2016 Quality Adjusted Life Years 31

5 Things You Should Do with EQ5D Data
4. Use your EQ-VAS data!
5. Last but not least: if you do need to use a value set to summarise your EQ5D data – e.g., for estimating QALYs – make sure you do sensitivity analysis to alternative value sets.
11/17/2016 Quality Adjusted Life Years 32

Quality Adjusted Life Years11/17/2016 34

European Network for Health Technology Assessment
Endpoints used for relative effectiveness assessment of pharmaceuticals:
HEALTH-RELATED QUALITY OF LIFE and UTILITY MEASURES
Quality Adjusted Life Years
EUnetHTA Joint Action WP5 – Relative Effectiveness Assessment (REA) of
Pharmaceuticals – Model for Rapid Relative Effectiveness Assessment of
Pharmaceuticals, February 2013, Final version
11/17/2016 35

Health-related quality of life and utility measures
• A general recommendation applicable to all types of Relative Effectiveness Assessment (REA), irrespective of their particular purpose, is to require the inclusion of a disease or population specific AND a generic HRQL measure for most adequately capturing the impact of a disease on daily life.
• In case there is a need for the calculation of QALYs, a utility measure (Time Trade-Off or Standard Gamble) OR generic HRQL instrument associated with a reference set of utility values is recommended.
Quality Adjusted Life Years11/17/2016 36

11/17/2016 Quality Adjusted Life Years 37

Health-utility data may be generated using one of the following categories of instruments
1. A generic preference-based measure (PBM) (e.g., EQ-5D, Health Utilities Index [HUI], Short-Form Six-Dimensions [SF-6D, derived from SF-36], 15D, Assessment of Quality of Life [AQoL], or Quality of Well-being [QWB])
2. A condition-specific PBM (e.g., the Asthma Quality of Life Utility
Index [AQL-5D] or the European Organization for Research and
Treatment of Cancer eight dimensions [EORTC-8D]);
3. A non–preference-based, condition-specific patient-reported
outcome measure mapped onto a generic, preference-based
measure
11/17/2016 Quality Adjusted Life Years 38
V A L U E IN HE A L T H 1 9 ( 2 0 1 6 ) 7 0 4 – 7 1 9

Quality Adjusted Life Years
QALY: The Holy Grail?
MEASURING IS KNOWING ?
IT’s ALL ABOUT THE PATIENT(S) !
11/17/2016 39

PHARMED
http://www.frontiersin.org/Pharmaceutical_Medicine_and_Outcomes_Research
THANK YOU !
Quality Adjusted Life Years
11/17/2016 40