Embed Size (px)
Citation preview

Does angiography help in risk
stratification?
Derek Harrington
Maidstone and Tunbridge Wells NHS Trust

Kent and Sussex Hospital, Tunbridge Wells
Medium sized DGH 300,000 population
Two Consultant Cardiologists
Derek Harrington
Clive Lawson

Derek and Clive

Does angiography help in risk
stratification?
Should coronary angiography be
performed on ACS patients in
DGHs without on site PCI?

0 1 2 3 4 5 6Time (months)
0
4
8
12
16
20
% P
atie
nts
with
10
en
dp
oin
t
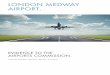
CONSINV
O.R 0.78
95% CI (0.62, 0.97)
p=0.025
19.4%
15.9%
TACTICS TIMI 18
Cannon et al NEJM 2001

Invasive ACS - the DGH view
• Identify all high / intermediate risk
patients
• Appropriate medical therapy
• Arrange angiography / revascularisation
within 48 hours

Invasive ACS - the DGH view
• 48 hours not achieved in many tertiary
centres
• Miller, Lipscomb, Curzen 2003
– Waiting time 13 days vs 5 days
– “This inequity of access is determined by
postcode rather than clinical priority”

Invasive ACS – the DGH view
• Large numbers of patients, 10 per week
– “U&Es, Trop I”
• Long transfer time (3 – 4 weeks, Mean 22 days)
• Potentially one ward full of patients waiting transfer for angiography / revascularisation
• Majority asymptomatic

Alternative approaches
• Further risk stratify, exercise testing etc,
with outpatient investigation for some

Local Coronary Angiography

TW ACS
• The majority of patients undergo
angiography within one week
• Decision to discharge etc, based upon
anatomy + other risk factors

DGH angiography, arguments
against
• Too dangerous in DGH
• Large numbers of patients will require a
second procedure
• Angiography will delay definitive
treatment

Too dangerous in the DGH
• Common sense
• TW n=215 complications=0
• Published series suggest that DGH
angiography is safe
• Large programme of DGH catheter
laboratories
• Generally more senior operators

DGH angiography, arguments
against
• Too dangerous in DGH
• Large numbers of patients will require a
second procedure
• Angiography will delay definitive
treatment

Need for a second procedure
PCI CABG Medical
TACTICS 41 20 39
FRISC II 43 35 22
RITA III 35 21 44
TW 44 31 25
Approx 60% patients will not require further angiography

TACTICS – medical treatment
Invasive
strategy
Conservative
strategy
MACE 10.8 10.3
Death or Non
fatal MI5.9 5.1

DGH angiography, arguments
against
• Too dangerous in DGH
• Large numbers of patients will require a
second procedure
• Angiography will delay definitive
treatment


Angiography delays definitive
treatment
• LMS
• Proximal LAD
• 3VD – Early surgical referral
Rapid Transfer

Angiography will delay definitive
treatment
• Home for early “elective PCI”
• Earlier identification of very high risk
and surgical patients
• More tertiary referral beds for
“interventional transfers”

Conclusions
• Safe in DGH
• Some patients will require a second procedure
• Early Angiography may enable rapid revascularisation
• Marked reduction in bed occupancy, happier patients
• A prelude to DGH angioplasty