Embed Size (px)
Citation preview

Post kidney transplantation VUR
Doaa M. SalahLecturer of Pediatrics
2015

PrevalenceRisk Factors.Impact on graft functionPreventionManagement Center study
VUR post KTX

PrevalenceRisk Factors.Impact on graft functionPreventionManagement Center study
VUR post KT

The exact incidence of post TX VUR unknown as most cases asymptomatic and the only diagnostic tools is VCUG (not routine)

In pediatrics, frequency is 36%, 34%, 55% in 3 studies done in 1987, 1999, 2000 respectively compared to 2- 80% in adults.
Prevalence

PrevalenceRisk Factors.Impact on graft functionPreventionManagement Center study
VUR post KT

(Bootsma., etal.,The clinical significance of VUR into transplanted kidney,clinical. Transplantation. 1987;1: 311-315).
Risk Factors
Primary disease
Bladder capacity
Duration of RRT
Procedure of ureteral
anastomosis
Donor Type

The gender has no impact on VUR rate after renal transplant.
But male liable to develop post transplant retention while female have increased risk of UTI.
(Farr et al., transplantaion,2014)

Primary Reflux


Even after surgical correction of VUR before transplantation the frequency of f UTI remained higher than that in kidney transplant recipients without VUR.
J Urol. 2006; 175(4):1490-2
Does pre-transplantation antireflux surgery eliminate post-renal transplantation pyelonephritis in children?

Bladder capacity decrease because of long term dialysis, it exceed 150 ml at 1 year post transplantation
A small bladder can be used in renal transplantation but it may increase the risk of VUR.
(Takamitsue et al., Correlation between pre transplant dialysis duration, bladder capacity and prevelance of VUR to the graft,
Transplantation.2011;92:311-315)

Before implantation of donor kidney in the recipient
(International Journal of Urology, 2011)
Cystoplasty
Role of surgeon before TX is lower UT
Sterile Continent Compliant





The slandered is ureteroneocystostomy(trans vesical or extra vesical, antireflux and non antireflux) If double ureters…. managed as double blood supply to
some extend Other alternatives as ureteroenterostomy in intestinal
conduit or pouch or pyelovesicostomy if the native ureter and graft ureter are unsuitable for urinery tract reconstruction.
Urinary tract reconstruction in TX



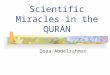
The Lich-Gregoir anastomosis is created by performing a cystotomy for 2 to 3 cm on the anterolateral surface of the bladder dome to expose mucosa of the bladder wall. A small incision is made in the mucosa. The transplanted ureter is trimmed and spatulated posteriorly. The mucosa of the bladder is sutured to the ureteral end with interrupted absorbable sutures. The detrusor muscle is closed over the anastomosis to create a submucosal tunnel with an antireflux mechanism

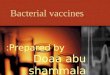
The Politano-Leadbetter anastomosis is created by performing a cystotomy on the anterior side to visualize the interior of the bladder and expose the trigone. A second cystotomy is performed to create a new ureteric orifice. The transplanted ureter is tunneled submucosally for approximately 2 cm. The distal site is trimmed and spatulated anteriorly at an optimal length to ensure a tension-free anastomosis. The distal ureter is sutured to the bladder mucosa with interrupted absorbable stitches. The cystotomy is closed in two layers to ensure a watertight anastomosis.

LG significantly associated with lower incidence of urinary leakage and hematuria but no significant difference in stricture or reflux
(Victor et al.,ureterovesical anastomosis techniques: systemic review and meta-analysis. Transplant international 2014)
Techniques of ureter vesical anastomosis

PrevalenceRisk Factors.Impact on graft functionPreventionManagement Center study
VUR post KT

Controversial
Impact on graft function

Immediate graft dysfunction (first week) Early graft dysfunction (1-12 week) Late acute graft dysfunction (>3monthes) Chronic graft dysfunction (years)
Graft Dysfunction


Nephrol.Dial.Transplant (2000);15: 1852-1858.


VUR increase the risk of UTI and pyelonephriyis VUR possibly lead to hypertenstion and CAN
(Howie et al., Reflux nephropathy in transplants. Pediatri Nephrol 2002;17: 485)
(Favi et alm, long term clinical impact of VUR in KTX. Transplant Proceedings 2009;41:1218)

PrevalenceRisk Factors.Impact on graft functionPreventionManagement Center study
VUR post KT


Lower UT evaluation
(voiding diary)
Prevention


Lower UT evaluation
VCUG(Detruser capacity, deformity, VUR , uretheral abnormality)
Prevention




Lower UT evaluation
VUDS (detruser evaluation: capacity, contractilitym, compliance, dysynergyia). Bladder deformity, VUR and uretheral deformability
Prevention



Studies evaluating VCUGs in asymptomatic renal transplant recipients have revealed VUR rates up to 86%
Pre protocol VCUG early after transplantation ??? The incidence of VUR is high although antireflux
procedures used for implantation
(American Journal of Transplantation 2013;13:130-135)
Prevention

Universal prophylaxis involves giving an antimicrobial agent to all patients.
Trimethoprim-sulfamethoxazole (TMP-SMX) is given universally to all transplant recipients who do not have sulfa allergies.
TMP-SMX is effective for the prevention of Pneumocystis pneumonia (PCP).
It provides effective prophylaxis against other pathogens, including Listeria monocytogenes and Toxoplasma gondii.
(Fishman et al., 1998)
Antibiotic Prophylaxis

PrevalenceRisk Factors.Impact on graft functionPreventionManagement Center study
VUR post KT

Routine functional studies not indicated in potential recipients Recipients with neurovesical dysfunction VCUG and
pressure flow urodynamic study with or without cystoscopy High pressure urine storage antimuscarinic
medications or CISC before TX Oliguric pt. start CISC before TX to allow teaching
the family Those unable to carry CISC urinery diversion
(suprapupic cath, conduit, pouch or augmentation)
(International Journal of Urology, 2011;18:185-193)
Bladder Dysfunction

Long term Ab prophylaxis is sufficient for the majority of cases with post TX VUR
Antibiotic Prophylaxis

Surgical intervention is only indicated in intractable cases
(recurrent graft UTI, UTI refractory to therapy with grade 4 to 5 reflux result in renal scaring or compromise graft function) Reimplantation Endoscopic injection of a bulking substance to the
muscular post wall of the ureter vesical junction
Surgery

PrevalenceRisk Factors.Impact on graft functionPreventionManagement Center study
VUR post KT

54 pediatric transplant recipient All received antibiotic prophylaxsis at least 6 mo
Obstructive uropathy diseases in 24% (included PUV 12.9%, vesicoureteric reflux 9.3%, neurogenic baldder 1.9%) 40% had UTI during their F/U period 54% of the episodes were in first 6 mo (40% had recurrent UTI, 2% simple non recurrent UTI,
50% asymptomatic bacturia, 9% had pyelonephritis) UTI significantlly higher in cases with primery obstructive
uropathy
Center Study

Febrile UTI represents 40.9% of the studied UTI group compared to 54.4% with no symptoms.
6 cases (27% of UTI cases had variable degrees of VUR )
The outcome (graft survival) was similar in UTI and non UTI cases. Although UTI tend to affect graft function in low GFR levels <60 ml/min/1.73m2

Thank you