Embed Size (px)
Citation preview
Do pathological changes in tau protein isoforms manifest in cerebrospinal fluid of tauopathy patients?
Development and validation of sensitive immuno-PCR assays
Rohan de Silva, DPhil
Reta Lila Weston InstituteUCL Institute of NeurologyLondon
Barcelona, November 2012
2
UCL Institute of Neurology/National Hospital of Neurologyand Neurosurgery
Queen Square
1 Wakefield Street
The need for diagnostic biomarkers in neurodegenerative disorders
• Definitive diagnosis is done post mortem• Accurate diagnosis important for treatment
options• Identification of prodromal cases crucial
for preventive intervention
3
• The tau protein and neurodegenerative disorders
4
• The tau protein and neurodegenerative disorders
• Current tau-based CSF assays
5
• The tau protein and neurodegenerative disorders
• Current tau-based CSF assays
• Sensitive immuno-PCR assays for CSF tau isoforms
6
7
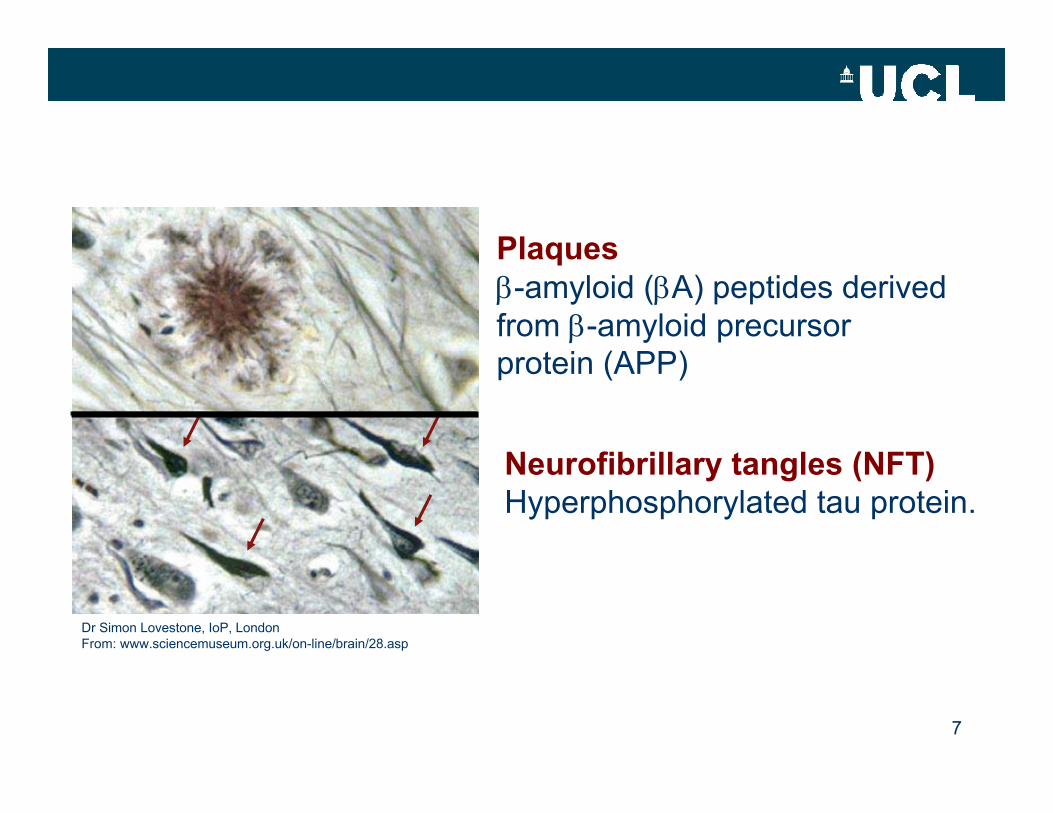
Dr Simon Lovestone, IoP, LondonFrom: www.sciencemuseum.org.uk/on-line/brain/28.asp
Plaquesβ-amyloid (βA) peptides derivedfrom β-amyloid precursorprotein (APP)
Neurofibrillary tangles (NFT)Hyperphosphorylated tau protein.
The tauopathiesAlzheimer’s diseaseALS/parkinsonism-dementia complexArgyrophilic grain diseaseCorticobasal degenerationCreutzfeld-Jakob diseaseDementia pugilisticaDiffuse neurofibrillary tangles with calcificationDown’s syndromeFTDP-17TGerstmann-Sträussler-Scheinker diseaseHallervorden-Spatz diseaseMyotonic dystrophyNiemann-Pick diseaseNon-Guamanian motor neuron disease with neurofibrillary tanglesPick’s diseasePostencephalitic parkinsonismPrion protein cerebral amyloid angiopathyProgressive subcortical gliosisProgressive supranuclear palsySupacute sclerosing panencephalitisTangle only dementia
8
Dr Simon Lovestone, IoP, LondonFrom: www.sciencemuseum.org.uk/on-line/brain/28.asp
9
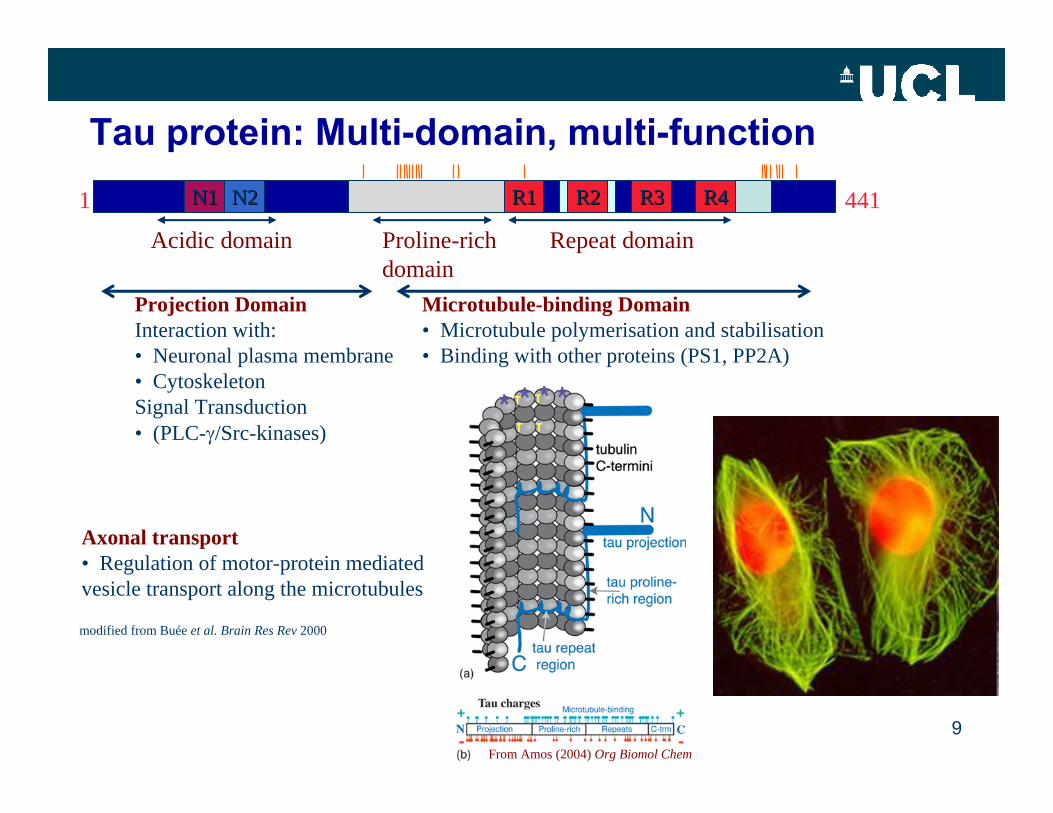
Tau protein: Multi-domain, multi-functionN1N1 N2N2 R2R2 R3R31 441R1R1 R4R4
Acidic domain Proline-rich domain
Repeat domain
Projection DomainInteraction with:• Neuronal plasma membrane• CytoskeletonSignal Transduction• (PLC-γ/Src-kinases)
Microtubule-binding Domain• Microtubule polymerisation and stabilisation• Binding with other proteins (PS1, PP2A)
modified from Buée et al. Brain Res Rev 2000
Axonal transport• Regulation of motor-protein mediated vesicle transport along the microtubules
From Amos (2004) Org Biomol Chem
10
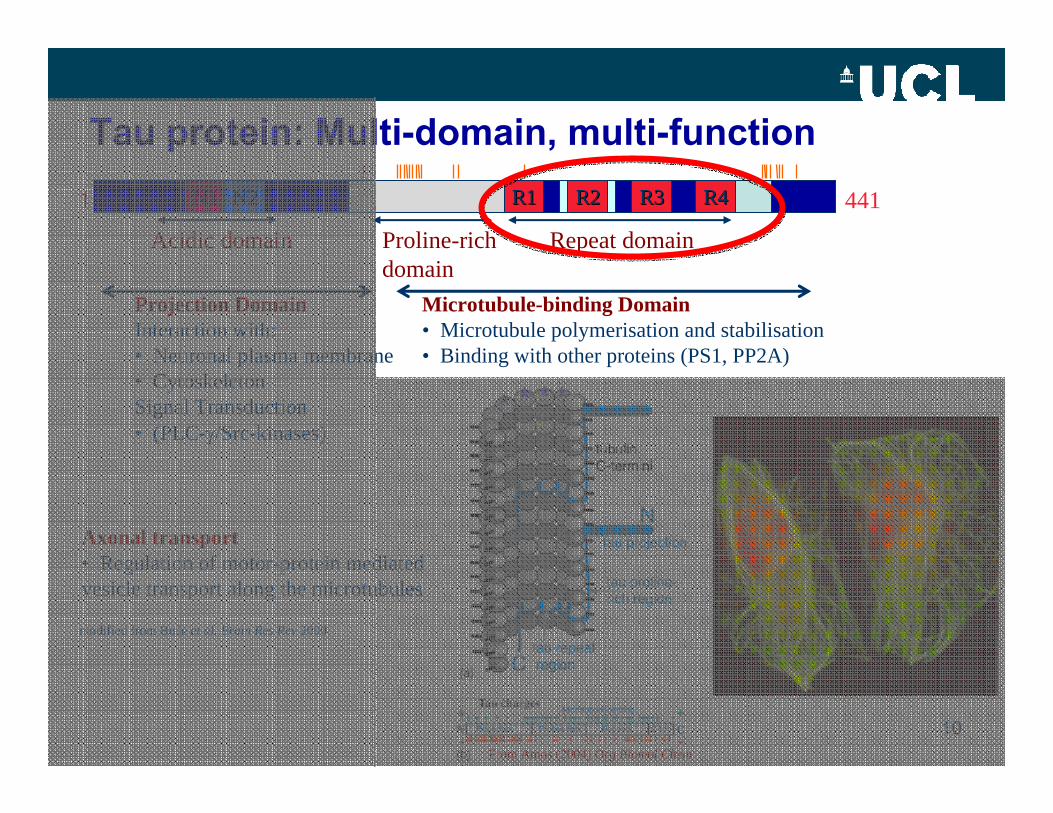
Tau protein: Multi-domain, multi-functionN1N1 N2N2 R2R2 R3R31 441R1R1 R4R4
Acidic domain Proline-rich domain
Repeat domain
Projection DomainInteraction with:• Neuronal plasma membrane• CytoskeletonSignal Transduction• (PLC-γ/Src-kinases)
Microtubule-binding Domain• Microtubule polymerisation and stabilisation• Binding with other proteins (PS1, PP2A)
modified from Buée et al. Brain Res Rev 2000
Axonal transport• Regulation of motor-protein mediated vesicle transport along the microtubules
From Amos (2004) Org Biomol Chem
11
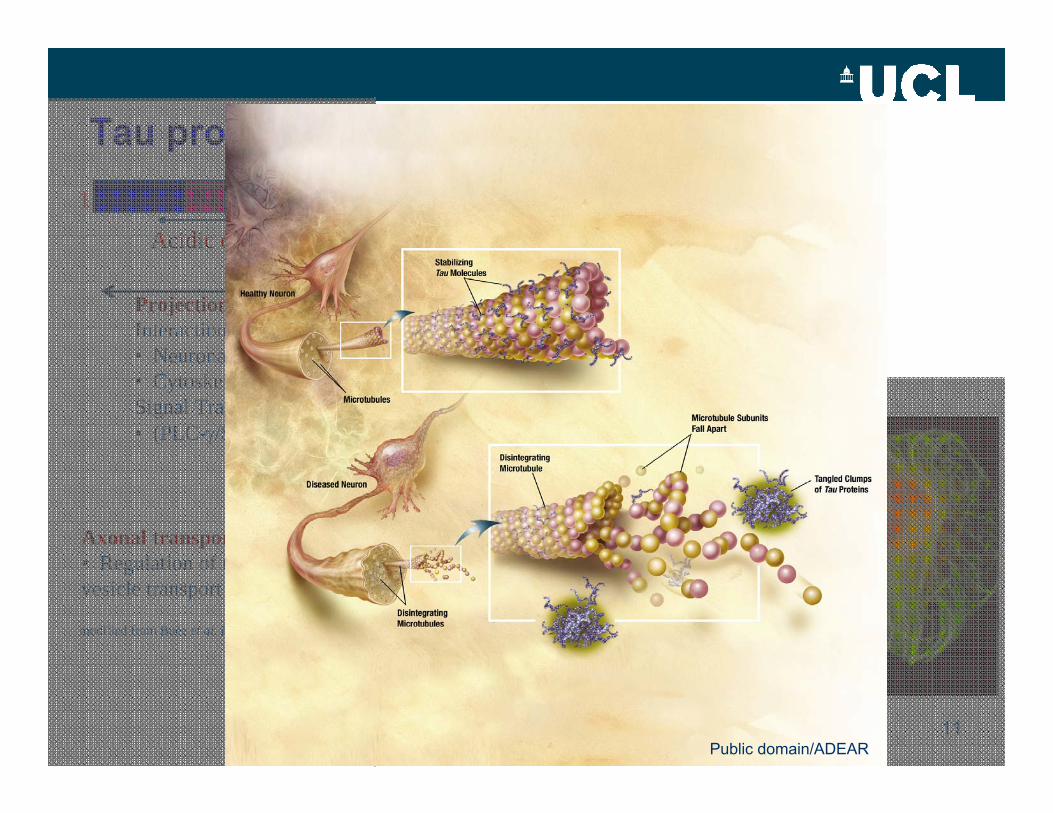
Tau protein: Multi-domain, multi-functionN1N1 N2N2 R2R2 R3R31 441R1R1 R4R4
Acidic domain Proline-rich domain
Repeat domain
Projection DomainInteraction with:• Neuronal plasma membrane• CytoskeletonSignal Transduction• (PLC-γ/Src-kinases)
Microtubule-binding Domain• Microtubule polymerisation and stabilisation• Binding with other proteins (PS1, PP2A)
modified from Buée et al. Brain Res Rev 2000
Axonal transport• Regulation of motor-protein mediated vesicle transport along the microtubules
From Amos (2004) Org Biomol Chem Public domain/ADEAR
1
1
1
1
1
1
441
412
383
410
381
352
2N,4R1N,4R
0N,4R
2N,3R1N,3R
0N,3R
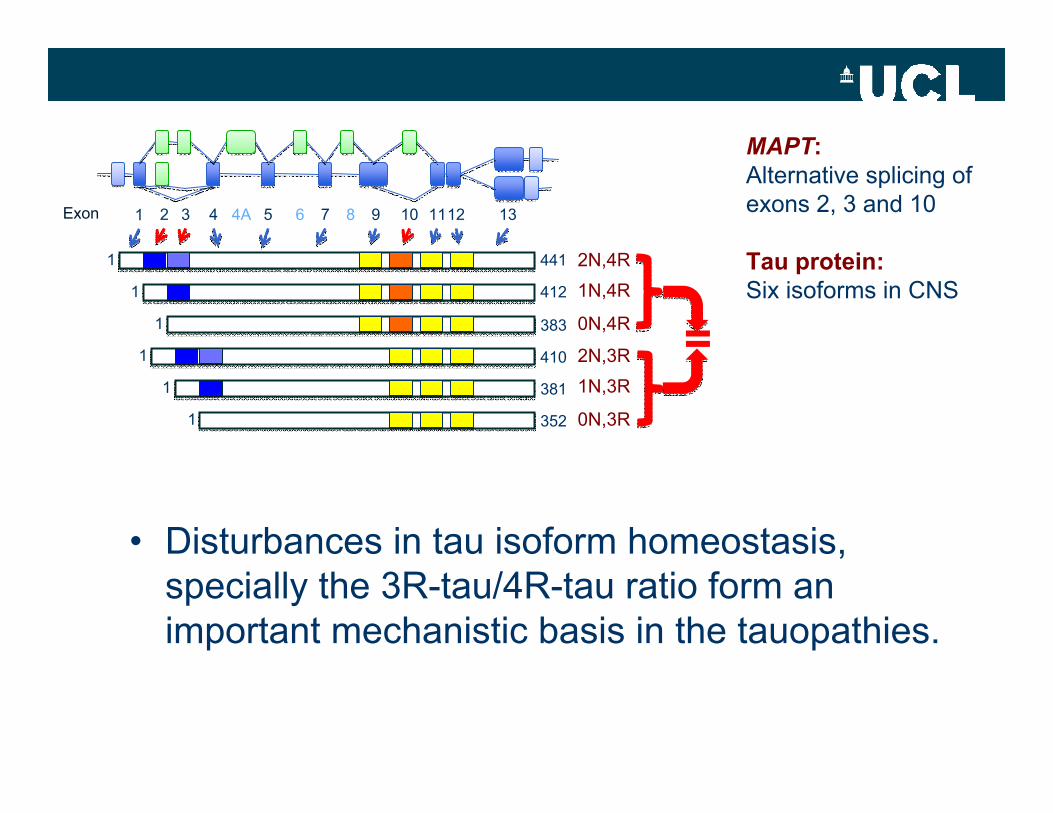
Exon 1 2 3 4 4A 5 6 7 8 9 10 1112 13
MAPT:Alternative splicing of exons 2, 3 and 10
Tau protein:Six isoforms in CNS
=
• Disturbances in tau isoform homeostasis, specially the 3R-tau/4R-tau ratio form an important mechanistic basis in the tauopathies.
13
1
1
1
1
1
1
441
412
383
410
381
352
2N,4R1N,4R
0N,4R
2N,3R1N,3R
0N,3R
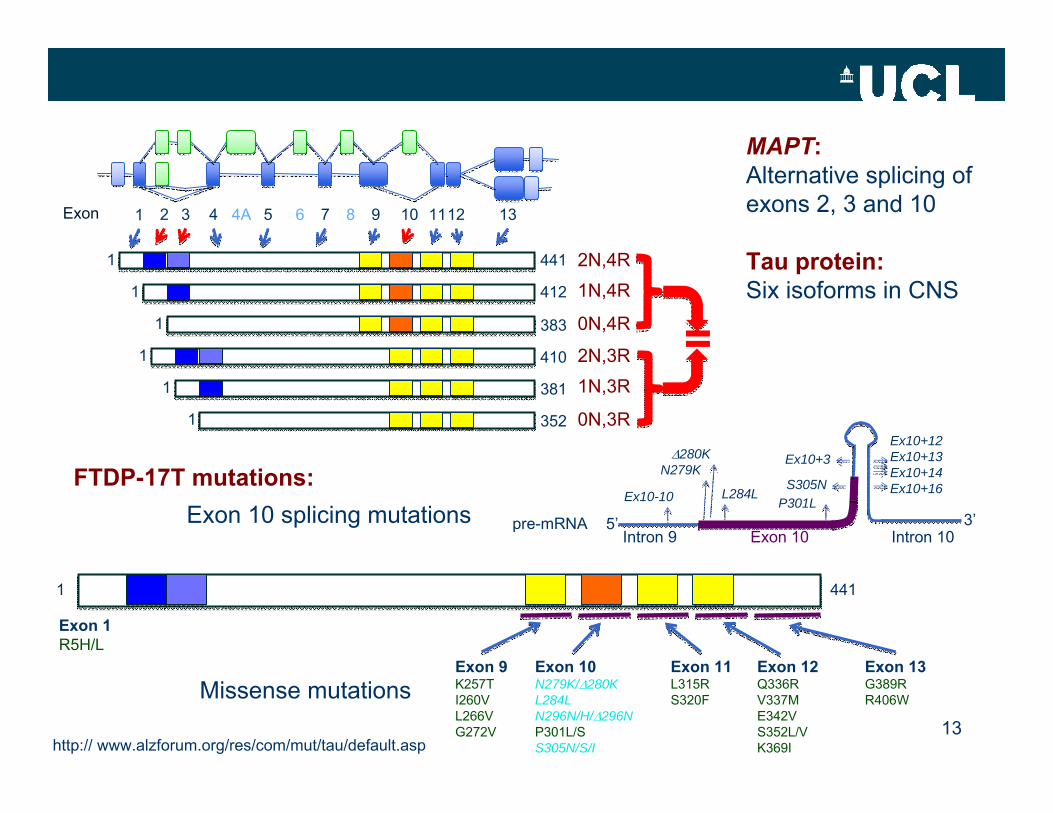
Exon 1 2 3 4 4A 5 6 7 8 9 10 1112 13
5’ 3’pre-mRNAIntron 9 Exon 10 Intron 10
Ex10+16
Ex10+12Ex10+13Ex10+14
Ex10+3
S305NP301L
L284L
Δ280KN279K
Ex10-10Exon 10 splicing mutations
1 441
Exon 1R5H/L
Exon 9K257TI260VL266VG272V
Exon 10N279K/Δ280KL284LN296N/H/Δ296NP301L/SS305N/S/I
Exon 11L315RS320F
Exon 12Q336RV337ME342VS352L/VK369I
Exon 13G389RR406WMissense mutations
FTDP-17T mutations:
http:// www.alzforum.org/res/com/mut/tau/default.asp
MAPT:Alternative splicing of exons 2, 3 and 10
Tau protein:Six isoforms in CNS
=
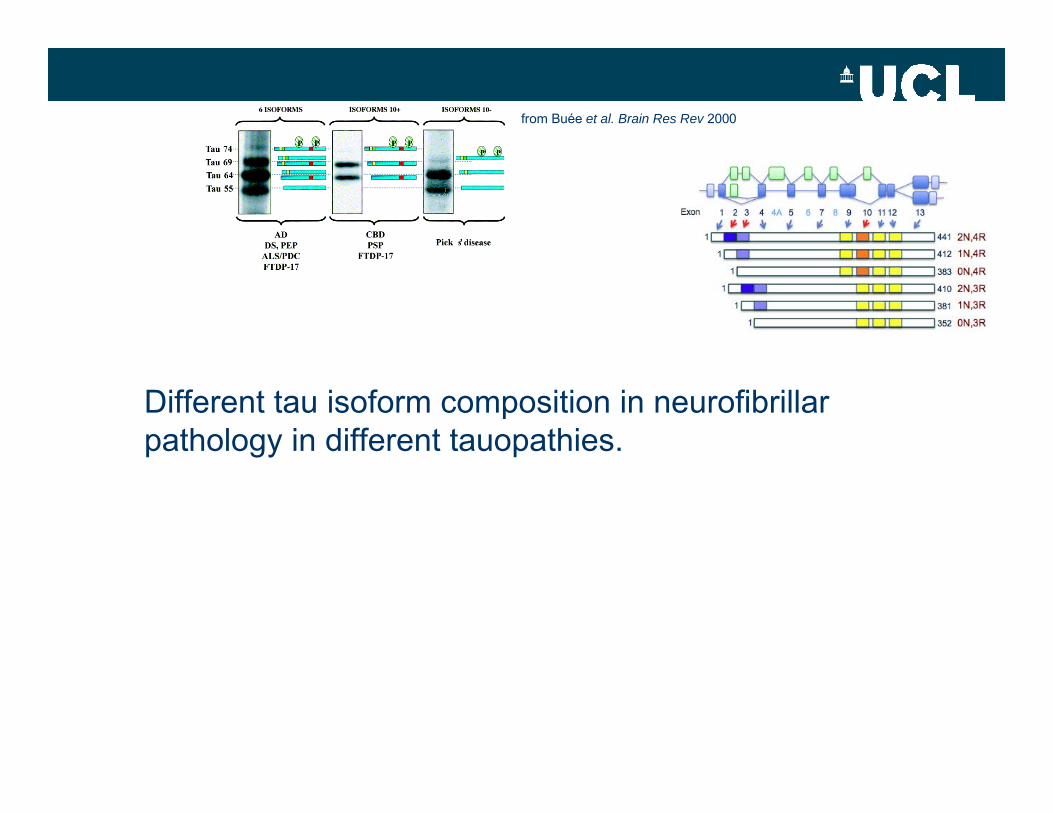
from Buée et al. Brain Res Rev 2000
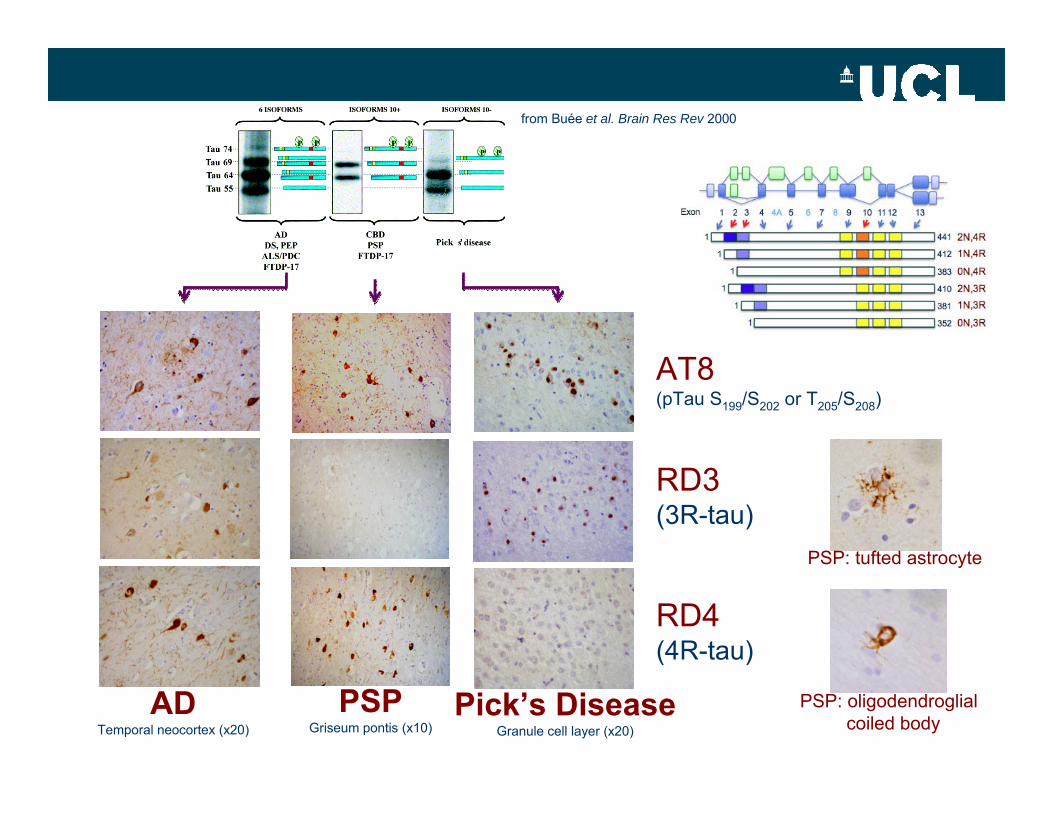
Different tau isoform composition in neurofibrillarpathology in different tauopathies.
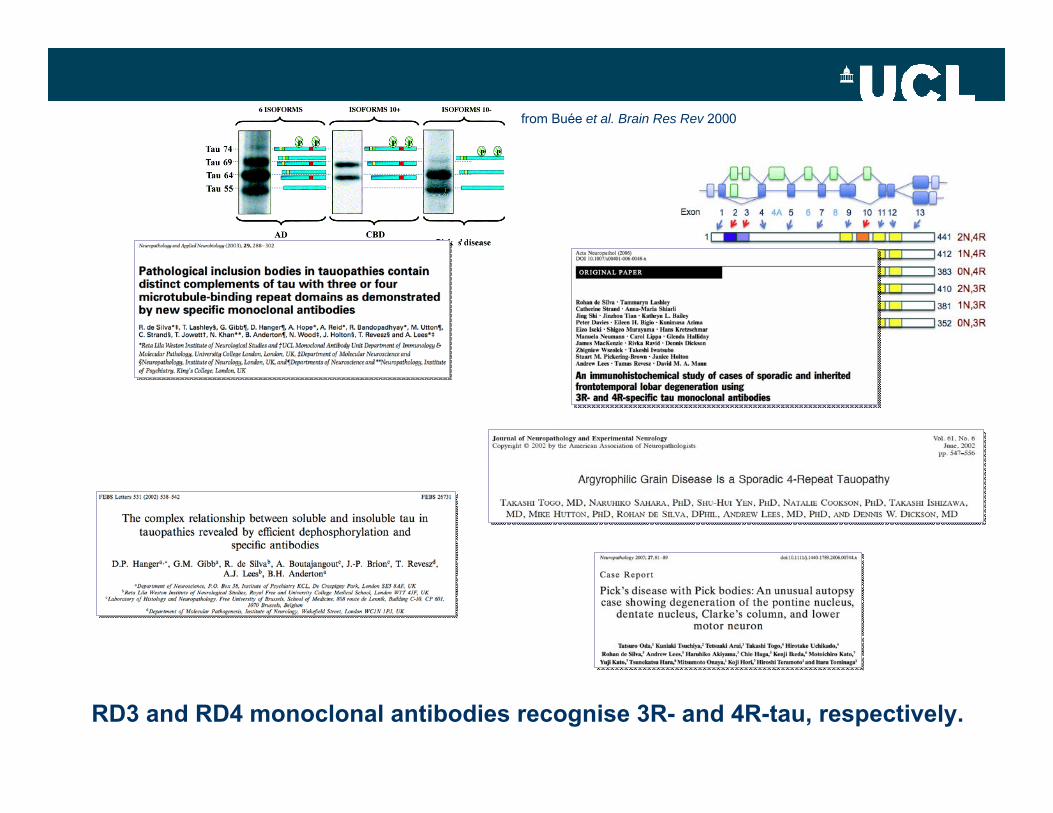
from Buée et al. Brain Res Rev 2000
RD3 and RD4 monoclonal antibodies recognise 3R- and 4R-tau, respectively.
from Buée et al. Brain Res Rev 2000
ADTemporal neocortex (x20)
PSPGriseum pontis (x10)
Pick’s DiseaseGranule cell layer (x20)
AT8(pTau S199/S202 or T205/S208)
RD3(3R-tau)
RD4(4R-tau)
PSP: tufted astrocyte
PSP: oligodendroglial coiled body
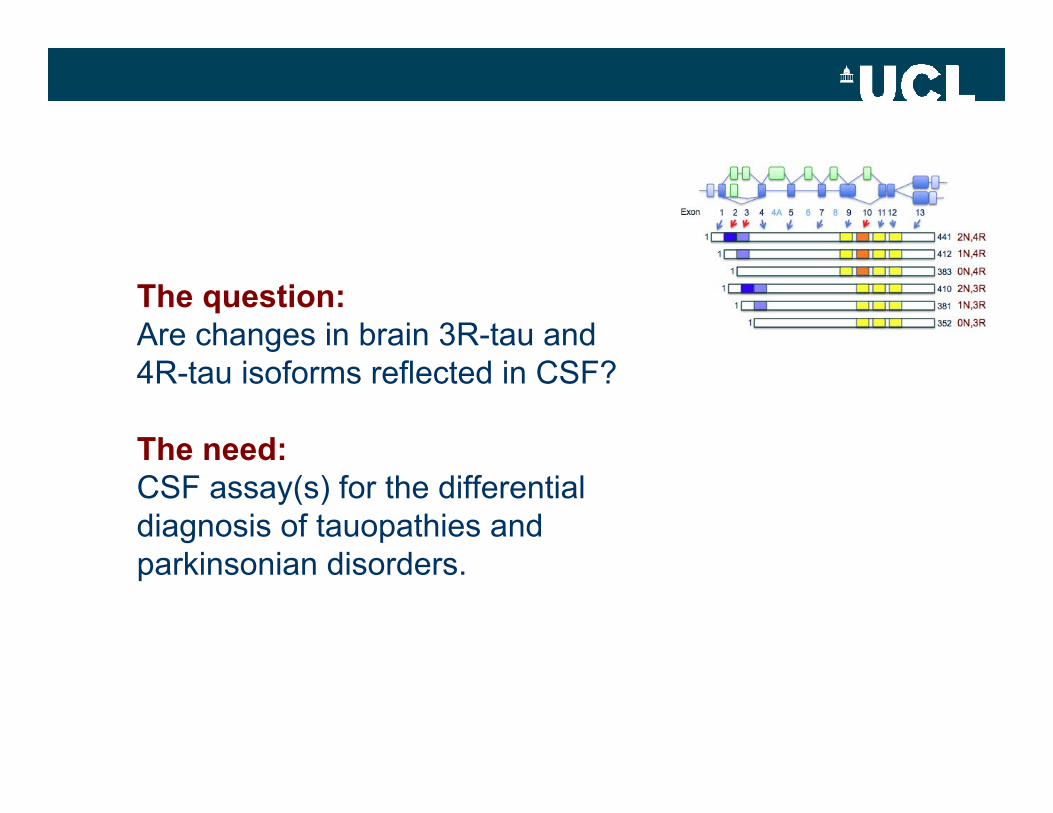
The question: Are changes in brain 3R-tau and 4R-tau isoforms reflected in CSF?
The need: CSF assay(s) for the differential diagnosis of tauopathies and parkinsonian disorders.
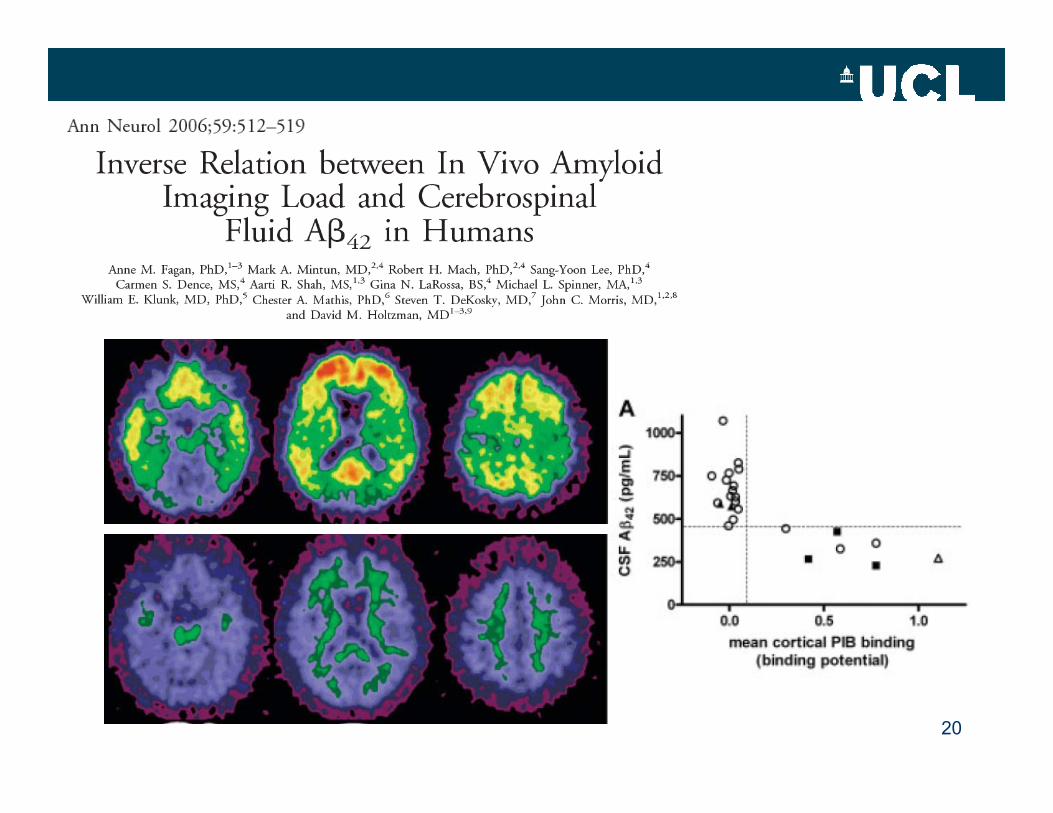
CSF biomarkers in AD
• Decreased Aβ42 due to:
– Increased sequestration– Aβ oligomerisation– Unknown matrix effects (Slemmon et al 2012 J Neurochem)
• Increased tau and phospho-tau (p-Thr181) due to:
– Axonal degeneration– Active release
18
CSF biomarkers in AD
• Decreased Aβ42 due to:
– Increased sequestration– Aβ oligomerisation– Unknown matrix effects (Slemmon et al 2012 J Neurochem)
• Increased tau and phospho-tau (p-Thr181) due to:
– Axonal degeneration– Active release
19
20
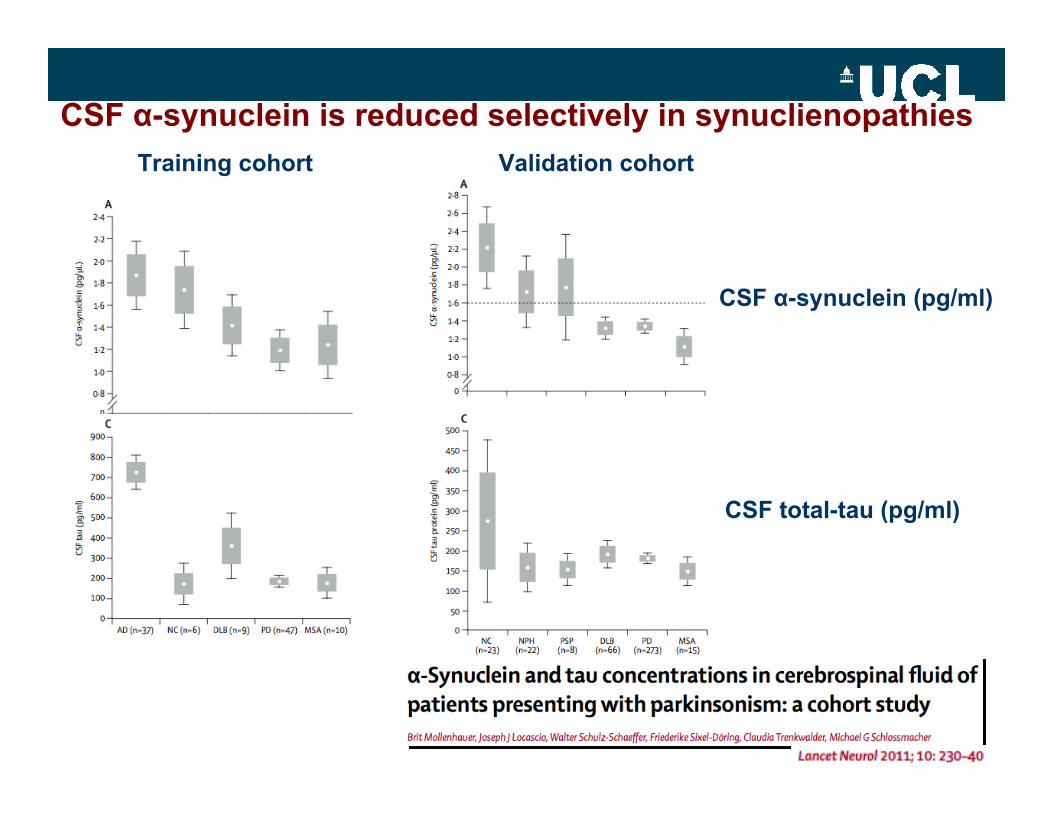
CSF α-synuclein is reduced selectively in synuclienopathies
21
CSF α-synuclein (pg/ml)
CSF total-tau (pg/ml)
Training cohort Validation cohort
CSF biomarkers in AD
• Decreased Aβ42 due to:
– Increased sequestration– Aβ oligomerisation– Unknown matrix effects (Slemmon et al 2012 J Neurochem)
• Increased tau and phospho-tau (p-Thr181) due to:
– Axonal degeneration– Active release
22
CSF biomarkers in AD
• Decreased Aβ42 due to:
– Increased sequestration– Aβ oligomerisation– Unknown matrix effects (Slemmon et al 2012 J Neurochem)
• Increased tau and phospho-tau (p-Thr181) due to:
– Axonal degeneration– Active release
23
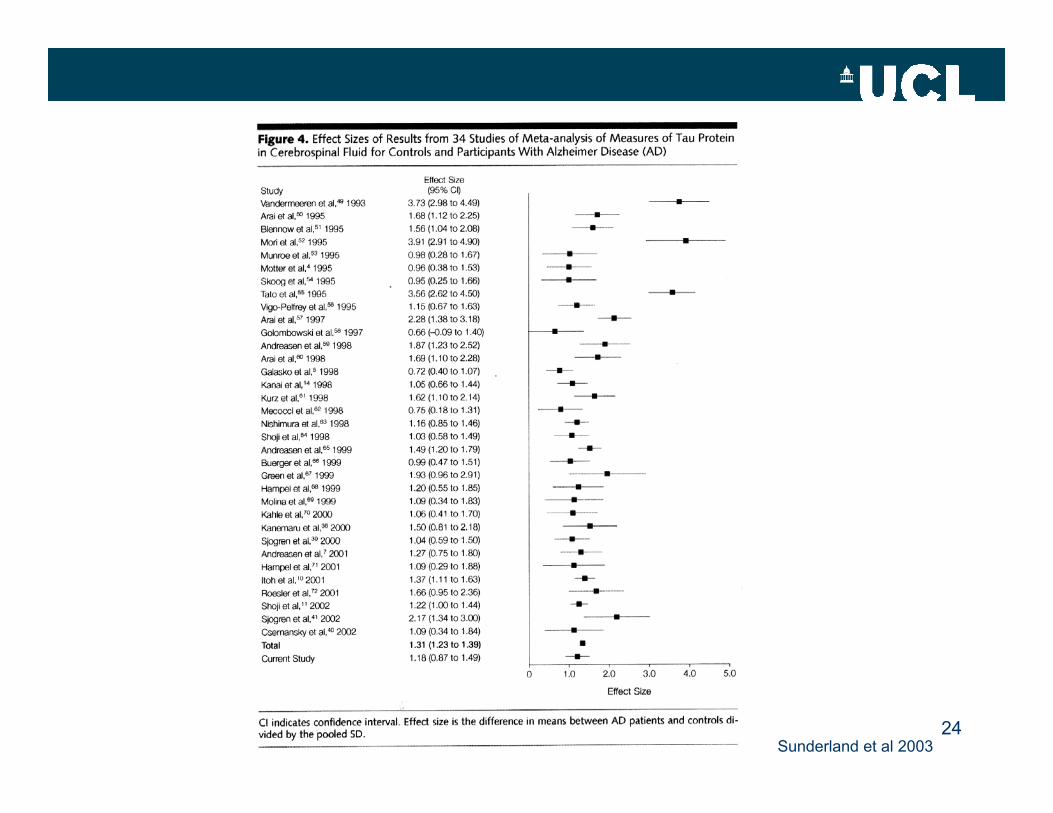
24Sunderland et al 2003
25
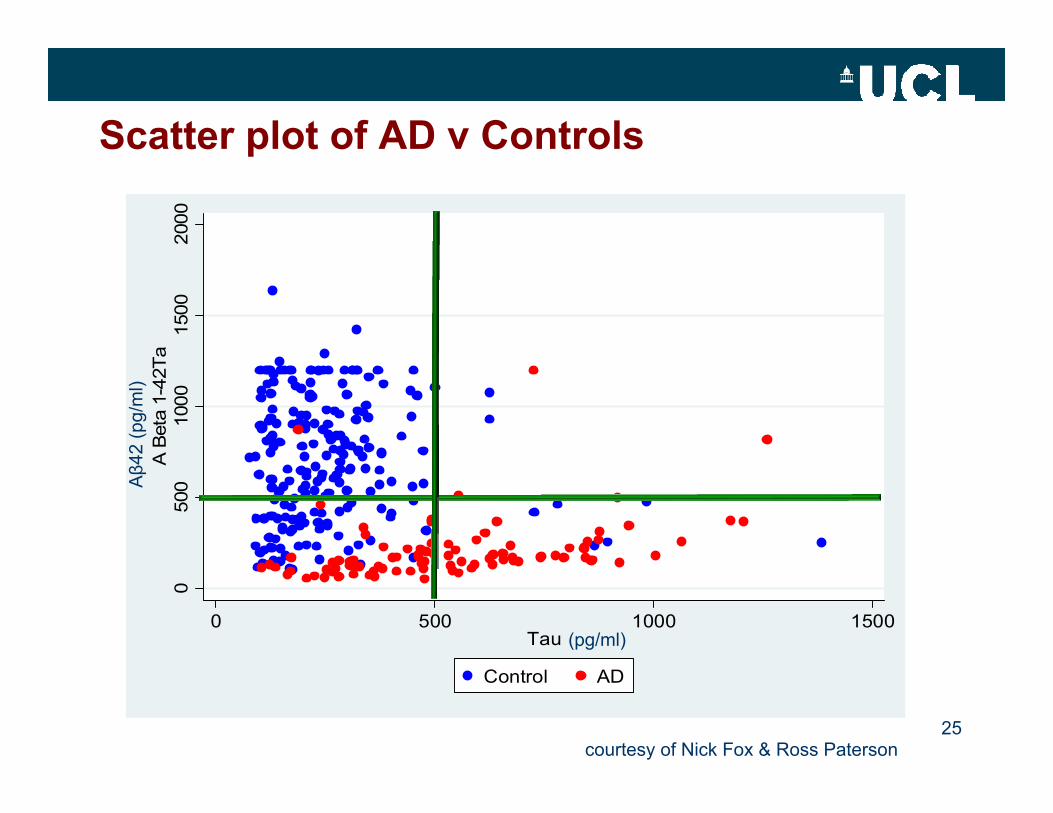
Scatter plot of AD v Controls0
500
1000
1500
2000
A B
eta
1-42
Ta
0 500 1000 1500Tau
Control AD
(pg/ml)
Aβ42
(pg/
ml)
courtesy of Nick Fox & Ross Paterson
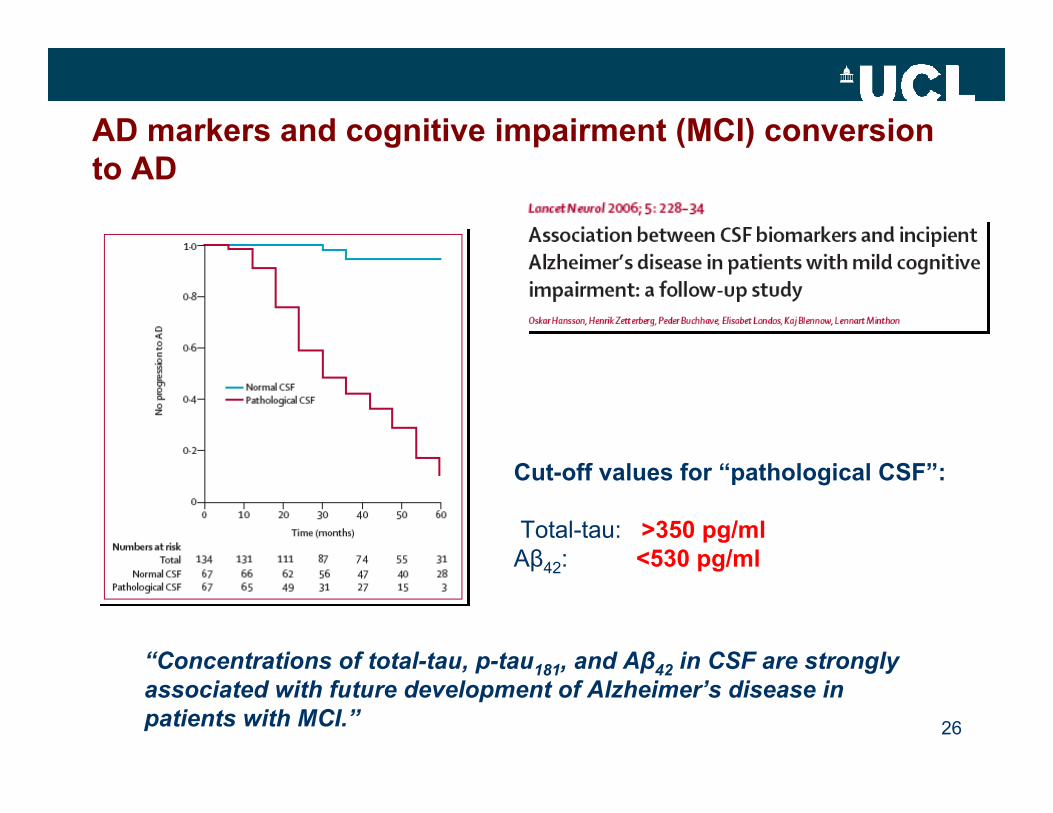
AD markers and cognitive impairment (MCI) conversion to AD
26
Cut-off values for “pathological CSF”:
Total-tau: >350 pg/mlAβ42: <530 pg/ml
“Concentrations of total-tau, p-tau181, and Aβ42 in CSF are strongly associated with future development of Alzheimer’s disease in patients with MCI.”
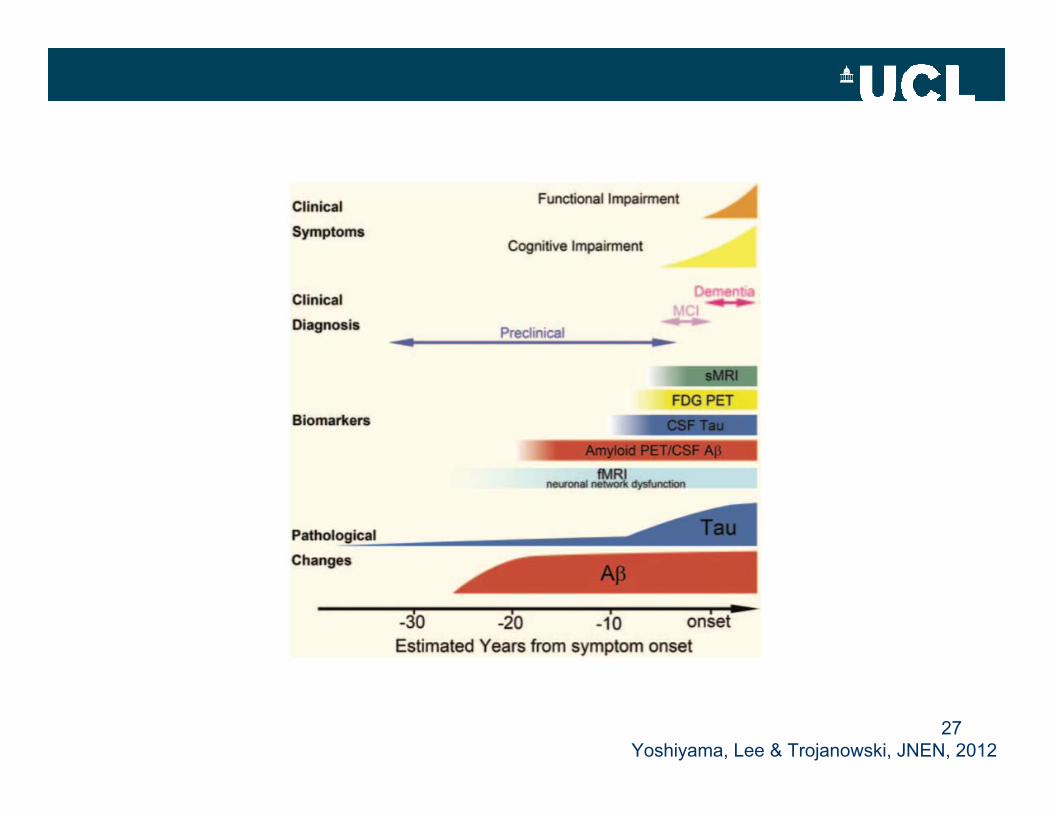
27Yoshiyama, Lee & Trojanowski, JNEN, 2012
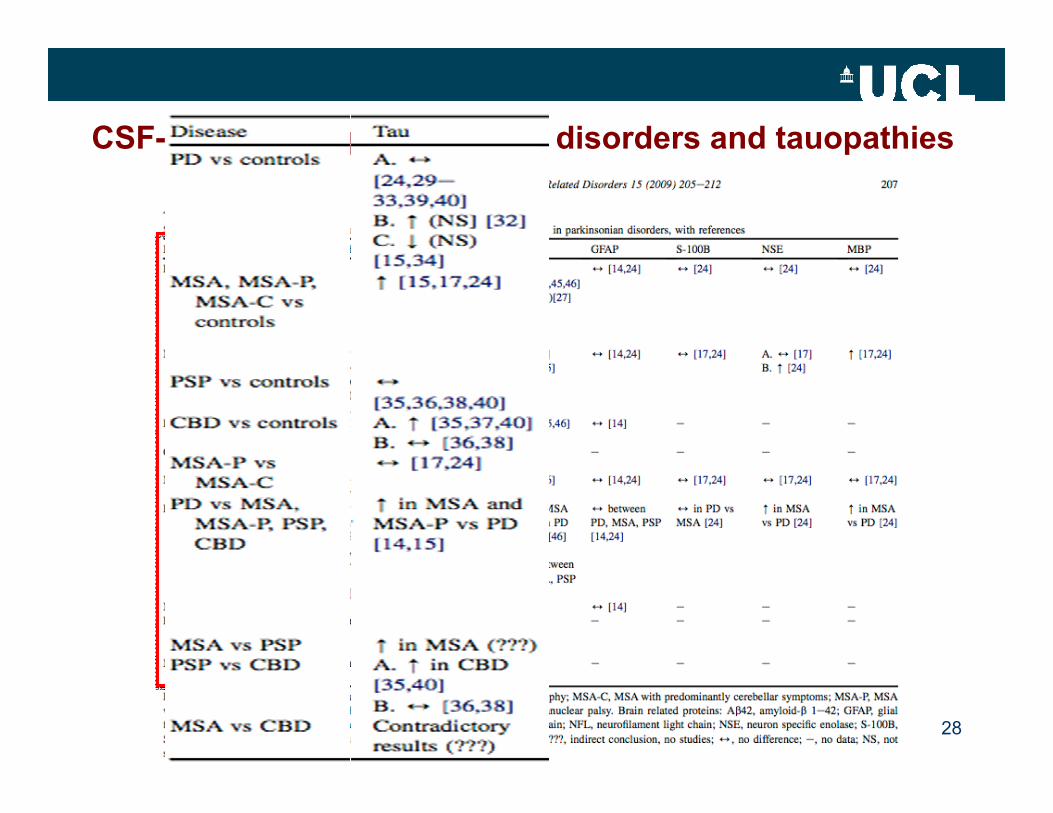
CSF-tau in other parkinsonian disorders and tauopathies
28
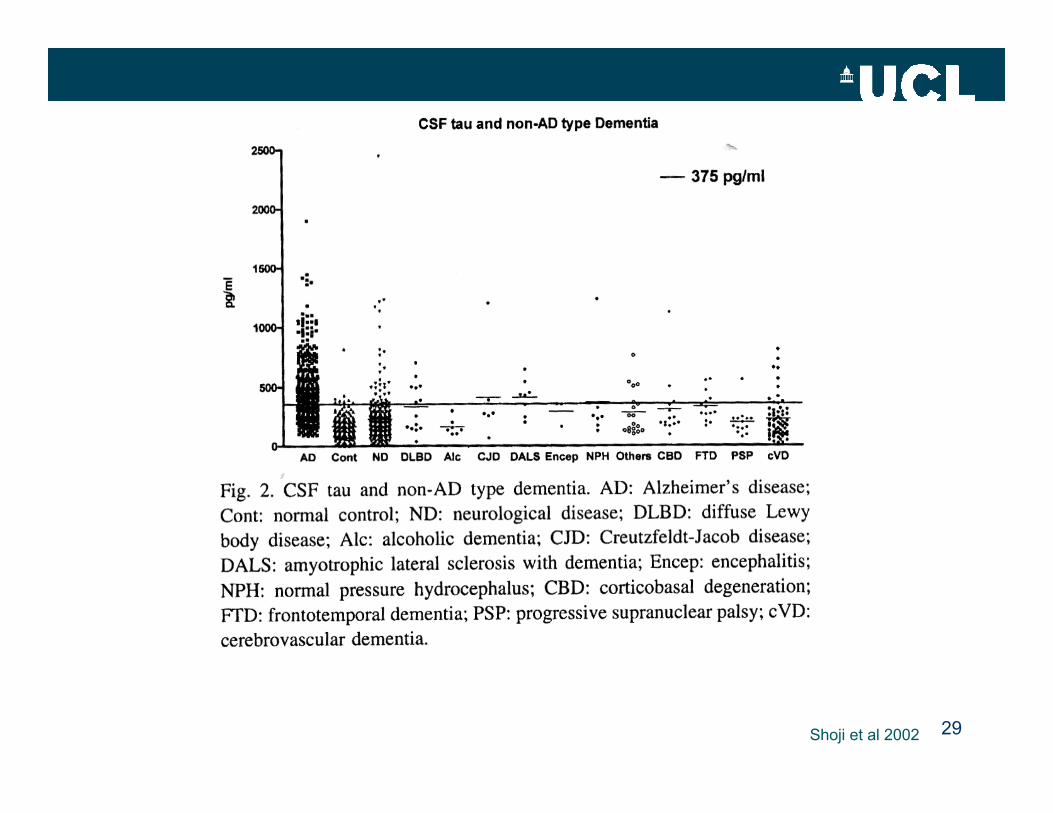
29Shoji et al 2002
30
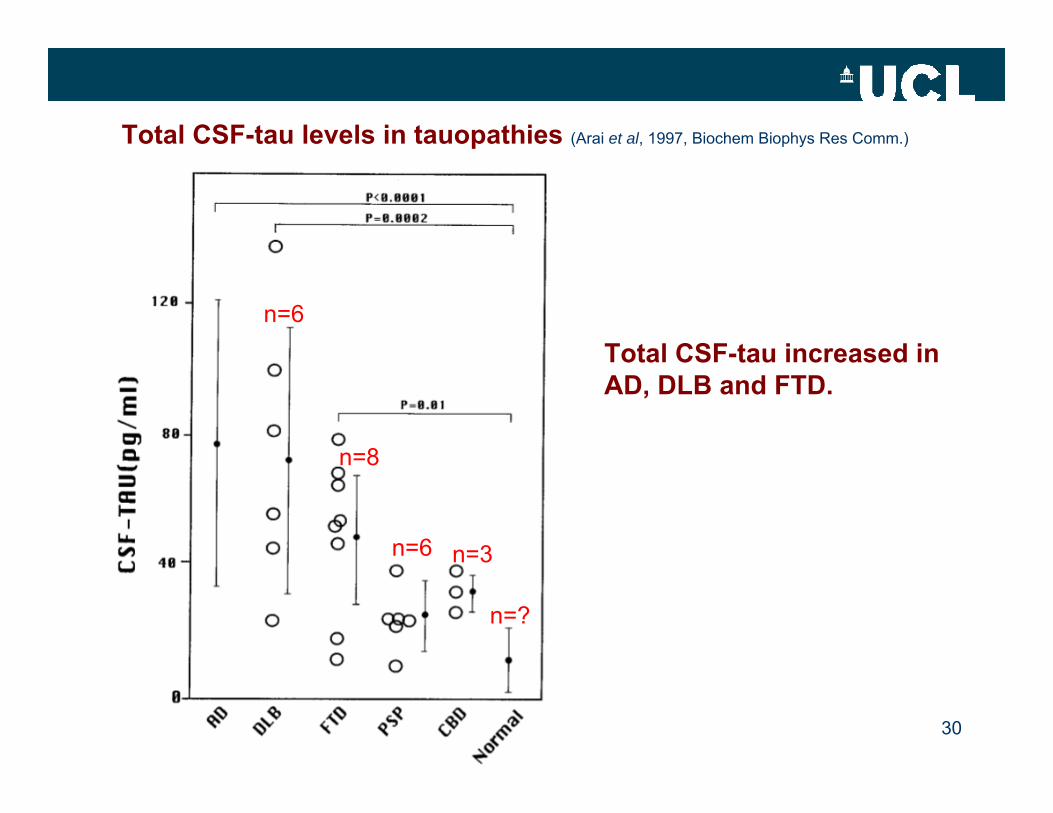
Total CSF-tau levels in tauopathies (Arai et al, 1997, Biochem Biophys Res Comm.)
n=6
n=6
n=8
n=3
n=?
Total CSF-tau increased inAD, DLB and FTD.
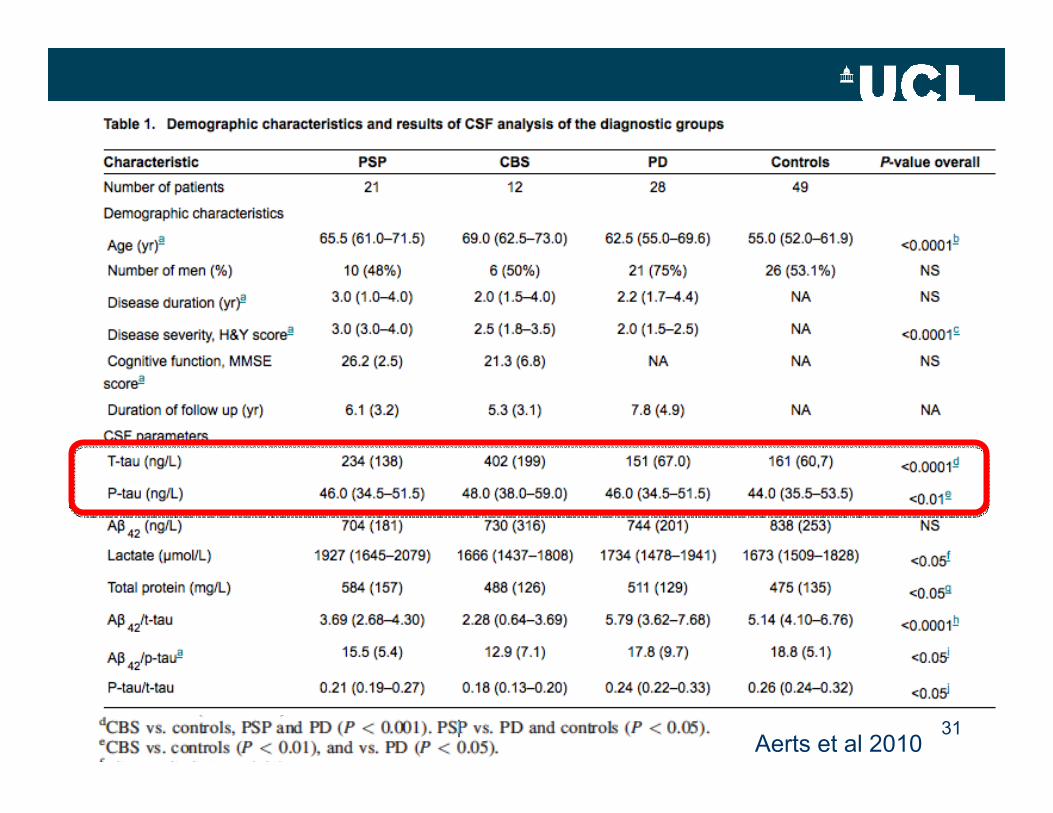
31Aerts et al 2010
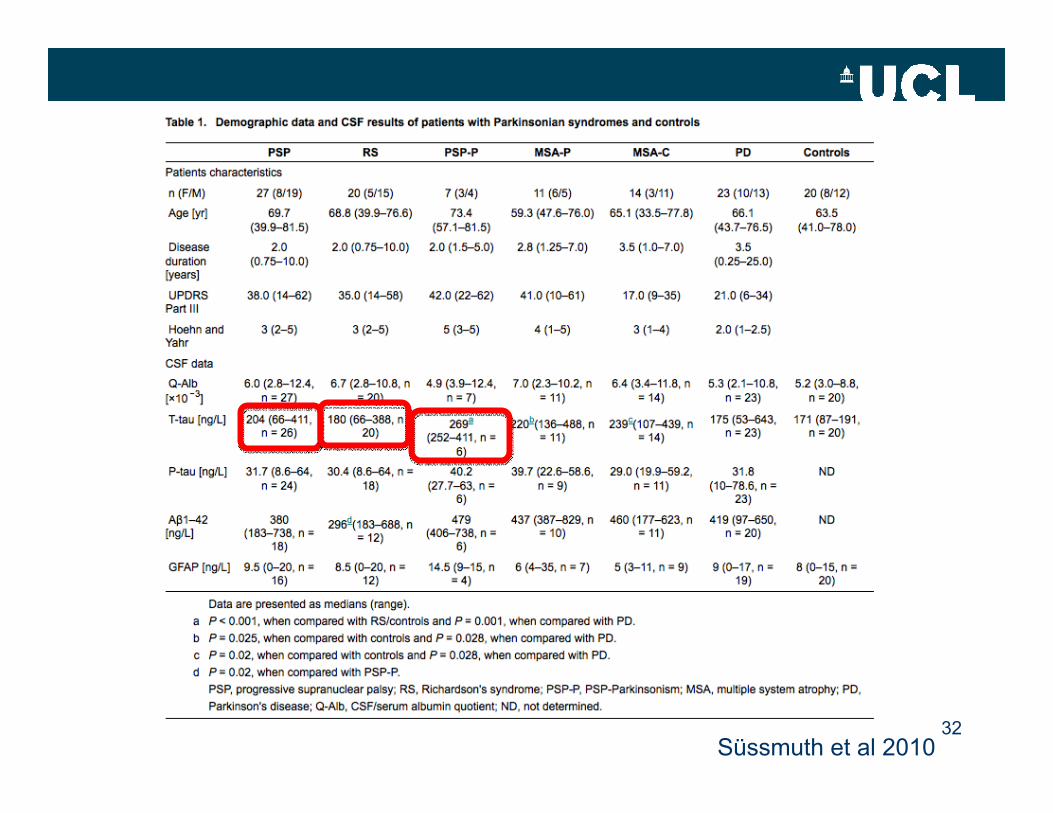
32Süssmuth et al 2010
33
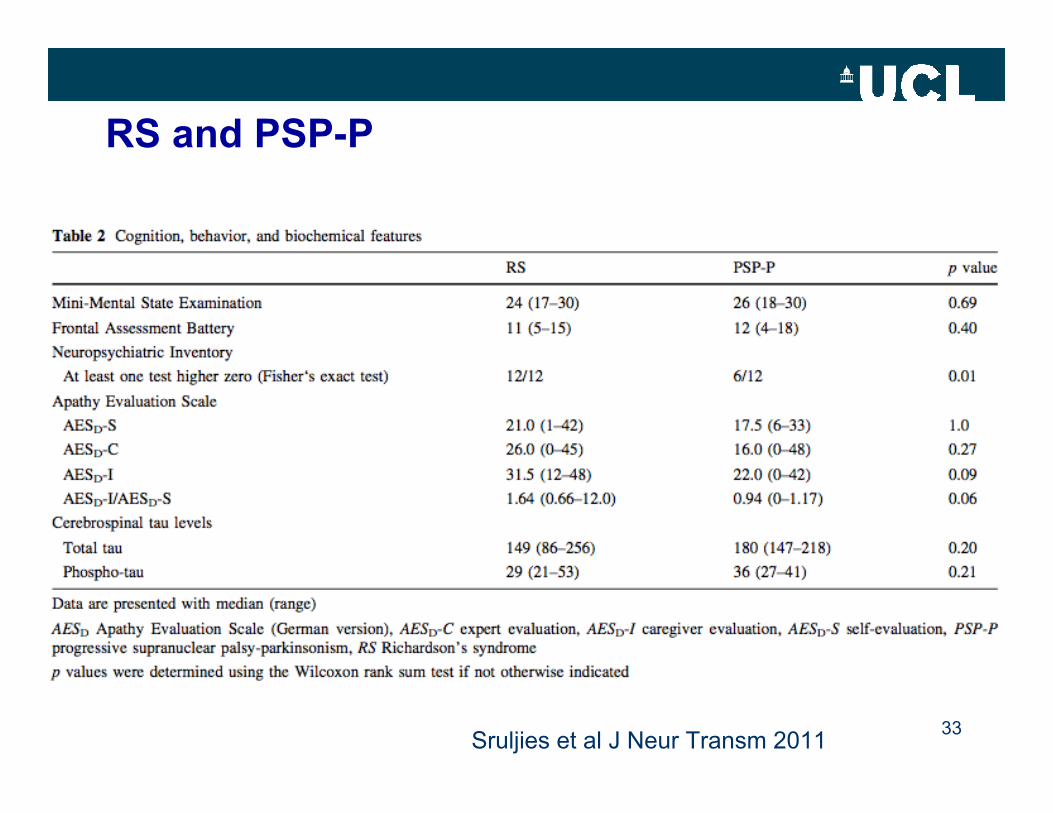
RS and PSP-P
Sruljies et al J Neur Transm 2011
Would 3R-tau and 4R-tau levels in CSF discriminate between tauopathies?
• Are changes in tau isoform homeostasis (pathology or gene mutations) reflected in CSF?
• Would PSP and CBD (and FTDP17 with exon 10 splicing mutations) have elevated 4R-tau in CSF?
• Does PiD have elevated 3R-tau?
34
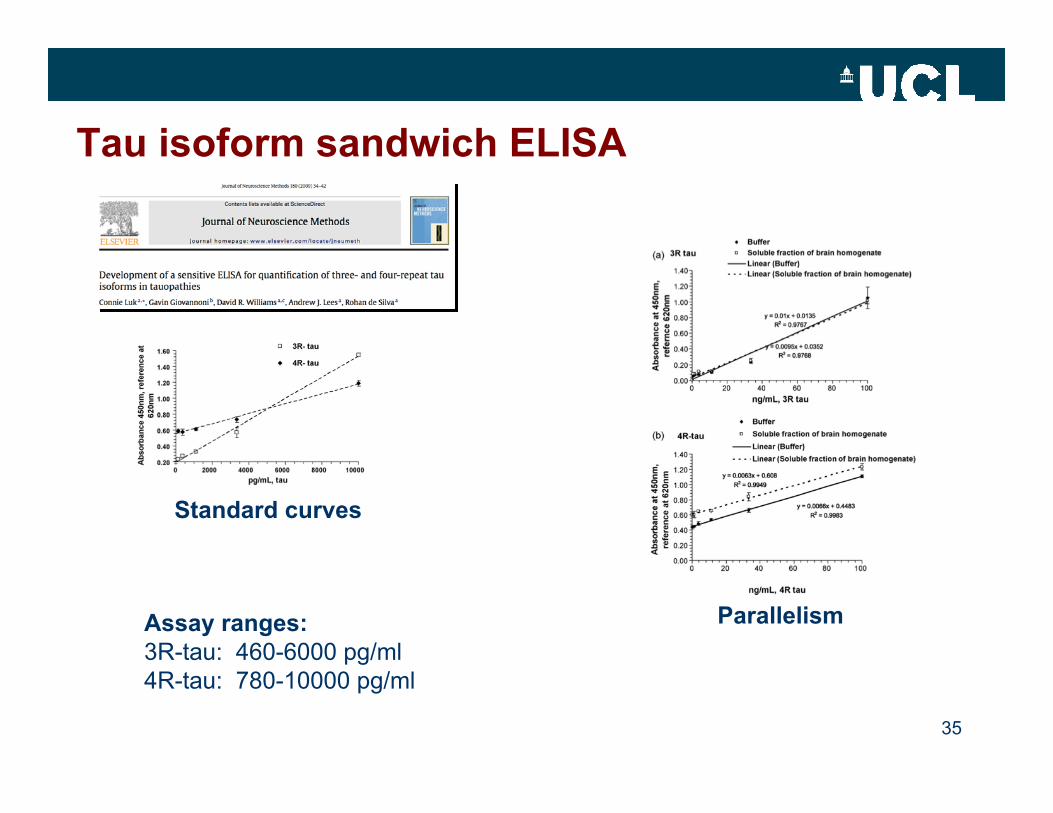
Tau isoform sandwich ELISA
35
Assay ranges:3R-tau: 460-6000 pg/ml4R-tau: 780-10000 pg/ml
Standard curves
Parallelism
36
37
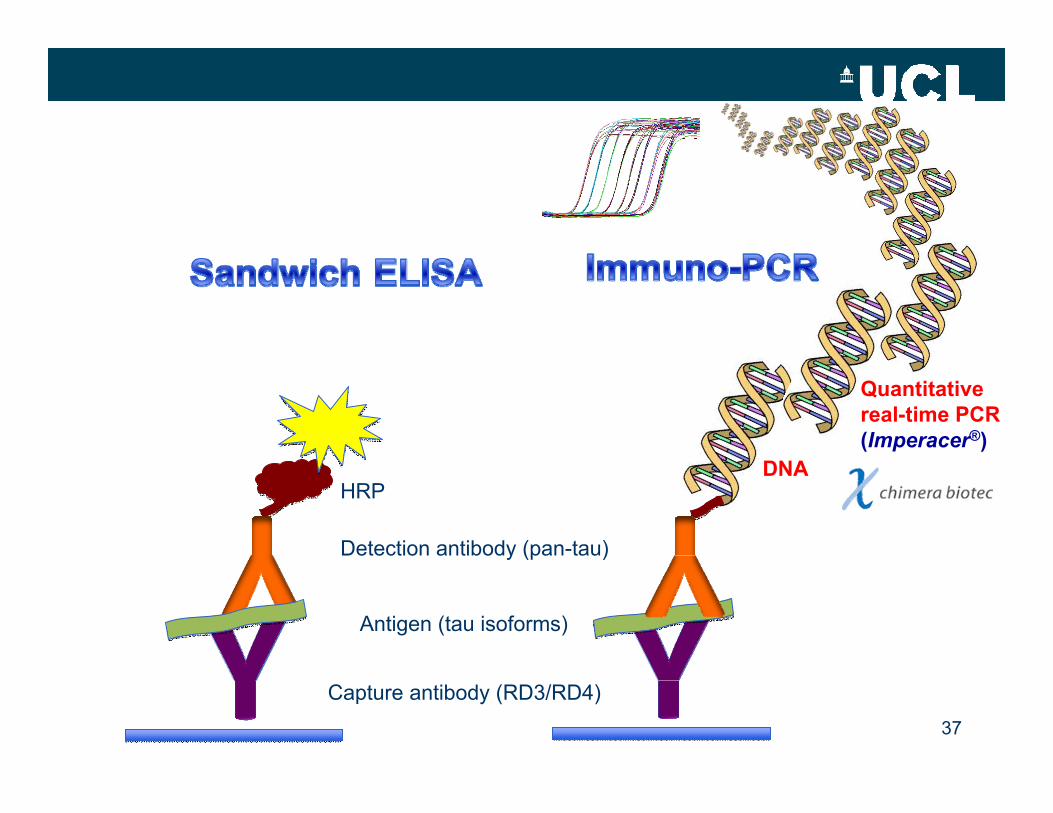
Capture antibody (RD3/RD4)
Antigen (tau isoforms)
Detection antibody (pan-tau)
HRPDNA
Quantitativereal-time PCR(Imperacer®)
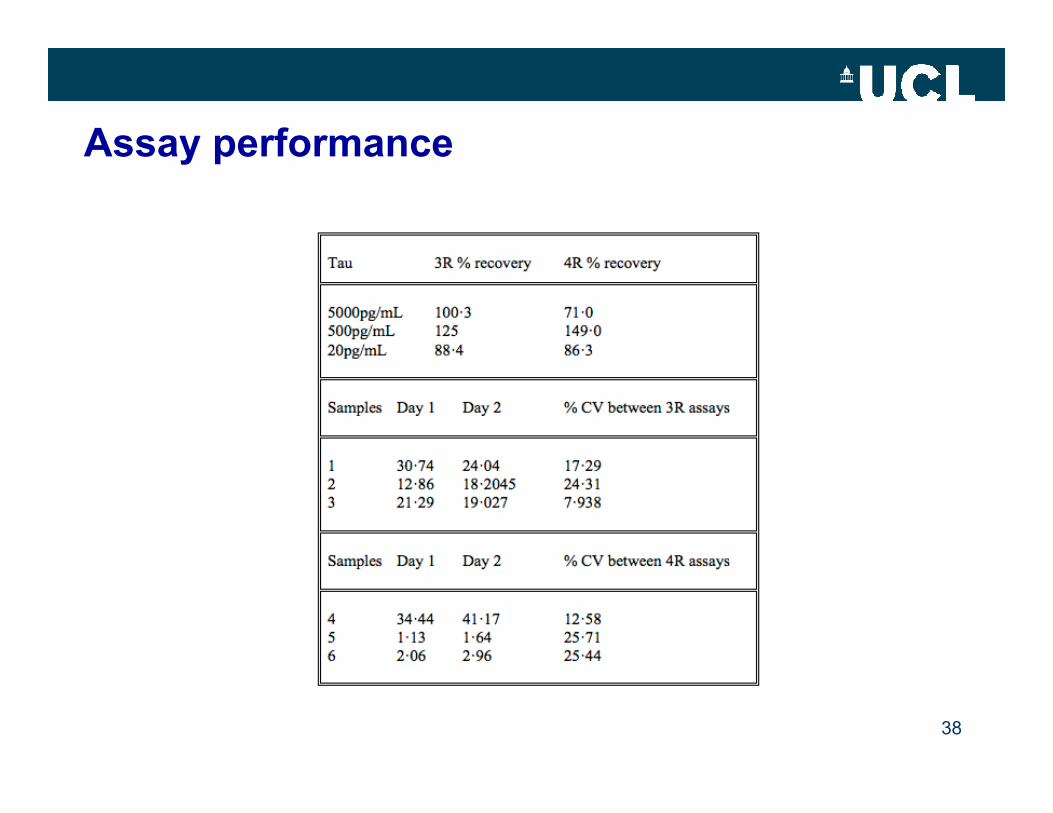
Assay performance
38
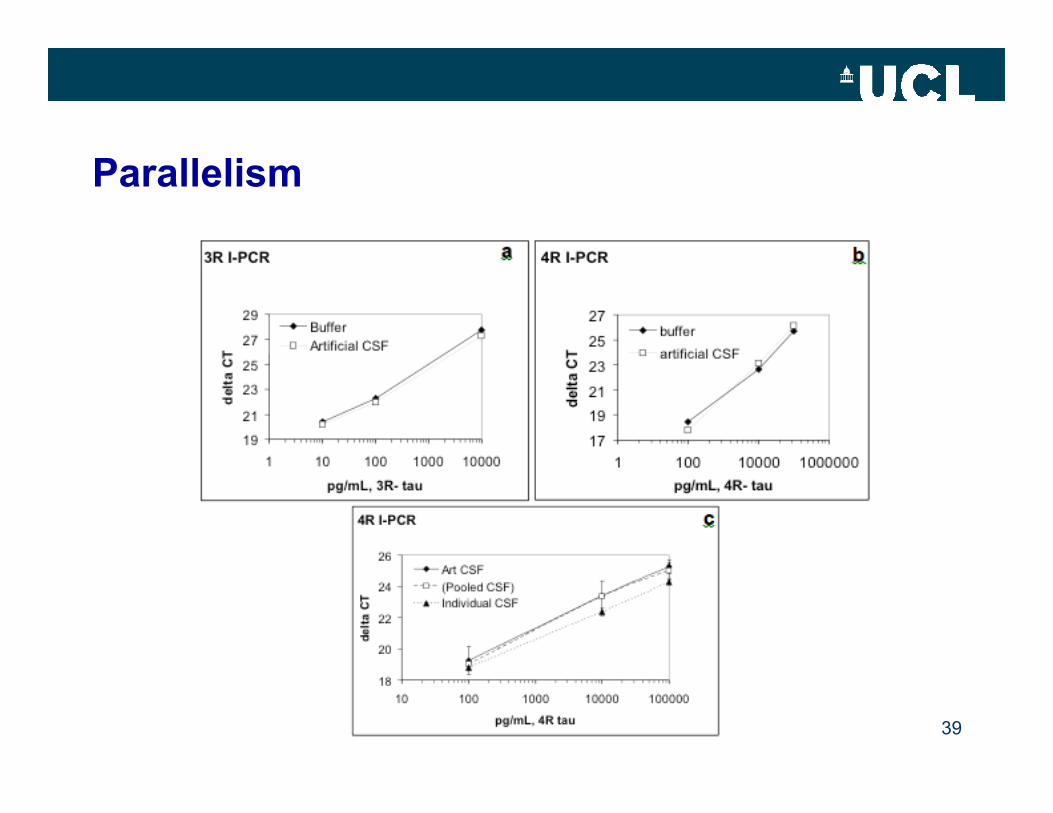
Parallelism
39
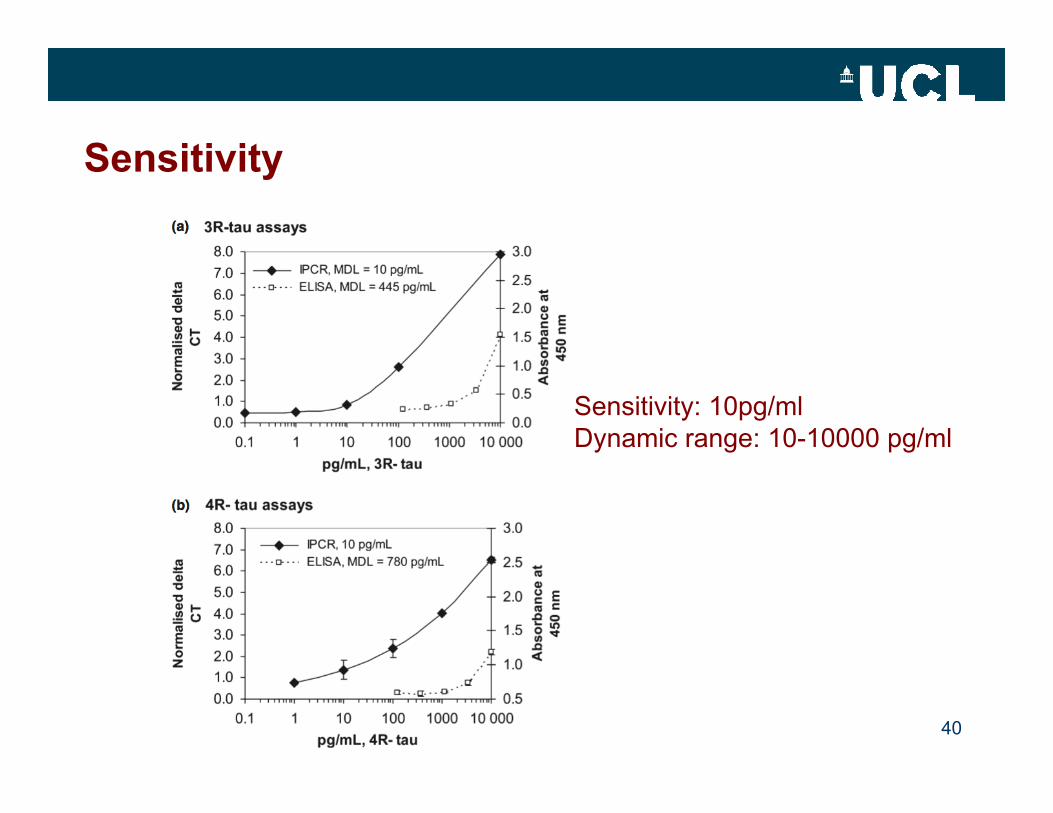
Sensitivity
40
Sensitivity: 10pg/mlDynamic range: 10-10000 pg/ml
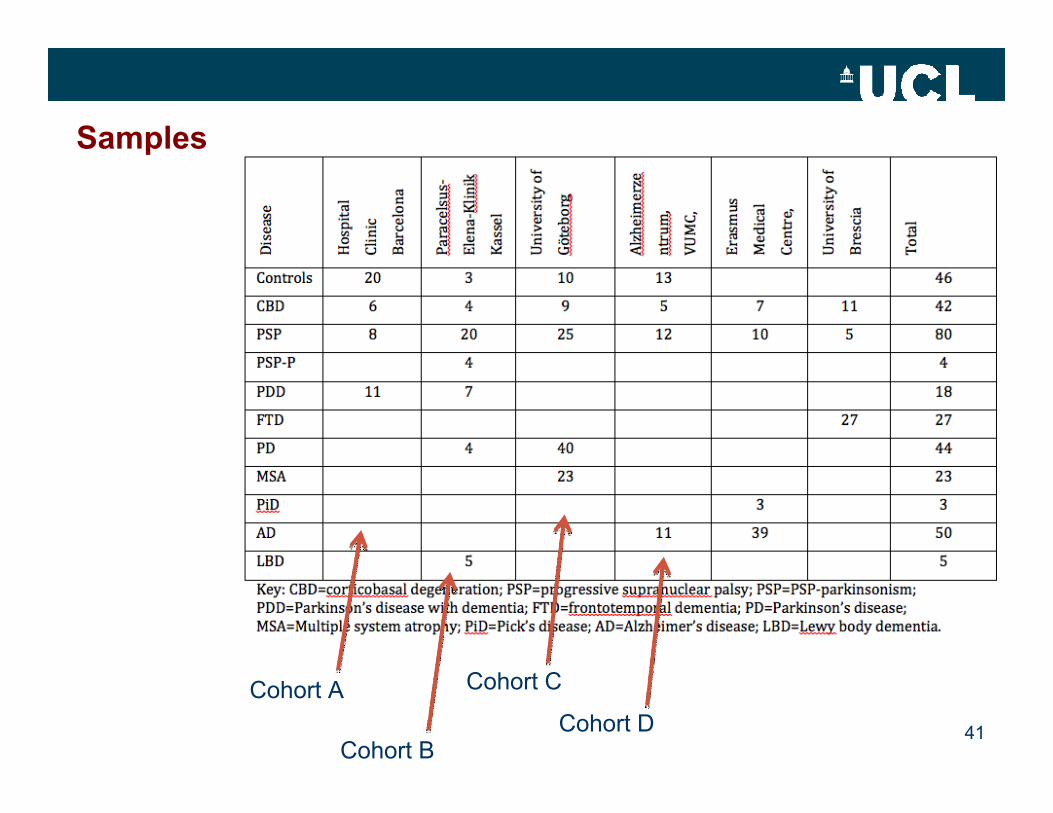
Samples
41
Cohort A
Cohort B
Cohort C
Cohort D
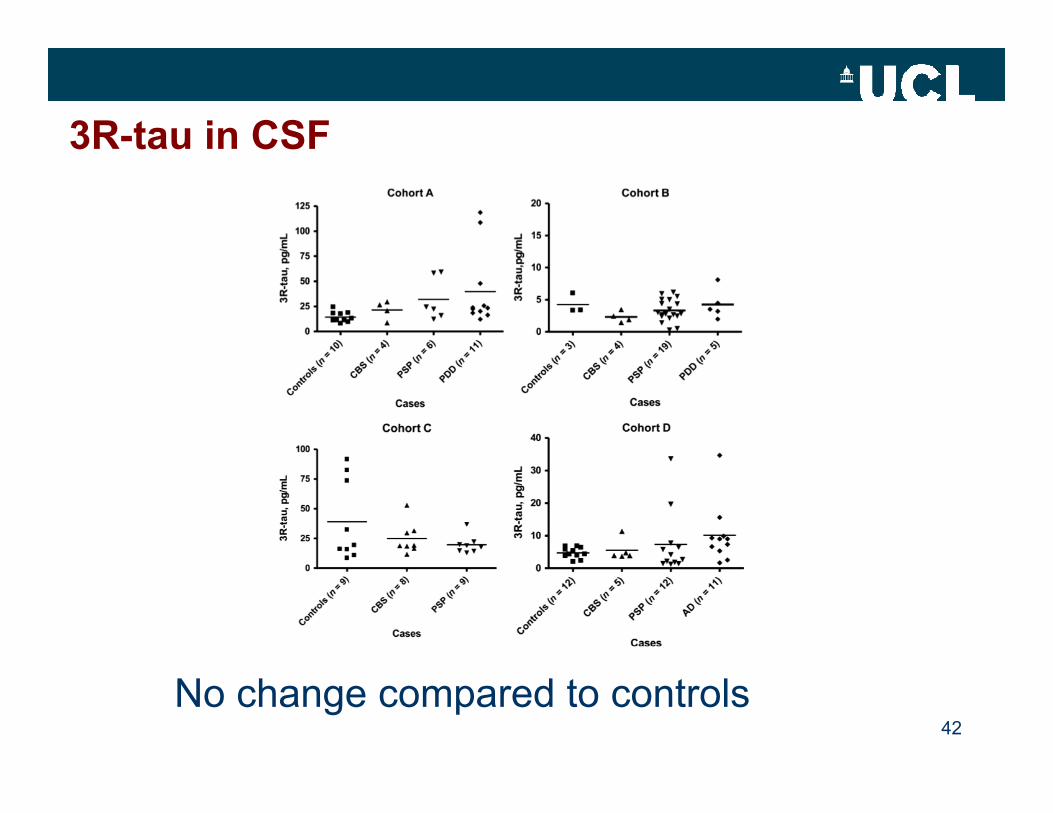
3R-tau in CSF
42No change compared to controls
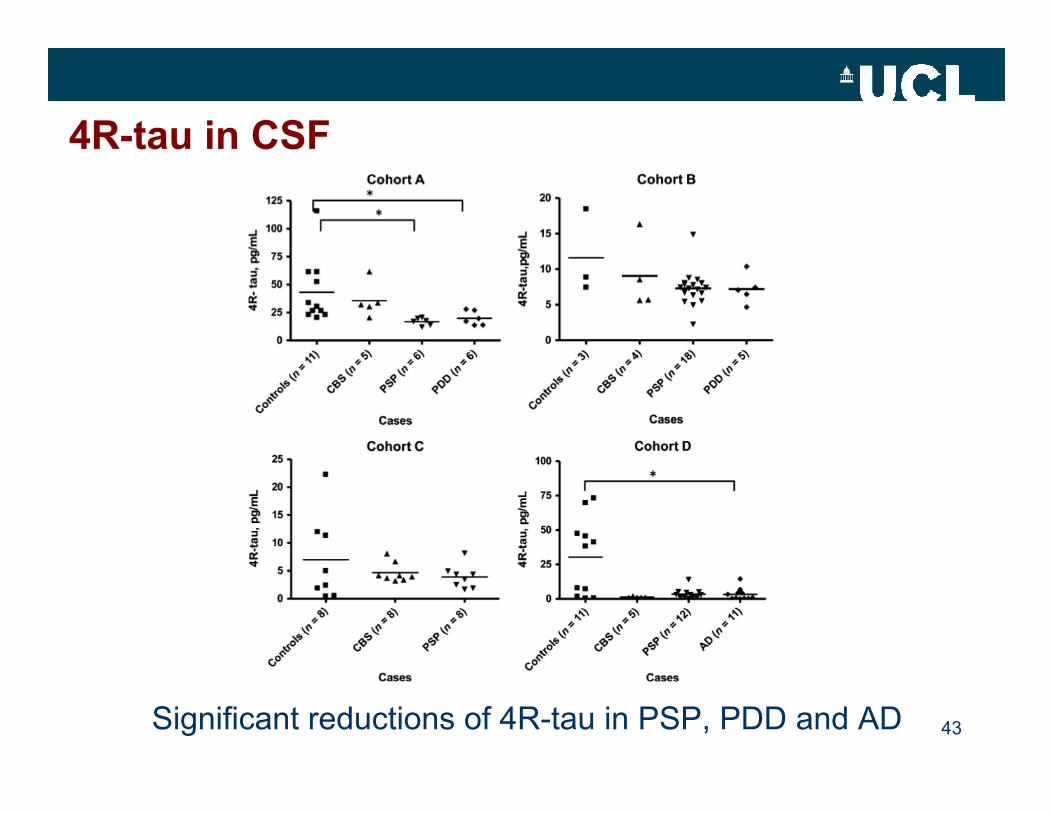
4R-tau in CSF
43Significant reductions of 4R-tau in PSP, PDD and AD
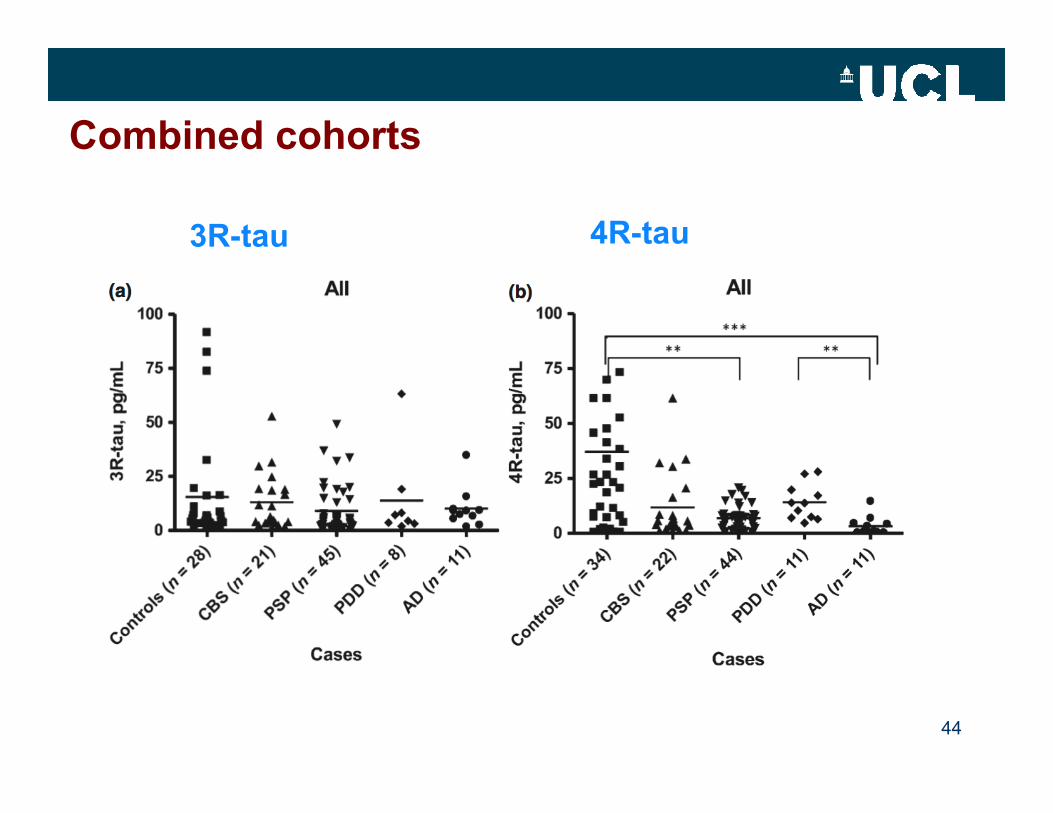
Combined cohorts
44
3R-tau 4R-tau
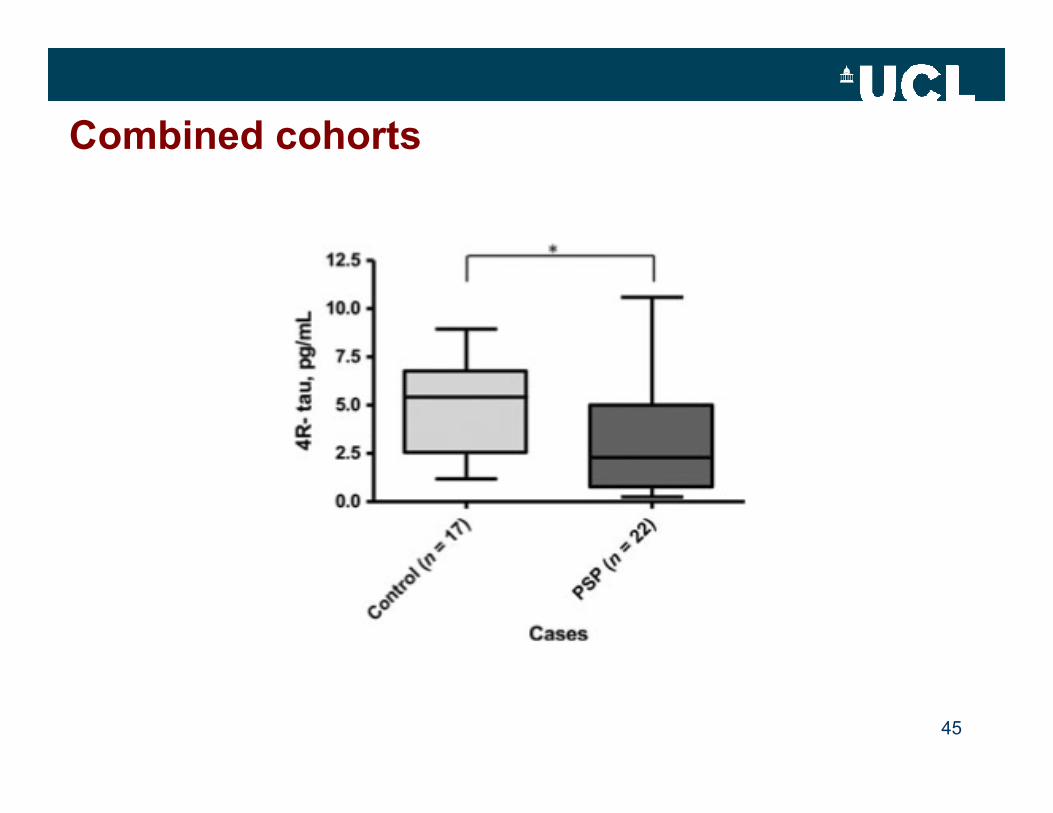
Combined cohorts
45
Conclusions 1
• No reliable biomarker for differential diagnosis of parkinsonian disorders with tau pathology– No consistent changes in total- and phospho-tau measures.
• Disturbed 3R-/4R-tau isoform homeostasis in many tauopathies (FTLD-tau mutations and tau pathology)
• Immuno-PCR assays allow measurement of 3R- and 4R-tau in CSF showing selective decrease of 4R-tau in tauopathies.– Reduction of 4R-tau not restricted to 4R-tauopathies (PSP and CBS).
46
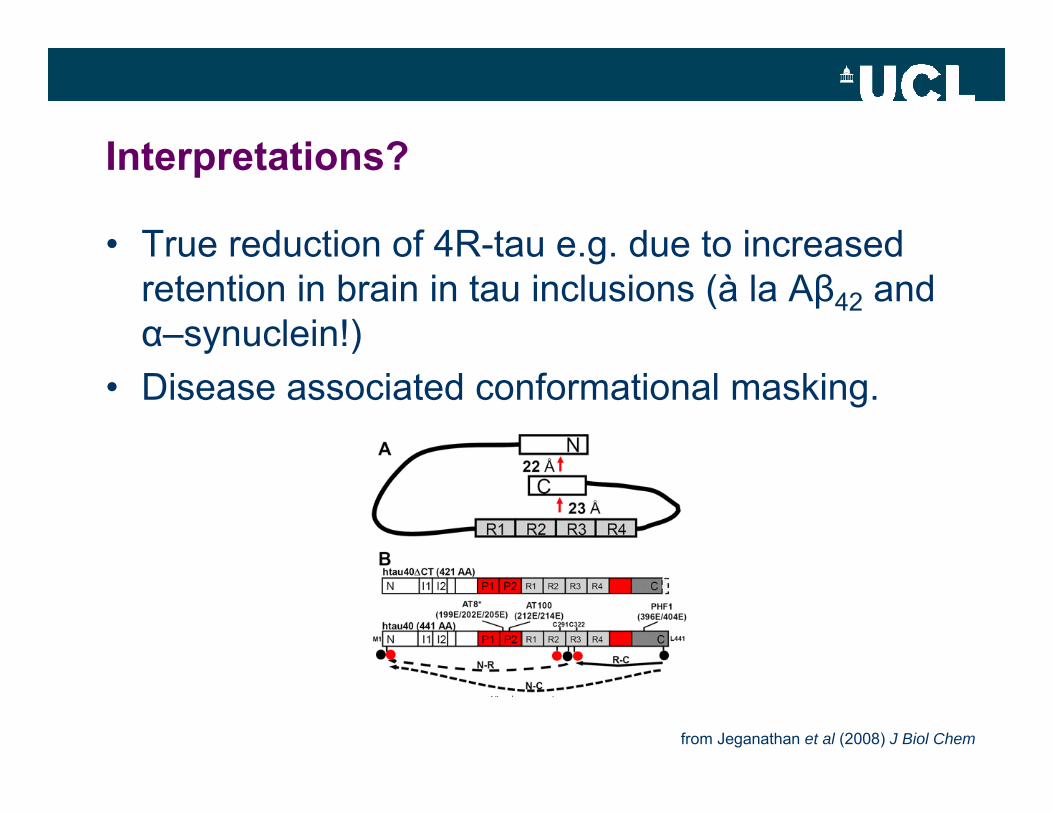
Interpretations?
• True reduction of 4R-tau e.g. due to increased retention in brain in tau inclusions (à la Aβ42 and α–synuclein!)
• Disease associated conformational masking.
from Jeganathan et al (2008) J Biol Chem
48
AcknowledgementsReta Lila Weston Institute/UCL Institute of Neurology
•Dr Connie Luk
•Andrew Lees•John Hardy•Tamas Revesz•Nick Fox
•Roberto Simone•Victoria Kay•Fidel Anaya•Nadia Magdalinou•Geshanthi Hondhamuni•Sylvia Agathou•Khawar Hussain•Alan Pittman•Amanda Myers
•Mark Spengler•Sven Schulz•Ron Wacker•Beena Punnamoottil
Sample contributions
Barcelona•Yaroslau Compta•Maria José Martí•Ana CámaraGothenburg•Henrik Zetterberg•Kaj Blennow•Radu ConstantinescuAmsterdam•Yolande Pijnenburg
Rotterdam•John Van Swieten•Wan Zheng ChiuBrescia•Barbara BorroniGöttingen•Brit Mollenhauer•Claudia TrenkwalderTübingen•Walter MätzlerMelbourne•David Williams•Perdita Cheshire