Embed Size (px)
Citation preview

PP-DEP-GBR-0026 January 2017
DMPA use and fracture risk:
an update
1
Prescribing Information and adverse event reporting for Depo-Provera®
(Medroxyprogesterone Acetate) is available on slides 8-9

PP-DEP-GBR-0026 January 2017
DMPA, medroxyprogesterone acetate; UK, United Kingdom.
1. Lanza LL, et al. Obstet Gynecol 2013;121:593–600.
The Lanza study design
• A retrospective, non-randomised, cohort study of 312,395 women using UK
population-based data from the General Practice Research Database1
• Women aged 15–50 years of age at the first contraceptive prescription were
included1
• A subcohort of 166,367 women had baseline data available for the 6 months
before the first prescription
• All incident fractures were included; fracture incidence and risk factors
before starting contraceptive use (DMPA or other) were estimated1
• Fracture incidence was estimated before and after the start of
contraceptive use for DMPA users and non-users1
2
Main objective: to analyse fracture incidence in users of DMPA and users of other
hormonal contraceptives before and after the start of contraceptive use1
PP-DEP-GBR-0026 January 2017
CI, confidence interval; DMPA, medroxyprogesterone acetate; IRR, incidence rate ratio.
1. Lanza LL, et al. Obstet Gynecol 2013;121:593–600.
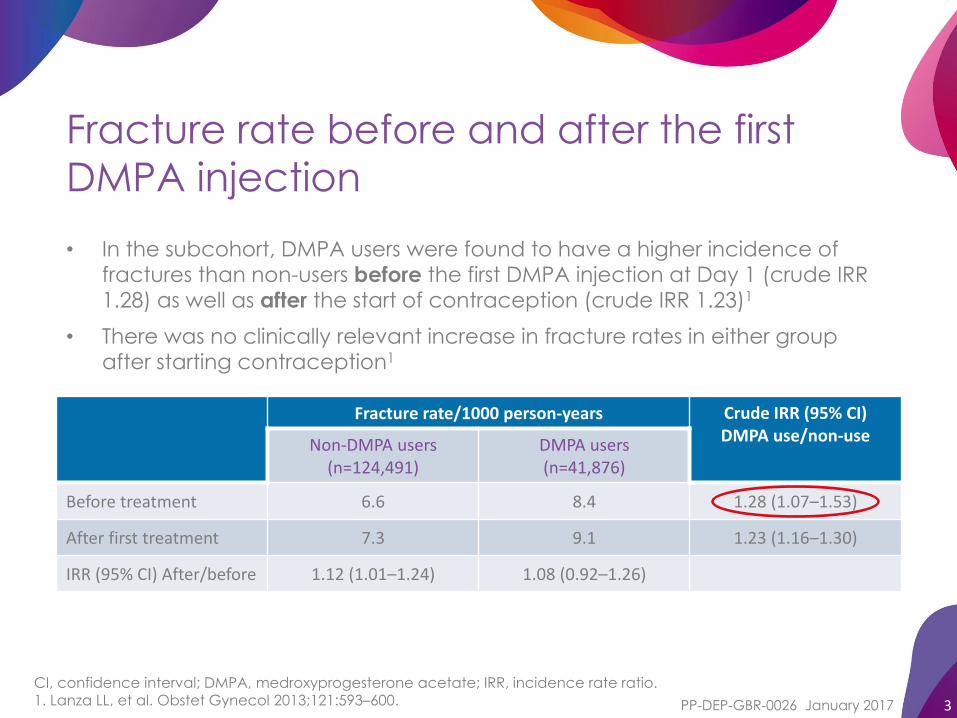
Fracture rate before and after the first
DMPA injection
• In the subcohort, DMPA users were found to have a higher incidence of
fractures than non-users before the first DMPA injection at Day 1 (crude IRR
1.28) as well as after the start of contraception (crude IRR 1.23)1
• There was no clinically relevant increase in fracture rates in either group
after starting contraception1
3
Fracture rate/1000 person-years Crude IRR (95% CI)DMPA use/non-use
Non-DMPA users (n=124,491)
DMPA users (n=41,876)
Before treatment 6.6 8.4 1.28 (1.07–1.53)
After first treatment 7.3 9.1 1.23 (1.16–1.30)
IRR (95% CI) After/before 1.12 (1.01–1.24) 1.08 (0.92–1.26)
PP-DEP-GBR-0026 January 2017
CI, confidence interval; DMPA, medroxyprogesterone acetate; IRR, incidence rate ratio.
* IRR adjusted for age and risk factor for DMPA use during the study period compared with non-use of DMPA.
†Incident rate ratios are standardised for age in 5-year groups and for each factor (one at a time).
1. Lanza LL, et al. Obstet Gynecol 2013;121:593–600.
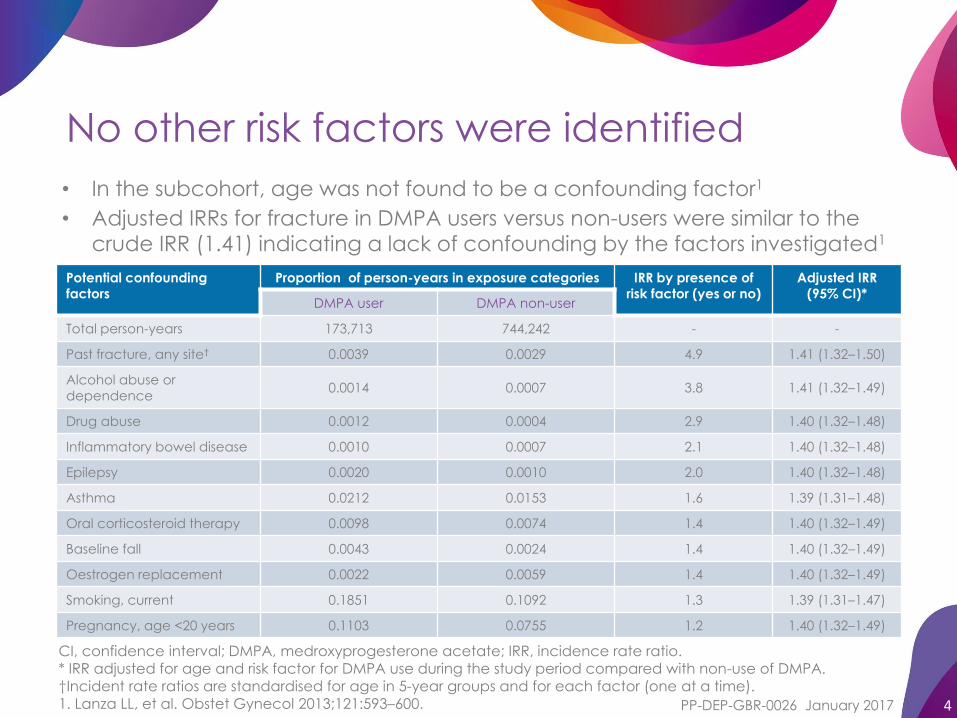
No other risk factors were identified
Potential confounding
factors
Proportion of person-years in exposure categories IRR by presence of
risk factor (yes or no)
Adjusted IRR
(95% CI)*DMPA user DMPA non-user
Total person-years 173,713 744,242 - -
Past fracture, any site† 0.0039 0.0029 4.9 1.41 (1.32–1.50)
Alcohol abuse or
dependence0.0014 0.0007 3.8 1.41 (1.32–1.49)
Drug abuse 0.0012 0.0004 2.9 1.40 (1.32–1.48)
Inflammatory bowel disease 0.0010 0.0007 2.1 1.40 (1.32–1.48)
Epilepsy 0.0020 0.0010 2.0 1.40 (1.32–1.48)
Asthma 0.0212 0.0153 1.6 1.39 (1.31–1.48)
Oral corticosteroid therapy 0.0098 0.0074 1.4 1.40 (1.32–1.49)
Baseline fall 0.0043 0.0024 1.4 1.40 (1.32–1.49)
Oestrogen replacement 0.0022 0.0059 1.4 1.40 (1.32–1.49)
Smoking, current 0.1851 0.1092 1.3 1.39 (1.31–1.47)
Pregnancy, age <20 years 0.1103 0.0755 1.2 1.40 (1.32–1.49)
4
• In the subcohort, age was not found to be a confounding factor1
• Adjusted IRRs for fracture in DMPA users versus non-users were similar to the
crude IRR (1.41) indicating a lack of confounding by the factors investigated1

PP-DEP-GBR-0026 January 2017
CI, confidence interval; DMPA, medroxyprogesterone acetate; IRR, incidence rate ratio.
1. Lanza LL, et al. Obstet Gynecol 2013;121:593–600.
Fracture rate and the number of DMPA
injections
• In the full cohort , compared with non-users of DMPA, the fracture rate was
greater in low-exposure DMPA users (1–7 injections) than in high-exposure
DMPA users (≥8 injections)
• When fracture site was analysed, DMPA users had no excess risk for axial
fractures compared with non-users
5
Number of DMPA injections
Fracture rate/1000 person-years*
Crude IRR (95% CI)
0 (non-users)† 6.4 1.00
1–7 (low exposure) 9.4 1.47 (1.40–1.54)
≥8 (high exposure) 7.8 1.22 (1.13–1.32)
*Age-standardised rates (not shown) are not different from the crude rates.
†Non-exposure includes person-years of never-users and person-years of DMPA users before first DMPA prescription.

PP-DEP-GBR-0026 January 2017
DMPA, medroxyprogesterone acetate;.
1. Lanza LL, et al. Obstet Gynecol 2013;121:593–600.
Lanza study: summary of key findings
The higher fracture rate observed in DMPA users compared with non-
users did not appear to be caused by DMPA:1
• DMPA users had a higher fracture rate than non-users before the start of
contraception and on Day 1 of starting contraception
• The fracture rate did not increase after initiation of contraception compared
with before treatment
• In the full cohort, fracture rate in high-exposure DMPA users was less than in
low-exposure users
• In the full cohort, there was no difference in the axial fracture rate between
DMPA users and non-users
6
Although DMPA users had more fractures than non-users, this association might be the
result of confounding by a pre-existing risk for fractures in women who choose DMPA
contraception1

PP-DEP-GBR-0026 January 2017
DMPA use and BMD post-menopauseOrr-Walker BJ, et al. 1998
BMD adjusted for weight and age
in post-menopausal women
7
BMD, bone mineral density; DMPA, medroxyprogesterone acetate.
1. Orr-Walker BJ, et al. Clin Endocrinol 1998;49:615–618.
2. Petitti DB, et al. Obstet Gynecol 2000;95:736–744.
Adapted from Orr-Walker et al. 1998.
Me
an
BM
D ±
SE (
g/c
m2)
• Orr-Walker conducted a cross-sectional
study to compare BMD in post-
menopausal former users of DMPA with
non-users (n=346)1
• There was no significant difference in bone
density between former DMPA users and
non-users in post-menopausal women1
• It was the opinion of the investigators that
previous DMPA-use was unlikely to have a
substantial impact on bone fracture risk in
the post-menopausal years1
The Lanza study did not determine if DMPA use during reproductive years
could impact fracture rate post-menopause; however, cross-sectional
studies found BMD in former DMPA users was similar to that of non-users1,2

PP-DEP-GBR-0026 January 2017
Depo-Provera 150 mg/ml
(medroxyprogesterone acetate)
ABBREVIATED PRESCRIBING INFORMATION (UK)
Please refer to the SmPC before prescribing
Depo-Provera 150 mg/ml.
Presentation: 1 ml Disposable syringe, containing
150 mg medroxyprogesterone acetate in a
Sterile suspension for injection.
Indication: Long-term contraceptive agent, in
women who have been counselled concerning
the likelihood of menstrual disturbance,
potential delay in return to full fertility and risks of
bone mineral density losses. Short-term
contraception for the following (i) for partners of
men undergoing vasectomy, until the
vasectomy becomes effective, (ii) in women
who are being immunised against rubella (iii) in
women awaiting sterilisation. May only be used
in adolescents (12-18 years) after other methods
of contraception were considered to be
unsuitable.
Dosage: First injection: 150mg intramuscular
injection during the first 5 days of a normal
menstrual cycle. Post Partum: Within 5 days
post-partum if not breast-feeding. Women in
puerperium can experience prolonged and
heavy bleeding, therefore caution is required,
and women should be advised accordingly. If
the puerperal woman will breast-feed, the initial
injection should be no sooner than 6 weeks post
partum. Further doses: These should be given at
12 week intervals, however as long as the
injection is given no later than 5 days after the
12 week interval, no additional contraception
measures are required. For partners of men
undergoing vasectomy, a second injection 12
weeks after the first may be necessary in a small
proportion of patients where the partner's sperm
count has not fallen to zero. If the dose repeat
interval is greater than 89 days (12 weeks and 5
days) for any reason, then pregnancy should be
excluded before the next injection is given and
the patient should use additional contraceptive
measures (e.g. barrier) for fourteen days after
this subsequent injection. Elderly: Not
appropriate. Children: Depo-Provera is not
indicated before menarche. Data in adolescent
females (12-18 years) is available, Refer to the
Summary of Product Characteristics for further
information. Other than concerns about loss of
BMD, the safety and effectiveness of Depo-
Provera is expected to be the same for
adolescents after menarche and adult females.
Depo-Provera may be poorly metabolised in
patients with severe liver insufficiency. No
dosage adjustment is required for renal
insufficiency. Administration: By deep
intramuscular injection. The sterile aqueous
suspension should be vigorously shaken just
before use to ensure the dose being given
represents a uniform suspension.
Contraindications: Known hypersensitivity to
medroxyprogesterone acetate or any of its
excipients. Pregnancy. Known or suspected
hormone-dependent malignancy of breast or
genital organs. Patients with presence or a
history of severe hepatic disease whose liver
function has not returned to normal. Patients
with abnormal uterine bleeding, whether
administered alone or in combination with
oestrogen until a definite diagnosis has been
established and the possibility of genital tract
malignancy eliminated.
Special Warnings and Precautions: Use of Depo-
Provera reduces serum oestrogen levels and is
associated with significant loss of BMD due to
the known effect of oestrogen deficiency on
the bone remodelling system. Bone loss is
greater with increasing duration of use, however
BMD appears to increase after Depo-Provera is
discontinued and ovarian oestrogen production
increases. In adolescents and women with
significant lifestyle and/or medical risk factors for
osteoporosis, other methods of contraception
should be considered before using Depo-
Provera. The administration of Depo-Provera
usually causes disruption of the normal
menstrual cycle. Bleeding patterns can include
amenorrhoea. Women should be counselled
that there is a potential for delay in return to full
fertility following use of the method, regardless
of the duration of use. Long-term case-
controlled surveillance of Depo-Provera users
found no overall increased risk of ovarian, liver,
or cervical cancer and a prolonged, protective
effect of reducing the risk of endometrial
cancer in the population of users. Refer to the
Summary of Product Characteristics for further
information. There is a tendency for women to
gain weight while on Depo-Provera therapy.
Reports of anaphylactic responses
(anaphylactic reactions, anaphylactic shock,
anaphylactoid reactions) have been received.
Should the patient experience pulmonary
embolism, cerebrovascular disease or retinal
thrombosis while receiving Depo-Provera, the
drug should not be re-administered.
8
Depo-Provera® Abbreviated
Prescribing Information slide 1 of 2

PP-DEP-GBR-0026 January 2017
Patients with a history of endogenous
depression should be carefully monitored.
Some patients may complain of premenstrual
type depression while on Depo-Provera
therapy. As with any intramuscular injection,
especially if not administered correctly, there is
a risk of abscess formation at the site of
injection, which may require medical and/or
surgical intervention. Patients with a history of
the following conditions should be carefully
monitored: endogenous depression (including
premenstrual-type depression), migraine or
unusually severe headaches, acute visual
disturbances of any kind, pathological changes
in liver function or hormone levels. Diabetic
patients should be carefully monitored while
receiving DMPA; increases and decreases in
total cholesterol, triglycerides and low-density
lipoprotein (LDL) cholesterol have been
observed. DMPA have been associated with a
15-20% reduction in serum high density
lipoprotein (HDL) cholesterol levels. Potential for
an increased risk of coronary disease should be
considered prior to use. Doctors should carefully
consider the use of DMPA in patients with
recent trophoblastic disease before levels of
human chorionic gonadotrophin have returned
to normal. Pathologists should be informed of
the patient's use of Depo-Provera if endometrial
or endocervical tissue is submitted for
examination. Results of certain laboratory tests
may be affected. Refer to the Summary of
Product Characteristics for further information.
Drug interactions: Aminoglutethimide
administered concurrently may significantly
depress bioavailability. The possibility of
interaction (including oral anticoagulants)
should be borne in mind in patients receiving
concurrent treatment with other drugs.
Medroxyprogesterone acetate (MPA) is
metabolized in-vitro primarily by hydroxylation
via the CYP3A4. Specific drug-drug interaction
studies evaluating the clinical effects with
CYP3A4 inducers or inhibitors on MPA have not
been conducted and therefore the clinical
effects of CYP3A4 inducers or inhibitors are
unknown. Pregnancy and Lactation: Check for
pregnancy before initial injection, and also if
administration of subsequent injection is
delayed beyond 89 days (12 weeks and 5
days). Effects on ability to drive and use
machines: Depo-Provera may cause
headaches and dizziness. Patients should be
advised not to drive or operate machinery if
affected. Side-effects: Very common (≥1/10):
nervousness, abdominal pain or discomfort,
headache, weight increased or decreased.
Common (≥1/100 to <1/10):depression, libido
decrease, nausea, abdominal distention,
alopecia, acne, rash, back pain, dizziness, ,
pain in extremity, vaginal discharge, breast
tenderness, dysmenorrhea, genitourinary tract
infection, oedema/fluid retention, asthenia .
Uncommon (≥ 1/1000 to < 1/100): drug
hypersensitivity, increased or decreased
appetite, insomnia, seizure, somnolence,
paraesthesia, hot flush, dyspnoea, hepatic
function abnormal, hirsutism, urticaria, pruritus,
chloasma, dysfunctional uterine bleeding
(irregular, increased, decreased, spotting),
galactorrhoea, pelvic pain, dyspareunia,
suppressed lactation, chest pain. Other side
effects include: breast cancer, anaemia, ,
anaphylactic reaction, anaphylactoid
reaction, angioedema, anorgasmia, emotional
disturbance, affective disorder, irritability,
anxiety, migraine, paralysis, syncope, vertigo,
tachycardia, embolism and thrombosis, deep
vein thrombosis, thrombophlebitis, hypertension,
varicose veins, pulmonary embolism, rectal
haemorrhage, gastrointestinal disorder,
jaundice, hepatic enzyme abnormal,
lipodystrophy acquired, dermatitis, ecchymosis,
scleroderma, skin striae, arthralgia, muscle
spasms, osteoporosis, osteoporotic fractures,
vaginitis, amenorrhoea, breast pain,
metrorrhagia, menometrorrhagia, menorrhagia,
vulvovaginal dryness, breastatrophy, ovarian
cyst, premenstrual syndrome, endometrial
hyperplasia, breast mass, nipple exudate
bloody, vaginal cyst, breast enlargement, lack
of return to fertility, sensation of pregnancy,
pyrexia, fatigue, injection site reaction, ,
dysphonia, VIIth nerve paralysis, axillary swelling,
, glucose tolerance decreased, cervical smear
abnormal.
Refer to the Summary of Product
Characteristics for more detailed information
on side-effects.
Package Quantities and Basic NHS Cost: Single
1ml Syringe pack: £6.01. Legal Category: POM.
Marketing Authorisation Number and Holder: PL
00057/0965, Pfizer Limited, Ramsgate Road,
Sandwich, CT13 9NJ, UK. Last Updated: May
2016
Further information is available on request from:
Medical Information at Pfizer Limited, Walton
Oaks, Dorking Road, Tadworth, Surrey, KT20 7NS,
UK. Tel: +44 (0) 1304 616161
Ref: DP 14_0
9
Depo-Provera® Abbreviated
Prescribing Information slide 2 of 2

PP-DEP-GBR-0026 January 2017
Adverse Event Reporting
10
Adverse events should be reported
Reporting forms and information can be found at www.mhra.gov.uk/yellowcard
Adverse events should also be reported to Pfizer Medical Information on 01304 616161
The Yellow Card Scheme is run by the Medicines and Healthcare products Regulatory Agency (MHRA) and Commission on Human Medicines (CHM)
The Scheme is used to collect information from healthcare professionals and the general public on suspected adverse drug reactions (ADRs). The continued success of the Yellow Card Scheme depends on your willingness to report suspected adverse drug reactions
Both healthcare professionals and patients can submit information through the Yellow Card website





























