Embed Size (px)
Citation preview

1
Anesthesia
Distributed Research Networks and Opioids: A Veterans Health Affairs
Perspec=ve
Sesh Mudumbai M.D.,M.S.Assistant Professor, Departmentof Anesthesiology, Periopera6ve, andPain Medicine, Stanford University Schoolof MedicineStaff AnesthesiologistMedical Director for VISN 21 ClinicalInforma6cs Systems and Periopera6ve Analy6cs [email protected]
Jason Simcakoski
JASON SIMCAKOSKI MEMORIAL AND PROMISE ACT
Anesthesia2
LECTURE OBJECTIVES
• Introduc=on to FDA PMR Study 1A• Overview: HCSRN Virtual Data Warehouse
(VDW) within VHA• Use of VDW to evaluate Trajectories of Co--
Prescribing of Benzodiazepines
Anesthesia3
DISCLOSURES
• I have no conflicts of interest that could affect the content of my presenta6on.
• Funded research:– Food & Drug Administra=on PMR Study 3033--1A“A prospec6ve inves6ga6on of the risks of opioid misuse, abuse, andaddic6on among pa6ents treated with extended--release/long ac6ng(ER/LA) opioids for the treatment of chronic pain”– VA HSR&D Merit Grant I01 HX002314--01A1“Choosing Wisely: Barriers to De--implementa6on, Pa]erns, and Costs of Low Value Preopera6ve Tes6ng for Veterans Undergoing Low Risk Procedures”
Anesthesia4

ACKNOWLEDGEMENTS
Anesthesia5
Project Team– Adi6 Kapoor– Paul Chung– Jus6n Chambers– Lori McDonnell– Samantha Regala
Collaborators and Supporters– Laura Wu (CSP)– Randall Stafford (Stanford)– Steve Asch (Ci2i)– Todd Wagner (HERC and Ci2i)– David Clark (Anesthesiology)– Edward Mariano (Anesthesiology)– Jodie Tra`on (PERC)– Ciaran Phibbs (HERC)– Mei--Chiung.Shih (CSP)– Jennifer Lee (CSP)
Special Thanks: Dr. Ronald Pearl, Dr. Edward Mariano
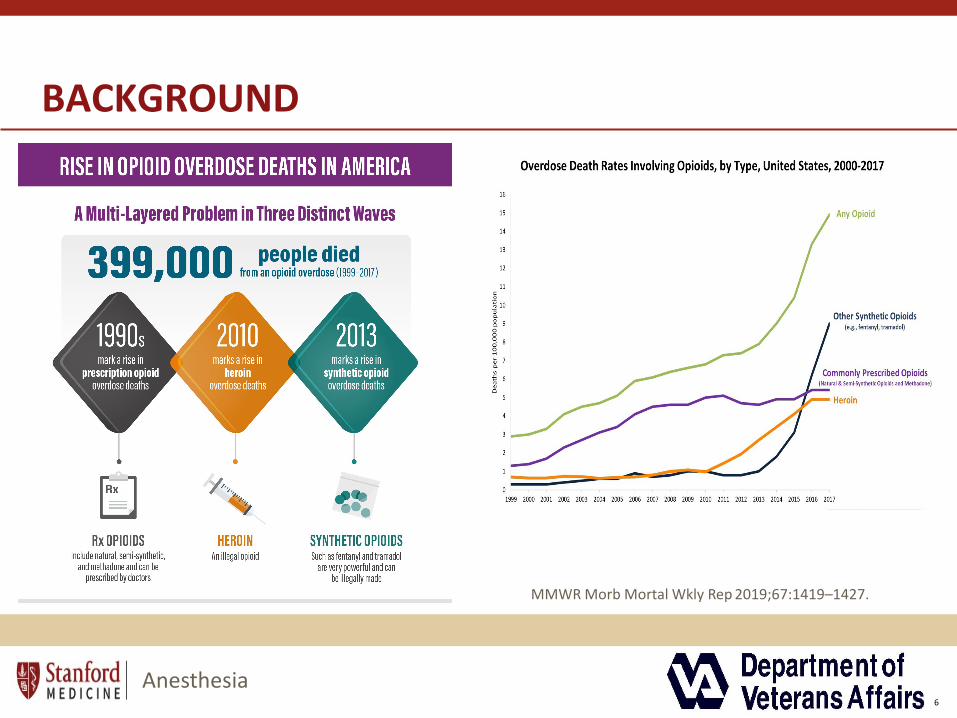
BACKGROUND
MMWR Morb Mortal Wkly Rep 2019;67:1419–1427.
Anesthesia6

LONG TERM RISKS AND BENEFITS OF OPIOIDS?
Anesthesia 77
• Magnitude of misuse, abuse, and addic6on among pa6ents who are treated with opioids for chronic pain?
• Insufficient data to es6mate how the risk of these outcomes varies by the presence of risk factors (other substance use and psychiatric disorders), among pa6ents treated with opioids over the long--term?
Chou R, Deyo R, Devine B, Hansen R, Sullivan S, Jarvik JG, Blazina I, Dana T, Bougatsos C, Turner J. The effec6veness and risks of long--term opioid treatment of chronic pain. Evidence report/technology assessment no. 218. (Prepared by the Pacific Northwest Evidence--basedPrac6ce Center under contract no. 290--2012--00014-- I). AHRQ publica6on no. 14-- E005-- EF. Rockville (MD): Agency for Healthcare Research and Quality; 2014

D E P A R T M E N T O F H E A L T H A N D H U M A N S E R V I C E S
F o o d a n d D r u g A d m i n i s t r a t i o n[ D o c k e t N o . F D A – 2 0 1 4 – N – 0 3 7 4 ]
P o s t m a r k e t i n g R e q u i r e m e n t s f o r t h e C l a s s - W i d e E x t e n d e d - R e l e a s e / L o n g -A c t i n g O p i o i d A n a l g e s i c s ; P u b l i c M e e t i n g ; R e q u e s t f o r C o m m e n t s
Exis6ng pharmacovigilance framework (i.e. FDASen6nel Ini6a6ve) insufficient.
Anesthesia8
BACKGROUND
FDA POSTMARKETING REQUIREMENT
• Es=mate the incidence of misuse, abuse, addic=on, overdose, and death associated with long--term use of opioids for chronic pain.
• Evaluate and quan=fy other risk factors for misuse, abuse, addic=on, overdose, and death associated with long--term use of opioids for chronic pain,
Anesthesia9

Anesthesia
Conceptual Model
11
Anesthesia
DATA SOURCES
EHRPa6ent
Reported Outcomes
Gene6c Samples
Data

Prospec=ve Study
Inclusion Criteria
30 days of new ER/LA opioid use*Age 18--79 years at incident prescrip6onEnrolled with medical and drug benefit for at least 12 months prior to incident use of opioids (HCSRN and VA only as enrollment is N/A to PBRNs)And2+ visits to par6cipa6ng clinic during 12 months prior to incident use of opioids (PBRN, HCSRN, and VA)Addi6onal prescrip6on/ order for an ER/LA opioid following at least 30 days of new useAbility to complete interview/self--administered ques6onnaires in EnglishWilling to provide informed consentExclusion Criteria
Not using an ER/LA opioid at the 6me of recruitment (self-- report)Cogni6ve impairment that interferes with the ability to consent or par6cipate in the interview, unavailable for 12 months of follow--up, or receiving hospice care as determined at the 6me of recruitmentDiagnosis of a terminal illness in the prior 12 months*New use defined as prescrip6on or prescrip6ons las6ng at least 30 days and no ER/LA opioid use in the prior 12 months. Prior IR opioid use allowed.
Cross--sec=onal study –same eligibility criteria except opioid users for at least 1 year and mustinclude 1+ prescrip6ons for ER/LA opioid
ELIGIBILITY CRITERIA

Anesthesia
Group Health Coopera=ve Seacle, WA
Kaiser Permanente Northwest Portland, OR
Kaiser Permanente Southern California Pasadena, CA
Henry Ford Health SystemsDetroit, MI
Geisinger Health SystemDanville, PA
Meyers Primary Care Ins=tute Worcester,MA
Albert Einstein College of Medicine, New York, NY
University of Florida Gainesville,FL
Veterans Administra=onPalo Alto, CA
Clinical DirectorsNetworkNew York, NY
1A Par=cipa=ng Study Sites
1313

WHY VA?
• High risk, vulnerable popula6on• Promotes generalizability• Lower socioeconomic strata• High prevalence of chronic pain; mental health
and substance use disorders• Detailed pharmacy data; longitudinal records• Mul6--year, mul6--healthcare system
collabora6on. Data may not be exported outside of VA.
Anesthesia14

DISTRIBUTED RESEARCH NETWORKS
Anesthesia15

DISTRIBUTED RESEARCH NETWORK
Anesthesia16
• Need for an efficient, reusable infrastructure• Assemble and analyze rou6nely collected healthcare
data• Rapidly generate reliable informa6on about
u6liza6on and outcomes of care needed to support decision making.
• Allows data holders to maintain physical and logical control over their data.
Ins6tute of Medicine. Ini6al Na6onal Priori6es for Compara6ve Effec6veness Research. June 2009

HCSRN EXAMPLE
Care Delivery & Health Plan Data Systems Various ETL
processesVDW data
remains at sites
HMORNParent Organizations
HMORNResearch Organizations
Multisite Project Team
VDW
VDW
Extraction of Limited orDe-identifed Data
Site A
VDWQA Feedback
Site B
Site C
Anesthesia17
DISTRIBUTED RESEARCH NETWORKS
Key Func6ons:• Distribute queries through network so`ware;• Execute the queries against the local data; and• Return aggregated results to the end--user.• Support both simple, menu--driven querying and
complex queries using customized analysis code.
Anesthesia18

FRAMEWORK TO POOL DATA USING VDW
P A V A U F M M C
EACH
SITE
HOU
SETH
EIR
OW
NVD
W
1 . C O H O R T I D E N T I F I C A T I O N A N D A N A L Y S I S D A T A S E T C R E A T E D U S I N G N D C2 . W E E K L Y N D C M A I N T E N A N C E A N D C O H O R T U P D A T E S
3 . C O H O R T A N D A N A L Y T I C D A T A S E T S S E N T T O G R O U P H E A L T H F R O M A L L S I T E S
G r o u p H e a l t h , c r e a t i n g s a s p r o g r a m s t h a t is r u n b y e a c h s i t e o n t h e i r V D W
K P N W D C C r e s p o n s i b l e f o r h e l p i n g t h e 3 s i t e c r e a t e t h e i r o w n V D W , i n c l u d i n g
r u n n i n g t h e Q A r e s u l t s
K P N W
K P S C
G e i s i n g e r
M e y e r s
P A V A
U F
M M C
P I L O T
S T E P 1S T E P 2
H e n r y F o r d
Anesthesia19

INITIAL FOCUS: VDW
Anesthesia20
Virtual Datawarehouse (VDW) development: A framework to share datawith Health Care Systems Research Network healthcare system.
The data warehouse normalizes VA data elements i.e. PHARMACY with HealthCare Systems Research Network data model.
Key Tables such as:o Demographicso Enrollmento Providero Encountero EverNDCo Pharmacyo Diagnoseso Procedureso Contacto Death

RELATIONAL DATABASE FOR VDW
AnesthesiaCourtesy from ‘MUSE Study’ 21

KEY ASPECTS FOR VDW
Anesthesia22
Data from October 2015 to present from VA EMR to populate the VDW tables.The intent of star6ng at October 2015 to minimize code complexi6es due
to the switch from ICD--9 to ICD--10.ALL pa6ents included, not just those who meet the project eligibility
criteria -- En6re popula6on be used for repor6ng purposesDynamically updated weekly and monthly

KEY USAGES WITH VDW
Anesthesia23
Weekly Workplan process for cohort development with VDWQuality assurance (QA) program via SAS for VDW tables at each siteMonthly descrip6ve reports on VDW tables to the lead siteAnaly6cal datasets for the study and FDA repor6ng.

KEY CONSTRAINTS FOR VDW
Anesthesia24
VDW database developed using Microso` SQLAll data transferred to SAS datasets to be accessible via SAS.All centralized QA, cohort iden6fica6on, and analysis programs distributed
via SAS.A site metadata dic6onary for mapping CDW to VDW
5 Steps for Pharmacy Data from CDW to VDW
1. Target to Source Mapping2. Data Query3. Quality Assurance4. Documenta=on5. Submit
EverNDC, Pharmacy tablesCDW EverNDC and RX tables
Anesthesia25

26
Anesthesia
Target table -- Ever NDC• The EVERNDC table is a lookup table containing all Na6onal Drug Codes (NDC)
found in t• Pharmacy
he PHARMdispensing
ACY table ats occurring a
each site.t site A will have at least one corresponding
RNDC table but not necessarily any records in site B'srecord in EVERNDC
site A's EVE table.
Variable Name
NDC HIPAA/CMS/NCPDP standard 5--4--2
Defini6on
The Na6ona configura6o
l Drug Code in the n without dashes
GENERIC
BRAND
The genericother labelsThe brand n
name of the drug expungedame of the drug in
n all upper case with form, strength, and
all upper case with form, strength, and other
UREUNIT_OF_MEAS
STRENGTH
labels expuThe unit of cleaning exc The drug str cleaning exc
ngedmeasure as reporte ept for storing valu ength as reported ept for storing valu
d in source data without standardiza6on or es in all upper case
in source data without standardiza6on or es in all upper case
Target Column Primary KeyForeign Key
Source Table/View
Source Column Transforma6on Rule
NDC PK, FK RxOut_RxOutpatFill
NDC straight move
GENERIC PK DIM.Na6onalDrug
DrugNameWithDose
na6onalDrug.na6onalDrugSID =RxOut_RxOutpatFill.na6onalDrugSID; na6onalDrug.sta3n = RxOut_RxOutpatFill.sta3n
BRAND Src.RxOut_RxOutpat
tradeLabelNam ie
na6onalDrug.na6onalDrugSID =RxOut_RxOutpat.na6onalDrugSID; na6onalDrug.sta3n = RxOut_RxOutpat.sta3n;
UNIT_OF_MEASURE dim.drugUnit drugUnit na6onalDrug.na6onalDrugSID =RxOut_RxOutpatFill.na6onalDrugSID; Na6onalDrug.drugUnitSID = drugUnit.DrugUnitSID; na6onalDrug.sta3n = RxOut_RxOutpatFill.sta3n = drugUnit.sta3n
STRENGTH DIM.Na6onalDrug; dim.drugUnit
Strength,drugUnit
na6onalDrug.na6onalDrugSID =RxOut_RxOutpatFill.na6onalDrugSID; Na6onalDrug.drugUnitSID = drugUnit.DrugUnitSID; na6onalDrug.sta3n = RxOut_RxOutpatFill.sta3n = drugUnit.sta3n
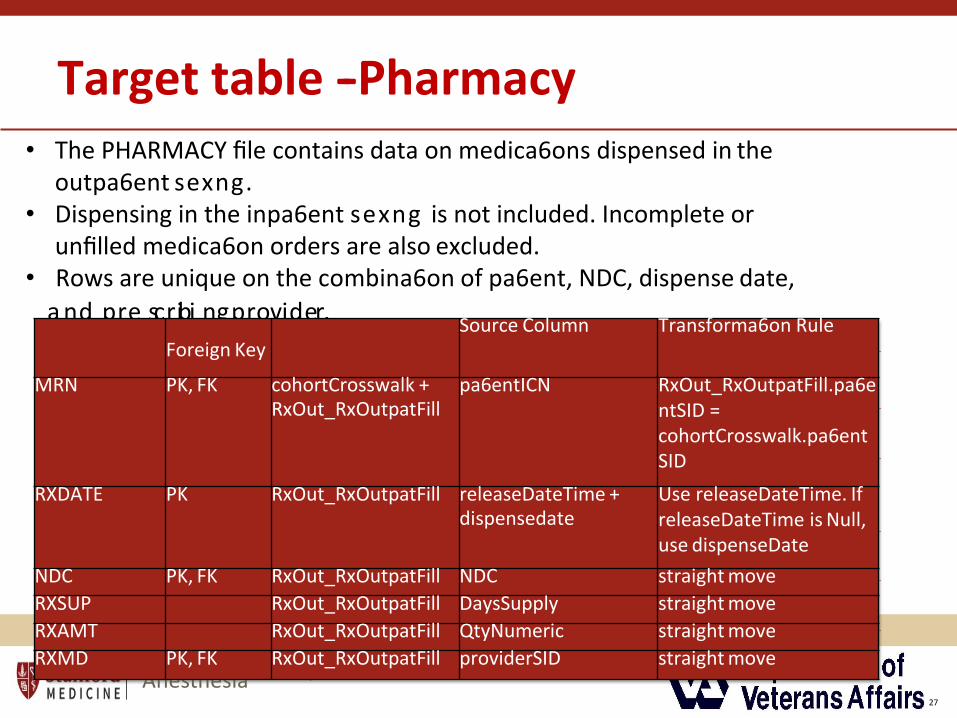
Target table -- Pharmacy
Variable Na
Anesthesia27
me Defini6on Medical record number is the unique pa6ent iden6fierMRN
RXDATE
within a site an
Date that medi
The Na6onal Dr
d should never leave
ca6on was dispense
ug Code in the HIPA
the site
d
A/CMS/NCPDPNDC
RXSUP
standard 5--4--2
Number of days
configura6on withou
of medica6on supp
t dashes.
lied
RXAMT Number of units (e.g. pills, tablets) dispensed
RXMD The provider that prescribed this medica6on
• The PHARMACY file contains data on medica6ons dispensed in the outpa6ent sexng.
• Dispensing in the inpa6ent sexng is not included. Incomplete or unfilled medica6on orders are also excluded.
• Rows are unique on the combina6on of pa6ent, NDC, dispense date,
Taargnedt CporluemscnrPibriimnagrypKreoyvSioduerrc.eTable/ViewForeign Key
Source Column Transforma6on Rule
MRN PK, FK cohortCrosswalk +RxOut_RxOutpatFill
pa6entICN RxOut_RxOutpatFill.pa6entSID = cohortCrosswalk.pa6ent SID
RXDATE PK RxOut_RxOutpatFill releaseDateTime +dispensedate
Use releaseDateTime. IfreleaseDateTime is Null, use dispenseDate
NDC PK, FK RxOut_RxOutpatFill NDC straight moveRXSUP RxOut_RxOutpatFill DaysSupply straight moveRXAMT RxOut_RxOutpatFill QtyNumeric straight moveRXMD PK, FK RxOut_RxOutpatFill providerSID straight move
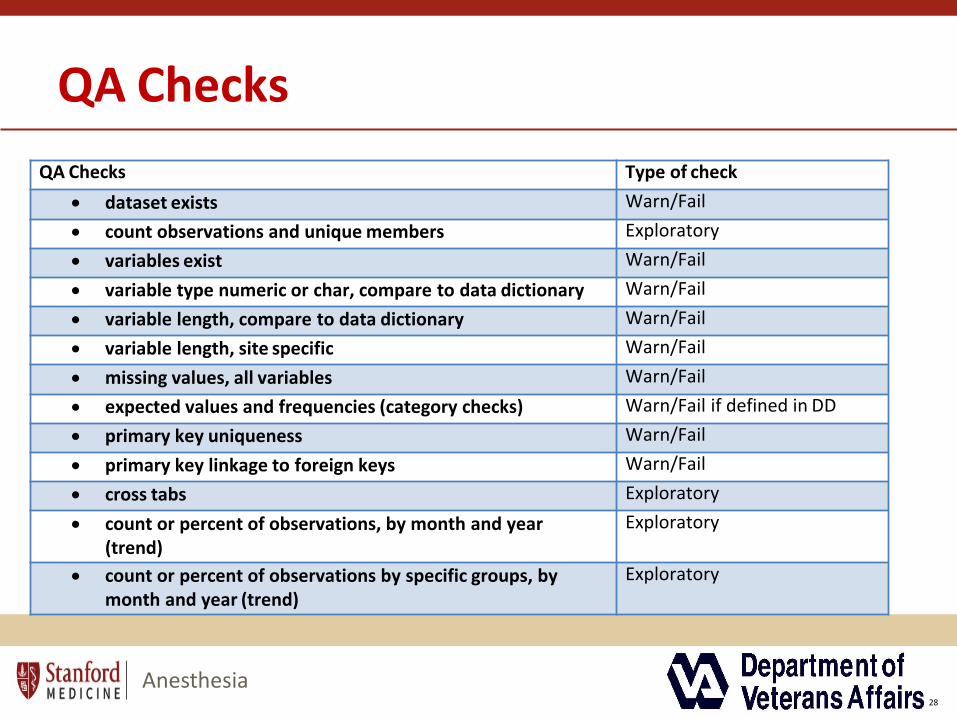
QA Checks
Anesthesia28
QA Checks Type of check• dataset exists Warn/Fail• count observations and unique members Exploratory• variables exist Warn/Fail• variable type numeric or char, compare to data dictionary Warn/Fail• variable length, compare to data dictionary Warn/Fail• variable length, site specific Warn/Fail• missing values, all variables Warn/Fail• expected values and frequencies (category checks) Warn/Fail if defined in DD• primary key uniqueness Warn/Fail• primary key linkage to foreign keys Warn/Fail• cross tabs Exploratory• count or percent of observations, by month and year
(trend)Exploratory
• count or percent of observations by specific groups, by month and year (trend)
Exploratory
Lessons Learnt
• VDW development –federated database challenging and painstaking due to its intensive itera6ve process
• Discussions needed on documenta6on early
Anesthesia29

TRAJECTORIES
• “The course of an outcome or observa6on over 6me or age”
• Can approximate how clinicians approach problems:– How are they doing now?– How did they get here?– Where will they go?
Hypertension. 2017;70:508--514
Anesthesia30

GROUP BASED TRAJECTORY MODELING (GBTM)
Anesthesia31
Iden6fies dis6nc6ve clusters of individual trajectorieswithin the popula6on
–Distribu6on of outcome (biomarkers) condi6onal on6me
–Popula6on: a mixture of dis6nct groups defined by theirtrajectories
–No assump6ons on distribu6on of trajectories.
–PROC Traj in SAS; R package lcmm

MODEL CHOICE
Anesthesia32
• Maximize Bayesian Informa6on Criterion (BIC)
𝐵𝐵𝐼𝐼𝐶𝐶=log 𝐿𝐿 −0.5𝑘𝑘log𝑁𝑁
L=value of the model’s maximum likelihood N=sample sizeK=the order of the polynomial used to model each trajectory and the number of groups
• Domain Knowledge

Trajectories of Concurrent Benzodiazepine Use in VHA Pa=ents Prescribed Opioids
Anesthesia33
• In about one--half of the deaths involving opioid analgesics, morethan one type of drug was specified as contribu6ng to the death,with benzodiazepines being the most frequent
• Within the Veterans Health Administra6on (VHA),benzodiazepines are o`en co--prescribed for outpa6enttreatment for pa6ents diagnosed with chronic pain and takingopioids.
• Given poten6al risks for seda6on or overdose, gaps remain inunderstanding the longitudinal pa]erns of underlyingbenzodiazepine consump6on.
• Objec=ves: 1) pa]erns of benzodiazepine use within a largeter6ary referral center; and 2) sub--groups of pa6ents along withtheir trajectories of overall benzodiazepine use
METHODS
Anesthesia34
• Cohort : VA Palo Alto : 10/01/2014 to 09/30/2017; >=3prescrip6ons for opioids and benzodiazepines + Z--classmedica6ons (zolpidem)
• Outcome: Valium equivalents (VEQ)
• Predictors: Demographics; Medica6on use ;Diagnoses; Co-- morbidi6es
• Analyses– Descrip6ve sta6s6cs– Group--based Trajectory Analysis– Overdose rates
RESULTS
Anesthesia35
Total= 2708 pa6ents----75%(benzo): 2031; Z--class: 677
Overall, older ( >50), male, white, had a lower comorbidity index, with a high prevalence of mental health diagnoses including depression, post--trauma6c stress disorder, chronic pain; and generalized anxiety disorder

RESULTS
Anesthesia36

RESULTS
Anesthesia37

RESULTS
Anesthesia38
CONCLUSIONS
Anesthesia39
• Majority of our pa6ents on opioid therapy were prescribed benzodiazepines with a significant percentage being prescribed Z--class medica6ons
• Pa6ents showed stable trajectories overall and when stra6fied by opioid daily MEQ dosing.
• Within the VHA, intensive management has resulted in stable use over 6me.
• Given ongoing concerns for respiratory depression withconcurrent benzodiazepine use, a]en6on may be moredirected to opioid dose escala6on.
THANK YOU!
Anesthesia40

RESULTS
Bup/Nal Groups differ• Age
(1=younger)• Comorbidity
levels (1=healthier)
• Depression (2 and 3)
Anesthesia41

Ques=ons?
Thank You !
Anesthesia42

References
Anesthesia43
• Brown J, Syat B, Lane K, et al. Blueprint for a distributed research network to conduct popula6on studies and safety surveillance. Effec6ve Health Care Research Report No. 27. (Prepared by the DEcIDE Centers at the HMO Research Network and the University of Pennsylvania Under Contract No. HHSA29020050033I T05.) Rockville, MD: Agency for Healthcare Research and Quality. June 2010. Available at: h]p://effec6vehealthcare.ahrq.gov/reports/ final.cfm.

Drug and Opioid--Involved Overdose Deaths — United States, 2013–2017. MMWR Morb Mortal Wkly Rep. ePub: 21 December 2018
Age--adjusted rate of drug overdosedeaths, by state —2013 and 2017
Background
Anesthesia44
Anesthesia45

DRN
Anesthesia46
• What are they?• Why are they useful?• Example of one?• The alterna6ve, distributed network configura6on leaves the data holder in
control of their protected data. The FDA Mini--Sen6nel program (an ac6ve surveillance system for monitoring the safety of FDA regulated medical products) is a good example. Queries are sent to each node (organisa6on) in the network. They each return results (o`en aggregated) in an agreed common data model, to a coordina6ng centre. A mapping must be agreed between each node and the common data model and the distributed implementa6on is more complex than the centralised approach. However, it overcomes many of the privacy issues and the par6cipa6ng organisa6ons maintain opera6onal control of their data (Brown 2015) . They may even choose to review each query before releasing the data.

Domains from CDW
Anesthesia47

Data Query -- Results
Pharmacy Table EverNDC Table

Anesthesia
Opioid RX Data for Study

Anesthesia
Data Query --Design
50

Anesthesia
Data Query --Design
51
Examples of DRNs
Anesthesia52
• Collabora6ve Research with Electronic Clinical Data ◊ Collabora6ve ResearchEnvironments –AHRQ ARRA Grants to Build Infrastructure for CER: PROSPECTStudies Enhanced Registries Distributed Research Networks (DRN) Electronic DataMethods (EDM) FORUM –Provide input at www.edm--forum.orgwww.edm--forum.org –DARTNet
• –Mini--Sen6nel (FDA)• –Observa6onal Medical Outcomes Partnership (OMOP) –HMO Research Network
(HMORN) –AHRQ Effec6ve Healthcare Program (DEcIDE) –Dartmouth CareCollabora6ve –VA Informa6cs and Compu6ng Infrastructure (VINCI) –NCRR -- CTSAprojects: Physio--MIMI, i2b2, TRIAD, REDCap 28
Distributed Research Networks
Anesthesia53
• A large public--private CER enterprise.
• Support high-- efficiency, pragma6c randomized trials
• Require large--scale clinical and administra6ve data networks that enable observa6onal studies of pa6ent care while protec6ng pa6ent privacy and data security.
Ins6tute of Medicine. Ini6al Na6onal Priori6es for Compara6ve Effec6veness Research. June 2009

Key Steps to assemble VDW
Anesthesia54
IRB and DART Approval–VINCI Workspace– CDW--Domain Checklist: Used to specify any CDW
Produc6on or Raw Domains the study might needto use..
–Real SSN Access Requests








![Welcome [med.stanford.edu]med.stanford.edu/.../aboutus/2017-MIPS-brochure.pdf · via sound (ultrasound, photoacoustic), magnetism (MRI or magnetic resonance imaging, MPI or magnetic](https://img.pdfslide.us/doc/110x75/5f0c64747e708231d4352ce6/welcome-med-med-via-sound-ultrasound-photoacoustic-magnetism-mri-or-magnetic.jpg)




















