Disorders of the eye
Disorders of the eyeIsaac AmankwaaDefinition of TermsVision:
Passage of rays of light from an object through the cornea, aqueous
humor, lens, and vitreous humor to the retina, and its appreciation
in the cerebral cortex.Emmetropia: Normal vision: rays of light
coming from an object at a distance of 20 feet (6 m) or more are
brought to focus on the retina by the lens.I. Amankwaa2Definition
of termsAmetropia: Abnormal vision.Myopia:
NearsightednessHyperopia: Farsightedness
I. Amankwaa3Definition of termsAccommodation: Focusing apparatus
of the eye adjusts to objects at different distances by means of
increasing the convexity of the lens (brought about by contraction
of the ciliary muscles).Presbyopia: The elasticity of the lens
decreases with increasing age; an emmetropic person with presbyopia
will read the paper at arm's length and will require prescription
lenses to correct the problem.I. Amankwaa4Definition of
termsAstigmatismrefractive error in which light rays are spread
over a diffuse area rather than sharply focused on the retina, a
condition caused by differences in the curvature of the cornea and
lens .
I. Amankwaa5Definition of termsEnucleation: complete removal of
the eye-ball and part of the optic nerve exenteration: surgical
removal of the entire contents of the orbit, including the eye-
ball and lids evisceration: removal of the intraocular contents
through a corneal or scleral incision; the optic nerve, sclera,
extraocular muscles, and sometimes, the cornea are left intact
I. Amankwaa6Common AbbreviationsOD (oculus dexter) or RE- right
eyeOS (oculus sinister) or LE- left eyeOU (oculus unitas)both
eyesIOPintraocular pressureIOLintraocular lensEOLextraocular
lens
I. Amankwaa7EYE CARE SPECIALISTSOphthalmologist: Physician
specializing in diagnosis, surgery, and treatment of the eye.
Ophthalmology specialists may focus their practice on a specific
part of the eye or disorder, such as a cornea specialist or
glaucoma specialist.Optometrist: Doctor of optometry who can
examine, diagnose, and manage visual problems and diseases of the
eye, but does not perform surgery.Optician: Fits, adjusts, and
gives eyeglasses or other devices on the written prescription of an
ophthalmologist or optometrist.Ocularist: Technician who makes
ophthalmic prostheses.I. Amankwaa8Nursing Care of patients
undergoing eye surgeryI. Amankwaa9Specific pre-op carePhysical
OrientationAssist the patient to learn details of his room such as
the location of furniture, doors, windows, and so forth.Familiarize
patient with the voices of those who will care for him after
surgery.Familiarize him with the daily sounds and noises in the
environment, since he will be more aware of sound without his
vision.
I. Amankwaa10Specific pre-op careObservationThe patient should
be observed for tendencies to cough or sneeze (smoker's cough,
allergies, and so forth). I. Amankwaa11Specific pre-op
careEducation.The patient must understand the objective of resting
the eyes & avoiding actions that increase intraocular
pressure.The head must be kept very still.No reading.No showers, no
shampooing, no tub baths.No bending over at the waist.No lifting of
heavy objects.No sleeping on the operative side. If both eyes are
affected, the patient must sleep on his back.I. Amankwaa12Specific
pre-op carePhysical Preparation.Instruct patient to wear dark
glasses if atropine drop have been usedA bowel prep is done the
evening prior to surgery to prevent the patient from straining at
stool during the immediate post-op period.Prepare the affected eye
by cleaning the skin of the side of the faceI. Amankwaa13Specific
pre-op carePhysical Preparation.Shaving of eyebrows, cutting of
eyelashes, and shaving of face should be done only on the order of
the surgeon.After the patient has been taken to surgery, prepare a
post-op bed, ensuring that the bed is equipped with side rails.Sand
bags should be made available for use in immobilizing the head.I.
Amankwaa14Post-operative careReturn from Surgery.The patient must
be lifted off the stretcher, he is not to move himself.The patient
should be positioned on his back or turned to the un-operated side
or as prescribed by the physician.Sandbags should be used to
immobilize the patient's head, if ordered.I.
Amankwaa15Post-operative careReturn from Surgery.If both eyes are
bandaged (they normally are), the side rails MUST be raised at all
times to protect the patient in the event he becomes disoriented
and attempts to get out of bed.Place the call bell within easy
reach of the patient's head and let the patient know exactly where
it is located.I. Amankwaa16Post-operative careReturn from
Surgery.Remind the patient that he should not cough, sneeze, or
blow his nose. him to inform the staff if he feels the urge, since
these actions will increase intraocular pressure.Eye pad and eye
shield should be kept in placeI. Amankwaa17Post-operative
careOrientation.Reinforce the physical orientation given during the
preoperative period by verbally reviewing the locations of objects
in the room.Orient the patient to other people in the room.The
patient should have an awareness of his surroundings and know what
to expect to avoid being startled or frightened.
I. Amankwaa18Post-operative carePrecautions.Avoid dislodgement
of the eye dressings by securing them with an eye shield or
reinforcing loose tape.Restrain the arms of children and
disoriented or uncooperative patients, as appropriate. Avoid
jarring or bumping the bed, as this may startle the patientI.
Amankwaa19Post-operative carePrecautions.A sleeping patient must be
watched constantly to ensure that proper positioning is maintained.
If the patient is newly blinded as a result of the surgery, observe
for depression and take precautions if patient is potentially
suicidalI. Amankwaa20Post-operative carePrecautions.Check the
physician's orders before giving anything by mouth. Nausea and
vomiting must be avoided.Additionally, the motion of chewing may be
contraindicatedI. Amankwaa21Post-operative careApproaching the
PatientALWAYS speak to the patient upon entering his area and
before touching him.Allay the patient's fears by explaining each
procedure or activity fully.Continue to reinforce his orientation
to the surroundings.Always let the patient know when you are
leaving his area.
I. Amankwaa22Post-operative careDiversional Activity.Provide
activities that are not fatiguing to the eyes if the eyes are not
bandaged.No readingMinimal televisionEncourage visitors to chat
with the patient or read to him.I. Amankwaa23DISORDERS OF THE EYE
LID
Hordeolum (stye)Chalazion (Meibomian
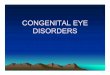
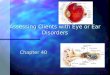
cyst)BlepharitisEntropionEctroponI. Amankwaa2424Structure of the
eyelidThe eyelid is made up of the Skinit is thin and characterized
by absence of fat.Muscle layerOrbiclaris oculi consist of
horizontal concentric fibres. levator palpebral superioris.The end
in an aponeurosis which is insertedTarsus Consists of dense fibers
tissue.Embidded in it are enormously developed sebaceous glands-the
meibomian glands.Mucous layerformed by the palpebral conjunctivaI.
Amankwaa25Structure of the eyelid
I. Amankwaa2626Glands of the eyelidMeibomian glands: They are
embedded in the tarsus and are modified sebaceous glands. They
secret an oily secretion. They open through vertically arranged
ducts into the lid margin.Glands of zeis: They are sebaceous glands
developed as outgrowth of the hair follcles of the eye lashes. They
are situated at the margin.Glands of moll: These are modified sweat
glandsI. Amankwaa27Eyelid marginEye lashes-arranged in 2-3 rows
anteriorly.Opening of the ducts of the meibomian gland
posteriorly.Glands of zies and moll
I. Amankwaa28Inflammation of the eyelidI. Amankwaa29HordeolumThe
term stye refers to an inflammation or infection of the glands and
follicles of the eyelid marginThere are two typesExternal Hordeolum
(stye)Internal HordeolumI. Amankwaa30Hordeolum External hordeolum
(stye) Acute bacterial infection of the lash follicle and its
associated gland of Zeis or Moll Internal hordeolum Acute bacterial
infection of Meibomian gland Infection usually staphylococcal I.
Amankwaa3131Acute hordeola Staph. abscess of Meibomian glands
Tender swelling May discharge through skin or conjunctiva Staph.
abscess of lash follicle and gland of Zeis or Moll Tender swelling
at lid margin May discharge through skinInternal hordeolum ( acute
chalazion )External hordeolum (stye)
Hordeolum s/sRed swelling appears in the lash line of the margin
of the lidPaintenderness edema of the lidsI.
Amankwaa3333HordeolumDiagnosisVisual examculture if
neededTreatmentHot compress to alleviate painTopical or systemic
antibioticsI. Amankwaa3434HordeolumTreatment and Nursing
Considerationwarm soaks to promote drainage, good hand washing and
eyelid hygieneTopical or systemic antibioticsIn some cases,
incision and drainage may be necessary. Teach patient how to clean
eyelid margins and not to squeeze the stye.I. Amankwaa3535CHALAZION
(MEIBOMIAN CYST)DefinitionA chalazion is noninfectious obstruction
of a meibomian gland causing extravasation of irritating lipid
material in the eyelid soft tissues with focal secondary
granulomatous inflammation.I. Amankwaa3636CHALAZION (MEIBOMIAN
CYST)Etiology, PathologyThe meibomian duct becomes obstructed
through proliferation of its epithelium and consequently the gland
enlarges.The fatty secretion escapes into the surrounding
tissue
I. Amankwaa3737Chalazion DiagnosisVisual
ExaminationTreatmentsmall ones usually disappear spontaneously
after a month or twolarge ones usually need surgical removalI.
Amankwaa3838
Treatment of chalazionInjection of local anaestheticInsertion of
clamp
Incision & curettageDifference between chalazion and
hordeolumChalaziatend to develop farther from the edge of the
eyelid than styes. Chalazion often larger thanstye,chalaziausually
isn't painful. Chalazion is not caused by an infection from
bacteria, Sometimes, when a astyedoesn't heal, it can turn into
achalazion
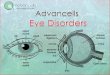
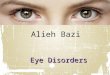
I. Amankwaa40pterygiumI. Amankwaa41Definition of pterygiumA
pterygium is a fleshy growth that invades the cornea. It is an
abnormal process in which the conjunctiva grows into the
cornea.
I. Amankwaa42
PterygiumThere are two types:Progressive Pterygium: These types
of pterygium are those which progress day by day.
Non Progressive Pterygium: Those which after limited growth has
been occur than stop their generationI. Amankwaa43Pterygium-
causesThe exact cause is not known.The probable causes are:Commonly
occurs in people living in hot & dry climate.Dusty
atmosphere.Common in outdoor workers.Common in males.It may occur
nasal than temporal side.
I. Amankwaa44symptomsRedness Irritation Dryness Tearing May
cause decreased vision ( when it reaches the visual axis of
cornea)I. Amankwaa45Treatment Local:Lubricant eye drops.Topical
steroids for inflammation.
Surgical:Surgical excision when the pterygium progressive
towards the cornea.
I. Amankwaa46
Precautions
cataractI. Amankwaa48Cataract DefinitionA cataract is a lens
opacity or cloudiness Clouding or opacity of the crystalline lens
that impairs vision.IncidenceCataract is the leading cause of
blindness in the worldCommon in individuals above 70 yrs
I. Amankwaa49Pathophysiology Cataract formation is characterized
chemically by a reduction in oxygen uptake and initial increase in
water content This is followed by dehydrationSodium and calcium
contents are increased
I. Amankwaa50Pathophysiology Potasium, ascorbic acid and protein
are decreased.The protein in the lens undergoes numerous age
related changes including yellowing.I. Amankwaa51Pathophysiology
Cataract progresses through the following clinical stages of
developmentImmature cataracts are not completely opaque, and some
light is transmitted through them, allowing useful visionMature
cataracts are completely opaque. The former term for this stage was
ripe. Vision is significantly reduced
I. Amankwaa52Pathophysiology Hyper-mature senile cataractCortex
is disintegrated and transformed Morphological
classificationSubcapsular cataractAnterior subcapsular
cataractPosterior subcapsular cataractNuclear cataract involves the
nucleus of the lensYellow to brown colorationCortical
cataractWedge-shaped or radial spoke-like opacitiesPolar cataractI.
Amankwaa54I. Amankwaa55
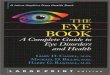
Nuclear cataract Central opacity in lensAssociated with
myopiaWorsen on progression
I. Amankwaa56CorticalInvolve the interior and posterior
equatorial cortex of the lensWorst in very bright light
I. Amankwaa57Posterior sub-capsular occurs in front of posterior
capsuleMostly occurs in younger individualsAssociated with
prolonged use of corticosteroids, diabetes, ocular traumaNear
vision is diminished
I. Amankwaa58Classification according to maturityAn immature
cataractA mature cataractHypermature cataractA morgagnian
cataract
I. Amankwaa59Etiological classificationSenile cataracts develop
in elderly peopleDue to chemical changes in lens proteinCongenital
cataracts occur in neonates Due to inborn errors of metabolism or
maternal rubella infectionI. Amankwaa60Etiological
classificationTraumatic cataractDevelops after a foreign body
injures the lens with sufficient force to allow aqueous or vitrous
humor to enter the lens capsule
I. Amankwaa61Causes and Risk FactorsCigarette smoking Long term
use of corticosteroids, especially high dosesSun light and ionizing
radiationDiabetesObesityEye injuries
cataracts 62CLINICAL MANIFESTATIONPainless, blurred visionThe
person perceived that surroundings are dimmerLight scattering is
commonMonocular diplopiaReduce visual acuity
cataracts 63Assessment and Diagnostic FindingsDecreased visual
acuity is directly proportionate to cataract density.The Snellen
visual acuity test, ophthalmoscopy, and slit lamp biomicroscopic
examination are used to establish the degree of cataract formation.
The degree of lens opacity does not always correlate with the
patients functional status.Some patients can perform normal
activities despite clinically significant cataracts. Others with
less lens opacification have a disproportionate decrease in visual
acuity; hence, visual acuity is an imperfect measure of visual
impairment.
64Medical ManagementNo nonsurgical treatment cures cataracts. In
the early stages of cataract development, glasses, contact lenses,
strong bifocals or magnifying lenses may improve vision. Reducing
glare with proper light and appropriate lighting can facilitate
reading. 65Medical ManagementMydriatics (atropine) can be used as
short-term treatment to dilate the pupil and allow more light to
reach the retina.66Surgical managementIntracapsular cataract
extraction (ICCE)The entire lens (ie, nucleus, cortex, and capsule)
is removed, and fine sutures close the incision. ICCE is
infrequently usedI. Amankwaa67Surgical managementExtracapsular
cataract extraction (ECCE)ECCE achieves the intactness of smaller
incisional wounds (less trauma to the eye) and maintenance of the
posterior capsule of the lens, reducing postoperative
complications, particularly retinal. In ECCE, a portion of the
anterior capsule is removed, allowing extraction of the lens
nucleus and cortex.
68Nursing ManagementProviding preoperative careTo reduce the
risk for retrobulbar hemorrhage, anticoagulation therapy is
withheld, if medically appropriate. Aspirin should be withheld for
5 to 7 days, nonsteroidal anti-inflammatory medications (NSAIDs)
for 3 to 5 days, and warfarin (Coumadin) until the prothrombin time
of 1.5 is almost reached.69Nursing ManagementProviding preoperative
careDilating drops are administered every 10 minutes for four doses
at least 1 hour before surgery.Additional dilating drops may be
administered in the operating room (immediately before surgery) if
the affected eye is not fully dilated. Prophylactic antibiotic,
corticosteroid, and NSAID drops may be used.70Providing
postoperative careThe nurse provides the patient with verbal and
written instruction regarding how to protect the eye, administer
medications, recognize signs of complications, and obtain emergency
care.The nurse instructs the patient regarding home care The nurse
also explains that there is minimal discomfort after surgery and
instructs the patient to take a mild analgesic agent PRN.
Antibiotic, anti-inflammatory, and corticosteroid eye drops or
ointments are prescribed postoperatively. 71ENTROPIONMechanism
inversion of eye lid into eyeEtiology Aging (course fibrous
tissue)Symptoms and Signsforeign body sensationtearing / itching /
rednessContinuous rubbing causes conjunctivitis or corneal
ulcersDecreased visual acuity if not correctedI. Amankwaa7272I.
Amankwaa73
I. Amankwaa74
EntropionDiagnosisvisual examinationTreatmentclean up on its
ownif not, minor surgeryI. Amankwaa7575ECTROPONMechanismouturned
eye lidsEtiologyElderly (weakness of eye lid muscles)Symptoms and
signsdryness of the exposed part of the eyetears run down the
cheeksif not treated can cause ulcers and permanent damage to
corneaI. Amankwaa7676I. Amankwaa77
EctropionDiagnosisvisual examinationTreatmentminor surgery if
doesnt disappearI. Amankwaa7878BLEPHAROPTOSIS
(PTOSIS)Mechanismweakness of eye muscle that raises eyelid
(superior rectus, superior oblique)EtiologyFamilial traumadiabetes
mellitus muscular dystrophymyasthenia gravis brain tumorsI.
Amankwaa7979BLEPHAROPTOSIS (PTOSIS)Symptoms and signs drooping
eyeblocks visionDiagnosisophthalmic examinationLab investigations
to rule out underlying disease Treatmentsurgery (strengthen
muscles)eye glasses with raised eyelid supporttreat underlying
diseaseI. Amankwaa8080I. Amankwaa81
Ocular TraumaLeading cause of blindness among children and young
adults, especially male trauma victims. Initial intervention
(non-ophthalmic Nurse) is performed in only two conditions:chemical
burns: irrigation of the eye with normal saline solution or even
plain tap water immediatelyForeign body: no absolute attempt is
made to remove the foreign material, small or big, or apply
pressure or patch to the injured eye. The eye must be protected
using a metal shield, if available, or a stiff paper cup.I.
Amankwaa82Assessment and Diagnostic FindingsObtain history (e.g.
preinjury vision in the affected eye or past ocular surgery.Details
related to the injurynature of the ocular injury (e.g. blunt
trauma)type of activity causing the injuryFor chemical eye burns,
the chemical agent must be identied The corneal surface is examined
for foreign bodies, wounds, and abrasionsPupillary size, shape, and
light reaction of the pupil of the affected eye are compared with
the other eye. I. Amankwaa83SPLASH INJURIES- managment Irrigate eye
with normal saline solutionIn cases of ruptured globe, cycloplegic
agents or topical antibiotics must be deferred because of potential
toxicity to exposed intra- ocular tissues. Further manipulation of
the eye must be avoided until the patient is under general
anesthesia. Parenteral, broad- spectrum antibiotics are
initiated.Tetanus antitoxin is administered, if indicated, as well
as analgesics. Any topical medication (e.g., anesthetic, dyes must
be sterile.
I. Amankwaa84Blunt ContusionDefinitionBruising of periorbital
soft tissueS/SSwelling and discoloration of the tissueBleeding into
the tissue and structures of the eyePainDiagnosisTests must
determine if injury to parts of eye and systemic traumaI.
Amankwaa85Blunt ContusionManagementTreatment to reduce swellingPain
management dependent on structures involvedNote: If there is any
possibility of a ruptured globe, a loose patch and shield should be
placed and ocular manipulation discouraged until ophthalmologist
assessment completed.
I. Amankwaa86Orbital FractureDefinitionFracture and dislocation
of walls of the orbit, orbital margins, or bothS/SMay be
accompanied by other signs of head
injuryRhinorrheaContusionDiplopia
I. Amankwaa87Orbital FractureDiagnosisX-ray, computed tomography
(CT)ManagementMay heal on own if no displacement or impingement on
other structuresSurgery (repair the orbital floor with plate
freeing entrapped orbital tissue)I. Amankwaa88Foreign
BodyIntroduction Foreign bodies can be found on the cornea (25% all
ocular injuries), conjunctiva Intraocular particles penetrate
sclera, cornea, globe
I. Amankwaa89Foreign BodyS/SSevere painLacrimationForeign body
sensationPhotophobiaRednessSwellingNote: Wood and plant foreign
body may cause severe infection within hours.
I. Amankwaa90Foreign BodyRemoval of foreign body through
irrigation, cottontipped applicator, or magnetAfter removal of a
foreign body from the surface of the eye, an antibiotic ointment is
applied, and the eye is patchedTreatment of intraocular foreign
body depends on size, magnetic properties, tissue reaction,
locationSurgical removal may be necessaryThe eye is examined daily
for evidence of infection until the wound is completely healedI.
Amankwaa91Laceration/PerforationDefinitionCutting or penetration of
soft tissue or globe S/SPainBleedingLacrimationPhotophobiaI.
Amankwaa92Laceration/PerforationManagementSurgical repairmethod of
repair depends on severity of injuryAntibioticstopically and
systemically complicationsretinal detachment, intraocular tissue
avulsion, and herniation)
I. Amankwaa93Ruptured GlobeDefinitionConcussive injury to globe
with tears in the ocular coats, usually the scleraClinical
manifestationsPainAltered intraocular pressureLimitation of gaze in
field of ruptureHyphemaHemorrhage (poor prognostic sign)
I. Amankwaa94Ruptured GlobeDiagnosis: CT, ultrasound
ManagementSurgical repairVitrectomyScleral
buckleAntibioticsSteroidsEnucleationI. Amankwaa95Burns-Chemical
burnsCausealkali or acid
agentS/SPainBurningLacrimationPhotophobiaI.
Amankwaa96Burns-Chemical burnsManagementCopious irrigation until pH
is 7Severe scarring may require keratoplastyAntibiotics
I. Amankwaa97Burns- Thermalusually burn to eyelidsmay be first-,
second-, or third-degreeS/SPainBurned skinBlisters I.
Amankwaa98Burns- ThermalManagementFirst aidapply sterile
dressingsPain controlLeave fluid blebs intactSuture eyelids
together to protect eyeif perforation a possibilitySkin grafting
with severe second- and third-degree burns
I. Amankwaa99Burns- UltravioletCauseexcessive exposure to
sunlight, sunlamp, snow blindness, weldings/sPaindelayed several
hours after exposureForeign body
sensationLacrimationPhotophobiaNote: Symptoms occur some time after
exposure.I. Amankwaa100Burns- UltravioletManagementPain
reliefCondition self-limitingBilateral patching with antibiotic
ointment and cycloplegics
I. Amankwaa101101HYPHEMADefinitionFrank bleeding into the
anterior chamber following contusion of the globe.It is usually due
to disruption of blood vessels in the iris or ciliary bodyThis
blood usually does not clotwithout bed rest, a red fluid meniscus
is form
HyphemaI. Amankwaa103
Classification Etiological classification Traumatic hyphaema -
most commonly blunt trauma Strenuous conditions - Whooping cough,
Asthma etc. Blood dyscrasia - Aplastic anaemia, leukemia,
hemophilia, von Willebrand disease etc. Neovascularization
(Rubeosis iridis) - Diabetes mellitusI. Amankwaa104Classification
Clinical Mild or simple hyphema (2-3mm)Moderate hyphema (3-5mm)
Severe hyphema more than half of anterior chamberTotal hyphema
anterior chamb full of bloodI. Amankwaa105Causes:Blunt
TraumaIntraocular surgeryLacerating traumaPenetrating and
perforating injuryIt also occurs spontaneously w/o any trauma,
usually neovascularization, tumor of eye (Retinoblastoma), uveitis
or vascular anomaliesUse of medicine which impair blood clotting
such as aspirin and analagesic PathophysiologyThere are 2 suggested
mechanism of hyphema formationDirect contusive force cause
mechanical tearing of blood vasculature of iris and or
angleConcussive trauma creating rapidly rising intravascular
pressure within the vessels resulting in rupture of vesselsSigns
and SymptomsBlurring of
visionPainPhotophobiaTearingGRADINGGradeSize of Hyphema0No layered
bloodcirculating red blood cells onlyILess than 1/3II1/3 to
1/2III1/2 to less than totalIVTotal
Treatment (medical)Sedation or complete bed rest with limited
activitesCycloplegics; Atropine 1% E/D 3. Anti inflamatoty -
Steroids, mild NSAIDs Ocular hypotensive agents in case of IOPPlace
shield or patch over involved eye or both eyes (controversial) Rx
of the causeAspirin and related analgesics w/c impair blood
clotting should not be used to relieve painAcetaminophen may be
substituted.
Treatment (surgical)Surgical Indication:Inc. IOP of >50
mmHgPersistently (5 to 7 days) high pressureEarly blood staining of
the corneaSimple removal of small amount of aqueous humour
(Anterior Chamber Paracentesis) or Irrigation of AC may be
effective
Surgical ManagementClots should never be removed by means of
forceps due to difficulty distinguishing clot from iris. Vitrectomy
irrigator aspirator maybe used to aspirate the blood. Corneal
ContusionDefinitionCorneal contusion is a contusion (blunt trauma)
is caused by the blunt force of the mechanical can cause ocular
adnexal or eye damage, caused by a variety of structural lesions in
the eye.I. Amankwaa115